Introduction
Kidney failure is defined by an estimated glomerular filtration rate (eGFR) of less than 15 mL/min/1.73 m² and can be managed through kidney transplantation, hemodialysis, peritoneal dialysis, or supportive care. The term "dialysis" is derived from the Greek words dia, meaning "through," and lysis, meaning "loosening or splitting." Dialysis is a treatment for kidney failure that helps remove waste products and excess fluid from the blood while maintaining the proper balance of essential minerals for normal body function.[1]
Over 3.5 million people worldwide, including about 540,000 in the United States, receive dialysis for chronic kidney failure, with nearly 90% undergoing hemodialysis.[2][3] The end-stage renal disease (ESRD) burden is attributed mainly to diabetes mellitus and hypertension, besides rarer causes like polycystic kidney disease, obstructive nephropathy, and glomerulonephritis. Dialysis for kidney failure can be classified into 2 broad types: hemodialysis and peritoneal dialysis. Hemodialysis includes several modalities, eg, intermittent hemodialysis (IHD) and continuous renal replacement therapy (CRRT), while peritoneal dialysis relies on the patient’s peritoneum as a natural filter for waste removal. Determining the optimal timing for initiating long-term dialysis in patients with kidney disease remains uncertain, with considerable variation across health systems.[4]
According to the United States Renal Data System, the proportion of patients starting dialysis at an eGFR 10 mL/min/1.73 m² or greater rose from 13% in the mid-1990s to 43% in 2010, then declined slightly to 39% in 2015.[5] The IDEAL study in 2010 found that planned early initiation of dialysis at eGFR 10 to 14 mL/min/1.73 m² in stage V chronic kidney disease patients did not improve survival or clinical outcomes compared with late initiation at eGFR 5 to 7 mL/min/1.73 m².[6] In practice, most late-start patients (76%) began dialysis at a mean eGFR of 9.8 mL/min/1.73 m² due to symptoms, eg, uremia or fluid overload, indicating that clinical presentation often guides timing more than eGFR alone.[7] Guidelines differ internationally: the United Kingdom recommends dialysis initiation at eGFR 5 to 7 mL/min/1.73 m² or with symptom onset, whereas Japanese guidelines suggest continuing conservative treatment until eGFR falls below 8 mL/min/1.73 m², even if symptoms occur.[8][9]
The Renal Physicians Association identifies patients with 2 or more of the following characteristics—age 75 years or older, high comorbidity burden (modified Charlson Comorbidity Index ≥8), significant functional impairment (Karnofsky Performance Status <40), or severe chronic malnutrition (serum albumin <2.5 g/dL)—as having a poor prognosis. Patients in this population should understand that dialysis may not improve survival or functional status and carries burdens that can reduce quality of life. Mortality among dialysis patients predominantly results from cardiovascular causes, followed by sepsis.[NIH. End Stage Renal Disease: Chapter 5. End Stage Renal Disease: Chapter 5. 2020]
High cardiovascular mortality may relate to chronic inflammation, extracellular volume shifts, dystrophic vascular calcification, and altered cardiovascular dynamics during dialysis. The SHARP study demonstrated a 17% reduction in major atherosclerotic events among patients with chronic kidney disease (CKD) receiving simvastatin–ezetimibe therapy.[10] Hypertension contributes to ESRD risk both as a cause and consequence of CKD. Cardioprotective strategies, including beta-blockers, aspirin, and renin-angiotensin-aldosterone system inhibitors, are recommended based on individual cardiovascular risk. Effective interprofessional collaboration among physicians, nurses, pharmacists, and other healthcare professionals is critical to optimizing outcomes for patients with ESRD who require dialysis.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Dialysis involves the removal of solutes and excess fluid across a semipermeable membrane by the following 3 primary mechanisms:
- Diffusion: This involves the movement of dissolved particles from an area of high concentration to a low concentration across a semipermeable membrane. Diffusion promotes the movement of smaller particles and occurs most rapidly when the concentration gradient across the semipermeable membrane is highest. Increasing the dialyzer size, dialysate flow, or the blood flow increases the rate of diffusion.
- Convection: This mechanism occurs when dissolved particles pass across a semipermeable membrane due to a pressure gradient. Larger particles are restricted, while particles that are smaller than the pores of the membrane pass freely. The removed solution is isotonic to the original, as the particles and water move together.
- Ultrafiltration: The movement of water across a semipermeable membrane due to hydrostatic pressure. Convection occurs with ultrafiltration.
Dialysate solution is a sterile fluid that contains sodium, buffer (eg, bicarbonate), chloride, potassium, magnesium, calcium, and dextrose. Dialysate usually contains potassium levels lower than 4.0 mEq/L and no phosphate, as these are elevated in patients with renal failure. The osmolality of the solution is maintained close to the osmolality of blood to prevent hemolysis. It lacks low-molecular-weight waste products present in uremic blood. When a semipermeable membrane separates uremic blood and dialysate, the flux rate of waste solutes from blood to dialysate exceeds the back-flux from the dialysate to blood. Eventually, the concentrations of permeable waste products in the dialysate and the blood become equal with no further net removal of the waste products.
Modern hollow-fiber dialyzers are plastic cartridges containing thousands of thin capillary fibers with microscopic pores that allow water and small molecules to pass through. Dialyzers differ in surface area, permeability, volume required to prime the cartridge, and membrane composition. Selecting specific dialyzer characteristics enables tailoring the dialysis prescription to the patient's clinical needs.
During dialysis, a concentration gradient is maintained (and equilibrium avoided) by continuously refilling the dialyzer with fresh dialysate and replacing dialyzed blood with undialyzed blood. “Countercurrent” flow maximizes the concentration difference of waste products between blood and dialysate. The diffusion rate of a solute depends on the magnitude of the concentration gradient, the mass transfer coefficient of the membrane, and the membrane surface area. The transfer coefficient depends on membrane thickness, solute size, and flow conditions on both sides of the membrane.
The Kt/V was a parameter introduced by Gotch and Sargent through their National Cooperative Dialysis Study.[11] Kt/V is a dimensionless ratio obtained by dividing the amount of plasma cleared of urea (Kt) by the distribution volume of urea (V). The urea-free plasma volume is a product of K, which is blood urea clearance, and t, which is the dialysis session length. A Kt/V of less than 0.8 was associated with higher morbidity or treatment failure, whereas a Kt/V of more than 1.0 was associated with improved outcomes. A Kt/V of 1.0 implies that the total blood volume cleared during a session equals the urea distribution volume.
Indications
Hemodialysis initiation is needed in patients with the following indications:
- Uremia with complications, eg, encephalopathy, pericarditis, neuropathy, seizures, platelet dysfunction with severe bleeding, intractable nausea or vomiting
- Toxic ingestion (eg, salicylates, ethylene glycol, methanol, lithium, metformin, barbiturates) or metabolic derangements leading to the overproduction of endogenous toxins (eg, ammonia) [12][13][14][15]
- Dyselectrolytemia, especially hyperkalemia with plasma potassium concentration greater than 6.5 mEq/L or hyperkalemia with electrocardiogram (ECG) changes
- Refractory acidosis (pH <7.2 and refractory to bicarbonate or unable to give bicarbonate due to volume overload) or symptomatic acidosis (eg, arrhythmias)
- Fluid overload refractory to diuretic therapy
The IHD system allows for more rapid ultrafiltration than any other renal replacement modality, making it the preferred choice for managing severe volume overload. Patient tolerance of rapid fluid removal may limit its use. CRRT provides continuous ultrafiltration for critically ill patients, supporting cardiovascular stability and maintaining metabolic balance. Although CRRT removes solutes and fluids less efficiently than IHD, its continuous delivery prevents the fluctuations associated with intermittent therapy, allowing consistent administration of medications, nutrition, and blood products while preserving overall stability. CRRT can also serve as an adjunctive therapy for cytokine release syndrome unresponsive to tocilizumab or corticosteroids by facilitating the removal of proinflammatory cytokines, including IL-6, from the circulation.[16]
The National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative (KDOQI) 2015 update offers guidelines for hemodialysis adequacy. Patients reaching CKD stage 4 (eGFR 15–29 mL/min/1.73 m²) or those approaching maintenance dialysis should receive counseling on kidney failure and available treatment options, including kidney transplantation, home or in-center hemodialysis, peritoneal dialysis, or conservative management. Education should also extend to family members and caregivers. Initiation of maintenance dialysis should be based on the presence of signs or symptoms of kidney failure, eg, pruritus, acid-base or electrolyte abnormalities, serositis, volume or blood pressure dysregulation, progressive nutritional deterioration despite dietary intervention, or cognitive impairment, rather than on kidney function alone in asymptomatic individuals.[17]
Contraindications
An absolute contraindication to hemodialysis is the inability to secure vascular access, and relative contraindications include:
- Difficult vascular access
- Needle phobia
- Cardiac failure
- Coagulopathy
Modern techniques are employed in patients with extensive vascular disease to improve the establishment and salvage of vascular access. Relative contraindications, eg, needle aversion, can be overcome by careful use of local anesthetics and nursing encouragement. Severe coagulopathy complicates anticoagulation maintenance in the extracorporeal circuit.
When the patient clearly expresses a wish to decline dialysis treatment, the clinician is obliged to respect that decision. Nonetheless, the nephrologist must ensure adequate addressing of all reversible factors, eg, unfounded fears about the dialysis process or a depressive illness clouding judgment. In competent patients refusing dialysis, especially those with multiple comorbidities, a shift is made to conservative management using all proper treatments apart from dialysis.
In patients with an unacceptably poor quality of life, the initiation of hemodialysis may offer limited survival benefit, with a substantial proportion of their remaining life spent undergoing or recovering from dialysis sessions. Symptoms of these patients can be managed with medication (ie, analgesics) and diet. In addition, low doses of gabapentin or pregabalin can be used for severe itching and insomnia.
Equipment
The hemodialysis circuit consists of 4 components (see Image. Types of Hemodialysis Access).[18]
Prefilter Segment
The prefilter segment carries blood from the patient's vascular access to the hemofilter. This portion of the circuit includes the blood tubing, a blood pump, and pressure sensors. Blood is aspirated into the prefilter circuit by the negative pressure generated by the blood pump, which is continuously monitored by an arterial access pressure sensor. The pump then propels blood through the hemofilter by creating positive pressure downstream of the pump. The combined effects of pump output and filter resistance are monitored by a prefilter pressure sensor positioned between the blood pump and the hemofilter. Internal filtration–enhanced hemodialysis (IFEHD), which uses an enhanced internal filtration dialyzer, may offer greater convenience than conventional hemodiafiltration therapies by eliminating the need for additional equipment (eg, a roller pump).[19]
Additionally, several auxiliary subcircuits may be connected to the prefilter segment, eg, a pre-blood pump infusion line, with its inlet located close to the vascular access, commonly used for citrate infusion when regional anticoagulation is employed. Another is a prefilter infusion pump circuit situated between the blood pump and the hemofilter, through which replacement fluid is delivered. A heparin infusion line is also integrated into this prefilter section of the circuit.
Dialysis Membrane or Hemofilte
The dialysis membrane or hemofilter is the component of the circuit through which solute and water are removed by convection, diffusion, or a combination of both, depending on the selected treatment modality. Blood enters and exits the cartridge through ports located at either end, while 2 additional lateral ports are used for dialysate inflow and effluent drainage; effluent pressure is continuously monitored by a sensor positioned between the filter and the effluent pump.
The hemofilter is a cylindrical cartridge containing bundles of semipermeable hollow capillary fibers that permit the transfer of solutes and fluid between the blood and surrounding compartments. Hemofilter membranes are advanced synthetic materials, primarily polysulfone (PSU), polyarylethersulfone (PAES), and modified acrylonitrile copolymers (AN69/AN69ST). The hollow fibers typically have an internal diameter of approximately 200 μm and a wall thickness of about 30 μm.[20][21] Membrane molecular weight cut-off varies by filter type. Dialysate and effluent flow around the exterior of these fibers. When convection alone is employed, the solute composition of the effluent closely mirrors that of plasma water entering the filter. In contrast, dialysate use establishes concentration gradients that facilitate the diffusive clearance of small solutes between blood and dialysate.
Before dialysate is delivered to the dialyzer, it is temperature-adjusted by heating to approximately 35 °C to 38 °C and then subjected to negative pressure to remove dissolved gases. Careful monitoring of dialysate osmolality is essential, as excessively hyperosmolar dialysate solutions may lead to hypernatremia and other electrolyte abnormalities. In contrast, hypo-osmolar solutions can precipitate rapid hemolysis, profound hyponatremia, and hyperkalemia. Dialysate temperatures below 35 °C may cause hypothermia in unconscious patients and shivering in conscious individuals, while temperatures exceeding 42 °C can lead to blood protein denaturation and hemolysis.
Postfilter Segment
The postfilter segment carries dialysed blood back to the patient. This portion of the circuit may include a postfilter infusion pump for administering postdilution replacement fluid and a venous air-removal chamber equipped with an air or bubble detector and an automatic blood-line clamp. Its primary role is to ensure patient safety, specifically by preventing accidental air entry into the circulation.[22] Additionally, an outflow pressure sensor is typically located within the bubble trap to monitor the venous return pressure. This measurement is critical for detecting circuit disconnections, as a sudden loss of resistance results in a pressure drop that triggers high-priority alarms and automatically ceases the blood pump.
Waste Fluid Circuits
Circuits carrying waste fluids contain the waste products. They can be measured for urea and other toxins (along with urine output, if any) to estimate the clearance of a particular substance further.
Future Directions
Wearable and implantable artificial kidneys are the future of hemodialysis, with lower operational costs helping overcome the infrastructural barriers to providing self-care treatment for renal failure. They employ a sorbent-based regenerative dialysis system called recirculating dialysate (REDY), in which solute waste from the spent dialysate passes through columns containing urease. Urea gets hydrolyzed into ammonia and carbon dioxide.
Hydration with water molecules produces ammonium and bicarbonate ions. Ammonium serves as a dietary acid remover and binds nitrogen from the dialysate. The dialysate then passes sequentially over the cation and anion exchange columns, during which cations, eg, potassium, calcium, and magnesium, as well as organic toxins, eg, phosphates and sulfates, are removed. Finally, the dialysate is recharged with calcium and magnesium and returned to flow through the dialyzer again. These battery-operated devices use sorbent cartridges and can be worn like a purse, belt, or vest.
An implantable artificial kidney utilizes silicon nanotechnology and tissue engineering to create a surgically implantable device that mimics the function of a native kidney. An implantable artificial kidney includes a high-efficiency filter, a hemocartridge containing microchips, and a bioreactor containing cultured renal tubular epithelial cells harvested from cadaveric kidneys, known as the biocartridge. The ultrafiltrate produced closely resembles urine. It avoids electrical pumps as the patient's blood pressure drives the device. No dialysate is needed, as the bio cartridge maintains a neutral fluid balance by reabsorbing salt and water while eliminating concentrated waste products. These devices provide gradual, continuous ultrafiltration therapy, which will reduce intradialytic hypotension and cardiac disease of dialysis.[23]
Personnel
A dialysis care team is an interprofessional group of qualified individuals contributing to holistic patient management and a smooth transition to a dialysis-dependent life. Nephrologists are team leaders with expertise in the treatment of renal conditions. They educate patients about disease progression and measures to slow the decline in renal function and encourage their participation in management decisions.
Advanced practitioners, eg, nurses and medical assistants, collaborate with nephrologists in managing kidney patients at medical offices and the dialysis unit. A nephrology nurse specializes in assessing dialysis patients, ensuring proper medication administration and treatment, and overseeing the dialysis process. They also supervise home programs, training patients and their care partners in administering self-dialysis modalities, eg, home hemodialysis and continuous ambulatory peritoneal dialysis (CAPD). A renal dietitian helps plan meals and tailor the diet to meet each patient's unique needs. They review dialysis adequacy, rehabilitation, bone management, and anemia management. Nephrology social workers counsel patients and their families to help them manage the challenges of renal disease. They can help individuals make lifestyle changes, identify sources of emotional support, locate services provided by agencies to meet patients' needs, and enhance the quality of life.
The patient care technician performs the dialysis treatment and monitors patients throughout, while biomedical technicians maintain the machines and water quality at the dialysis center. The vascular access care team includes a vascular access surgeon who creates and maintains dialysis access. The radiologist's imaging helps plan access surgery. The interventional radiologist places a catheter, repairs the fistula, and treats vascular thrombosis. The access coordinator reviews the access history, plans treatment, follows up to ensure that the appropriate treatment was received, and records the information. Billing personnel can answer questions about insurance coverage, billing, or payment. Pharmacists play a central role in managing medication regimens by identifying dialyzable drugs, adjusting dosing, and collaborating closely with nurses and prescribers to maintain medication safety.
A controlled trial in California demonstrated that social worker involvement in predialysis programs improved employment outcomes, quality of life, work attitudes, and self-esteem. National organizations, including the National Kidney Foundation, support patient education through web-based, printed, and audiovisual resources. Cardiology referral for echocardiography remains mandatory for all dialysis patients within 1 to 3 months of initiation, on an interdialytic day, and every 3 years thereafter, as accurate assessment of left ventricular systolic function strongly predicts cardiovascular disease and mortality. Furthermore, the National Kidney Foundation is a valuable member of the healthcare team, supporting research to manage renal disease, providing the community with valuable information about kidney disease, management options, diet, and rehabilitation, and offering programs and services for patients with kidney disease. However, the most important members of this dialysis care team are the patients themselves, their families, or caregivers.
Consultations
A single nephrology office consultation often fails to provide patients with an adequate understanding of chronic kidney disease. Enhanced care delivered by a predialysis interprofessional team leads to improved biochemical outcomes, a higher rate of planned dialysis initiation, fewer hospitalizations, and potential survival benefits. Despite these advantages, 36% of newly diagnosed ESRD patients in the United States in 2015 received no nephrology care before starting dialysis, resulting in more extended initial hospitalizations, increased complications, and higher mortality.
Early planning for dialysis access and, when feasible, preemptive renal transplantation offers the strongest opportunity for rehabilitation, since dialysis replaces only select filtration functions of the kidney and does not restore endocrine or anti-inflammatory activity. Consistent predialysis care correlates with improved clinical outcomes and reduced healthcare costs. Optimal management involves referral to an interprofessional team once declining GFR becomes apparent, ideally at least 12 months before dialysis. Dialysis timing can be estimated by extrapolating the eGFR trajectory to 10 mL/min/1.73 m².
Referral for interprofessional care occurs when eGFR reaches 15 mL/min/1.73 m², as comorbid conditions may precipitate abrupt renal decline requiring urgent dialysis. Group education sessions enable peer-to-peer learning, while support groups provide emotional reassurance for patients and families coping with ESRD. The care team typically includes a nurse educator, physical therapist, occupational therapist, dietitian, social worker, pharmacist, and, at times, a trained peer support volunteer. Effective collaboration and shared communication among team members guide individualized therapy. Use of an interprofessional dialysis access liaison has demonstrated improved fistula patency and reduced morbidity and mortality.[24][25][26][27]
Preparation
Vascular access is the essential first step in achieving effective hemodialysis. The gold standard is the distal AV fistula.[28] The alternatives are synthetic grafts and tunneled central venous catheters after a patient’s superficial veins have been exhausted. The recommended current strategy is to permanently catheterize only those patients on chronic hemodialysis who have exhausted their peripheral vascular beds. For hospitalized ICU patients requiring hemodialysis, hemodialysis catheters may be placed in the internal jugular, femoral, or subclavian veins, with the right internal jugular vein preferred.
Preparation of appropriate infrastructure for home hemodialysis should be undertaken only after confirming the absence of any legal restrictions from the central or local government. All prerequisites should be met, and the home should be structurally sound, free from dampness, mold, and excessive environmental pollution, with reliable electricity and an adequate water supply. Appropriate provisions must be made for reverse osmosis water purification and for the disposal of wastewater, dialysate, and biomedical waste.
Community house hemodialysis offers a homelike, noninstitutional setting with flexible scheduling, similar to home hemodialysis. Each patient has a separate space with a machine bay, dialysis equipment, and other consumables, and is responsible for their dialysis. For those who dialyze more frequently (5 or more times a week), a dedicated machine and space in the community hemodialysis location are the best options. Those on a thrice-a-week or alternate-day regimen can share a machine. The home hemodialysis program is responsible for the infrastructure, equipment, and maintenance of the community house.[29]
Patients seeking nocturnal dialysis are limited to their bedrooms, while those fearing unintentional needle dislodgement may prefer daytime dialysis. Those with larger, more static hemodialysis machines have limited options for machine placement. At the same time, mobile batch dialysis equipment can be relocated, provided the necessary peripheral equipment and outlets are in place. The provision and undertaking of home dialysis involves sharing and dividing responsibilities between the home hemodialysis program and the patient. Both parties and clinicians must understand their responsibilities. An agreement should be documented as a patient contract or in the unit's policies and procedures. The liability towards installation and maintenance should be made clear at the beginning.
Technique or Treatment
Hemodialysis Techniques
As discussed above, the essential first step is establishing vascular access. Options for access include catheters, arteriovenous fistulas (AVFs), and arteriovenous grafts (AVGs).[30][31][32][33] The "Fistula First" initiative encourages the creation of an arteriovenous fistula in most patients to provide reliable access to the circulation. However, most patients have an arteriovenous graft in which polytetrafluoroethylene prosthetic material is interposed between an artery and a vein due to inadequate vasculature.
Pediatric patients or patients with unstable blood pressure may require priming of the circuit with saline, albumin, or reconstituted whole blood. Blood is pumped through the dialyzer at a rate of 300 to 500 mL/min, while dialysate flows in a counter-current direction at 500 to 800 mL/min. Lower rates are used in neonates and pediatric patients, and critically ill patients who may not tolerate the rapid fluid removal and metabolic changes associated with IHD.
Negative hydrostatic pressure on the dialysate side is used to achieve adequate fluid removal (ultrafiltration). The chosen ultrafiltration rate for each session should achieve an optimal balance between euvolemia, solute clearance, and adequate blood pressure control, while minimising hemodynamic instability and intradialytic symptoms. Dialysate, or dialyzing fluid, is an electrolyte solution that approximates the electrolyte composition of extracellular fluid, with differences primarily in bicarbonate buffer and potassium concentrations. The solution's osmolality is close to that of plasma to prevent red blood cell hemolysis; the solution contains dextrose, sodium, potassium, magnesium, calcium, chloride, and bicarbonate. Dialysate may be generated online, prepared by mixing prepackaged salts, or supplied by the dialysis clinician.[34][35][36]
Dialysis targets depend on the urea reduction ratio, that is, the fraction of blood urea nitrogen reduced per hemodialysis session, ideally 65% to 70%. Most patients receiving IHD require anticoagulation therapy to maintain an activated clotting time 1.5 to 2 times normal to prevent clotting within the dialysis circuit. Unfractionated heparin is the most common anticoagulant used; however, if a regional anticoagulation (anticoagulation of the circuit without systemic effect) is desired, dialysate containing citrate can be used.[37] The citrate binds to calcium at the dialyzer membrane, reducing clotting within the dialyzer. Hemodialysis dose should be individualized, taking into account the adequacy of ultrafiltration, control of hyperkalemia, hyperphosphatemia, and acidosis, as well as fluid removal.[38]
Continuous renal replacement therapy has become a popular method of renal support in pediatric patients and is commonly used in critically ill patients. Compared with IHD, evidence suggests that CRRT may improve the chances of renal recovery in critically ill patients surviving acute kidney injury.[39][40] CRRT uses both diffusion and convection: dialysate allows diffusion to remove small molecules, while convection clears both small and larger molecules via high ultrafiltration rates. High ultrafiltration may require volume and electrolyte replacement to compensate for the loss of these substances.
Although slower flow rates make CRRT less efficient than IHD, its continuous nature allows equivalent daily clearance with fewer metabolic shifts, and newer CRRT devices can achieve near-IHD flow rates for faster solute removal. Commonly used CRRT modalities are continuous venovenous hemofiltration (CVVH), which relies on high convective clearance and requires replacement fluids; continuous venovenous hemodialysis (CVVHD), which primarily uses dialysate for diffusion with minimal convection; and continuous venovenous hemodiafiltration (CVVHDF), which combines dialysate and replacement fluids for both diffusion and convection.
Anticoagulation and Hemofiltration Fluid
Systemic heparinization can be used for anticoagulation; however, it may be associated with risks, eg, bleeding, heparin-induced thrombocytopenia, and the need for frequent monitoring to adjust the dose. Regional citrate anticoagulation acts by chelating calcium, a cofactor in the clotting cascade. Additionally, calcium is administered to the patient to prevent hypocalcemia. Citrate anticoagulation requires less frequent monitoring compared with heparin; however, disadvantages include the risk of acid–base disturbances, hypercalcemia or hypocalcemia, and citrate accumulation due to impaired metabolism or clearance. Anticoagulation should be used with caution in patients with underlying coagulation disorders.
Premade and fully compounded dialysate or hemofiltration fluid is usually used in CRRT. These fluids are available in a range of electrolyte concentrations to accommodate different clinical needs. Replacement fluids can be administered either before or after the hemofilter. Greater clearance can be achieved by increasing the dialysate or replacement fluid flow rate. A calcium gap, or citrate lock, occurs when excess citrate binds to free calcium in the patient, resulting in low ionized calcium despite normal or high total calcium levels.[41][42] Increasing clearance and reducing citrate delivery helps address this situation.
Quality of Life Concerns
Dialysis patients have a reduced health-related quality of life (HRQoL) associated with increased morbidity and mortality, including:
- Physical factors: These impairments are characterized by limited or impaired mobility and role limitations, manifesting as sleep disorders (eg, obstructive sleep apnea), fatigue, and restless legs.
- Mental factors: Mental health issues encompass depressive thinking and anxiety. Intensive hemodialysis has a positive impact on HRQoL by increasing the physical and psychological component scores and is also associated with significantly reduced postdialysis recovery time.[43]
Complications
Several complications are commonly associated with hemodialysis.
Intradialytic Hypotension
Intradialytic hypotension is defined as a decrease in systolic blood pressure of 20 mm Hg or greater, or a decrease in mean arterial blood pressure of 10 mm Hg, accompanied by associated clinical events.[44] This causes poor long-term outcomes due to increased mortality and increased rate of regional wall motion abnormalities during dialysis, known as myocardial stunning. A nadir systolic blood pressure lower than 90 mm Hg is associated with higher mortality.[45] Intradialytic hypotension may reflect severe underlying conditions, eg, infection, arrhythmias, myocardial ischemia, tamponade, hemorrhage, air embolism, or dialyzer reactions that require urgent recognition.
This complication can result from rapid or excessive ultrafiltration, reduced plasma osmolality, autonomic dysfunction, diminished cardiac reserve, intake of antihypertensive medications, or dialysate-related factors, eg, temperature and electrolyte composition.[46][47][48] Intradialytic hypotension usually presents as dizziness, light-headedness, nausea, dyspnea, or subtle symptoms. Management includes reducing the ultrafiltration rate, maintaining the patient in the Trendelenburg position, and administering oxygen and a normal saline fluid bolus.
Intradialytic Hypertension
Volume overload, sympathetic overactivity, activation of the renin-angiotensin system, medications, and arteriosclerosis can contribute to intradialytic hypertension.[49][50][51] Intradialytic hypertension can be treated by using antihypertensive medications and achieving euvolemia.
Muscle Cramps
The pathogenesis of muscle cramps in patients on dialysis is unknown. The origin of the cramps is considered neural and typically involves the lower extremity muscles; however, upper extremity muscles can also be involved. Electrolyte shifts (eg, hypokalemia and hypomagnesemia), changes in plasma osmolality, and plasma volume contraction can predispose individuals to cramps. Tissue hypoxia and other factors that trigger vasoconstriction and muscle hypoperfusion impair muscle relaxation. Treatment includes slowing the rate of ultrafiltration, increasing plasma osmolality with hypertonic saline, mannitol, or dextrose, using medications (eg, gabapentin or amitriptyline), massaging the affected extremity, and using warm compresses.[52][53]
Dialysis Disequilibrium Syndrome
Dialysis disequilibrium syndrome is more common in patients during or soon after their first treatment. This complication is a clinical syndrome characterized by neurologic deterioration, restlessness, mental confusion, headache, occasional muscle twitching, and coma. It occurs due to a substantial gradient in urea concentration between CSF and blood, which causes water to move into the central nervous system, thereby raising intracranial pressure. Patients undergoing fast dialysis develop seizures and cerebral edema more often. A reasonable goal for urea concentration reduction is 40% over 2 hours, with a urea reduction ratio of 0.4. Adding an osmotic agent to the blood could prevent the gradient from forming. Sodium, mannitol, high-glucose dialysate, and glycerol are usually added. Increasing the dialysate’s sodium concentration throughout treatment may be beneficial.[54][55]
Dialyzer Reactions
Anaphylactic type A reactions can present from mild-to-moderate symptoms, eg, itching, urticaria, coryza, watery eyes, abdominal cramping, fever, nausea, vomiting, and diarrhea to severe symptoms, eg, dyspnea, a feeling of impending doom, and hemodynamic instability. Symptoms may begin at any time during the first 30 minutes following dialysis.[56] The reaction can be due to hypersensitivity to ethylene oxide, used to sterilize dialyzers, or to bacterial peptide contamination. Anaphylactoid reactions are common in patients taking ACE inhibitors who undergo hemodialysis with AN-69 membranes, likely due to the enhanced generation of bradykinin from the membrane’s negatively charged surface, combined with ACE inhibition.[57][58][59] Surface-modified AN-69 membranes (AN-69 ST) or adjusting priming conditions can reduce bradykinin release and prevent these reactions, even in patients who continue to take ACE inhibitors.[60] Management includes termination of dialysis treatment, treatment with intravenous antihistamines, steroids, and epinephrine. Proper rinsing of dialyzers before use eliminates residual allergens and helps prevent them.
Type B reactions, which occur in patients dialyzed with new cellulosic membranes, are generally less severe than type A reactions and present with chest or back pain, dyspnea, nausea, vomiting, and hypotension. Symptoms usually appear within 15 to 30 minutes of starting dialysis and often improve as treatment continues. These reactions are mediated by complement activation and can be minimized by dialyzer reuse or by using more biocompatible membranes.[61][62]
Chest Pain and Dyspnea
Chest pain and dyspnea most often result from myocardial ischemia, volume shifts with rapid ultrafiltration, hypotension, or hypervolemia, but may also reflect severe conditions, eg, arrhythmias, hemolysis, air embolism, infection, or dialyzer reactions. Immediate management includes stopping ultrafiltration, reducing blood flow, positioning the patient in a supine position, administering oxygen, assessing vital signs, and evaluating for cardiac, hemolytic, or air embolic causes. Persistent symptoms, hypotension, hypoxemia, or suspected life-threatening etiologies require discontinuation of dialysis and urgent transfer to a hospital setting.
Hemolysis
Acute hemolysis during dialysis is a medical emergency characterized by port-wine appearance in the venous blood line, a marked fall in hematocrit, and a pink-colored plasma centrifuged blood sample. The patient should undergo hematologic investigations and be monitored for potential delayed hemolysis. A dialysate sample must be investigated to find the cause.
Air Embolism
Air embolism is a rare complication but can lead to hemodynamic collapse, cardiac arrest, and fatal consequences. Venous air embolism is often challenging to diagnose, and visualization of intracardiac air on transesophageal echocardiography is considered the most definitive diagnostic test.[63][64] Management includes placing the patient in the left lateral decubitus position with the head down or in the Trendelenburg position, administering 100% and hyperbaric oxygen, and withdrawing air from the cardiac chambers using a percutaneously inserted needle or a cardiac catheter.[65]
Fever
Patients undergoing hemodialysis are at increased risk for infection, and the development of fever during a hemodialysis session should prompt concern for a vascular access–related infection.
Other Complications
Other complications of hemodialysis include nausea and vomiting, headache, chest and back pain, and pruritus.[54][66][67][68] These symptoms may be related to an underlying disorder, hypotension, an early manifestation of disequilibrium syndrome, dyselectrolytemia, hypoglycemia, or psychological factors.[69][70] Acetaminophen and antiemetics administered during dialysis can help alleviate the symptoms.
In patients with recurrent and severe dialysis-associated headaches, reducing the duration of individual hemodialysis sessions to mitigate symptoms while increasing treatment frequency to preserve dialysis adequacy may be beneficial.[71] Switching to a different type of dialyzer membrane could reduce itching caused by low-grade hypersensitivity to blood circuit components.
Vascular Access Dysfunction
Vascular access dysfunction most commonly manifests as stenosis of arteriovenous access, which is the strongest determinant of the quality of life of a patient undergoing dialysis. This leads to reduced blood flow and an increased risk of thrombosis.[72] The formation of a catheter-related fibro-epithelial sheath also hampers blood flow. Urokinase instillation, endovascular catheter stripping, or replacement of the indwelling dialysis catheter in a subcutaneous tunnel reestablishes access.[73][74]
Electrolyte Imbalances
Electrolyte imbalances should be remediated by dialysis; however, they can also be precipitated by dialysis. Hyperkalemia is the most common and clinically significant complication in noncompliant patients, besides hypermagnesemia, hyponatremia, and hypocalcemia.[75] A cardiac arrest is twice as likely in patients undergoing hemodialysis as in those on peritoneal dialysis 3 months after dialysis initiation. Sudden cardiac deaths are most likely during the first 2 months after the initiation of hemodialysis. The predominant arrhythmias identified are ventricular fibrillation, pulseless electrical activity, and asystole. In the vascular access process, death may occur from cardiac arrhythmias, pulmonary edema, or contrast medium reaction.[72]
Vascular access precautions include avoiding additional trauma to the access arm, eg, wearing tight clothing or jewelry, carrying heavy objects, or sleeping on the affected limb. Blood draws and blood pressure measurements should not be performed on this arm. Needle insertion sites should be rotated to preserve access integrity, and gentle pressure should be applied after needle removal to achieve hemostasis. Patients should be instructed to contact a health care practitioner if bleeding persists or becomes profuse (>30 minutes). Bleeding, often related to heparin use during dialysis, can be effectively treated with protamine sulfate. Continuous monitoring of venous and arterial pressures is essential for detecting line disconnections. Needles should be securely taped, and safety measures such as wetness detectors and closed connector devices should be employed. Regular inspection of the access site for signs of infection (eg, redness, warmth, pain) is necessary. Loss of the normal bruit should prompt evaluation for access thrombosis to prevent limb ischemia.
Clinical Significance
CKD patients requiring dialysis accumulate uremic retention solutes, eg, asymmetric dimethylarginine (ADMA), indoxyl sulfate, and p-cresol, which may have proatherogenic properties. Failing kidneys produce lower amounts of cardiovascular disease and atherogenesis inhibitors like renalase, a soluble monoamine oxidase that regulates blood pressure. In addition, dialysis patients experience chronic inflammation. Biomarkers, eg, CRP, fibrinogen, pentraxin 3 (PTX3), interleukin 6 (IL-6), white blood cell count, and the presence of endothelial cells in circulation, independently predict mortality in CKD patients, as they indicate endothelial dysfunction.
Dialysis patients develop arterial sclerosis and secondary stiffening that commonly causes isolated systolic hypertension with raised pulse pressure. Intradialytic hypertension occurs in more chronically volume-overloaded patients with intradialytic vascular resistance surges attributable to acute changes in endothelial cell function during dialysis. Reducing dialysate sodium and including poorly dialyzed antihypertensives, eg, carvedilol, in the prescription can improve outcomes.[76]
Elevated lipoprotein (a) levels are associated with increased cardiovascular disease mortality. Cardiovascular diseases (CVD) and renal disease are closely associated, and patients having a history of both have higher morbidity and mortality. The presence of CKD increases the likelihood of CVD. Cardiovascular morbidity, mortality, and all-cause mortality are predicted by a fall in the eGFR and albuminuria. Albuminuria is a subtle indicator of kidney dysfunction, microvasculature health, and endothelial function. The early identification and management of cardiovascular risk factors in a patient with mildly reduced eGFR are imperative to ensuring that the patient does not die from CVD before requiring renal replacement therapy.
Cardiovascular pathologies in CKD range from generalized vasculopathy, vascular noncompliance, and calcification to left ventricular hypertrophy (LVH). The diseases that closely resemble congestive heart failure and fluid overload should be ruled out—for example, acute respiratory distress syndrome, bacterial pneumonia, cirrhosis, community-acquired pneumonia, and pulmonary fibrosis. Noncardiogenic causes of fluid overload often lack jugular venous distention and an S3 gallop. Measuring left ventricular pressure (LVP) through the pulmonary capillary wedge pressure (PCWP) helps distinguish between cardiogenic and non-cardiogenic pulmonary edema. PCWP is almost always low in those with noncardiogenic pulmonary edema. Other conditions considered among the differentials are pulmonary embolism, angina, coronary artery disease, aortic dissection, structural heart disease, hyperthyroidism, stress, and excess caffeine and nicotine, besides esophageal disorders like esophagitis, esophageal rupture, and esophageal spasm. The concurrent decrease in the functioning of both kidneys and the heart makes dialysis a critical intervention for preventing and treating life-threatening cardiac conditions.
Sustained high levels of fibroblast growth factor 23 lead to atrial fibrillation, LVH, and mortality. Other factors contributing to mortality risk are hyperphosphatemia, followed by hypercalcemia and parathyroid abnormalities. Mineral metabolism disorders account for about 17% of overall mortality in hemodialysis patients. In dialysis patients, early-onset extensive vascular calcification (coronary arteries) occurs, besides calcification of aortic and mitral valves, leading to progressive stenosis, morbidity, and mortality. Hemodialysis sessions are associated with cardiac arrhythmias like atrial fibrillation. Peripheral arterial disease is seen more commonly in dialysis patients with comorbidities (eg, diabetes and preexisting atherosclerosis). The risk is directly proportional to the duration of dialysis. Patients undergoing dialysis also have a 3 times higher risk of stroke.
Enhancing Healthcare Team Outcomes
Dialysis serves as a life-sustaining therapy for patients with advanced kidney disease or end-stage renal disease, offering two primary modalities: hemodialysis and peritoneal dialysis. Hemodialysis can be delivered intermittently (IHD) or continuously (CRRT), with IHD providing rapid ultrafiltration for acute volume overload and CRRT offering continuous fluid and solute removal to maintain hemodynamic and metabolic stability in critically ill patients. Appropriate timing for initiating dialysis depends on clinical symptoms, volume status, and functional decline rather than kidney function alone. Early counseling regarding treatment options, including home or in-center hemodialysis, peritoneal dialysis, kidney transplantation, or conservative management, supports informed decision-making for patients and their caregivers. Mortality among dialysis patients is predominantly cardiovascular, highlighting the need for risk mitigation through pharmacologic strategies and careful monitoring.
Effective management of dialysis requires coordinated interprofessional collaboration. Physicians, general practitioners, and advanced practitioners assess disease progression, determine timing and modality selection, and monitor clinical and laboratory parameters. Nurses provide patient education, monitor hemodynamic stability, and facilitate adherence to treatment plans. Pharmacists optimize medication management, ensure safe dosing, and support cardiovascular protection. Dietitians guide nutritional interventions, and social workers support patients and assist with resource access. Consistent communication across the care team ensures timely recognition of complications, individualized therapy adjustments, and comprehensive patient-centered care, ultimately improving clinical outcomes, safety, and quality of life for patients requiring dialysis.
Nursing, Allied Health, and Interprofessional Team Interventions
Home hemodialysis causes an additional burden for both caregivers and patients. However, imparting adequate pre-dialysis education, motivation, and training of patients and caregivers, assisted cannulation, home visits by nurses, and an organized framework for providing nursing, technical support, and respite care for patients have been shown to improve the adoption of home hemodialysis.
Sticking to a healthy diet has been shown to improve outcomes in patients undergoing hemodialysis.[77] A study has shown that periodic text messaging to advise dialysis patients on healthy eating habits has improved adherence to dietary recommendations and reduced the need for phosphate binder therapy. The reminders focus on guidance related to potassium, phosphorus, sodium, and fluid intake, as well as broader nutrition and lifestyle advice. These include encouraging the consumption of fresh, unprocessed foods to limit phosphate intake commonly found in packaged products; advising patients to read food labels carefully and select items containing less than 400 mg of sodium per 100 g; and recommending alternatives, eg, pasta, rice, and sweet potato, consumed 3 to 4 times per week, in place of regular potatoes to better control potassium intake.
Nursing, Allied Health, and Interprofessional Team Monitoring
Commencing home hemodialysis creates unique psychosocial issues affecting the patient and care partner. The home hemodialysis health care team must provide proactive interprofessional support, respite care, travel support, peer support, and financial support. Improper redressal of these aspects could cause patients to return to in-center hemodialysis. Some centers provide real-time monitoring of home hemodialysis treatments, and a panic button/alarm may be present to contact the local paramedic unit.[78]
Media
(Click Image to Enlarge)
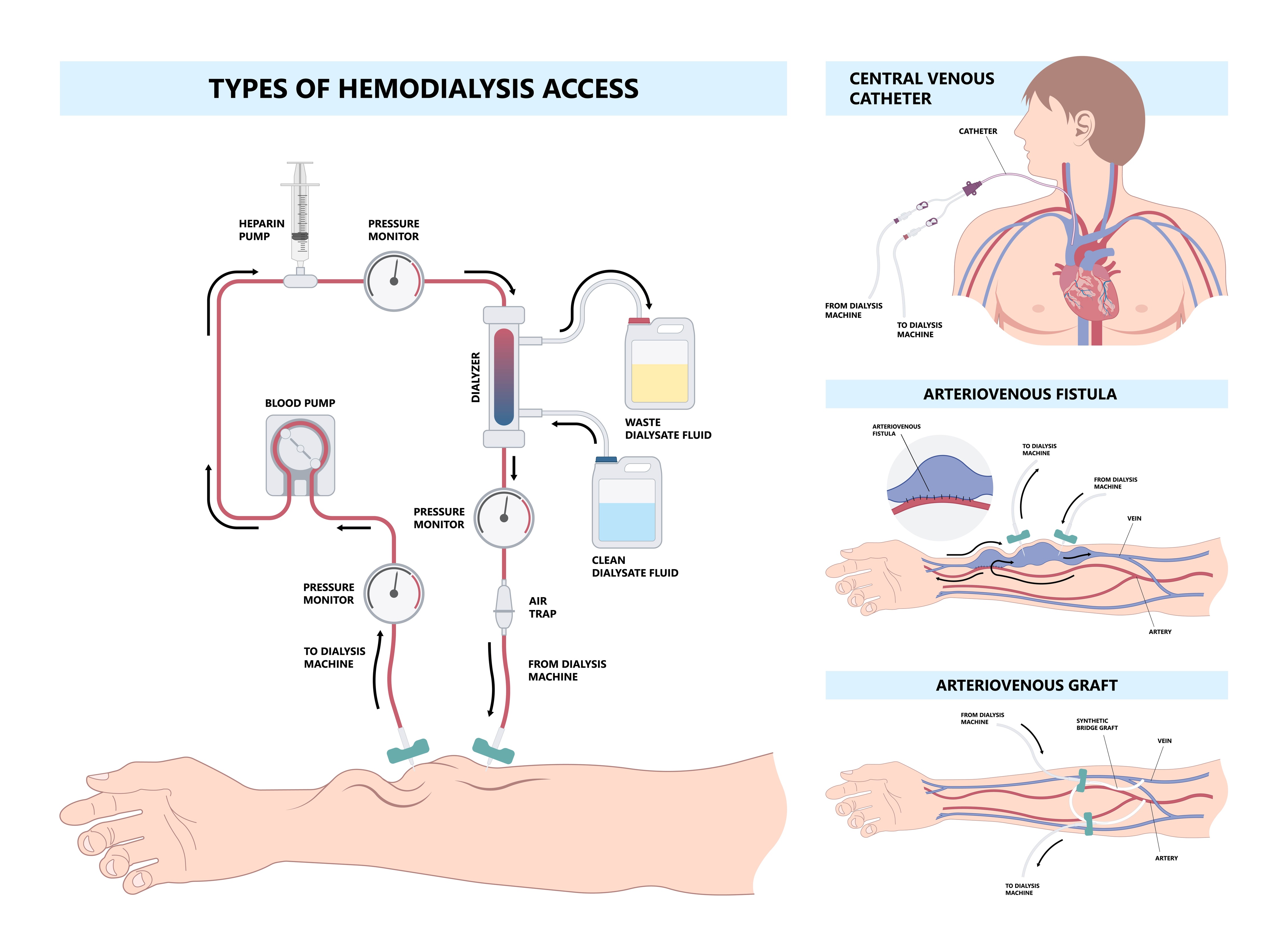
Types of Hemodialysis Access. Illustration of the main methods used for vascular access in hemodialysis: the central venous catheter, arteriovenous fistula, and arteriovenous graft. The section on the central venous catheter shows a flexible tube inserted into a large vein in the neck, chest, or groin, with external ports that connect to the dialysis machine. The arteriovenous fistula is depicted as a surgically created direct connection between an artery and a vein, typically in the forearm, allowing for repeated needle access and efficient blood flow during dialysis. The arteriovenous graft is shown as a synthetic tube that connects an artery and a vein, serving as an alternative when a fistula cannot be created.
Pepermpron - stock.adobe.com
References
Voelker R. What Is Dialysis? JAMA. 2025 May 20:333(19):1752. doi: 10.1001/jama.2025.1905. Epub [PubMed PMID: 40079957]
Flythe JE, Watnick S. Dialysis for Chronic Kidney Failure: A Review. JAMA. 2024 Nov 12:332(18):1559-1573. doi: 10.1001/jama.2024.16338. Epub [PubMed PMID: 39356511]
Liyanage T, Ninomiya T, Jha V, Neal B, Patrice HM, Okpechi I, Zhao MH, Lv J, Garg AX, Knight J, Rodgers A, Gallagher M, Kotwal S, Cass A, Perkovic V. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet (London, England). 2015 May 16:385(9981):1975-82. doi: 10.1016/S0140-6736(14)61601-9. Epub 2015 Mar 13 [PubMed PMID: 25777665]
Level 1 (high-level) evidenceHsu CY, Parikh RV, Pravoverov LN, Zheng S, Glidden DV, Tan TC, Go AS. Implication of Trends in Timing of Dialysis Initiation for Incidence of End-stage Kidney Disease. JAMA internal medicine. 2020 Dec 1:180(12):1647-1654. doi: 10.1001/jamainternmed.2020.5009. Epub [PubMed PMID: 33044519]
Saran R, Robinson B, Abbott KC, Agodoa LYC, Bragg-Gresham J, Balkrishnan R, Bhave N, Dietrich X, Ding Z, Eggers PW, Gaipov A, Gillen D, Gipson D, Gu H, Guro P, Haggerty D, Han Y, He K, Herman W, Heung M, Hirth RA, Hsiung JT, Hutton D, Inoue A, Jacobsen SJ, Jin Y, Kalantar-Zadeh K, Kapke A, Kleine CE, Kovesdy CP, Krueter W, Kurtz V, Li Y, Liu S, Marroquin MV, McCullough K, Molnar MZ, Modi Z, Montez-Rath M, Moradi H, Morgenstern H, Mukhopadhyay P, Nallamothu B, Nguyen DV, Norris KC, O'Hare AM, Obi Y, Park C, Pearson J, Pisoni R, Potukuchi PK, Repeck K, Rhee CM, Schaubel DE, Schrager J, Selewski DT, Shamraj R, Shaw SF, Shi JM, Shieu M, Sim JJ, Soohoo M, Steffick D, Streja E, Sumida K, Kurella Tamura M, Tilea A, Turf M, Wang D, Weng W, Woodside KJ, Wyncott A, Xiang J, Xin X, Yin M, You AS, Zhang X, Zhou H, Shahinian V. US Renal Data System 2018 Annual Data Report: Epidemiology of Kidney Disease in the United States. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2019 Mar:73(3 Suppl 1):A7-A8. doi: 10.1053/j.ajkd.2019.01.001. Epub 2019 Feb 21 [PubMed PMID: 30798791]
Cooper BA, Branley P, Bulfone L, Collins JF, Craig JC, Fraenkel MB, Harris A, Johnson DW, Kesselhut J, Li JJ, Luxton G, Pilmore A, Tiller DJ, Harris DC, Pollock CA, IDEAL Study. A randomized, controlled trial of early versus late initiation of dialysis. The New England journal of medicine. 2010 Aug 12:363(7):609-19. doi: 10.1056/NEJMoa1000552. Epub 2010 Jun 27 [PubMed PMID: 20581422]
Level 1 (high-level) evidenceLameire N, Van Biesen W. The initiation of renal-replacement therapy--just-in-time delivery. The New England journal of medicine. 2010 Aug 12:363(7):678-80. doi: 10.1056/NEJMe1006669. Epub 2010 Jun 27 [PubMed PMID: 20581421]
Gilbert J, Lovibond K, Mooney A, Dudley J, Guideline Committee. Renal replacement therapy: summary of NICE guidance. BMJ (Clinical research ed.). 2018 Oct 19:363():k4303. doi: 10.1136/bmj.k4303. Epub 2018 Oct 19 [PubMed PMID: 30341093]
Watanabe Y, Yamagata K, Nishi S, Hirakata H, Hanafusa N, Saito C, Hattori M, Itami N, Komatsu Y, Kawaguchi Y, Tsuruya K, Tsubakihara Y, Suzuki K, Sakai K, Kawanishi H, Inaguma D, Yamamoto H, Takemoto Y, Mori N, Okada K, Hataya H, Akiba T, Iseki K, Tomo T, Masakane I, Akizawa T, Minakuchi J, “Hemodialysis Initiation for Maintenance Hemodialysis” Guideline Working Group, Japanese Society for Dialysis Therapy. Japanese society for dialysis therapy clinical guideline for "hemodialysis initiation for maintenance hemodialysis". Therapeutic apheresis and dialysis : official peer-reviewed journal of the International Society for Apheresis, the Japanese Society for Apheresis, the Japanese Society for Dialysis Therapy. 2015 Mar:19 Suppl 1():93-107. doi: 10.1111/1744-9987.12293. Epub [PubMed PMID: 25817934]
Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C, Wanner C, Krane V, Cass A, Craig J, Neal B, Jiang L, Hooi LS, Levin A, Agodoa L, Gaziano M, Kasiske B, Walker R, Massy ZA, Feldt-Rasmussen B, Krairittichai U, Ophascharoensuk V, Fellström B, Holdaas H, Tesar V, Wiecek A, Grobbee D, de Zeeuw D, Grönhagen-Riska C, Dasgupta T, Lewis D, Herrington W, Mafham M, Majoni W, Wallendszus K, Grimm R, Pedersen T, Tobert J, Armitage J, Baxter A, Bray C, Chen Y, Chen Z, Hill M, Knott C, Parish S, Simpson D, Sleight P, Young A, Collins R, SHARP Investigators. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): a randomised placebo-controlled trial. Lancet (London, England). 2011 Jun 25:377(9784):2181-92. doi: 10.1016/S0140-6736(11)60739-3. Epub 2011 Jun 12 [PubMed PMID: 21663949]
Level 1 (high-level) evidenceGotch FA, Sargent JA. A mechanistic analysis of the National Cooperative Dialysis Study (NCDS). Kidney international. 1985 Sep:28(3):526-34 [PubMed PMID: 3934452]
Elshihabi I, Brzowski A, Kaye C, Kearon P. Efficiency of hemodialysis therapy for a urea cycle defect in a neonate. Clinical nephrology. 1995 Mar:43(3):208-9 [PubMed PMID: 7774084]
Brophy PD, Tenenbein M, Gardner J, Bunchman TE, Smoyer WE. Childhood diethylene glycol poisoning treated with alcohol dehydrogenase inhibitor fomepizole and hemodialysis. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2000 May:35(5):958-62 [PubMed PMID: 10793034]
Brown MJ, Shannon MW, Woolf A, Boyer EW. Childhood methanol ingestion treated with fomepizole and hemodialysis. Pediatrics. 2001 Oct:108(4):E77 [PubMed PMID: 11581485]
Gitomer JJ, Khan AM, Ferris ME. Treatment of severe theophylline toxicity with hemodialysis in a preterm neonate. Pediatric nephrology (Berlin, Germany). 2001 Oct:16(10):784-6 [PubMed PMID: 11605782]
Constantinescu C, Pasca S, Tat T, Teodorescu P, Vlad C, Iluta S, Dima D, Tomescu D, Scarlatescu E, Tanase A, Sigurjonsson OE, Colita A, Einsele H, Tomuleasa C. Continuous renal replacement therapy in cytokine release syndrome following immunotherapy or cellular therapies? Journal for immunotherapy of cancer. 2020 May:8(1):. doi: 10.1136/jitc-2020-000742. Epub [PubMed PMID: 32474415]
National Kidney Foundation. KDOQI Clinical Practice Guideline for Hemodialysis Adequacy: 2015 update. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2015 Nov:66(5):884-930. doi: 10.1053/j.ajkd.2015.07.015. Epub [PubMed PMID: 26498416]
Level 2 (mid-level) evidenceJuncos LA, Chandrashekar K, Karakala N, Baldwin I. Vascular access, membranes and circuit for CRRT. Seminars in dialysis. 2021 Nov:34(6):406-415. doi: 10.1111/sdi.12977. Epub 2021 May 3 [PubMed PMID: 33939859]
Mineshima M, Ishimori I, Sakiyama R. Validity of internal filtration-enhanced hemodialysis as a new hemodiafiltration therapy. Blood purification. 2009:27(1):33-7. doi: 10.1159/000167006. Epub 2009 Jan 23 [PubMed PMID: 19169015]
Ronco C, Clark WR. Haemodialysis membranes. Nature reviews. Nephrology. 2018 Jun:14(6):394-410. doi: 10.1038/s41581-018-0002-x. Epub [PubMed PMID: 29730670]
Sakai K. Dialysis membranes for blood purification. Frontiers of medical and biological engineering : the international journal of the Japan Society of Medical Electronics and Biological Engineering. 2000:10(2):117-29 [PubMed PMID: 10898241]
Ku L, Weinberg L, Seevanayagam S, Baldwin I, Opdam H, Doolan L. Massive air embolism from continuous venovenous haemofiltration causing electromechanical dissociation in a cardiac surgical patient. Critical care and resuscitation : journal of the Australasian Academy of Critical Care Medicine. 2012 Jun:14(2):154-8 [PubMed PMID: 22697625]
Salani M, Roy S, Fissell WH 4th. Innovations in Wearable and Implantable Artificial Kidneys. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2018 Nov:72(5):745-751. doi: 10.1053/j.ajkd.2018.06.005. Epub 2018 Aug 23 [PubMed PMID: 30146422]
Rodriguez JA, Armadans L, Ferrer E, Olmos A, Codina S, Bartolomé J, Borrellas J, Piera L. The function of permanent vascular access. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2000 Mar:15(3):402-8 [PubMed PMID: 10692528]
Level 2 (mid-level) evidenceTurmel-Rodrigues L, Pengloan J, Rodrigue H, Brillet G, Lataste A, Pierre D, Jourdan JL, Blanchard D. Treatment of failed native arteriovenous fistulae for hemodialysis by interventional radiology. Kidney international. 2000 Mar:57(3):1124-40 [PubMed PMID: 10720965]
Turmel-Rodrigues L, Pengloan J, Baudin S, Testou D, Abaza M, Dahdah G, Mouton A, Blanchard D. Treatment of stenosis and thrombosis in haemodialysis fistulas and grafts by interventional radiology. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2000 Dec:15(12):2029-36 [PubMed PMID: 11096150]
Ethier J, Mendelssohn DC, Elder SJ, Hasegawa T, Akizawa T, Akiba T, Canaud BJ, Pisoni RL. Vascular access use and outcomes: an international perspective from the Dialysis Outcomes and Practice Patterns Study. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2008 Oct:23(10):3219-26. doi: 10.1093/ndt/gfn261. Epub 2008 May 29 [PubMed PMID: 18511606]
Level 3 (low-level) evidenceFerrari G, Talassi E, Baraldi C, Lambertini D, Tarchini R. [Vascular access validity and treatment efficiency in hemodialysis]. Giornale italiano di nefrologia : organo ufficiale della Societa italiana di nefrologia. 2003 May-Jun:20 Suppl 22():S22-9 [PubMed PMID: 12851917]
Agar JW, Perkins A, Heaf JG. Home hemodialysis: infrastructure, water, and machines in the home. Hemodialysis international. International Symposium on Home Hemodialysis. 2015 Apr:19 Suppl 1():S93-S111. doi: 10.1111/hdi.12290. Epub [PubMed PMID: 25925829]
Maya ID, Oser R, Saddekni S, Barker J, Allon M. Vascular access stenosis: comparison of arteriovenous grafts and fistulas. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2004 Nov:44(5):859-65 [PubMed PMID: 15492952]
Agarwal AK, Haddad NJ, Vachharajani TJ, Asif A. Innovations in vascular access for hemodialysis. Kidney international. 2019 May:95(5):1053-1063. doi: 10.1016/j.kint.2018.11.046. Epub 2019 Mar 4 [PubMed PMID: 30922666]
Schmidli J, Widmer MK, Basile C, de Donato G, Gallieni M, Gibbons CP, Haage P, Hamilton G, Hedin U, Kamper L, Lazarides MK, Lindsey B, Mestres G, Pegoraro M, Roy J, Setacci C, Shemesh D, Tordoir JHM, van Loon M, Esvs Guidelines Committee, Kolh P, de Borst GJ, Chakfe N, Debus S, Hinchliffe R, Kakkos S, Koncar I, Lindholt J, Naylor R, Vega de Ceniga M, Vermassen F, Verzini F, Esvs Guidelines Reviewers, Mohaupt M, Ricco JB, Roca-Tey R. Editor's Choice - Vascular Access: 2018 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2018 Jun:55(6):757-818. doi: 10.1016/j.ejvs.2018.02.001. Epub 2018 May 2 [PubMed PMID: 29730128]
Level 1 (high-level) evidenceBeathard GA, Lok CE, Glickman MH, Al-Jaishi AA, Bednarski D, Cull DL, Lawson JH, Lee TC, Niyyar VD, Syracuse D, Trerotola SO, Roy-Chaudhury P, Shenoy S, Underwood M, Wasse H, Woo K, Yuo TH, Huber TS. Definitions and End Points for Interventional Studies for Arteriovenous Dialysis Access. Clinical journal of the American Society of Nephrology : CJASN. 2018 Mar 7:13(3):501-512. doi: 10.2215/CJN.11531116. Epub 2017 Jul 20 [PubMed PMID: 28729383]
Dhondt AW, Vanholder RC, De Smet RV, Claus SA, Waterloos MA, Glorieux GL, Delanghe JR, Lameire NH. Studies on dialysate mixing in the Genius single-pass batch system for hemodialysis therapy. Kidney international. 2003 Apr:63(4):1540-7 [PubMed PMID: 12631371]
Dhondt A, Eloot S, Wachter DD, Smet RD, Waterloos MA, Glorieux G, Lameire N, Verdonck P, Vanholder R. Dialysate partitioning in the Genius batch hemodialysis system: effect of temperature and solute concentration. Kidney international. 2005 Jun:67(6):2470-6 [PubMed PMID: 15882294]
Clark WR, Turk JE Jr. The NxStage System One. Seminars in dialysis. 2004 Mar-Apr:17(2):167-70 [PubMed PMID: 15043625]
Davenport A. Alternatives to standard unfractionated heparin for pediatric hemodialysis treatments. Pediatric nephrology (Berlin, Germany). 2012 Oct:27(10):1869-79. doi: 10.1007/s00467-012-2129-5. Epub 2012 Feb 29 [PubMed PMID: 22374405]
Brown EA, Johansson L, Farrington K, Gallagher H, Sensky T, Gordon F, Da Silva-Gane M, Beckett N, Hickson M. Broadening Options for Long-term Dialysis in the Elderly (BOLDE): differences in quality of life on peritoneal dialysis compared to haemodialysis for older patients. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2010 Nov:25(11):3755-63. doi: 10.1093/ndt/gfq212. Epub 2010 Apr 16 [PubMed PMID: 20400451]
Level 2 (mid-level) evidenceSun Z, Ye H, Shen X, Chao H, Wu X, Yang J. Continuous venovenous hemofiltration versus extended daily hemofiltration in patients with septic acute kidney injury: a retrospective cohort study. Critical care (London, England). 2014 Apr 9:18(2):R70. doi: 10.1186/cc13827. Epub 2014 Apr 9 [PubMed PMID: 24716613]
Level 2 (mid-level) evidenceSchneider AG, Bellomo R, Bagshaw SM, Glassford NJ, Lo S, Jun M, Cass A, Gallagher M. Choice of renal replacement therapy modality and dialysis dependence after acute kidney injury: a systematic review and meta-analysis. Intensive care medicine. 2013 Jun:39(6):987-97. doi: 10.1007/s00134-013-2864-5. Epub 2013 Feb 27 [PubMed PMID: 23443311]
Level 1 (high-level) evidenceBunchman TE, Maxvold NJ, Barnett J, Hutchings A, Benfield MR. Pediatric hemofiltration: Normocarb dialysate solution with citrate anticoagulation. Pediatric nephrology (Berlin, Germany). 2002 Mar:17(3):150-4 [PubMed PMID: 11956849]
Meier-Kriesche HU, Gitomer J, Finkel K, DuBose T. Increased total to ionized calcium ratio during continuous venovenous hemodialysis with regional citrate anticoagulation. Critical care medicine. 2001 Apr:29(4):748-52 [PubMed PMID: 11373461]
Kraus MA, Fluck RJ, Weinhandl ED, Kansal S, Copland M, Komenda P, Finkelstein FO. Intensive Hemodialysis and Health-Related Quality of Life. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2016 Nov:68(5S1):S33-S42. doi: 10.1053/j.ajkd.2016.05.023. Epub [PubMed PMID: 27772641]
Level 2 (mid-level) evidenceKooman J, Basci A, Pizzarelli F, Canaud B, Haage P, Fouque D, Konner K, Martin-Malo A, Pedrini L, Tattersall J, Tordoir J, Vennegoor M, Wanner C, ter Wee P, Vanholder R. EBPG guideline on haemodynamic instability. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2007 May:22 Suppl 2():ii22-44 [PubMed PMID: 17507425]
Flythe JE, Xue H, Lynch KE, Curhan GC, Brunelli SM. Association of mortality risk with various definitions of intradialytic hypotension. Journal of the American Society of Nephrology : JASN. 2015 Mar:26(3):724-34. doi: 10.1681/ASN.2014020222. Epub 2014 Sep 30 [PubMed PMID: 25270068]
Flythe JE, Kunaparaju S, Dinesh K, Cape K, Feldman HI, Brunelli SM. Factors associated with intradialytic systolic blood pressure variability. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2012 Mar:59(3):409-18. doi: 10.1053/j.ajkd.2011.11.026. Epub 2011 Dec 29 [PubMed PMID: 22209553]
van der Sande FM, Kooman JP, Leunissen KM. Intradialytic hypotension--new concepts on an old problem. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2000 Nov:15(11):1746-8 [PubMed PMID: 11071958]
Reilly RF. Attending rounds: A patient with intradialytic hypotension. Clinical journal of the American Society of Nephrology : CJASN. 2014 Apr:9(4):798-803. doi: 10.2215/CJN.09930913. Epub 2014 Jan 2 [PubMed PMID: 24385517]
Georgianos PI, Agarwal R. Aortic Stiffness, Ambulatory Blood Pressure, and Predictors of Response to Antihypertensive Therapy in Hemodialysis. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2015 Aug:66(2):305-12. doi: 10.1053/j.ajkd.2015.01.018. Epub 2015 Mar 25 [PubMed PMID: 25818679]
Agarwal R, Light RP. Arterial stiffness and interdialytic weight gain influence ambulatory blood pressure patterns in hemodialysis patients. American journal of physiology. Renal physiology. 2008 Feb:294(2):F303-8 [PubMed PMID: 18160623]
Converse RL Jr, Jacobsen TN, Toto RD, Jost CM, Cosentino F, Fouad-Tarazi F, Victor RG. Sympathetic overactivity in patients with chronic renal failure. The New England journal of medicine. 1992 Dec 31:327(27):1912-8 [PubMed PMID: 1454086]
Kesik G, Ozdemir L, Yıldırım T, Jabrayilov J, Çeliksöz G. Effects of warm or cold compresses applied to the legs during hemodialysis on cramps, fatigue, and patient comfort: A placebo-controlled randomized trial. Hemodialysis international. International Symposium on Home Hemodialysis. 2023 Apr:27(2):117-125. doi: 10.1111/hdi.13070. Epub 2023 Feb 14 [PubMed PMID: 36788410]
Level 1 (high-level) evidenceMastnardo D, Lewis JM, Hall K, Sullivan CM, Cain K, Theurer J, Huml A, Sehgal AR. Intradialytic Massage for Leg Cramps Among Hemodialysis Patients: a Pilot Randomized Controlled Trial. International journal of therapeutic massage & bodywork. 2016 Jun:9(2):3-8 [PubMed PMID: 27257445]
Level 1 (high-level) evidenceGozubatik-Celik G, Uluduz D, Goksan B, Akkaya N, Sohtaoglu M, Uygunoglu U, Kircelli F, Sezen A, Saip S, Karaali Savrun F, Siva A. Hemodialysis-related headache and how to prevent it. European journal of neurology. 2019 Jan:26(1):100-105. doi: 10.1111/ene.13777. Epub 2018 Oct 11 [PubMed PMID: 30102816]
Karunaratne K, Taube D, Khalil N, Perry R, Malhotra PA. Neurological complications of renal dialysis and transplantation. Practical neurology. 2018 Apr:18(2):115-125. doi: 10.1136/practneurol-2017-001657. Epub 2017 Dec 28 [PubMed PMID: 29288211]
Daugirdas JT, Ing TS. First-use reactions during hemodialysis: a definition of subtypes. Kidney international. Supplement. 1988 Mar:24():S37-43 [PubMed PMID: 2966256]
Simon P, Potier J, Thebaud HE. [Risk factors for acute hypersensitivity reactions in hemodialysis]. Nephrologie. 1996:17(3):163-70 [PubMed PMID: 9064565]
Brunet P, Jaber K, Berland Y, Baz M. Anaphylactoid reactions during hemodialysis and hemofiltration: role of associating AN69 membrane and angiotensin I-converting enzyme inhibitors. American journal of kidney diseases : the official journal of the National Kidney Foundation. 1992 May:19(5):444-7 [PubMed PMID: 1585932]
Parnes EL, Shapiro WB. Anaphylactoid reactions in hemodialysis patients treated with the AN69 dialyzer. Kidney international. 1991 Dec:40(6):1148-52 [PubMed PMID: 1762316]
Thomas M, Valette P, Mausset AL, Déjardin P. High molecular weight kininogen adsorption on hemodialysis membranes: influence of pH and relationship with contact phase activation of blood plasma. influence of pre-treatment with poly(ethyleneimine). The International journal of artificial organs. 2000 Jan:23(1):20-6 [PubMed PMID: 12118833]
Hakim RM, Breillatt J, Lazarus JM, Port FK. Complement activation and hypersensitivity reactions to dialysis membranes. The New England journal of medicine. 1984 Oct 4:311(14):878-82 [PubMed PMID: 6332276]
Craddock PR, Fehr J, Dalmasso AP, Brighan KL, Jacob HS. Hemodialysis leukopenia. Pulmonary vascular leukostasis resulting from complement activation by dialyzer cellophane membranes. The Journal of clinical investigation. 1977 May:59(5):879-88 [PubMed PMID: 856872]
Muth CM, Shank ES. Gas embolism. The New England journal of medicine. 2000 Feb 17:342(7):476-82 [PubMed PMID: 10675429]
Mammoto T, Hayashi Y, Ohnishi Y, Kuro M. Incidence of venous and paradoxical air embolism in neurosurgical patients in the sitting position: detection by transesophageal echocardiography. Acta anaesthesiologica Scandinavica. 1998 Jul:42(6):643-7 [PubMed PMID: 9689268]
Orebaugh SL. Venous air embolism: clinical and experimental considerations. Critical care medicine. 1992 Aug:20(8):1169-77 [PubMed PMID: 1643897]
Scherer JS, Combs SA, Brennan F. Sleep Disorders, Restless Legs Syndrome, and Uremic Pruritus: Diagnosis and Treatment of Common Symptoms in Dialysis Patients. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2017 Jan:69(1):117-128. doi: 10.1053/j.ajkd.2016.07.031. Epub 2016 Sep 29 [PubMed PMID: 27693261]
Arzhan S, Roumelioti ME, Unruh ML. Itch and Ache on Dialysis: New Approaches to Manage Uremic Pruritus and Restless Legs. Blood purification. 2020:49(1-2):222-227. doi: 10.1159/000504081. Epub 2019 Dec 18 [PubMed PMID: 31851986]
Moledina DG, Perry Wilson F. Pharmacologic Treatment of Common Symptoms in Dialysis Patients: A Narrative Review. Seminars in dialysis. 2015 Jul-Aug:28(4):377-83. doi: 10.1111/sdi.12378. Epub 2015 Apr 25 [PubMed PMID: 25913502]
Level 3 (low-level) evidenceBarrett BJ, Vavasour HM, Major A, Parfrey PS. Clinical and psychological correlates of somatic symptoms in patients on dialysis. Nephron. 1990:55(1):10-5 [PubMed PMID: 2352574]
Milinkovic M, Zidverc-Trajkovic J, Sternic N, Trbojevic-Stankovic J, Maric I, Milic M, Andric B, Nikic P, Jovanovic P, Rosic P, Stojimirovic B. Hemodialysis headache. Clinical nephrology. 2009 Feb:71(2):158-63 [PubMed PMID: 19203508]
Tandon T, Sinha AD, Agarwal R. Shorter delivered dialysis times associate with a higher and more difficult to treat blood pressure. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2013 Jun:28(6):1562-8. doi: 10.1093/ndt/gfs597. Epub 2013 Jan 24 [PubMed PMID: 23348881]
Masud A, Costanzo EJ, Zuckerman R, Asif A. The Complications of Vascular Access in Hemodialysis. Seminars in thrombosis and hemostasis. 2018 Feb:44(1):57-59. doi: 10.1055/s-0037-1606180. Epub 2017 Sep 12 [PubMed PMID: 28898900]
Khatri VP, Pavlides CA. Method of salvaging long-term dialysis catheters. The American surgeon. 1995 Nov:61(11):1013-5 [PubMed PMID: 7486414]
Quarello F, Forneris G, Borca M, Pozzato M. Do central venous catheters have advantages over arteriovenous fistulas or grafts? Journal of nephrology. 2006 May-Jun:19(3):265-79 [PubMed PMID: 16874685]
Nakhoul GN, Huang H, Arrigain S, Jolly SE, Schold JD, Nally JV Jr, Navaneethan SD. Serum Potassium, End-Stage Renal Disease and Mortality in Chronic Kidney Disease. American journal of nephrology. 2015:41(6):456-63. doi: 10.1159/000437151. Epub 2015 Jul 25 [PubMed PMID: 26228532]
Van Buren PN, Inrig JK. Mechanisms and Treatment of Intradialytic Hypertension. Blood purification. 2016:41(1-3):188-93. doi: 10.1159/000441313. Epub 2016 Jan 15 [PubMed PMID: 26765312]
Su G, Saglimbene V, Wong G, Natale P, Ruospo M, Craig JC, Hegbrant J, Carrero JJ, Strippoli GFM. Healthy Lifestyle and Mortality Among Adults Receiving Hemodialysis: The DIET-HD Study. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2022 May:79(5):688-698.e1. doi: 10.1053/j.ajkd.2021.07.022. Epub 2021 Sep 20 [PubMed PMID: 34547395]
Bennett PN, Schatell D, Shah KD. Psychosocial aspects in home hemodialysis: a review. Hemodialysis international. International Symposium on Home Hemodialysis. 2015 Apr:19 Suppl 1():S128-34. doi: 10.1111/hdi.12258. Epub [PubMed PMID: 25925820]