Introduction
A hangman’s fracture is defined as spondylolisthesis between the 2nd (C2) and 3rd (C3) cervical vertebrae following bilateral fractures of the C2 pars interarticularis (see Image. Hangman's Fracture on Radiography). Although traumatic spondylolisthesis of C2, also known as the axis, was first described in 1866, the term “hangman’s fracture” was introduced in 1965.[1] This condition is the 2nd most common fracture involving the axis after odontoid fractures and accounts for approximately 4% to 20% of all cervical fractures.[2][3] Steele's rule of 3rds states that the cross-sectional area at the atlas (1st cervical vertebra, C1) level may be divided into 3 equal components: the dens, the surrounding space, and the spinal cord. The relatively larger available space for the spinal cord at this level contributes to the lower incidence of neurologic injury associated with hangman’s fractures.[4] Accurate diagnosis relies on advanced imaging to assess the extent of injury. Classification systems guide treatment decisions and distinguish stable from unstable injuries.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Schneider et al coined the term "hangman’s fracture" in 1965. Although the term historically implied a hyperextension and distraction injury, as occurs in judicial hangings, the contemporary mechanism of injury is hyperextension combined with axial loading of the cervical spine.[5] Hangman’s fractures most commonly result from motor vehicle collisions, falls, diving injuries, or contact sports.
Epidemiology
Fractures of the cervical spine occur in 1% to 3% of all trauma cases, of which 9% to 18% involve C2. The incidence of C2 fractures has doubled from 3 per 100,000 to 6 per 100,000 between 1997 and 2014, according to the Swedish National Patient Registry.
Fractures of the odontoid process are more common, representing 35% to 78% of all C2 fractures in the general population and 89% of fractures in adults older than 70. Hangman’s fractures account for 11% to 25% of all C2 fractures.[6] Recent research demonstrates a higher frequency of hangman’s fractures in men, primarily affecting young and middle-aged adults, with a lower incidence in older cohorts.
A study of 216 patients with a mean age of 49.7 years analyzed the geriatric population (18.5%) separately from younger patients and demonstrated a male predominance, with ratios of 3:1 in patients aged 18 to 64 and 2:1 in patients older than 65.[7] An earlier study of 58 patients reported a mean age of 62.7 years (standard deviation 25 years), with a male-to-female ratio of 1:1.2. Motor vehicle accidents were the most common cause of injury in both cohorts.
Pathophysiology
Consideration of the unique anatomy of the atlas-axis complex is vital when managing associated injuries. Unlike the subaxial cervical spine, the C1–C2 complex lacks an intervertebral disc and contains specialized ligaments that support the cranium and provide the largest contribution to cervical rotation. The transverse foramen, which transmits the vertebral artery through the cervical spine, lies in close proximity to the C2 pedicle and pars interarticularis, slightly weakening this region and predisposing it to fracture.
Two hypotheses have been proposed to explain the pathogenesis of hangman’s fracture. The internal gear hypothesis suggests that a trabecular void and the abrupt transition from the bicolumnar to the tricolumnar unit place the isthmus of the axis at increased risk of injury. The leaf spring hypothesis proposes that the C2 pedicle functions as the shackle within the vertebral assembly, representing the structural weak point.
The extension-compression subtype of a hangman’s fracture arises from pincer-like compression of the C2 pedicle between the adjoining articular processes of C1 and C3. The flexion subtype results from bending failure of the pedicle over the fulcrum formed by the superior facet of C3. Flexion-type injuries carry an increased risk of damage to the C2–C3 disc anteriorly and the C1–C2 posterior ligament complex posteriorly.[8]
Multiple grading systems exist for hangman’s fractures. However, the Levine and Edwards classification remains the most widely used.
Levine and Edwards Classification
Angulation in the Levine and Edwards system is measured as the angle between the inferior endplates of C2 and C3. Anterior subluxation of C2 on C3 greater than 3 mm indicates disruption of the C2–C3 intervertebral disc. This grading system does not apply to the pediatric population.[9]
Type 1 fractures involve less than 3 mm of C2 on C3 subluxation, result from axial loading, and are considered stable. Management typically involves a rigid cervical collar.
Type 2 fractures demonstrate C2–C3 disc disruption and posterior longitudinal ligament injury, with subluxation greater than 3 mm and angulation exceeding 11°. Subluxation less than 5 mm requires reduction with axial traction and immobilization in a halo for 6 to 12 weeks, whereas subluxation greater than 5 mm may necessitate surgical intervention. Type 2a fractures exhibit less displacement but greater angular deformity, result from flexion injury, and are unstable. These injuries are not amenable to axial traction and require halo immobilization.
Type 3 fractures are characterized by C2–C3 facet joint dislocation and anterior longitudinal ligament disruption. These unstable injuries may be associated with a neurologic deficit and typically require surgical management.
Francis Grading System
The Francis grading system evaluates hangman’s fractures based on angulation and displacement. Angulation is measured as the degree of anterior deviation from a posterior vertebral line drawn straight from the C3 vertebral body. Displacement is assessed by the magnitude of the anterolisthesis and graded as greater than or less than 3.5 mm.[10]
Type 1 fractures exhibit less than 11° of angulation and less than 3.5 mm of displacement. Type 2 fractures demonstrate greater than 11° of angulation with less than 3.5 mm of displacement. Type 3 fractures show less than 11° of angulation and greater than 3.5 mm of displacement. Type 4 fractures combine greater than 11° of angulation with displacement exceeding 3.5 mm. Type 5 fractures involve complete disruption of the intervertebral disc.
Differences Between Typical and Atypical Fractures
Not all C2 hangman’s fractures may be classified using standard systems. Typical hangman’s fractures result in separation of the anterior elements from the posterior elements of the C2 vertebra, increasing the space available for the spinal cord and reducing the risk of neurologic injury.[11] Meanwhile, atypical hangman’s fractures involve the posterior aspect of the C2 vertebral body rather than the bilateral pars interarticularis, limiting the increase in spinal canal space and elevating the risk of neurologic compromise. Atypical fractures also include variants with unusual fracture or displacement patterns. Coronal vertical fractures affect the posterior aspect of the C2 body.[12] Isolated C2–C3 facet dislocations may also occur.[13] C2–C3 spondylolisthesis can result from injury to the capsular ligament of the facet joint and the posterior spinous ligamentous complex.[14] Atypical hangman's fractures may also involve the pedicles.[15]
History and Physical
Recognition of hangman’s fractures must extend beyond obvious mechanisms, such as motor vehicle collisions and high-impact falls, as low-energy or blunt trauma, particularly in older patients, can produce significant unstable injuries. History should include assessment of fracture risk factors, such as osteoporosis, metastatic disease, or vitamin D deficiency. Physical examination may reveal posterior neck tenderness, radiculopathy, myelopathy, and posterior fossa signs secondary to vertebral artery injury. A comprehensive neurologic examination is required, including cranial nerve status, sensory and motor function, and rectal tone.
Evaluation
Laboratory tests should be obtained as an adjunct to overall medical assessment. Normalized hemoglobin, hematocrit, prothrombin time, partial thromboplastin time, international normalized ratio, and platelet counts are required prior to operative intervention.
Radiography
Evaluation with x-rays provides limited but important information. Proper radiographic technique must capture the cervical spine from the occiput through the C7–T1 disc space, which is essential in the assessment of cervical spine trauma. Lateral, anteroposterior, and open-mouth odontoid views are required. Approximately 93% of cervical spine injuries are visible on combined lateral, anteroposterior, and odontoid radiographs. X-rays are effective for assessing cervical alignment during the acute phase, the postoperative period, and long-term follow-up. Li et al reported that the presence of a posterior vertebral wall fracture with translation of at least 1.8 mm and C2–C3 angulation of at least 5.5° on x-ray predisposes patients with hangman’s fractures to partial neurologic deficit.[16]
Computed Tomography
Computed tomography (CT) is the mainstay of imaging for hangman’s fractures.[17] CT is the preferred modality for determining fracture morphology and evaluating associated C2 injuries (see Image. Three-Dimensional Computed Tomography of a Hangman's Fracture). CT scanning is indicated when clinical suspicion remains high despite unremarkable findings on plain radiography. CT is also critical for preoperative planning when surgical intervention is indicated. However, this imaging technique does not directly assess the spinal cord, soft tissues, or ligamentous structures. Complete evaluation requires dedicated thin-cut CT reconstructions. Noncontrast-enhanced CT is sufficient for assessing bony anatomy and characterizing fractures, and may be combined with CT angiography when evaluating vertebral and vascular anatomy.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is essential for assessing soft-tissue injuries, including ligamentous structures, intervertebral discs, spinal cord components, and nerve roots. Noncontrast MRI is particularly useful for determining the acute nature of a fracture when this information is otherwise unknown. T2 signal hyperintensities and STIR (short τ inversion recovery) changes within the dens, ligaments, or surrounding soft tissue can identify critical components of the injury. MRI carries a lower risk than flexion-extension cervical radiography.
The Effendi, Levine, and Francis classifications are based exclusively on static radiographs. Management decisions also depend on the integrity of the C2–C3 disc and the anterior and posterior longitudinal ligaments. MRI provides essential information regarding concurrent instability, which may be indicated by C2–C3 angulation of at least 11°, C2–C3 translation of at least 3.5 mm, the presence of teardrop fractures involving C2 or C3, and association with C2–C3 discoligamentous injury.[18]
Vascular Imaging
Vascular imaging may be indicated in the evaluation of cervical spine fractures. The vertebral artery’s 2nd segment (V2) traverses the transverse foramina of C2 through C6, while the 3rd segment (V3) runs extradurally, exiting the C2 foramen across the sulcus arteriosus, placing it at risk for injury. A series found that 15% of patients with fractures of C1 to C2 sustained vertebral artery injuries, with type III odontoid fractures conferring the greatest risk. Untreated vertebral artery injury carries a stroke rate of 24%. CT angiography may be performed in conjunction with CT fracture imaging, taking kidney function into account. Level III evidence supports screening of patients with fractures involving C1 to C3 using multislice, multidetector CT angiography. Magnetic resonance angiography is not recommended as the sole imaging modality for evaluating the vertebral arteries. First-line investigation with percutaneous angiography is considered overly aggressive.[19][20]
Treatment / Management
Treatment options include conservative management, cervical or halo-vest orthosis, and surgical intervention. Fracture stability and the presence of neurologic deficits aid in determining the appropriate strategy.
External Fixation
A rigid cervical collar constitutes the initial treatment for hangman’s fractures. Nonunion occurs in up to 50% of odontoid fractures but is rare in hangman’s fractures, with approximately 90% achieving healing with immobilization alone. Level III evidence indicates that hangman’s fractures may be initially managed using either halo-vest or rigid collar immobilization, producing a reduction rate of 97% to 100% and a fusion rate of 93% to 100%. External orthoses should be maintained for 8 to 14 weeks. Older patients demonstrate poor tolerance of halo-vest orthosis, making rigid cervical collars the preferred 1st-line management in this group.[21][22][23](B3)
Nonoperative treatment is recommended for extension-type Levine-Edwards type I and type II hangman’s fractures. Flexion-type Levine-Edwards type IIa and type III fractures require surgical intervention.[24](B2)
A systematic review demonstrated that conservative treatment achieves sequentially lower fusion rates, from nearly 100% in Levine-Edwards type I fractures to approximately 30% in type III fractures. This approach is time-consuming and carries a high risk of nonunion. In a study of 625 patients treated with halo-vest immobilization, patients older than 80 years exhibited higher risks of complications, mortality, and readmissions.[25] Another study of 189 patients, 71.1% of whom sustained C2 fractures managed with halos, reported a mortality rate of 8.3%, a treatment failure rate of 10.7%, and a complication rate of 46.3%.[26]
Internal Fixation
Surgical fixation may be indicated in the presence of any of the following:
- Severe angulation of C2 on C3 (Francis II and IV, Levine II)
- Disruption of the C2–C3 disc space (Francis V, Levine II)
- Anterior displacement of C2 greater than 50% on C3
- Inability to establish or maintain alignment with external immobilization
- Nonunion following external immobilization
The primary objective of surgical intervention is to achieve early anatomical stability while preserving maximal cervical range of motion.[27] Abnormal angulations and incomplete reduction compromise biomechanical loading, increasing the risk of persistent neck pain, nonunion, and implant failure. Surgical strategies include halo traction, anterior or posterior standalone fusion, and global anterior-posterior fusion. Internal fixation may be accomplished through anterior approaches or various posterior constructs.
Anterior approach
Anterior cervical discectomy of C2 to C3 and fusion with anterior plating stabilizes the C2 and C3 vertebral bodies. The primary advantage of the anterior approach is preservation of C1 motion, which significantly reduces morbidity compared to posterior fixation.
Posterior approach
Posterior fixation for hangman’s fractures may be achieved using several constructs, including C1–C2 transarticular screws, C1 lateral mass and C2 pedicle screws, C1 lateral mass and C2 pars interarticularis screws, and C1–C2 wiring as an adjunct technique. Fixation may be extended to the C3 lateral mass if disruption of the C2–C3 intervertebral disc or facet joint capsules is present.[28](A1)
Selection of the posterior fixation technique requires comprehensive evaluation by a neurosurgeon or orthopedic spine surgeon, considering factors such as surgeon experience, fracture location, vertebral artery anatomy, biomechanical suitability, and patient-specific anatomical variations. Preoperative vascular imaging is essential to determine the course of the vertebral artery in the V2 and V3 segments. Assessment of overall functional status, medical optimization, and bone health is critical in operative planning. Flexion-type injuries that compromise the posterior ligamentous complex necessitate C1–C2 posterior fixation according to the tension band principle, whereas extension-type injuries require fixation at the C2–C3 level, which may be performed via anterior or posterior approaches.
Levine-Edwards type II fractures are primarily managed with anterior C2–C3 fusion. Levine-Edwards type III fractures may also be treated with anterior C2–C3 fusion if reducible following traction. Irreducible type III fractures typically require posterior fusion and may necessitate global fixation. An anterior standalone approach using an extended cantilever beam technique that includes C4 has demonstrated effective reduction and stability in Levine-Edwards type III hangman’s fractures. Posterior approaches generally provide superior restoration of cervical sagittal balance compared to anterior approaches.[29]
Prerequisites for posterior pars screw fixation include reducing fracture translation to less than 3 mm and maintaining an intact anterior longitudinal ligament. Pars screws in type II fractures should be supplemented with concurrent C3 lateral mass fixation. This technique limits C1–C2 motion and does not address the anterior disc. Anterior fixation is recommended for C2–C3 disc disruption. C3 corpectomy may be required for spinal cord decompression.[30] The accuracy of screw placement may be enhanced using robot-assisted methods and intraoperative navigation systems.[31][32][33] Minimally invasive techniques using tubular retractor systems with neuronavigation have also been described.[34][35](B3)
Some strategies can help improve precision in fracture fixation, protect neurovascular structures, and preserve postoperative cervical mobility. Preoperative angiography allows assessment of the course and integrity of the vertebral artery. Intraoperative risk of arterial injury can be mitigated by utilizing color-coded duplex ultrasound.[36][37] Use of a C2 spinous muscle complex graft, compared with iliac bone, minimizes donor site morbidity and complications.[38] Zero-profile implants reduce dysphagia and preserve motion at the atlantoaxial joint.[39] C2 pedicle reformation using Herbert compression and lag screws maintains cervical mobility.[40][41] Constructs extending to C4 may be required to prevent kyphotic deformity.[42][43] Hangman’s fractures generally demonstrate excellent clinical outcomes, with low risks of mortality and neurologic complications.(B3)
Differential Diagnosis
Differential diagnoses include pseudosubluxation, most commonly occurring at C2 on C3, and congenital spondylosis of C2. The Mach effect should also be considered.
Prognosis
Successful repair of a fractured vertebra may result in an excellent recovery and a favorable long-term prognosis. Some cases require fusion of C2 and C3. Posterior fusion for 3-part fractures of the axis has demonstrated excellent outcomes.[44] In a study of more than 30 patients with hangman’s fractures, 85% achieved full recovery within a year.[45] A retrospective review of older patients with hangman’s fractures reported bony fusion in nearly 90% of cases, reaching 100% when including patients who required surgical intervention after initial fusion failure.[46]
Complications
Complications of hangman’s fractures can be significant and require careful consideration (see Image. Swan Neck Deformity in Neglected Traumatic Spondylolisthesis). A vertebral artery arteriovenous fistula may develop, resulting from traumatic disruption of the arterial wall and abnormal communication with adjacent veins, potentially leading to hemorrhage or ischemia.[47][48] Occlusion or dissection of the vertebral artery constitutes another vascular complication, which can compromise the posterior circulation and increase the risk of stroke.[49][50] Brown-Sequard syndrome may result from hemisection or asymmetric spinal cord injury, producing ipsilateral motor deficits and contralateral sensory loss.[51] Concurrent spinal cord injury is more likely in atypical fractures, as well as Levine-Edwards type IIa and type III fractures, given the greater displacement and instability associated with these patterns, which can result in neurological compromise.
Complications of different management strategies include postoperative self-limiting dysphagia, which has a reported incidence of 22.6% during the 1st week and 9.7% at 3 months, with very few cases being permanent. The risk of dysphagia is higher with anterior plating and minimized with zero-profile implants. Postoperative dysphonia has a reported incidence of 24.5% during the 1st week and 3.8% at 3 months.[52] Intraoperative vertebral artery injury may occur. Halo-related complications include pin-site infections, pin loosening, and restricted neck movements.
Deterrence and Patient Education
Routine patient counseling should emphasize safe daily practices, including motor vehicle safety through seatbelt use, fall prevention in older adults through home safety modifications, medication review, osteoporosis screening and treatment, and sports safety with appropriate protective equipment. Most cases of hangman’s fractures do not require surgical intervention and generally carry a good prognosis with proper stabilization and patient adherence. Rigid cervical collars may be necessary to limit movement, promote healing, and prevent further injury. Halo immobilization may be required in some cases. Surgical intervention is less commonly indicated. All aspects of the procedure should be explained thoroughly, emphasizing the high likelihood of successful recovery. Patients should be given realistic expectations regarding recovery time, which may extend up to a year, and counseled that chronic neck pain or stiffness may persist regardless of the chosen treatment modality.
Pearls and Other Issues
The following are important points to remember when managing hangman's fractures:
- A rigid cervical collar should be applied immediately in the emergency room setting.
- The majority of hangman’s fractures may be effectively managed with external orthosis alone.
- Vascular imaging is indicated for all fractures involving C1 to C3.
Minimizing complications entails accurate fracture assessment, appropriate immobilization, and timely surgical intervention for unstable or complex patterns. Preventive measures focus on safe activity practices, fall prevention, and reinforcement of patient compliance with immobilization protocols.
Enhancing Healthcare Team Outcomes
An interprofessional team optimally manages spinal fractures to ensure favorable outcomes and minimize complications. The emergency medicine and trauma team is responsible for initial cervical spine stabilization, performing primary and secondary surveys, rapidly identifying neurologic deficits, and ordering urgent imaging studies. Team members include physician assistants, nurse practitioners, orthopedic and neurologic specialists, intensivists or hospitalists, orthopedic and neurology nurses, and rehabilitation therapists. Physical therapy contributes to functional recovery in both surgical and nonsurgical cases. Coordination among these professionals improves patient outcomes.
Imaging is essential for the accurate diagnosis of a hangman’s fracture. Missed injuries carry significant risk, whereas most patients achieve full recovery with appropriate external support and time.[53]
Media
(Click Image to Enlarge)

Hangman's Fracture on Radiography. This lateral cervical spine radiograph demonstrates a traumatic spondylolisthesis of C2. Bilateral fractures through the pars interarticularis are visible, resulting in anterior displacement of the C2 vertebral body relative to C3.
Contributed by Sunil Munakomi, MD
(Click Image to Enlarge)
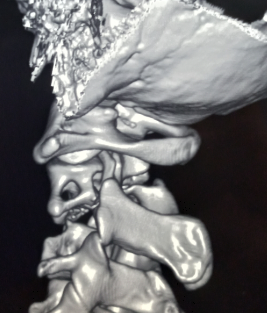
Three-Dimensional Computed Tomography of a Hangman's Fracture. This 3-dimensional image provides a clear visualization of bilateral pars interarticularis fractures. Anterior translation of the C2 vertebral body relative to C3 is prominent in this oblique view. The spatial relationship between the atlas and the axis remains largely intact.
Contributed by Sunil Munakomi, MD
(Click Image to Enlarge)

Swan Neck Deformity in Neglected Traumatic Spondylolisthesis. This lateral radiograph of the cervical spine shows a chronic, unmanaged hangman’s fracture. Progressive anterior subluxation of the C2 vertebral body has resulted in a compensatory hyperlordotic curvature of the upper cervical segments. Malalignment of the vertebral bodies creates a characteristic swan neck appearance.
Contributed by Sunil Munakomi, MD
References
Mudumba VS, Pavan S, Alugolu R. Saradhi's single stage, anterior sequential reduction utilizing C3 for type III hangman's fracture: A novel technique. Journal of craniovertebral junction & spine. 2022 Jan-Mar:13(1):80-84. doi: 10.4103/jcvjs.jcvjs_83_21. Epub 2022 Mar 9 [PubMed PMID: 35386244]
Cai Y, Khanpara S, Timaran D, Spence S, McCarty J, Aein A, Nunez L, Arevalo O, Riascos R. Traumatic spondylolisthesis of axis: clinical and imaging experience at a level one trauma center. Emergency radiology. 2022 Aug:29(4):715-722. doi: 10.1007/s10140-022-02041-5. Epub 2022 May 11 [PubMed PMID: 35543854]
Turtle J, Kantor A, Spina NT, France JC, Lawrence BD. Hangman's Fracture. Clinical spine surgery. 2020 Nov:33(9):345-354. doi: 10.1097/BSD.0000000000001093. Epub [PubMed PMID: 33044269]
Spence KF Jr, Decker S, Sell KW. Bursting atlantal fracture associated with rupture of the transverse ligament. The Journal of bone and joint surgery. American volume. 1970 Apr:52(3):543-9 [PubMed PMID: 5425648]
SCHNEIDER RC, LIVINGSTON KE, CAVE AJ, HAMILTON G. "HANGMAN'S FRACTURE" OF THE CERVICAL SPINE. Journal of neurosurgery. 1965 Feb:22():141-54 [PubMed PMID: 14288425]
Robinson AL, Olerud C, Robinson Y. Epidemiology of C2 Fractures in the 21st Century: A National Registry Cohort Study of 6,370 Patients from 1997 to 2014. Advances in orthopedics. 2017:2017():6516893. doi: 10.1155/2017/6516893. Epub 2017 Oct 17 [PubMed PMID: 29181200]
Level 3 (low-level) evidenceLi G, Wang Q. Analysis of the clinical characteristics of adult patients with hangman's fractures: A retrospective study based on multicenter clinical data. Frontiers in surgery. 2023:10():949987. doi: 10.3389/fsurg.2023.949987. Epub 2023 Apr 4 [PubMed PMID: 37082367]
Level 2 (mid-level) evidenceMenon VK. Mechanically Relevant Anatomy of the Axis Vertebra and Its Relation to Hangman's Fracture: An Illustrated Essay. Neurospine. 2019 Jun:16(2):223-230. doi: 10.14245/ns.1938140.070. Epub 2019 Jun 30 [PubMed PMID: 31261461]
Levine AM, Edwards CC. The management of traumatic spondylolisthesis of the axis. The Journal of bone and joint surgery. American volume. 1985 Feb:67(2):217-26 [PubMed PMID: 3968113]
Francis WR, Fielding JW, Hawkins RJ, Pepin J, Hensinger R. Traumatic spondylolisthesis of the axis. The Journal of bone and joint surgery. British volume. 1981:63-B(3):313-8 [PubMed PMID: 7263740]
Scholz M, Kandziora F, Kobbe P, Matschke S, Schleicher P, Josten C, Spine Section of the German Society for Orthopaedics and Trauma. Treatment of Axis Ring Fractures: Recommendations of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU). Global spine journal. 2018 Sep:8(2 Suppl):18S-24S. doi: 10.1177/2192568217745061. Epub 2018 Sep 7 [PubMed PMID: 30210957]
Pinter ZW, Lawson BK, Freedman BA, Sebastian AS. Atypical hangman's fracture with concomitant subaxial fracture-dislocation treated with circumferential fusion of C2-C5-a case report. Spinal cord series and cases. 2020 Dec 2:6(1):108. doi: 10.1038/s41394-020-00365-3. Epub 2020 Dec 2 [PubMed PMID: 33268764]
Level 3 (low-level) evidencePrasad GL. Traumatic irreducible non-Hangman's type bilateral C2-C3 high-grade facet dislocation: technical nuance. British journal of neurosurgery. 2023 Oct:37(5):1387-1390. doi: 10.1080/02688697.2020.1854683. Epub 2020 Dec 2 [PubMed PMID: 33263442]
Jain S, Mishra K, Gandhi A, Garg D. Curious Case of Atypical Hangman's Fracture: C2-C3 Listhesis without Pars Fracture. Journal of neurosciences in rural practice. 2020 Oct:11(4):663-666. doi: 10.1055/s-0040-1716988. Epub 2020 Oct 29 [PubMed PMID: 33144811]
Level 3 (low-level) evidenceAljuboori Z, Hoz S, Boakye M. Failure of C2-3 anterior arthrodesis for the treatment of atypical Hangman's fractures: A three case series. Surgical neurology international. 2020:11():52. doi: 10.25259/SNI_49_2020. Epub 2020 Mar 21 [PubMed PMID: 32257578]
Level 2 (mid-level) evidenceLi G, Wang Q. Analysis of the clinical characteristics and predisposing factors for neurological deficit with Hangman fractures. Journal of orthopaedic surgery and research. 2023 Mar 9:18(1):179. doi: 10.1186/s13018-023-03650-7. Epub 2023 Mar 9 [PubMed PMID: 36890563]
Mizels J, Connelly JW, Spina N, Lawrence B, Karamian BA. Hangman's Fractures: A Review of Current Concepts in Evaluation and Management. Clinical spine surgery. 2024 Nov 1:37(9):365-371. doi: 10.1097/BSD.0000000000001694. Epub 2024 Sep 24 [PubMed PMID: 39315683]
Kim SK, Rhee JM, Park ET, Seo HY. Surgical Outcomes for C(2) Tear Drop Fractures: Clinical Relevance to Hangman's Fracture and C(2-3) Discoligamentous Injury. Orthopaedic surgery. 2021 Dec:13(8):2363-2372. doi: 10.1111/os.13163. Epub 2021 Nov 17 [PubMed PMID: 34791834]
Gupta P, Kumar A, Gamangatti S. Mechanism and patterns of cervical spine fractures-dislocations in vertebral artery injury. Journal of craniovertebral junction & spine. 2012 Jan:3(1):11-5. doi: 10.4103/0974-8237.110118. Epub [PubMed PMID: 23741123]
Pratt H, Davies E, King L. Traumatic injuries of the c1/c2 complex: computed tomographic imaging appearances. Current problems in diagnostic radiology. 2008 Jan-Feb:37(1):26-38 [PubMed PMID: 18054664]
Tuite GF, Papadopoulos SM, Sonntag VK. Caspar plate fixation for the treatment of complex hangman's fractures. Neurosurgery. 1992 May:30(5):761-4; discussion 764-5 [PubMed PMID: 1584391]
Coric D, Wilson JA, Kelly DL Jr. Treatment of traumatic spondylolisthesis of the axis with nonrigid immobilization: a review of 64 cases. Journal of neurosurgery. 1996 Oct:85(4):550-4 [PubMed PMID: 8814154]
Level 3 (low-level) evidenceSonntag VK, Hadley MN. Nonoperative management of cervical spine injuries. Clinical neurosurgery. 1988:34():630-49 [PubMed PMID: 3288418]
Prost S, Barrey C, Blondel B, Fuentes S, Barresi L, Nicot B, Challier V, Lleu M, Godard J, Kouyoumdjian P, Lonjon N, Marinho P, Freitas E, Schuller S, Allia J, Berthiller J, Charles YP, French Society for Spine Surgery (SFCR). Hangman's fracture: Management strategy and healing rate in a prospective multi-centre observational study of 34 patients. Orthopaedics & traumatology, surgery & research : OTSR. 2019 Jun:105(4):703-707. doi: 10.1016/j.otsr.2019.03.009. Epub 2019 Apr 17 [PubMed PMID: 31005699]
Level 2 (mid-level) evidenceKurucan E, Sulovari A, Thirukumaran C, Greenstein A, Molinari R, Mesfin A. Volume-outcome relationship in halo vest utilization for C2 fractures. The spine journal : official journal of the North American Spine Society. 2020 Oct:20(10):1676-1684. doi: 10.1016/j.spinee.2020.05.543. Epub 2020 May 28 [PubMed PMID: 32474222]
Isidro S, Molinari R, Ikpeze T, Hernandez C, Mahmoudi MS, Mesfin A. Outcomes of Halo Immobilization for Cervical Spine Fractures. Global spine journal. 2019 Aug:9(5):521-526. doi: 10.1177/2192568218808293. Epub 2019 Feb 11 [PubMed PMID: 31431875]
Verma S, Singh PK, Agrawal M, Sawarkar D, Borkar SA, Kumar A, Garg K, Agrawal D, Gupta D, Satyarthee G, Chandra SP, Kale SS. Use of Intraoperative Imaging to Preserve C1-C2 Mobility in Complex Atlas-Hangman Fractures. Neurology India. 2022 Jan-Feb:70(1):209-214. doi: 10.4103/0028-3886.336335. Epub [PubMed PMID: 35263885]
Menger RP, Storey CM, Nixon MK, Haydel J, Nanda A, Sin A. Placement of C1 Pedicle Screws Using Minimal Exposure: Radiographic, Clinical, and Literature Validation. International journal of spine surgery. 2015:9():43. doi: 10.14444/2043. Epub 2015 Aug 12 [PubMed PMID: 26484006]
Level 1 (high-level) evidenceJin C, Xie N, Ren Y, Liu X, Tang F, Guo Q, Jia L, Cheng L. How Does Cervical Sagittal Balance Change After Hangman Fracture Treated with Anterior or Posterior Approach Surgery? World neurosurgery. 2020 Jun:138():e767-e777. doi: 10.1016/j.wneu.2020.03.070. Epub 2020 Mar 19 [PubMed PMID: 32201290]
Patel JYK, Kundnani VG, Kuriya S, Raut S, Meena M. Unstable Hangman's fracture: Anterior or posterior surgery? Journal of craniovertebral junction & spine. 2019 Oct-Dec:10(4):210-215. doi: 10.4103/jcvjs.JCVJS_112_19. Epub 2020 Jan 23 [PubMed PMID: 32089613]
Jun XH, Yi L. Percutaneous Fixation of Levine-Edwards Type II Hangman's Fractures Under the Guidance of an Orthopedic Robot. Orthopedics. 2023 Jan-Feb:46(1):59-63. doi: 10.3928/01477447-20221031-08. Epub 2022 Nov 7 [PubMed PMID: 36343643]
Sacino AN, Materi J, Davidar AD, Judy B, Liu A, Hwang B, Theodore N. Robot-assisted atlantoaxial fixation: illustrative cases. Journal of neurosurgery. Case lessons. 2022 Jun 20:3(25):CASE22114. doi: 10.3171/CASE22114. Epub 2022 Jun 20 [PubMed PMID: 35733845]
Level 3 (low-level) evidenceAsuzu DT, Buchholz AL. MAZOR-X robotic-navigated percutaneous C2 screw placement for hangman's fracture: a case report. Journal of spine surgery (Hong Kong). 2021 Sep:7(3):439-444. doi: 10.21037/jss-20-676. Epub [PubMed PMID: 34734148]
Level 3 (low-level) evidenceMan Kyu C, Youngseok K, Ki Hong K, Dae-Hyun K. Direct trans-pedicular screw fixation for atypical hangman's fracture: A minimally invasive technique using the tubular retractor system. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2019 Dec:70():146-150. doi: 10.1016/j.jocn.2019.08.046. Epub 2019 Aug 17 [PubMed PMID: 31431401]
Soliman MAR, Kwan BYM, Jhawar BS. Minimally Invasive Unilateral Percutaneous Transfracture Fixation of a Hangman's Fracture Using Neuronavigation and Intraoperative Fluoroscopy. World neurosurgery. 2019 Feb:122():90-95. doi: 10.1016/j.wneu.2018.10.140. Epub 2018 Nov 1 [PubMed PMID: 30391610]
Daves GD Jr. The occurrence of natural stable analogues. Implications for the design of therapeutic agents. Acta pharmaceutica Suecica. 1987:24(6):275-88 [PubMed PMID: 3330895]
Level 3 (low-level) evidenceOswald KAC, Deml MC, Heldner MR, Seiffge D, Bigdon SF, Albers CE. Intraoperative color-coded duplex ultrasound for safe surgical reduction of displaced hangman fractures in patients with atypical course of the vertebral artery: A case report of two patients. Trauma case reports. 2022 Feb:37():100573. doi: 10.1016/j.tcr.2021.100573. Epub 2021 Dec 9 [PubMed PMID: 34917739]
Level 3 (low-level) evidenceXu D, Gan K, Wang Y, Wang Y, Ma W. Comparison of C2-3 Pedicle Screw Fixation With C2 Spinous Muscle Complex and Iliac Bone Graft for Instable Hangman Fracture. Frontiers in surgery. 2021:8():723078. doi: 10.3389/fsurg.2021.723078. Epub 2021 Nov 26 [PubMed PMID: 34901137]
Ashraf AM, Houten JK. A Potentially Advantageous Use of a Zero-Profile, Stand-Alone Anterior Interbody Spacer at C2-3 for the Treatment of Hangman's Fracture: A Technical Case Report. Cureus. 2021 Jun:13(6):e16059. doi: 10.7759/cureus.16059. Epub 2021 Jun 30 [PubMed PMID: 34354875]
Level 3 (low-level) evidenceBasankin IV, Giulzatyan АА, Nesterenko PB, Bagaudinov АB, Tayurski DА, Mukhanov МL. Experience of Using Transpedicular Osteosynthesis in Traumatic Spondylolisthesis of the Axis. Sovremennye tekhnologii v meditsine. 2021:13(5):47-53. doi: 10.17691/stm2021.13.5.06. Epub 2021 Oct 29 [PubMed PMID: 35265349]
Liu Y, Zhu Y, Li X, Chen J, Yang S, Yang H, Jiang W. A new transpedicular lag screw fixation for treatment of unstable Hangman's fracture: a minimum 2-year follow-up study. Journal of orthopaedic surgery and research. 2020 Sep 1:15(1):372. doi: 10.1186/s13018-020-01911-3. Epub 2020 Sep 1 [PubMed PMID: 32873313]
Agrawal M, Sawarkar D, Singh PK, Mishra S, Meena R, Gupta DK, Chandra PS, Kale SS. Posterior fixation for paediatric and adolescent unstable hangman's fracture: evolution to C1 sparing techniques. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2021 Jul:37(7):2319-2327. doi: 10.1007/s00381-021-05140-9. Epub 2021 Mar 30 [PubMed PMID: 33783618]
Sawarkar D, Agrawal M, Singh PK, Mishra S, Agrawal D, Kumar A, Verma S, Doddamani R, Meena R, Garg K, Gurjar H, Chandra PS, Kale SS. Evolution to Pedicle Reformation Technique in Surgical Management of Hangman's Fracture. World neurosurgery. 2021 May:149():e481-e490. doi: 10.1016/j.wneu.2021.02.001. Epub 2021 Feb 7 [PubMed PMID: 33567364]
Yuan S, Wei B, Tian Y, Yan J, Xu W, Wang L, Liu X. Posterior temporary C1-2 fixation for 3-part fractures of the axis (odontoid dens and Hangman fractures). Medicine. 2018 Nov:97(48):e12957. doi: 10.1097/MD.0000000000012957. Epub [PubMed PMID: 30508884]
Ryken TC, Hadley MN, Aarabi B, Dhall SS, Gelb DE, Hurlbert RJ, Rozzelle CJ, Theodore N, Walters BC. Management of isolated fractures of the axis in adults. Neurosurgery. 2013 Mar:72 Suppl 2():132-50. doi: 10.1227/NEU.0b013e318276ee40. Epub [PubMed PMID: 23417186]
Yunde A, Furuya T, Orita S, Ohtori S, Yokogawa N, Nakashima H, Segi N, Funayama T, Ikegami S, Nakajima H, Watanabe K, Hasegawa T, Tonomura H, Terashima Y, Hashimoto K, Suzuki N, Uei H, Kiyasu K, Tominaga H, Sakai D, Kaito T, Inoue G, Okada S, Imagama S, Kato S. Hangman's Fracture in Geriatric Population: A Nationwide Multicenter Study in Japan. Global spine journal. 2025 Mar:15(2):921-929. doi: 10.1177/21925682231216925. Epub 2023 Nov 17 [PubMed PMID: 37977098]
Level 2 (mid-level) evidenceKarakoyun DO, Yılmaz A, Uzlu O, Dağlıoğlu E, Işık HS. Vertebral arteriovenous fistula due to blunt neck trauma: A case report. Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES. 2022 Jun:28(6):871-875. doi: 10.14744/tjtes.2020.72506. Epub [PubMed PMID: 35652878]
Level 3 (low-level) evidenceSarath Chander V, Govindasamy R, Rudrappa S, Gopal S. Unstable Hangman Fracture Complicated by Vertebral-Venous Fistula: Surgical Considerations and Review of Literature. World neurosurgery. 2021 Jan:145():409-415. doi: 10.1016/j.wneu.2020.09.109. Epub 2020 Sep 25 [PubMed PMID: 32987171]
Kaiser R, Saur K, Smolanka A, Ullas G, Beneš V. Type-III Hangman's fracture combined with serious cerebrovascular injury after near-hanging: a first case report and review of the literature. British journal of neurosurgery. 2023 Aug:37(4):825-828. doi: 10.1080/02688697.2019.1671952. Epub 2019 Sep 28 [PubMed PMID: 31566025]
Level 3 (low-level) evidenceLáinez Ramos-Bossini AJ, Gálvez López R, Pastor Rull J. Vertebral artery dissection secondary to hangman's fracture. Medicina clinica. 2020 Mar 13:154(5):195-196. doi: 10.1016/j.medcli.2019.02.008. Epub 2019 Apr 4 [PubMed PMID: 30954291]
Foster MA, Gridley DG, Lettieri SC, Feiz-Erfan I. Brown-Sequard syndrome associated with hangman fracture after blunt trauma: A case report. Surgical neurology international. 2022:13():150. doi: 10.25259/SNI_897_2021. Epub 2022 Apr 15 [PubMed PMID: 35509566]
Level 3 (low-level) evidenceYang Y, Dai L, Ma L, Gao X, Liu H. Incidence of dysphagia and dysphonia after Hangman's fractures: Evidence from 93 patients. Medicine. 2018 Dec:97(49):e13552. doi: 10.1097/MD.0000000000013552. Epub [PubMed PMID: 30544470]
Pehler S, Jones R, Staggers JR, Antonetti J, McGwin G, Theiss SM. Clinical Outcomes of Cervical Facet Fractures Treated Nonoperatively With Hard Collar or Halo Immobilization. Global spine journal. 2019 Feb:9(1):48-54. doi: 10.1177/2192568218771911. Epub 2018 May 10 [PubMed PMID: 30775208]
Level 2 (mid-level) evidence