Introduction
Toxoplasmosis is one of the most common central nervous system (CNS) infections in patients with advanced HIV infection who are not receiving appropriate toxoplasmosis prophylaxis, especially those who are not receiving antiretroviral therapy. Cerebral toxoplasmosis usually manifests as one or more CNS mass lesions. In addition to toxoplasmosis, opportunistic infections that typically present with mass-like lesions include primary CNS lymphoma, which is typically associated with Epstein-Barr virus, CNS tuberculosis, and, occasionally, progressive multifocal leukoencephalopathy.[1][2][3][4][5][6]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The causative agent is Toxoplasma gondii, an exclusively intracellular, coccidian protozoan parasite with worldwide distribution. Transmission occurs following ingestion of infectious oocysts from contaminated meat, food, or water. Infectious oocysts are abundant in damp, shaded soil and cat litter contaminated with feline feces. The tissues of pigs, lambs, goats, deer, and bears can become infected when these animals consume vegetation, water, or soil contaminated with cat-shed oocysts. Humans then acquire infection primarily through 2 routes: eating undercooked meat from infected intermediate hosts or directly ingesting oocysts from environmental contamination. Felines are the only animals in which T gondii can complete its reproductive cycle.
The T gondii parasite can exist as a sporulated oocyst, an unsporulated oocyst, or an intracellular tissue cyst. The sporulated oocyst is the infectious form for humans and is found in the soil. Unsporulated oocysts are released into the environment, mainly into soil through cat feces. After release, oocysts sporulate outside the cat and become infectious. Sporulated oocysts can remain infectious in the soil for months. Once ingested, the oocysts migrate from the intestinal epithelium to tissues and can spread to all organs and systems in the body. In tissues, the parasite develops into intracellular tissue cysts. Tissue cysts are usually slow-growing and dormant bradyzoites for years in immunocompetent hosts, whereas immunosuppression can cause cyst reactivation, rapid division, and active disease due to tachyzoites.[7] Latent infection can reactivate because of progressive loss of cellular immunity in patients with advanced HIV infection, after solid organ or stem cell transplant, with prolonged corticosteroid use, with monoclonal antibody therapy, or during chemotherapy.[7][8][9][10]
Epidemiology
According to a systematic review of observational studies conducted over decades that summarized the prevalence of Toxoplasma gondii seropositivity among people with HIV globally, 35.8% of people living with HIV had latent infection.[11] The highest seroprevalence estimates among people living with HIV were reported in resource-limited countries (54.7%) compared with high-income countries (26.3%). The incidence of symptomatic toxoplasmosis in people living with HIV continues to decline in areas with widespread antiretroviral therapy use, although cases still occur, particularly in individuals with advanced immunosuppression or delayed HIV diagnosis. Results from a recent Asia-Pacific cohort study showed that most cases occurred in individuals not receiving antiretroviral therapy, especially those with CD4 counts of 200 cells/µL or fewer, and that injection drug use and hepatitis B coinfection were additional risk factors.[4]
The prevalence of toxoplasmosis across all patient types, including immunocompromised and immunocompetent individuals, is much lower in high-income regions, such as Europe and North America, than in South America and Africa, except in Australia, which has the highest prevalence (54%).[12] The National Health and Nutrition Examination Survey reported that overall Toxoplasma seroprevalence in the US population from 2011 to 2014 was about 11%, with higher rates in certain subgroups and geographic regions.[13][14]
Although cats and related felines have traditionally been associated with toxoplasmosis, infection prevalence is not related to cat ownership. In patients with HIV and Toxoplasma seropositivity who have a CD4 count less than 100 cells/µL and are not receiving appropriate prophylaxis, the probability of developing reactivated toxoplasmosis is as high as 30%. Apart from oral transmission, toxoplasmosis can also be transmitted transplacentally from a pregnant patient to the fetus or through the transplant of an infected organ.
Pathophysiology
After a host ingests the infective forms, Toxoplasma gondii invades the intestinal epithelium and disseminates throughout the body. In tissues, most often the brain but potentially any tissue, the organisms encyst and remain dormant until immunity wanes. The dormant forms are called bradyzoites, whereas the actively replicating forms are called tachyzoites. Primary toxoplasmosis is often subclinical but may rarely present symptomatically in a seronegative immunocompromised person who has been recently exposed to the infective forms. In this scenario, IgM against Toxoplasma often yields a positive result, whereas IgG level results are negative, unlike most reactivation cases, in which IgG is the only serologic test result that is positive. As previously outlined, in most situations, clinical toxoplasmosis in patients with HIV is due to the reactivation of latent infection when immunity wanes.[15][16][17]
Toxoplasmosis can cause disease in any organ or organ system. In immunocompetent individuals, the most common presentation is Toxoplasma lymphadenitis. Other nonspecific manifestations include fever, malaise, arthralgia, myalgia, and sore throat resembling mononucleosis. Rarely, fatal toxoplasmosis with myocarditis, pneumonitis, and CNS manifestations has been reported in immunocompetent patients, possibly due to virulent strains.
Histopathology
The histology usually reveals diffuse encephalitis, cyst-containing lesions, microglial nodules, and lymphocytic vasculitis.
History and Physical
Cerebral toxoplasmosis (toxoplasmic encephalitis), usually with 1 or more ring-enhancing brain lesions, is the typical presentation in patients with HIV. Among patients with HIV, the most common presentation is focal encephalitis, which is characterized by headache, focal neurologic deficits, confusion, seizures, and reduced consciousness.[18] Symptoms are often subacute, ranging from a few days to a month. Fever may be present, but is usually absent. Findings from studies suggested that a chronic Toxoplasma infection may not be completely asymptomatic, and behavioral changes and neuropsychiatric disorders may occur in some patients. Mental status changes may range from a dull affect to stupor and coma, often secondary to global encephalitis or increased intracranial pressure. Conversely, the latent or dormant phase is usually asymptomatic.
Although uncommon, other manifestations such as pulmonary toxoplasmosis, chorioretinitis, hepatitis, and myocarditis have been reported. Involvement of the spinal cord leading to sensory and motor weakness with bladder and bowel involvement has also been reported. Pulmonary toxoplasmosis can often be mistaken for other atypical forms of pneumonia. Pulmonary toxoplasmosis may resemble pneumocystis pneumonia or be confused with pulmonary infection secondary to cytomegalovirus, Mycobacterium tuberculosis, Histoplasma capsulatum, Cryptococcus spp, and Coccidioides spp. Mortality from pulmonary toxoplasmosis remains high despite appropriate therapy. Diagnosis is made through bronchoalveolar lavage polymerase chain reaction testing for T gondii. Rarely, toxoplasmosis may present as disseminated disease.
Evaluation
No routine laboratory findings are specific to toxoplasmosis. However, lactate dehydrogenase levels can be markedly increased in patients with disseminated toxoplasmosis and pulmonary disease.[2][19][20] A presumptive diagnosis of cerebral toxoplasmosis in a patient with HIV can be made when the following criteria are present:
- CD4 count of fewer than 100 cells/µL without effective prophylaxis
- A compatible clinical syndrome (as described above in the History and Physical section)
- A positive T gondii IgG antibody result
- Anti-Toxoplasma IgM antibodies are usually absent except rarely in cases of primary infection. Quantitative IgG antibody titers are not helpful in diagnosis.
- MRI brain imaging with contrast demonstrates typical radiographic findings, most commonly 1 or more ring-enhancing lesions with or without surrounding edema (see Image. Cerebral Toxoplasmosis).
If the above criteria are present, the probability of cerebral toxoplasmosis is at least 90%. However, clinicians should recognize that positive serologic test results do not confirm the diagnosis, and negative serologic test results imply that cerebral toxoplasmosis is unlikely, though not impossible. The ring-enhancing brain lesions on brain MRI findings may be multiple (67%) or single (33%), with a predilection for involvement of the basal ganglia, corticomedullary junction, or brain white matter. (see Image. Cerebral Toxoplasmosis).
A more definitive diagnosis can be made by obtaining a lumbar puncture if it is safe to perform. Cerebrospinal fluid analysis often shows mononuclear pleocytosis, elevated protein levels, and, sometimes, reduced CSF glucose levels.[21] Polymerase chain reaction testing for T gondii in CSF is 100% specific but only 44% to 65% sensitive. Therefore, positive CSF polymerase chain reaction results establish the diagnosis of cerebral toxoplasmosis, but negative results do not rule it out.
More recently, the enzyme-linked immunosorbent assay for detecting IgG avidity has been introduced. IgG avidity, which reflects the antibody's affinity for the antigen, typically shows low levels in acute infection but high levels in chronic or long-standing infection. IgG avidity testing is especially useful for distinguishing recent from chronic Toxoplasma infections in pregnant women who may transmit the infection vertically to their offspring. A combination of maternal IgG, IgM, and IgG avidity tests helps minimize false-positive results, especially when positive IgM results persist for a long time, as is often seen in toxoplasmosis. Vertical transmission risk is increased with recent infection or infection acquired in the first or second trimester of pregnancy compared with chronic infection acquired before pregnancy.[22][23]
A brain biopsy can be obtained when the diagnosis is in doubt, and alternative diagnoses are considered. Findings in cerebral toxoplasmosis may show necrotic abscesses with blood vessel thrombosis and necrosis. Cysts containing bradyzoites may often be found coexisting with numerous active tachyzoites. In most cases, a brain biopsy is not required for diagnosis.
Although advanced molecular diagnostics, such as real-time isothermal amplification and next-generation sequencing, are being explored, the standard of care remains a combination of clinical presentation, serology, and neuroimaging for presumptive diagnosis. Newer diagnostic modalities, however, are not yet widely adopted in routine clinical practice.[24] Most commonly, people living with HIV and suspected toxoplasmic encephalitis are treated empirically, without a definitive diagnosis (such as a brain biopsy). Because patients often have a good clinical response to therapy, histologic diagnosis is typically not required.
Treatment / Management
The treatment of toxoplasmosis in patients with HIV includes:
- Antimicrobial therapy directed against T gondii
- Antiretroviral therapy for immune recovery
Initial-phase therapy is followed by secondary prophylaxis or maintenance therapy, which continues until CD4-positive T-lymphocyte counts exceed 200 cells/µL for more than 6 months. The preferred drugs used in the initial phase of toxoplasmosis are pyrimethamine plus sulfadiazine plus leucovorin or trimethoprim-sulfamethoxazole. In patients with sulfonamide allergy, treatment options include pyrimethamine plus clindamycin plus leucovorin or atovaquone alone. Desensitization should be attempted when sulfonamide-containing therapy is clinically indicated. Atovaquone can be used alone or combined with either sulfadiazine or pyrimethamine. Leucovorin should always be included whenever pyrimethamine is used because pyrimethamine is a dihydrofolate reductase inhibitor, and leucovorin, or folinic acid, can reduce hematopoietic adverse effects. The initial phase of treatment should be given for 6 weeks after the resolution of signs and symptoms before the maintenance phase begins. In addition to awaiting immune recovery, secondary prophylaxis provides continuous therapy against dormant cystic forms, which may rupture and reinitiate the infectious process at any time. Maintenance therapy, preferably either double-strength trimethoprim-sulfamethoxazole twice daily or pyrimethamine plus sulfadiazine plus leucovorin, is necessary to prevent relapses.[HIV.gov. Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV]
In patients with sulfonamide allergy, desensitization should be initiated; in the meantime, atovaquone therapy, with or without pyrimethamine, should be started. For pregnant patients who acquire primary infection during pregnancy, spiramycin is recommended during the first 14 weeks of gestation to reduce fetal transmission because the drug is concentrated in the placenta and is nonteratogenic. For primary maternal infections acquired beyond 14 weeks or when fetal transmission is confirmed, treatment remains the same as in the nonpregnant population, with pyrimethamine plus sulfadiazine and leucovorin. Pyrimethamine and sulfadiazine are avoided in the first trimester due to teratogenicity.
Most clinicians use corticosteroids when edema is present, but study results have shown their use to be neither beneficial nor harmful. Adjunctive corticosteroids should be administered only to treat mass effect associated with focal brain lesions or related edema, or to control clinically significant immune reconstitution inflammatory syndrome symptoms, in conjunction with antiretroviral therapy and anti-Toxoplasma therapy. Corticosteroids should be discontinued when clinically possible to avoid further immunosuppression. For patients in whom the diagnosis of toxoplasmic encephalitis is presumptive based on clinical response, the clinical team should recognize that central nervous system lymphoma may also respond to corticosteroids.
The treatment course is often dramatic, with half of patients showing neurologic improvement by day 3 and, in most cases, by day 7 after treatment initiation. When patients have no significant improvement or have worsening symptoms by days 10 to 14 of therapy, repeat imaging and possibly a brain biopsy should be considered. Persistent neurologic sequelae may remain in 37% of survivors, and the death rate at 1 year varies from 10% to 60%. Therapies that target latent cysts and have improved safety profiles remain needed, but no new agents have been adopted into the standard of care, according to results from a 2023 study.[24] Additionally, clinicians should be aware that the initiation of antiretroviral therapy or effective antiretroviral therapy can result in immune reconstitution inflammatory syndrome in patients with central nervous system toxoplasmosis.
Differential Diagnosis
The differential diagnoses for HIV-1–associated toxoplasmosis include the following:
- CNS lymphoma: CNS lymphoma can be radiographically indistinguishable from CNS toxoplasmosis on brain MRI and CT. Lymphoma should be considered next in the differential diagnosis when imaging findings are not characteristic of toxoplasmic encephalitis.
- CNS tuberculosis
- CNS cryptococcosis (cryptococcoma)
- CNS aspergillosis
- Progressive multifocal leukoencephalopathy caused by the JC virus
- Pyogenic bacterial brain abscess
- CNS metastatic cancer brain lesions
Complications
Complications of HIV-1–associated toxoplasmosis include the following:
- Changes in personality
- Seizures
- Cranial nerve palsy
- Hemiparesis
- Hemianopia
- Ataxia
- Aphasia
Postoperative and Rehabilitation Care
Once antimicrobial treatment has started, improvement is gradual and may take several weeks. Imaging studies should be repeated in 4 to 6 weeks to determine whether the lesion is decreasing in size, or sooner if the patient clinically worsens or does not show appropriate improvement. Long-term therapy is continued at low doses. If the absolute CD4 count improves to more than 200 cells/µL for 6 months and the lesion resolves, therapy may be discontinued.
Deterrence and Patient Education
Patients with HIV–1–associated toxoplasmosis should be advised to avoid eating raw or undercooked meat and wash their hands thoroughly after handling cat litter or soil.
Pearls and Other Issues
Prophylaxis against T gondii reactivation in seropositive individuals with CD4+ T-lymphocyte counts of fewer than 100 cells/µL is strongly recommended. Trimethoprim-sulfamethoxazole is mainly used. Other options include dapsone, after testing for glucose-6-phosphate dehydrogenase (G6PD) gene deficiency, plus pyrimethamine and leucovorin, or atovaquone with or without pyrimethamine and leucovorin. Once the absolute CD4+ count improves to greater than 200 cells/µL and remains greater than 200 cells/µL for at least 6 months, secondary prophylaxis for toxoplasmic encephalitis can be discontinued; primary prophylaxis can be discontinued once the CD4+ count is greater than 200 cells/µL for 3 months or longer. In conclusion, toxoplasmosis should always be included in the differential diagnosis of central nervous system lesions in patients with advanced HIV. Diagnosis combines clinical symptoms and signs, serology, and imaging. Cerebrospinal fluid analysis may further support the diagnosis. Brain biopsy is often reserved for difficult cases. Treatment is often dramatic, and most patients have a favorable clinical outcome.
Enhancing Healthcare Team Outcomes
The role of the interprofessional healthcare team is critical in the care of patients with HIV and CNS toxoplasmosis. Patients should be educated to wash their hands after contact with cat litter. Additionally, patients should wash their hands after contact with raw meat and wear gloves when gardening. Because these patients are typically prescribed many medications, including antiretroviral therapy, an anti–Toxoplasmosis regimen, and treatment for other, often concomitant, opportunistic infections, medication adherence should be emphasized.
Patients with HIV and CNS toxoplasmosis require maintenance prophylaxis with trimethoprim-sulfamethoxazole until the absolute CD4 count is greater than 200 cells/µL; once the absolute CD4 count remains greater than 200 cells/µL for at least 6 months, secondary prophylaxis can be discontinued. The prognosis of CNS toxoplasmosis in patients with HIV is guarded. Results from a systematic review and meta-analysis of studies using trimethoprim-sulfamethoxazole for secondary prophylaxis showed a relapse rate of up to 16.4%.[25] If CNS toxoplasmosis is not adequately treated, complications such as deafness, seizures, and blindness can occur.[26][27]
Media
(Click Image to Enlarge)
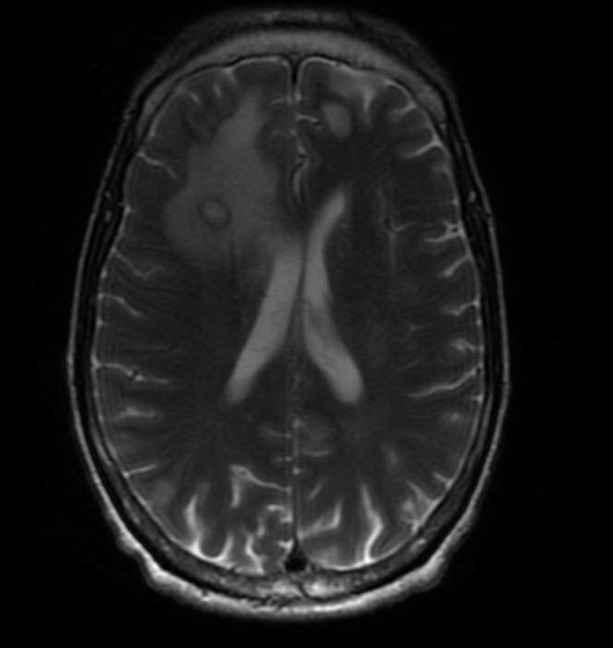
Cerebral Toxoplasmosis. This image shows a transverse section of the brain on T2-weighted MRI, with and without contrast. The ring-enhancing lesion with surrounding edema and minimal midline shift is characteristic of toxoplasmosis.
Contributed by F Ayoade, MD
References
Giovane RA, Lavender PD. Central Nervous System Infections. Primary care. 2018 Sep:45(3):505-518. doi: 10.1016/j.pop.2018.05.007. Epub 2018 Jul 9 [PubMed PMID: 30115337]
Paquet C, Yudin MH. No. 285-Toxoplasmosis in Pregnancy: Prevention, Screening, and Treatment. Journal of obstetrics and gynaecology Canada : JOGC = Journal d'obstetrique et gynecologie du Canada : JOGC. 2018 Aug:40(8):e687-e693. doi: 10.1016/j.jogc.2018.05.036. Epub [PubMed PMID: 30103893]
Tan IL, Smith BR, von Geldern G, Mateen FJ, McArthur JC. HIV-associated opportunistic infections of the CNS. The Lancet. Neurology. 2012 Jul:11(7):605-17. doi: 10.1016/S1474-4422(12)70098-4. Epub [PubMed PMID: 22710754]
Lee KH, Jiamsakul A, Kiertiburanakul S, Borse R, Khol V, Yunihastuti E, Azwa I, Somia IKA, Chaiwarith R, Pham TN, Khusuwan S, Do CD, Kumarasamy N, Gani Y, Ditangco R, Ng OT, Pujari S, Lee MP, Avihingsanon A, Chen HP, Zhang F, Tanuma J, Ross J, Choi JY. Risk factors for toxoplasmosis in people living with HIV in the Asia-Pacific region. PloS one. 2024:19(7):e0306245. doi: 10.1371/journal.pone.0306245. Epub 2024 Jul 1 [PubMed PMID: 38950027]
Bowen LN, Smith B, Reich D, Quezado M, Nath A. HIV-associated opportunistic CNS infections: pathophysiology, diagnosis and treatment. Nature reviews. Neurology. 2016 Oct 27:12(11):662-674. doi: 10.1038/nrneurol.2016.149. Epub [PubMed PMID: 27786246]
Ammassari A, Cingolani A, Pezzotti P, De Luca DA, Murri R, Giancola ML, Larocca LM, Antinori A. AIDS-related focal brain lesions in the era of highly active antiretroviral therapy. Neurology. 2000 Oct 24:55(8):1194-200 [PubMed PMID: 11071499]
Matta SK, Rinkenberger N, Dunay IR, Sibley LD. Toxoplasma gondii infection and its implications within the central nervous system. Nature reviews. Microbiology. 2021 Jul:19(7):467-480. doi: 10.1038/s41579-021-00518-7. Epub 2021 Feb 24 [PubMed PMID: 33627834]
Aerts R, Mehra V, Groll AH, Martino R, Lagrou K, Robin C, Perruccio K, Blijlevens N, Nucci M, Slavin M, Bretagne S, Cordonnier C, European Conference on Infections in Leukaemia group. Guidelines for the management of Toxoplasma gondii infection and disease in patients with haematological malignancies and after haematopoietic stem-cell transplantation: guidelines from the 9th European Conference on Infections in Leukaemia, 2022. The Lancet. Infectious diseases. 2024 May:24(5):e291-e306. doi: 10.1016/S1473-3099(23)00495-4. Epub 2023 Dec 19 [PubMed PMID: 38134949]
Pittman KJ, Knoll LJ. Long-Term Relationships: the Complicated Interplay between the Host and the Developmental Stages of Toxoplasma gondii during Acute and Chronic Infections. Microbiology and molecular biology reviews : MMBR. 2015 Dec:79(4):387-401. doi: 10.1128/MMBR.00027-15. Epub [PubMed PMID: 26335719]
Montoya JG, Liesenfeld O. Toxoplasmosis. Lancet (London, England). 2004 Jun 12:363(9425):1965-76 [PubMed PMID: 15194258]
Level 3 (low-level) evidenceWang ZD, Wang SC, Liu HH, Ma HY, Li ZY, Wei F, Zhu XQ, Liu Q. Prevalence and burden of Toxoplasma gondii infection in HIV-infected people: a systematic review and meta-analysis. The lancet. HIV. 2017 Apr:4(4):e177-e188. doi: 10.1016/S2352-3018(17)30005-X. Epub 2017 Feb 1 [PubMed PMID: 28159548]
Level 1 (high-level) evidenceSengupta PP, Jacob SS, Suresh KP, Rajamani S, Maharana SM. Exploring global trends in human toxoplasmosis seroprevalence by meta-analysis. Experimental parasitology. 2025 Aug:275():108971. doi: 10.1016/j.exppara.2025.108971. Epub 2025 Jun 23 [PubMed PMID: 40562157]
Level 1 (high-level) evidenceJones JL, Kruszon-Moran D, Elder S, Rivera HN, Press C, Montoya JG, McQuillan GM. Toxoplasma gondii Infection in the United States, 2011-2014. The American journal of tropical medicine and hygiene. 2018 Feb:98(2):551-557. doi: 10.4269/ajtmh.17-0677. Epub 2017 Dec 14 [PubMed PMID: 29260660]
Jones JL, Kruszon-Moran D, Rivera HN, Price C, Wilkins PP. Toxoplasma gondii seroprevalence in the United States 2009-2010 and comparison with the past two decades. The American journal of tropical medicine and hygiene. 2014 Jun:90(6):1135-9. doi: 10.4269/ajtmh.14-0013. Epub 2014 Apr 7 [PubMed PMID: 24710615]
Ho YC, Sun HY, Chen MY, Hsieh SM, Sheng WH, Chang SC. Clinical presentation and outcome of toxoplasmic encephalitis in patients with human immunodeficiency virus type 1 infection. Journal of microbiology, immunology, and infection = Wei mian yu gan ran za zhi. 2008 Oct:41(5):386-92 [PubMed PMID: 19122919]
Barragan A, Sibley LD. Transepithelial migration of Toxoplasma gondii is linked to parasite motility and virulence. The Journal of experimental medicine. 2002 Jun 17:195(12):1625-33 [PubMed PMID: 12070289]
Dhakal R, Gajurel K, Pomares C, Talucod J, Press CJ, Montoya JG. Significance of a Positive Toxoplasma Immunoglobulin M Test Result in the United States. Journal of clinical microbiology. 2015 Nov:53(11):3601-5. doi: 10.1128/JCM.01663-15. Epub 2015 Sep 9 [PubMed PMID: 26354818]
Javvi F, Sahebi K, Asgari Q, Mikaeili F, Teimouri A. Clinical courses and outcomes of cerebral toxoplasmosis in HIV-positive patients in Shiraz, Southern Iran: a retrospective study. BMC infectious diseases. 2025 Jul 1:25(1):817. doi: 10.1186/s12879-025-11231-8. Epub 2025 Jul 1 [PubMed PMID: 40596926]
Level 2 (mid-level) evidenceButt AA, Michaels S, Kissinger P. The association of serum lactate dehydrogenase level with selected opportunistic infections and HIV progression. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases. 2002 Sep:6(3):178-81 [PubMed PMID: 12718831]
Christo PP, Vilela Mde C, Bretas TL, Domingues RB, Greco DB, Livramento JA, Teixeira AL. Cerebrospinal fluid levels of chemokines in HIV infected patients with and without opportunistic infection of the central nervous system. Journal of the neurological sciences. 2009 Dec 15:287(1-2):79-83. doi: 10.1016/j.jns.2009.09.002. Epub 2009 Sep 25 [PubMed PMID: 19782379]
DeMent SH, Cox MC, Gupta PK. Diagnosis of central nervous system Toxoplasma gondii from the cerebrospinal fluid in a patient with acquired immunodeficiency syndrome. Diagnostic cytopathology. 1987 Jun:3(2):148-51 [PubMed PMID: 2439268]
Tork M, Sadeghi M, Asgarian-Omran H, Basirpour B, Ahmadi S, Ghasemzadeh F, Sarvi S, Gholami S, Hosseini SA, Daryani A, Aghayan SA. Assessment of simultaneous IgM, IgG avidity, and IgA testing in diagnosis of acute toxoplasmosis in pregnant women: a systematic review and meta-analysis study. BMC pregnancy and childbirth. 2025 May 6:25(1):537. doi: 10.1186/s12884-025-07580-6. Epub 2025 May 6 [PubMed PMID: 40329230]
Level 1 (high-level) evidenceTeimouri A, Mohtasebi S, Kazemirad E, Keshavarz H. Role of Toxoplasma gondii IgG Avidity Testing in Discriminating between Acute and Chronic Toxoplasmosis in Pregnancy. Journal of clinical microbiology. 2020 Aug 24:58(9):. doi: 10.1128/JCM.00505-20. Epub 2020 Aug 24 [PubMed PMID: 32321784]
Dian S, Ganiem AR, Ekawardhani S. Cerebral toxoplasmosis in HIV-infected patients: a review. Pathogens and global health. 2023 Feb:117(1):14-23. doi: 10.1080/20477724.2022.2083977. Epub 2022 Jun 11 [PubMed PMID: 35694771]
Connolly MP, Haitsma G, Hernández AV, Vidal JE. Systematic review and meta-analysis of secondary prophylaxis for prevention of HIV-related toxoplasmic encephalitis relapse using trimethoprim-sulfamethoxazole. Pathogens and global health. 2017 Sep:111(6):327-331. doi: 10.1080/20477724.2017.1377974. Epub [PubMed PMID: 29052492]
Level 1 (high-level) evidenceRobert-Gangneux F, Meroni V, Dupont D, Botterel F, Garcia JMA, Brenier-Pinchart MP, Accoceberry I, Akan H, Abbate I, Boggian K, Bruschi F, Carratalà J, David M, Drgona L, Djurković-Djaković O, Farinas MC, Genco F, Gkrania-Klotsas E, Groll AH, Guy E, Hirzel C, Khanna N, Kurt Ö, Junie LM, Lazzarotto T, Len O, Mueller NJ, Munoz P, Pana ZD, Roilides E, Stajner T, van Delden C, Villena I, Pelloux H, Manuel O. Toxoplasmosis in Transplant Recipients, Europe, 2010-2014. Emerging infectious diseases. 2018 Aug:24(8):1497-1504. doi: 10.3201/eid2408.180045. Epub [PubMed PMID: 30014843]
Halonen SK, Weiss LM. Toxoplasmosis. Handbook of clinical neurology. 2013:114():125-45. doi: 10.1016/B978-0-444-53490-3.00008-X. Epub [PubMed PMID: 23829904]
Level 3 (low-level) evidence