Introduction
Hepatitis D virus (HDV) was discovered in 1977 in patients with chronic hepatitis B virus (HBV) infection.[1] Originally considered an unrecognized HBV antigen, the HDV nuclear antigen was later discovered to be a distinct pathogen, originally termed the delta agent. HDV is considered a hybrid virus because it uses hepatitis B surface antigen (HBsAg) as its envelope protein, allowing it to infect only patients who are concomitantly infected with HBV.[2] HDV also interferes with HBV replication, resulting in low levels of HBV DNA.[3] HDV is also unique because it is the smallest known virus to infect humans.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
HDV infection causes acute and chronic inflammatory liver disease and is transmitted parenterally. While in developed nations this is usually due to intravenous drug use, in resource-limited settings, transmission occurs due to inadequate sterilization practices. Risk factors include blood transfusions and intravenous drug use.[4] Infection is categorized as either coinfection (acute simultaneous infection with HDV and HBV) or superinfection (HDV infection in a person with chronic hepatitis B).
Epidemiology
Even though HDV depends on HBV, its geographical distribution differs from that of HBV, partly due to differences in transmission mode. HDV is transmitted via the parenteral route through blood or blood product exposure. Sexual transmission is infrequent, and vertical transmission is rare.[5][6] Information on HDV epidemiology has mostly been obtained from HBV carriers superinfected with HDV. Approximately 5% of HBV carriers are also estimated to have HDV.[7] Recently, there has been a significant decline in HDV transmission, primarily attributed to a decrease in the incidence of HBV infection. This decline is largely due to improved socioeconomic conditions, increased awareness of infectious disease transmission, and increased HBV vaccination rates.[7]
Recent study results determined that the HDV prevalence among HBV-infected individuals in the United States was 1.2%, which is lower than previous estimates.[8] HDV is most prevalent in the Mediterranean, East Africa, the Amazon Basin, the Middle East, central and northern Asia, and certain areas of the Pacific.[9] In Western countries, HDV infection is infrequent, occurring only in high-risk populations such as intravenous drug users, individuals from areas with a high prevalence of HDV, and recipients of multiple transfusions. While the prevalence is less than 1% in North America, it exceeds 2% in other parts of the world, although few population-level studies exist.[10]
Pathophysiology
Structurally, HDV comprises a ribonucleic acid (RNA) genome, hepatitis D antigen (HDAg), and a lipoprotein envelope from HBV. The genome encodes only the HDAg. There are 2 types of HDAg, named after their size: long and short. Viral replication occurs in hepatocytes, and the virus is unique because it uses host RNA polymerase II to transcribe its messenger RNA. Although short HDAg proteins activate viral replication via direct binding to HDV RNA, the long HDAg proteins direct viral assembly and inhibit viral replication. The virus is completely assembled after incorporating the HBV envelope, after which it is released.[2][11][12]
HDV infection only occurs in the presence of HBV. In individuals susceptible to HBV, coinfection with both viruses results in acute HBV and HDV infection. Clinically, coinfection resembles classic acute HBV, except for a biphasic course of 2 peaks in serum alanine aminotransferase levels, several weeks apart. HBV infection must be established first during acute coinfection before HDV replication begins. Coinfection may be more severe than HBV monoinfection, with an increased risk for liver failure. Most patients recover during acute coinfection with HBV and HDV, and approximately 5% of patients develop chronic infection, defined as persistence of infection beyond 6 months.[5][13]
In individuals who are chronic carriers of HBsAg, a superinfection can occur, which may present as severe acute hepatitis or exacerbation of preexisting chronic HBV. In patients with chronic HBV infection, acute HDV infection may be mistaken for an HBV flare. In those with undiagnosed HBV infection, the clinical presentation and initial investigations may be mistaken for acute HBV infection if HDV superinfection is not considered. The clinical course of superinfection is often more severe than that during an HBV/HDV coinfection. Because HBsAg allows for continuous viral replication, 90% of these individuals progress to chronic HDV. Chronic HDV infection causes more severe morbidity (progressive fibrosis, cirrhosis, hepatocellular carcinoma, and hepatic decompensation) than chronic HBV infection.[14] In cases of triple infection with HBV, hepatitis C virus (HCV), and HDV, either HDV or HCV will predominate, depending on the geographic region, host immune factors, activity, and HDV genotype.
Although the mechanism by which HDV induces liver damage is not entirely known, it is thought to be due to the host's immune response.[15] The spectrum of damage can range from asymptomatic to fulminant liver failure. HDV superinfection tends to have a more rapid course and increases the risk of hepatocellular carcinoma.[16] The degree of injury depends on various factors, including the HDV genotype, host immune response, and HBV genotype. Classically, there are 3 main HDV genotypes: 1, 2, and 3. Additionally, other genotypes have been identified but are not yet well characterized. Genotype 1 is the predominant type in Western countries and, when associated with acute hepatitis D, has a fulminant course.[17] Once chronic, genotype 1 can exacerbate existing HBV disease and rapidly progress to liver cirrhosis, but it can also have an indolent course. Genotype 2 is most common in Asia and is less frequently associated with fulminant liver disease and the progression of chronic liver disease.[18] Genotype 3 is most prevalent in South America and may cause severe acute hepatitis, which can progress to liver failure.[19] Other important risk factors include HDV RNA persistence, obesity, diabetes mellitus, and alcohol use.[20]
Histopathology
HDV causes the same histological changes in the liver parenchyma as other viral infections, resulting in necrosis and inflammation of hepatocytes. In acute disease, intralobular infiltration of inflammatory cells (lymphocytes, macrophages) is present along with cytoplasmic eosinophilia. Chronic hepatitis is characterized by periportal necrosis and is often accompanied by nodular changes.
History and Physical
Hepatitis D is clinically similar to other viral hepatic infections. Most patients are asymptomatic, but depending on the severity, signs and symptoms may include fever, abdominal pain, nausea, vomiting, jaundice, confusion, bruising, or bleeding.
Evaluation
In response to HDAg, antibodies (anti-HDV) of the IgM and IgG subtypes are produced. The 3 infection patterns (acute HDV/HBV coinfection, acute HDV superinfection, and chronic HDV infection) vary in the serum levels of HDV RNA, HDAg, and anti-HDV antibodies as well as HBV serum biomarkers (See Image. Hepatitis D Stages, Serological Markers, and the 3 Infection Patterns). Because HDV depends on HBV, the presence of HBsAg is required for diagnosis. Additionally, detecting IgM antibodies against the hepatitis B core antigen (IgM anti-HBc) is necessary to diagnose acute HBV/HDV coinfection.[21][22]
HDAg is detected early but is short-lived in acute HDV infection, often requiring repeated confirmation testing. Detection of anti-HDV is delayed in acute infection and may be the only means to diagnose acute HDV if other HDV infection markers are absent. The pattern of the IgM class of anti-HDV antibodies depends on the course of acute hepatitis D. If HDV infection is self-limited, the detection of anti-HDV IgM is transient and delayed.[21][23][24] If HDV infection progresses to chronicity, anti-HDV IgM is present in high titers and for a prolonged duration. Because anti-HDV IgM occurs in both acute and chronic HDV infections, it cannot be used to distinguish between them.[25][26]
Historically, HDAg detection was considered the gold standard for diagnosing active HDV infection. As anti-HDV antibodies form immune complexes with HDAg, detecting HDAg via the required immunoblot assay is difficult and time-consuming. Therefore, HDV RNA detection via reverse transcriptase–polymerase chain reaction is the most sensitive and practical test for detecting active HDV infection.[27][28]
High-risk individuals (intravenous drug users, individuals from HDV-endemic areas) or those with a severe course and who have acute hepatitis B may have HDV coinfection. Patients with coinfection have high titers of IgM anti-HBc. In these individuals, HDV biomarkers can rise before or after HBV biomarkers. Occasionally, patients who present during the second phase of biphasic hepatitis seroconvert to anti-HBs, but may still have a positive result for high-titer IgM anti-HBc.
When the etiology of hepatitis is undetermined in chronic HBV carriers, HDV testing should be performed to exclude acute HDV superinfection. Distinguishing between HDV superinfection and HBV/HDV coinfection can be difficult when superinfection occurs in undiagnosed chronic HBV carriers. In cases of superinfection, HBsAg and HDV RNA remain detectable without IgM anti-HBc. Notably, patients with undetected chronic HBV are at risk of missed diagnosis of HDV if they present with acute symptoms or flares.
HDV testing should be considered in high-risk individuals with chronic hepatitis B to rule out concurrent chronic HDV infection. Coinfection can be diagnosed by detecting total anti-HDV antibodies, followed by confirmatory staining for HDAg in liver tissues or measuring serum HDV RNA. Because HBV replication is suppressed in chronic HDV infection, hepatitis B e-antibodies are typically present. Additionally, testing for hepatitis C, hepatitis A, and other causes of acute and chronic liver injury should be considered.
Treatment / Management
While no treatments are available for acute HDV infection, per the European Association for the Study of the Liver guidelines, chronic hepatitis D infection requires treatment.[29] Serum HBsAg, HDV RNA, anti-HDV antibodies, elevated liver enzymes, or evidence of chronic liver damage define chronic disease. Although not approved by the US Food and Drug Administration for chronic HDV, interferon alpha (IFN-α) has shown benefit in most clinical trials.[30] Expert guidelines recommend the pegylated form of IFN-α. IFN-α is available for off-label use in most countries for a 48-week course.[31][32] Decompensated liver disease is a contraindication because of the risk of further deterioration of liver function and opportunistic infection.(A1)
Bulevirtide is an entry inhibitor that blocks sodium taurocholate cotransporting polypeptide (NTCP) receptor–mediated viral entry. Based on the trials in phases 2 and 3, this medication has been granted conditional approval in Europe.[33][34][33] Lonafarnib inhibits HDV assembly and is also being tested in late-stage clinical trials.[35] Given the lack of promising evidence, nucleotide analogues are not currently recommended to treat chronic hepatitis D infection. Tobevibart (VIR-3434) targets the antigenic loop of HBsAg, neutralizes HBV/HDV entry while reducing HBsAg levels, and is currently in clinical trials.[36] RNA interference therapies, such as JNJ-3989 and elecsiran, degrade HBV transcripts, including HBsAg messenger RNA, thereby indirectly inhibiting HDV replication. Results from the MARCH study found that elebsiran combined with pegylated IFN-α demonstrated robust HBsAg and HDV RNA suppression, supporting continued clinical investigation.[37][38](A1)
The goal of treatment is suppression of HDV replication, demonstrated by the undetectable HDV RNA in serum and HDAg in the liver. The ideal endpoint would be clearance of HBsAg. Acceptable endpoints include alanine aminotransferase level normalization and greater than 2 log HDV RNA decline at treatment completion. As measured by HDV RNA, Virological response should ideally be assessed every 6 months during treatment and yearly thereafter.[29] HDV RNA suppression below the lower limit of quantification serves as an alternative therapeutic target, necessitating sustained virologic monitoring and individualized management.[39] Continuous HDV RNA suppression over 48 weeks for maintenance therapy minimizes hepatic inflammation and slows disease progression.(A1)
In cases of decompensated liver disease, liver transplant is the only viable option.[40] However, there is a high risk of recurrence of HDV infection, so hepatitis B immunoglobulin and nucleotide analogues are strongly recommended for allograft recipients posttransplant.[29] The level of hepatitis B immunoglobulin should be maintained above 100 mIU/mL after liver transplant.[29](A1)
Differential Diagnosis
The differential diagnoses for HDV include the following:
- Alcohol-associated hepatitis
- Autoimmune hepatitis
- Budd-Chiari syndrome
- Cholangitis
- Cholecystitis
- Hepatitis A virus infection
- Hepatitis B virus infection
- Hepatitis C virus infection
- Liver abscess
Prognosis
In patients of HDV-HBV coinfection, the risk of deterioration is greater than in those with HBV infection alone.[41] When HDV superinfects patients with chronic HBV, it most commonly results in chronic HDV infection; however, in a minority of patients, spontaneous resolution occurs in 20% to 30%. Approximately two-thirds of chronically infected individuals develop cirrhosis, and hepatocellular carcinoma may develop within 5 to 10 years.[42]
Complications
Acute HDV infection is associated with a greater risk of progression to acute liver failure. Chronic HDV infection increases the risk of cirrhosis compared with chronic HBV infection. Complications of decompensated cirrhosis include hepatic encephalopathy, variceal bleeding, ascites, and spontaneous bacterial peritonitis. Furthermore, the risk of hepatocellular carcinoma may also be increased.
Deterrence and Patient Education
HDV represents a severe hepatic infection that occurs exclusively in individuals with concurrent hepatitis B virus (HBV) infection. Patients should be educated on primary prevention strategies, including HBV vaccination, avoidance of percutaneous exposure through contaminated needles, and adherence to safe sexual practices.
Clinical guidelines recommend systematic HDV screening for all patients with HBV infection, with an emphasis on individuals presenting with high-risk epidemiological factors or unexplained hepatic dysfunction. Patients should be educated that early identification coupled with appropriate lifestyle interventions, including abstinence from alcohol and hepatotoxic agents, can mitigate hepatic injury progression and optimize clinical outcomes.
Pearls and Other Issues
The following are key points that clinicians should keep in mind regarding HDV:
- Because HDV depends on HBV, prevention is achieved with HBV vaccination. If an individual is immune to HBV, they are subsequently protected against HDV. Patients at risk of contracting HDV infection should be encouraged to receive the hepatitis B vaccine.
- Patients with unexplained acute flares of hepatitis and those with rapid progression to cirrhosis should be screened for HDV.
- Based on the most recent European Association for the Study of the Liver guidelines, screening for HDV should be performed at least once in all patients with positive HBsAg testing.[29]
- Retesting may be considered yearly in patients who remain at risk for infection.
Enhancing Healthcare Team Outcomes
Effective management of hepatitis D virus infection requires a comprehensive approach integrating clinical skills, ethical responsibilities, and coordinated strategies across the interprofessional team. Clinicians apply diagnostic and therapeutic expertise, while nurses provide patient education and monitoring to ensure adherence and safety. Pharmacists contribute by optimizing antiviral regimens, counseling on adverse effects, and reviewing drug–drug interactions.
Ethical responsibilities include maintaining transparency in prognosis, ensuring informed consent, and addressing health disparities in high-risk populations. Communication among clinicians, nurses, pharmacists, and other healthcare professionals supports the timely identification of disease progression, coordinated care transitions, and the integration of preventive strategies, such as hepatitis B vaccination. This interprofessional collaboration enhances patient-centered care, improves outcomes, minimizes treatment-related risks, and strengthens overall team performance in managing HDV.
Media
(Click Image to Enlarge)
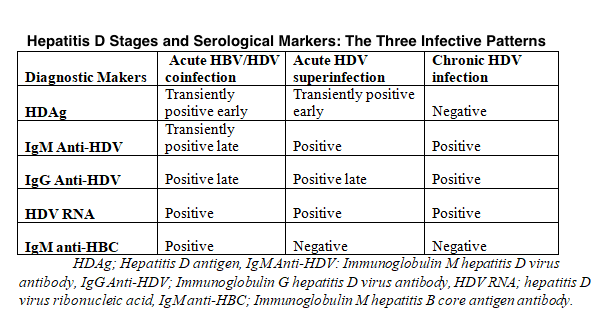
Hepatitis D Stages, Serological Markers, and the 3 Infection Patterns. The 3 infection patterns have different HDV RNA, HDAg, anti-HDV antibody, and HBV biomarker levels.
Contributed by U Masood, MD
References
Rizzetto M, Canese MG, Gerin JL, London WT, Sly DL, Purcell RH. Transmission of the hepatitis B virus-associated delta antigen to chimpanzees. The Journal of infectious diseases. 1980 May:141(5):590-602 [PubMed PMID: 6989929]
Level 3 (low-level) evidencePolson AG, Bass BL, Casey JL. RNA editing of hepatitis delta virus antigenome by dsRNA-adenosine deaminase. Nature. 1996 Apr 4:380(6573):454-6 [PubMed PMID: 8602246]
Level 3 (low-level) evidenceNegro F, Lok AS. Hepatitis D: A Review. JAMA. 2023 Dec 26:330(24):2376-2387. doi: 10.1001/jama.2023.23242. Epub [PubMed PMID: 37943548]
Patel EU, Thio CL, Boon D, Thomas DL, Tobian AAR. Prevalence of Hepatitis B and Hepatitis D Virus Infections in the United States, 2011-2016. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2019 Aug 1:69(4):709-712. doi: 10.1093/cid/ciz001. Epub [PubMed PMID: 30605508]
Liaw YF, Chiu KW, Chu CM, Sheen IS, Huang MJ. Heterosexual transmission of hepatitis delta virus in the general population of an area endemic for hepatitis B virus infection: a prospective study. The Journal of infectious diseases. 1990 Nov:162(5):1170-2 [PubMed PMID: 2121838]
Weisfuse IB, Hadler SC, Fields HA, Alter MJ, O'Malley PM, Judson FN, Ostrow DG, Altman NL. Delta hepatitis in homosexual men in the United States. Hepatology (Baltimore, Md.). 1989 Jun:9(6):872-4 [PubMed PMID: 2714738]
Gaeta GB, Stroffolini T, Chiaramonte M, Ascione T, Stornaiuolo G, Lobello S, Sagnelli E, Brunetto MR, Rizzetto M. Chronic hepatitis D: a vanishing Disease? An Italian multicenter study. Hepatology (Baltimore, Md.). 2000 Oct:32(4 Pt 1):824-7 [PubMed PMID: 11003629]
Level 2 (mid-level) evidenceStark DL, Falekun S, Jorgensen S, Slev P. Prevalence of Hepatitis D in the United States. The journal of applied laboratory medicine. 2025 Sep 3:10(5):1133-1139. doi: 10.1093/jalm/jfaf092. Epub [PubMed PMID: 40626720]
Wedemeyer H, Manns MP. Epidemiology, pathogenesis and management of hepatitis D: update and challenges ahead. Nature reviews. Gastroenterology & hepatology. 2010 Jan:7(1):31-40. doi: 10.1038/nrgastro.2009.205. Epub [PubMed PMID: 20051970]
Miao Z, Zhang S, Ou X, Li S, Ma Z, Wang W, Peppelenbosch MP, Liu J, Pan Q. Estimating the Global Prevalence, Disease Progression, and Clinical Outcome of Hepatitis Delta Virus Infection. The Journal of infectious diseases. 2020 Apr 27:221(10):1677-1687. doi: 10.1093/infdis/jiz633. Epub [PubMed PMID: 31778167]
Level 2 (mid-level) evidenceNegro F, Korba BE, Forzani B, Baroudy BM, Brown TL, Gerin JL, Ponzetto A. Hepatitis delta virus (HDV) and woodchuck hepatitis virus (WHV) nucleic acids in tissues of HDV-infected chronic WHV carrier woodchucks. Journal of virology. 1989 Apr:63(4):1612-8 [PubMed PMID: 2926865]
Level 3 (low-level) evidenceNi Y, Lempp FA, Mehrle S, Nkongolo S, Kaufman C, Fälth M, Stindt J, Königer C, Nassal M, Kubitz R, Sültmann H, Urban S. Hepatitis B and D viruses exploit sodium taurocholate co-transporting polypeptide for species-specific entry into hepatocytes. Gastroenterology. 2014 Apr:146(4):1070-83. doi: 10.1053/j.gastro.2013.12.024. Epub 2013 Dec 19 [PubMed PMID: 24361467]
Level 3 (low-level) evidenceSmedile A, Farci P, Verme G, Caredda F, Cargnel A, Caporaso N, Dentico P, Trepo C, Opolon P, Gimson A, Vergani D, Williams R, Rizzetto M. Influence of delta infection on severity of hepatitis B. Lancet (London, England). 1982 Oct 30:2(8305):945-7 [PubMed PMID: 6127458]
Smedile A, Dentico P, Zanetti A, Sagnelli E, Nordenfelt E, Actis GC, Rizzetto M. Infection with the delta agent in chronic HBsAg carriers. Gastroenterology. 1981 Dec:81(6):992-7 [PubMed PMID: 7286594]
Level 2 (mid-level) evidenceBichko V, Netter HJ, Wu TT, Taylor J. Pathogenesis associated with replication of hepatitis delta virus. Infectious agents and disease. 1994 Apr-Jun:3(2-3):94-7 [PubMed PMID: 7812659]
Level 3 (low-level) evidenceRomeo R, Del Ninno E, Rumi M, Russo A, Sangiovanni A, de Franchis R, Ronchi G, Colombo M. A 28-year study of the course of hepatitis Delta infection: a risk factor for cirrhosis and hepatocellular carcinoma. Gastroenterology. 2009 May:136(5):1629-38. doi: 10.1053/j.gastro.2009.01.052. Epub 2009 Jan 29 [PubMed PMID: 19208358]
Niro GA, Smedile A, Andriulli A, Rizzetto M, Gerin JL, Casey JL. The predominance of hepatitis delta virus genotype I among chronically infected Italian patients. Hepatology (Baltimore, Md.). 1997 Mar:25(3):728-34 [PubMed PMID: 9049226]
Level 3 (low-level) evidenceWu JC, Choo KB, Chen CM, Chen TZ, Huo TI, Lee SD. Genotyping of hepatitis D virus by restriction-fragment length polymorphism and relation to outcome of hepatitis D. Lancet (London, England). 1995 Oct 7:346(8980):939-41 [PubMed PMID: 7564729]
Casey JL, Brown TL, Colan EJ, Wignall FS, Gerin JL. A genotype of hepatitis D virus that occurs in northern South America. Proceedings of the National Academy of Sciences of the United States of America. 1993 Oct 1:90(19):9016-20 [PubMed PMID: 8415646]
Level 3 (low-level) evidencePalom A, Rodríguez-Tajes S, Navascués CA, García-Samaniego J, Riveiro-Barciela M, Lens S, Rodríguez M, Esteban R, Buti M. Long-term clinical outcomes in patients with chronic hepatitis delta: the role of persistent viraemia. Alimentary pharmacology & therapeutics. 2020 Jan:51(1):158-166. doi: 10.1111/apt.15521. Epub 2019 Nov 13 [PubMed PMID: 31721254]
Level 2 (mid-level) evidenceAragona M, Macagno S, Caredda F, Crivelli O, Lavarini C, Maran E, Farci P, Purcell RH, Rizzetto M. Serological response to the hepatitis delta virus in hepatitis D. Lancet (London, England). 1987 Feb 28:1(8531):478-80 [PubMed PMID: 2881041]
Xavier SR, Dos Santos Barcelos IC, Gandra IB, Pereira SP, Ribeiro AJ, Silva KA, Resende CAA, da Silva Lopes L, Machado RCR, Silva LMS, Silva LS, Ferreira LC, de Souza LFA, Souza RB, Passos-Silva AM, da Paz MC, Fumagalli MAC, Coelho EAF, Giunchetti RC, Machado JM, Gonçalves AAM, Dos Santos Pereira S, da Matta DA, Souza Vieira D, Galdino AS. Proteins and peptides as antigen candidates for the immunodiagnosis of hepatitis D. Amino acids. 2025 Jul 4:57(1):35. doi: 10.1007/s00726-025-03465-2. Epub 2025 Jul 4 [PubMed PMID: 40613912]
Shattock AG, Morgan BM. Sensitive enzyme immunoassay for the detection of delta antigen and anti-delta, using serum as the delta antigen source. Journal of medical virology. 1984:13(1):73-82 [PubMed PMID: 6363622]
Buti M, Esteban R, Jardí R, Esteban JI, Guardia J. Serological diagnosis of acute delta hepatitis. Journal of medical virology. 1986 Jan:18(1):81-5 [PubMed PMID: 3944592]
Bonino F, Heermann KH, Rizzetto M, Gerlich WH. Hepatitis delta virus: protein composition of delta antigen and its hepatitis B virus-derived envelope. Journal of virology. 1986 Jun:58(3):945-50 [PubMed PMID: 3701932]
Level 3 (low-level) evidenceButi M, Esteban R, Jardi R, Rodriguez-Frias F, Casacuberta J, Esteban JI, Allende E, Guardia J. Chronic delta hepatitis: detection of hepatitis delta virus antigen in serum by immunoblot and correlation with other markers of delta viral replication. Hepatology (Baltimore, Md.). 1989 Dec:10(6):907-10 [PubMed PMID: 2583685]
Dinolfo L, Abate ML, Bertolo P, Bosio P, Rosina F, Cavicchini A, Rizzetto M, Negro F. Detection of hepatitis D virus RNA in serum by a reverse transcription, polymerase chain reaction-based assay. International journal of clinical & laboratory research. 1995:25(1):35-9 [PubMed PMID: 7787208]
Level 3 (low-level) evidenceMederacke I, Bremer B, Heidrich B, Kirschner J, Deterding K, Bock T, Wursthorn K, Manns MP, Wedemeyer H. Establishment of a novel quantitative hepatitis D virus (HDV) RNA assay using the Cobas TaqMan platform to study HDV RNA kinetics. Journal of clinical microbiology. 2010 Jun:48(6):2022-9. doi: 10.1128/JCM.00084-10. Epub 2010 Mar 29 [PubMed PMID: 20351206]
European Association for the Study of the Liver. EASL Clinical Practice Guidelines on hepatitis delta virus. Journal of hepatology. 2023 Aug:79(2):433-460. doi: 10.1016/j.jhep.2023.05.001. Epub 2023 Jun 24 [PubMed PMID: 37364791]
Level 1 (high-level) evidenceAbbas Z, Khan MA, Salih M, Jafri W. Interferon alpha for chronic hepatitis D. The Cochrane database of systematic reviews. 2011 Dec 7:2011(12):CD006002. doi: 10.1002/14651858.CD006002.pub2. Epub 2011 Dec 7 [PubMed PMID: 22161394]
Level 1 (high-level) evidenceSandmann L, Wedemeyer H. Interferon-based treatment of chronic hepatitis D. Liver international : official journal of the International Association for the Study of the Liver. 2023 Aug:43 Suppl 1():69-79. doi: 10.1111/liv.15410. Epub 2022 Sep 2 [PubMed PMID: 36002390]
Ouranos K, Mylona EK, Dellis C, Bakaloudi DR, Shehadeh F, Noureddin M, Kalligeros M, Mylonakis E. Comparative Efficacy of Treatment Regimens for Chronic Hepatitis D Virus Infection: A Systematic Review and Network Meta-Analysis. Liver international : official journal of the International Association for the Study of the Liver. 2025 Aug:45(8):e70232. doi: 10.1111/liv.70232. Epub [PubMed PMID: 40668572]
Level 1 (high-level) evidenceAsselah T, Chulanov V, Lampertico P, Wedemeyer H, Streinu-Cercel A, Pântea V, Lazar S, Placinta G, Gherlan GS, Bogomolov P, Stepanova T, Morozov V, Syutkin V, Sagalova O, Manuilov D, Mercier RC, Ye L, Da BL, Chee G, Lau AH, Osinusi A, Bourliere M, Ratziu V, Pol S, Hilleret MN, Zoulim F. Bulevirtide Combined with Pegylated Interferon for Chronic Hepatitis D. The New England journal of medicine. 2024 Jul 11:391(2):133-143. doi: 10.1056/NEJMoa2314134. Epub 2024 Jun 6 [PubMed PMID: 38842520]
Lampertico P, Bogomolov PO, Chulanov V, Stepanova T, Morozov V, Allweiss L, Dandri M, Burhenne J, Blank A, Ciesek S, Elsner C, Dittmer U, An Q, Manuilov D, Da BL, Flaherty JF, Urban S, Wedemeyer H. Phase 2 Randomised Study of Bulevirtide as Monotherapy or Combined With Peg-IFNα-2a as Treatment for Chronic Hepatitis Delta. Liver international : official journal of the International Association for the Study of the Liver. 2025 Feb:45(2):e70008. doi: 10.1111/liv.70008. Epub [PubMed PMID: 39853842]
Level 1 (high-level) evidenceYurdaydin C, Keskin O, Yurdcu E, Çalişkan A, Önem S, Karakaya F, Kalkan Ç, Karatayli E, Karatayli S, Choong I, Apelian D, Koh C, Heller T, Idilman R, Bozdayi AM, Glenn JS. A phase 2 dose-finding study of lonafarnib and ritonavir with or without interferon alpha for chronic delta hepatitis. Hepatology (Baltimore, Md.). 2022 Jun:75(6):1551-1565. doi: 10.1002/hep.32259. Epub 2021 Dec 23 [PubMed PMID: 34860418]
Lempp FA, Volz T, Cameroni E, Benigni F, Zhou J, Rosen LE, Noack J, Zatta F, Kaiser H, Bianchi S, Lombardo G, Jaconi S, Vincenzetti L, Imam H, Soriaga LB, Passini N, Belnap DM, Schulze A, Lütgehetmann M, Telenti A, Cathcart AL, Snell G, Purcell LA, Hebner CM, Urban S, Dandri M, Corti D, Schmid MA. Potent broadly neutralizing antibody VIR-3434 controls hepatitis B and D virus infection and reduces HBsAg in humanized mice. Journal of hepatology. 2023 Nov:79(5):1129-1138. doi: 10.1016/j.jhep.2023.07.003. Epub 2023 Jul 17 [PubMed PMID: 37459920]
Park J, Sayed A, Nasir SA, Lim JK. Advances in treatment of hepatitis delta virus infection: Update on novel investigational drugs. World journal of virology. 2025 Jun 25:14(2):102673. doi: 10.5501/wjv.v14.i2.102673. Epub [PubMed PMID: 40575639]
Level 3 (low-level) evidenceZhou J, Kaiser H, Rocha E, Terrell AN, Corti D, Purcell LA, Lempp FA, Puschnik AS. Therapy with murinized tobevibart and elebsiran is efficacious in a liver-chimeric mouse model of HDV infection. JHEP reports : innovation in hepatology. 2025 Jun:7(6):101400. doi: 10.1016/j.jhepr.2025.101400. Epub 2025 Mar 22 [PubMed PMID: 40486136]
Ghany MG, Buti M, Lampertico P, Lee HM, 2022 AASLD-EASL HBV-HDV Treatment Endpoints Conference Faculty. Guidance on treatment endpoints and study design for clinical trials aiming to achieve cure in chronic hepatitis B and D: Report from the 2022 AASLD-EASL HBV-HDV Treatment Endpoints Conference. Journal of hepatology. 2023 Nov:79(5):1254-1269. doi: 10.1016/j.jhep.2023.06.002. Epub 2023 Jun 21 [PubMed PMID: 37377088]
Muhammad H, Tehreem A, Hammami MB, Ting PS, Idilman R, Gurakar A. Hepatitis D virus and liver transplantation: Indications and outcomes. World journal of hepatology. 2021 Mar 27:13(3):291-299. doi: 10.4254/wjh.v13.i3.291. Epub [PubMed PMID: 33815673]
Caviglia GP, Ciancio A, Rizzetto M. A Review of HDV Infection. Viruses. 2022 Aug 10:14(8):. doi: 10.3390/v14081749. Epub 2022 Aug 10 [PubMed PMID: 36016371]
Chang TE, Su CW, Huang YS, Huang YH, Hou MC, Wu JC. Hepatitis D virus dual infection increased the risk of hepatocellular carcinoma compared with hepatitis B virus mono infection: A meta-analysis. Journal of the Chinese Medical Association : JCMA. 2022 Jan 1:85(1):30-41. doi: 10.1097/JCMA.0000000000000606. Epub [PubMed PMID: 35006125]
Level 1 (high-level) evidence