Introduction
Varicella-zoster virus (VZV), also known as human herpesvirus 3, is the causative agent of chickenpox (varicella) and shingles (herpes zoster). VZV is a neurotropic human herpes virus belonging to the Alphaherpesvirinae subfamily.[1] Herpes zoster is a viral disease caused by reactivation of VZV, which remains dormant in the sensory ganglia of the cranial nerves or the dorsal root ganglia after a previous varicella infection. VZV latency is largely controlled by cell-mediated immunity, and reactivation is thought to result from the loss of this immune surveillance.[2][3][4]
The incidence of herpes zoster is strongly correlated with immune status. Individuals with high immunity levels rarely develop shingles. Even after herpes zoster resolves, many patients continue to experience moderate to severe pain known as postherpetic neuralgia.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
After reactivation, the virus replicates in neuronal cell bodies, and virions are shed from the cells and are carried down the nerve to the area of skin innervated by that ganglion. In the skin, the virus causes local inflammation and blistering. The pain caused by zoster results from virus-associated inflammation of affected nerves.[5][6][7]
Triggers for herpes zoster include:
- Emotional stress
- Immunosuppressive medications
- Acute or chronic illness
- Re-exposure to the varicella zoster virus
- Presence of a malignant neoplasm
Epidemiology
The incidence of herpes zoster ranges from 1.2 to 3.4 per 1000 persons per year among younger healthy individuals, whereas the incidence is 3.9 to 11.8 per 1000 persons per year among patients older than 65 years. Herpes zoster has no seasonal variation. Recurrences are most common in immunosuppressed individuals.
Pathophysiology
Cutaneous lesions of herpes zoster induce varicella-zoster virus–specific T-cell proliferation, whereas the production of interferon α leads to the resolution of herpes zoster. In immunocompetent patients, specific antibodies (IgG, IgM, and IgA) are produced more rapidly and reach higher titers during reactivation (herpes zoster) than during the primary infection, leading to long-lasting, enhanced, cell-mediated immunity to varicella-zoster virus.
The cutaneous presentation is centripetal and follows a dermatome. In most cases, the lumbar and cervical roots are involved, whereas motor involvement is rare. The infection is contagious to individuals with no prior immunity to the varicella-zoster virus; however, transmission rates are low. The virus can be transmitted either through direct skin contact or by inhaling infected droplets. Furthermore, concurrent herpesvirus infections can also occur. Herpes simplex virus, cytomegalovirus, Epstein-Barr virus, and human herpesviruses have all been identified in patients with shingles.
History and Physical
Zoster characteristically presents with a prodrome of fever, malaise, and excruciating burning pain, followed by the outbreak of vesicles that appear in 1 to 3 crops over 3 to 5 days. Lesions are distributed unilaterally within a single dermatome (see Image. Herpes Zoster). Clinically, lesions start as closely grouped erythematous papules that rapidly become vesicles on an erythematous and edematous base and may occur in continuous or interrupted bands in 1, 2, or more contiguous dermatomes unilaterally (see Image. Herpes Zoster Rash). Commonly involved dermatomes include the thoracic (53%), cervical (20%), trigeminal (15%), and lumbosacral (11%). Herpes zoster can also present with ophthalmic involvement.
The 3 phases of the infection include:
- Preeruptive stage: The preeruptive stage presents with abnormal skin sensations or pain within the affected dermatome. The preeruptive stage occurs at least 48 hours before any obvious lesions appear. At the same time, the individual may experience headaches, general malaise, and photophobia.
- Acute eruptive phase: The acute eruptive phase is marked by the vesicles and the symptoms seen in the preeruptive phase (see Image. Herpes Zoster Vesicles). The lesions initially appear as macules and quickly progress to painful vesicles. The vesicles often rupture, ulcerate, and eventually crust over. Patients are most infectious in this stage until the lesions dry out. Pain is severe during this phase and often unresponsive to traditional pain medications. The phase may last 2 to 4 weeks, but the pain may continue.
- Chronic infection: Chronic infection is characterized by recurrent pain lasting more than 4 weeks. In addition to pain, patients experience paresthesias, shock-like sensations, and dysesthesias. The pain is disabling and may last 12 months or longer.
Herpes zoster has specific presentations when the ear and mouth are involved. For example, shingles oticus is also known as Ramsay Hunt syndrome type 2. This condition results from the virus spreading from the facial nerve to the vestibulocochlear nerve, which innervates the inner ear, causing hearing loss and vertigo (rotational dizziness). Moreover, zoster may occur in the mouth if the maxillary or mandibular division of the trigeminal nerve is affected. Clinically, oral zoster presents with vesicles or erosions occurring over the mucous membrane of the upper jaw (palate and gums of the upper teeth) or the lower jaw (tongue or gums of the lower teeth). Oral involvement may occur alone or in combination with the lesions on the skin over the cutaneous distribution of the same trigeminal branch. Because of the close relationship of blood vessels to nerves, the virus can spread to involve the blood vessels, compromise the blood supply, and cause ischemic necrosis. Complications such as osteonecrosis, tooth loss, periodontitis, pulp calcification, pulp necrosis, periapical lesions, and tooth developmental anomalies can result from oral zoster.
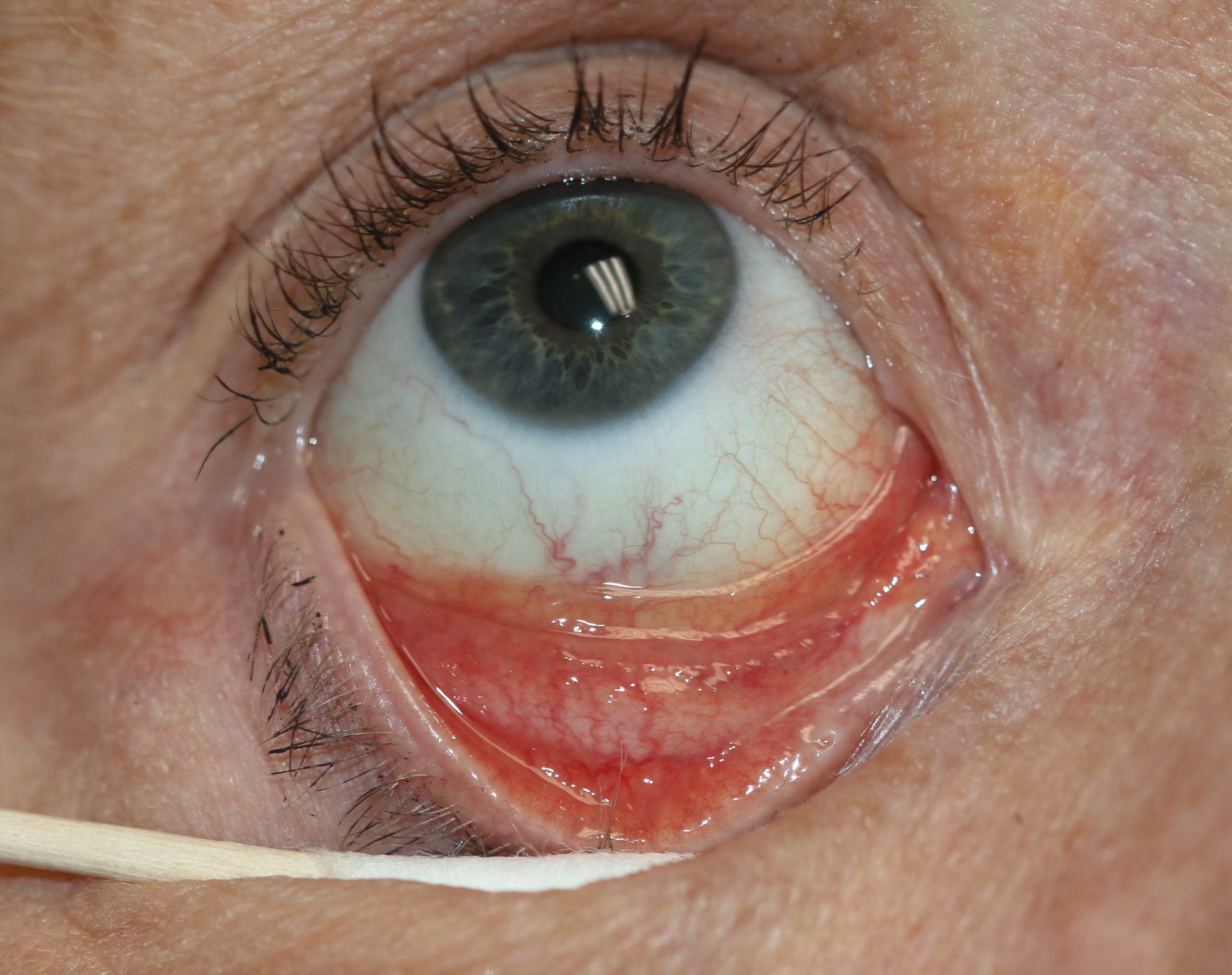
Herpes zoster can also involve the eye and central nervous system. The ophthalmic division of the trigeminal nerve is the most commonly involved branch, causing ophthalmic zoster. The skin of the forehead, upper eyelid, and orbital region may be involved (see Image. Causes of Epiphora). Ophthalmic zoster occurs in approximately 10% to 25% of cases and presents with features of keratitis, uveitis, and optic nerve palsies (see Image. Follicular Conjunctivitis). The Hutchinson eye sign is the presence of vesicles on the tip of the nose or nasal mucosa on the ipsilateral side of herpes zoster ophthalmicus infection, indicating involvement of the nasociliary branch of the ophthalmic division of the trigeminal nerve (see Image. Herpes Zoster Ophthalmicus With Hutchinson Sign). Notably, central nervous system involvement is not uncommon. Because the virus resides in the sensory root ganglia, VZV can affect any part of the brain, causing cranial nerve palsies, muscular weakness, diaphragmatic paralysis, neurogenic bladder, Guillain-Barré syndrome, and myelitis. In severe cases, patients may develop encephalitis.
Disseminated zoster is defined as more than 20 skin lesions developing outside the primarily affected area or dermatomes directly adjacent to it. In addition to the skin, other organs may also be affected, causing hepatitis or encephalitis, making this condition potentially lethal.[8] Zoster sine herpete is a condition characterized by radicular pain along a dermatomal distribution without the presence of an erythematous or vesicular rash.[9] Postherpetic neuralgia is the persistence of pain for 3 months after the onset of herpes zoster. Postherpetic neuralgia is the most common complication seen in older adults with involvement of the ophthalmic division of the trigeminal nerve. Risk factors for postherpetic neuralgia include advanced age, severe prodromal pain, severe pain during an attack, severe rash, and immunosuppression. Finally, varicella may lead to infection in the fetus during pregnancy and complications in the newborn, but chronic infection or reactivation, known as herpes zoster, is not associated with fetal infection.
Evaluation
Herpes zoster is clinically diagnosed based on burning pain, characteristic morphology, and typical distribution. Herpes simplex virus can occasionally produce a rash in a pattern called zosteriform herpes simplex.[10][11][12]
Dermatoscopy of herpes zoster consistently shows the following:
- An erythematous background, indicating increased vascularity, is the most common finding and is seen in 100% of cases.
- Round, cloudy-white polyglobular structures representing grouped vesicles are observed in 53% to 80% of patients.
- Central brown dots are present in 50% to 80% of cases and likely correlate with the crusted centers of vesicular lesions (see Image. Dermoscopic Vesicles in Herpes Zoster).
- The distinctive halo sign appears due to the contrast between the yellowish or brownish crusted centers of vesicles and the surrounding erythematous background, creating an annular pattern around each element of the rash (see Image. Dermoscopic Halo Sign in Herpes Zoster).
Dermatoscopy plays a significant role in the early diagnosis of herpes zoster, enabling diagnosis approximately 1.62 days earlier than clinical evaluation alone. These dermoscopic features assist clinicians in differentiating herpes zoster from other similar dermatologic conditions and enable earlier initiation of treatment.[13]
Tests for varicella-zoster virus include the following:
- The Tzanck smear of vesicular fluid shows multinucleated giant cells. The Tzanck smear has lower sensitivity and specificity than direct fluorescent antibody testing or polymerase chain reaction (PCR).
- Varicella-zoster virus–specific IgM antibody in blood is detected during active infection with chickenpox or shingles but not when the virus is dormant.
- Direct fluorescent antibody testing of vesicular fluid or corneal fluid can be done when eye involvement is present.
- PCR testing can be performed on vesicular fluid, corneal lesions, or blood in patients with ocular involvement or disseminated infection.
Molecular biology tests based on in vitro nucleic acid amplification (PCR tests) are currently considered the most reliable. The nested PCR test has high sensitivity but is susceptible to contamination, which can lead to false-positive results. The latest real-time PCR tests are rapid, easy to perform, associated with a lower risk of contamination, and more sensitive than viral cultures.
Treatment / Management
Antiviral therapy hastens lesion resolution, reduces acute pain, and helps prevent postherpetic neuralgia, especially in older adults. The standard therapy for herpes zoster is acyclovir and its prodrug valacyclovir. Acyclovir and valacyclovir are processed to nucleoside analogues that specifically block viral DNA replication in affected cells. Oral bioavailability of acyclovir is 10% to 30%. Approximately 15% is metabolized in the liver, whereas 85% of acyclovir is excreted unchanged by the kidney through glomerular filtration and tubular secretion. Acute crystalline nephropathy is a reversible form of acute kidney injury caused by intratubular precipitation of acyclovir crystals and obstruction; histology may show crystals in the distal tubules with patchy interstitial infiltration, without tubular necrosis.[14](B3)
Mutations in the viral thymidine kinase or DNA polymerase confer acyclovir resistance. For patients with acyclovir-resistant herpes zoster, famciclovir is an alternative. Valganciclovir is a valine ester prodrug of ganciclovir that can be administered orally, and recent findings showed activity against varicella-zoster virus.
Doses:
- Acyclovir: 800 mg, 5 times daily for 5 days
- Valacyclovir: 1 g 3 times daily for 5 days
- Famciclovir: 500 mg 3 times daily for 7 days
In immunocompromised patients, intravenous acyclovir is administered at 10 mg/kg every 8 hours for 7 days. Ideal body weight should be used for patients with obesity. Intravenous infusion is preferred over 1 hour, using a diluted 5% dextrose in water solution or 0.9% sodium chloride, to a final concentration of 7 mg/mL or less at a constant rate to prevent renal damage. Please see StatPearls' companion reference, "Acyclovir," for further information.
Topical antibiotic creams such as mupirocin or framycetin help prevent secondary bacterial infection, and analgesics help relieve pain. Occasionally, severe pain may require an opioid medication. Topical lidocaine and nerve blocks may also reduce pain.[10][15][16] (B3)
Pharmacologically, first-line systemic treatments consist of anticonvulsants such as gabapentin and pregabalin. Pregabalin, in particular, may provide faster pain relief than gabapentin, but both require careful dose titration and monitoring for adverse effects such as sedation and cognitive impairment. Tricyclic antidepressants such as amitriptyline and nortriptyline are also commonly used because of their analgesic properties; nortriptyline tends to be better tolerated. Opioids such as tramadol are considered third-line because of concerns about adverse effects and dependency. These systemic agents often require combination therapy to optimize pain control while minimizing adverse events.[17][18](B2)
Topical therapies include 5% lidocaine and 8% capsaicin patches. Lidocaine patches provide localized pain relief with minimal systemic effects, making them suitable for older adults and patients with comorbidities. Capsaicin patches, derived from chili peppers, desensitize peripheral nociceptors, with higher-concentration patches offering prolonged analgesia after a 30- to 90-min application under medical supervision.
Interventional pain treatment techniques such as the modified Jaipur block (local anesthetics combined with corticosteroids), spinal cord stimulation, and dorsal root entry zone lesioning have gained attention. These techniques are particularly helpful in refractory cases or for patients with severe neuropathic pain. The modified Jaipur block is a local subcutaneous infiltration of 2% lidocaine, 0.5% bupivacaine, and methylprednisolone. The involved dermatomes are identified, scarred areas are avoided, and areas of maximum pain are identified. At these sites, 2 mL is injected subcutaneously, with a maximum of 8-10 injections per sitting. In the original Jaipur block, the corticosteroid traditionally used was dexamethasone.[17] Additionally, nonpharmacological approaches are emerging adjunctive therapies, including frequency-specific microcurrent therapy that reduces burning and stabbing pain in patients with postherpetic neuralgia unresponsive to medications. Transcutaneous electrical nerve stimulation combined with other agents such as methylcobalamin has also demonstrated beneficial effects.(B2)
Prevention remains essential, with herpes zoster vaccination significantly lowering the incidence and severity of both herpes zoster and postherpetic neuralgia in immunocompetent older adults. The recombinant zoster vaccine (Shingrix; GlaxoSmithKline) is a subunit vaccine containing an adjuvant that the Advisory Committee on Immunization Practices recommended for use in adults 50 years or older in 2017. In October 2021, the Advisory Committee on Immunization Practices approved the recombinant zoster vaccine for preventing herpes zoster in adults 19 years or older who are or will be at an increased risk of herpes zoster due to immunodeficiency or immunosuppression caused by known diseases or therapy.[19](A1)
Differential Diagnosis
Cutaneous lesions of herpes zoster should be differentiated from herpes simplex, dermatitis herpetiformis, impetigo, contact dermatitis, candidiasis, drug reactions, and insect bites. Preceding pain without the development of skin lesions in herpes zoster should be differentiated from cholecystitis and biliary colic, renal colic, trigeminal neuralgia, and dental infection. Herpes zoster typically involves only 1 side of the oral cavity, distinguishing it from other oral blistering conditions. In the mouth, herpes zoster initially presents as vesicles that break down quickly, leaving ulcers that heal within 10 to 14 days. The prodromal pain before the rash may be confused with a toothache, leading to unnecessary dental treatment.
The differential diagnosis includes:
- Cellulitis
- Chickenpox
- Cnidaria envenomation
- Contact stomatitis
- Dermatologic manifestations of herpes simplex infection
- Ecthyma
- Erysipelas
- Erysipeloid
- Folliculitis
- Human cowpox infections
- Irritant contact dermatitis
- Insect bites
- Paederus dermatitis [20]
- Lichen striatus
- Mucosal candidiasis
Prognosis
Herpes zoster usually resolves within 10 to 15 days in healthy individuals and has an excellent prognosis in younger patients. However, older adults and immunocompromised individuals face significantly higher risks of complications, including severe pain and potentially life-threatening disseminated infections. The principal morbidity is postherpetic neuralgia, which can persist for months and profoundly affect quality of life. Vaccination with the recombinant zoster vaccine can reduce the incidence and severity of herpes zoster. Ultimately, outcomes are most favorable with early diagnosis and prompt initiation of antiviral therapy.
Complications
Complications include:
- Postherpetic neuralgia
- Bacterial infection
- Ocular complications, including chronic ocular inflammation, vision loss, and debilitating pain
- Ramsay Hunt syndrome
- Meningoencephalitis
- Motor paralysis
- Pneumonitis
- Hepatitis
- Aseptic meningitis
- Peripheral motor neuropathy
- Guillain-Barré syndrome
- Transverse myelitis
- Cardiac arrhythmias
- Urinary retention and hematuria
Deterrence and Patient Education
Prevention of herpes zoster focuses on vaccination, specifically the recombinant zoster vaccine (Shingrix), which is recommended for adults older than 50 years and immunocompromised individuals, as it significantly reduces the incidence of both herpes zoster and postherpetic neuralgia. Patient education should stress prompt medical attention after the appearance of erythematous vesicles and ipsilateral pain. Patients should avoid direct contact with high-risk groups, such as pregnant women, immunocompromised people, and those who have never had chickenpox. Promoting vaccine use and public awareness will help minimize disease burden and improve quality of life.
Enhancing Healthcare Team Outcomes
Shingles is a common infectious disorder in older adults with significant morbidity. The condition has no cure but can be prevented in most patients through vaccination. When eye involvement is present, patients must be referred promptly to an ophthalmologist. Healthcare professionals, including primary care clinicians, nurse practitioners, internists, and pharmacists, should educate patients on the benefits of the vaccine.[21][22]
Media
(Click Image to Enlarge)

Herpes Zoster. Herpes zoster presents as a unilateral, dermatomal vesicular eruption on an erythematous base.
(Click Image to Enlarge)

Herpes Zoster Rash. Herpes Zoster, aka shingles, typically presents with severe pain accompanied by a unilateral rash. The symptoms have a dermatomal distribution. The trunk and the face are most commonly involved.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
Follicular Conjunctivitis. Inflammation is noted with viral infections like herpes zoster, Epstein-Barr virus infection, infectious mononucleosis, and chlamydial infections, as well as in reaction to topical medications and molluscum contagiosum. Follicular conjunctivitis has been described in patients with COVID-19. The inferior and superior tarsal conjunctiva and the fornices show gray-white elevated swellings about 0.5 to 1 mm in diameter and have a velvety appearance.
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)

Causes of Epiphora. The conditions that can cause epiphora include herpes zoster with keratitis (A), lacrimal mucocele (B), corneal calcific keratopathy (C), floppy eyelid syndrome (D), kissing puncta syndrome (E), and pemphigoid disease with trichiasis and obliteration of puncta (F).
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)

Herpes Zoster Ophthalmicus With Hutchinson Sign. Herpes Zoster, aka shingles, can involve the ophthalmic division of the trigeminal nerve, resulting in herpes zoster ophthalmicus. The Hutchinson sign, or herpetic lesions in the nasal area, may precede this condition.
(Click Image to Enlarge)

Herpes Zoster Vesicles. Herpes zoster commonly presents as grouped vesicles on an erythematous base in a unilateral dermatomal distribution.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
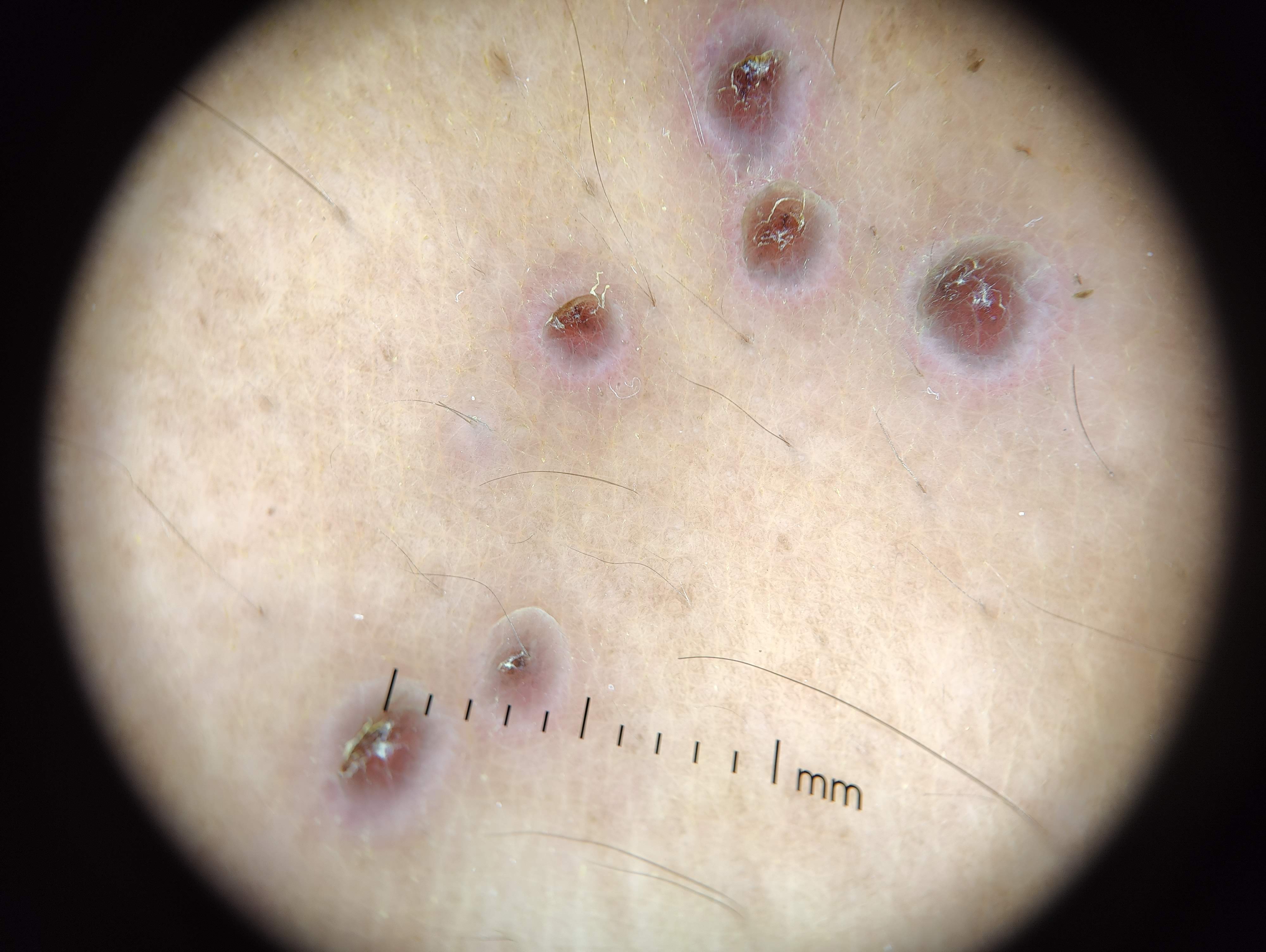
Dermoscopic Halo Sign in Herpes Zoster. Dermoscopy of herpes zoster may show crusted vesicles with central brown dots surrounded by erythema, creating the characteristic halo sign.
Contributed by M Shah, MD
(Click Image to Enlarge)
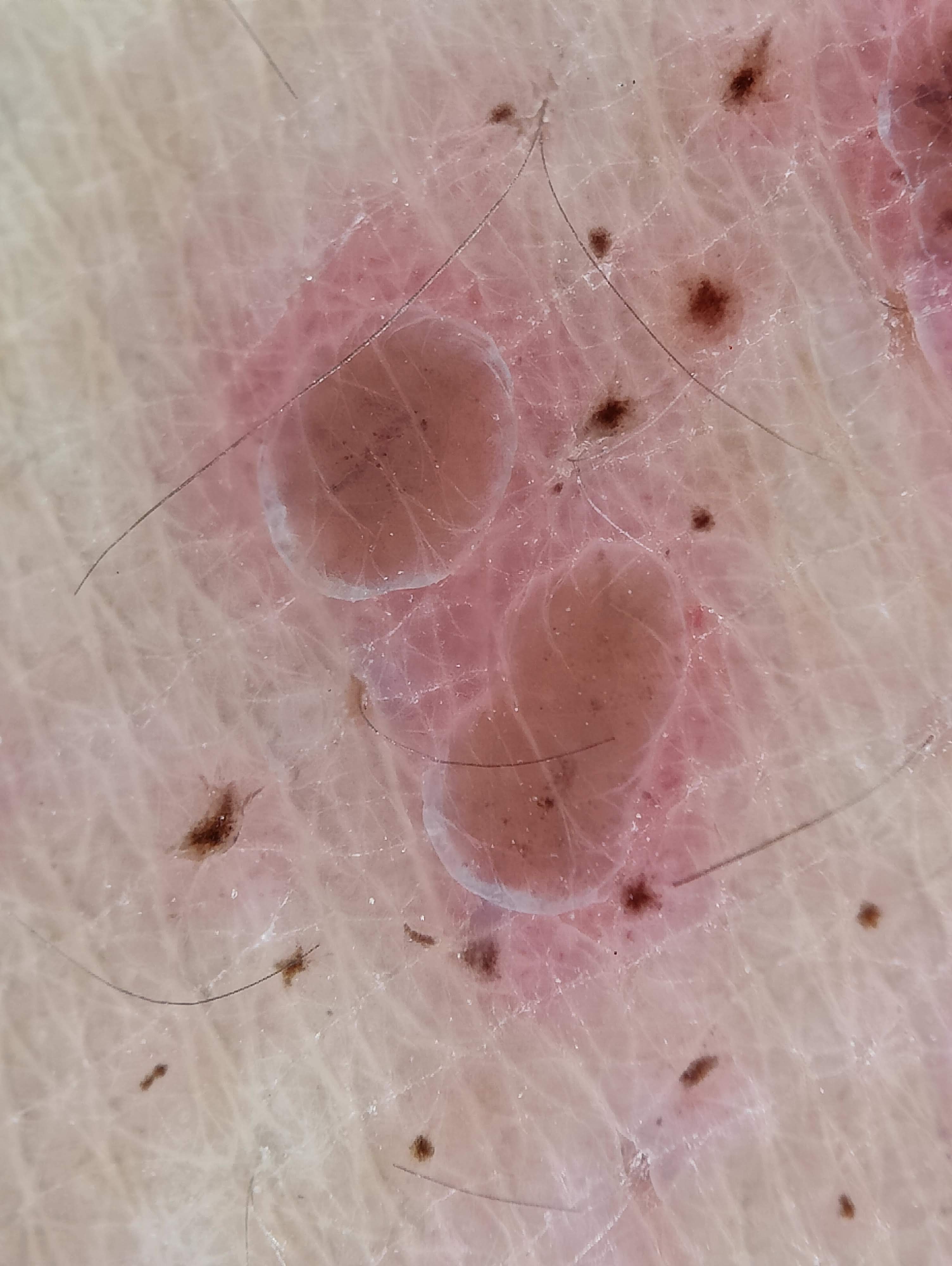
Dermoscopic Vesicles in Herpes Zoster. Dermoscopy of herpes zoster may show round, cloudy white polyglobular structures corresponding to grouped vesicles, along with central brown dots that correlate with crusted vesicular centers.
Contributed by M Shah, MD
References
Patil A, Goldust M, Wollina U. Herpes zoster: A Review of Clinical Manifestations and Management. Viruses. 2022 Jan 19:14(2):. doi: 10.3390/v14020192. Epub 2022 Jan 19 [PubMed PMID: 35215786]
Heineman TC, Cunningham A, Levin M. Understanding the immunology of Shingrix, a recombinant glycoprotein E adjuvanted herpes zoster vaccine. Current opinion in immunology. 2019 Aug:59():42-48. doi: 10.1016/j.coi.2019.02.009. Epub 2019 Apr 17 [PubMed PMID: 31003070]
Level 3 (low-level) evidenceWatanabe D. [Cutaneous Herpesvirus Infection]. Brain and nerve = Shinkei kenkyu no shinpo. 2019 Apr:71(4):302-308. doi: 10.11477/mf.1416201266. Epub [PubMed PMID: 30988211]
Yu YH, Lin Y, Sun PJ. Segmental zoster abdominal paresis mimicking an abdominal hernia: A case report and literature review. Medicine. 2019 Apr:98(15):e15037. doi: 10.1097/MD.0000000000015037. Epub [PubMed PMID: 30985652]
Level 3 (low-level) evidenceSenderovich H, Grewal J, Mujtaba M. Herpes zoster vaccination efficacy in the long-term care facility population: a qualitative systematic review. Current medical research and opinion. 2019 Aug:35(8):1451-1462. doi: 10.1080/03007995.2019.1600482. Epub 2019 Apr 23 [PubMed PMID: 30913912]
Level 2 (mid-level) evidenceWarren-Gash C, Forbes HJ, Williamson E, Breuer J, Hayward AC, Mavrodaris A, Ridha BH, Rossor MN, Thomas SL, Smeeth L. Human herpesvirus infections and dementia or mild cognitive impairment: a systematic review and meta-analysis. Scientific reports. 2019 Mar 18:9(1):4743. doi: 10.1038/s41598-019-41218-w. Epub 2019 Mar 18 [PubMed PMID: 30894595]
Level 1 (high-level) evidenceDavis AR, Sheppard J. Herpes Zoster Ophthalmicus Review and Prevention. Eye & contact lens. 2019 Sep:45(5):286-291. doi: 10.1097/ICL.0000000000000591. Epub [PubMed PMID: 30844951]
Moon YS, Cho WJ, Jung YS, Lee JS. Disseminated Zoster Involving the Whole Body in an Immunocompetent Patient Complaining of Left Leg Radiating Pain and Weakness: A Case Report and Literature Review. Geriatric orthopaedic surgery & rehabilitation. 2022:13():21514593221119619. doi: 10.1177/21514593221119619. Epub 2022 Aug 10 [PubMed PMID: 35983318]
Level 3 (low-level) evidenceYoon SH, Shetty-Das R. Zoster Sine Herpete: Confirmatory Diagnosis Using Varicella-Zoster Virus DNA Polymerase Chain Reaction Analysis of Intact Skin Scrapings. Cureus. 2023 Jul:15(7):e41965. doi: 10.7759/cureus.41965. Epub 2023 Jul 16 [PubMed PMID: 37588338]
Baumrin E, Van Voorhees A, Garg A, Feldman SR, Merola JF. A systematic review of herpes zoster incidence and consensus recommendations on vaccination in adult patients on systemic therapy for psoriasis or psoriatic arthritis: From the Medical Board of the National Psoriasis Foundation. Journal of the American Academy of Dermatology. 2019 Jul:81(1):102-110. doi: 10.1016/j.jaad.2019.03.017. Epub 2019 Mar 15 [PubMed PMID: 30885757]
Level 3 (low-level) evidenceMiles LW, Williams N, Luthy KE, Eden L. Adult Vaccination Rates in the Mentally Ill Population: An Outpatient Improvement Project. Journal of the American Psychiatric Nurses Association. 2020 Mar/Apr:26(2):172-180. doi: 10.1177/1078390319831763. Epub 2019 Mar 13 [PubMed PMID: 30866701]
Rooney BV, Crucian BE, Pierson DL, Laudenslager ML, Mehta SK. Herpes Virus Reactivation in Astronauts During Spaceflight and Its Application on Earth. Frontiers in microbiology. 2019:10():16. doi: 10.3389/fmicb.2019.00016. Epub 2019 Feb 7 [PubMed PMID: 30792698]
Bazzacco G, Conforti C, Toffoli L, Zelin E, Zalaudek I, di Meo N. Dermoscopic Features of Herpes Zoster: Case Series and Review of the Literature. Dermatology practical & conceptual. 2023 Jul 1:13(3):. doi: 10.5826/dpc.1303a149. Epub 2023 Jul 1 [PubMed PMID: 37557161]
Level 2 (mid-level) evidenceKenzaka T, Sugimoto K, Goda K, Akita H. Acute kidney injury and acyclovir-associated encephalopathy after administration of valacyclovir in an elderly person with normal renal function: A case report and literature review. Medicine. 2021 May 28:100(21):e26147. doi: 10.1097/MD.0000000000026147. Epub [PubMed PMID: 34032768]
Level 3 (low-level) evidenceHurley LP, Allison MA, Dooling KL, O'Leary ST, Crane LA, Brtnikova M, Beaty BL, Allen JA, Guo A, Lindley MC, Kempe A. Primary care physicians' experience with zoster vaccine live (ZVL) and awareness and attitudes regarding the new recombinant zoster vaccine (RZV). Vaccine. 2018 Nov 19:36(48):7408-7414. doi: 10.1016/j.vaccine.2018.09.018. Epub 2018 Oct 26 [PubMed PMID: 30420121]
Syed YY. Recombinant Zoster Vaccine (Shingrix(®)): A Review in Herpes Zoster. Drugs & aging. 2018 Dec:35(12):1031-1040. doi: 10.1007/s40266-018-0603-x. Epub [PubMed PMID: 30370455]
Sharma RK, Gupta M, Tegta GR, Verma G, Rani R. Post Herpetic Neuralgia: A Retrospective Study to Evaluate Response to Modified Jaipur Block with Increased Concentration of Dexamethasone. Indian journal of dermatology. 2021 Sep-Oct:66(5):459-464. doi: 10.4103/ijd.IJD_390_20. Epub [PubMed PMID: 35068498]
Level 2 (mid-level) evidenceLim DZJ, Tey HL, Salada BMA, Oon JEL, Seah ED, Chandran NS, Pan JY. Herpes Zoster and Post-Herpetic Neuralgia-Diagnosis, Treatment, and Vaccination Strategies. Pathogens (Basel, Switzerland). 2024 Jul 17:13(7):. doi: 10.3390/pathogens13070596. Epub 2024 Jul 17 [PubMed PMID: 39057822]
Xia Y, Zhang X, Zhang L, Fu C. Efficacy, effectiveness, and safety of herpes zoster vaccine in the immunocompetent and immunocompromised subjects: A systematic review and network meta-analysis. Frontiers in immunology. 2022:13():978203. doi: 10.3389/fimmu.2022.978203. Epub 2022 Sep 30 [PubMed PMID: 36248796]
Level 1 (high-level) evidenceTamilselvan B, Shanmugam S, Shakthi P. A Case Series of Paederus Dermatitis: Understanding Its Varied and Diverse Clinical Presentations. Cureus. 2024 Feb:16(2):e54148. doi: 10.7759/cureus.54148. Epub 2024 Feb 13 [PubMed PMID: 38496106]
Level 2 (mid-level) evidenceMospan CM, Colvin N. What are the new vaccination recommendations for herpes zoster? JAAPA : official journal of the American Academy of Physician Assistants. 2018 Oct:31(10):14-15. doi: 10.1097/01.JAA.0000545079.16968.0e. Epub [PubMed PMID: 30252758]
Hawkins KL, Gordon KS, Levin MJ, Weinberg A, Battaglia C, Rodriguez-Barradas MC, Brown ST, Rimland D, Justice A, Tate J, Erlandson KM, VACS Project Team. Herpes Zoster and Herpes Zoster Vaccine Rates Among Adults Living With and Without HIV in the Veterans Aging Cohort Study. Journal of acquired immune deficiency syndromes (1999). 2018 Dec 1:79(4):527-533. doi: 10.1097/QAI.0000000000001846. Epub [PubMed PMID: 30179984]