Introduction
Hookworms are nematode parasites that are usually transmitted through infested soil. They usually affect the poorest individuals in tropical and subtropical areas. Two species are mainly responsible for human infections: Ancylostoma duodenale and Necator americanus. They can cause chronic infection of the intestinal tract and ingest their host's blood, leading to iron-deficiency anemia in most cases. Moreover, pulmonary manifestations may result from larval migration. An estimated 1.38 to 4 million disability-adjusted life years (DALYs) are lost worldwide each year as a result of hookworm infections, which translates into a significant financial burden of 2.4 to 138.9 billion dollars. In tropical areas, hookworm remains a significant neglected tropical disease; however, the estimated worldwide burden has changed somewhat. While multiple medications are available to treat hookworm infections, prevention remains vital in combating complications.[1][2][3][4][5][WHO. Soil-Transmitted Helminth Infections. 2023.]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Ancylostoma duodenale and Necator americanus are the principal species that infect humans. With a pooled prevalence of 12%, Ancylostoma ceylanicum is the second most common hookworm species infecting people in the Asia-Pacific region. Although much less than A duodenale or N americanus, A ceylanicum does cause intestinal blood loss (about 0.03 mL/worm/day from repeated blood meals), despite previous beliefs to the contrary. A ceylanicum has been found in the Americas, including Ecuador, according to recent molecular research, extending its known geographic range beyond Asia. Given the high genetic diversity across Southeast Asia and the emergence of benzimidazole resistance in Ancylostoma ceylanicum, the parasite's zoonotic transmission among humans, dogs, and cats poses a serious One Health concern. Ancylostoma caninum, a dog hookworm, might cause enteritis and ileitis. Ancylostoma braziliense is the primary cause of cutaneous larva migrans.[6][7][8][9][CDC. Zoonotic Ancylostoma Ceylanicum Infection in Coyotes. 2024][Tenorio JC et al. Can Resistant Ancylostoma Ceylanicum Arise and Spread Between Humans and Animals?. 2024]
Epidemiology
Worldwide, approximately 406 to 480 million people are infected with hookworms, with the Global Burden of Disease study 2021 reporting 642.72 million cases. Infection predominates within developing countries and leads to huge losses of economic productivity due to anemia, worsening the already existing poverty and disease. Hookworm infections are responsible for approximately 1.38 to 4 million disability adjusted life years lost annually. Necator americanus causes approximately 79% of human hookworm infections worldwide and predominates globally, while Ancylostoma ceylanicum is a significant third species in the Asia-Pacific (pooled prevalence of approximately 12%, second most common after N americanus there). Ancylostoma duodenale remains endemic to the Mediterranean, the Middle East, northern India, and northern China.
Risk factors for hookworm infection include low socioeconomic status, exposure to infected soil, walking barefoot, poor sanitation, and inadequate personal hygiene. Children and pregnant women are at the highest risk. Transmission is affected by multiple factors, including a warm, moist climate, a contaminated water supply, and poor sanitation.[CDC. About Hookworm. 2024][10][11][1][6][12][13][14]
Pathophysiology
Transmission Mechanisms
In soil, the hookworm eggs hatch, and first-stage rhabditiform L1 larvae develop in a few days. They molt twice to become the infective filariform L3 larvae, which are about 0.5 to 0.6 mm long and can live for 3 to 4 weeks under suitable conditions. The larvae inhabit soil or grass until they come into contact with human skin, at which point they initiate an infection.
Necator americanus larvae penetrate human skin within 5 to 30 minutes, while A duodenale takes 1 to 6 hours, facilitated by larval proteases (N americanus) and hyaluronidase (A duodenale), which degrade the dermal extracellular matrix. Rarely, orally ingested larvae can penetrate the buccal mucosa or pharyngeal epithelium to enter the bloodstream directly, bypassing cutaneous penetration
Skin penetration occurs through a chemical process initiated by proteolytic enzymes produced by certain glands in the larvae. Necator americanus produces proteases that can degrade connective tissue components, eg, collagen and elastin. On the other hand, Ancylostoma larvae produce a hyaluronidase enzyme that degrades the dermal barrier, allowing them to migrate through the skin. One of the significant larval secretions is the Ancylostoma secreted proteins, which are essential for larval development and host immune modulation, and account for about one-third of its secreted proteins.
After skin penetration, the larvae migrate passively through the bloodstream to the right side of the heart and hence to the pulmonary vasculature (see Image. Hookworm Infection). During pulmonary migration, larvae can trigger type I hypersensitivity reactions in some individuals, manifesting as Loeffler syndrome (eosinophilic pneumonia), though the precise immune mechanisms remain incompletely understood. They penetrate the alveoli and migrate through the bronchial tree to the pharynx and then to the intestinal tract.
Once the larvae reach the duodenum and have molted twice, they become L5 immature worms. A duodenale uses teeth-like cutting plates in its buccal capsule to attach to the mucosa, while N americanus uses a cutting plate without true teeth. Ingestion of blood is facilitated by metalloproteases and anticoagulant peptides, which maintain the fluidity of blood flow across mucosal injury by preventing coagulation. However, the process by which hemoglobin is consumed in the parasite's gut is poorly understood. Worms mature in 4 to 6 weeks into adult sexually differentiated worms. After mating, the female produces up to 30,000 eggs per day, which exit the host to continue the lifecycle.
Pathophysiologic Changes
Blood loss in heavily infected persons could reach up to 9.0 mL/day and occurs by 2 mechanisms. The first is through consumption by the parasite, which accounts for a small portion of blood loss. The primary mechanism of blood loss occurs through leakage around the mucosal attachment site. Iron deficiency anemia occurs when the host is unable to compensate for blood loss, especially during heavy infections and in nutritionally deprived individuals. The primary risk factor for anemia is worm burden; in children, however, anemia can occur with a lower worm burden.
Simultaneous protein loss might occur and result in symptomatic hypoalbuminemia and hypoproteinemia, leading to anasarca due to hypoalbuminemia, further exacerbating malnutrition. Hookworm elicits systemic eosinophilia during larval migration through the lungs and tissues, peaking at 5 to 9 weeks postinfection as adult worms establish in the duodenal mucosa; mucosal eosinophils accumulate locally at attachment sites, contributing to inflammation without effective expulsion of worms.
Parasites can persist for years in their hosts and, accordingly, have evolved multiple strategies to ensure survival. The parasite uses broad-spectrum protease inhibitors to neutralize the host's immune defenses. While it helps the parasite protect itself from proteolytic enzymes, it worsens the host's malnutrition by interfering with absorption. Moreover, the parasite induces apoptosis of T lymphocytes and modulates cytokine responses to inhibit local immune activation. Interestingly, individuals with hookworm infection, as well as those with other helminths, have a broader range of gut microbiota. Preliminary human challenge studies and small trials suggest hookworm therapy may modulate immune responses in celiac disease and irritable bowel disease. Still, larger phase 2 and 3 trials are needed to establish efficacy and safety.[1][7][13][15][16][17]
Histopathology
Small bowel biopsy shows eosinophilic infiltration and cross-sections of hookworms embedded in the mucosa with surrounding hemorrhage and proteinaceous exudate (see Images. Hookworm Histopathology and Hookworm Transverse Section). Larval migration causes pulmonary eosinophilic infiltrates.[18]
History and Physical
Hookworm infections are usually asymptomatic. Symptoms usually relate to the stage of parasite development and the site of infection in the host, typically beginning at the time of skin penetration as localized pruritic erythematous papules or macules (ground itch), lasting 1 to 2 weeks at the site of larval skin penetration.[12][16] Hookworm-related cutaneous larva migrans (creeping eruptions) is associated with zoonotic hookworms. Creeping eruption (cutaneous larva migrans) results from zoonotic hookworms (A braziliense, A caninum) unable to penetrate beyond the stratum corneum.
Hookworm infections are endemic in many developing countries. However, travelers to endemic areas and healthcare workers with soil contact often experience symptoms upon return to their developed countries. Infections start as an erythematous papule that later develops into characteristic serpiginous tunnels beneath the skin, 1 to 5 cm in length, as larvae become unable to penetrate the deep layers of the skin and remain in its superficial layers. Infection often affects the hands and feet, as these are the usual contact sites with soil.[1][19]
During pulmonary migration of A duodenale or N americanus larvae (not cutaneous larva migrans), patients may develop cough, wheezing, and eosinophilic pneumonia (Loeffler syndrome). Loeffler syndrome is usually self-limiting. Treatment is rarely required. With peroral infection, nausea, vomiting, pharyngeal irritation, cough, and dyspnea might occur (Wakana syndrome).
Once worms reach the small intestine, nonspecific abdominal symptoms may occur, eg, abdominal pain and distension, diarrhea, occult blood in the stool, and occasionally melena. The small size of hookworms (<1.5 cm) makes intestinal obstruction or surgical complications extremely rare.[1][16] The central feature of hookworm infection is iron-deficiency anemia secondary to blood loss, either through direct parasite consumption or through blood leakage from the attachment site to the gut.[20]
Additionally, hypoalbuminemia might lead to edema formation and generalized anasarca. Occasionally, some patients crave soil and ingest dirt. Severe anemia may paradoxically cause pica (craving nonfood substances, eg, soil), which can perpetuate reinfection by allowing contaminated soil to be ingested.[1][16][13]
Evaluation
Laboratory Studies
The clinical features of hookworm infections are usually nonspecific and can be misleading. Therefore, a thorough understanding of the epidemiology, clinical features, and laboratory findings is crucial for accurate diagnosis.[1][16]
Stool microscopy using direct wet mount (immediate detection) or concentration techniques (formol-ether sedimentation) identifies hookworm eggs (see Image: Hookworm Eggs). The Kato-Katz thick smear quantifies eggs per gram for epidemiologic surveys but underestimates light infections due to variable egg output. In hospitals, laboratories tend to use egg concentration techniques, whereas for screening and public health control, simple tests, eg, the Kato-Katz technique, are often used. Kato-Katz smears are usually used in epidemiological studies because they provide an indirect measure of worm burden. Precision is limited by variations in egg production, especially with less severe infections. The IgG4 serologic assay might identify recent infection, but it remains nonspecific.[7][16]
Multiplex molecular detection of soil-transmitted helminth eggs in stool samples has been developed and provides high sensitivity and specificity.[21][22] A duplex real-time PCR assay for the simultaneous detection of N americanus and A duodenale has recently demonstrated high sensitivity and specificity when compared with traditional microscopic methods.[23] If available, these molecular detection methods should be considered as an alternative and adjunctive approach to traditional stool analysis.
Eosinophilia raises suspicion of hookworm infection, but this finding is nonspecific. Systemic and mucosal eosinophilia is common in hookworm infections and detectable in the blood even before worms reach the intestine, with levels peaking after adult worms colonize the intestinal mucosa.[1] When stool microscopy yields false-negative results, capsule endoscopy can be particularly helpful for directly visualizing hookworms in the small intestine.
Endoscopy Studies
Hookworm detection on capsule endoscopy images has improved significantly thanks to recent advances in artificial intelligence. After being trained on thousands of capsule endoscopy images, deep convolutional neural networks can now process over 10,000 images in about 7 minutes, achieving a sensitivity of 92.2%, a specificity of 91.1%, and an overall accuracy of 91.2%. When conventional stool tests are negative for obscure gastrointestinal bleeding, these AI-assisted detection systems may be particularly helpful. They also show promise for automated diagnosis. The sensitivity of stool microscopy is estimated at 70% to 80%, supporting the use of capsule endoscopy as an additional diagnostic technique.[24][25]
Treatment / Management
Hookworm Infection Treatment
The primary drugs used to treat hookworm infections are albendazole and mebendazole. Meta-analyses support single-dose albendazole (400 mg) over mebendazole (500 mg) in terms of superior cure rates (approximately 72% vs approximatley 30%). Treatment with 3 consecutive daily doses of either agent achieves superior cure and egg-reduction rates (~90%), though less convenient for mass drug administration. A 3-day regimen of mebendazole 100 mg twice daily is suitable for uncomplicated cases. Pyrantel pamoate (11 mg/kg daily × 3 days, max 1 g/dose) is an alternative when benzimidazole resistance is suspected (emerging globally) or in pregnancy (second and third trimester, when benzimidazoles are contraindicated).[1]
Systematic meta-analyses show that single-dose albendazole 400 mg is preferred for mass treatment (Egg Reduction Rate 93%-94%, Cure Rate 72%-78%). Triple-daily doses provide superior efficacy (Cure Rate >90%) for individual therapy of stable cases (no severe anemia requiring transfusion and no cardiopulmonary compromise). Albendazole 800 mg achieves a cure rate of up to 94.1% in adults, but is not used in mass campaigns due to safety/cost concerns.
In phase 2b clinical trials conducted in 2024, emodepside, a novel anthelmintic initially developed for veterinary use, demonstrated exceptional efficacy. Emodepside had a cure rate of 96.6% in a Tanzanian randomized controlled trial with 293 participants, compared with 81.2% for standard-dose albendazole (P = 0.0001). Three hours after treatment, the most frequent adverse effects were mild and included headache (38%), dizziness (30%), and blurred vision (39%). By acting on parasite ion channels, emodepside appears to function differently from benzimidazoles, which could be advantageous given the development of drug resistance. Phase 3 clinical trials are in progress as of 2025.[26][27](A1)
Treatment efficacy varies by infection severity, geographic distribution, and age group. Both mebendazole and albendazole are usually safe with a few transient adverse effects, eg, dizziness, headache, and abdominal upset.[1][28] Pregnant and lactating women have an increased risk of anemia from hookworm infections. Albendazole and mebendazole were both pregnancy category C under the prior FDA system; data on their use in pregnant women are limited. Whether albendazole or mebendazole is excreted in human milk is unknown. While albendazole requires caution in breastfeeding, the WHO allows the use of mebendazole in lactating women.[29](B3)
Preventive Treatment
The WHO recommends preventive treatment with a single dose of albendazole (400 mg) or mebendazole (500 mg) after the first trimester of pregnancy in areas where soil-transmitted helminth prevalence exceeds 20%. Recent large-scale studies analyzing over 800,000 births demonstrate that deworming during antenatal care reduces the risk of neonatal mortality by 14% and low birth weight by 11% in low-transmission settings. Benefits are enhanced when deworming is combined with iron supplementation. The global target is to achieve 75% deworming coverage among pregnant women by 2030, though current coverage varies substantially between countries.[WHO. Deworming in Pregnant Women. 2023][WHO. Deworming Women During Pregnancy has a Positive Effect on Child Survival and Health. 2021][30]
Drug Resistance
While definitive evidence of benzimidazole resistance in human hookworms remains limited, growing concerns exist following repeated mass drug administration campaigns. Reports of reduced albendazole efficacy require careful interpretation, as factors such as meal timing (associated with timing after the last meal and nutritional status), infection intensity, and hookworm species can significantly impact treatment outcomes. Accurate detection of drug resistance is complicated by high inter-individual variation in pharmacokinetics and limitations in WHO-recommended survey designs, which may lead to overestimation of drug efficacy. Resistance surveillance, routine efficacy testing, and the potential use of combination therapies are increasingly recommended to detect and prevent emerging resistance. Pyrantel pamoate and levamisole are alternative treatments, but neither has equal efficacy with albendazole.[31]
Supportive Therapies
Cutaneous larva migrans is usually self-limited and confined to the skin. However, treatment is sometimes needed, and it responds well to oral albendazole or ivermectin. Coadministration of deworming and iron supplementation has a greater impact on anemia, especially in nutritionally deficient populations. In a study of 746 schoolchildren, multivitamins and supplements, along with anthelmintic medications, increased hemoglobin levels, regardless of initial hemoglobin levels or nutritional status.[29][32] Blood transfusion should be considered for patients with severe anemia (hemoglobin <7 g/dL) or hemodynamic instability. Nutritional support and frequent monitoring of response are recommended for individuals with severe disease. (B3)
Long-Term Monitoring
Data to guide long-term treatment monitoring is unavailable. Therefore, given the risk of therapy failure and reinfection, follow-up of clinical symptoms, anemia, and stool testing is recommended. A follow-up at 1, 4, and 12 months appears appropriate in this context.[33]
Differential Diagnosis
Other intestinal causes of iron deficiency anemia should be excluded when evaluating patients with suspected hookworm infection, including:
- Malabsorption
- Gastric or oesophageal erosions
- Peptic ulcer disease
- Gastrointestinal malignancies
Moreover, the differential diagnosis includes other helminthic infestations that share standard features with hookworm infections, including:
- Ascariasis
- Schistosomiasis
- Strongyloidiasis
Cutaneous manifestations require differentiation from other conditions, eg, contact dermatitis, migratory myiasis, scabies, and cercarial dermatitis.[7]
Prognosis
Hookworm infection tends to cause morbidity rather than mortality. In adults, anemia and malnutrition reduce productivity, thereby increasing poverty. During pregnancy, iron demand increases, and as a result, this class of patients is at higher risk, affecting both the mother's and the fetus's well-being. Schoolchildren are at risk of a decline in cognitive function and academic achievement. In contrast, preschool children have less severe anemia due to lower worm burdens and better iron stores than school-age children and pregnant women.
A growing concern exists regarding treatment failure, especially after mass drug administration campaigns. Data illustrating the effect of deworming interventions on quality of life is insufficient. Additionally, a new generation of broad-spectrum agents needs to be developed, and further assessment of the efficacy of combination therapy on outcomes is needed.
Reinfection poses a major challenge in hookworm control, with moderate reinfection rates of 23.5% at 4 months and 33.3% at 6 months posttreatment supporting the need for repeated drug regimens in highly endemic areas. Important risk factors include living with more than 5 family members, infrequent latrine use, not wearing shoes, and participation in irrigation activities. Community prevalence was reduced by 63% using mass drug administration with a triple-drug combination (ie, ivermectin, diethylcarbamazine, and albendazole) compared to 43% with a double-drug combination (diethylcarbamazine and albendazole). Triple therapy provides broader coverage against lymphatic filariasis and soil-transmitted helminths, achieving greater reduction in community transmission through multi-species elimination and demonstrating substantial indirect benefits beyond direct treatment effects.[7][34][35][36]
Complications
Adult hookworm infection complications often include iron deficiency anemia; however, it may rarely present with an overt gastrointestinal bleed. Other associated complications include cutaneous larva migrans and eosinophilic pneumonia.[33]
Deterrence and Patient Education
Mass drug administration campaigns are effective in reducing the prevalence and burden of the infection. However, after stopping the medication, reinfection rates are usually high. Prevention is primarily achieved through health education campaigns focused on food sanitation, safe drinking water, handwashing, and proper footwear.[16][37]
With several phase 1 clinical trials completed in 2024, vaccine development has made significant progress. In hookworm-endemic regions of Gabon, coadministration of the Na-GST-1 (Necator americanus glutathione-S-transferase-1) and Na-APR-1 (M74) (aspartic protease-1) vaccine candidates has shown safety and immunogenicity in both adults and children aged 6 to 10 years. These antigens target the parasite's blood-digestion pathway. Targeting both larval and adult stages is crucial, as recent human challenge studies using irradiated N americanus larvae have demonstrated partial protection against infection. The European Union-funded WORMVACS2.0 project (2024-2029) is developing a comprehensive multiantigen vaccine, and phase 3 efficacy trials are expected to begin. The goal of the vaccination is to produce neutralizing antibodies that hinder adult worms' ability to feed on blood and stop larval development in the gut.[28][38][39] [James Cook University. Vaccine Effort Targets Hookworm Larvae. Dec, 2024]
Poverty reduction and economic development have contributed more to eliminating hookworm infection than any other factor, but this has not been easy.[13]
Pearls and Other Issues
Factors that should be kept in mind when managing hookworm infections include:
- Hookworm infections are currently considered one of the most underfunded neglected tropical diseases.
- Millions of people worldwide are infected with the parasite, especially in poorer tropical countries.
- Ancylostoma duodenale and Necator americanus are the main species that infect humans. A ceylanicum, A.caninum, and A braziliense are other minor causes.
- Hookworm infections are usually asymptomatic; symptoms vary by life-cycle stage, from cutaneous ground itch to respiratory symptoms, to the main feature of iron-deficiency anemia, and, on rare occasions, intestinal bleeding.
- Diagnosis depends on both epidemiological, clinical, and microscopic evaluation.
- Management is mainly by either single-dose albendazole or multidose mebendazole, with emodepside emerging as a highly effective new option in clinical trials. Mass treatment is helpful in endemic areas.
- Health education and sanitation are the mainstays of disease prevention. No licensed vaccine is available yet, but multiple candidates (Na-GST-1 and Na-APR-1) have completed Phase 1 trials and are progressing toward efficacy studies.
Enhancing Healthcare Team Outcomes
Hookworm infection represents a major neglected tropical disease caused primarily by Ancylostoma duodenale and Necator americanus. Transmission occurs when infective larvae in contaminated soil penetrate human skin and migrate through the bloodstream to the lungs, where they mature into adults and attach to the mucosa, feeding on host blood. Chronic infection may lead to iron-deficiency anemia, protein loss, and malnutrition, particularly in children and pregnant individuals. Clinical manifestations vary by stage of infection and may include pruritic skin lesions, pulmonary symptoms such as eosinophilic pneumonia, and gastrointestinal complaints. Accurate diagnosis relies on clinical suspicion, careful history taking, and stool microscopy, while treatment typically involves anthelmintic therapy and nutritional support.
Effective diagnosis and management require coordinated interprofessional collaboration. General practitioners often serve as the first point of contact and must recognize nonspecific symptoms and initiate appropriate diagnostic evaluation or referral. Infectious disease specialists and gastroenterologists contribute expertise in complex presentations and treatment strategies, while histopathologists support accurate stool examination and laboratory confirmation. Pharmacists verify medication regimens, monitor for drug interactions, and reinforce adherence to anthelmintic therapy. Nurses play an essential role in patient education, monitoring treatment response, and counseling travelers on hygiene and the prevention of exposure. Public health professionals, clinicians, and local authorities collaborate to improve sanitation, implement preventive deworming strategies, and promote community awareness. Strong interprofessional communication and care coordination enhance patient-centered care, improve outcomes, support patient safety, and strengthen team performance in the management and prevention of hookworm infection.
Media
(Click Image to Enlarge)
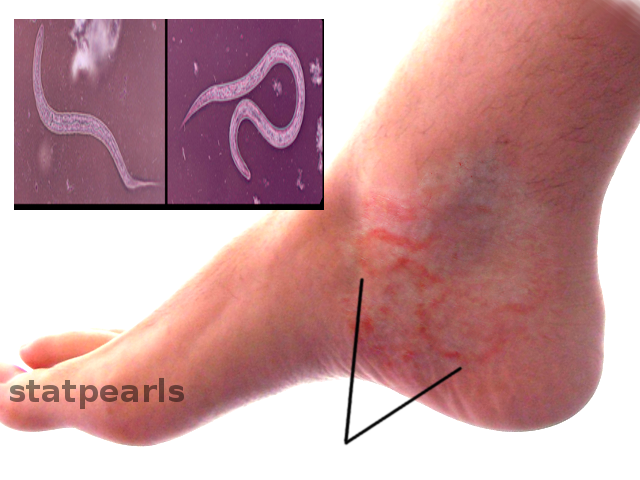
Hookworm Infection. After skin penetration, the larvae migrate passively through the bloodstream to the right side of the heart and hence to the pulmonary vasculature.
Contributed by O Chaigasame, MD
(Click Image to Enlarge)

Hookworm Eggs. Stool microscopy using direct wet mount (immediate detection) or concentration techniques (formol-ether sedimentation) identifies hookworm eggs.
Centers for Disease Control and Prevention
(Click Image to Enlarge)

Hookworm Histopathology. Adult hookworms (Ancylostoma spp.) attached to canine small intestinal mucosa, demonstrating characteristic buccal capsule attachment, hemorrhage at feeding sites, and mucosal inflammation. Macroscopic pathology equivalent showing worm cross-sections embedded in tissue with surrounding damage—key visual for duodenal histopathology.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
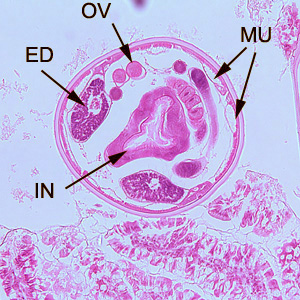
Hematoxylin and eosin (H&E)-stained histopathology of a transverse section through an adult hookworm (Ancylostoma duodenale or Necator americanus) embedded in duodenal mucosa. Labeled features include the oral vestibule (OV), esophageal duct (ED), intestine (IN), and muscular uterus (MU) filled with eggs; note surrounding eosinophilic infiltrate, hemorrhage, and mucosal erosion at the attachment site.
Public Health Image Library, Division of Parasitic Diseases and Malaria, Public Domain, Centers for Disease Control and Prevention
References
Loukas A, Hotez PJ, Diemert D, Yazdanbakhsh M, McCarthy JS, Correa-Oliveira R, Croese J, Bethony JM. Hookworm infection. Nature reviews. Disease primers. 2016 Dec 8:2():16088. doi: 10.1038/nrdp.2016.88. Epub 2016 Dec 8 [PubMed PMID: 27929101]
Wei KY, Yan Q, Tang B, Yang SM, Zhang PB, Deng MM, Lü MH. Hookworm Infection: A Neglected Cause of Overt Obscure Gastrointestinal Bleeding. The Korean journal of parasitology. 2017 Aug:55(4):391-398. doi: 10.3347/kjp.2017.55.4.391. Epub 2017 Aug 31 [PubMed PMID: 28877570]
Periago MV, Bethony JM. Hookworm virulence factors: making the most of the host. Microbes and infection. 2012 Dec:14(15):1451-64. doi: 10.1016/j.micinf.2012.09.002. Epub 2012 Sep 21 [PubMed PMID: 23006854]
Level 3 (low-level) evidenceBartsch SM, Hotez PJ, Asti L, Zapf KM, Bottazzi ME, Diemert DJ, Lee BY. The Global Economic and Health Burden of Human Hookworm Infection. PLoS neglected tropical diseases. 2016 Sep:10(9):e0004922. doi: 10.1371/journal.pntd.0004922. Epub 2016 Sep 8 [PubMed PMID: 27607360]
Wong Y, Rosa BA, Becker L, Camberis M, LeGros G, Zhan B, Bottazzi ME, Fujiwara RT, Ritmejeryte E, Laha T, Chaiyadet S, Taweethavonsawat P, Brindley PJ, Bracken BK, Giacomin PR, Mitreva M, Loukas A. Proteomic characterization and comparison of the infective and adult life stage secretomes from Necator americanus and Ancylostoma ceylanicum. PLoS neglected tropical diseases. 2025 Jan:19(1):e0012780. doi: 10.1371/journal.pntd.0012780. Epub 2025 Jan 20 [PubMed PMID: 39832284]
Albonico M, Savioli L. Hookworm: a neglected resurgent infection. BMJ (Clinical research ed.). 2017 Oct 24:359():j4813. doi: 10.1136/bmj.j4813. Epub 2017 Oct 24 [PubMed PMID: 29066626]
Brooker S, Bethony J, Hotez PJ. Human hookworm infection in the 21st century. Advances in parasitology. 2004:58():197-288 [PubMed PMID: 15603764]
Level 3 (low-level) evidenceAguilar-Rodríguez D, Seco-Hidalgo V, Lopez A, Romero-Sandoval N, Calvopiña M, Guevara A, Baldeón L, Rodríguez A, Mejia R, Nutman TB, Sears WJ, Cooper PJ. Geographic Distribution of Human Infections with Zoonotic Ancylostoma ceylanicum and Anthropophilic Hookworms in Ecuador: A Retrospective Analysis of Archived Stool Samples. The American journal of tropical medicine and hygiene. 2024 Mar 6:110(3):460-469. doi: 10.4269/ajtmh.23-0469. Epub 2024 Jan 23 [PubMed PMID: 38266286]
Level 2 (mid-level) evidenceTahar AS, Habeebur-Rahman SP, Yaman K, Ngui R, Lim LLA, Edwin J, Saboden NS, Manggi T, Tan CS. Genetic diversity of Ancylostoma ceylanicum and first molecular detection of Ancylostoma braziliense in stray dogs from Sarawak, Malaysia. Scientific reports. 2025 Apr 26:15(1):14586. doi: 10.1038/s41598-025-99092-8. Epub 2025 Apr 26 [PubMed PMID: 40281043]
Sarkar ER, Sikder S, Giacomin P, Loukas A. Hookworm vaccines: current and future directions. Expert review of vaccines. 2024 Jan-Dec:23(1):1029-1040. doi: 10.1080/14760584.2024.2410893. Epub 2024 Nov 15 [PubMed PMID: 39350544]
Level 3 (low-level) evidenceChen J, Gong Y, Chen Q, Li S, Zhou Y. Global burden of soil-transmitted helminth infections, 1990-2021. Infectious diseases of poverty. 2024 Oct 24:13(1):77. doi: 10.1186/s40249-024-01238-9. Epub 2024 Oct 24 [PubMed PMID: 39444032]
Parija SC, Chidambaram M, Mandal J. Epidemiology and clinical features of soil-transmitted helminths. Tropical parasitology. 2017 Jul-Dec:7(2):81-85. doi: 10.4103/tp.TP_27_17. Epub [PubMed PMID: 29114484]
Hotez PJ, Brooker S, Bethony JM, Bottazzi ME, Loukas A, Xiao S. Hookworm infection. The New England journal of medicine. 2004 Aug 19:351(8):799-807 [PubMed PMID: 15317893]
Level 3 (low-level) evidenceJiraanankul V, Aphijirawat W, Mungthin M, Khositnithikul R, Rangsin R, Traub RJ, Piyaraj P, Naaglor T, Taamasri P, Leelayoova S. Incidence and risk factors of hookworm infection in a rural community of central Thailand. The American journal of tropical medicine and hygiene. 2011 Apr:84(4):594-8. doi: 10.4269/ajtmh.2011.10-0189. Epub [PubMed PMID: 21460016]
Pearson MS, Tribolet L, Cantacessi C, Periago MV, Valero MA, Jariwala AR, Hotez P, Diemert D, Loukas A, Bethony J. Molecular mechanisms of hookworm disease: stealth, virulence, and vaccines. The Journal of allergy and clinical immunology. 2012 Jul:130(1):13-21. doi: 10.1016/j.jaci.2012.05.029. Epub [PubMed PMID: 22742835]
Level 3 (low-level) evidenceJourdan PM, Lamberton PHL, Fenwick A, Addiss DG. Soil-transmitted helminth infections. Lancet (London, England). 2018 Jan 20:391(10117):252-265. doi: 10.1016/S0140-6736(17)31930-X. Epub 2017 Sep 4 [PubMed PMID: 28882382]
Wright V, Bickle Q. Immune responses following experimental human hookworm infection. Clinical and experimental immunology. 2005 Nov:142(2):398-403 [PubMed PMID: 16232230]
Zhang F, Tao Y, Niu J. Hookworm Infection Mimicking Early Gastric Mucosal Carcinoma: Magnifying Endoscopy Findings in Two Cases. JGH open : an open access journal of gastroenterology and hepatology. 2025 Sep:9(9):e70279. doi: 10.1002/jgh3.70279. Epub 2025 Sep 16 [PubMed PMID: 40964068]
Level 3 (low-level) evidenceFeldmeier H, Schuster A. Mini review: Hookworm-related cutaneous larva migrans. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology. 2012 Jun:31(6):915-8. doi: 10.1007/s10096-011-1404-x. Epub 2011 Sep 16 [PubMed PMID: 21922198]
Level 3 (low-level) evidenceLoukas A, Prociv P. Immune responses in hookworm infections. Clinical microbiology reviews. 2001 Oct:14(4):689-703, table of contents [PubMed PMID: 11585781]
Level 3 (low-level) evidenceStracke K, Clarke N, Awburn CV, Vaz Nery S, Khieu V, Traub RJ, Jex AR. Development and validation of a multiplexed-tandem qPCR tool for diagnostics of human soil-transmitted helminth infections. PLoS neglected tropical diseases. 2019 Jun:13(6):e0007363. doi: 10.1371/journal.pntd.0007363. Epub 2019 Jun 17 [PubMed PMID: 31206520]
Level 1 (high-level) evidenceNevin WD, Cunningham LJ, Mason J, Adams ER, Jones J, Woolley SD, Lamb LE, Beeching NJ, Fletcher TE, O'Shea MK. A comparative study of traditional and molecular diagnostic methods for detection of gastrointestinal parasites in Nepalese migrants to the UK. The Journal of infection. 2024 Dec:89(6):106324. doi: 10.1016/j.jinf.2024.106324. Epub 2024 Oct 19 [PubMed PMID: 39433178]
Level 2 (mid-level) evidenceThakur M, Mewara A, Lakshmi PVM, Guleria S, Khurana S. Evaluation of duplex TaqMan real-time PCR assay for the simultaneous detection of Ancylostoma duodenale and Necator americanus. Indian journal of medical microbiology. 2026 May-Jun:61():101115. doi: 10.1016/j.ijmmb.2026.101115. Epub 2026 Apr 15 [PubMed PMID: 41990408]
Ghoshal UC, Roy A, Goenka MK. Capsule endoscopy for small bowel bleed: Current update. Indian journal of gastroenterology : official journal of the Indian Society of Gastroenterology. 2024 Oct:43(5):896-904. doi: 10.1007/s12664-024-01637-8. Epub 2024 Aug 2 [PubMed PMID: 39093511]
Takebe T, Osawa S, Watanabe Y, Yamagata S, Aoyama T, Kawamura Y, Manabe A, Kisamori T, Sano M, Sugimoto K. Endoscopic Diagnosis of Necator americanus Infection Presenting With Persistent Iron-Deficiency Anemia: Usefulness of Image-Enhanced Endoscopy and Capsule Endoscopy. DEN open. 2027 Apr:7(1):e70352. doi: 10.1002/deo2.70352. Epub 2026 May 22 [PubMed PMID: 42256607]
Taylor L, Ahmada AA, Ali MS, Ali SM, Hattendorf J, Mohammed IS, Keiser J. Efficacy and safety of emodepside compared with albendazole in adolescents and adults with hookworm infection in Pemba Island, Tanzania: a double-blind, superiority, phase 2b, randomised controlled trial. Lancet (London, England). 2024 Aug 17:404(10453):683-691. doi: 10.1016/S0140-6736(24)01403-X. Epub [PubMed PMID: 39153818]
Level 1 (high-level) evidenceTaylor L, Many S, Jeanguenat H, Hattendorf J, Sayasone S, Keiser J. Efficacy and safety of ascending doses of emodepside in comparison with ivermectin in adults infected with Strongyloides stercoralis in Laos: a phase 2a, dose-ranging, randomised, parallel-group, placebo-controlled, single-blind clinical trial. The Lancet. Infectious diseases. 2025 Nov:25(11):1254-1264. doi: 10.1016/S1473-3099(25)00255-5. Epub 2025 Jun 25 [PubMed PMID: 40580974]
Level 1 (high-level) evidenceHotez PJ, Beaumier CM, Gillespie PM, Strych U, Hayward T, Bottazzi ME. Advancing a vaccine to prevent hookworm disease and anemia. Vaccine. 2016 Jun 3:34(26):3001-3005. doi: 10.1016/j.vaccine.2016.03.078. Epub 2016 Mar 31 [PubMed PMID: 27040400]
Brooker S, Hotez PJ, Bundy DA. Hookworm-related anaemia among pregnant women: a systematic review. PLoS neglected tropical diseases. 2008 Sep 17:2(9):e291. doi: 10.1371/journal.pntd.0000291. Epub 2008 Sep 17 [PubMed PMID: 18820740]
Level 3 (low-level) evidenceSassa M, Yoneoka D, Ng CFS, Cao AQ, Devanathan G, Hashizume M, Nomura S. A comprehensive assessment of deworming coverage among pregnant women in low- and middle-income countries, 2000-30. Journal of global health. 2024 Mar 1:14():04002. doi: 10.7189/jogh.14.04002. Epub 2024 Mar 1 [PubMed PMID: 38419465]
Coffeng LE, Stolk WA, de Vlas SJ. Predicting the risk and speed of drug resistance emerging in soil-transmitted helminths during preventive chemotherapy. Nature communications. 2024 Feb 6:15(1):1099. doi: 10.1038/s41467-024-45027-2. Epub 2024 Feb 6 [PubMed PMID: 38321011]
Friis H, Mwaniki D, Omondi B, Muniu E, Thiong'o F, Ouma J, Magnussen P, Geissler PW, Michaelsen KF. Effects on haemoglobin of multi-micronutrient supplementation and multi-helminth chemotherapy: a randomized, controlled trial in Kenyan school children. European journal of clinical nutrition. 2003 Apr:57(4):573-9 [PubMed PMID: 12700619]
Level 3 (low-level) evidenceSharma V, Gunjan D, Chhabra P, Sharma R, Rana SS, Bhasin DK. Gastrointestinal bleeding in the tropics: Look for the hookworm. Tropical doctor. 2017 Jan:47(1):48-51 [PubMed PMID: 27075012]
Speich B, Moser W, Ali SM, Ame SM, Albonico M, Hattendorf J, Keiser J. Efficacy and reinfection with soil-transmitted helminths 18-weeks post-treatment with albendazole-ivermectin, albendazole-mebendazole, albendazole-oxantel pamoate and mebendazole. Parasites & vectors. 2016 Mar 2:9():123. doi: 10.1186/s13071-016-1406-8. Epub 2016 Mar 2 [PubMed PMID: 26935065]
Belay S, Alemu G, Hailu T. Pattern and predictor of hookworm re-infection among schoolchildren in three districts of Amhara Region, northwest Ethiopia. PloS one. 2024:19(5):e0303502. doi: 10.1371/journal.pone.0303502. Epub 2024 May 28 [PubMed PMID: 38805475]
Tobon Ramos JA, Maure T, Carias L, Lew D, Goss C, Samuel A, Tavul L, Fischer PU, Weil GJ, Laman M, Robinson LJ, Pomat W, King CL. Impact of mass drug administration with ivermectin, diethylcarbamazine, and albendazole for lymphatic filariasis on hookworm and Strongyloides stercoralis infections in Papua New Guinea. PLoS neglected tropical diseases. 2025 Mar:19(3):e0012851. doi: 10.1371/journal.pntd.0012851. Epub 2025 Mar 10 [PubMed PMID: 40063867]
Bieri FA, Gray DJ, Williams GM, Raso G, Li YS, Yuan L, He Y, Li RS, Guo FY, Li SM, McManus DP. Health-education package to prevent worm infections in Chinese schoolchildren. The New England journal of medicine. 2013 Apr 25:368(17):1603-12. doi: 10.1056/NEJMoa1204885. Epub [PubMed PMID: 23614586]
Level 1 (high-level) evidenceZinsou JF, Diemert DJ, Dejon-Agobé JC, Adégbité BR, Honkpehedji YJ, Vodonou KG, Bikangui R, Edoa JR, Massinga Loembe M, Li G, Yazdanbakhsh M, Bottazzi ME, van Leeuwen R, Kremsner PG, Hotez PJ, Bethony JM, Grobusch MP, Adegnika AA. Safety and immunogenicity of the co-administered Na-APR-1 and Na-GST-1 hookworm vaccines in school-aged children in Gabon: a randomised, controlled, observer-blind, phase 1, dose-escalation trial. The Lancet. Infectious diseases. 2024 Jul:24(7):760-774. doi: 10.1016/S1473-3099(24)00104-X. Epub 2024 Mar 18 [PubMed PMID: 38513684]
Level 1 (high-level) evidenceDiemert DJ, Zumer M, Bova M, Gibbs-Tewary C, Malkin EM, Campbell D, Hoeweler L, Li G, Bottazzi ME, Hotez PJ, Bethony JM. Randomized, observer-blind, controlled Phase 1 study of the safety and immunogenicity of the Na-GST-1/Alhydrogel hookworm vaccine with or without a CpG ODN adjuvant in hookworm-naïve adults. PLoS neglected tropical diseases. 2024 Dec:18(12):e0012788. doi: 10.1371/journal.pntd.0012788. Epub 2024 Dec 30 [PubMed PMID: 39775205]
Level 1 (high-level) evidence