Introduction
A hiatal hernia is a condition characterized by the abnormal protrusion of the upper part of the stomach or other abdominal organs through the diaphragm's esophageal hiatus. Study results suggest that 50% to 94% of patients with gastroesophageal reflux disease (GERD) have a sliding hiatal hernia (see Image. Hiatal Hernia on Fluoroscopy).[1] The diaphragm is a voluntary or striated muscle that separates the thoracic and abdominal cavities and serves as the primary muscle of respiration; there are separate openings for the inferior vena cava, the esophagus, and the aorta, arranged from anterior to posterior. The esophageal diaphragmatic hiatus is clinically relevant in hiatal hernia, as it permits protrusion of the stomach into the thoracic cavity. Hiatal hernias can produce heartburn, regurgitation, dysphagia, chest pain, and shortness of breath. The condition occurs more frequently in adults than in children and, rarely, results in life-threatening complications, such as incarceration of herniated contents or bleeding from Cameron ulcers.
The region where the esophagus joins the stomach is known as the gastroesophageal junction (GEJ). The lower esophageal sphincter (LES) is a physiologic high-pressure zone located immediately distal to the GEJ that functions as a barrier to reflux. Normally, approximately 2 cm of the distal esophagus resides below the diaphragm. In a hiatal hernia, the stomach protrudes through the esophageal hiatus into the thoracic cavity, displacing the LES. Laxity of the LES permits gastric contents and acid to reflux into the esophagus, resulting in GERD. Small hiatal hernias are frequently asymptomatic and are generally managed with medical therapy. Larger paraesophageal hiatal hernias usually require surgical intervention (see Image. Massive Hiatal Hernia).[2][3]
Hiatal hernias are classified into 4 types. The categories are described as follows:
- Type I: Sliding hiatal hernia, representing more than 95% of cases. The gastric fundus or cardia protrudes into the mediastinum along with the GEJ (see Images. Type I Hiatal Hernia and Sliding Hiatal Hernia on Barium Study).
- Type II: Paraesophageal hiatal hernia, where the fundus is displaced into the mediastinum while the GEJ remains below the esophageal hiatus. This type is the rarest of hiatal hernias.
- Type III: Mixed paraesophageal and sliding hernia, with both the GEJ and a variable portion of the stomach extending into the mediastinum (see Image. Radiographic Appearance of a Mixed Paraesophageal Hernia).
- Type IV: Herniation of the stomach along with an additional abdominal organ, such as the colon, small intestine, or spleen, into the thoracic cavity.[4][5]
Type I is referred to as a "sliding hiatal hernia," whereas types II to IV are classified as paraesophageal hernias (PEHs). All hiatal hernias are typically repaired surgically using various procedures, frequently combined with fundoplication of the stomach.[6][7]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Hiatal hernias can be congenital but are more frequently acquired. Prevalence increases with age, as older individuals may develop large hiatal hernias or PEHs. Age-related loss of muscular flexibility and connective tissue elasticity is a predisposing factor for hiatal hernia formation. A shortened esophagus, whether congenital or secondary to esophagitis, may tether the stomach and promote herniation. Weakness of the phrenoesophageal connective tissue represents another etiology, predisposing to PEH formation. A combined PEH and sliding hernia may develop when tissue laxity at the hiatus coexists with this weakness.[8]
Epidemiology
The prevalence of hiatal hernia increases with age. Approximately 55% to 60% of individuals older than 50 years have a hiatal hernia, and adults older than 70 are more likely to present with large hiatal hernias.[9] Despite this prevalence, only about 10% of patients or fewer develop symptoms. The vast majority, approximately 90%, of hiatal hernias are type I sliding hernias, whereas type II PEHs account for less than 5% of all hiatal hernias.[10]
Pathophysiology
Acquired hiatal hernias are associated with increased intra-abdominal pressure, typically arising from obesity, pregnancy, chronic constipation, and chronic obstructive pulmonary disease. Prevalence is higher in women, potentially due to elevated intra-abdominal pressure during pregnancy. Hiatal hernias are most common in Western Europe and North America and are rare in rural Africa. Certain collagen vascular anomalies have been identified in patients with large hiatal hernias.[Kriley et al, 2023]
Most patients with hiatal hernias present with symptoms of acid reflux resulting from LES incompetence. The antireflux barrier comprises the LES and the hiatal crural diaphragm. In a hiatal hernia, upward and radial displacement of the stomach compromises crural diaphragm function, contributing to reflux.[11] Large hiatal hernias may also produce mechanical symptoms, including dysphagia, shortness of breath, and chest pain. Rarely, complete migration of the stomach into the thoracic cavity results in gastric volvulus. While most gastric volvuli are chronic, some present acutely, with type IV PEH more likely to manifest acute incarceration.[12]
History and Physical
GERD symptoms are a common indication for evaluation of a hiatal hernia. Heartburn and regurgitation represent the typical manifestations of GERD. Although heartburn is the most frequent symptom, some patients present with extraesophageal or atypical symptoms, including chronic cough, hoarseness, or asthma. Regurgitation and extraesophageal manifestations generally indicate disease progression.
However, the presence of symptoms alone is not sufficient for the diagnosis of GERD. Approximately one-third of patients with heartburn exhibit erosive esophagitis on upper endoscopy; another third have nonerosive reflux disease (NERD), characterized by a normal-appearing esophagus with a positive pH test; and the remaining third demonstrates reflux hypersensitivity or functional heartburn. Patients in the latter category respond poorly to both medical and surgical therapy.[13]
Regurgitation refers to the reflux of stomach acid into the upper aerodigestive tract and oral cavity. Severe regurgitation may prevent patients from lying flat, necessitating elevation of the head of the bed. The degree of bed elevation required serves as a simple indicator of regurgitation severity. Some patients experience choking due to aspiration of gastric contents into the airways. Regurgitation must be differentiated from vomiting, which usually arises from gastric or intestinal pathology. When vomiting predominates, the nature of the expelled content—digested or undigested—should be documented. The presence of undigested food may indicate an alternative pathology, such as achalasia or a Zenker diverticulum.
Dysphagia is another common complaint, particularly in patients with large hiatal hernias, which can cause mechanical obstruction. The differential diagnosis is broad and may include peptic esophageal stricture, esophageal carcinoma, epiphrenic or Zenker diverticulum, or esophageal motility disorders such as achalasia. Dyspnea may occur in patients with large hiatal hernias. Study results indicate that preoperative respiratory symptoms are present in 30% to 44% of cases, suggesting that pulmonary complications in patients with hiatal hernia are often underrecognized. Patients with hiatal hernias are frequently older and commonly have comorbid conditions that may contribute to respiratory impairment.[14]
Physical examination rarely confirms the diagnosis of hiatal hernia or GERD. Abnormal supraclavicular lymphadenopathy in patients presenting with heartburn and dysphagia may indicate esophageal or gastric malignancy and constitutes an important component of evaluation.[15][16] Abdominal examination, including assessment of prior surgical incisions, is relevant in patients being considered for operative repair of hiatal hernias. The presence of ventral hernias should be documented, as they may influence the surgical approach.
Evaluation
Preoperative workup in patients being considered for operative treatment confirms the diagnosis, excludes other pathologic entities, and guides the operative plan. Two essential tests are recommended for all patients with a hiatal hernia: a barium esophagram and upper endoscopy (ie, esophagogastroduodenoscopy or EGD). The remainder of the evaluation depends on the size of the hernia. These 2 tests are typically sufficient in patients with a large PEH, and additional studies are reserved for special circumstances.
Large PEHs comprise an anatomic defect that often warrants surgical correction, and objective evidence of GERD is not required prior to surgery. In contrast, patients with small hiatal hernias often need a more comprehensive upper gastrointestinal workup. Establishing a diagnosis of GERD is necessary in these patients to determine appropriate therapy, particularly if surgical intervention is being considered.
The barium esophagram is an effective first-line test because it is noninvasive and provides critical information about the esophagus and hiatal hernia. The esophagram evaluates the esophageal body, whether dilated or nondilated, and can indicate the presence of an esophageal motility disorder. In patients with achalasia, the esophageal body appears dilated with smooth narrowing at the LES. Hypermotility disorders may manifest as tertiary contractions or sawtooth waves. Both findings can occur in the presence of a hiatal hernia.
The LES may be visualized, and its relaxation assessed by observing the opening on cine images. The esophagram also provides an accurate estimate of hiatal hernia size and morphology and is considered the gold standard due to high sensitivity and specificity. Computed tomography of the chest may be used selectively in patients with suspected large or recurrent PEH, but is not routinely required for diagnosis (see Image. Type III Paraesophageal Hernia on Computed Tomography).
Endoscopy is an essential component in the evaluation of GERD and suspected hiatal hernia, particularly in patients being considered for surgical intervention (see Image. Endoscopic View of a Parahiatal Hernia). EGD identifies mucosal abnormalities, including carcinoma, and documents erosive esophagitis. Erosive esophagitis is graded using the Los Angeles (LA) classification, with LA grades B, C, or D considered diagnostic of GERD.[17] EGD is also used to detect Barrett esophagus. The presence of biopsy-proven Barrett esophagus or a peptic stricture constitutes objective evidence of GERD.
For patients with GERD symptoms without objective evidence of disease, a pH test is required to confirm pathologic acid exposure or increased acid exposure in the distal esophagus. The test may be performed using either a wireless probe or a catheter. For the wireless test, a probe is positioned 5 cm above the GEJ to measure acid exposure in the region. A 48-hour pH study conducted off medications is considered the gold standard for diagnosing acid reflux, though studies up to 96 hours may improve detection.[18]
The second approach, the pH impedance test, uses a catheter inserted into the distal esophagus via the nasal cavity. This method is considered more accurate than the wireless test and can detect both acid and nonacid reflux. Two metrics quantify acid reflux. The first, the DeMeester score, incorporates the percentage of time esophageal pH is below 4, the number of reflux episodes, the duration of the longest reflux episode, and the number of episodes lasting longer than 5 minutes. A DeMeester score of 14.7 or greater indicates significant GERD.[19] The second metric, now more commonly used, is acid exposure time. An acid exposure time greater than 6% in a 24-hour study or greater than 48 hours in a wireless study is considered diagnostic of GERD.
High-resolution esophageal manometry is generally recommended prior to surgical intervention.[20] High-resolution esophageal manometry helps exclude primary motility disorders, such as achalasia, which can mimic reflux symptoms through regurgitation. The test also aids in diagnosing hypomotility disorders, including ineffective esophageal motility and aperistalsis, for which patients require a partial fundoplication rather than a 360° Nissen fundoplication.
Hiatal hernia is frequently first identified during EGD performed for GERD symptoms. In addition to confirming a hiatal hernia, EGD assesses the presence and severity of erosive esophagitis. In patients with NERD and a small hiatal hernia, pH testing may be necessary to confirm GERD and exclude reflux hypersensitivity or functional heartburn. Detection of a large hiatal hernia during EGD warrants a barium esophagram to accurately determine hernia size.
Treatment / Management
Managing hiatal hernias depends on hernia type and symptom severity. Initial treatment for patients presenting with typical GERD symptoms, regardless of the presence or absence of a hiatal hernia, in an outpatient setting includes proton pump inhibitors (PPIs). For new-onset GERD symptoms, a once-daily PPI administered in the morning before meals is recommended for 8 weeks. EGD is indicated in cases of recurrent symptoms or incomplete symptom relief. Upon confirmation of objective evidence of GERD, PPI therapy may be increased to twice daily.[21]
Indications for surgical therapy have evolved since the advent of PPIs. Surgery should be considered for patients with a life expectancy greater than 8 years who require lifelong therapy due to a mechanically defective LES.[22][23][24] Antireflux surgery (ARS) is recommended for patients who do not respond to PPI therapy, have severe erosive esophagitis (LA grade C or D), or present with a symptomatic, large PEH.(A1)
Individuals with longstanding symptoms or incomplete resolution while on medical therapy are also candidates for ARS. Some patients elect ARS due to concerns regarding lifelong PPI use. Most procedures are performed electively. However, emergency surgery is occasionally required. PEH, particularly in patients with gastric volvulus, can present with incarceration and acute symptoms, including nausea, vomiting, and chest pain. Immediate decompression of the stomach with a nasogastric tube or EGD is required, followed by urgent or delayed elective repair (see Image. Gastric Volvulus on Contrast Radiography).
Surgical repair of hiatal hernias involves 3 key tenets: obtaining at least 2 cm of relaxed intra-abdominal esophageal length, performing hiatal closure, and undertaking a fundoplication. Implemented concurrently, these steps restore the antireflux barrier. Historically, this restoration was achieved through ARS. However, endoscopic options are now available for patients with GERD and small hiatal hernias.
One such procedure is transoral incisionless fundoplication (TIF). TIF is indicated for patients with mild-to-moderate GERD symptoms, NERD, LA grades A or B esophagitis, or small hiatal hernias less than 2 cm.[25] The procedure creates a full-thickness serosa-serosa plication measuring 3 to 5 cm in length and 200° to 300° in circumference. TIF is considered superior to PPIs but less effective than ARS.(B3)
ARS, performed laparoscopically or robotically, is considered superior to medical or endoscopic therapies. Although techniques vary significantly, the 3 key tenets of ARS are generally observed, with modifications based on individual patient presentation. The key steps of ARS are as follows:
- Division of short gastric vessels
- Division of the gastrohepatic ligament
- Creation of a retroesophageal window and placement of a Penrose drain
- Hiatal dissection, including division of the phrenoesophageal ligament and entry into the mediastinum
- Mobilization of the esophagus and attainment of adequate intra-abdominal esophageal length
- Closure of the hiatal defect
- Construction of the fundoplication
Excision of the hernia sac is recommended in patients with a large PEH. Mesh may be used selectively to reinforce the hiatal closure, although it does not reduce long-term recurrence of hiatal hernias. The key steps of the operation are illustrated in a video atlas available from an external source.[SAGES, 2026]
Several different types of fundoplications have been described. Each is designed to restore the antireflux barrier while accommodating variations in esophageal motility and patient anatomy. The Nissen fundoplication (360° wrap) entails completely encircling the GEJ with the stomach fundus. A bougie 56F to 60F (French gauge) ensures proper approximation without excessive tightness of the wrap. A 2-cm wrap is constructed by anchoring one side of the stomach fundus to the other, incorporating the longitudinal muscle of the esophagus.[26] The procedure has been associated with impaired ability to belch or vomit and with gas bloat.
Historically, partial fundoplication was the procedure of choice when esophageal motility was a concern. Several partial fundoplications have been described, with the most common being the Toupet procedure, which creates a 3-cm posterior (270°) wrap, and the Dor procedure, which establishes an anterior (200°) wrap. Partial fundoplications are associated with fewer adverse effects than the Nissen fundoplication. Results from longitudinal studies demonstrate that both Toupet and Nissen fundoplications provide comparable symptom relief, with fewer adverse effects observed in the Toupet fundoplication. While the Dor fundoplication is occasionally used for GERD, it is more commonly performed in patients undergoing Heller myotomy for achalasia.
Magnetic sphincter augmentation (MSA) provides an alternative to fundoplication. The procedural steps are similar. However, instead of creating a fundoplication, a device composed of magnetized titanium beads is placed around the distal esophagus above the GEJ. The device opens to allow food to pass into the stomach and closes afterward to prevent acid reflux. Results from comparative studies indicate that MSA provides clinical efficacy comparable to that of fundoplication.
Differential Diagnosis
The differential diagnosis of hiatal hernias overlaps with that of GERD, which can be extensive. Typical heartburn is characterized by an epigastric, caustic, burning sensation rather than radiating pressure. A thorough history can distinguish GERD from acute coronary syndrome, peptic ulcer disease, biliary disorders, and pancreatitis. GERD must also be differentiated from reflux hypersensitivity or functional heartburn, which can mimic typical reflux symptoms.[27] Patients with large PEHs may present with dysphagia. The differential diagnosis of dysphagia includes peptic esophageal stricture, esophageal carcinoma, epiphrenic or Zenker diverticulum, and esophageal motility disorders such as achalasia.
Extraesophageal GERD symptoms often arise from respiratory tract involvement, manifesting as laryngeal or pulmonary symptoms. Determining the underlying cause can be challenging, requiring consideration of primary esophageal motility disorders, gastric or esophageal carcinoma, and primary pulmonary disease. Alternative etiologies should be investigated when the primary workup is inconclusive. Consultation with a pulmonologist is frequently warranted in such cases.[28] Appropriate diagnostic workup, including EGD and barium esophagram, is essential for establishing an accurate diagnosis. Assessment findings also guide subsequent management.
Prognosis
Operative management has markedly improved outcomes for hiatal hernias over the past 2 decades. Symptom improvement and perioperative complications have decreased with increased surgical experience, particularly in high-volume centers.[29] Prognosis varies according to the size of the hiatal hernia. Successful management relies on an evidence-based diagnosis rather than on symptoms alone.
The success of hiatal hernia surgery may be measured by evaluating symptom relief, reduction in esophageal acid exposure, incidence of complications, and the need for reoperation. Patients with small hiatal hernias who undergo surgery generally experience excellent outcomes with sustained symptom relief. Results from a prospective study of 100 patients followed for 10 years after ARS showed a 90% reduction in symptoms at the end of follow-up.
Patients with large PEHs demonstrate a 50% radiologic recurrence rate at 5 years, even when mesh is used to reinforce the hiatal closure. Most recurrences occur within the first 2 years after surgery, and less than 10% of patients with recurrent hernias require reoperation for recurrent symptoms.[30][31] The odds of recurrence are higher when the majority of the stomach resides in the chest compared with smaller hernias containing only the fundus.[32] Surgical outcomes are improved when procedures are performed by high-volume surgeons.
Repair of PEHs provides relief of mechanical symptoms, including dysphagia and dyspnea. A recent meta-analysis systematically reviewed the relationship between pulmonary function and hiatal hernia repair, encompassing 5 cohort studies with a total of 262 participants. Significant improvements were observed in forced expiratory volume in 1 second, forced vital capacity, and total lung capacity following surgical repair. Residual volume and carbon monoxide diffusing capacity did not improve significantly. Overall, these findings indicate that surgical repair may benefit patients with associated pulmonary symptoms.
Complications
Large, untreated hiatal hernias can result in gastric volvulus, strangulation, or acute presentation following trauma. The most common postoperative effects include transient dysphagia, gas bloat, and impaired ability to belch or vomit, which occur more frequently after a Nissen fundoplication. Postoperative dysphagia is generally transient, most often resulting from edema and the newly constructed fundoplication, and typically resolves without intervention. Dysphagia is also a recognized complication of MSA.
Significant complications after surgery are relatively uncommon, typically minor, and often not directly attributable to the procedure itself. Data from a single institution demonstrated that adults older than 72 with high frailty have double the risk of morbidity following elective PEH repair. These findings are consistent with national data, indicating that age and frailty are significant predictors of morbidity after emergent hernia repair.[33][34] The overall 30-day mortality rate associated with ARS is approximately 0.19%.
Complications specific to ARS include capnothorax and gastroesophageal or hepatosplenic injuries. Capnothorax is the most common intraoperative complication, occurring in less than 2% of patients. Gastric or esophageal injuries occur in approximately 1% of patients undergoing Nissen fundoplication, most often during reoperations. Splenic and liver injuries may result in bleeding and are reported in about 2.3% of cases. Major hepatosplenic injury is rare. Postoperative dysphagia is generally transient, most frequently caused by edema and the newly constructed fundoplication, and typically resolves without intervention.[35]
Postoperative and Rehabilitation Care
Postoperative management after hiatal hernia repair varies according to the type of operation, surgeon preference, and institutional protocols. Many surgeons obtain a barium esophagram on the first postoperative day to assess transit through the newly constructed fundoplication or PEH repair, particularly following large PEH repair (see Image. Paraesophageal Hernia Esophagram).
Dietary advancement also differs by procedure. After fundoplication, patients typically begin a liquid diet for 1 to 2 weeks, followed by a gradual progression over several weeks. Patients undergoing MSA initiation begin a solid diet immediately to facilitate device movement and prevent peridevice scar formation. Most patients are discharged home within 1 to 2 days. However, older adults or individuals with large PEH may require prolonged hospitalization or transfer to a rehabilitation facility, especially in cases presenting with acute incarceration.
Deterrence and Patient Education
Prevention of hiatal hernia focuses on measures that reduce intra-abdominal pressure, including maintaining a healthy weight, avoiding heavy lifting, and practicing proper posture. Dividing meals into smaller, more frequent portions and remaining upright after eating further reduces risk. Consumption of spicy foods, excessive caffeine, and alcohol should be avoided, and dinner should be consumed at least 2 to 3 hours before bedtime. Adherence to prescribed medications and postoperative instructions is essential for patients undergoing treatment for GERD or hiatal hernia-related symptoms. Postoperative guidance typically includes dietary modifications tailored to the recovery period.
Pearls and Other Issues
The vast majority of patients with small hiatal hernias and GERD may be managed successfully with PPIs. Patients who are refractory to medical therapy or present with large, symptomatic PEHs benefit from ARS. Close monitoring is essential because smaller hiatal hernias generally have more favorable outcomes, and prompt referral to an experienced surgeon is recommended if symptoms do not resolve with medications. Prolonged trials of multiple medications or repeated switching is not supported by evidence and may not serve the patient’s best interest. Timely surgical evaluation is advised for patients with large, symptomatic PEHs who are appropriate surgical candidates.
Enhancing Healthcare Team Outcomes
A hiatal hernia occurs when the upper portion of the stomach or other abdominal organs are displaced through the diaphragm’s esophageal hiatus into the chest cavity, compromising the LES. This structural abnormality can cause GERD, heartburn, regurgitation, or dysphagia, and the condition's prevalence increases with age and conditions that elevate intra-abdominal pressure. Type I sliding hiatal hernias account for most cases and are typically managed medically, whereas larger PEHs often require surgical repair.
Effective management of hiatal hernias relies on coordinated, interprofessional care. Physicians and advanced practitioners evaluate symptom severity, guide diagnostic testing, and determine appropriate medical or surgical treatment. Nurses and dietitians provide patient education, postoperative care, and counseling on lifestyle modifications. Pharmacists ensure safe medication use and monitor for interactions with acid-suppressive therapies. Radiologists and gastroenterologists contribute to diagnostic imaging and endoscopy. Clear communication, shared decision-making, and coordinated follow-up among all team members optimize patient outcomes, enhance safety, and support high-quality, patient-centered care.
Media
(Click Image to Enlarge)

Massive Hiatal Hernia. This contrast-enhanced abdominopelvic computed tomography scan shows a hiatal hernia accompanied by gastric volvulus and obstruction at the diaphragm.
Contributed by E Shufflebarger, MD
(Click Image to Enlarge)

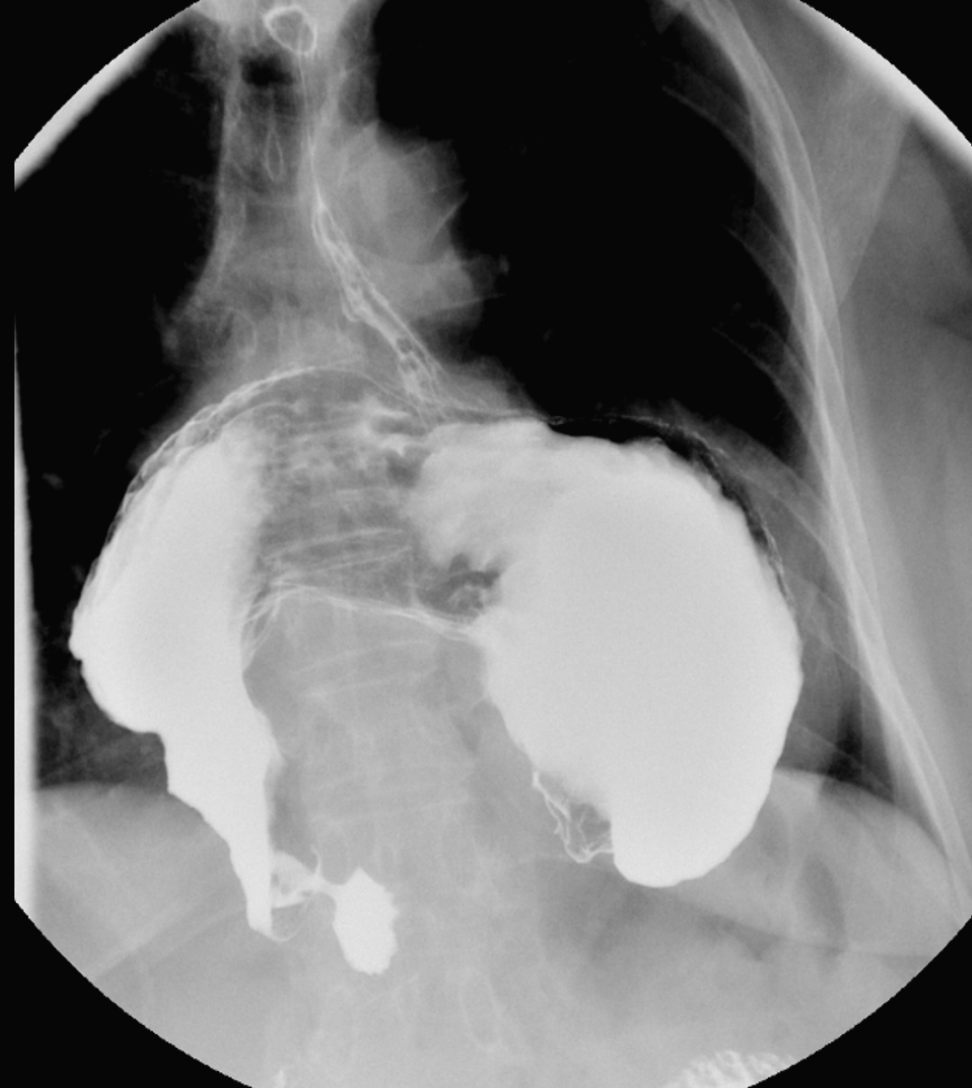
Type I Hiatal Hernia. This barium swallow esophagogram shows a classic sliding hiatal hernia where the gastroesophageal junction migrates cephalad through the esophageal hiatus.
Personal
(Click Image to Enlarge)
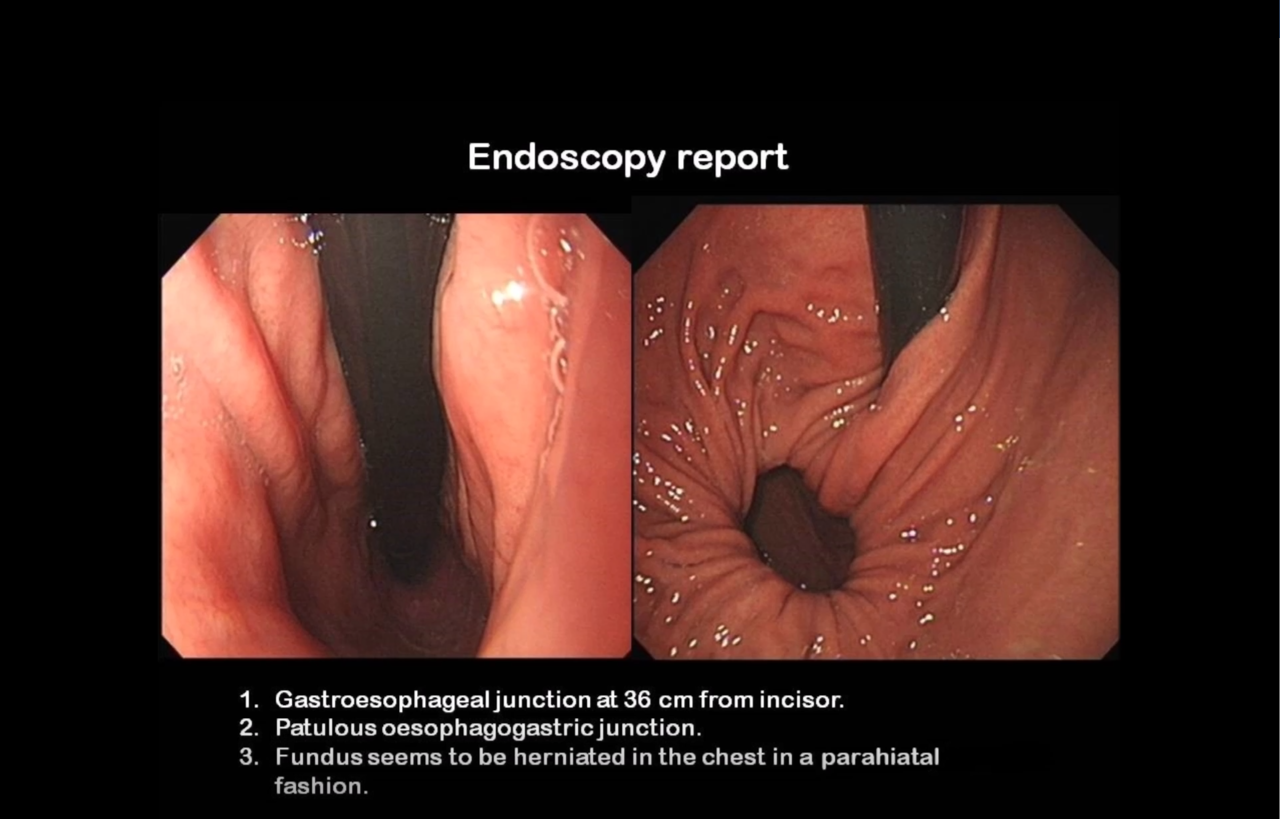
Endoscopic View of a Parahiatal Hernia. Findings include the following: 1) gastroesophageal junction at 36 cm from incisor; 2) patulous esophagogastric junction; and 3) fundus seems to be herniated in the chest in a parahiatal fashion.
Contributed by AM Isla, FRCS
(Click Image to Enlarge)

Sliding Hiatal Hernia on Barium Study. The image demonstrates upward displacement of the stomach through the diaphragm, consistent with a sliding hiatal hernia.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
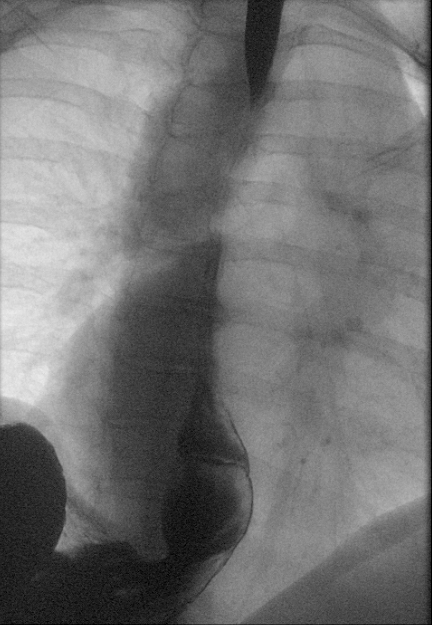
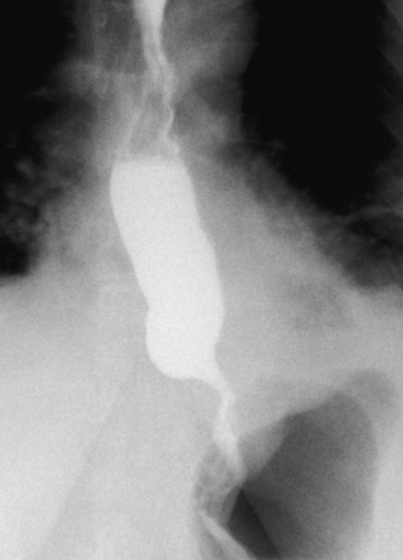
Hiatal Hernia on Fluoroscopy. This fluoroscopic image demonstrates a hiatal hernia of the esophagus.
Contributed by Dr Dawood Tafti.
(Click Image to Enlarge)
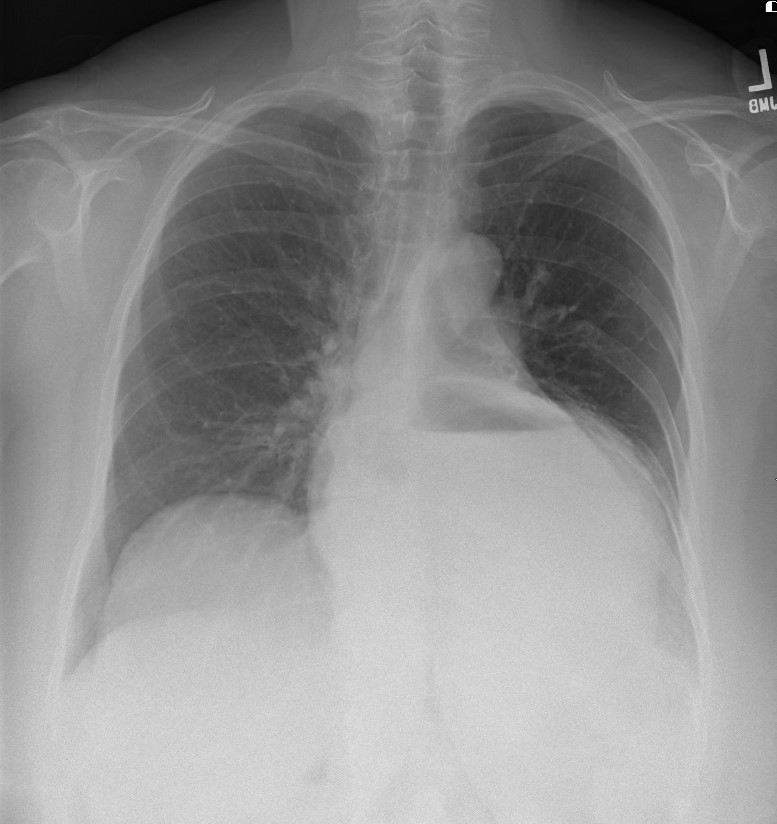
Radiographic Appearance of a Mixed Paraesophageal Hernia. A large gas-filled structure with an air-fluid level is seen in the retrocardiac space on this chest film. This finding represents a type III hernia where both the gastroesophageal junction and the gastric fundus have protruded above the diaphragm.
Contributed by Alyssa Pastorino, DO
(Click Image to Enlarge)

Type III Paraesophageal Hernia on Computed Tomography. This coronal view demonstrates combined sliding and paraesophageal herniation, with a significant portion of the stomach displaced above the diaphragm.
Personal
(Click Image to Enlarge)
Gastric Volvulus on Contrast Radiography. A contrast-enhanced radiograph showing abnormal rotation of the stomach, resulting in a distorted and malpositioned gastric outline.
Personal
(Click Image to Enlarge)
Paraesophageal Hernia Esophagram. Postoperative esophagram demonstrates no recurrent paraesophageal hernia with normal contrast passage through the fundoplication.
Personal
References
Nugraha HG, Agustina M, Nataprawira HM. Diagnostic challenges of hiatal hernia Type IV: An imaging perspective. Radiology case reports. 2025 Jan:20(1):437-441. doi: 10.1016/j.radcr.2024.09.147. Epub 2024 Oct 30 [PubMed PMID: 39534747]
Level 3 (low-level) evidenceKahrilas PJ, Kim HC, Pandolfino JE. Approaches to the diagnosis and grading of hiatal hernia. Best practice & research. Clinical gastroenterology. 2008:22(4):601-16. doi: 10.1016/j.bpg.2007.12.007. Epub [PubMed PMID: 18656819]
McNellage L, Pacheco ZS, Shufflebarger EF. Massive Hiatal Hernia With Acute Gastric Volvulus Masked as a Suspected Food Poisoning: A Case Report. Cureus. 2023 Sep:15(9):e44943. doi: 10.7759/cureus.44943. Epub 2023 Sep 9 [PubMed PMID: 37818520]
Level 3 (low-level) evidenceWang Y, Lv Y, Liu Y, Xie C. The effect of surgical repair of hiatal hernia (HH) on pulmonary function: a systematic review and meta-analysis. Hernia : the journal of hernias and abdominal wall surgery. 2023 Aug:27(4):839-848. doi: 10.1007/s10029-023-02756-5. Epub 2023 Feb 24 [PubMed PMID: 36826630]
Level 1 (high-level) evidenceAlvarez LA, Debski AM, Egli AE, Hatlovic MA, Rosenthal OD, Gardner S. Hiatal Hernia of Stomach and Lesser Omentum in a Cadaver: Is It a Type III or IV? Cureus. 2024 Mar:16(3):e55431. doi: 10.7759/cureus.55431. Epub 2024 Mar 3 [PubMed PMID: 38567228]
Turaga AH. Hiatal Hernia to Bochdalek: A Case Report. Cureus. 2023 Aug:15(8):e43859. doi: 10.7759/cureus.43859. Epub 2023 Aug 21 [PubMed PMID: 37736470]
Level 3 (low-level) evidenceAili A, Maimaitiming M, Li Y, Maisiyiti A, Wang Z, Tusuntuoheti Y, Abudureyimu K. Laparoscopic hiatal hernia repair for treating patients with massive hiatal hernia and iron-deficiency anaemia. BMC surgery. 2023 Sep 26:23(1):293. doi: 10.1186/s12893-023-02184-3. Epub 2023 Sep 26 [PubMed PMID: 37752453]
Fuchs KH, Kafetzis I, Hann A, Meining A. Hiatal Hernias Revisited-A Systematic Review of Definitions, Classifications, and Applications. Life (Basel, Switzerland). 2024 Sep 11:14(9):. doi: 10.3390/life14091145. Epub 2024 Sep 11 [PubMed PMID: 39337928]
Level 1 (high-level) evidenceBalasubramanian G, Singh M, Gupta N, Gaddam S, Giacchino M, Wani SB, Moloney B, Higbee AD, Rastogi A, Bansal A, Sharma P. Prevalence and predictors of columnar lined esophagus in gastroesophageal reflux disease (GERD) patients undergoing upper endoscopy. The American journal of gastroenterology. 2012 Nov:107(11):1655-61. doi: 10.1038/ajg.2012.299. Epub 2012 Oct 2 [PubMed PMID: 23032983]
Richter JE, Rubenstein JH. Presentation and Epidemiology of Gastroesophageal Reflux Disease. Gastroenterology. 2018 Jan:154(2):267-276. doi: 10.1053/j.gastro.2017.07.045. Epub 2017 Aug 3 [PubMed PMID: 28780072]
Tack J, Pandolfino JE. Pathophysiology of Gastroesophageal Reflux Disease. Gastroenterology. 2018 Jan:154(2):277-288. doi: 10.1053/j.gastro.2017.09.047. Epub 2017 Oct 14 [PubMed PMID: 29037470]
Pather K, Dowdall R, Mobley EM, Sacco J, Puri R. Definitive, urgent repair of acutely incarcerated paraesophageal hernias is comparable to an elective repair. Surgical endoscopy. 2025 Jul:39(7):4558-4563. doi: 10.1007/s00464-025-11847-6. Epub 2025 Jun 9 [PubMed PMID: 40490576]
Patel D, Fass R, Vaezi M. Untangling Nonerosive Reflux Disease From Functional Heartburn. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2021 Jul:19(7):1314-1326. doi: 10.1016/j.cgh.2020.03.057. Epub 2020 Apr 1 [PubMed PMID: 32246998]
Kamarajah SK, Boyle C, Navidi M, Phillips AW. Critical appraisal of the impact of surgical repair of type II-IV paraoesophageal hernia (POH) on pulmonary improvement: A systematic review and meta-analysis. The surgeon : journal of the Royal Colleges of Surgeons of Edinburgh and Ireland. 2020 Dec:18(6):365-374. doi: 10.1016/j.surge.2020.01.006. Epub 2020 Feb 8 [PubMed PMID: 32046901]
Level 1 (high-level) evidenceGadenstätter M, Wykypiel H, Schwab GP, Profanter C, Wetscher GJ. Respiratory symptoms and dysphagia in patients with gastroesophageal reflux disease: a comparison of medical and surgical therapy. Langenbeck's archives of surgery. 1999 Dec:384(6):563-7 [PubMed PMID: 10654272]
Sfara A, Dumitrascu DL. The management of hiatal hernia: an update on diagnosis and treatment. Medicine and pharmacy reports. 2019 Oct:92(4):321-325. doi: 10.15386/mpr-1323. Epub 2019 Oct 25 [PubMed PMID: 31750430]
Yadlapati R, Gyawali CP, Pandolfino JE, CGIT GERD Consensus Conference Participants. AGA Clinical Practice Update on the Personalized Approach to the Evaluation and Management of GERD: Expert Review. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2022 May:20(5):984-994.e1. doi: 10.1016/j.cgh.2022.01.025. Epub 2022 Feb 2 [PubMed PMID: 35123084]
Level 3 (low-level) evidenceGyawali CP, Yadlapati R, Fass R, Katzka D, Pandolfino J, Savarino E, Sifrim D, Spechler S, Zerbib F, Fox MR, Bhatia S, de Bortoli N, Cho YK, Cisternas D, Chen CL, Cock C, Hani A, Remes Troche JM, Xiao Y, Vaezi MF, Roman S. Updates to the modern diagnosis of GERD: Lyon consensus 2.0. Gut. 2024 Jan 5:73(2):361-371. doi: 10.1136/gutjnl-2023-330616. Epub 2024 Jan 5 [PubMed PMID: 37734911]
Level 3 (low-level) evidenceMainie I, Tutuian R, Shay S, Vela M, Zhang X, Sifrim D, Castell DO. Acid and non-acid reflux in patients with persistent symptoms despite acid suppressive therapy: a multicentre study using combined ambulatory impedance-pH monitoring. Gut. 2006 Oct:55(10):1398-402 [PubMed PMID: 16556669]
Slater BJ, Collings A, Dirks R, Gould JC, Qureshi AP, Juza R, Rodríguez-Luna MR, Wunker C, Kohn GP, Kothari S, Carslon E, Worrell S, Abou-Setta AM, Ansari MT, Athanasiadis DI, Daly S, Dimou F, Haskins IN, Hong J, Krishnan K, Lidor A, Litle V, Low D, Petrick A, Soriano IS, Thosani N, Tyberg A, Velanovich V, Vilallonga R, Marks JM. Multi-society consensus conference and guideline on the treatment of gastroesophageal reflux disease (GERD). Surgical endoscopy. 2023 Feb:37(2):781-806. doi: 10.1007/s00464-022-09817-3. Epub 2022 Dec 18 [PubMed PMID: 36529851]
Level 3 (low-level) evidenceKatz PO, Dunbar KB, Schnoll-Sussman FH, Greer KB, Yadlapati R, Spechler SJ. ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. The American journal of gastroenterology. 2022 Jan 1:117(1):27-56. doi: 10.14309/ajg.0000000000001538. Epub [PubMed PMID: 34807007]
Hart AM. Evidence-based recommendations for GERD treatment. The Nurse practitioner. 2013 Aug 10:38(8):26-34; quiz 34-5. doi: 10.1097/01.NPR.0000431881.25363.84. Epub [PubMed PMID: 23812348]
Abbas AE, Deschamps C, Cassivi SD, Allen MS, Nichols FC 3rd, Miller DL, Pairolero PC. Barrett's esophagus: the role of laparoscopic fundoplication. The Annals of thoracic surgery. 2004 Feb:77(2):393-6 [PubMed PMID: 14759403]
Level 2 (mid-level) evidenceEpstein D, Bojke L, Sculpher MJ, REFLUX trial group. Laparoscopic fundoplication compared with medical management for gastro-oesophageal reflux disease: cost effectiveness study. BMJ (Clinical research ed.). 2009 Jul 14:339():b2576. doi: 10.1136/bmj.b2576. Epub 2009 Jul 14 [PubMed PMID: 19654097]
Level 1 (high-level) evidenceFass R. An Overview of Transoral Incisionless Fundoplication and Magnetic Sphincter Augmentation for GERD. Gastroenterology & hepatology. 2017 Jan:13(1):50-52 [PubMed PMID: 28420946]
Level 3 (low-level) evidenceDeMeester SR. Laparoscopic Hernia Repair and Fundoplication for Gastroesophageal Reflux Disease. Gastrointestinal endoscopy clinics of North America. 2020 Apr:30(2):309-324. doi: 10.1016/j.giec.2019.12.007. Epub 2020 Feb 6 [PubMed PMID: 32146948]
Yadlapati R, Pandolfino JE. Personalized Approach in the Work-up and Management of Gastroesophageal Reflux Disease. Gastrointestinal endoscopy clinics of North America. 2020 Apr:30(2):227-238. doi: 10.1016/j.giec.2019.12.002. Epub 2020 Jan 22 [PubMed PMID: 32146943]
Vaezi MF, Katzka D, Zerbib F. Extraesophageal Symptoms and Diseases Attributed to GERD: Where is the Pendulum Swinging Now? Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2018 Jul:16(7):1018-1029. doi: 10.1016/j.cgh.2018.02.001. Epub 2018 Feb 7 [PubMed PMID: 29427733]
Dallemagne B, Weerts J, Markiewicz S, Dewandre JM, Wahlen C, Monami B, Jehaes C. Clinical results of laparoscopic fundoplication at ten years after surgery. Surgical endoscopy. 2006 Jan:20(1):159-65 [PubMed PMID: 16333553]
Oelschlager BK, Pellegrini CA, Hunter JG, Brunt ML, Soper NJ, Sheppard BC, Polissar NL, Neradilek MB, Mitsumori LM, Rohrmann CA, Swanstrom LL. Biologic prosthesis to prevent recurrence after laparoscopic paraesophageal hernia repair: long-term follow-up from a multicenter, prospective, randomized trial. Journal of the American College of Surgeons. 2011 Oct:213(4):461-8. doi: 10.1016/j.jamcollsurg.2011.05.017. Epub 2011 Jun 29 [PubMed PMID: 21715189]
Level 1 (high-level) evidenceSmith CD, McClusky DA, Rajad MA, Lederman AB, Hunter JG. When fundoplication fails: redo? Annals of surgery. 2005 Jun:241(6):861-9; discussion 869-71 [PubMed PMID: 15912035]
Lidor AO, Steele KE, Stem M, Fleming RM, Schweitzer MA, Marohn MR. Long-term quality of life and risk factors for recurrence after laparoscopic repair of paraesophageal hernia. JAMA surgery. 2015 May:150(5):424-31. doi: 10.1001/jamasurg.2015.25. Epub [PubMed PMID: 25785415]
Level 2 (mid-level) evidenceWang TN, An BW, Wang TX, McNamara M, Sweigert PJ, Yuce TK, Heh V, Collins CE, Haisley KR, Perry KA. The effect of frailty and age on outcomes in elective paraesophageal hernia repair. Surgical endoscopy. 2023 Dec:37(12):9514-9522. doi: 10.1007/s00464-023-10363-9. Epub 2023 Sep 13 [PubMed PMID: 37704792]
Kumar SS, Rama M, Koeneman S, Tannouri S, Tatarian T, Palazzo F. Morbidity and mortality following hiatal hernia repair in geriatric patients: a multicenter research network study. Surgical endoscopy. 2024 Jul:38(7):3999-4005. doi: 10.1007/s00464-024-10956-y. Epub 2024 Jun 10 [PubMed PMID: 38858249]
Niebisch S, Fleming FJ, Galey KM, Wilshire CL, Jones CE, Litle VR, Watson TJ, Peters JH. Perioperative risk of laparoscopic fundoplication: safer than previously reported-analysis of the American College of Surgeons National Surgical Quality Improvement Program 2005 to 2009. Journal of the American College of Surgeons. 2012 Jul:215(1):61-8; discussion 68-9. doi: 10.1016/j.jamcollsurg.2012.03.022. Epub 2012 May 10 [PubMed PMID: 22578304]
Level 2 (mid-level) evidence