Definition/Introduction
A common definition of aerospace medicine is the study of normal physiology in an abnormal environment. A subspecialty of occupational medicine, aerospace medicine is challenged by the need to safeguard the health of individuals working in a dynamic atmosphere characterized by decreasing pressure and oxygen content, coupled with increasing altitude. Comprehension of physical changes occurring during ascent from sea level is essential for addressing the medical needs of pilots, aircrew, and aircraft passengers. Understanding chemical gas laws that describe the behavior of atmospheric gases, as well as gases within the human body, is critical to the practice of aerospace medicine. Henry’s law is one of the most pertinent gas laws in aerospace medicine. Named after the English physician William Henry, Henry’s law defines the relationship between the partial pressure of gases overlying a solution and the gases’ ability to dissolve in that solution.[1]
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
Henry’s law states that, when a gaseous mixture (eg, the atmosphere) is in contact with a solution, the amount of gas dissolved in the solution is directly proportional to the partial pressure of that gas. "Gas partial pressure" refers to the portion of total pressure contributed by that gas within a gas mixture. According to Henry’s law, an increase in gas pressure over a liquid results in a proportional increase in the amount of gas dissolved in the liquid. Conversely, a decrease in gas pressure results in a reduction in dissolved gas within the solution.
Henry’s law is demonstrated by opening a newly pressurized soda bottle. Upon removal of the cap, the carbon dioxide-rich gas phase in contact with the liquid surface rapidly escapes, resulting in a precipitous drop in gas pressure. Consequently, dissolved carbon dioxide decreases, and gas comes out of solution as bubbles and foam. Maintenance of adequate gas pressure over a liquid preserves dissolved gases within the solution.[2][3] Presented as a formula, Henry’s law can be written as follows:
P1 / A1 = P2 / A2
The left side shows the ratio of P1, the initial partial pressure of a gas overlying a solution, to A1, the corresponding amount of gas dissolved in the solution at that pressure. The right side shows the ratio of P2, the partial pressure of the same gas at a different condition, to A2, the corresponding amount of dissolved gas at this new pressure. Equality between both sides indicates that a change in P2 is accompanied by a proportional change in A2.
Blood functions as a solution containing multiple dissolved gases. These gases remain in solution (ie, blood) at sea level. Ambient air at sea level is composed of approximately 78.1% nitrogen, 21% oxygen, 0.9% argon, 0.04% carbon dioxide, and trace gases. However, arterial blood gas partial pressures do not solely reflect atmospheric composition. Arterial oxygen partial pressure (PaO2) is typically approximately 95 mm Hg, lower than atmospheric oxygen tension due to ventilation–perfusion relationships, while arterial carbon dioxide partial pressure (PaCO2) is approximately 40 mm Hg, substantially higher than the negligible carbon dioxide concentration in ambient air.
Ambient atmospheric pressure decreases as altitude increases. In accordance with Henry’s law, the amount of gas that can remain dissolved in blood decreases proportionally. Rapid ascent may result in supersaturation of dissolved gases, particularly nitrogen, which is metabolically inert and not consumed by tissues, leading to intravascular bubble formation similar to the soda bottle example.
A distinction is required between this altitude-related mechanism and the more commonly described decompression sickness associated with scuba diving. Nitrogen is inhaled under elevated ambient pressure at depth during diving, resulting in increased dissolution of this gas in blood and tissues compared with sea level conditions. Ambient pressure decreases sharply during rapid ascent, and supersaturated nitrogen leaves the solution as bubbles. The soda bottle analogy corresponds most directly to the diving scenario.
The mechanism is reversed at altitude. Ambient pressure falls below the equilibrium pressure at which blood gases were previously dissolved, promoting bubble formation without prior high-pressure gas loading. Oxygen may theoretically come out of solution at altitude. However, most oxygen in blood is bound to hemoglobin, and unbound oxygen is rapidly consumed by tissue metabolism, making clinically significant oxygen bubble formation unlikely.[4]
Nitrogen bubbles within the vascular system can result in various forms of "decompression illness," a term encompassing both the discomfort associated with decompression sickness and more severe conditions such as arterial gas embolism. Partial mitigation of this risk is achieved through cabin pressurization. In addition, gradual rates of ascent reduce the likelihood of supersaturation and subsequent bubble formation. Controlled ascent profiles and cabin pressurization largely explain the absence of clinically significant bubble formation during commercial airline flights.
In most commercial and military fixed-wing aircraft, cabin pressurization is typically maintained at a level equivalent to an altitude of approximately 8,000 ft (2,438 m). Unpressurized flight up to 10,000 ft (3,048 m) is generally considered acceptable, although supplemental oxygen is typically recommended above this threshold, with regulatory requirements varying by jurisdiction and aircraft type. Unpressurized flight above 12,000 ft (3,658 m) is generally discouraged.
Henry’s law has limitations. The validity of this principle is greatest at low gas concentrations and decreases at higher concentrations, where nonideal gas-solution interactions may reduce accuracy (see Image. Graphical Representation of Henry's Law). [Source: Sander et al. Henry’s law constants (IUPAC Recommendations 2021). 2021]
Clinical Significance
Henry’s law is relevant to aerospace medicine in several ways. Notably, this law accurately describes the phenomena underlying decompression illness and provides a framework for the measures used in the treatment of these conditions.
Although Henry’s law applies to both aerospace and underwater medicine, manifestations in flight do not perfectly correspond to those observed underwater. Manifestations such as decompression sickness are directly related to absolute altitude achieved and duration of exposure. Cabin pressurization reduces the effects of decompression illness and permits pilots and crew members to operate at altitude without the full physiologic consequences of ambient pressure reduction. High-altitude flight in pressurized aircraft remains subject to operational constraints. These constraints arise primarily from structural and aerodynamic limitations, the risk of hypoxia following rapid decompression, and equipment considerations, rather than nitrogen supersaturation risk alone. At sufficiently high altitudes, even pressurized cabins cannot fully prevent inert gas supersaturation, and this factor remains relevant in the design of high-altitude operational protocols.
Current data suggest that aircrew and passengers in a pressurized cabin are less likely to experience decompression illness at exposures equivalent to altitudes below 18,000 ft (5,486 m).[5] This threshold is not absolute. Individual risk varies with factors that include prior dive history, physical exertion at altitude, age, presence of a patent foramen ovale, and hydration status. In civilian and military aviation, risk reduction for decompression illness is more challenging in rotor-wing and helicopter operations among pilots and crew. These aircraft have operational requirements that generally preclude cabin pressurization and, therefore, operate at lower altitudes to limit physiologic consequences of inert gas supersaturation.
Several interventions with effects governed by Henry’s law are effective in preventing and managing altitude-related conditions. Breathing gas mixtures used in high-altitude aircraft typically contain higher oxygen concentrations than ambient air, serving 2 purposes: prevention of hypoxia and promotion of denitrogenation. A diffusion gradient is established by reducing the inspired partial pressure of nitrogen. This gradient drives nitrogen movement from tissues and blood into the lungs, where exhalation occurs. Reduction of total body nitrogen burden decreases the risk of supersaturation at altitude. The same principle underlies the recommendation for oxygen mask use during airline emergencies involving compromised cabin pressurization. Cabin pressurization remains the primary preventive measure for reducing decompression risk.
Additionally, Henry’s law has broader clinical significance in aerospace medicine beyond decompression illness. Henry’s law describes the solubility behavior of oxygen and carbon dioxide and underlies principles of gas exchange and tissue oxygenation. Identification of tissues most susceptible to bubble formation, including the central nervous system and joints, is based in part on this principle. The equation informs pre-breathing protocols before high-altitude or extravehicular operations, operational planning to minimize altitude exposure risks, and the design of aircraft cabin pressurization systems to maintain safe inert gas levels. Henry’s law also guides practices in hyperbaric medicine and spaceflight physiology, including the development of oxygen pre-breathing protocols for space suit use and airlock transitions.
Pulse oximetry provides a useful method for monitoring oxygenation and identifying hypoxia but does not measure inert gas saturation. In operational settings, inert gas burden is managed through pre-breathing protocols, altitude exposure limits, and ascent rate guidelines rather than real-time direct measurement. This limitation reflects the lack of widely available clinical tools for direct assessment of inert gas saturation.
The ideal approach to managing symptoms of in-flight bubble formation involves 3 principal steps. First, altitude reduction should occur as rapidly and safely as possible, ideally to sea level. Second, administration of therapeutic supplemental oxygen should be initiated. Supplemental oxygen eliminates nitrogen from the inspired gas mixture and establishes a diffusion gradient that accelerates nitrogen elimination from tissues and blood, thereby reducing supersaturation and driving bubble formation. Finally, landing should be prioritized to allow evaluation by a flight surgeon to determine whether further intervention is required.
Prompt transfer to a hyperbaric chamber should be strongly considered if symptoms persist or significant central nervous system manifestations are present. Hyperbaric therapy increases the ambient pressure surrounding the patient, which, in accordance with Henry’s law, promotes the dissolution of nitrogen bubbles back into solution within the bloodstream. The decision to pursue hyperbaric oxygen therapy depends on symptom severity, classification of decompression illness as type I or II, and facility availability, and should be guided by a flight surgeon assessment.[6][7]
Nursing, Allied Health, and Interprofessional Team Interventions
Effective management of decompression illness and altitude-related conditions requires a coordinated, interprofessional approach in which all team members share a foundational understanding of the underlying physiology. Nursing staff are often the first to assess and monitor patients presenting with decompression-related symptoms. Working knowledge of Henry’s law enables recognition of clinically significant changes, including evolving neurological deficits, joint pain, or cardiopulmonary compromise, and supports accurate, efficient communication with the treating physician or advanced practitioner. Timely and precise communication of symptom onset, altitude or dive exposure history, and symptom progression is critical, as delays in recognition or clinical handoff can significantly worsen outcomes in conditions such as arterial gas embolism or type II decompression sickness.
Advanced practitioners, including physician assistants and nurse practitioners, may independently manage initial stabilization, administer supplemental oxygen, and coordinate transfer to hyperbaric facilities, particularly in austere or remote environments where physician availability is limited. Application of Henry’s law informs clinical decision-making related to oxygen therapy, altitude restriction counseling, and referral thresholds.
Pharmacists contribute meaningfully to the interprofessional team by ensuring appropriate availability of adjunct medications used in decompression illness management, including analgesics, antiplatelet agents, and intravenous fluids, and by providing counseling on drug interactions relevant to hyperbaric oxygen therapy. Pharmacists also educate patients regarding medications that may alter gas solubility or increase the risk of decompression-related injury.
Ethical and professional obligations require all team members to maintain competency in physiological principles relevant to their scope of practice, advocate for patient safety in high-risk operational environments, and support a culture of open interprofessional communication. Clinical responsibilities include prompt escalation of concerns in the setting of worsening symptoms and avoidance of anchoring bias toward benign diagnoses when relevant exposure histories are present.
Care coordination is particularly important in decompression illness, given the frequent need for rapid transfer to specialized hyperbaric facilities. A clear chain of communication between flight surgeons, emergency physicians, hyperbaric medicine specialists, nursing staff, and transport teams is essential to minimize treatment delays. Implementation of pre-established transfer protocols and clear delineation of roles directly improve patient safety and outcomes. Regular interprofessional simulation training involving decompression illness scenarios further enhances team performance and reduces response time during real clinical events.
Media
(Click Image to Enlarge)
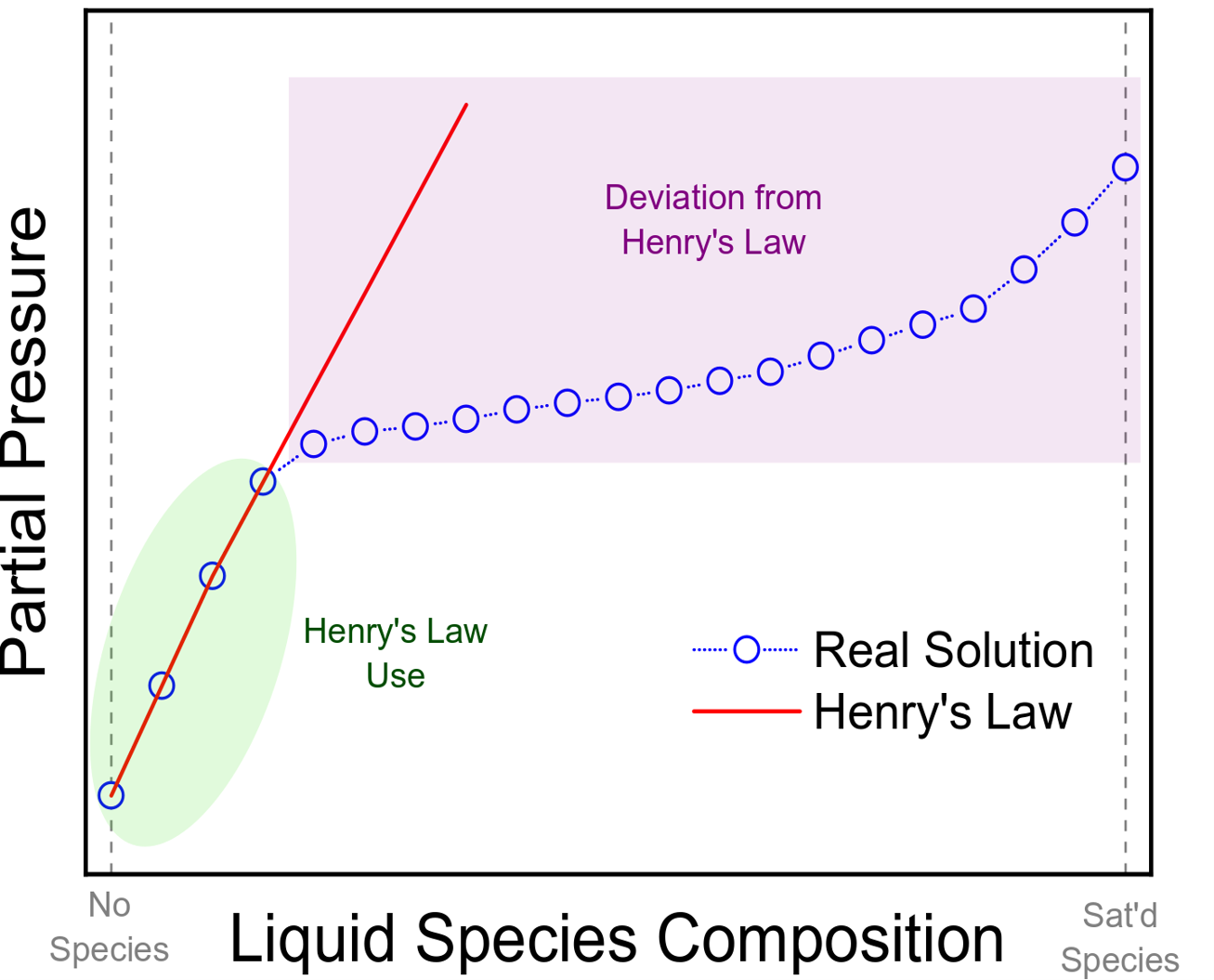
Graphical Representation of Henry's Law. This plot demonstrates the relationship between partial pressure and liquid species composition, highlighting the linear range where Henry's law remains applicable. The data points illustrate how real solutions begin to diverge from the ideal behavior predicted by the law as concentration increases. Specifically, Henry’s law is valid at low solute concentrations but is not applicable at higher concentrations.
Contributed by KM Tenny, PhD, MS
References
Ferraro G , Jadhav AJ , Barigou M . A Henry's law method for generating bulk nanobubbles. Nanoscale. 2020 Aug 7:12(29):15869-15879. doi: 10.1039/d0nr03332d. Epub 2020 Jul 22 [PubMed PMID: 32696779]
Liger-Belair G, Cilindre C. How Many CO(2) Bubbles in a Glass of Beer? ACS omega. 2021 Apr 13:6(14):9672-9679. doi: 10.1021/acsomega.1c00256. Epub 2021 Mar 31 [PubMed PMID: 33869947]
Ahmed Khaireh M, Liger-Belair G, Bonhommeau DA. Toward In Silico Prediction of CO(2) Diffusion in Champagne Wines. ACS omega. 2021 May 4:6(17):11231-11239. doi: 10.1021/acsomega.0c06275. Epub 2021 Apr 20 [PubMed PMID: 34056278]
Storz JF, Bautista NM. Altitude acclimatization, hemoglobin-oxygen affinity, and circulatory oxygen transport in hypoxia. Molecular aspects of medicine. 2022 Apr:84():101052. doi: 10.1016/j.mam.2021.101052. Epub 2021 Dec 5 [PubMed PMID: 34879970]
Ånell R, Grönkvist M, Gennser M, Eiken O. High-altitude decompression strain can be reduced by an early excursion to moderate altitude while breathing oxygen. European journal of applied physiology. 2021 Nov:121(11):3225-3232. doi: 10.1007/s00421-021-04794-2. Epub 2021 Aug 19 [PubMed PMID: 34410475]
Mitchell SJ. Decompression illness: a comprehensive overview. Diving and hyperbaric medicine. 2024 Mar 31:54(1Suppl):1-53. doi: 10.28920/dhm54.1.suppl.1-53. Epub [PubMed PMID: 38537300]
Level 3 (low-level) evidenceLe DQ, Dayton PA, Tillmans F, Freiberger JJ, Moon RE, Denoble P, Papadopoulou V. Ultrasound in decompression research: fundamentals, considerations, and future technologies. Undersea & hyperbaric medicine : journal of the Undersea and Hyperbaric Medical Society, Inc. 2021 First Quarter:48(1):59-72. doi: 10.22462/01.03.2021.8. Epub [PubMed PMID: 33648035]