Introduction
Hepatorenal syndrome (HRS) is a multiorgan condition that affects both the kidneys and the liver.[1] This disease is a cause of acute kidney injury that can occur in patients with decompensated cirrhosis. Portal hypertension, arising from increased intrahepatic vascular resistance, triggers progressive splanchnic arterial vasodilation mediated by nitric oxide, carbon monoxide, and endocannabinoids.[2]
This vasodilation creates effective arterial hypovolemia, activating compensatory neurohumoral systems—the renin-angiotensin-aldosterone system, sympathetic nervous system, and arginine vasopressin—leading to sodium and water retention that manifests as ascites, the hallmark of decompensated cirrhosis.[3] Systemic inflammation, driven by bacterial translocation and release of pathogen-associated molecular patterns and damage-associated molecular patterns from injured hepatocytes, further exacerbates circulatory dysfunction and contributes to multiorgan failure.[4]
Acute kidney injury (AKI) occurs in up to 50% of those hospitalized with decompensated cirrhosis, conferring substantial morbidity and mortality.[5] While patients remain susceptible to common AKI causes, including hypovolemia, acute tubular necrosis, and rarely postrenal obstruction, the hemodynamic derangements of advanced cirrhosis predispose patients to a unique form of functional renal failure, HRS. Hypovolemia-induced AKI can result from gastrointestinal losses, variceal hemorrhage, or excessive diuresis. Acute tubular necrosis can develop from prolonged ischemia, septic shock, or nephrotoxic medications. Differentiating between these phenotypes is critical to guide therapy.[6]
Hepatorenal syndrome represents a distinct entity accounting for 15% to 20% of AKI cases in cirrhosis. Three defining features characterize HRS: marked reduction in glomerular filtration rate without substantial histological changes in the kidney; potential reversibility with pharmacologic therapy or liver transplantation; and frequent association with multiorgan dysfunction. The pathogenesis reflects extreme circulatory dysfunction, wherein progressive splanchnic vasodilation and declining effective arterial blood volume trigger maximal activation of vasoconstrictor systems, leading to profound renal arterial vasoconstriction that severely impairs renal blood flow. Contributing factors include cirrhotic cardiomyopathy with reduced cardiac output, impaired renal autoregulation, and insufficient prostaglandin-mediated vasodilation to maintain renal perfusion.[7]
The first association of renal failure with cirrhosis was observed in the late 1800s. In the mid to late 1900s, results from further research indicated that renal failure in cirrhosis was hemodynamically mediated. These findings were demonstrated in patients with hepatorenal syndrome who had normal kidney histology and no proteinuria. Additional clinical evidence was demonstrated when kidney transplants from patients with HRS were performed into patients with chronic kidney disease, and the resulting improvement of renal function in patients with cirrhosis who underwent a liver transplant. Further research investigating renal clearance established an association between renal vasoconstriction and HRS.[8]
The conceptualization of HRS has evolved substantially since the first diagnostic criteria emerged in 1979. The International Club of Ascites established landmark criteria in 1996, defining HRS as serum creatinine exceeding 1.5 mg/dL and distinguishing type 1 HRS (rapidly progressive, creatinine greater than 2.5 mg/dL within 2 weeks) from type 2 HRS (slowly progressive dysfunction).[6] A major revision occurred in 2015 when criteria were harmonized with Kidney Disease: Improving Global Outcomes definitions, eliminating arbitrary creatinine thresholds and defining AKI as an increase of at least 0.3 mg/dL within 48 hours or at least 50% above baseline within 7 days. This paradigm shift enabled earlier diagnosis, particularly in populations with lower baseline creatinine. The nomenclature evolved concurrently: type 1 HRS became hepatorenal syndrome-acute kidney injury (HRS-AKI), typically triggered by bacterial infections; type 2 HRS became hepatorenal syndrome-chronic kidney disease (HRS-CKD), defined as an estimated glomerular filtration rate less than 60 mL/min/1.73 m² that persists beyond 3 months.[1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
HRS-AKI develops in the setting of advanced cirrhosis with ascites, frequently precipitated by identifiable triggering events that induce inflammation.[9] Bacterial infections constitute the predominant precipitating factor, present in approximately half of HRS-AKI cases.[10][11] Spontaneous bacterial peritonitis represents the most common infectious trigger, with HRS-AKI incidence reaching 30% among affected patients.[12] The pathogenic mechanism involves systemic inflammatory responses that amplify the release of vasodilatory mediators, exacerbating circulatory dysfunction and reducing renal perfusion.
Other bacterial infections beyond peritonitis also predispose patients to HRS-AKI. Additional precipitants include gastrointestinal hemorrhage causing hypovolemia, excessive diuretic therapy producing volume depletion, and large-volume paracentesis without adequate albumin replacement. Nephrotoxic medications, particularly nonsteroidal anti-inflammatory drugs that inhibit compensatory prostaglandin-mediated renal vasodilation, represent iatrogenic triggers. However, approximately half of HRS-AKI episodes occur without identifiable precipitating factors, reflecting the underlying hemodynamic fragility inherent to advanced decompensated cirrhosis.[13][14][15][16]
Epidemiology
Acute kidney injury occurs in 22% to 53% of those hospitalized with cirrhosis, with prevalence doubling from 15% in 2004 to 30% in 2016.[17] HRS-AKI constitutes 12% to 32% of all AKI cases, representing the third most common etiology after hypovolemia-induced injury and acute tubular necrosis.[6] Most patients present with stage 1 (69%), whereas stages 2 and 3 account for 19% and 13%, respectively. HRS-AKI portends a grave prognosis, with 90-day mortality approximating 50%, comparable to acute tubular necrosis but substantially higher than hypovolemia-induced injury.[5][18]
Pathophysiology
The pathophysiological cascade originates from portal hypertension, which triggers the production of vasodilatory mediators within the splanchnic circulation. Progressive splanchnic arterial vasodilation redistributes blood flow away from other vascular territories, creating effective arterial hypovolemia despite overall plasma volume expansion and reduced mean arterial pressure.[15][19] Sepsis can precipitate HRS in patients with cirrhosis because it triggers systemic release of sepsis-related vasoactive mediators, similar to those released in portal hypertension.[20]
Compensatory activation of neurohumoral systems ensues, including the renin-angiotensin-aldosterone system, sympathetic nervous system, and arginine vasopressin, initially maintaining arterial pressure and renal perfusion.[21] These systems promote sodium and water retention, manifesting as ascites and hypervolemic hyponatremia. As cirrhosis advances, progressive splanchnic vasodilation intensifies neurohumoral activation, culminating in severe vasoconstriction of afferent glomerular arterioles that critically impairs renal blood flow and glomerular filtration rate, precipitating HRS-AKI. Clinical evidence shows escalating neurohumoral activity across the spectrum of cirrhosis, supporting this paradigm. Vasoconstrictor therapy combined with albumin can reverse renal failure in many patients by counteracting splanchnic vasodilation and restoring effective arterial volume.
Cirrhotic cardiomyopathy contributes significantly to the pathogenesis.[22] Early cirrhosis exhibits hyperdynamic circulation with elevated cardiac output compensating for reduced systemic vascular resistance. Advanced stages manifest impaired contractile responsiveness, electrophysiological abnormalities, and diastolic dysfunction, reducing cardiac output and further compromising renal perfusion. Nonselective β-blockers can exacerbate this process by diminishing left ventricular function in patients with refractory ascites.
Renal autoregulation becomes impaired in cirrhosis, correlating with portal pressure, cardiac output, and norepinephrine levels. Prostaglandins normally counteract vasoconstrictor effects, maintaining renal perfusion; however, their production decreases in decompensated cirrhosis, while local vasoconstrictors such as endothelin increase. Additionally, nonsteroidal anti-inflammatory drugs can precipitate HRS-AKI by inhibiting compensatory prostaglandin synthesis.
Systemic inflammation constitutes an additional pathogenic mechanism. Bacterial translocation from intestinal dysbiosis releases pathogen-associated molecular patterns, while hepatocyte injury liberates damage-associated molecular patterns, including uric acid, heat-shock proteins, and S100 proteins. These activate innate immune cells, generating proinflammatory cytokines such as interleukin-6, interleukin-8, and tumor necrosis factor-α, which are significantly elevated in patients with HRS-AKI compared with patients without renal dysfunction. Inflammatory mediators exacerbate arterial vasodilation and may directly injure the kidneys, though this remains unproven. The pathogenesis thus integrates circulatory dysfunction, cardiac impairment, impaired renal autoregulation, prostaglandin deficiency, and systemic inflammation in a complex interplay culminating in functional renal failure without substantial histological abnormalities.[23]
Histopathology
As noted above, HRS is associated with normal kidney histology as the damage is hemodynamically mediated.
History and Physical
Patients with hepatorenal syndrome present with signs and symptoms of severe liver failure. These patients may initially present with fatigue and lethargy, which can be multifactorial. Reduced appetite may be amplified by increasing nausea. Over time, patients become progressively more jaundiced, first seen in the sclera and then spreading distally. The liver's synthetic function becomes affected, and patients become coagulopathic and more likely to bleed.
As these changes progress, there is a slow, gradual buildup of ascitic fluid in the peritoneum due to intravascular albumin loss and reduced oncotic pressure. Confusion due to hepatic encephalopathy is likely the last and most severe stage of liver disease and occurs because the liver cannot break down toxic metabolites, particularly ammonia. Importantly, patients may report decreased urination with progressively smaller volumes as oliguria develops.[24]
Evaluation
Acute Kidney Injury Definition
The International Club of Ascites (ICA), harmonizing with Kidney Disease: Improving Global Outcomes criteria, defines AKI as either an absolute serum creatinine increase of greater than 0.3 mg/dL (26.5 μmol/L) within 48 hours or a greater than 50% increase from baseline presumed to have occurred within 7 days. Baseline creatinine is the value obtained within the previous 3 months; when multiple values are available, the most recent value (close to hospital admission) is used. Without prior values, admission creatinine serves as a baseline. The 2019 ICA consensus incorporated urinary output less than 0.5 mL/kg/h for 6 consecutive hours as an additional criterion. AKI stages by severity include stage 1A (creatinine increase ≥0.3 mg/dL to <1.5 mg/dL); stage 1B (≥1.5 mg/dL to twice the baseline creatinine); stage 2 (2–3 times the baseline creatinine); and stage 3 (>3 times the baseline creatinine, ≥4.0 mg/dL with acute elevation ≥0.3 mg/dL, or renal replacement therapy initiation).[1][6]
Types of Hepatorenal Syndrome
Hepatorenal syndrome manifests in 2 fundamentally distinct forms based on temporal evolution and the trajectory of renal function.
Hepatorenal syndrome–acute kidney injury
Formerly designated type 1 HRS, this acute presentation develops in decompensated cirrhosis with ascites, meeting full AKI criteria. Diagnosis requires fulfillment of ICA-AKI criteria combined with the following: decompensated cirrhosis; absent or partial response to a 2-day albumin volume expansion (1 g/kg daily, maximum 100 g); absence of shock; no nephrotoxic medication exposure; and absence of structural kidney disease (ie, proteinuria >500 mg/d, microhematuria >50 erythrocytes/high-power field, abnormal ultrasonography). Fractional sodium excretion less than 0.2% suggests renal vasoconstriction (<0.1% highly predictive). HRS-AKI frequently precipitates following bacterial infections, particularly spontaneous bacterial peritonitis, occurring in approximately 30% of cases.[25][26]
Non-AKI hepatorenal syndrome
This type encompasses functional renal impairment that does not meet AKI criteria, subdivided temporally into 2 entities based on duration: hepatorenal syndrome–acute kidney disease (HRS-AKD) presents with an estimated glomerular filtration rate less than 60 mL/min/1.73 m² persisting for less than 3 months, with less than a 50% serum creatinine increase from baseline outpatient value within 3 months. Hepatorenal syndrome–chronic kidney disease (HRS-CKD), previously termed type 2 HRS, is characterized by an estimated glomerular filtration rate of less than 60 mL/min/1.73 m² sustained for more than 3 months without structural kidney disease, typically associated with refractory ascites and gradual functional deterioration.[6]
Acute Disease Quality Initiative/International Club of Ascites, ADQI-ICA, 2024 Consensus Controversy
The 2024 joint ADQI-ICA consensus challenged traditional diagnostic approaches, recommending crystalloids over albumin for initial volume resuscitation and limiting albumin administration to 24 hours rather than 48 hours for the diagnosis of HRS-AKI, arguing that systematic 48-hour albumin administration delays terlipressin initiation in euvolemic patients and risks fluid overload. However, subsequent evidence demonstrated that significant response proportions (34%) occurred specifically between 24 and 48 hours after albumin initiation, with excellent overall response rates applying the European Association for the Study of the Liver algorithm without substantial treatment delays. Consequently, the European Association for the Study of the Liver guidelines continue to recommend the 48-hour albumin challenge for AKI stage 1B or higher, maintaining established diagnostic rigor while the ADQI-ICA recommendations await prospective validation.[27][28] See Table. Diagnostic Criteria and Classification of Hepatorenal Syndrome in Cirrhosis, which summarizes the diagnostic criteria and classification of HRS.
Table. Diagnostic Criteria and Classification of Hepatorenal Syndrome in Cirrhosis
|
Classification |
Diagnostic Criteria and Definitions |
|
Hepatorenal syndrome (ICA 2015/2019) |
Required criteria (all must be present): • Decompensated cirrhosis with ascites • No improvement in serum creatinine after 48 hours of volume expansion with albumin (1 g/kg body weight daily, maximum 100 g/day). Note: Immediate diagnosis is permissible in euvolemic or hypervolemic patients according to the ADQI-ICA guidelines, but requires further validation. • Absence of shock • No current or recent exposure to nephrotoxic medications • Absence of structural renal disease evidenced by: Proteinuria ≤500 mg/24 hoursMicrohematuria ≤50 red blood cells per high-power fieldNormal renal ultrasonographic findings Supportive finding: • Fractional excretion of sodium <0.2% (highly predictive if <0.1%) |
|
Acute kidney injury (ICA-AKI 2015/2019) |
Defined by any one of the following: • Absolute increase in serum creatinine ≥0.3 mg/dL (≥26.5 μmol/L) within 48 hours • Percentage increase in serum creatinine ≥50% from baseline value, known or presumed to have occurred within the preceding 7 days • Urine output <0.5 mL/kg/h for ≥6 consecutive hours Baseline serum creatinine definition: Serum creatinine value obtained within the previous 3 months; when multiple values are available, use the measurement closest to hospital admission; in the absence of prior values, admission serum creatinine serves as baseline |
|
AKI staging system |
Stage 1A: Serum creatinine increase ≥0.3 mg/dL to final value <1.5 mg/dL (<133 μmol/L) Stage 1B: Serum creatinine increase ≥0.3 mg/dL to final value ≥1.5 mg/dL (≥133 μmol/L) Stage 2: Serum creatinine elevation 2.0–2.9 times baseline value Stage 3: Serum creatinine elevation ≥3.0 times baseline value or absolute value ≥4.0 mg/dL (≥353.6 μmol/L) with acute increase ≥0.3 mg/dL or initiation of renal replacement therapy |
|
HRS-AKI |
Acute kidney injury fulfilling International Club of Ascites AKI criteria in conjunction with diagnostic criteria for hepatorenal syndrome in patients with decompensated cirrhosis and ascites (Formerly designated type 1 hepatorenal syndrome) |
|
Acute kidney disease (AKD) and chronic kidney disease (CKD) |
AKD: Estimated glomerular filtration rate <60 mL/min/1.73 m² persisting <3 months CKD: Estimated glomerular filtration rate <60 mL/min/1.73 m² persisting ≥3 months |
|
HRS-NAKI (Non-AKI HRS) |
Functional renal impairment in cirrhotic patients not fulfilling acute kidney injury criteria, subdivided into: HRS-AKD: Estimated glomerular filtration rate <60 mL/min/1.73 m² for <3 months with <50% increase in serum creatinine from baseline outpatient value, fulfilling hepatorenal syndrome criteria HRS-CKD: Estimated glomerular filtration rate <60 mL/min/1.73 m² for ≥3 months, fulfilling hepatorenal syndrome criteria (HRS-CKD, formerly designated type 2 hepatorenal syndrome) |
|
KDIGO CKD classification |
GFR categories (mL/min/1.73 m²): G1: ≥90 (normal or elevated) G2: 60–89 (mild reduction) G3a: 45–59 (mild to moderate reduction) G3b: 30–44 (moderate to severe reduction) G4: 15–29 (severe reduction) G5: <15 (kidney failure) Albuminuria categories (mg/g creatinine): A1: <30 (normal to mildly increased) A2: 30–300 (moderately increased) A3: >300 (severely increased) |
ADQI, Acute Disease Quality Initiative; AKD, acute kidney disease; AKI, acute kidney injury; CKD, chronic kidney disease; GFR, glomerular filtration rate; HRS, hepatorenal syndrome; HRS-AKD, hepatorenal syndrome–acute kidney disease; HRS-AKI, hepatorenal syndrome–acute kidney injury; HRS-CKD, hepatorenal syndrome–chronic kidney disease; HRS-NAKI, non–acute kidney injury hepatorenal syndrome; ICA, International Club of Ascites; ICA-AKI, International Club of Ascites–acute kidney injury; KDIGO, Kidney Disease: Improving Global Outcomes
Evaluation
The initial evaluation begins with AKI severity staging, followed by a systematic evaluation. Upon AKI diagnosis, diuretics require immediate discontinuation. The evaluation includes review of nephrotoxic medication exposure (nonsteroidal anti-inflammatory drugs, aminoglycosides, radiocontrast agents); screening for bacterial infection with prompt antibiotic initiation; urinalysis for proteinuria, hematuria, and cellular casts; and renal ultrasonography to exclude obstruction. Hypovolemic patients should receive appropriate volume resuscitation with crystalloids for fluid losses and packed erythrocytes for hemorrhage (see Image. Hepatorenal Syndrome Diagnostic Algorithm).
Patients without overt hypovolemia (AKI stage ≥1B per European Association for Study of the Liver) should undergo an albumin challenge of 1 g/kg daily (maximum 100 g) for 48 hours. Persistent AKI after albumin warrants assessment of HRS-AKI criteria. Differentiating HRS-AKI from acute tubular necrosis is challenging; urinary neutrophil gelatinase-associated lipocalin (uNGAL) demonstrates superior discriminative capacity, with elevated levels (>220 ng/mL) indicating tubular injury. Alternative biomarkers, including interleukin-18 and kidney injury molecule-1, show inferior performance. Fractional sodium excretion greater than 0.2% suggests HRS-AKI, though it lacks specificity.[5][29][30]
Treatment / Management
Hepatorenal syndrome involves establishing euvolemia while stopping all nephrotoxic agents. The active medical treatment of HRS is aimed at splanchnic vasoconstriction, which increases systemic vascular resistance and mean arterial pressure. This counter-regulatory mechanism suppresses the renin-angiotensin-aldosterone system and the sympathetic nervous system. This process reduces renal vasoconstriction and improves renal blood flow.
Terlipressin combined with albumin constitutes the first-line HRS-AKI treatment. Terlipressin, a vasopressin V1a-receptor agonist, induces splanchnic vasoconstriction, counteracts pathologic vasodilation, reduces portal pressure, and augments mean arterial pressure and renal perfusion.[31][32][33][34][35] Albumin increases effective arterial blood volume through both oncotic and nononcotic mechanisms, thereby enhancing cardiac contractility. Terlipressin is initiated at 1 mg intravenously every 6 hours, followed by dose escalation to 2 mg every 6 hours at 48 to 72 hours, if response is inadequate (creatinine reduction <20% to 30%). Continuous infusion (2 mg daily initially, escalating every 48 hours to a maximum of 12 mg daily) demonstrates equivalent efficacy with reduced adverse effects.[35][36] (A1)
The suggested albumin dose is 20 to 40 g daily, largely empirical and guided by volume assessment using point-of-care ultrasonography.[37] Adverse effects of terlipressin necessitate vigilant monitoring, including ischemic complications (myocardial, peripheral, mesenteric); respiratory failure from pulmonary edema; and volume overload.[38][39][40] Alternative vasoconstrictors include norepinephrine (0.5–3 mg/h continuous infusion in the intensive care unit) when terlipressin is unavailable, demonstrating potentially comparable efficacy. Midodrine plus octreotide is significantly inferior in response (29% versus 70%), but may be considered if terlipressin or norepinephrine is contraindicated.[41](A1)
Definitive Management
Liver transplant represents the optimal treatment, offering the highest survival benefit. Patients who do not respond to pharmacotherapy and meet indications for renal replacement therapy (uremic complications, refractory acidosis, electrolyte derangements, pulmonary edema) can receive continuous renal replacement therapy as a bridge to transplant; mortality exceeds 80% at 90 days without transplant. Simultaneous liver-kidney transplant consideration requires individualized assessment based on AKI duration, response to therapy, and underlying chronic kidney disease.
Differential Diagnosis
The differential diagnosis of HRS includes prerenal, intrinsic renal disease, and obstruction.
- Glomerulopathy:
- Hepatitis C virus– and hepatitis B virus–associated nephropathies
- Immunoglobulin A nephropathy
- Prerenal causes:
- Diuretics
- Cardiac dysfunction
- Excess laxatives
- Inadvertent fluid restriction
- Acute variceal bleeding
- Tubular injury:
- Ischemic (eg, acute variceal bleeding, septic shock, prolonged prerenal state, high-dose vasopressors, possible terlipressin effect)
- Toxic (especially cholemic nephropathy)
- Drugs
- Interstitial nephritis
- Obstructive nephropathy:
- Association with midodrine; possibly as a precipitant (see Image. Acute Kidney Injury)
Prognosis
HRS-AKI has a very poor prognosis. Results from a recent study indicated that among 198 hospitalized individuals, the median overall survival from vasopressor initiation was only 48 days, and transplant-free survival was 28 days. Notably, 33.8% of patients died during hospitalization, and 31.3% required renal replacement therapy.[38]
Complications
Complications of HRS include:
- Progression to chronic kidney disease and end-stage kidney disease
- Progression to multiorgan failure and acute-on-chronic liver failure
- Persistent hepatorenal syndrome may necessitate a combined liver and kidney transplant (simultaneous or sequential)
- Uremic complications, such as severe metabolic acidosis, encephalopathy, hyperkalemia, pericarditis, and other manifestations, may necessitate renal replacement therapy
Deterrence and Patient Education
Patients with decompensated cirrhosis and caregivers should be educated about the main triggers of hepatorenal syndrome, especially infections. Strategies to reduce the risk of spontaneous bacterial peritonitis must be taught. Patients and caregivers should also be advised to avoid nephrotoxic medications, including common analgesics such as nonsteroidal anti-inflammatory drugs, and to adhere to the interdisciplinary team's fluid and diuretic recommendations.
Enhancing Healthcare Team Outcomes
Coordination of risk assessment and treatment must occur between nurses, hepatologists, nephrologists, and intensivists to optimize care for these patients. Patients with HRS have very high rates of infection and hemodynamic compromise. Early identification and treatment of patients with HRS are imperative to reducing morbidity and mortality. The care of patients with HRS necessitates a collaborative approach among health care professionals to ensure patient-centered care and improve overall outcomes.
Nephrologists, hepatologists, gastroenterologists, emergency medicine clinicians, critical care clinicians, nurses, pharmacists, and other health professionals involved in the care of these patients should possess the essential clinical skills and knowledge to accurately diagnose and treat HRS. This includes expertise in recognizing varied clinical presentations and understanding the nuances of diagnostic techniques such as ultrasonography and laboratory values. These teams have been shown to improve outcomes in patients with this condition. Patient and caregiver education about triggering factors (most importantly infections), medication adherence, and adherence to dietary recommendations is essential to prevent morbidity from hepatorenal syndrome.
A strategic approach is equally crucial, involving evidence-based strategies to optimize treatment plans and minimize adverse effects. Ethical considerations must guide decision-making, ensuring informed consent and respecting patient autonomy in treatment choices. Each healthcare professional must be aware of their responsibilities and contribute their unique expertise to the patient's care plan, fostering an interdisciplinary approach.
Effective interprofessional communication is paramount, allowing seamless information exchange and collaborative decision-making among team members. Care coordination plays a pivotal role in ensuring that the patient's journey from diagnosis to treatment and follow-up is well-managed, minimizing errors and enhancing patient safety. By embracing these principles of skill, strategy, ethics, responsibilities, interprofessional communication, and care coordination, health care professionals can deliver patient-centered care, ultimately improving patient outcomes and enhancing team performance in the treatment of patients with hepatorenal syndrome.
Media
(Click Image to Enlarge)
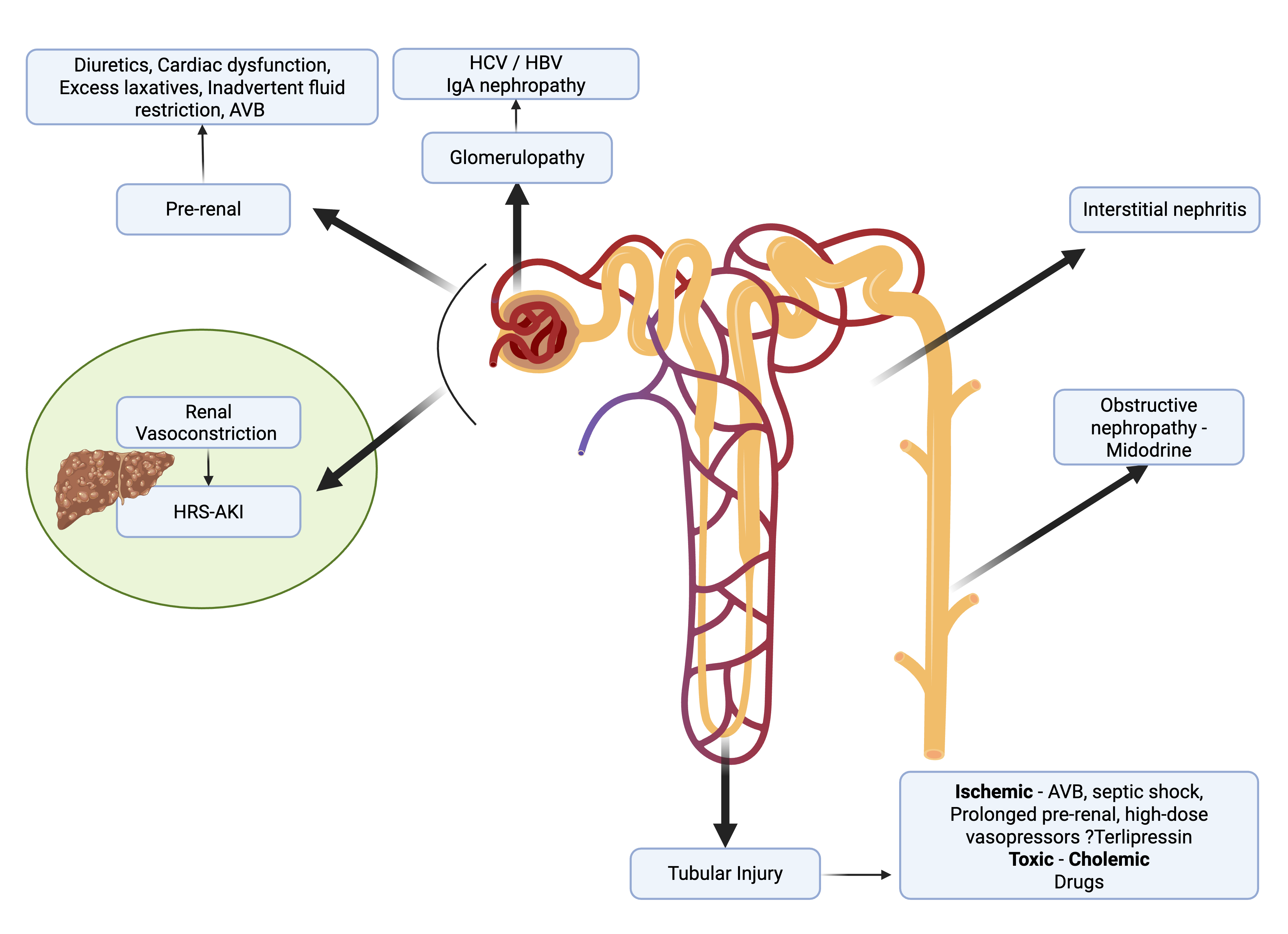
Acute Kidney Injury. Differential diagnosis of acute kidney injury in a patient with cirrhosis of the liver.
Contributed by V Girish, MD
(Click Image to Enlarge)
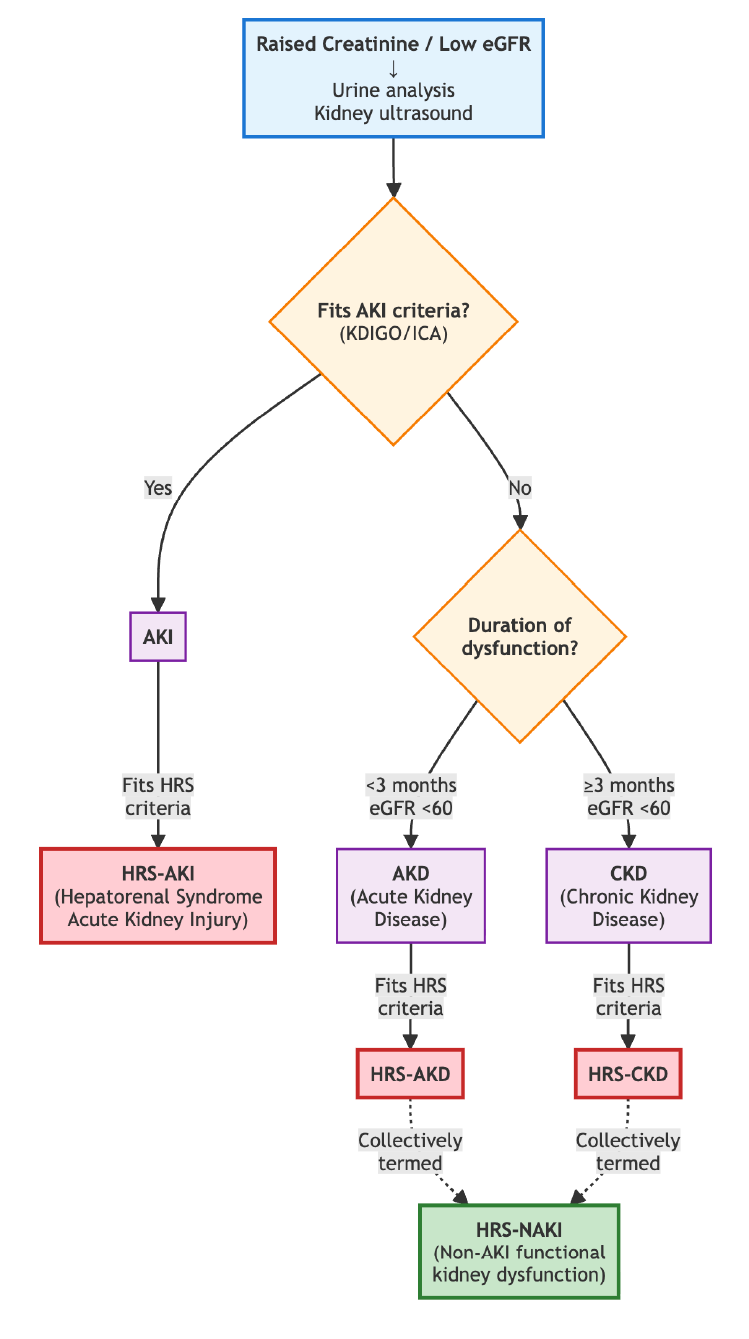
Hepatorenal Syndrome Diagnostic Algorithm. Flowchart showing the main diagnostic pathway from initial presentation through classification of each subtype of hepatorenal syndrome.
Contributed by V Girish, MD
References
Nadim MK, Kellum JA, Forni L, Francoz C, Asrani SK, Ostermann M, Allegretti AS, Neyra JA, Olson JC, Piano S, VanWagner LB, Verna EC, Akcan-Arikan A, Angeli P, Belcher JM, Biggins SW, Deep A, Garcia-Tsao G, Genyk YS, Gines P, Kamath PS, Kane-Gill SL, Kaushik M, Lumlertgul N, Macedo E, Maiwall R, Marciano S, Pichler RH, Ronco C, Tandon P, Velez JQ, Mehta RL, Durand F. Acute kidney injury in patients with cirrhosis: Acute Disease Quality Initiative (ADQI) and International Club of Ascites (ICA) joint multidisciplinary consensus meeting. Journal of hepatology. 2024 Jul:81(1):163-183. doi: 10.1016/j.jhep.2024.03.031. Epub 2024 Mar 26 [PubMed PMID: 38527522]
Level 2 (mid-level) evidenceMaiwall R, Singh SP, Angeli P, Moreau R, Krag A, Singh V, Singal AK, Tan SS, Puri P, Mahtab M, Lau G, Ning Q, Sharma MK, Rao PN, Kapoor D, Gupta S, Duseja A, Wadhawan M, Jothimani D, Saigal S, Taneja S, Shukla A, Puri P, Govil D, Pandey G, Madan K, Eapen CE, Benjamin J, Chowdhury A, Singh S, Salao V, Yang JM, Hamid S, Shalimar, Jasuja S, Kulkarni AV, Niriella MA, Tevethia HV, Arora V, Mathur RP, Roy A, Jindal A, Saraf N, Verma N, De A, Choudhary NS, Mehtani R, Chand P, Rudra O, Sarin SK. APASL clinical practice guidelines on the management of acute kidney injury in acute-on-chronic liver failure. Hepatology international. 2024 Jun:18(3):833-869. doi: 10.1007/s12072-024-10650-0. Epub 2024 Apr 5 [PubMed PMID: 38578541]
Level 1 (high-level) evidenceMaiwall R, Kumar S, Chandel SS, Kumar G, Rastogi A, Bihari C, Sharma MK, Thakur B, Jamwal K, Nayak S, Mathur RP, Sarin SK. AKI in patients with acute on chronic liver failure is different from acute decompensation of cirrhosis. Hepatology international. 2015 Oct:9(4):627-39. doi: 10.1007/s12072-015-9653-x. Epub 2015 Sep 2 [PubMed PMID: 26329121]
Sánchez-Aldehuelo R, Villanueva C, Genescà J, García-Pagán JC, Castillo E, Calleja JL, Aracil C, Bañares R, Téllez L, Paule L, Morillas RM, Poca M, Peñas B, Augustin S, Abraldes JG, Alvarado-Tapias E, Bosch J, Albillos A. Progressive systemic inflammation precedes decompensation in compensated cirrhosis. JHEP reports : innovation in hepatology. 2025 Feb:7(2):101231. doi: 10.1016/j.jhepr.2024.101231. Epub 2024 Oct 5 [PubMed PMID: 39850960]
Khemichian S, Nadim MK, Terrault NA. Update on Hepatorenal Syndrome: From Pathophysiology to Treatment. Annual review of medicine. 2025 Jan:76(1):373-387. doi: 10.1146/annurev-med-050223-112947. Epub [PubMed PMID: 39869432]
Girish V, Maiwall R. Tracking the trajectory of kidney dysfunction in cirrhosis: the acute kidney injury: chronic kidney disease spectrum. Clinical and molecular hepatology. 2025 Jul:31(3):730-752. doi: 10.3350/cmh.2024.1060. Epub 2025 Mar 26 [PubMed PMID: 40138802]
Brick CR, Cailes B, Majumdar A, Testro A, Sinclair M, Al-Fiadh A, Weinberg L, Ramachandran J, Gill M, Farouque O, Koshy AN. CardioHepatology: Exploring the Interplay Between Cirrhosis, Cirrhotic Cardiomyopathy, Coronary Artery Disease, and Liver Transplantation. Heart, lung & circulation. 2025 Dec:34(12):1362-1372. doi: 10.1016/j.hlc.2025.06.1022. Epub 2025 Nov 3 [PubMed PMID: 41188159]
Amin AA, Alabsawy EI, Jalan R, Davenport A. Epidemiology, Pathophysiology, and Management of Hepatorenal Syndrome. Seminars in nephrology. 2019 Jan:39(1):17-30. doi: 10.1016/j.semnephrol.2018.10.002. Epub [PubMed PMID: 30606404]
Maiwall R, Kumar S, Chaudhary AK, Maras J, Wani Z, Kumar C, Rastogi A, Bihari C, Vashisht C, Sarin SK. Serum ferritin predicts early mortality in patients with decompensated cirrhosis. Journal of hepatology. 2014 Jul:61(1):43-50. doi: 10.1016/j.jhep.2014.03.027. Epub 2014 Mar 26 [PubMed PMID: 24681346]
Fernández J, Acevedo J, Prado V, Mercado M, Castro M, Pavesi M, Arteaga M, Sastre L, Juanola A, Ginès P, Arroyo V. Clinical course and short-term mortality of cirrhotic patients with infections other than spontaneous bacterial peritonitis. Liver international : official journal of the International Association for the Study of the Liver. 2017 Mar:37(3):385-395. doi: 10.1111/liv.13239. Epub 2016 Sep 20 [PubMed PMID: 27558198]
Clària J, Stauber RE, Coenraad MJ, Moreau R, Jalan R, Pavesi M, Amorós À, Titos E, Alcaraz-Quiles J, Oettl K, Morales-Ruiz M, Angeli P, Domenicali M, Alessandria C, Gerbes A, Wendon J, Nevens F, Trebicka J, Laleman W, Saliba F, Welzel TM, Albillos A, Gustot T, Benten D, Durand F, Ginès P, Bernardi M, Arroyo V, CANONIC Study Investigators of the EASL-CLIF Consortium and the European Foundation for the Study of Chronic Liver Failure (EF-CLIF). Systemic inflammation in decompensated cirrhosis: Characterization and role in acute-on-chronic liver failure. Hepatology (Baltimore, Md.). 2016 Oct:64(4):1249-64. doi: 10.1002/hep.28740. Epub 2016 Aug 25 [PubMed PMID: 27483394]
Albillos A, Martin-Mateos R, Van der Merwe S, Wiest R, Jalan R, Álvarez-Mon M. Cirrhosis-associated immune dysfunction. Nature reviews. Gastroenterology & hepatology. 2022 Feb:19(2):112-134. doi: 10.1038/s41575-021-00520-7. Epub 2021 Oct 26 [PubMed PMID: 34703031]
Serper M, Tang H, Zhang S, McCullough A, Kaplan DE, Taddei TH, Mahmud N. Clinical outcomes and care for spontaneous bacterial peritonitis: A national cohort study. Hepatology (Baltimore, Md.). 2025 Nov 1:82(5):1187-1197. doi: 10.1097/HEP.0000000000001251. Epub 2025 Jan 29 [PubMed PMID: 39879583]
Level 2 (mid-level) evidenceNadim MK, Kellum JA, Durand F. From protocol to precision: The evolving diagnosis of hepatorenal syndrome. Journal of hepatology. 2026 Jan:84(1):e19-e21. doi: 10.1016/j.jhep.2025.07.027. Epub 2025 Aug 5 [PubMed PMID: 40759199]
Ginès P, Cárdenas A, Arroyo V, Rodés J. Management of cirrhosis and ascites. The New England journal of medicine. 2004 Apr 15:350(16):1646-54 [PubMed PMID: 15084697]
Girish V, Maiwall R. Editorial: Solving the acute kidney injury puzzle in alcohol-associated hepatitis-Challenges and insights. Alimentary pharmacology & therapeutics. 2024 Oct:60(7):963-964. doi: 10.1111/apt.18206. Epub 2024 Sep 3 [PubMed PMID: 39225450]
Level 3 (low-level) evidencePatidar KR, Belcher JM, Regner KR, St Hillien SA, Simonetto DA, Asrani SK, Neyra JA, Sharma P, Velez JCQ, Wadei H, Nadim MK, Chung RT, Seethapathy R, Parada XV, Ouyang T, Ufere NN, Robinson JE, McLean Diaz P, Wilechansky RM, Przybyszewski EM, Smith TN, Ali AA, Orman ES, Schulz P, Siddiqui SM, Shabbir R, Liu LJ, Cama-Olivares A, Flannery AH, Baker ML, Gunasekaran D, Aswine A, Issa R, Li J, Verma S, Chalmers D, Varghese V, Lam W, Mohamed M, Kovacic R, Gaddy A, Attieh RM, Cortes P, Semnani S, Wang L, Khemichian S, Allegretti AS, from the HRS-HARMONY consortium. Incidence and outcomes of acute kidney injury including hepatorenal syndrome in hospitalized patients with cirrhosis in the US. Journal of hepatology. 2023 Dec:79(6):1408-1417. doi: 10.1016/j.jhep.2023.07.010. Epub 2023 Jul 28 [PubMed PMID: 37517455]
Maiwall R, Sharma F. AKI in ACLF: navigating the complex therapeutic puzzle. Expert review of gastroenterology & hepatology. 2025 Jan-Feb:19(2):165-180. doi: 10.1080/17474124.2025.2456121. Epub 2025 Jan 23 [PubMed PMID: 39825627]
Sarin SK, Sharma P. Terlipressin: an asset for hepatologists! Hepatology (Baltimore, Md.). 2011 Aug:54(2):724-8. doi: 10.1002/hep.24519. Epub [PubMed PMID: 21735463]
Angeli P, Tonon M, Pilutti C, Morando F, Piano S. Sepsis-induced acute kidney injury in patients with cirrhosis. Hepatology international. 2016 Jan:10(1):115-23. doi: 10.1007/s12072-015-9641-1. Epub 2015 Jul 4 [PubMed PMID: 26141259]
Nadim MK, Garcia-Tsao G. Acute Kidney Injury in Patients with Cirrhosis. The New England journal of medicine. 2023 Feb 23:388(8):733-745. doi: 10.1056/NEJMra2215289. Epub [PubMed PMID: 36812435]
Premkumar M, Kajal K, Roy A, Izzy M, Divyaveer S, Kulkarni AV, Artru F, Sharma P, Sandhu A, Sihag BK, Bahl A, De A, Verma N, Taneja S, Duseja AK, Pal A, Bhujade H, Reddy KR. Point-of-care ultrasound (POCUS)-guided volume management and the effect of cirrhotic cardiomyopathy on acute kidney injury outcomes in cirrhosis. Hepatology (Baltimore, Md.). 2025 Sep 23:():. doi: 10.1097/HEP.0000000000001524. Epub 2025 Sep 23 [PubMed PMID: 40986890]
Incicco S, Angeli P, Piano S. Infectious Complications of Portal Hypertension. Clinics in liver disease. 2024 Aug:28(3):525-539. doi: 10.1016/j.cld.2024.03.007. Epub 2024 Apr 27 [PubMed PMID: 38945641]
Arroyo V, Moreau R, Jalan R, Ginès P, EASL-CLIF Consortium CANONIC Study. Acute-on-chronic liver failure: A new syndrome that will re-classify cirrhosis. Journal of hepatology. 2015 Apr:62(1 Suppl):S131-43. doi: 10.1016/j.jhep.2014.11.045. Epub [PubMed PMID: 25920082]
Ma AT, Solé C, Juanola A, Escudé L, Napoleone L, Avitabile E, Pérez-Guasch M, Carol M, Pompili E, Gratacós-Ginés J, Soria A, Rubio AB, Cervera M, Moreta MJ, Morales-Ruiz M, Solà E, Poch E, Fabrellas N, Graupera I, Pose E, Ginès P. Prospective validation of the EASL management algorithm for acute kidney injury in cirrhosis. Journal of hepatology. 2024 Sep:81(3):441-450. doi: 10.1016/j.jhep.2024.03.006. Epub 2024 Mar 11 [PubMed PMID: 38479614]
Level 1 (high-level) evidenceAngeli P, Garcia-Tsao G, Nadim MK, Parikh CR. News in pathophysiology, definition and classification of hepatorenal syndrome: A step beyond the International Club of Ascites (ICA) consensus document. Journal of hepatology. 2019 Oct:71(4):811-822. doi: 10.1016/j.jhep.2019.07.002. Epub 2019 Jul 11 [PubMed PMID: 31302175]
Level 3 (low-level) evidenceAngeli P, Labenz C, Piano S, Juanola A, Krag A, Caraceni P, Trebicka J, Maiwall R, Singh V, Pose E, Gambino C, Marciano S, Galle PR, Sarin SK, Ginès P, Kamath PS. Albumin infusion in hepatorenal syndrome-acute kidney injury: New evidence challenges recent consensus. Journal of hepatology. 2025 Sep:83(3):800-802. doi: 10.1016/j.jhep.2025.04.011. Epub 2025 Apr 17 [PubMed PMID: 40250764]
Level 3 (low-level) evidenceNadim MK, Kellum JA, Durand F. Reply to: "Shortening the albumin challenge from 48 to 24 hours may lead to overdiagnosis of hepatorenal syndrome-acute kidney injury and overtreatment with terlipressin". Journal of hepatology. 2025 Feb:82(2):e100-e101. doi: 10.1016/j.jhep.2024.10.025. Epub 2024 Oct 23 [PubMed PMID: 39454689]
Maiwall R, Pasupuleti SSR, Rastogi A, Sharma F, Hidam AK, Thomas S, Sarin SK. AARC score and urine NGAL predict terlipressin non-response and mortality in patients with acute-on-chronic liver failure. Hepatology international. 2025 Feb:19(1):222-233. doi: 10.1007/s12072-024-10749-4. Epub 2024 Nov 28 [PubMed PMID: 39607651]
Maiwall R, Pasupuleti SSR, Hidam AK, Rastogi A, Thomas S, Kumar G, Kumar A, Sarin SK. Non-resolution of acute kidney injury in the first week portends the development of chronic kidney disease in critically ill patients with cirrhosis. Alimentary pharmacology & therapeutics. 2023 Sep:58(6):593-610. doi: 10.1111/apt.17639. Epub 2023 Jul 16 [PubMed PMID: 37455381]
Ma AT, Juanola A, Patidar KR, Barone A, Incicco S, Kulkarni AV, Verma N, Lange CM, Xie Q, Alessandria C, Cerda Reyes E, Maiwall R, Kim JH, Marciano S, Farias AQ, Toledo C, Nardelli S, Vorobioff JD, Roblero JP, Thévenot T, Papp M, Maan R, Solé C, Cordova-Gallardo J, Simonetto DA, Fouad Y, Balcar L, Raevens S, Nabilou P, Caraceni P, Merli M, Presa J, Laleman W, Krag A, Bruns T, Pereira G, Mattos AZ, Arab JP, Wentworth B, Abdelkader NA, Wong YJ, Kim SE, Roux O, Takkenberg RB, Galante A, Goncalves LL, Pyrsopoulos NT, Pérez Hernández JL, Asrani SK, Torre A, Díaz-Ferrer J, Orman ES, Perricone G, Gadano A, Ivashkin V, Fassio E, Marino M, Vargas V, Rabinowich L, Montes P, Mohammed A, Carrera E, Cabrera MC, Girala M, Samant H, Madaleno J, Kim WR, Ferreira CN, Allegretti AS, Sarin SK, Ginès P, Angeli P, Solà E, Piano S, International Club of Ascites GLOBAL AKI team. Real-World Use of Terlipressin in Cirrhosis and Acute Kidney Injury: Frequent Use Beyond Hepatorenal Syndrome. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2026 Apr:24(4):1079-1091. doi: 10.1016/j.cgh.2025.08.031. Epub 2025 Sep 8 [PubMed PMID: 40930302]
Wong F, Pappas SC. Terlipressin use in hepatorenal syndrome-acute kidney injury in cirrhosis. Intensive care medicine. 2025 Jan:51(1):213-214. doi: 10.1007/s00134-024-07681-4. Epub 2024 Oct 23 [PubMed PMID: 39441357]
Torp N, China L, Israelsen M, Forrest E, Freemantle N, Trebicka J, Krag A, O'Brien A. Targeted albumin infusions in hospitalized patients with cirrhosis receiving terlipressin: A post-hoc analysis of ATTIRE. Annals of hepatology. 2025 Jul-Dec:30(2):101941. doi: 10.1016/j.aohep.2025.101941. Epub 2025 Jul 1 [PubMed PMID: 40609902]
Jindal A, Singh H, Kumar G, Arora V, Sharma MK, Maiwall R, Rajan V, Tewathia HV, Vasishtha C, Sarin SK. Early Versus Standard Initiation of Terlipressin for Acute Kidney Injury in ACLF: A Randomized Controlled Trial (eTerli Study). Digestive diseases and sciences. 2024 Jun:69(6):2204-2214. doi: 10.1007/s10620-024-08423-8. Epub 2024 Apr 18 [PubMed PMID: 38637454]
Level 1 (high-level) evidenceArora V, Maiwall R, Rajan V, Jindal A, Muralikrishna Shasthry S, Kumar G, Jain P, Sarin SK. Terlipressin Is Superior to Noradrenaline in the Management of Acute Kidney Injury in Acute on Chronic Liver Failure. Hepatology (Baltimore, Md.). 2020 Feb:71(2):600-610. doi: 10.1002/hep.30208. Epub 2019 Feb 20 [PubMed PMID: 30076614]
Cavallin M, Piano S, Romano A, Fasolato S, Frigo AC, Benetti G, Gola E, Morando F, Stanco M, Rosi S, Sticca A, Cillo U, Angeli P. Terlipressin given by continuous intravenous infusion versus intravenous boluses in the treatment of hepatorenal syndrome: A randomized controlled study. Hepatology (Baltimore, Md.). 2016 Mar:63(3):983-92. doi: 10.1002/hep.28396. Epub 2016 Feb 3 [PubMed PMID: 26659927]
Level 1 (high-level) evidenceGirish V, Maiwall R. Revisiting septic shock in cirrhosis: a call for personalized management. Expert review of gastroenterology & hepatology. 2024 Dec:18(12):795-813. doi: 10.1080/17474124.2024.2443813. Epub 2025 Jan 2 [PubMed PMID: 39744868]
Sanyal AJ, Reddy KR, Brown KA, Landis CS, Cullaro G, Huang X, Kelkar SS, Raina R, Corman S, Kebede N, Edmundson P, Jamil K, Allegretti AS. Challenges in the Treatment of Hepatorenal Syndrome-Acute Kidney Injury: A US Chart Review of Treatment Patterns and Survival Outcomes. JGH open : an open access journal of gastroenterology and hepatology. 2025 Sep:9(9):e70255. doi: 10.1002/jgh3.70255. Epub 2025 Sep 14 [PubMed PMID: 40958936]
Allegretti AS, Levitsky J, Sharma P, Ouyang T, Jamil K, Silvey S, Bajaj JS. Predictors of response to terlipressin therapy in hepatorenal syndrome: Metabolomic and proteomic analysis from the CONFIRM trial. Hepatology communications. 2025 Aug 1:9(8):. doi: 10.1097/HC9.0000000000000766. Epub 2025 Jul 14 [PubMed PMID: 40658810]
Cullaro G, Allegretti AS, Patidar KR, Jamil K, Velez JCQ. The relationship between mean arterial pressure and terlipressin in hepatorenal syndrome-acute kidney injury reversal: A post hoc analysis. Hepatology (Baltimore, Md.). 2026 Jan 1:83(1):94-104. doi: 10.1097/HEP.0000000000001295. Epub 2025 Mar 7 [PubMed PMID: 40053863]
Cavallin M, Kamath PS, Merli M, Fasolato S, Toniutto P, Salerno F, Bernardi M, Romanelli RG, Colletta C, Salinas F, Di Giacomo A, Ridola L, Fornasiere E, Caraceni P, Morando F, Piano S, Gatta A, Angeli P, Italian Association for the Study of the Liver Study Group on Hepatorenal Syndrome. Terlipressin plus albumin versus midodrine and octreotide plus albumin in the treatment of hepatorenal syndrome: A randomized trial. Hepatology (Baltimore, Md.). 2015 Aug:62(2):567-74. doi: 10.1002/hep.27709. Epub 2015 Feb 13 [PubMed PMID: 25644760]
Level 1 (high-level) evidence