Introduction
Heterotopic ossification is the pathological formation of mature, lamellar bone in extraskeletal soft tissues such as muscles, tendons, and ligaments, without direct continuity to the periosteum. Heterotopic ossification is a frequent and clinically significant complication encountered in various rehabilitation and surgical settings, particularly following orthopaedic procedures such as total hip arthroplasty (THA), trauma, burns, spinal cord injury (SCI), traumatic brain injury (TBI), stroke, and joint replacement surgeries.[1][2][3]
First described as “paraosteoarthropathy” in paraplegic soldiers during World War I, heterotopic ossification continues to present a substantial burden in civilian and military populations. The pathogenesis of heterotopic ossification involves an initial inciting event, typically soft-tissue trauma, followed by an inflammatory cascade that recruits mesenchymal stem cells and induces their differentiation into chondrocytes and osteoblasts, ultimately leading to ectopic bone formation via endochondral ossification. While acquired heterotopic ossification remains the primary concern in orthopaedic and neurorehabilitation practice, rare hereditary forms include fibrodysplasia ossificans progressiva, progressive osseous heteroplasia, and Albright’s hereditary osteodystrophy. These genetic disorders are governed by distinct mechanisms and are not the focus of this discussion.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Heterotopic ossification can be classified into 3 main categories: traumatic, neurogenic, and genetic. The most common is traumatic, which occurs after injuries such as fractures, arthroplasty, muscular trauma, joint dislocations, or burns. In total joint arthroplasty, heterotopic ossification is most frequently observed after hip, knee, elbow, and shoulder replacements. Chronic muscular trauma can lead to traumatic myositis ossificans, with the quadriceps femoris and brachialis muscles being the most commonly affected.
The second category is neurogenic, associated with neurologic insults such as stroke, SCI, traumatic brain injury, and brain tumors.[5] Neurogenic heterotopic ossification most commonly involves the hips, the extensor side of the elbows, shoulders, and knees, though rare sites include incisions, kidneys, the uterus, the corpora cavernosum, and the gastrointestinal tract. The exact mechanism is not fully understood and is discussed further in the Pathophysiology section. Risk factors include spasticity, older age, pressure ulcers, deep vein thrombosis, tracheostomy, long bone fractures, prior injury to the same area, edema, immobility, long-term coma, and severity of trauma, TBI, SCI, or stroke. In the THA population, high- and moderate-risk factors include men with bilateral THA, prior history of heterotopic ossification, ankylosing spondylitis, diffuse idiopathic skeletal hyperostosis, or Paget disease.[6]
The third and rarest category is genetic, including fibrodysplasia ossificans progressiva, a disorder characterized by abnormal, progressive bone formation in soft tissues following injury. This condition manifests at birth with malformations of the great toe and leads to widespread skeletal immobilization due to progressive ectopic bone formation. Minor trauma, intramuscular injections, and surgical procedures can precipitate flare-ups, making early recognition and avoidance of unnecessary interventions essential to prevent irreversible functional decline.[4]
Epidemiology
The prevalence of heterotopic ossification varies widely depending on the underlying clinical context.[1] In patients undergoing THA, reported incidence rates range from 8% to 90%, with an overall average prevalence estimated around 53%, particularly in those with high-risk factors such as men, cemented components, and older age.[2] Heterotopic ossification is approximately twice as common in men as in women; however, women aged 65 and older may also have an elevated risk.
Following acetabular fractures, the incidence ranges from 17% to 100%, whereas in burn injuries, the incidence is lower, with rates reported at 0.2% to 4%.[7][8] Among patients with neurological injury, neurogenic heterotopic ossification occurs in 10% to 20% of cases. More specifically, adult patients with SCI have a 20% to 30% incidence, whereas patients with TBI demonstrate a 10% to 20% incidence. In pediatric TBI populations, the prevalence ranges from 3% to 20%.[9] Clinically, heterotopic ossification can result in substantial morbidity due to pain, joint contracture, ankylosis, limited mobility, and secondary complications such as disuse osteopenia and fracture risk.
Pathophysiology
The exact mechanism of heterotopic ossification in traumatic and neurogenic cases is unknown, but 2 common factors precede its formation—the first being trauma or an inciting neurological event.[10] In the SCI population, it is hypothesised that acute rehabilitation, transfer activities, and repeated microtrauma during activities of daily living can accumulate mechanical stress, predisposing individuals to heterotopic ossification. Second, after trauma or neurological injury, tissue expression of bone morphogenetic proteins (BMPs) changes. BMPS stimulate mesenchymal spindle stem cells, also known as satellite cells, to migrate to the injured area, where they differentiate into fibroblasts and, eventually, osteoblasts.
Evidence indicates that alkaline phosphatase also contributes to ectopic bone formation. Alkaline phosphatase suppresses inhibitors of bone formation and is known to be elevated in vascular smooth muscle tissue in the presence of inflammatory cytokines and macrophages.[10] After migration, mesenchymal spindle cells differentiate into fibroblasts, which then secrete immature connective tissue composed of collagen and extracellular matrix. With continued tissue irritation, fibroblastic metaplasia is activated, transforming fibroblasts into chondrocytes through a process similar to endochondral ossification. Some of the chondrocytes continue to deposit collagen into the cartilage matrix while the remaining chondrocytes transform into osteoblasts. By 1 to 2 weeks, new osteoid is present within the tissue, and new bone formation starts to form within the osteoid. Osteoblasts then begin to degrade and replace the cartilage with bone. Calcium pyrophosphate within the osteoid is slowly replaced by hydroxyapatite crystals as the bone mineralises and matures.[11]
The pathogenesis of neurogenic heterotopic ossification following SCI has been investigated in murine models. Heterotopic bone formation occurs after combined injury to the central nervous system and skeletal muscle. This process results from dysregulation of normal muscle repair. Under physiological conditions, fibro-adipogenic progenitor cells undergo tumor necrosis factor-induced apoptosis by inflammatory macrophages, thereby preventing fibrosis.[12]
Following SCI, these progenitors escape apoptosis, accumulate, and differentiate into osteoblasts.[13] This shift toward osteogenesis is driven by stress-induced adrenal glucocorticoid release, particularly corticosterone, which amplifies local inflammation and promotes excessive secretion of oncostatin M and interleukin-1β in injured muscle.[14] These bind to their receptors and promote osteogenic proliferation, explaining the higher incidence of neurogenic heterotopic ossification observed in patients with traumatic brain or SCI who develop gram-negative infections. Lipopolysaccharides from gram-negative organisms induce heterotopic bone formation by activating Toll-like receptor 4 on macrophages and muscle fibro-adipogenic progenitors, thereby increasing macrophage secretion of oncostatin M and interleukin-1β.[15][16]
Heterotopic ossification is a complex, multifactorial process. Rooted in mechanisms similar to fibrodysplasia ossificans progressiva, involving mutations in activin receptor–like kinase 2 (activin A receptor type I) that cause aberrant BMP signalling. Trauma-induced heterotopic ossification is characterized by increased BMP-2 and BMP-4 activity, leading to downstream Smad1/5/8 phosphorylation and osteogenic gene activation. Additional contributors include tyrosine kinase with immunoglobulin-like and epidermal growth factor-like domains 2–positive progenitor cells, fibroblasts capable of transdifferentiation, and environmental factors such as hypoxia and pH.[17][18]
Histopathology
Microscopic examination of the biopsy in myositis ossificans revealed an outer zone of hypercellular spindle cells and woven bone surrounding an inner zone of trapped muscle with normal osteoblasts continuing to lay down bone. Heterotopic ossification can be distinguished from osteosarcoma by its characteristic zonation pattern, which progresses from central immature fibrous tissue to peripheral mature bone. In contrast, osteosarcoma demonstrates mature bone formation within the central zone.[5]
Histologically, heterotopic ossification is characterized by lamellar bone formation within soft tissue, frequently via an endochondral ossification pathway. At initial injury, there is a proliferation of hypercellular spindle cells. Cartilage and woven bone start to form 2 weeks after injury. Trabecular bone starts to form from weeks 2 to 5 with mature fatty bone marrow. After 6 weeks, lamellar bone matures.[19]
History and Physical
Heterotopic ossification usually occurs 3 to 12 weeks after the inciting injury, but it can take up to 6 months to present.[20] Look for a history of recent arthroplasty (eg, THA or total knee replacement), as well as stroke, SCI, TBI, or burns. The most common presentation is pain and decreased range of motion. Patients often complain of joint stiffness. Other common signs to look for are local edema, effusion, erythema, warmth, and tenderness in the tissue or joint.[5]
Localized soft-tissue swelling may mimic a deep vein thrombosis. The patient may also present with a low-grade fever. Since spasticity is a risk factor, the patient may present with spasticity near the affected joint. Other risk factors to look for in the history are prolonged coma, tracheostomy or gastric tube, immobility, pressure ulcers, and associated long bone fractures.[21] The greatest risk of developing heterotopic ossification also occurs during the 3- to 4-month post-injury period.
Evaluation
Laboratory Studies
Alkaline phosphatase has historically been the most commonly ordered laboratory test for heterotopic ossification; however, levels may remain normal in the early stages of bone formation.[22] Elevation may not occur until up to 2 weeks after injury and can increase to as much as 3.5 times the normal value by 10 weeks post-injury. In the THA population, serum alkaline phosphatase levels greater than 250 have been shown to correlate with heterotopic ossification and injury severity. Clinicians should note that alkaline phosphatase levels may also be falsely elevated in the presence of associated long-bone injuries.
Erythrocyte sedimentation rate (ESR) is another inflammatory marker that is used. ESR greater than 35 mm/hr can indicate the development of heterotopic ossification.[23] C-reactive protein is another inflammatory marker that can be elevated in earlyheterotopic ossification. Both are nonspecific. Creatine kinase can be used to assess the severity of heterotopic ossification; however, it is not highly specific.[5] Results from a study of 18 patients with SCI determined that an elevated creatine kinase may be associated with a more aggressive course of heterotopic ossification and may show possible resistance to etidronate therapy.[24]
Imaging
Plain radiographs
Plain radiographs are first-line but have poor early sensitivity; they are generally used for grading. Radiographs show circumferential bone formation around or near a joint with a radiolucent center (see Images. Heterotopic Ossification of the Elbow, Radiograph and Heterotopic Ossification, Radiograph). Radiographs are specific for heterotopic ossification but not sensitive in early disease. Plain films may not be positive until 3 to 4 weeks after heterotopic ossification is detected on a bone scan. Therefore, the triple-phase bone scan is the most sensitive. A bone scan can reveal heterotopic ossification as early as 2.5 weeks after injury.[5]
MRI
In the acute or early phase of disease, MRI remains the gold standard for detecting soft-tissue masses.[25]
Computed tomography
This imaging may be used to delineate the area of bone formation prior to surgery, but its role in the evaluation/diagnosis of heterotopic ossification is not established.[10] MRI may also be used, but it is not cost-effective unless the bone encompasses neurologic structures. Other imaging techniques that are uncommonly used include ultrasound and 3-dimensional stereolithography. Computed tomography may be used preoperatively to better define the extent and location of mature bone prior to surgical resection; however, its role in the initial evaluation and diagnosis of heterotopic ossification is limited.[10] MRI may also assist with surgical planning, but it is generally not cost-effective unless heterotopic bone involves or threatens neurologic structures.
Ultrasound
Ultrasound detects early lesions preoperatively.[26]
Positron emission tomography, single-photon emission computed tomography, and Raman spectroscopy
Advanced imaging modalities, including positron emission tomography, single-photon emission computed tomography, and Raman spectroscopy, are considered experimental but show promise for early detection and assessment of disease activity.[27][28]
Treatment / Management
Prophylaxis
The approach to prophylaxis involves identifying patients at high risk of developing heterotopic ossification. Routine prophylaxis is not recommended. Preventive treatment strategies for heterotopic ossification remain largely undefined, primarily because the cellular and molecular pathways underlying the condition are not yet fully understood. Early passive ROM exercises should be initiated once heterotopic ossification is confirmed to prevent joint ankylosis.
- Nonsteroidal anti-inflammatory drugs
- Nonsteroidal anti-inflammatory drugs (NSAIDs) remain the mainstay of pharmacologic prophylaxis. Indomethacin, administered at 25 mg 3 times daily for 3 to 6 weeks postoperatively, has been the historical standard.[29][30] NSAIDs inhibit cyclooxygenase (COX)-1 and COX-2, thereby reducing prostaglandin-mediated osteogenesis.[29] Other NSAIDs that have been proven effective are meloxicam, celecoxib, rofecoxib, and ibuprofen.
- Selective COX-2 inhibitors such as etoricoxib have demonstrated equivalent efficacy to non-selective NSAIDs in preventing heterotopic ossification, while reducing gastrointestinal side effects and risk of bleeding. Etoricoxib has been effective when administered at 90 mg daily in patients with THA.[31][32]
- Limitations: Risk of gastrointestinal irritation, renal dysfunction, and impaired bone healing—especially concerning in fracture settings.[33]
- Careful monitoring must be done for the risk of bleeding, especially with concurrent chemoprophylaxis for venous thromboembolism. Concurrent prophylaxis is advised for gastrointestinal ulcers.
- Bisphosphonates
- These antiresorptive agents inhibit osteoclast-mediated bone turnover and mineralisation. While etidronate and alendronate have shown some efficacy in reducing the development of heterotopic ossification, clinical results remain inconsistent. Some study results support their use in high-risk individuals, while others advise against routine prophylaxis due to a lack of reproducible benefit.
- For SCI-associated heterotopic ossification, the recommended treatment is 20 mg/kg per day for 2 weeks, followed by 10 mg/kg per day for 10 weeks, for a total treatment period of 12 weeks. For THA, the recommended treatment is 20 mg/kg per day for 1 month preoperatively, followed by the same dose for 3 months postoperatively.[30]
- External-beam radiation therapy is most commonly used after total joint arthroplasty. A single dose of 700 to 800 g (centigray) is administered up to 24 hours preoperatively or within 72 hours postoperatively.[34]
- Radiotherapy
- Low-dose external-beam radiotherapy (700–800 cGy) delivered within 24 hours preoperatively or within 3 days postoperatively reduces the incidence of heterotopic ossification, particularly after THA and SCI. Radiotherapy is especially useful in NSAID-intolerant patients or those at very high risk of recurrence.[35][36]
- The adverse effects of radiotherapy include delayed wound healing, soft-tissue fibrosis, and potential interference with implant osseointegration, especially in cementless THA.
(A1)
Surgical Treatment
Surgical excision of heterotopic ossification is indicated in patients with functionally limiting joint ankylosis, persistent pain or reduced range of motion, and in cases where there is interference with prosthetic function or personal hygiene
Timing is crucial to minimize recurrence risk, with resection ideally delayed until radiological and clinical signs of ossification maturity:
- ≥6 months after trauma-related heterotopic ossification
- ≥12 months after SCI
- ≥18 months after traumatic brain injury
Risks and complications of surgical intervention:
- Infection
- Wound breakdown
- Neurovascular injury (eg, sciatic nerve in hip heterotopic ossification)
- Recurrence of heterotopic ossification
- In some series (eg, acetabular heterotopic ossification), complication rates after excision have reached 33%.
Differential Diagnosis
In the SCI population, deep vein thrombosis (DVT), cellulitis, abscess, hematoma, and tumor (osteosarcoma, osteochondroma) are the most common differential diagnoses to consider, particularly when plain film x-ray is negative. Other common differential diagnoses are hardware infection, thrombophlebitis, and osteomyelitis.[5] A venous Doppler should be ordered to rule out a DVT. Cellulitis and abscesses can be difficult to assess because white blood cell counts and inflammatory markers can be elevated in the setting of heterotopic ossification.
Elevated alkaline phosphatase can help distinguish heterotopic ossification from other infectious conditions. Computed tomography/MRI with contrast can help differentiate heterotopic ossification from hematoma, thrombophlebitis, osteomyelitis, and tumor, but it is not the most cost-effective modality. Triple-phase bone scan remains the most sensitive for detecting heterotopic ossification, especially early on, because it may take up to 6 weeks from the initial presentation of symptoms for heterotopic ossification to appear on an x-ray.
Radiation Oncology
Radiation therapy is more effective than NSAIDs in multiple trials. The effectiveness of indomethacin versus radiation therapy for heterotopic ossification prevention was compared in a prospective randomized trial comparing post-open reduction/internal fixation surgery for patients with an acetabular fracture. Radiation therapy was given as 8 Gy in 1 fraction within 72 hours of surgery, and indomethacin was given for 6 weeks. There was a greater risk of nonunion of long-bone fractures among those who received indomethacin compared with radiation therapy (26% vs 7%, P = 0.004).[37] A subsequent meta-analysis by Pakos et al analyzed 7 randomized trials for 1143 patients and found that radiation therapy was almost twice as effective as NSAIDs. Still, the absolute benefit was less than 2%, with efficacy being dose-dependent.[38]
Radiation Dosing and Fractionation
Radiation oncologists have evaluated numerous radiotherapy fractionation regimens to find the optimal total therapeutic dose for preventing heterotopic ossification in high-risk individuals. In 1987, Anthony et al compared 20 Gy in 10 fractions with 10 Gy in 5 fractions, favouring the higher-dose regimen as marginally more effective in reducing heterotopic ossification, but at the cost of increased radiation-related toxicity (19.4% vs 7.3%).[39] Subsequently, Sylvester et al analyzed outcomes in 28 patients treated with the same fractionation regimen and concluded that both were equally effective when radiotherapy was delivered within 4 days postoperatively.[40] More recently, Ruo Redda et al evaluated the prophylactic role of x-rays in high-risk patients and demonstrated superior outcomes with a single 7 Gy fraction, achieving complete pathological response in 76% of patients.[34]
Radiation Timing
Radiation therapy is typically given preoperatively within 24 hours or postoperatively within 72 hours. If surgery is planned, it is ideal that the patient be consulted and consented to before surgery, since the anesthesia may render the patient unable to give informed consent. Also, the patient could be in more pain postoperatively and may not be able to lie still during treatment. However, in trauma or emergencies, the radiation would be given postoperatively.
A randomized, multi-institutional trial by Gregoritch et al compared patients treated with preoperative vs postoperative 7 to 8 Gy in 1 fraction and found that radiographic and clinical failure rates between the 2 groups were not significantly different.[41] This was examined in another randomized study of 161 patients, who were treated either preoperatively (less than 4 hours before surgery) or postoperatively (less than 72 hours after surgery). There was no significant difference among patients with Brooker grades 0 to 2; however, treatment failures in the overall cohort were significantly lower in the postoperative group. This was likely due to a higher biological equivalent dose as the preoperative group received 7 Gy in 1 fraction, while the postoperative group received 17.5 Gy in 5 fractions. Despite these findings, the current standard is to use a single fraction of 7 to 8 Gy at a single dose, administered preoperatively within 24 hours or postoperatively within 72 hours.
Treatment Planning
The general principles of treatment planning include the use of standard techniques, the use of immobilization devices when needed, and patient positioning to ensure consistent, reproducible daily treatments. Target volumes should encompass the bone surfaces most commonly involved in heterotopic ossification, particularly periarticular regions. Heterotopic ossification frequently develops between the femoral head and pelvis, extending from the greater trochanter to the ilium or from the lesser trochanter to the ischium; therefore, these surfaces should be included within the radiation field.
Radiation techniques for treating heterotopic ossification of the hip have been well described, as this is the most commonly treated site. The patient is treated in a comfortable, reproducible supine position. Each field is customized to the patient’s anatomy. Still, generally, the cranial border is about 3 cm above the acetabulum, the inferior border about 3 cm below the lesser trochanter of the femoral head, or could include the upper third of the implant shaft (if used), with a field size of about 14 x 10 cm. Soft tissue can be blocked by collimating the field to use the field edges, or by using multi-leaf collimators to shape the field, allowing about a 1.5 to 2 cm margin on the bone and prior areas of heterotopic ossification. Three-dimensional conformal radiotherapy using anterior-posterior/posterior-anterior fields with 6 to 15 megavoltage photons is often used to create a homogeneous plan that covers the target to at least the 95% isodose line while minimizing dose to the surrounding soft tissue and skin (see Image. Heterotopic Ossification of the Hip).
The hip is the most common site of heterotopic ossification and the most common site of treatment. However, other joints are also susceptible to heterotopic ossification. Radiation therapy has also been effective in these areas, particularly with the elbow. Results from a study of 36 patients treated at the Cleveland Clinic with 7 Gy in 1 fraction following elbow surgery found that radiation therapy was associated with favorable functional and radiographic outcomes.[42]
Furthermore, results from a retrospective study by Strauss et al of 44 patients found radiographic evidence of heterotopic ossification in 48%, with no complications after high-risk elbow surgery.[43] Favorable outcomes were reported from a case series of 9 patients with clinically significant heterotopic ossification at the elbow. Fractionation consisted of 5 Gy in 2 fractions and 6 to 7 Gy in 1 fraction, with a median follow-up of 7.7 months; there were no failures, and most patients showed clinical improvement.[44]
Toxicity and Adverse Effect Management
Heterotopic ossification is not a malignant condition, but it can cause pain, limited mobility, and negatively affect quality of life. Thus, the benefits of treatment must be weighed against the risks. Patients are often counseled that the low radiation therapy dose used for heterotopic ossification prophylaxis significantly reduces the risk of heterotopic ossification, with minimal adverse effects, and is considered a safe treatment overall. Potential side effects are rare but include fatigue, wound healing delays, joint swelling, and an extremely low chance of secondary cancer from the radiation therapy.
Secondary malignancies from radiation can develop in the bone or tissues included in a previous radiation therapy field. Since the total dose for heterotopic ossification prophylaxis is very low, the risk of secondary malignancies is also extremely low, but not 0. At least 2 case reports have described secondary malignancies after a single fraction. The first case described a 51-year-old patient who received 7 Gy x 1 for heterotopic ossification 15 years earlier. He underwent a second course of 7 Gy x 1 for debilitating heterotopic ossification but developed high-grade undifferentiated sarcoma of the proximal thigh 16 months after his second treatment.[45]
Another case described a 26-year-old man who underwent surgery for an acetabular fracture and received 7 Gy in 1 fraction postoperatively for heterotopic ossification prophylaxis. He presented 11 years later with osteosarcoma of the treated area, which was treated definitively with neoadjuvant cisplatin and doxorubicin (Adriamycin), with plans for surgical resection at the time of the report.[46] Otherwise, there are no other reported cases of secondary malignancies from radiation therapy given for heterotopic ossification prophylaxis treatment.
Trochanteric nonunion and wound healing complications are also potential toxicities from radiation therapy. Results from one study showed that the nonunion rate ranged from 12% to 30% after radiation therapy, whereas it was 2% to 15% lower in those who did not receive radiation therapy.[47] Since modern THA hardware is cementless and porous, it may rely on bony ingrowth at the acetabular or proximal femoral surfaces. There is concern that radiation therapy may inhibit the necessary bony ingrowth and lead to prosthesis failure, which has prompted some clinicians to use shielding of the acetabular cup to prevent this complication. However, a clinical study of patients who received preoperative and postoperative radiation therapy found no evidence of prosthesis failure, even without shielding.[48]
For young men, infertility can also be an adverse effect of radiation therapy. A dosage of 70 to 100 cGy of radiation may cause oligospermia during treatment of the pelvic disease, whereas higher doses may cause azoospermia. Moreover, wearing a lead testicular shield during radiation therapy may help prevent infertility. Patients should also be advised about the possible effects of radiation therapy on fertility.[49]
Staging
Staging is most often used for surgical planning and less commonly for rehabilitation management. The Brooker Classification System, used to assess the severity of heterotopic ossification in the hip, is the most commonly employed staging system and relies on plain radiographs to visually evaluate the presence and extent of bone deposition.[20] A simplified version, called the Della Valle classification system, has been proposed.[50] None of the most commonly used rating systems account for patient function or range of motion, so a modified Brooker classification scale has been proposed that does.
The Brooker Classification divides the extent of heterotopic ossification formation in the hip into 4 classes:
- Class 1: Islands of bone within the soft tissues around the hip
- Class 2: Bone spurs that originate from the pelvis or proximal end of the femur, leaving at least 1 cm between opposing bone surfaces
- Class 3: Bone spurs originating from the pelvis or proximal end of the femur, with a reduced space between opposing bone surfaces of less than 1 cm
- Class 4: Ankylosis of the hip
The Della Valle Classification system:
- Grade A: Absence of heterotopic ossification (or if bone is present, it may be greater than or equal to 1 island of bone of less than 1 cm in length
- Grade B: Presence of greater than or equal to 1 islands of bone at least 1 cm in length, with 1 cm distance between opposing surfaces of bone
- Grade C: Bone spurs arising from the pelvis or femur with less than 1 cm between opposing surfaces or bone ankylosis [50]
Prognosis
Complications of heterotopic ossification include decreased function and mobility, peripheral nerve entrapment, and pressure ulcers. Up to 70% of cases involving heterotopic ossification are asymptomatic. Ankylosis, vascular compression, and lymphedema can occur with heterotopic ossification.[51] Prognosis is generally good after surgery. The mean time from injury to surgery is 3.6 years.
Following surgical resection of heterotopic ossification around the hip joint, hip range of motion has been shown to improve from 24.3° to approximately 98.5 °. Range of motion is maintained at follow-up 6 months post-surgery. Complications from surgical resection of heterotopic ossification, such as infection, severe hematoma, and deep vein thrombosis, have been reported.[10]
Consultations
A general or orthopedic surgery consultation is appropriate once the heterotopic bone has matured. Referral is indicated when the condition causes functional limitations, including impaired mobility, reduced ability to perform self-care or activities of daily living, or difficulty for caregivers in assisting with hygiene and daily care.
Pearls and Other Issues
Key points to keep in mind regarding heterotopic ossification include:
- Heterotopic ossification is a common rehabilitation complication after joint arthroplasty, TBI, stroke, SCI, and burns.
- Prevention should be a priority for those with a high amount of identifiable risk factors.
- Risk factors include spasticity, older age, pressure ulcer, the presence of deep vein thrombosis, having a tracheostomy, long bone fractures, prior injury to the same area, edema, immobility, long-term coma, and severity of the injury.
- A triple-phase bone scan is most sensitive for detecting heterotopic ossification. Plain radiographs are specific but may not be visible until the bone has matured, which can take up to 6 weeks.
- Prevention with range of motion (ROM), control of spasticity, NSAIDs (indomethacin, COX-2 inhibitors), bisphosphonates (etidronate), and external beam radiation in joint replacement.
- Treatment with ROM, NSAIDs (SCI population), bisphosphonates (SCI and THA), and surgery (TBI population)
- Absolute treatment with surgery only after heterotopic ossification has fully matured, which can take up to 12 to 18 months.
- Current pharmacological treatment options are limited, unsafe, and only prevent the progression of the disease. A bone that has already formed can limit a person's function and still require surgical revision despite ROM exercises and pharmacological intervention. There is limited research on effective prophylactic and therapeutic options, when to initiate treatment, and the continued effectiveness of novel treatments in specific patient populations.
Enhancing Healthcare Team Outcomes
Heterotopic ossification is optimally managed through an interprofessional healthcare team. The condition is challenging to diagnose due to the absence of specific biomarkers, and available treatments remain limited in effectiveness. Current management strategies include mobilization with ROM exercises, pharmacologic therapy such as indomethacin and etidronate, and surgical resection.
Once heterotopic ossification is confirmed, early implementation of passive ROM exercises is recommended to help prevent joint ankylosis. Definitive treatment involves surgical resection of mature heterotopic bone once it has fully matured. Referral for orthopedic surgical consultation is appropriate only when meaningful functional improvement is anticipated, including gains in mobility, transfers, hygiene, and activities of daily living.
Media
(Click Image to Enlarge)
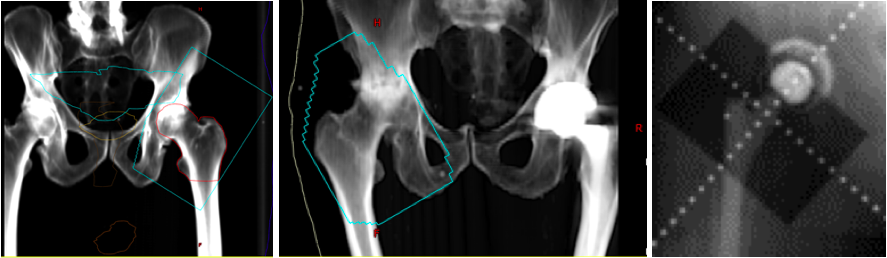
Heterotopic Ossification of the Hip. Digitally reconstructed radiographs (DRR) based on original portal images showing fields of three patients receiving radiation for heterotopic ossification of the hip. The blue line represents the field edge in the first two images. Take note that the surfaces of the greater trochanter to the ilium and the lesser trochanter to the ischium are not blocked out since this is the most common location for HO formation. The third image shows the shielding of the acetabular cup to prevent bony ingrowth and prosthesis failure.
Contributed by NP Amin, MD
(Click Image to Enlarge)

Heterotopic Ossification of the Elbow, Radiograph. Radiographs are specific for heterotopic ossification but not sensitive in early disease. Plain films may not be positive until 3 to 4 weeks after heterotopic ossification is detected on a bone scan.
Contributed by Eric Sun, DO
(Click Image to Enlarge)

Heterotopic Ossification, Radiograph. Radiographs are specific for heterotopic ossification but not sensitive in early disease. Plain films may not be positive until 3 to 4 weeks after heterotopic ossification is detected on a bone scan.
Contributed by O Chaigasame, MD
References
Ranganathan K, Loder S, Agarwal S, Wong VW, Forsberg J, Davis TA, Wang S, James AW, Levi B. Heterotopic Ossification: Basic-Science Principles and Clinical Correlates. The Journal of bone and joint surgery. American volume. 2015 Jul 1:97(13):1101-11. doi: 10.2106/JBJS.N.01056. Epub [PubMed PMID: 26135077]
Kayani B, Wignadasan W, Fontalis A, Haddad FS. Challenges and advances in the management of heterotopic ossification in total hip arthroplasty. Bone & joint research. 2025 Apr 16:14(4):351-355. doi: 10.1302/2046-3758.144.BJR-2024-0323.R1. Epub 2025 Apr 16 [PubMed PMID: 40235394]
Level 3 (low-level) evidenceKaplan FS, Glaser DL, Hebela N, Shore EM. Heterotopic ossification. The Journal of the American Academy of Orthopaedic Surgeons. 2004 Mar-Apr:12(2):116-25 [PubMed PMID: 15089085]
Pignolo RJ, Shore EM, Kaplan FS. Fibrodysplasia ossificans progressiva: clinical and genetic aspects. Orphanet journal of rare diseases. 2011 Dec 1:6():80. doi: 10.1186/1750-1172-6-80. Epub 2011 Dec 1 [PubMed PMID: 22133093]
Shehab D, Elgazzar AH, Collier BD. Heterotopic ossification. Journal of nuclear medicine : official publication, Society of Nuclear Medicine. 2002 Mar:43(3):346-53 [PubMed PMID: 11884494]
Iorio R, Healy WL. Heterotopic ossification after hip and knee arthroplasty: risk factors, prevention, and treatment. The Journal of the American Academy of Orthopaedic Surgeons. 2002 Nov-Dec:10(6):409-16 [PubMed PMID: 12470043]
Medina A, Shankowsky H, Savaryn B, Shukalak B, Tredget EE. Characterization of heterotopic ossification in burn patients. Journal of burn care & research : official publication of the American Burn Association. 2014 May-Jun:35(3):251-6. doi: 10.1097/BCR.0b013e3182957768. Epub [PubMed PMID: 23872497]
Yeung P, Zarnett O, Lefaivre KA, Guy P. Risk Factors for the Development of Heterotopic Ossification Following Acetabular Fractures: A Systematic Review. JBJS reviews. 2022 Sep 1:10(9):. doi: 10.2106/JBJS.RVW.20.00263. Epub 2022 Sep 22 [PubMed PMID: 36137013]
Level 1 (high-level) evidenceCipriano CA, Pill SG, Keenan MA. Heterotopic ossification following traumatic brain injury and spinal cord injury. The Journal of the American Academy of Orthopaedic Surgeons. 2009 Nov:17(11):689-97 [PubMed PMID: 19880679]
Yoon BH, Park IK, Sung YB. Ankylosing Neurogenic Myositis Ossificans of the Hip: A Case Series and Review of Literature. Hip & pelvis. 2018 Jun:30(2):86-91. doi: 10.5371/hp.2018.30.2.86. Epub 2018 Jun 4 [PubMed PMID: 29896457]
Level 2 (mid-level) evidenceRossier AB, Bussat P, Infante F, Zender R, Courvoisier B, Muhelm G, Donath A, Vasey H, Taillard W, Lagier R, Gabbiani G, Baud CA, Pouezat JA, Very JM, Hachen HJ. Current facts of para-osteo-arthropathy (POA). Paraplegia. 1973 May:11(1):38-78 [PubMed PMID: 4576824]
Lemos DR, Babaeijandaghi F, Low M, Chang CK, Lee ST, Fiore D, Zhang RH, Natarajan A, Nedospasov SA, Rossi FM. Nilotinib reduces muscle fibrosis in chronic muscle injury by promoting TNF-mediated apoptosis of fibro/adipogenic progenitors. Nature medicine. 2015 Jul:21(7):786-94. doi: 10.1038/nm.3869. Epub 2015 Jun 8 [PubMed PMID: 26053624]
Tseng HW, Girard D, Alexander KA, Millard SM, Torossian F, Anginot A, Fleming W, Gueguen J, Goriot ME, Clay D, Jose B, Nowlan B, Pettit AR, Salga M, Genêt F, Bousse-Kerdilès ML, Banzet S, Lévesque JP. Spinal cord injury reprograms muscle fibroadipogenic progenitors to form heterotopic bones within muscles. Bone research. 2022 Feb 25:10(1):22. doi: 10.1038/s41413-022-00188-y. Epub 2022 Feb 25 [PubMed PMID: 35217633]
Alexander KA, Tseng HW, Lao HW, Girard D, Barbier V, Ungerer JPJ, McWhinney BC, Samuel SG, Fleming W, Winkler IG, Salga M, Genêt F, Banzet S, Ruitenberg MJ, Lévesque JP. A glucocorticoid spike derails muscle repair to heterotopic ossification after spinal cord injury. Cell reports. Medicine. 2024 Dec 17:5(12):101849. doi: 10.1016/j.xcrm.2024.101849. Epub 2024 Dec 9 [PubMed PMID: 39657663]
Salga M, Samuel SG, Tseng HW, Gatin L, Girard D, Rival B, Barbier V, Bisht K, Shatunova S, Debaud C, Winkler IG, Paquereau J, Dinh A, Genêt G, Kerever S, Abback PS, Banzet S, Genêt F, Lévesque JP, Alexander KA. Bacterial Lipopolysaccharides Exacerbate Neurogenic Heterotopic Ossification Development. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research. 2023 Nov:38(11):1700-1717. doi: 10.1002/jbmr.4905. Epub 2023 Sep 23 [PubMed PMID: 37602772]
Reznik JE, Biros E, Marshall R, Jelbart M, Milanese S, Gordon S, Galea MP. Prevalence and risk-factors of neurogenic heterotopic ossification in traumatic spinal cord and traumatic brain injured patients admitted to specialised units in Australia. Journal of musculoskeletal & neuronal interactions. 2014 Mar:14(1):19-28 [PubMed PMID: 24583537]
van Dinther M, Visser N, de Gorter DJ, Doorn J, Goumans MJ, de Boer J, ten Dijke P. ALK2 R206H mutation linked to fibrodysplasia ossificans progressiva confers constitutive activity to the BMP type I receptor and sensitizes mesenchymal cells to BMP-induced osteoblast differentiation and bone formation. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research. 2010 Jun:25(6):1208-15. doi: 10.1359/jbmr.091110. Epub [PubMed PMID: 19929436]
Shore EM, Xu M, Feldman GJ, Fenstermacher DA, Cho TJ, Choi IH, Connor JM, Delai P, Glaser DL, LeMerrer M, Morhart R, Rogers JG, Smith R, Triffitt JT, Urtizberea JA, Zasloff M, Brown MA, Kaplan FS. A recurrent mutation in the BMP type I receptor ACVR1 causes inherited and sporadic fibrodysplasia ossificans progressiva. Nature genetics. 2006 May:38(5):525-7 [PubMed PMID: 16642017]
Al-Jarallah K, Al-Saeed O, Shehab D, Dashti K, Sheikh M. Ossification of ligamentum flavum in Middle East Arabs: a hospital-based study. Medical principles and practice : international journal of the Kuwait University, Health Science Centre. 2012:21(6):529-33. doi: 10.1159/000339120. Epub 2012 Jun 8 [PubMed PMID: 22687823]
Level 2 (mid-level) evidenceMary Jiayi T, Linda P, Michael P, Hans K, Markku N, Richard J, Bo Angela W, May T, Elizabeth B, Edward C. Potential discrepancy between plain films and CT scans in Brooker classification of heterotopic ossification. The British journal of radiology. 2017 Dec:90(1080):20170263. doi: 10.1259/bjr.20170263. Epub 2017 Oct 3 [PubMed PMID: 28972793]
Citak M, Suero EM, Backhaus M, Aach M, Godry H, Meindl R, Schildhauer TA. Risk factors for heterotopic ossification in patients with spinal cord injury: a case-control study of 264 patients. Spine. 2012 Nov 1:37(23):1953-7. doi: 10.1097/BRS.0b013e31825ee81b. Epub [PubMed PMID: 22614800]
Level 2 (mid-level) evidenceKjaersgaard-Andersen P, Pedersen P, Kristensen SS, Schmidt SA, Pedersen NW. Serum alkaline phosphatase as an indicator of heterotopic bone formation following total hip arthroplasty. Clinical orthopaedics and related research. 1988 Sep:(234):102-9 [PubMed PMID: 3136963]
Level 1 (high-level) evidenceKjaersgaard-Andersen P, Schmidt SA, Pedersen NW, Kristensen SS, Pedersen P. Erythrocyte sedimentation rate and heterotopic bone formation after cemented total hip arthroplasty. Clinical orthopaedics and related research. 1989 Nov:(248):189-94 [PubMed PMID: 2509120]
Level 1 (high-level) evidenceSherman AL, Williams J, Patrick L, Banovac K. The value of serum creatine kinase in early diagnosis of heterotopic ossification. The journal of spinal cord medicine. 2003 Fall:26(3):227-30 [PubMed PMID: 14997963]
Level 2 (mid-level) evidenceDevilbiss Z, Hess M, Ho GWK. Myositis Ossificans in Sport: A Review. Current sports medicine reports. 2018 Sep:17(9):290-295. doi: 10.1249/JSR.0000000000000515. Epub [PubMed PMID: 30204632]
Song B, Sambasivan A. Utilization of Diagnostic Ultrasound in Early Detection of Heterotopic Ossification Causing Ulnar Nerve Compression. American journal of physical medicine & rehabilitation. 2021 Feb 1:100(2):e23. doi: 10.1097/PHM.0000000000001461. Epub [PubMed PMID: 32371626]
Eekhoff EMW, Botman E, Coen Netelenbos J, de Graaf P, Bravenboer N, Micha D, Pals G, de Vries TJ, Schoenmaker T, Hoebink M, Lammertsma AA, Raijmakers PGHM. [18F]NaF PET/CT scan as an early marker of heterotopic ossification in fibrodysplasia ossificans progressiva. Bone. 2018 Apr:109():143-146. doi: 10.1016/j.bone.2017.08.012. Epub 2017 Aug 18 [PubMed PMID: 28826841]
Peterson JR, Okagbare PI, De La Rosa S, Cilwa KE, Perosky JE, Eboda ON, Donneys A, Su GL, Buchman SR, Cederna PS, Wang SC, Kozloff KM, Morris MD, Levi B. Early detection of burn induced heterotopic ossification using transcutaneous Raman spectroscopy. Bone. 2013 May:54(1):28-34. doi: 10.1016/j.bone.2013.01.002. Epub 2013 Jan 11 [PubMed PMID: 23314070]
Joice M, Vasileiadis GI, Amanatullah DF. Non-steroidal anti-inflammatory drugs for heterotopic ossification prophylaxis after total hip arthroplasty: a systematic review and meta-analysis. The bone & joint journal. 2018 Jul:100-B(7):915-922. doi: 10.1302/0301-620X.100B7.BJJ-2017-1467.R1. Epub [PubMed PMID: 29954195]
Aubut JA, Mehta S, Cullen N, Teasell RW, ERABI Group, Scire Research Team. A comparison of heterotopic ossification treatment within the traumatic brain and spinal cord injured population: An evidence based systematic review. NeuroRehabilitation. 2011:28(2):151-60. doi: 10.3233/NRE-2011-0643. Epub [PubMed PMID: 21447915]
Level 1 (high-level) evidenceBrunnekreef JJ, Hoogervorst P, Ploegmakers MJ, Rijnen WH, Schreurs BW. Is etoricoxib effective in preventing heterotopic ossification after primary total hip arthroplasty? International orthopaedics. 2013 Apr:37(4):583-7. doi: 10.1007/s00264-013-1781-0. Epub 2013 Jan 29 [PubMed PMID: 23359100]
Vasileiadis GI, Sioutis IC, Mavrogenis AF, Vlasis K, Babis GC, Papagelopoulos PJ. COX-2 inhibitors for the prevention of heterotopic ossification after THA. Orthopedics. 2011 Jun:34(6):467. doi: 10.3928/01477447-20110427-23. Epub [PubMed PMID: 21661680]
Kan SL, Yang B, Ning GZ, Chen LX, Li YL, Gao SJ, Chen XY, Sun JC, Feng SQ. Nonsteroidal Anti-inflammatory Drugs as Prophylaxis for Heterotopic Ossification after Total Hip Arthroplasty: A Systematic Review and Meta-Analysis. Medicine. 2015 May:94(18):e828. doi: 10.1097/MD.0000000000000828. Epub [PubMed PMID: 25950691]
Level 1 (high-level) evidenceRuo Redda MG, De Colle C, Bianco L, Ruggieri A, Nassisi D, Rossi A, Gino E, Airaldi C. Heterotopic ossifications: role of radiotherapy as prophylactic treatment. La Radiologia medica. 2018 Jun:123(6):463-468. doi: 10.1007/s11547-018-0853-z. Epub 2018 Feb 3 [PubMed PMID: 29397526]
Popovic M, Agarwal A, Zhang L, Yip C, Kreder HJ, Nousiainen MT, Jenkinson R, Tsao M, Lam H, Milakovic M, Wong E, Chow E. Radiotherapy for the prophylaxis of heterotopic ossification: a systematic review and meta-analysis of published data. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2014 Oct:113(1):10-7. doi: 10.1016/j.radonc.2014.08.025. Epub 2014 Sep 11 [PubMed PMID: 25220370]
Level 1 (high-level) evidenceMilakovic M, Popovic M, Raman S, Tsao M, Lam H, Chow E. Radiotherapy for the prophylaxis of heterotopic ossification: A systematic review and meta-analysis of randomized controlled trials. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2015 Jul:116(1):4-9. doi: 10.1016/j.radonc.2015.05.022. Epub 2015 Jul 7 [PubMed PMID: 26163090]
Level 1 (high-level) evidenceBurd TA, Hughes MS, Anglen JO. Heterotopic ossification prophylaxis with indomethacin increases the risk of long-bone nonunion. The Journal of bone and joint surgery. British volume. 2003 Jul:85(5):700-5 [PubMed PMID: 12892193]
Level 1 (high-level) evidencePakos EE, Ioannidis JP. Radiotherapy vs. nonsteroidal anti-inflammatory drugs for the prevention of heterotopic ossification after major hip procedures: a meta-analysis of randomized trials. International journal of radiation oncology, biology, physics. 2004 Nov 1:60(3):888-95 [PubMed PMID: 15465207]
Level 1 (high-level) evidenceAnthony P, Keys H, Evarts CM, Rubin P, Lush C. Prevention of heterotopic bone formation with early post operative irradiation in high risk patients undergoing total hip arthroplasty: comparison of 10.00 Gy vs 20.00 Gy schedules. International journal of radiation oncology, biology, physics. 1987 Mar:13(3):365-9 [PubMed PMID: 3104246]
Sylvester JE, Greenberg P, Selch MT, Thomas BJ, Amstutz H. The use of postoperative irradiation for the prevention of heterotopic bone formation after total hip replacement. International journal of radiation oncology, biology, physics. 1988 Mar:14(3):471-6 [PubMed PMID: 3343154]
Gregoritch SJ, Chadha M, Pelligrini VD, Rubin P, Kantorowitz DA. Randomized trial comparing preoperative versus postoperative irradiation for prevention of heterotopic ossification following prosthetic total hip replacement: preliminary results. International journal of radiation oncology, biology, physics. 1994 Aug 30:30(1):55-62 [PubMed PMID: 8083129]
Level 3 (low-level) evidenceRobinson CG, Polster JM, Reddy CA, Lyons JA, Evans PJ, Lawton JN, Graham TJ, Suh JH. Postoperative single-fraction radiation for prevention of heterotopic ossification of the elbow. International journal of radiation oncology, biology, physics. 2010 Aug 1:77(5):1493-9. doi: 10.1016/j.ijrobp.2009.06.072. Epub [PubMed PMID: 20637977]
Level 2 (mid-level) evidenceStrauss JB, Wysocki RW, Shah A, Chen SS, Shah AP, Abrams RA, Cohen MS. Radiation therapy for heterotopic ossification prophylaxis afer high-risk elbow surgery. American journal of orthopedics (Belle Mead, N.J.). 2011 Aug:40(8):400-5 [PubMed PMID: 22016869]
Level 2 (mid-level) evidenceHeyd R, Strassmann G, Schopohl B, Zamboglou N. Radiation therapy for the prevention of heterotopic ossification at the elbow. The Journal of bone and joint surgery. British volume. 2001 Apr:83(3):332-4 [PubMed PMID: 11341414]
Mourad WF, Packianathan S, Shourbaji RA, Russell G, Khan MA, Vijayakumar S. Radiation-induced sarcoma following radiation prophylaxis of heterotopic ossification. Practical radiation oncology. 2012 Apr-Jun:2(2):151-4. doi: 10.1016/j.prro.2011.06.005. Epub 2011 Jul 22 [PubMed PMID: 24674090]
Farris MK, Chowdhry VK, Lemke S, Kilpatrick M, Lacombe M. Osteosarcoma following single fraction radiation prophylaxis for heterotopic ossification. Radiation oncology (London, England). 2012 Aug 21:7():140. doi: 10.1186/1748-717X-7-140. Epub 2012 Aug 21 [PubMed PMID: 22908888]
Level 3 (low-level) evidenceBalboni TA, Gobezie R, Mamon HJ. Heterotopic ossification: Pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. International journal of radiation oncology, biology, physics. 2006 Aug 1:65(5):1289-99 [PubMed PMID: 16863921]
Seegenschmiedt MH, Keilholz L, Martus P, Goldmann A, Wölfel R, Henning F, Sauer R. Prevention of heterotopic ossification about the hip: final results of two randomized trials in 410 patients using either preoperative or postoperative radiation therapy. International journal of radiation oncology, biology, physics. 1997 Aug 1:39(1):161-71 [PubMed PMID: 9300751]
Level 1 (high-level) evidencePatel H, Silverman CL, Carrascosa L, Malkani A, Yashar CM. Evaluation of scrotal and testicular radiation doses for heterotopic ossification prophylaxis. American journal of orthopedics (Belle Mead, N.J.). 2008 Sep:37(9):E163-6 [PubMed PMID: 18982191]
Della Valle AG, Ruzo PS, Pavone V, Tolo E, Mintz DN, Salvati EA. Heterotopic ossification after total hip arthroplasty: a critical analysis of the Brooker classification and proposal of a simplified rating system. The Journal of arthroplasty. 2002 Oct:17(7):870-5 [PubMed PMID: 12375245]
Level 2 (mid-level) evidenceBehery OA, Dai AZ, McLaurin TM. Posttraumatic Heterotopic Ossification of the Hip. Journal of orthopaedic trauma. 2018 Aug:32 Suppl 1():S18-S19. doi: 10.1097/BOT.0000000000001197. Epub [PubMed PMID: 29985897]