Introduction
Hand hygiene is the most critical intervention for patient safety, as contaminated hands are the primary source of health care–associated infections (HAIs). Maintaining proper hygiene strategies is essential in all clinical settings, with recent data suggesting that evidence-based infection control could prevent up to 70% of HAIs.[1][2]
International infection control guidelines consistently identify hand hygiene as the cornerstone of strategies to reduce pathogen transmission in healthcare environments. Proper adherence to recommended hand hygiene indications during patient care is therefore essential to interrupt the spread of microorganisms between patients, healthcare workers, and the clinical environment.[3]
Despite this, a significant gap remains between guidelines and practice. Compliance remains alarmingly low, with more than 60% of healthcare professionals failing to consistently follow established protocols, indicating that clinical knowledge alone is insufficient and suggesting that systemic or environmental barriers continue to hinder routine adherence.[4]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
According to the Centers for Disease Control and Prevention (CDC), the impact of hand hygiene on pathogen transmission is closely related to skin anatomy. The skin serves as a critical protective barrier against microorganisms and environmental hazards.[5] Structurally, it consists of the epidermis (with the stratum corneum as its outermost layer), dermis, and hypodermis.
Resident flora colonizes the skin surface and deeper skin structures, including hair follicles and sebaceous glands. These microorganisms contribute to skin health by providing microbial antagonism and competing for nutrients. Although typically nonpathogenic on intact skin, they can cause infection if introduced into sterile body sites, the eyes, or areas of nonintact skin.[6][Springer. Textbook of Plastic and Reconstructive Surgery. 2022.]
In contrast, healthcare professionals acquire transient microorganisms through direct contact with patients or contaminated surfaces. These organisms colonize the superficial layers of the skin and are more easily removed with routine hand hygiene. Transient flora are the primary organisms transmitted via healthcare professionals' hands and are most strongly associated with HAIs.[7][8][9][10][11]
Indications
The CDC defines hand hygiene as cleansing the hands with soap and water, antiseptic hand washes, alcohol-based hand rubs (eg, sanitizers, foams, or gels), and surgical hand antisepsis. Healthcare professionals should use soap and water for hand hygiene when hands are visibly soiled or contaminated with blood or body fluids, before eating, and after using the restroom.[3]
The World Health Organization (WHO) developed the Five Moments for Hand Hygiene in 2009 to guide clinical practice. Healthcare professionals should perform hand hygiene:
- Before touching a patient
- Before performing a clean or aseptic procedure
- After exposure to body fluids or after glove removal
- After contact with a patient
- After contact with the patient’s immediate environment [3]
Healthcare facilities increasingly monitor staff adherence to hand hygiene practices, with increasing compliance as part of ongoing efforts to enhance patient safety and reduce infection risk.
When hands are not visibly soiled, healthcare professionals should use alcohol-based hand rubs as the preferred method for hand hygiene. These products are faster and more convenient than soap and water while remaining highly effective. Clinicians should apply alcohol-based hand rubs according to manufacturer recommendations, typically placing 3 to 5 mL in the palm and rubbing all hand surfaces vigorously until dry, which generally takes about 20 seconds.[3]
Healthcare professionals caring for immunocompromised patients must strictly adhere to hand hygiene practices, as this population is particularly susceptible to opportunistic infections. Handwashing with soap and water effectively removes most transient gram-negative organisms within seconds, while chlorhexidine-based preparations may provide enhanced activity against transient gram-positive bacteria.[12] Handwashing with soap and water is specifically required following potential exposure to spore-forming or non-enveloped pathogens such as Clostroidies difficile, norovirus, and Bacillus anthracis. Because these organisms are resistant to alcohol-based and many antiseptic agents, mechanical removal through vigorous handwashing is necessary to eliminate spores from the skin.[13][14][15]
Although routine hand hygiene is essential for all patient interactions, more stringent protocols are required in operative and invasive settings. Surgical hand antisepsis, commonly referred to as the surgical scrub, is designed to achieve a greater and more sustained reduction in microbial burden before sterile procedures. The CDC recommends that agents used for surgical hand antisepsis significantly reduce microbial burden on intact skin, possess broad-spectrum antimicrobial activity, act rapidly, provide persistent effects, and minimize skin irritation.
Equipment
Required Equipment for Routine Handwashing
- Clean running water (preferably warm)
- Sink with appropriate drainage
- Soap (antimicrobial or nonantimicrobial)
- Paper towels or clean disposable drying materials
- Waste receptacle for towel disposal (hands-free preferred)
- Alcohol-based hand sanitizer (if used as an adjunct when hands are not visibly soiled)
- Nail cleaner or pick (if visibly soiled debris is present) [3]
Required Equipment for Surgical Hand Antisepsis
- Hands-free sink (eg, foot-, knee-, or sensor-operated controls)
- Running water (temperature-controlled)
- Pre-packaged sterile scrub/nail kit
- Antimicrobial surgical scrub solution (eg, chlorhexidine or povidone-iodine)
- Alcohol-based surgical hand rub (if using alcohol-based technique)
- Sterile towels for drying hands and forearms
- Surgical attire, such as a cap, mask, eye protection, and shoe covers
- Sterile gloves (to be donned after antisepsis is complete) [16][17]
Personnel
Hand hygiene is a shared responsibility that requires consistent adherence across all disciplines, including clinicians, advanced practice practitioners, nurses, allied health professionals, infection prevention specialists, and support staff, with patient and caregiver engagement as active partners in infection prevention to reduce health care–associated infections and improve patient safety.
Healthcare professionals who have direct patient contact should keep their fingernails short, clean, and free of artificial nails and nail polish. Long or artificial nails are associated with increased colonization of pathogens in the nail area and have been linked to outbreaks of infection, particularly in intensive care units, neonatal intensive care units, and surgical settings.[18][19] Well-manicured nails and adherence to the facility-specific guidelines outlining artificial nail policies are vital to hand hygiene practices. Current guidelines suggest nails should be less than 0.5 cm long.[3]
Technique or Treatment
Handwashing Technique
Handwashing is the process of cleansing the hands with antimicrobial or nonantimicrobial soap and water for at least 15 to 20 seconds using friction to remove microorganisms from all surfaces of the hands and wrists. Proper technique is essential to ensure effective decontamination and prevent pathogen transmission.
The procedure should begin by standing in front of the sink while avoiding contact with sink surfaces, as this may lead to contamination and require restarting the process. Warm water should be used to wet the hands and wrists thoroughly. Hands should be kept below the elbows throughout the procedure to allow water to flow from less contaminated to more contaminated areas, facilitating the removal of microorganisms.
Approximately 3 to 5 mL of soap should be applied and evenly distributed to create a lather. Vigorous friction should be performed for a minimum of 15 to 20 seconds, ensuring the cleaning of all surfaces, including the palms, dorsum of the hands, wrists, interdigital spaces, fingertips, thumbs, cuticles, and areas beneath the nails. Techniques such as interlacing fingers and alternating palm-to-dorsum movements help ensure complete coverage. The WHO recommends a structured 6-step approach that includes palm-to-palm, right palm over the left dorsum and vice versa, palm-to-palm with fingers interlaced, backs of fingers to opposing palms, and rubbing of thumbs and fingertips (see Image. Hand Washing Technique, Hand Hygiene).[3]
Hands and wrists should then be rinsed thoroughly with water to ensure complete removal of soap. During rinsing, the hands should be kept below the elbows to prevent recontamination. Drying should be performed using a clean or disposable towel, avoiding contact with sink surfaces or faucet handles. A towel should be used to turn off the water to prevent recontamination. In some clinical settings, such as surgical or trauma bays, sinks may be equipped with automatic shut-off timers to further reduce contamination risk.
Surgical Hand Antisepsis
Surgical hand antiseptic practices originated in the late 19th century and remain a cornerstone of preventing surgical site infections. Unlike routine hand hygiene, surgical hand antisepsis requires a more rigorous technique to eliminate transient microorganisms and significantly reduce resident skin flora before invasive procedures. Failure to adequately perform surgical hand antisepsis can result in the transfer of pathogens to the operative field, contributing to surgical site infections, one of the most common healthcare-associated infections in surgical patients.[20][21]
According to the CDC, surgical hand preparation involves using either antimicrobial soap or an alcohol-based hand rub before donning sterile gloves. These methods are designed to achieve rapid, broad-spectrum antimicrobial activity with sustained effects throughout the procedure.[20]
Technique
Before beginning the surgical scrub, all jewelry, including rings, watches, and bracelets, should be removed, and the hands and forearms should be inspected for cuts, abrasions, or skin breakdown. Appropriate personal protective equipment, including caps, masks, eye protection, and shoe covers, should be applied before initiating the procedure. Using hands-free controls (eg, foot or knee pedals), healthcare professionals should adjust the water to a comfortable warm temperature. The hands and forearms should be rinsed while maintaining the hands above the elbows to prevent contamination from water runoff. Debris beneath the fingernails should be removed using a nail cleaner under running water.
When using an antimicrobial scrub, the hands, fingers, and forearms should be scrubbed systematically with a sterile, single-use sponge or brush for approximately 2 to 6 minutes, following manufacturer and institutional guidelines. Scrubbing should ensure thorough coverage of all surfaces, including nails, interdigital spaces, palms, dorsum of the hands, and forearms. Prolonged scrub times (eg, ≥10 minutes) provide no additional benefit and increase the risk of skin irritation. Some institutions use shorter, staged scrub techniques or alcohol-based formulations instead of traditional scrubbing.[20][21]
After scrubbing, the antiseptic agent should be rinsed off, allowing water to flow from the fingertips toward the elbows while maintaining proper hand positioning. Hands and forearms should remain elevated and away from the body at all times. This positioning is essential because, after scrubbing, the hands are the cleanest area, while the forearms and elbows are relatively less clean; keeping the hands elevated prevents the backflow of contaminated water. The water should be turned off using hands-free controls. The clinician should then proceed to the sterile field and dry the hands and forearms using a sterile towel, beginning with 1 hand and using a separate portion (or towel) for the other to prevent cross-contamination. After drying, alcohol-based hand rubs, if used, should be applied according to manufacturer recommendations and allowed to dry completely before donning sterile gloves.[20][21]
Clinical Significance
Hand hygiene is a critical component of infection prevention, as it significantly reduces the transmission of microorganisms and health care–associated infections and reduces the risk of occupational exposure to infectious diseases.[22]
Health care–associated infections are associated with increased morbidity, mortality, and healthcare costs.[23] Consistent adherence to proper hand hygiene practices is therefore essential to delivering safe, high-quality, and cost-effective patient care.[24]
Multiple factors, including education, workflow design, ergonomics, and staffing, are associated with hand hygiene compliance and represent key targets for improving adherence.[24] Addressing these factors through system-level and behavioral interventions is key to improving adherence and reducing infection rates.[25][26][27]
Enhancing Healthcare Team Outcomes
Handwashing is a foundational component of infection prevention and control in clinical practice. This procedure involves cleansing the hands with soap and water or using alcohol-based hand rubs to remove transient microorganisms and reduce pathogen transmission between patients, healthcare providers, and the healthcare environment. Adherence to proper technique and timing is critical, particularly in alignment with the WHO Five Moments for Hand Hygiene: before touching a patient, before clean or aseptic procedures, after body fluid exposure, after touching a patient, and after contact with the patient's surroundings. Consistent application of these principles remains one of the most effective strategies for reducing HAIs and improving patient safety. Effective hand hygiene requires coordinated efforts across the healthcare team, including clinicians, advanced practitioners, nurses, pharmacists, and other allied health professionals.
Clinicians, nurses, and advanced care practitioners play a key role in setting expectations, modeling adherence, and integrating hand hygiene into clinical decision-making and patient care. Leadership is responsible for ensuring access to appropriate resources, implementing policies, monitoring adherence, and incorporating hand hygiene into staff orientation and ongoing training. System-level strategies such as audits, feedback mechanisms, and performance improvement initiatives help sustain compliance and accountability.
Interprofessional communication strengthens adherence by promoting shared responsibility and mutual accountability among team members. Open dialogue allows staff to address lapses promptly and reinforces standardized practices across disciplines. Additionally, engaging patients and visitors as active participants in care enhances safety. These individuals should be encouraged to speak up when they witness lapses in hand hygiene, fostering a transparent, safety-focused environment. Through collaborative practice, consistent communication, and strong leadership support, healthcare teams can improve patient-centered care, reduce infection risk, enhance safety outcomes, and optimize overall team performance.
Media
(Click Image to Enlarge)
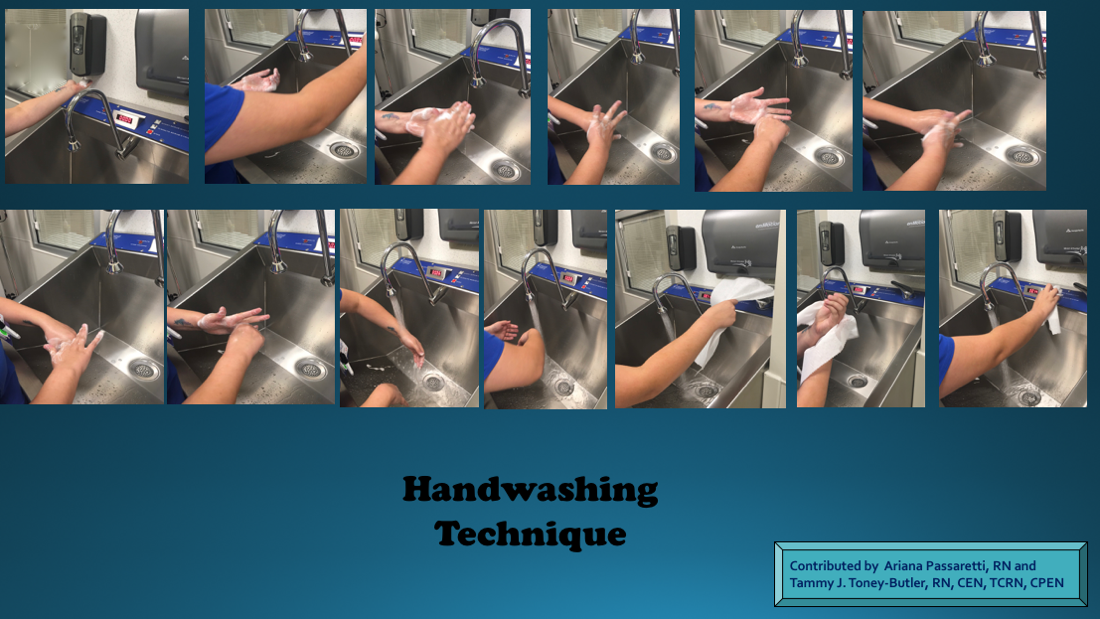
Hand Washing Technique, Hand Hygiene
Contributed by A Passaretti, RN, and TJ Toney-Butler, RN, CEN, TCRN, CPEN
References
Lotfinejad N, Peters A, Tartari E, Fankhauser-Rodriguez C, Pires D, Pittet D. Hand hygiene in health care: 20 years of ongoing advances and perspectives. The Lancet. Infectious diseases. 2021 Aug:21(8):e209-e221. doi: 10.1016/S1473-3099(21)00383-2. Epub [PubMed PMID: 34331890]
Level 3 (low-level) evidenceBlomgren PO, Leo Swenne C, Lytsy B, Hjelm K. Hand hygiene knowledge among nurses and nursing students-a descriptive cross-sectional comparative survey using the WHO's "Hand Hygiene Knowledge Questionnaire". Infection prevention in practice. 2024 Jun:6(2):100358. doi: 10.1016/j.infpip.2024.100358. Epub 2024 Mar 11 [PubMed PMID: 38586127]
Level 2 (mid-level) evidence. WHO Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge Clean Care Is Safer Care. 2009:(): [PubMed PMID: 23805438]
Level 3 (low-level) evidenceAfework A, Tamene A. Uncovering the obstacles: a comprehensive analysis of barriers to hand hygiene adherence among healthcare providers: a systematic review. BMC infectious diseases. 2025 Apr 10:25(1):502. doi: 10.1186/s12879-025-10924-4. Epub 2025 Apr 10 [PubMed PMID: 40211179]
Level 1 (high-level) evidenceHoang D, Khawar N, George M, Gad A, Sy F, Narula P. Video didactic at the point of care impacts hand hygiene compliance in the neonatal intensive care unit (NICU). Journal of healthcare risk management : the journal of the American Society for Healthcare Risk Management. 2018 Apr:37(4):9-15. doi: 10.1002/jhrm.21314. Epub 2018 Feb 6 [PubMed PMID: 29405485]
Kampf G, Kramer A. Epidemiologic background of hand hygiene and evaluation of the most important agents for scrubs and rubs. Clinical microbiology reviews. 2004 Oct:17(4):863-93, table of contents [PubMed PMID: 15489352]
Kapil R, Bhavsar HK, Madan M. Hand hygiene in reducing transient flora on the hands of healthcare workers: an educational intervention. Indian journal of medical microbiology. 2015 Jan-Mar:33(1):125-8. doi: 10.4103/0255-0857.148409. Epub [PubMed PMID: 25560015]
Biezen R, Grando D, Mazza D, Brijnath B. Visibility and transmission: complexities around promoting hand hygiene in young children - a qualitative study. BMC public health. 2019 Apr 11:19(1):398. doi: 10.1186/s12889-019-6729-x. Epub 2019 Apr 11 [PubMed PMID: 30975108]
Level 2 (mid-level) evidenceKang YS, Chang YJ. Using a motion-controlled game to teach four elementary school children with intellectual disabilities to improve hand hygiene. Journal of applied research in intellectual disabilities : JARID. 2019 Jul:32(4):942-951. doi: 10.1111/jar.12587. Epub 2019 Apr 2 [PubMed PMID: 30941883]
Le CD, Lehman EB, Nguyen TH, Craig TJ. Hand Hygiene Compliance Study at a Large Central Hospital in Vietnam. International journal of environmental research and public health. 2019 Feb 19:16(4):. doi: 10.3390/ijerph16040607. Epub 2019 Feb 19 [PubMed PMID: 30791457]
Korhonen A, Vuori A, Lukkari A, Laitinen A, Perälä M, Koskela T, Pölkki T. Increasing nursing students' knowledge of evidence-based hand-hygiene: A quasi-experimental study. Nurse education in practice. 2019 Feb:35():104-110. doi: 10.1016/j.nepr.2018.12.009. Epub 2019 Jan 2 [PubMed PMID: 30772734]
Alothman A. Infection control and the immunocompromised host. Saudi journal of kidney diseases and transplantation : an official publication of the Saudi Center for Organ Transplantation, Saudi Arabia. 2005 Oct-Dec:16(4):547-55 [PubMed PMID: 18202509]
Level 3 (low-level) evidenceYap M, Chau ML, Hartantyo SHP, Oh JQ, Aung KT, Gutiérrez RA, Ng LC. Microbial Quality and Safety of Sushi Prepared with Gloved or Bare Hands: Food Handlers' Impact on Retail Food Hygiene and Safety. Journal of food protection. 2019 Apr:82(4):615-622. doi: 10.4315/0362-028X.JFP-18-349. Epub [PubMed PMID: 30907665]
Level 2 (mid-level) evidenceMutters R, Warnes SL. The method used to dry washed hands affects the number and type of transient and residential bacteria remaining on the skin. The Journal of hospital infection. 2019 Apr:101(4):408-413. doi: 10.1016/j.jhin.2018.12.005. Epub 2018 Dec 8 [PubMed PMID: 30537524]
Boyce JM. Hand and environmental hygiene: respective roles for MRSA, multi-resistant gram negatives, Clostridioides difficile, and Candida spp. Antimicrobial resistance and infection control. 2024 Sep 27:13(1):110. doi: 10.1186/s13756-024-01461-x. Epub 2024 Sep 27 [PubMed PMID: 39334403]
Olivia C, Ibrahim K, Kurniawan T. Which Surgical Hand Preparation Method Is More Effective? A Comparative Study of Hand Rub and Hand Scrub. Nursing reports (Pavia, Italy). 2025 Jul 2:15(7):. doi: 10.3390/nursrep15070242. Epub 2025 Jul 2 [PubMed PMID: 40710937]
Level 2 (mid-level) evidenceCanton SP, Foley CE, Fulcher I, Newcomb LK, Rindos N, Donnellan NM. Reliability and Discriminant Validity of a Checklist for Surgical Scrubbing, Gowning and Gloving. International journal of medical students. 2022:10(1):18-24. doi: 10.5195/ijms.2021.1221. Epub 2022 Apr 5 [PubMed PMID: 35692606]
Moolenaar RL, Crutcher JM, San Joaquin VH, Sewell LV, Hutwagner LC, Carson LA, Robison DA, Smithee LM, Jarvis WR. A prolonged outbreak of Pseudomonas aeruginosa in a neonatal intensive care unit: did staff fingernails play a role in disease transmission? Infection control and hospital epidemiology. 2000 Feb:21(2):80-5 [PubMed PMID: 10697282]
Parry MF, Grant B, Yukna M, Adler-Klein D, McLeod GX, Taddonio R, Rosenstein C. Candida osteomyelitis and diskitis after spinal surgery: an outbreak that implicates artificial nail use. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2001 Feb 1:32(3):352-7 [PubMed PMID: 11170941]
Widmer AF, Rotter M, Voss A, Nthumba P, Allegranzi B, Boyce J, Pittet D. Surgical hand preparation: state-of-the-art. The Journal of hospital infection. 2010 Feb:74(2):112-22. doi: 10.1016/j.jhin.2009.06.020. Epub 2009 Aug 28 [PubMed PMID: 19716627]
Level 3 (low-level) evidenceTanner J, Dumville JC, Norman G, Fortnam M. Surgical hand antisepsis to reduce surgical site infection. The Cochrane database of systematic reviews. 2016 Jan 22:2016(1):CD004288. doi: 10.1002/14651858.CD004288.pub3. Epub 2016 Jan 22 [PubMed PMID: 26799160]
Level 1 (high-level) evidenceAllegranzi B, Pittet D. Role of hand hygiene in healthcare-associated infection prevention. The Journal of hospital infection. 2009 Dec:73(4):305-15. doi: 10.1016/j.jhin.2009.04.019. Epub 2009 Aug 31 [PubMed PMID: 19720430]
Glowicz JB, Landon E, Sickbert-Bennett EE, Aiello AE, deKay K, Hoffmann KK, Maragakis L, Olmsted RN, Polgreen PM, Trexler PA, VanAmringe MA, Wood AR, Yokoe D, Ellingson KD. SHEA/IDSA/APIC Practice Recommendation: Strategies to prevent healthcare-associated infections through hand hygiene: 2022 Update. Infection control and hospital epidemiology. 2023 Mar:44(3):355-376. doi: 10.1017/ice.2022.304. Epub 2023 Feb 8 [PubMed PMID: 36751708]
Yue J, Pan H. Enhancing hand hygiene compliance in healthcare settings: a long time intervention study. Frontiers in public health. 2025:13():1588336. doi: 10.3389/fpubh.2025.1588336. Epub 2025 Aug 20 [PubMed PMID: 40910066]
Suen LKP, So ZYY, Yeung SKW, Lo KYK, Lam SC. Epidemiological investigation on hand hygiene knowledge and behaviour: a cross-sectional study on gender disparity. BMC public health. 2019 Apr 11:19(1):401. doi: 10.1186/s12889-019-6705-5. Epub 2019 Apr 11 [PubMed PMID: 30975130]
Level 2 (mid-level) evidenceGuo N, Ma H, Deng J, Ma Y, Huang L, Guo R, Zhang L. Effect of hand washing and personal hygiene on hand food mouth disease: A community intervention study. Medicine. 2018 Dec:97(51):e13144. doi: 10.1097/MD.0000000000013144. Epub [PubMed PMID: 30572426]
Gomez NJ. Hand Washing Adherence - Is That Really Our Goal? Nephrology nursing journal : journal of the American Nephrology Nurses' Association. 2018 Jul-Aug:45(4):393-394 [PubMed PMID: 30303649]