Introduction
Herpangina is an acute viral infection that primarily affects infants and young children and is most commonly caused by coxsackievirus A and other enteroviruses. Herpangina is characterized by the sudden onset of fever, sore throat, and small vesicular or ulcerative lesions in the posterior oropharynx, particularly the soft palate and tonsillar pillars. The disease occurs most frequently during the summer and early fall and spreads through fecal-oral and respiratory routes, especially in childcare and school settings. Although herpangina is usually self-limited, early recognition is important to ensure appropriate supportive treatment and to prevent unnecessary antibiotic use. Although herpangina is primarily a pediatric disease, rare cases have also been reported in neonates, adolescents, and adults.[1][2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Herpangina is primarily caused by viruses belonging to the genus Enterovirus within the family Picornaviridae. The most common causative agents are coxsackievirus A, particularly serotypes A1 to A10 and A16, although other enteroviruses such as coxsackievirus B and echovirus have also been implicated. These viruses are nonenveloped, single-stranded RNA viruses that replicate in the gastrointestinal tract and are transmitted primarily through fecal–oral and respiratory routes. Following entry into the host, viral replication occurs in the lymphoid tissues of the oropharynx and intestinal mucosa, leading to viremia and the development of the characteristic vesicular lesions in the posterior oropharynx.[4] Enterovirus B group serotypes, including B3, have also been implicated in epidemic clusters, demonstrating that multiple enterovirus lineages can produce the characteristic vesicular pharyngitis seen in herpangina.[5]
Epidemiology
Herpangina occurs worldwide but is most commonly seen in infants and young children, particularly those younger than 10 years. In the US, infections caused by enteroviruses typically show a seasonal pattern, with cases peaking during the summer and early fall. Transmission occurs through fecal-oral spread, respiratory droplets, and close contact, which facilitates outbreaks in childcare centers, schools, and other community settings. Surveillance studies in the US and other countries have identified several circulating serotypes, including coxsackievirus A serotypes A2, A4, A6, and A10, as well as other nonpolio enteroviruses, which vary by year and geographic region. Recent surveillance data suggest that patterns of enterovirus circulation may fluctuate following changes in public health measures during the COVID-19 pandemic.[6][7][8]
Pathophysiology
Herpangina is caused by nonpolio enteroviruses, primarily coxsackievirus A serotypes, which enter the host via the oral or respiratory route. The virus replicates in the lymphoid tissue of the oropharynx and intestinal mucosa, leading to viremia and subsequent development of the characteristic vesicular or ulcerative lesions in the posterior oropharynx. Infection also triggers a host immune response, resulting in systemic symptoms such as fever, malaise, and sore throat.[6][7][8]
History and Physical
History
Children with herpangina usually present with a sudden onset of fever, sore throat, irritability, and decreased appetite. Some may also report headache, malaise, or mild abdominal discomfort. The illness often develops rapidly over 1 to 2 days, and outbreaks commonly occur during the summer and early fall. A recent history of exposure to other children with similar symptoms in childcare or school settings is common. Older children may report back pain and headache, and some patients may develop anorexia, dehydration, or abdominal pain. Depending on severity and organ system involvement, patients may also report headaches, neck stiffness, confusion, seizures, muscle weakness, or difficulty breathing.
Physical Examination
On examination, small vesicles or shallow ulcers are seen in the posterior oropharynx, including the soft palate, tonsillar pillars, and uvula, while the anterior oral cavity is usually spared. Cervical lymphadenopathy may be mild, and patients may appear irritable or lethargic due to fever. Other findings are generally minimal, and systemic involvement is rare, making the diagnosis largely clinical, based on characteristic lesions and seasonal presentation.[Merck Manual. Herpangina][Medscape. Herpangina]
The occurrence and characteristics of the rash may vary by viral subtype. Neurologic findings, such as neck stiffness or paralysis, may be present in cases complicated by meningitis, acute flaccid paralysis, encephalitis, or encephalomyelitis. Dehydration is a common complication, with signs such as dry mouth and decreased skin turgor. The history and physical examination should also focus on ruling out other serious febrile exanthems, including Kawasaki disease, Rocky Mountain spotted fever, eczema herpeticum, and toxic shock syndrome, which can present similarly.
Evaluation
The diagnosis of herpangina is primarily clinical, based on history and characteristic posterior oropharyngeal vesicular or ulcerative lesions; routine laboratory tests are often unnecessary in uncomplicated cases. Laboratory evaluation may include a complete blood count and basic metabolic panel to assess for dehydration or alternative diagnoses, but test results are usually normal. Confirmatory testing is reserved for complicated diseases, outbreaks, or epidemiologic purposes; reverse transcription polymerase chain reaction for nonpolio enteroviruses from throat swabs, stool, cerebrospinal fluid, or vesicular fluid is the preferred method because of high sensitivity and rapid turnaround. Viral culture and paired serology, showing a 4-fold rise in antibody titers, are used less commonly. Imaging and additional studies, (eg, lumbar puncture or central nervous system imaging), may be indicated if clinicians are concerned about complications such as aseptic meningitis, encephalitis, or acute flaccid paralysis.[Medscape. Herpangina]
Treatment / Management
Herpangina is typically a self-limited viral illness, and treatment is primarily supportive, focusing on symptom relief, hydration, and prevention of complications. Treatment can be broadly categorized into general care, symptomatic treatment, and antiviral therapy considerations.
General
Patients should have a well-ventilated and clean environment to reduce the risk of transmission. General supportive care includes maintaining adequate hydration and proper nutrition. Children should be encouraged to consume light, soft, or semiliquid foods to ensure adequate caloric intake, while avoiding hot, spicy, or irritating foods that may aggravate oral lesions.
Maintaining good oral hygiene is also important. Patients may rinse their mouths with normal saline after meals, while younger children who are unable to rinse may have their oral cavity gently wiped with saline-soaked gauze. If normal saline is unavailable, mildly salted water can be used as an alternative. Adequate oral fluid intake should be emphasized, particularly in children with fever or reduced oral intake. For those with significant feeding difficulties or at risk of dehydration, oral rehydration solutions containing electrolytes are recommended. Patients should be monitored for signs of dehydration or worsening symptoms during the illness.[9](B3)
Symptomatic
Fever is one of the most common symptoms associated with herpangina. For children with temperatures of 38.5 °C (101.3 °F) or higher, antipyretic medications such as acetaminophen or ibuprofen may be administered according to age-appropriate dosing recommendations. Adequate hydration should be maintained while using these medications.
Nonpharmacologic measures such as cool compresses or tepid sponging may also provide additional comfort. Topical anesthetic preparations containing lidocaine or diphenhydramine are generally not recommended for the treatment of oral lesions in herpangina because of limited evidence of benefit and the potential risk of systemic toxicity in young children. In rare cases, younger children with high fever may develop febrile seizures, which require prompt treatment according to standard pediatric seizure protocols. Benzodiazepines such as intravenous midazolam may be used when clinically indicated.[9](B3)
Antiviral
Currently, no specific antiviral therapy is recommended for the routine treatment of herpangina. Supportive care remains the primary treatment approach. Results from some studies suggest that interferon-alfa spray may have benefits through local immunomodulatory and antiviral effects on mucosal immunity, although its routine use remains limited and the evidence is not yet sufficient to support widespread recommendation.[6]
Differential Diagnosis
Herpangina may present with symptoms overlapping with those of several infectious and inflammatory pediatric conditions. Careful clinical evaluation, including the distribution of oral lesions, associated systemic findings, and the characteristics of the rash, is important for distinguishing herpangina from other illnesses (see Image. Differential Diagnoses for Pediatric Oral Lesions). Diseases and conditions that should be considered in the differential diagnosis include:
- Eczema herpeticum
- Toxic shock syndrome
- Measles
- Varicella
- Kawasaki disease
- Insect bites or hypersensitivity reactions
- Rocky Mountain spotted fever
- Drug eruption or medication-related hypersensitivity reactions
- Erythema multiforme major
These conditions may present with fever, mucocutaneous lesions, or a rash that can resemble the clinical manifestations of herpangina. However, distinguishing features such as lesion distribution, systemic involvement, epidemiologic exposure, and laboratory findings help establish the correct diagnosis.
Prognosis
Herpangina is usually a mild illness that resolves spontaneously. With proper care, isolation, good nutrition, and adequate hydration, most children recover within about 10 days. Treatment mainly focuses on relieving fever and mouth pain, and young children with high fever should be monitored closely for febrile seizures. In rare cases, serious complications such as flaccid paralysis, meningitis, encephalitis, or myocarditis can occur, so patients should be monitored carefully for any warning signs.
Complications
Herpangina is usually a mild illness, but some viruses that cause it, especially enterovirus 71, can lead to serious complications. Complications may include brainstem encephalitis, acute flaccid paralysis, aseptic meningitis, and myocarditis. Patients who develop these complications can become very ill and often require hospitalization, and in some cases, care in the intensive care unit.
Deterrence and Patient Education
Families should be informed that herpangina is usually a mild illness that resolves spontaneously. Because herpangina commonly affects children and may cause concern for parents, reassurance and clear guidance are important. Caregivers should be advised to keep the child isolated in a well-ventilated room until symptoms improve and to ensure adequate hydration and proper nutrition.
Good hygiene is essential to prevent the spread of infection. Frequent handwashing should be encouraged, especially after changing diapers, feeding the child, or handling items the child has used. Cleaning and disinfecting surfaces and objects the child frequently touches is also recommended. Although most children can be treated at home, caregivers should stay in contact with the clinician and watch for any worsening symptoms. Follow-up visits are usually not necessary because the illness typically resolves quickly.
Enhancing Healthcare Team Outcomes
Herpangina is usually a mild viral infection, but in rare cases, it can cause serious complications. Diagnosis is mainly based on clinical symptoms, with additional tests reserved for unclear cases. Effective treatment of herpangina relies on strong teamwork among healthcare professionals. Clinicians, nurses, advanced practitioners, and pharmacists must communicate clearly about the patient’s condition, treatment plan, and any warning signs of complications. Coordinating care ensures that families receive consistent guidance on symptom treatment, hydration, nutrition, and infection prevention. Ethical practice, attention to patient safety, and shared responsibility help improve outcomes and reduce stress for both patients and families. Regular updates and collaboration among the interprofessional team enhance overall team performance and patient-centered care.
Media
(Click Image to Enlarge)
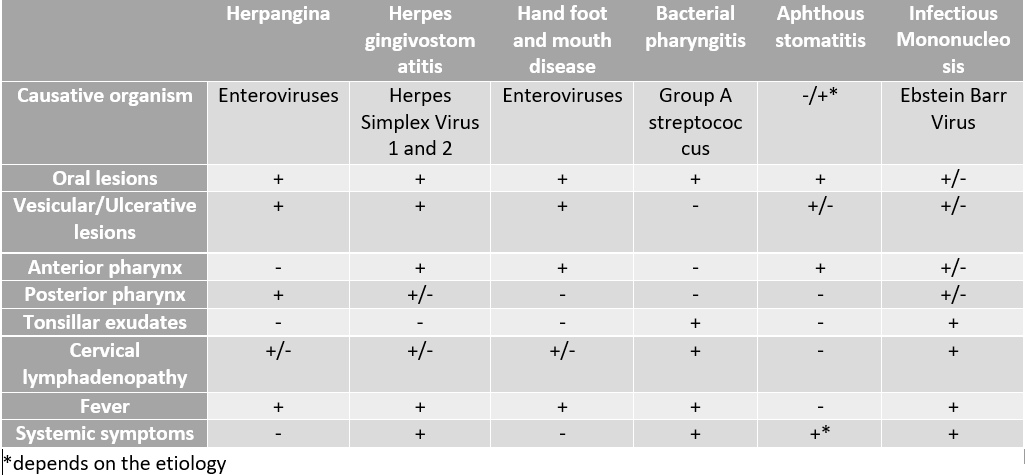
Differential Diagnoses for Pediatric Oral Lesions. This table outlines the causative agents and characteristic clinical features used to differentiate between common pediatric conditions presenting with oral lesions.
Contributed by R Ali, MD
References
Esposito S, Principi N. Hand, foot and mouth disease: current knowledge on clinical manifestations, epidemiology, aetiology and prevention. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology. 2018 Mar:37(3):391-398. doi: 10.1007/s10096-018-3206-x. Epub 2018 Feb 6 [PubMed PMID: 29411190]
Freeman MC, Messacar K. Enterovirus and Parechovirus Neurologic Infections in Children: Clinical Presentations and Neuropathogenesis. Journal of the Pediatric Infectious Diseases Society. 2025 Jan 20:14(1):. pii: piae069. doi: 10.1093/jpids/piae069. Epub [PubMed PMID: 39776161]
Solomon T, Lewthwaite P, Perera D, Cardosa MJ, McMinn P, Ooi MH. Virology, epidemiology, pathogenesis, and control of enterovirus 71. The Lancet. Infectious diseases. 2010 Nov:10(11):778-90. doi: 10.1016/S1473-3099(10)70194-8. Epub 2010 Oct 18 [PubMed PMID: 20961813]
Xing B, Hu L, Hu X, Sun Y, Liang Z, Fu J, Liang Y, Chen Y, Li Y, Chen L, Wang L, Wang W, Lu Y, Wang S. Epidemiological, clinical, and molecular characteristics of coxsackievirus A2 infections during a herpangina outbreak in children on an Island in Eastern China in 2024: a surveillance-based study. Gut pathogens. 2025 Nov 4:17(1):85. doi: 10.1186/s13099-025-00762-9. Epub 2025 Nov 4 [PubMed PMID: 41189016]
Level 2 (mid-level) evidenceNakayama T, Urano T, Osano M, Hayashi Y, Sekine S, Ando T, Makinom S. Outbreak of herpangina associated with Coxsackievirus B3 infection. The Pediatric infectious disease journal. 1989 Aug:8(8):495-8 [PubMed PMID: 2549494]
Abzug MJ. The enteroviruses: problems in need of treatments. The Journal of infection. 2014 Jan:68 Suppl 1():S108-14. doi: 10.1016/j.jinf.2013.09.020. Epub 2013 Oct 8 [PubMed PMID: 24119825]
Pons-Salort M, Grassly NC. Serotype-specific immunity explains the incidence of diseases caused by human enteroviruses. Science (New York, N.Y.). 2018 Aug 24:361(6404):800-803. doi: 10.1126/science.aat6777. Epub [PubMed PMID: 30139872]
Chen J, You P, Li Y, Chen X, Zhang N, Ma C, Zhang Y, Lv T. Molecular epidemiology and genetic characteristics of enterovirus A identified in pediatric patients with hand, foot, and mouth disease and herpangina in Linyi, China, 2023-2024, following the relaxation of COVID-19 policies. BMC infectious diseases. 2026 Jan 29:26(1):. doi: 10.1186/s12879-026-12710-2. Epub 2026 Jan 29 [PubMed PMID: 41612251]
Sawyer MH. Enterovirus infections: diagnosis and treatment. Current opinion in pediatrics. 2001 Feb:13(1):65-9 [PubMed PMID: 11176247]
Level 3 (low-level) evidence