Introduction
HIV can infect individuals of any age, gender, race, or social class. Due to the effectiveness of antiretroviral therapy, HIV infection is now seen as a manageable chronic disease. However, despite significant advancements in controlling the virus, the disease remains a major global health concern fed by and contributing to inequities.
The Joint United Nations Programme on HIV/AIDS (UNAIDS) estimates that 630,000 individuals died from AIDS-related causes in 2024.[UNAIDS.Global AIDS Update.2025] Forty million people are living with HIV, of whom 60% live in Africa, and 1.4 million of whom are children. In addition, 1.3 million individuals acquire HIV each year, most commonly through heterosexual contact.
The Centers for Disease Control and Prevention (CDC) estimated that 1.2 million people in the United States (US) were living with HIV at the end of 2022, of which 13% were unaware of their status.[HIVGov.US HIV Statistics.2025] Male-to-male sexual (MSM) contact accounts for 66% of all new HIV diagnoses in the US, with heterosexual contact accounting for 24% and intravenous drug use for 3%.[CDC.HIV Surveillance Report.2025] High-risk groups included MSM, transgender individuals, those with multiple partners or who do not use condoms, individuals who trade sex for money, goods, or services, those living in locations where the incidence is 3% or greater, and individuals who have had sexually transmitted infections (STIs) or who share injection drug needles, syringes, or other equipment.[1]
While new HIV diagnoses have declined significantly from their peak in the 1980s, progress on further reducing them has stalled in recent years, with an estimated 38,000 new diagnoses each year.[HIVGov.EHE Overview.2025] An analysis of US data from 2009 showed that 91.5% of HIV transmissions were from People Living With HIV (PLWH) who are undiagnosed and PLWH who are diagnosed but not in care.[2] Such analyses strengthen the case for systematically improving the HIV care continuum for better HIV prevention.[HIVGov.HIV Care Continuum.2025]
Targets and initiatives set by the United Nations (UN), the World Health Organization (WHO), and public health agencies of individual countries have fostered significant progress in scaling up testing and implementing antiretroviral therapy. However, knowledge of HIV status, use of preventive services, and access to retention in care for PLWH remain suboptimal in the United States and worldwide, with significant inequities between populations. UNAIDS has set the following "95-95-95" goals for 2025:
- Where 95% of all individuals with HIV know their status
- When 95% of all those who have HIV receive antiretroviral therapy
- With 95% of all individuals on antiretroviral therapy achieving viral suppression
Global progress has been made, with 26.9 million lives saved; however, the international community was not on track to achieve these ambitious goals, and by 2025, this progress became less likely due to major disruptions in global aid.[UNAIDS.Global AIDS Update.2025][3] (Please refer to the Monitoring, Surveillance, and Reporting and the Enhancing Healthcare Team Outcomes sections for more information on the 95-95-95 goals).
Understanding the biomedical HIV prevention approaches for clinicians is an essential part of an overall public health strategy to achieve global and national targets and reduce the global burden of this disease, as well as the modes of transmission of HIV, biomedical strategies for at-risk populations, implementation considerations for select populations, and public health measures of relevance across an interprofessional team. Please see StatPearls' companion resource, "HIV and AIDS," "HIV Testing,” and "HIV Antiretroviral Therapy," for further information on these HIV topics.
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
HIV infection can be transmitted through sexual intercourse, exposure to infected blood, or perinatally. The degree of viremia in the source individual, the general health of the exposed individual, the presence of other STIs in the exposed individual, and the use of preventive measures all affect the actual transmission rate. The development of effective, patient-centered clinical programming and services to prevent HIV depends on an understanding of these factors. (Please refer to the Other Issues section for more information on specific risk groups and factors influencing transmission rates, including poverty, stigma, and access to healthcare services.)
HIV Viremia in the Source Individual
Each log increase in viral load is estimated to increase the risk of HIV transmission 2.5-fold, with no viral transmission events noted from individuals who had a baseline viral load of less than 1500 copies/mL.[4] Patients with acute infections have a high viral load and experience viral shedding in bodily fluids, which increases their risk of transmitting the infection to their contacts.[5][6] On the other hand, sustained viral suppression minimizes the risk of transmission to an uninfected individual (serodiscordant).[7]
Prevention Strategies for the Sexual Transmission of HIV
Sexual transmissions account for the bulk of new infections in the US and worldwide. Receptive anal intercourse is the highest-risk sexual practice for HIV transmission, with approximately 138 infections per 10,000 exposures with an infected source, while insertive anal intercourse has an 11 in 10,000 exposure risk.[8] The risk of receptive and insertive vaginal intercourse is 8 and 4 per 10,000 exposures, respectively. The presence of other STIs, particularly those that are ulcerative, can result in HIV detection in bodily fluids, even in the presence of adequate serum control of HIV.[9][10][11][12]
Available barrier methods for the prevention of HIV transmission and other STIs include male and female condoms and dental dams. Male condoms remain the mainstay of barrier HIV prevention measures as they are cheap, readily available, effective, and protect against many other STIs. A Cochrane review found that consistent use of condoms during every sexual encounter resulted in an 80% decrease in HIV incidence.[13] Another meta-analysis showed condoms reduce HIV transmission by more than 70% when used consistently by HIV-serodiscordant heterosexual couples.[14] Therefore, the American College of Physicians and the HIV Medicine Association recommend the wide availability of condoms and education regarding their proper use to minimize the risk of HIV transmission.[15]
The use of male condoms is primarily the decision of the insertive male partner, with the receiving partner having little control. Female condoms have the advantage of transferring decision-making to the female, yet the method lacks widespread acceptance and understanding. Dental dams can be used during cunnilingus or anilingus, although these are likewise not commonly integrated into regular use.
Voluntary male medical circumcision is an effective preventive strategy to reduce the risk of heterosexually acquired HIV infections in men in settings with generalized epidemics, eg, in Eastern and Southern Africa.[WHO.Global HIV, Hepatitis, and STI Health Strategies.2022] One study from South Africa reported a 60% decrease in the risk of HIV infection amongst circumcised males as compared to uncircumcised men after controlling for behavioral factors, condom use, and health-seeking behaviors.[16] Adverse events related to circumcision are infrequent (1.5%) and usually resolve quickly.[17]
Prevention Strategies for Blood-Borne HIV Transmission
Needle-sharing injection drug use currently represents the most significant risk of HIV transmission via the blood-borne route, with an estimated 63 infections for every 10,000 exposures from an infected source. Sterile syringe programs (SSPs) are highly effective in decreasing the risk of HIV via this route but are often underutilized and face regulatory restrictions in some places.
The healthcare system has nearly eliminated transfusion-related transmission of HIV by effectively screening donors and testing all blood products. Otherwise, transfusion of HIV-infected blood almost always transmits the virus to the recipient.[18] Universal precautions for healthcare workers effectively decreased occupational exposure. The risk of HIV transmission from the reuse of needles and other medical equipment in healthcare settings has markedly declined since 2000, when the WHO began safe injection campaigns worldwide. Between 2010 and 2010, the global proportion of all HIV transmissions attributed to unsafe medical injections was estimated to have decreased by 87%, from 5% to 9% to less than 1.3%.[19] Similar decreases were seen for hepatitis B and C viruses (HBV and HCV). Iatrogenic risks of HIV transmission remain for those requiring medical care during times of political strife, war, or migration, where infection prevention and control procedures are substandard.
Prevention Strategies for Maternal-Infant HIV Transmission
Without treatment, the risk of vertical transmission from mother to infant is 15% to 30% with an additional risk of 10% to 20% associated with breastfeeding.[20] The effectiveness of treatment in preventing transmission depends on how early treatment is initiated and the viral load during pregnancy. Antiretroviral therapy with viral suppression throughout pregnancy and childbirth, combined with antiretroviral therapy for the infant for 4 to 6 weeks after birth, has been shown to decrease the overall rate of HIV transmission to 0.1% to 0.5%.[21]
Clinical Significance
Pharmacologic HIV Prevention Strategies
Abstinence and condom use are effective at preventing HIV and STI infection, but high-risk persons do not consistently use these methods. After testing for HIV, antiretroviral medications used either as preexposure prophylaxis (PrEP), postexposure prophylaxis (PEP), or treatment as prevention (TasP) are highly effective in decreasing the transmission of HIV (see Table. HIV Prevention Measures). A cornerstone of any HIV prevention strategy, antiretrovirals should be offered to all at-risk individuals. PrEP and TasP require intensive patient engagement and frequent follow-up visits at a health facility. They must be given in conjunction with access to condoms, regular testing for STIs, and intensive counseling for behavioral risk reduction, including safer sex or injection practices as appropriate. Patients must be advised that antiretrovirals do not prevent pregnancy or STIs (eg, syphilis, chlamydia, and gonorrhea).
Individuals most at risk of HIV often have challenges with adhering to therapy due to multiple structural barriers, and loss to follow-up is common.[22] PrEP navigators, telehealth or telephone check-ins, smartphone reminders, delivery services, directly observed therapy, and pillboxes may enhance adherence. Substance use treatment and mental health services should be integrated into HIV treatment and preventive services as appropriate.
Treatment as Prevention
All PLWH should be treated with antiretroviral therapy as soon as they are diagnosed.[23] This approach extends their lives and prevents onward transmission of the virus.[24] TasP is the initiation of antiretroviral therapy (typically a 3-drug antiretroviral regimen) in PLWH to prevent further transmission to uninfected persons. An overwhelming body of evidence supports the TasP approach, also known as "undetectable=untransmittable" (U=U). Clinical data only support U=U for sexual transmission. Even with undetectable viral loads, HIV transmission still occurs perinatally and via breast milk, and TasP's effectiveness in preventing exposure through blood has not been determined.[Panel on Antiretroviral Guidelines for Adults and Adolescents.[NIH.Antiretroviral HIV Agent Guidelines.2024]
From 2011 to 2019, the HPTN052, PARTNER 1, PARTNER 2, and Opposites Attract studies followed mixed-status MSM and heterosexual couples to assess HIV transmission rates from the partner living with HIV on antiretroviral therapy. These showed 100% efficacy in preventing HIV transmission if antiretroviral therapy is taken as prescribed, and an undetectable viral load is achieved (defined as <200 copies of HIV-1 RNA/mL of plasma).[25][26][27]
For both clinical and public health outcomes, HIV treatment with antiretroviral therapy as soon as possible and preferably within 7 days after diagnosis is recommended for all individuals with HIV, regardless of their CD4 count or the stage of the disease.[NIH.Antiretroviral HIV Agent Guidelines.2024][WHO.Global HIV, Hepatitis, and STI Health Strategies.2022] Uptake and adherence remain suboptimal in the US and worldwide. Many factors contribute to this, including undiagnosed HIV infection, lack of access to quality healthcare, poor linkage between testing and treatment, uneven knowledge gaps in the understanding of U=U, personal factors, and the social context in which HIV infection occurs.[28][29][30] For example, the CDC estimates that 35% of individuals under clinical care for HIV in 2022 did not achieve viral suppression, and 46% were not retained in care, defined as either a CD4 or viral load within 3 months.[CDC.HIV in the US Factsheet.2024]
Supporting patients to achieve and maintain an undetectable viral load is crucial to maximizing the benefits of TasP, including guidance on taking antiretroviral therapy as prescribed, frequent viral load testing until viral suppression is achieved (typically within 6 months), and regular follow-up testing every 3 to 6 months thereafter, to ensure long-term adherence to therapy. Viral load increases within a few weeks if treatment is stopped.[25] Patient-centered interventions, such as text reminders, community health workers and advocates, and men- and youth-friendly services, may facilitate patient linkage to care and adherence to treatment. Please see StatPearls' companion resource, "HIV and AIDS," for further information on treatment indications, options, adverse effects, and contraindications, and the latest Health and Human Services (HHS) guidelines for the use of antiretroviral agents in adults and adolescents with HIV.[NIH.Antiretroviral HIV Agent Guidelines.2024]
Preexposure Prophylaxis
Multiple large trials demonstrated the efficacy of oral and injectable PrEP in decreasing HIV transmission risk to individuals at high risk of acquiring HIV across sex, age, and risk category. The risk of HIV is 86% lower for patients who take oral PrEP consistently compared to those who take a placebo.[31] The effectiveness of PrEP is significantly reduced with inconsistent use. More recent studies have shown that long-acting injectable cabotegravir and lenacapavir were superior to oral PrEP.[32][33][34][35] The first long-acting injectable PrEP, cabotegravir, was approved in the US in 2021 and recommended by the CDC.[CDC.PrEP Prevention of HIV Infection Guidelines.2021] The FDA approved the use of lenacapvir as PrEP in 2025, and both the CDC and the WHO have recommended lenacapavir as PrEP.[WHO.FDA Approval of Lenacapavir.2025][CDC.Clinical Recommendation for Lenacapavir in HIV Preexposure Prophylaxis.2025][WHO.Recommendation for Lenacapavir in HIV Prevention.2025]
Updated national and local guidelines should be consulted when assisting patients in making decisions for PrEP. In August 2023, based on FDA approvals and CDC recommendations, the US Preventive Services Task Force recommended oral tenofovir disoproxil fumarate/emtricitabine (TDF/FTC), oral tenofovir alafenamide/emtricitabine (TAF/FTC), or injectable cabotegravir for use in at-risk adults and adolescents weighing at least 35 kg (77 lb) to reduce the risk of sexually acquired HIV. TAF/FTC is not recommended for women at risk, as this therapy was not studied for persons at risk of vaginal acquisition of HIV.[USPSTF.Preexposure Prophylaxis for HIV Prevention.2023]
The dapivirine vaginal ring has been recommended by the WHO for HIV preexposure prophylaxis and is approved by the European Medicines Agency but not the US FDA. Dapivirine can reduce the risk of HIV infection by 63% in women who consistently use the ring; however, this therapy is best implemented in settings with generalized HIV epidemics where it is most applicable.
Preexposure Prophylaxis Clinical Guidance
Sexually active adults and adolescents who have had anal or vaginal sex in the past 6 months with any of the following criteria are eligible for and should be offered PrEP:
- A partner with HIV (especially if the partner has an unknown or detectable viral load)
- A bacterial STI in the last 6 months
- A history of inconsistent or no condom use with partners whose HIV status is unknown
- Individuals who inject drugs and share injection equipment
- All patients who request it, regardless of known risk factors, since many individuals hesitate to share details of their sexual or drug use behaviors.[CDC.Clinical Guidance for PrEP.2025]
The choice of PrEP regimen should be based on a discussion between the patient and clinician and based on the person's risk factor profile, comorbid conditions, preference for oral or injectable medications, and ability to take medications reliably, in addition to the adverse effect profile and cost of the medication if not covered through insurance or pharmaceutical-sponsored programs.[1]
Oral PrEP can be taken as 1 tablet once a day of TDF/FTC (300 mg/200 mg) by all those at risk of acquiring HIV, including those who are pregnant or breastfeeding.[1] One tablet orally of tenofovir alafenamide (TAF)/FTC (25 mg/200 mg) daily is an equal alternative for cisgender men and others at risk who do not have receptive vaginal sex, including those at risk solely due to injection drug use. Using TAF for individuals in these populations with a creatinine clearance between 30 and 60 mL/min, or those with a history of known osteoporosis or osteopenia, is preferable. However, TAF/FTC is not indicated for women at risk of HIV via vaginal penetration, as no trial data are available for this population.[1]
MSM who can identify high-risk sexual events at least 2 hours beforehand can take oral PrEP "on demand."[1] This preventive strategy is also known as episodic or "2:1:1" on-demand, whereby PrEP is taken as 2 tablets of TDF/FTC orally at least 2 hours, but up to 24 hours before the sexual encounter, and then 1 tablet on each of the 2 days after the sexual encounter.[CDC.Oral HIV PrEP Guidance.2024] TAF/FTC cannot be used for episodic PrEP. Episodic PrEP is not indicated for individuals at risk of HIV from receptive vaginal or neovaginal sex or injection drug use due to the lack of studies in these populations. Episodic therapy must be used with caution in transgender women receiving gender-affirming therapy, as PrEP may take longer to reach adequate concentrations in rectal tissues to prevent HIV.[1]
Cabotegravir can be used for the prevention of sexual transmission of HIV across populations, including those PWID who are also at risk of acquiring HIV through sex and pregnant individuals.[1] Cabotegravir is administered as a gluteal intramuscular injection every 8 weeks, with an optional 28-day oral lead-in period preceding the first injection. Lenacapavir involves a mandatory oral loading dose for 2 days beginning on the day of the first subcutaneous injection, and is then administered subcutaneously every 26 weeks.
Preexposure Prophylaxis Discontinuation Testing
PrEP should be started as soon as possible for those at risk, including on the same day if the patient is willing and has no signs or symptoms of acute HIV, a documented negative HIV test result no more than 1 week prior, and has no contraindicated medications or conditions (see Image. HIV Testing and PrEP Discontinuation). An HIV antigen-antibody test is done after initiation of PrEP if the decision to start is based on a rapid or point-of-care HIV test. As tenofovir rarely causes renal disease, patients opting for oral PrEP must have a creatinine clearance of at least 60 mL/min or at least 30 mL/min at baseline for TDF and TAF, respectively, and subsequently undergo retesting at 6- to 12-month intervals. Testing of blood for HBV antigens informs the choice of PrEP, as TDF/FTC is also used to treat HBV; the presence of HBV would not exclude using PrEP, but the patient would need to be evaluated and counselled separately because the stoppage of TDF may result in a hepatitis flare from an HBV viral rebound.
The patient must have a negative HIV test result at least every 3 months before receiving each prescription refill for oral drugs or at least every 2 months before each injection, as taking PrEP with preexisting HIV can result in resistance and suboptimal viral control if infected (see Image. HIV Testing and PrEP).[CDC.Oral HIV PrEP Guidance.2024] All persons being considered for PrEP must have a recently documented negative HIV antigen-antibody test result. If these patients have taken oral PrEP or postexposure prophylaxis in the past 3 months, or injectable cabotegravir in the past 12 months, the CDC recommends testing with both an HIV antigen-antibody assay and an HIV-1 RNA assay.[UAB.Baseline Evaluation and Starting HIV PrEP.2025] After starting PrEP, patients should be tested for HIV and STIs every 3 to 6 months with a combined HIV antigen-antibody assay or a blood-based point-of-care test. Following discontinuation of PrEP, there should be retesting for HIV for 45 days.[BASHH.HIV PrEP Guidelines.2025] The detection of HIV may be significantly delayed after cessation of injectable long-acting PrEP, so prolonged testing up to 12 months after PrEP is necessary, bearing in mind that nucleic acid amplification methods are the most likely to detect a new infection.
Postexposure Prophylaxis
The decision to begin PEP is based on calculating the risk of taking PEP against the risk of acquiring HIV after a specific exposure. HIV risk depends on the likelihood that the source person has HIV and, if so, whether the viral load is detectable and the type of exposure, for example, the type of sexual encounter, size of the needle in a needle stick exposure, and type and size of mucosal exposure.
Nonoccupational PEP (nPEP) is given when an individual seeks medical treatment within 72 hours after being exposed in a nonoccupational setting to semen, vaginal fluid, or blood that is confirmed or suspected to be infected with HIV. If the source individual is known not to have HIV by testing or the exposure is more than 72 hours in the past, nPEP is not indicated. If the exposure source is known to have HIV, the type of exposure needs to be evaluated for the significance of the risk. If the HIV status of the source patient is unknown, evaluation is on a case-by-case basis. A rapid HIV test should be obtained, and an assessment made for any other potential exposure-related risks, eg, STIs, hepatitis B and C, and pregnancy. In occupational PEP (oPEP), the opportunity to test and monitor the source person exists in most cases.
In both oPEP and nPEP, antiretroviral therapy must be started as soon as possible, preferably within 72 hours of exposure, and continued for 4 weeks. The preferred regimen for nPEP and oPEP in otherwise healthy adults and adolescents is 1 tablet of TDF/emtricitabine once daily, with either raltegravir 400 mg twice daily or dolutegravir 50 mg once daily, for a duration of 4 weeks.[CDC.Clinical Guidance for PEP.2025]
Patients seeking nPEP should be referred for PrEP if they are at repeated risk for HIV infection or if nPEP has been sought more than once in the past 12 months. PEP regimens have few adverse effects and minimal risk of HIV resistance, yet use by clinicians is still low. Healthcare practitioners should take full advantage of the PEP consultation service for clinicians; a hotline is available in the US at 844-275-6222.[AETC.National Clinician Consultation Center.2025]
Table. HIV Prevention Measures
|
Strategy |
Typical Efficacy Versus HIV Acquisition* |
Indications |
Key Precautions |
|
Efficacy of 70% to 91% (when consistently practiced) |
Anyone choosing to avoid sex (temporarily or long-term) |
|
|
|
Condoms (External/Internal) [14] |
Approximately 70% to 90% risk reduction efficacy with consistent, correct use |
|
|
|
Voluntary Male Medical Circumcision [38][WHO.Global HIV, Hepatitis, and STI Health Strategies.2022] |
Efficacy of approximately 50% to 60% reduction in female-to-male acquisition |
Heterosexual men in high-prevalence settings |
|
|
Efficacy of approximately 100% when the HIV-positive partner has a viral load of <200 copies/mL |
|
|
|
|
Dapivirine Vaginal Ring [40][WHO.Dapivirine Vaginal Ring HIV Prevention.2022] |
|
Cisgender women at substantial risk who want a monthly user-controlled option |
|
|
Oral TDF/FTC (Preexposure Prophylaxis) [CDC.Clinical Guidance for PrEP.2025][NIHGov.Preexposure Prophylaxis.2025] |
|
|
|
|
Oral TAF/FTC (Preexposure Prophylaxis) [41][CDC.Clinical Guidance for PrEP.2025] |
|
MSM and transgender women without vaginal exposure risk |
|
|
Injectable Cabotegravir (Preexposure Prophylaxis) [CDC.Clinical Guidance for PrEP.2025][32][33] |
|
Patients preferring injections or with pill adherence issues |
|
|
Injectable Lenacapavir (Preexposure Prophylaxis) [WHO.Recommendation for Lenacapavir in HIV Prevention.2025] |
|
Patients preferring injections or with pill adherence issues |
|
|
Nonoccupational Postexposure Prophylaxis [CDC.Clinical Guidance for PrEP.2025] |
Effective if started ≤72h, 28-day 3-drug regimen (randomized control trials are unethical, so no specific data available) |
After sexual, needle, or other nonoccupational exposures |
|
|
Occupational Postexposure Prophylaxis [CDC.Clinical Guidance for PrEP.2025] |
A 28-day 3-drug regimen is typically used (randomized control trials are unethical, so no specific data available, except for an 81% reduction with zidovudine only in a historic case-control study) |
Percutaneous/mucosal occupational exposures |
|
|
Prevention of Mother-to-Child Transmission [NIHgov.HIV and Pregnancy.2025][WHO.Mother-To-Child HIV Transmission.2025] |
Use antiretroviral therapy for an approximately 99% reduction |
Pregnant women must be tested for HIV and if positive, must initiate antiretroviral therapy and continue postpartum, including avoidance of breastfeeding postpartum |
If HIV is untreated or viral loads exceed 1,000 copies/mL during pregnancy, a cesarean delivery (or cesarean section) is indicated |
* Efficacy estimates assume consistent and correct use of biomedical interventions; real-world effectiveness depends heavily on adherence and exposure type.
Other Issues
Population-Specific HIV Transmission Prevention Strategies
More than 40 years of global experience in preventing HIV has demonstrated that a patient-centered approach is required for optimal prevention and treatment of HIV. Clinicians must be aware of groups at higher risk of transmission to tailor and improve the quality of services offered by programs to people with or at high risk of HIV.
Mother-to-child HIV transmission
The global reduction in HIV transmission from mother to child is a significant public health victory, with universal testing and the offering of treatment being the cornerstones of prevention. The WHO has the triple aim to eliminate maternal-child transmission of HIV, HBV, and syphilis and has advanced a 4-pillar strategy.[WHO.Global HIV, Hepatitis, and STI Health Strategies.2022] All individuals, irrespective of risk status, should be tested if trying to conceive and as early as possible in pregnancy. Those who are at higher risk should have repeat testing in the third trimester, including in areas with high HIV incidence.[HIVgov.HIV Antiretroviral Drugs in Pregnancy.2025] Some US states and territories mandate repeat third-trimester testing.[CHLP.Compendium of State HIV Testing Laws.2011] HIV transmission is further reduced if rapid HIV testing is performed at the time of delivery, if the HIV status of a client is unknown, or if they live in a high-incidence area.
Testing must be paired with the immediate offer of antiretroviral therapy with a recommended 3-drug regimen preconception or as early as possible during pregnancy. The necessary support should be given to help pregnant persons achieve undetectable levels rapidly.[HIVgov.HIV Antiretroviral Drugs in Pregnancy.2025] Give zidovudine intrapartum to all women with a high viral load or at risk of high viral load, whether or not they are on antiretroviral therapy. All infants exposed to HIV in the perinatal period should receive 1 or more antiretroviral drugs, dosed appropriately for the infant’s gestational age and weight and initiated as close to the time of birth as possible, preferably within 6 hours.
Breast milk can also transmit HIV to the child. Using infant formula or donor human milk instead of breast milk eliminates the risk. Individuals who achieve and maintain viral suppression may opt to breastfeed with the understanding that the risk of transmission to the child is less than 1% but not zero.[HIVgov.HIV Antiretroviral Drugs in Pregnancy.2025]
Gay, bisexual, and other men who have sex with men transmission
As the group with the highest rate of HIV in the US, people who have male-to-male sexual contact are a priority group for HIV prevention. Anal intercourse is the highest risk sexual behavior for HIV transmission, with receptive anal sex being 13 times riskier than penetrative anal sex.[8] Gay and bisexual men are also at higher risk of STIs, which increases the risk of HIV transmission. In 2022, 86% of gay and bisexual men were reported to know of their HIV status, similar to other people with HIV, and 68% achieved viral suppression on antiretroviral therapy. An estimated 93% of gay and bisexual men in the US were aware of PrEP in 2023.[CDC.HIV and Gay and Bisexual Men.2024]
However, inequalities exist across subpopulations. Black gay and bisexual men are the subpopulation most affected by HIV in the US, comprising 32% of all MSM living with HIV at year-end 2022. Hispanic/Latino gay and bisexual men are likewise disproportionately affected at 28% of all MSM living with HIV. Gay and bisexual men in these groups are less often aware of their HIV status and have lower awareness and use of PrEP as compared to other gay and bisexual men. While linkage-to-care and viral suppression rates are lower in Black gay and bisexual men as compared to other gay and bisexual men. However, this is not the case for Hispanic/Latino gay and bisexual men.[CDC.HIV and Gay and Bisexual Men.2024]
Black gay and bisexual men are at greater risk of being exposed to HIV because of the higher prevalence of HIV in this group, a greater likelihood of sexual partners of the same race, and lower use of PrEP as compared to other ethnicities. Addressing racism, discrimination, HIV stigma, and homophobia, as well as poverty, homelessness, incarceration, and other factors, might give access to quality healthcare services and improve health outcomes.
People who inject drugs
About 3.7 million people in the US used injected drugs in 2018, a number that increased significantly over the previous 10 years.[41] PWID of all genders who share syringes or other drug equipment are at a very high risk of becoming infected with HIV, hepatitis B and C, and other pathogens due not only to injection drug use but also because of at-risk sexual encounters.
In 2018, only 55% of PWID met CDC guidelines for annual HIV testing, and nearly one-third reported using a syringe after someone else had previously used it, which was more common among young PWID.[42] However, this group of people experiences numerous barriers to care, including homelessness, incarceration, and lack of health insurance. Greater efforts are necessary to increase the rates of testing, linkage to care, and retention in care, as well as viral suppression.
The most effective means for preventing PWID from transmitting or acquiring HIV is to stop injecting. However, individuals may be unable or unwilling to do so at a given point in time, or they may have little or no access to effective treatment services. The WHO and other HIV experts recommend a comprehensive set of harm reduction services for this population, including Syringe Services Programs (SSPs), opioid agonist maintenance therapy for those dependent on opioids, and the community distribution of opioid antagonist therapy for the management of overdose, in addition to services for testing, diagnosis, and management of HIV and viral hepatitis.[WHO.Recommended Interventions for People Who Inject Drugs.2023]
SSPs are highly effective at decreasing rates of HIV, viral hepatitis, and other infections, approximately halving the incidence of HIV and HCV.[CDC.Syringe Services Programs.2024] They are cost-saving to the health care system and do not increase illegal drug use or crime. SSPs are also an effective mechanism to reach PWID, an often highly marginalized population, that can facilitate access to PrEP, provide harm reduction education, increase access to condoms, and connect individuals to HIV testing and treatment facilities. A systematic review found that PWID have a high awareness and willingness to use PrEP, but PrEP uptake was low (0%-3%).[43]
Populations with socioeconomic barriers to care
The End the HIV Epidemic in the US, announced in 2019, aimed to reduce new infections by 75% within 5 years and achieve at least a 90% reduction within 10 years.[HIVGov.EHE Overview.2025] CDC leaders have stated that to make significant strides in the campaign against HIV, “will require a comprehensive strategy including community-based, targeted, and self-testing, a cohort approach for persons with HIV to meet their service needs, PrEP for all persons at substantial risk for acquiring HIV, expanded comprehensive syringe services programs, housing stability, and detection of and response to growing clusters of infections.” [44]
Globally, the WHO has previously set the 95-95-95 goal. Challenges to this international goal include limitations of healthcare systems (eg, those experienced in low- and middle-income countries) as well as inequalities in specific populations. For example, in South Africa, female sex workers and MSM living with HIV were less likely to know their HIV-positive status than the general population and thus often present with advanced HIV infection before initiating antiretroviral therapy. Antiretroviral therapy coverage of children living with HIV is well below that of adults.[45] At the global level, the impact of PrEP is limited by multiple barriers across social, structural, and individual levels. Stigma and discrimination often associate PrEP with promiscuity or HIV infection, deterring groups like female sex workers, men who have sex with men, and transgender women from accepting the prevention measure. Misconceptions, limited awareness, low perceived risk, and partner disapproval further reduce uptake, eg, in persons living with a serodiscordant partner. Cultural discomfort with discussing sexuality also impedes access. Structural challenges include high medication and monitoring costs, inadequate funding, and poor access to clinics—especially in rural or resource-limited settings. Clinician-related barriers, eg, limited knowledge, bias about sexual behaviors, or how non-HIV-specialists do not view at-risk persons as being at-risk, thus missing opportunities to prescribe treatment or prevention. At the individual level, adverse effects, adherence difficulties with daily pills, and concerns about risk compensation undermine use. Additionally, distrust in healthcare systems discourages individuals from engaging in care. While long-acting injectable PrEP may ease adherence, rollout is hindered by high costs, infrastructure demands, and insurance complexities.
Public HIV Education and Testing for Transmission Prevention
Public and patient education remains a cornerstone of primary HIV prevention, with clinicians, public health agencies and organizations, and community partners all playing a role. All adolescents and adults who are sexually active or inject nonprescribed drugs should be aware of measures to prevent the acquisition of HIV.[46][WHO.HIV and AIDS.2025] Preventive measures that should be advised include:
- Use male or female condoms consistently during penetrative sex.
- Get tested regularly for HIV and STIs.
- Use antiretroviral drugs for preexposure prophylaxis if recommended by a clinician.
- Request postexposure prophylaxis if concerned about a risky exposure.
- Use harm reduction services where available for people who inject and use nonprescribed drugs.
- Consider voluntary medical male circumcision if living in a setting with a generalized epidemic.
For those living or at high risk of acquiring HIV, interprofessional teams, including community health workers, nurses, pharmacists, and mental health professionals, are required to reinforce these messages, ensure adherence to medications, and provide a linkage to ancillary services to improve linkage to and retention in care. In the US, the Ryan White HIV/AIDS Education and Training Center (AETC) Program has materials to train nurses, physicians, advanced practice registered nurses, physician assistants/associates, pharmacists, behavioral health professionals, health profession faculty, clinical leaders, healthcare teams, and oral health professionals.[AETC.Ryan White HIV/AIDS Education and Training Center.2025]
Measures targeting clinicians are also necessary, as some may not be aware of prevention measures (eg, PrEP and TasP/U=U) or have judgmental attitudes that lead to a lack of sharing information regarding these strategies with people at risk of or living with HIV.[28] Education targeting healthcare practitioners should be comprehensive to ensure that information and support are readily available to patients when and where needed, including primary care practitioners well known to the patient and others with less frequent connections, eg, community health workers, pharmacists, or specialist physicians.
HIV testing
Easy access to HIV testing is the pivotal first step in HIV care and prevention. Testing facilitates early diagnosis and treatment of HIV, significantly improving the long-term health of PLWH. In the US, an estimated 30% of all HIV infections are transmitted by people who are unaware of their HIV status, which underscores that testing is also a prevention measure.[2]
The CDC recommends screening broadly within the US population.[CDC.HIV Screening Recommendations.2025] The following screening regimen is recommended for the following populations:
- At least once for everyone between the ages of 13 and 64 as part of routine health care
- In healthcare settings for all adolescents, adults, and pregnant individuals
- At least once a year for anyone with a higher risk of acquiring HIV, including:
- Those who have had more than 1 partner since their last test
- Those who have been diagnosed with an STI, hepatitis, or tuberculosis
- Individuals who shared needles, exchanged sex for drugs or money, had sex with someone with HIV, or have had same-sex intercourse with a man
- All pregnant women before or as soon as possible after conception and in the third trimester if risk factors exist [HIVgov.HIV Antiretroviral Drugs in Pregnancy.2025]
Currently, 3 primary types of HIV testing may be used, with variable times between exposure to HIV and test positivity. However, none can detect the virus immediately after diagnosis. Generally speaking, HIV can be detected earlier in venous blood than from a finger stick sample or oral fluid.[CDC.HIV Screening Recommendations.2025] These primary methods include:
- Antibody tests: This testing method can detect HIV within 23 to 90 days after exposure to HIV (ie, it takes at least 23 days and up to 90 days after exposure for the test to become positive). They are the technology used for the most rapid tests and the only Food and Drug Administration-approved HIV self-test.
- Antigen-antibody tests: This testing method detects the viral p24 antigen and antibodies, which the immune system develops in response to the virus. Antigen-antibody tests are commonly used for laboratory testing and can detect HIV 18 to 45 days after exposure. A rapid fingerstick antigen-antibody test can detect the virus in 18 to 90 days.
- Nucleic acid tests: These tests detect the actual virus in the blood and can detect HIV within 10 to 33 days after exposure. Nucleic acid tests are used as a confirmatory test after an antibody or antibody-antigen test, or when someone has a recent exposure and a negative antibody or antibody-antigen test result.
In addition to testing in healthcare settings, self-testing, and testing of self-collected samples, testing in nonclinical or community settings is a vital tool to make testing easy and accessible to individuals in various mental, social, or geographic contexts. Often paired with other HIV prevention services or STI testing, testing in nonclinical settings can be an effective means of bringing testing to people who may otherwise not get tested, particularly those who are highly stigmatized and at high risk. Research shows that MSM who use take-home tests test themselves more frequently, identify more infections, do not increase risky sexual behaviors, and share their results with their social networks, raising others' awareness of their HIV infection.[55][47]
Quality HIV prevention and care services access
Sufficient and stable funding for HIV programming is of critical importance, influencing the availability and penetration of interventions, particularly in low- and middle-income countries.[45] Indeed, in areas of Africa where funding has supported widespread testing and treatment paired with a variety of patient-centered measures tailored to at-risk populations, population-level viral suppression has exceeded that of the US.[30] Remarkably, by 2024, Eastern and Southern Africa had reached 93-91-95 in the 95-95-95 targets for testing, treatment, and viral suppression, respectively, in PLWH.[UNAIDS.Global AIDS Update.2025] However, the 2025 disruptions to the global funding and infrastructure for HIV care threaten to undermine this progress.
While PrEP shows considerable promise, by 2024, PrEP was made available to less than a fifth of the 21 million people the WHO targeted as eligible.[UNAIDS.Global AIDS Update.2025] Additionally, recommendations for PrEP have not been adopted in national guidelines in Russia, China, Angola, Libya, Sudan, and Venezuela, amongst others.[WHO.Global Implementation of WHO HIV Policy.2023] The addition of PrEP to locally available prevention measures is necessary to end global transmission of HIV, particularly in areas with a high burden of HIV.[46]
Putting patients at the center enables maximum benefit from TaSP, PrEP, and other prevention measures, leading to improved clinical and public health outcomes.[WHO.Framework for People Centered Health Services.2016][WHO.Men and HIV Interventions.2023] For example, due to its ease of use for those facing barriers to regular, daily medication use, cabotegravir or lenacapavir may be ideal for PrEP. To improve patient-centered care, the WHO recommends linking strategies and treatment of related diseases or syndromes, eg, in its strategy for HIV, viral hepatitis, and STIs.[WHO.Global HIV, Hepatitis, and STI Health Strategies.2022] Important patient-centered outcomes, eg, self-stigma, can be reduced through interventions (eg, TasP), in addition to more standard outcomes, eg, increased testing, adherence to therapy, and viral suppression.[48][49] Conveying the U=U message to PLWH is essential for clinicians
Systems, sectors, and partnerships must be optimized for impact. Strategies and programs should be based on a cohesive theoretical model of change that addresses individual, clinician, and institutional barriers to coordinate care activities across sectors, ensures consistent implementation, and achieves the desired outcomes.[WHO.Global HIV, Hepatitis, and STI Health Strategies.2022] A growing body of public health intervention research on the influence of social and structural determinants of health, intersectionality, and patient-centered interventions helps guide quality improvement measures for HIV prevention.
Including communities and civil society in advocacy, service delivery, and policymaking ensures that services are culturally appropriate and responsive to the needs of the population they serve. For example, partnering with community organizations has been shown to improve linkage to care for HIV treatment, decreasing the time to viral suppression and reducing the risk of HIV transmission.[22] When implemented broadly in locally defined at-risk populations, the use of PrEP as prescribed could have a powerful influence on reducing incident HIV transmission at the population level. Community-level interventions, eg, door-to-door HIV prevention services, may be beneficial in areas of high incidence, eg, urban areas with high levels of poverty.[50]
A clear understanding of the social context in which HIV infection occurs is vital to providing high-quality programming. For example, while TasP use has increased over time, particularly among MSM, its optimal use is hampered by disbelief that U=U among people who do not have HIV and those living in Africa. Acceptability is high once the science is understood. HIV care and prevention models that address the overlapping clinical and social complexities faced by many equity-deserving populations can lead to better clinical outcomes. Structural interventions to improve socioeconomic conditions may also reduce HIV infection rates.[51][52][53]
Specialist or targeted clinics for HIV care may best serve people who experience a high degree of stigma, including people who are Indigenous or transgender, who inject drugs, or who sell sex, and those at risk due to multiple factors. While research shows comprehensive SSPs for PWID to be safe, effective, cost-effective, and an important factor in reducing the transmission of viral hepatitis, HIV, and other infections, these programs are not always offered or face regulatory restrictions in many areas.[CDC.Syringe Services Programs.2024]
HIV Surveillance and Reporting
Monitoring, surveillance, and reporting are essential for improving access to quality services, responding to outbreaks, and determining progress toward HIV prevention objectives across diverse populations, as outlined in the US EHE initiative and the WHO’s 95-95-95 goals. In collaboration with local or state public health authorities, clinicians can contribute to these efforts by fully completing required reporting forms and participating in efforts to streamline and improve surveillance. The WHO, national and state disease control and prevention centers (eg, the CDC) are primary data sources for monitoring HIV trends and progress toward goals.
HIV Research and Innovation
Research and innovation are essential to enhancing the effectiveness of HIV prevention measures. These range from improved diagnostics to more swiftly and accurately detecting HIV to implementation research to determine, for example, who best delivers an intervention, or where an intervention should be delivered, or how best testing and treatment can be linked in a specific population. WHO priorities for HIV research include the expansion of antiretroviral drug-based prevention options such as woman-controlled technologies, long-acting antiretrovirals, subcutaneous implants, the development of biologicals such as broadly neutralizing antibodies for HIV prevention, and multipurpose tools that could prevent pregnancy, STIs, and HIV in 1 device.[WHO.Global HIV, Hepatitis, and STI Health Strategies.2022]
A successful vaccine has been elusive, but one study that used a broadly neutralizing monoclonal antibody for HIV prevention has raised the possibility of eventual success.[54] Understanding the genetic basis for HIV acquisition has resulted in a novel but complex avenue to cure HIV in a handful of patients. The first such cure was reported in 2008 in an individual with HIV-1 who underwent allogeneic hematopoietic stem cell transplantation for acute myeloid leukemia using cells from a donor with a homozygous mutation in the HIV coreceptor CCR5 (CCR5Δ32/Δ32) and subsequently maintained HIV remission without the need for antiretroviral therapy.[55] Most of the subsequent transplant recipients who were cured of HIV also received stem-cell transplants from donors with a double CCR5Δ32 mutation, but some had donors with only 1 or no copies of the mutation, leading researchers to wonder precisely why these patients were cured of HIV and others were not.
Enhancing Healthcare Team Outcomes
HIV remains a leading public health challenge despite advances that transformed it into a manageable chronic disease with antiretroviral therapy. Globally, more than 40 million people live with HIV, with 1.3 million new infections and over 600,000 AIDS-related deaths annually. In the US, an estimated 1.2 million people are living with HIV, yet 13% remain undiagnosed, fueling ongoing transmission. Biomedical prevention strategies, including PrEP, PEP, and TasP, offer highly effective means to reduce new infections; however, gaps in implementation and retention in care hinder progress toward UNAIDS’ 95-95-95 targets.
Optimizing patient-centered HIV prevention and care requires coordinated interprofessional collaboration to support individuals with HIV or at high risk of HIV and to ensure factors within organizational, community, and policy environments support the prevention of HIV. Physicians, general practitioners, and advanced practitioners must screen at-risk individuals, initiate ART promptly, and integrate PrEP and PEP into care. Nurses support adherence, provide education, and monitor treatment outcomes, while pharmacists ensure safe medication use and reinforce adherence strategies. Effective communication across the care team and with patients helps address inequities, reduce stigma, and promote engagement in care. Coordinated strategies that emphasize prevention, early diagnosis, and long-term retention improve patient safety, health outcomes, and overall team performance in combating HIV.
Media
(Click Image to Enlarge)
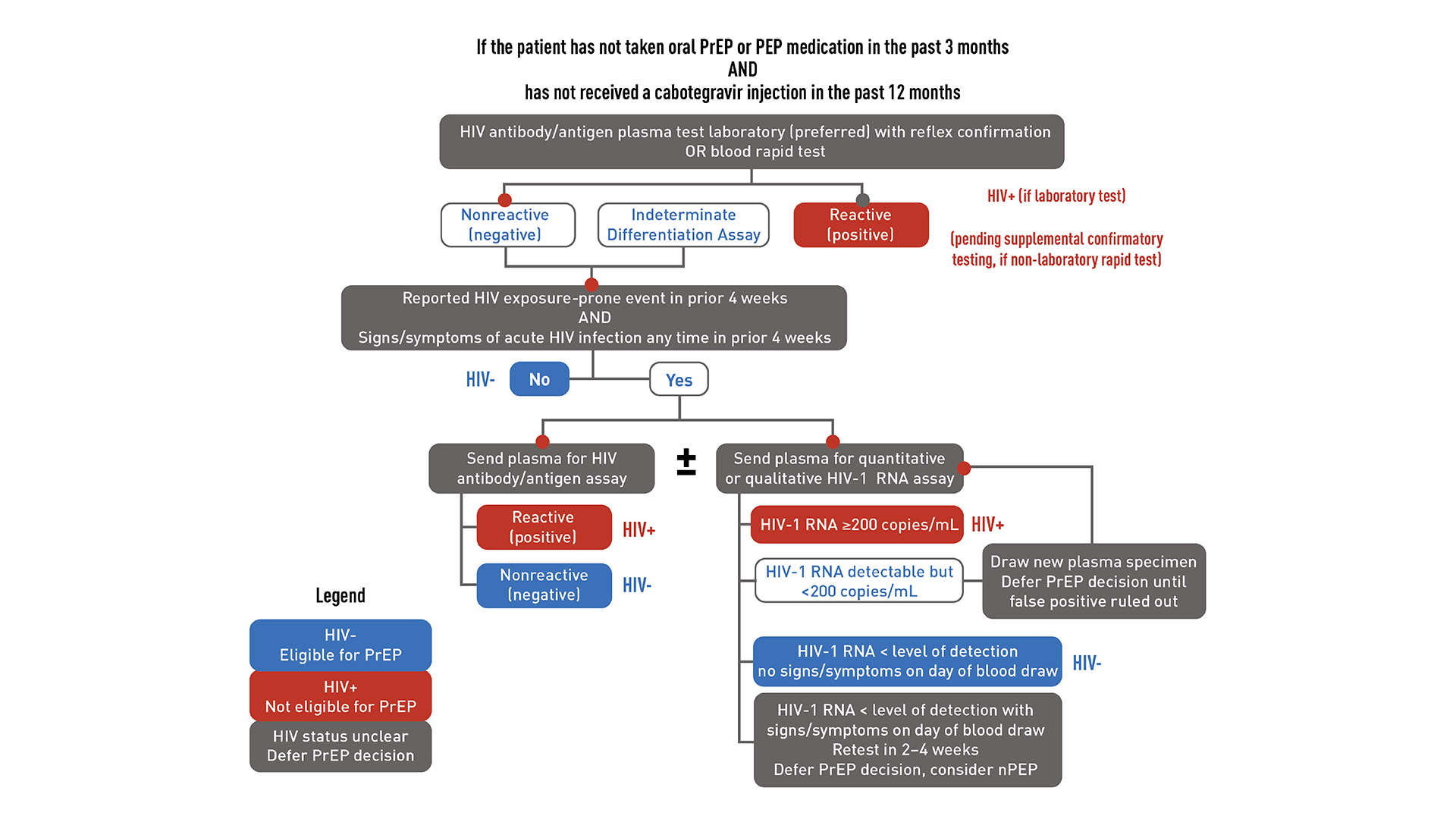
HIV Testing and PrEP Discontinuation. This image demonstrates HIV testing recommended for patients starting or restarting PrEP after a long stop.
Centers for Disease Control and Prevention
(Click Image to Enlarge)
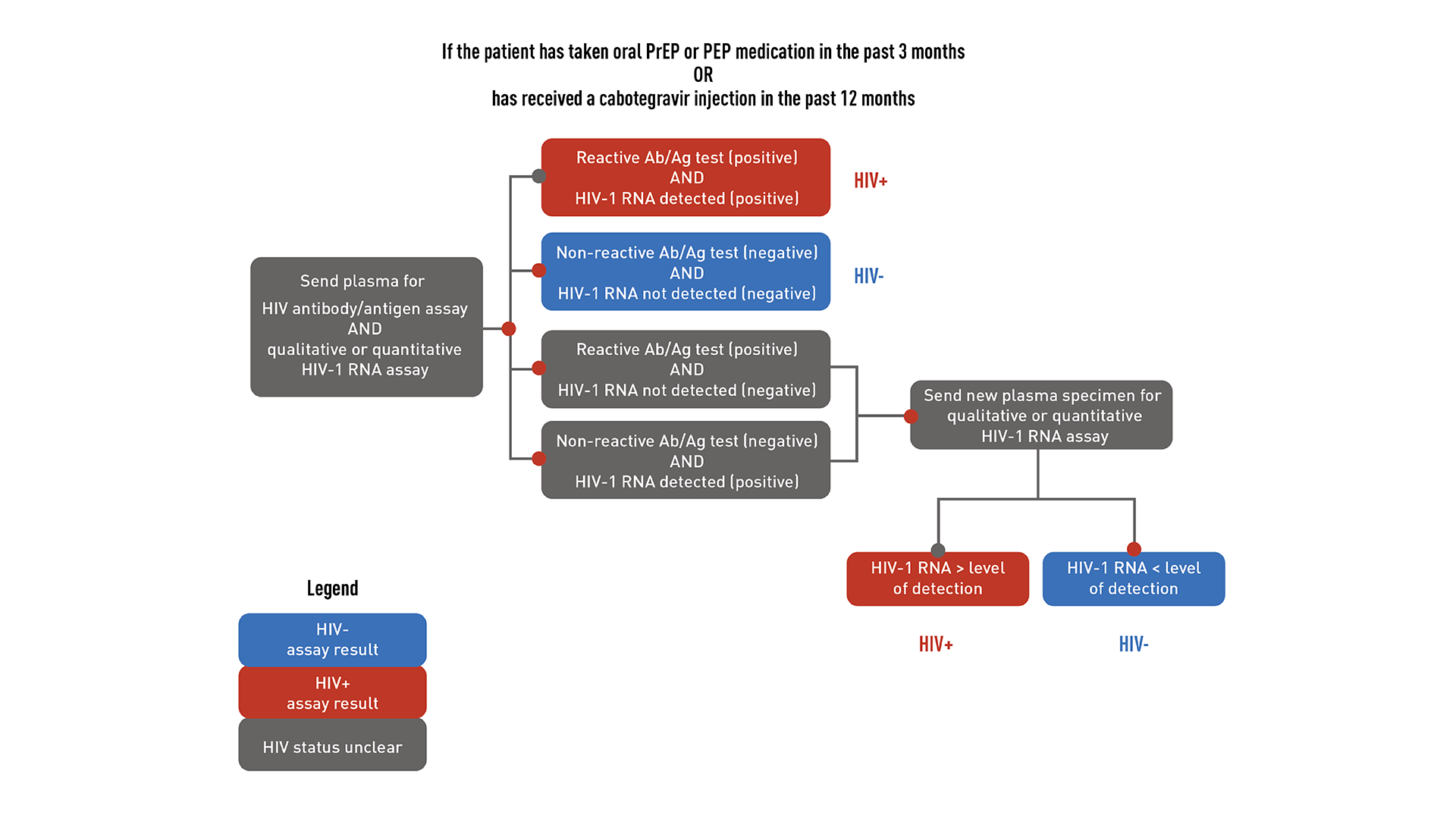
HIV testing for patients who are taking or have recently taken PrEP.
Centers for Disease Control and Prevention
References
Chou R, Spencer H, Bougatsos C, Blazina I, Ahmed A, Selph S. Preexposure Prophylaxis for the Prevention of HIV: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2023 Aug 22:330(8):746-763. doi: 10.1001/jama.2023.9865. Epub [PubMed PMID: 37606667]
Level 1 (high-level) evidenceSkarbinski J, Rosenberg E, Paz-Bailey G, Hall HI, Rose CE, Viall AH, Fagan JL, Lansky A, Mermin JH. Human immunodeficiency virus transmission at each step of the care continuum in the United States. JAMA internal medicine. 2015 Apr:175(4):588-96. doi: 10.1001/jamainternmed.2014.8180. Epub [PubMed PMID: 25706928]
Beyrer C, Ratevosian J, Gelderblom H, Rosenberg NE. The HIV/AIDS pandemic: where are we now? AIDS (London, England). 2025 Sep 1:39(11):1497-1504. doi: 10.1097/QAD.0000000000004308. Epub 2025 Jul 31 [PubMed PMID: 40755211]
Quinn TC, Wawer MJ, Sewankambo N, Serwadda D, Li C, Wabwire-Mangen F, Meehan MO, Lutalo T, Gray RH. Viral load and heterosexual transmission of human immunodeficiency virus type 1. Rakai Project Study Group. The New England journal of medicine. 2000 Mar 30:342(13):921-9 [PubMed PMID: 10738050]
Powers KA, Poole C, Pettifor AE, Cohen MS. Rethinking the heterosexual infectivity of HIV-1: a systematic review and meta-analysis. The Lancet. Infectious diseases. 2008 Sep:8(9):553-63. doi: 10.1016/S1473-3099(08)70156-7. Epub 2008 Aug 4 [PubMed PMID: 18684670]
Level 1 (high-level) evidencePilcher CD, Joaki G, Hoffman IF, Martinson FE, Mapanje C, Stewart PW, Powers KA, Galvin S, Chilongozi D, Gama S, Price MA, Fiscus SA, Cohen MS. Amplified transmission of HIV-1: comparison of HIV-1 concentrations in semen and blood during acute and chronic infection. AIDS (London, England). 2007 Aug 20:21(13):1723-30 [PubMed PMID: 17690570]
Level 2 (mid-level) evidenceCohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, Hakim JG, Kumwenda J, Grinsztejn B, Pilotto JH, Godbole SV, Chariyalertsak S, Santos BR, Mayer KH, Hoffman IF, Eshleman SH, Piwowar-Manning E, Cottle L, Zhang XC, Makhema J, Mills LA, Panchia R, Faesen S, Eron J, Gallant J, Havlir D, Swindells S, Elharrar V, Burns D, Taha TE, Nielsen-Saines K, Celentano DD, Essex M, Hudelson SE, Redd AD, Fleming TR, HPTN 052 Study Team. Antiretroviral Therapy for the Prevention of HIV-1 Transmission. The New England journal of medicine. 2016 Sep 1:375(9):830-9. doi: 10.1056/NEJMoa1600693. Epub 2016 Jul 18 [PubMed PMID: 27424812]
Level 3 (low-level) evidencePatel P, Borkowf CB, Brooks JT, Lasry A, Lansky A, Mermin J. Estimating per-act HIV transmission risk: a systematic review. AIDS (London, England). 2014 Jun 19:28(10):1509-19. doi: 10.1097/QAD.0000000000000298. Epub [PubMed PMID: 24809629]
Level 1 (high-level) evidenceSheth PM, Kovacs C, Kemal KS, Jones RB, Raboud JM, Pilon R, la Porte C, Ostrowski M, Loutfy M, Burger H, Weiser B, Kaul R, Toronto Mucosal Immunology Group. Persistent HIV RNA shedding in semen despite effective antiretroviral therapy. AIDS (London, England). 2009 Sep 24:23(15):2050-4. doi: 10.1097/QAD.0b013e3283303e04. Epub [PubMed PMID: 19710596]
Politch JA, Mayer KH, Welles SL, O'Brien WX, Xu C, Bowman FP, Anderson DJ. Highly active antiretroviral therapy does not completely suppress HIV in semen of sexually active HIV-infected men who have sex with men. AIDS (London, England). 2012 Jul 31:26(12):1535-43. doi: 10.1097/QAD.0b013e328353b11b. Epub [PubMed PMID: 22441253]
Level 2 (mid-level) evidenceDonoval BA, Landay AL, Moses S, Agot K, Ndinya-Achola JO, Nyagaya EA, MacLean I, Bailey RC. HIV-1 target cells in foreskins of African men with varying histories of sexually transmitted infections. American journal of clinical pathology. 2006 Mar:125(3):386-91 [PubMed PMID: 16613341]
Level 1 (high-level) evidenceReynolds SJ, Risbud AR, Shepherd ME, Rompalo AM, Ghate MV, Godbole SV, Joshi SN, Divekar AD, Gangakhedkar RR, Bollinger RC, Mehendale SM. High rates of syphilis among STI patients are contributing to the spread of HIV-1 in India. Sexually transmitted infections. 2006 Apr:82(2):121-6 [PubMed PMID: 16581736]
Weller S, Davis K. Condom effectiveness in reducing heterosexual HIV transmission. The Cochrane database of systematic reviews. 2002:(1):CD003255 [PubMed PMID: 11869658]
Level 2 (mid-level) evidenceGiannou FK, Tsiara CG, Nikolopoulos GK, Talias M, Benetou V, Kantzanou M, Bonovas S, Hatzakis A. Condom effectiveness in reducing heterosexual HIV transmission: a systematic review and meta-analysis of studies on HIV serodiscordant couples. Expert review of pharmacoeconomics & outcomes research. 2016 Aug:16(4):489-99. doi: 10.1586/14737167.2016.1102635. Epub 2015 Oct 21 [PubMed PMID: 26488070]
Level 1 (high-level) evidenceLubinski C, Aberg J, Bardeguez AD, Elion R, Emmanuel P, Kuritzkes D, Saag M, Squires KE, Weddle A, Rainey J, Zerehi MR, Ralston JF, Fleming DA, Bronson D, Cooke M, Cutler C, Ejnes Y, Gluckman R, Liebow M, Musana K, Mayer ME, Purtle MW, Reynolds PP, Viswanathan L, Weiss KB, Yehia B. HIV policy: the path forward--a joint position paper of the HIV Medicine Association of the Infectious Diseases Society of America and the American College of Physicians. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2009 May 15:48(10):1335-44 [PubMed PMID: 19385087]
Auvert B, Taljaard D, Lagarde E, Sobngwi-Tambekou J, Sitta R, Puren A. Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: the ANRS 1265 Trial. PLoS medicine. 2005 Nov:2(11):e298 [PubMed PMID: 16231970]
Level 1 (high-level) evidenceBailey RC, Moses S, Parker CB, Agot K, Maclean I, Krieger JN, Williams CF, Campbell RT, Ndinya-Achola JO. Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. Lancet (London, England). 2007 Feb 24:369(9562):643-56 [PubMed PMID: 17321310]
Level 1 (high-level) evidenceBaggaley RF, Boily MC, White RG, Alary M. Risk of HIV-1 transmission for parenteral exposure and blood transfusion: a systematic review and meta-analysis. AIDS (London, England). 2006 Apr 4:20(6):805-12 [PubMed PMID: 16549963]
Level 1 (high-level) evidencePépin J, Abou Chakra CN, Pépin E, Nault V, Valiquette L. Evolution of the global burden of viral infections from unsafe medical injections, 2000-2010. PloS one. 2014:9(6):e99677. doi: 10.1371/journal.pone.0099677. Epub 2014 Jun 9 [PubMed PMID: 24911341]
Teasdale CA, Marais BJ, Abrams EJ. HIV: prevention of mother-to-child transmission. BMJ clinical evidence. 2011 Jan 17:2011():. pii: 0909. Epub 2011 Jan 17 [PubMed PMID: 21477392]
Luzuriaga K, Mofenson LM. Eliminating Pediatric HIV-1 Infection. The New England journal of medicine. 2016 Jul 14:375(2):193-4. doi: 10.1056/NEJMc1604016. Epub [PubMed PMID: 27410941]
Mayer KH. Introduction: Linkage, engagement, and retention in HIV care: essential for optimal individual- and community-level outcomes in the era of highly active antiretroviral therapy. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2011 Jan 15:52 Suppl 2():S205-7. doi: 10.1093/cid/ciq043. Epub [PubMed PMID: 21342908]
Horberg M, Thompson M, Agwu A, Colasanti J, Haddad M, Jain M, McComsey G, Radix A, Rakhmanina N, Short WR, Singh T, Tookes H. Primary Care Guidance for Providers of Care for Persons With Human Immunodeficiency Virus: 2024 Update by the HIV Medicine Association of the Infectious Diseases Society of America. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2024 Oct 12:():. pii: ciae479. doi: 10.1093/cid/ciae479. Epub 2024 Oct 12 [PubMed PMID: 39393187]
Sigaloff KC, Lange JM, Montaner J. Global response to HIV: treatment as prevention, or treatment for treatment? Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2014 Jul:59 Suppl 1(Suppl 1):S7-S11. doi: 10.1093/cid/ciu267. Epub [PubMed PMID: 24926037]
Eisinger RW, Dieffenbach CW, Fauci AS. HIV Viral Load and Transmissibility of HIV Infection: Undetectable Equals Untransmittable. JAMA. 2019 Feb 5:321(5):451-452. doi: 10.1001/jama.2018.21167. Epub [PubMed PMID: 30629090]
Rodger AJ, Cambiano V, Bruun T, Vernazza P, Collins S, van Lunzen J, Corbelli GM, Estrada V, Geretti AM, Beloukas A, Asboe D, Viciana P, Gutiérrez F, Clotet B, Pradier C, Gerstoft J, Weber R, Westling K, Wandeler G, Prins JM, Rieger A, Stoeckle M, Kümmerle T, Bini T, Ammassari A, Gilson R, Krznaric I, Ristola M, Zangerle R, Handberg P, Antela A, Allan S, Phillips AN, Lundgren J, PARTNER Study Group. Sexual Activity Without Condoms and Risk of HIV Transmission in Serodifferent Couples When the HIV-Positive Partner Is Using Suppressive Antiretroviral Therapy. JAMA. 2016 Jul 12:316(2):171-81. doi: 10.1001/jama.2016.5148. Epub [PubMed PMID: 27404185]
Rodger AJ, Cambiano V, Bruun T, Vernazza P, Collins S, Degen O, Corbelli GM, Estrada V, Geretti AM, Beloukas A, Raben D, Coll P, Antinori A, Nwokolo N, Rieger A, Prins JM, Blaxhult A, Weber R, Van Eeden A, Brockmeyer NH, Clarke A, Del Romero Guerrero J, Raffi F, Bogner JR, Wandeler G, Gerstoft J, Gutiérrez F, Brinkman K, Kitchen M, Ostergaard L, Leon A, Ristola M, Jessen H, Stellbrink HJ, Phillips AN, Lundgren J, PARTNER Study Group. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): final results of a multicentre, prospective, observational study. Lancet (London, England). 2019 Jun 15:393(10189):2428-2438. doi: 10.1016/S0140-6736(19)30418-0. Epub 2019 May 2 [PubMed PMID: 31056293]
Level 2 (mid-level) evidenceBor J, Fischer C, Modi M, Richman B, Kinker C, King R, Calabrese SK, Mokhele I, Sineke T, Zuma T, Rosen S, Bärnighausen T, Mayer KH, Onoya D. Changing Knowledge and Attitudes Towards HIV Treatment-as-Prevention and "Undetectable = Untransmittable": A Systematic Review. AIDS and behavior. 2021 Dec:25(12):4209-4224. doi: 10.1007/s10461-021-03296-8. Epub 2021 May 25 [PubMed PMID: 34036459]
Level 1 (high-level) evidenceBorsa A, Siegel K. Navigating the Viral Divide: Sexual and Gender Minority Community Perspectives on Treatment as Prevention. AIDS education and prevention : official publication of the International Society for AIDS Education. 2023 Oct:35(5):406-419. doi: 10.1521/aeap.2023.35.5.406. Epub [PubMed PMID: 37843907]
Level 3 (low-level) evidenceHavlir D, Lockman S, Ayles H, Larmarange J, Chamie G, Gaolathe T, Iwuji C, Fidler S, Kamya M, Floyd S, Moore J, Hayes R, Petersen M, Dabis F, (Universal Test, Treat Trials) UT3 Consortium. What do the Universal Test and Treat trials tell us about the path to HIV epidemic control? Journal of the International AIDS Society. 2020 Feb:23(2):e25455. doi: 10.1002/jia2.25455. Epub [PubMed PMID: 32091179]
O Murchu E, Marshall L, Teljeur C, Harrington P, Hayes C, Moran P, Ryan M. Oral pre-exposure prophylaxis (PrEP) to prevent HIV: a systematic review and meta-analysis of clinical effectiveness, safety, adherence and risk compensation in all populations. BMJ open. 2022 May 11:12(5):e048478. doi: 10.1136/bmjopen-2020-048478. Epub 2022 May 11 [PubMed PMID: 35545381]
Level 1 (high-level) evidenceDelany-Moretlwe S, Hughes JP, Bock P, Ouma SG, Hunidzarira P, Kalonji D, Kayange N, Makhema J, Mandima P, Mathew C, Spooner E, Mpendo J, Mukwekwerere P, Mgodi N, Ntege PN, Nair G, Nakabiito C, Nuwagaba-Biribonwoha H, Panchia R, Singh N, Siziba B, Farrior J, Rose S, Anderson PL, Eshleman SH, Marzinke MA, Hendrix CW, Beigel-Orme S, Hosek S, Tolley E, Sista N, Adeyeye A, Rooney JF, Rinehart A, Spreen WR, Smith K, Hanscom B, Cohen MS, Hosseinipour MC, HPTN 084 study group. Cabotegravir for the prevention of HIV-1 in women: results from HPTN 084, a phase 3, randomised clinical trial. Lancet (London, England). 2022 May 7:399(10337):1779-1789. doi: 10.1016/S0140-6736(22)00538-4. Epub 2022 Apr 1 [PubMed PMID: 35378077]
Level 1 (high-level) evidenceLandovitz RJ, Donnell D, Clement ME, Hanscom B, Cottle L, Coelho L, Cabello R, Chariyalertsak S, Dunne EF, Frank I, Gallardo-Cartagena JA, Gaur AH, Gonzales P, Tran HV, Hinojosa JC, Kallas EG, Kelley CF, Losso MH, Madruga JV, Middelkoop K, Phanuphak N, Santos B, Sued O, Valencia Huamaní J, Overton ET, Swaminathan S, Del Rio C, Gulick RM, Richardson P, Sullivan P, Piwowar-Manning E, Marzinke M, Hendrix C, Li M, Wang Z, Marrazzo J, Daar E, Asmelash A, Brown TT, Anderson P, Eshleman SH, Bryan M, Blanchette C, Lucas J, Psaros C, Safren S, Sugarman J, Scott H, Eron JJ, Fields SD, Sista ND, Gomez-Feliciano K, Jennings A, Kofron RM, Holtz TH, Shin K, Rooney JF, Smith KY, Spreen W, Margolis D, Rinehart A, Adeyeye A, Cohen MS, McCauley M, Grinsztejn B, HPTN 083 Study Team. Cabotegravir for HIV Prevention in Cisgender Men and Transgender Women. The New England journal of medicine. 2021 Aug 12:385(7):595-608. doi: 10.1056/NEJMoa2101016. Epub [PubMed PMID: 34379922]
Kelley CF, Acevedo-Quiñones M, Agwu AL, Avihingsanon A, Benson P, Blumenthal J, Brinson C, Brites C, Cahn P, Cantos VD, Clark J, Clement M, Creticos C, Crofoot G, Diaz RS, Doblecki-Lewis S, Gallardo-Cartagena JA, Gaur A, Grinsztejn B, Hassler S, Hinojosa JC, Hodge T, Kaplan R, Lacerda M, LaMarca A, Losso MH, Valdez Madruga J, Mayer KH, Mills A, Mounzer K, Ndlovu N, Novak RM, Perez Rios A, Phanuphak N, Ramgopal M, Ruane PJ, Sánchez J, Santos B, Schine P, Schreibman T, Spencer LY, Van Gerwen OT, Vasconcelos R, Vasquez JG, Zwane Z, Cox S, Deaton C, Ebrahimi R, Wong P, Singh R, Brown LB, Carter CC, Das M, Baeten JM, Ogbuagu O, PURPOSE 2 Study Team. Twice-Yearly Lenacapavir for HIV Prevention in Men and Gender-Diverse Persons. The New England journal of medicine. 2025 Apr 3:392(13):1261-1276. doi: 10.1056/NEJMoa2411858. Epub 2024 Nov 27 [PubMed PMID: 39602624]
Bekker LG, Das M, Abdool Karim Q, Ahmed K, Batting J, Brumskine W, Gill K, Harkoo I, Jaggernath M, Kigozi G, Kiwanuka N, Kotze P, Lebina L, Louw CE, Malahleha M, Manentsa M, Mansoor LE, Moodley D, Naicker V, Naidoo L, Naidoo M, Nair G, Ndlovu N, Palanee-Phillips T, Panchia R, Pillay S, Potloane D, Selepe P, Singh N, Singh Y, Spooner E, Ward AM, Zwane Z, Ebrahimi R, Zhao Y, Kintu A, Deaton C, Carter CC, Baeten JM, Matovu Kiweewa F, PURPOSE 1 Study Team. Twice-Yearly Lenacapavir or Daily F/TAF for HIV Prevention in Cisgender Women. The New England journal of medicine. 2024 Oct 3:391(13):1179-1192. doi: 10.1056/NEJMoa2407001. Epub 2024 Jul 24 [PubMed PMID: 39046157]
Smith DK, Herbst JH, Zhang X, Rose CE. Condom effectiveness for HIV prevention by consistency of use among men who have sex with men in the United States. Journal of acquired immune deficiency syndromes (1999). 2015 Mar 1:68(3):337-44. doi: 10.1097/QAI.0000000000000461. Epub [PubMed PMID: 25469526]
Johnson WD, O'Leary A, Flores SA. Per-partner condom effectiveness against HIV for men who have sex with men. AIDS (London, England). 2018 Jul 17:32(11):1499-1505. doi: 10.1097/QAD.0000000000001832. Epub [PubMed PMID: 29794493]
Siegfried N, Muller M, Deeks JJ, Volmink J. Male circumcision for prevention of heterosexual acquisition of HIV in men. The Cochrane database of systematic reviews. 2009 Apr 15:2009(2):CD003362. doi: 10.1002/14651858.CD003362.pub2. Epub 2009 Apr 15 [PubMed PMID: 19370585]
Level 1 (high-level) evidenceBavinton BR, Pinto AN, Phanuphak N, Grinsztejn B, Prestage GP, Zablotska-Manos IB, Jin F, Fairley CK, Moore R, Roth N, Bloch M, Pell C, McNulty AM, Baker D, Hoy J, Tee BK, Templeton DJ, Cooper DA, Emery S, Kelleher A, Grulich AE, Opposites Attract Study Group. Viral suppression and HIV transmission in serodiscordant male couples: an international, prospective, observational, cohort study. The lancet. HIV. 2018 Aug:5(8):e438-e447. doi: 10.1016/S2352-3018(18)30132-2. Epub 2018 Jul 17 [PubMed PMID: 30025681]
Stalter RM, Dong TQ, Hendrix CW, Palanee-Phillips T, van der Straten A, Hillier SL, Kiweewa FM, Mgodi NM, Marzinke MA, Bekker LG, Soto-Torres L, Baeten JM, Brown ER, MTN-020/ASPIRE Study Team. Assessing Per-Sex-Act HIV-1 Risk Reduction Among Women Using the Dapivirine Vaginal Ring. The Journal of infectious diseases. 2024 Apr 12:229(4):1158-1165. doi: 10.1093/infdis/jiad550. Epub [PubMed PMID: 38099506]
Bradley H, Hall EW, Asher A, Furukawa NW, Jones CM, Shealey J, Buchacz K, Handanagic S, Crepaz N, Rosenberg ES. Estimated Number of People Who Inject Drugs in the United States. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2023 Jan 6:76(1):96-102. doi: 10.1093/cid/ciac543. Epub [PubMed PMID: 35791261]
Strathdee SA, Kuo I, El-Bassel N, Hodder S, Smith LR, Springer SA. Preventing HIV outbreaks among people who inject drugs in the United States: plus ça change, plus ça même chose. AIDS (London, England). 2020 Nov 15:34(14):1997-2005. doi: 10.1097/QAD.0000000000002673. Epub [PubMed PMID: 32826391]
Mistler CB, Copenhaver MM, Shrestha R. The Pre-exposure Prophylaxis (PrEP) Care Cascade in People Who Inject Drugs: A Systematic Review. AIDS and behavior. 2021 May:25(5):1490-1506. doi: 10.1007/s10461-020-02988-x. Epub [PubMed PMID: 32749627]
Level 1 (high-level) evidenceHall HI, Brooks JT, Mermin J. Can the United States achieve 90-90-90? Current opinion in HIV and AIDS. 2019 Nov:14(6):464-470. doi: 10.1097/COH.0000000000000578. Epub [PubMed PMID: 31425180]
Level 3 (low-level) evidenceFrescura L, Godfrey-Faussett P, Feizzadeh A A, El-Sadr W, Syarif O, Ghys PD, on and behalf of the 2025 testing treatment target Working Group. Achieving the 95 95 95 targets for all: A pathway to ending AIDS. PloS one. 2022:17(8):e0272405. doi: 10.1371/journal.pone.0272405. Epub 2022 Aug 4 [PubMed PMID: 35925943]
Gandhi RT, Bedimo R, Hoy JF, Landovitz RJ, Smith DM, Eaton EF, Lehmann C, Springer SA, Sax PE, Thompson MA, Benson CA, Buchbinder SP, Del Rio C, Eron JJ Jr, Günthard HF, Molina JM, Jacobsen DM, Saag MS. Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2022 Recommendations of the International Antiviral Society-USA Panel. JAMA. 2023 Jan 3:329(1):63-84. doi: 10.1001/jama.2022.22246. Epub [PubMed PMID: 36454551]
Katz DA, Golden MR, Hughes JP, Farquhar C, Stekler JD. HIV Self-Testing Increases HIV Testing Frequency in High-Risk Men Who Have Sex With Men: A Randomized Controlled Trial. Journal of acquired immune deficiency syndromes (1999). 2018 Aug 15:78(5):505-512. doi: 10.1097/QAI.0000000000001709. Epub [PubMed PMID: 29697595]
Level 1 (high-level) evidenceRendina HJ, Talan AJ, Cienfuegos-Szalay J, Carter JA, Shalhav O. Treatment Is More Than Prevention: Perceived Personal and Social Benefits of Undetectable = Untransmittable Messaging Among Sexual Minority Men Living with HIV. AIDS patient care and STDs. 2020 Oct:34(10):444-451. doi: 10.1089/apc.2020.0137. Epub [PubMed PMID: 33064015]
Okamoto EE, Anam FR, Batiste S, Dukashe M, Castellanos E, Poonkasetwattana M, Richman B. Ending AIDS as a public health threat: the imperative for clear messaging on U=U, viral suppression, and zero risk. The lancet. HIV. 2024 Nov:11(11):e783-e790. doi: 10.1016/S2352-3018(24)00241-8. Epub [PubMed PMID: 39477558]
Tanner MR, Iqbal K, Dominguez KL, Zhu W, Obi J, Hoover KW. Key Factors for Successful Implementation of HIV Prevention Services by THRIVE Community Collaboratives. Public health reports (Washington, D.C. : 1974). 2022 Mar-Apr:137(2):310-316. doi: 10.1177/00333549211005793. Epub 2021 Mar 25 [PubMed PMID: 33765400]
Iskarpatyoti BS, Lebov J, Hart L, Thomas J, Mandal M. Evaluations of Structural Interventions for HIV Prevention: A Review of Approaches and Methods. AIDS and behavior. 2018 Apr:22(4):1253-1264. doi: 10.1007/s10461-017-1997-x. Epub [PubMed PMID: 29273945]
Stone J, Artenie A, Hickman M, Martin NK, Degenhardt L, Fraser H, Vickerman P. The contribution of unstable housing to HIV and hepatitis C virus transmission among people who inject drugs globally, regionally, and at country level: a modelling study. The Lancet. Public health. 2022 Feb:7(2):e136-e145. doi: 10.1016/S2468-2667(21)00258-9. Epub 2022 Jan 7 [PubMed PMID: 35012711]
Low AJ, Mburu G, Welton NJ, May MT, Davies CF, French C, Turner KM, Looker KJ, Christensen H, McLean S, Rhodes T, Platt L, Hickman M, Guise A, Vickerman P. Impact of Opioid Substitution Therapy on Antiretroviral Therapy Outcomes: A Systematic Review and Meta-Analysis. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2016 Oct 15:63(8):1094-1104. doi: 10.1093/cid/ciw416. Epub 2016 Jun 25 [PubMed PMID: 27343545]
Level 1 (high-level) evidenceCorey L, Gilbert PB, Juraska M, Montefiori DC, Morris L, Karuna ST, Edupuganti S, Mgodi NM, deCamp AC, Rudnicki E, Huang Y, Gonzales P, Cabello R, Orrell C, Lama JR, Laher F, Lazarus EM, Sanchez J, Frank I, Hinojosa J, Sobieszczyk ME, Marshall KE, Mukwekwerere PG, Makhema J, Baden LR, Mullins JI, Williamson C, Hural J, McElrath MJ, Bentley C, Takuva S, Gomez Lorenzo MM, Burns DN, Espy N, Randhawa AK, Kochar N, Piwowar-Manning E, Donnell DJ, Sista N, Andrew P, Kublin JG, Gray G, Ledgerwood JE, Mascola JR, Cohen MS, HVTN 704/HPTN 085 and HVTN 703/HPTN 081 Study Teams. Two Randomized Trials of Neutralizing Antibodies to Prevent HIV-1 Acquisition. The New England journal of medicine. 2021 Mar 18:384(11):1003-1014. doi: 10.1056/NEJMoa2031738. Epub [PubMed PMID: 33730454]
Level 1 (high-level) evidenceHütter G, Nowak D, Mossner M, Ganepola S, Müssig A, Allers K, Schneider T, Hofmann J, Kücherer C, Blau O, Blau IW, Hofmann WK, Thiel E. Long-term control of HIV by CCR5 Delta32/Delta32 stem-cell transplantation. The New England journal of medicine. 2009 Feb 12:360(7):692-8. doi: 10.1056/NEJMoa0802905. Epub [PubMed PMID: 19213682]