Introduction
Greenstick fractures are common pediatric orthopedic injuries that are characterized by bending and partial fracturing of the bone without complete disruption, resulting in cortical and periosteal disruption on one side while the opposite cortex remains intact. The pediatric skeleton is structurally and biologically distinct from the adult skeleton, reflecting the demands of rapid longitudinal growth. Compared with adult bone, developing bone contains a higher proportion of cartilage and exhibits greater pliability, allowing greater energy absorption and a greater tendency to bend under load rather than sustain a complete cortical break. These material properties, combined with robust healing potential, create pediatric-specific injury patterns and management considerations.[1]
A key anatomic feature underlying these differences is the open physis (growth plate), a highly organized cartilaginous structure responsible for longitudinal growth before skeletal maturity. In long bones, the physis lies between the epiphysis and the metaphysis. The epiphysis is adjacent to the joint surface, whereas the metaphysis is the flared region transitioning to the diaphysis or shaft. Growth at the physis occurs through endochondral ossification, defined by progressive replacement of a cartilage scaffold by bone. Endochondral ossification occurs in long bones, in contrast to intramembranous ossification, which forms many flat bones. Histologically, the physis is organized into functional zones that reflect chondrocyte differentiation and matrix maturation, including the resting (reserve), proliferative, hypertrophic, and provisional calcification zones, where calcified cartilage undergoes remodeling with vascular invasion and new bone deposition.[2]
Beyond the physis, the material properties of pediatric bone favor bending and incomplete fracture rather than the complete cortical disruption more commonly seen in adults. Pediatric bone has lower osteoid density and greater porosity than adult bone, with a larger relative contribution of Haversian canals. Greater porosity and lower osteoid density allow energy absorption and deformation before fracture. Energy absorption and deformation are further enhanced by the thicker, stronger, and more biologically active pediatric periosteum. A robust periosteal sleeve functions as a stabilizing hinge, limiting displacement, supporting rapid healing and remodeling, and contributing to distinctive pediatric fracture patterns, such as greenstick fractures. These incomplete, partial-thickness fractures are analogous to a bent fresh "green" twig.[3][4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The most common cause is low- or moderate-energy trauma to the upper extremity, such as a fall onto an outstretched hand (FOOSH) during play or sports. Greenstick fractures most often occur in the forearm.[5][6] Less commonly, greenstick fractures follow higher-energy mechanisms, as in motor vehicle collisions or direct blows. Nonaccidental trauma is an important etiologic consideration when the reported mechanism is absent, inconsistent with developmental stage, or discordant with physical examination findings.[7]
Host factors that reduce bone mineralization increase fracture susceptibility. For example, pediatric studies and meta-analyses consistently demonstrate an association between low serum 25-hydroxyvitamin D concentrations and increased fracture risk.[8]
Epidemiology
Greenstick fractures are among the most common fracture types in children, occurring most frequently in those younger than 10 years, although fractures can occur at any age.[9] Greenstick fractures occur equally in boys and girls, but the average age at presentation is higher in boys than in girls.[10][11] Incidence fluctuates seasonally, peaking during the spring and summer when children are more active outdoors and reaching the lowest levels during winter.[12] The upper extremities are the most common sites of greenstick fractures because FOOSH is the predominant injury mechanism. Accidental trauma, particularly falls during play or sports, is the leading cause.[13]
Pathophysiology
Greenstick fractures occur when trauma bends a bone, causing the outer (convex) cortex to crack while the inner (concave) cortex compresses and bends without complete disruption. Greater pliability and energy absorption in pediatric bone than in adult bone allow incomplete fracture rather than complete cortical disruption.[14] A thick, biologically active pediatric periosteum helps maintain cortical continuity, limiting displacement and contributing to the characteristic hinged, incomplete fracture pattern.[15] The most common clinical findings are localized pain, swelling, point tenderness, and refusal to use the affected limb, often accompanied by mild angulation or visible deformity when bending is substantial.[16]
Histopathology
The histopathology of a greenstick fracture demonstrates incomplete cortical failure. The tension (convex) cortex shows a partial cortical break with microcracking and focal disruption of the periosteal attachment, whereas the compression (concave) cortex remains continuous but demonstrates plastic deformation and microdamage.[17] The periosteum is a major source of osteochondral progenitors during secondary bone healing. The periosteum in greenstick fractures is typically disrupted on the tension side and relatively preserved on the hinge side, contributing to asymmetric periosteal callus formation.[18]
At the injury site, ruptured vessels generate an early fracture hematoma composed of fibrin, erythrocytes, marrow-derived cells, and infiltrating inflammatory cells.[19] Histologic repair progresses through granulation tissue formation and then callus formation. Woven bone forms through intramembranous ossification near stable, well-perfused surfaces, whereas fibrocartilage develops in regions of greater motion and later undergoes endochondral ossification and mineralization to form a hard callus.[20] Remodeling follows through osteoclast-mediated resorption, replacement of woven bone with lamellar bone, and restoration of normal cortical architecture.
History and Physical
Greenstick fractures most often follow a FOOSH or another low- to moderate-energy mechanism that bends the limb, such as a sports collision, playground fall, or direct blow. Patients typically report immediate pain at the injury site, with worsening pain during limb use or rotation. Some children may avoid using the affected extremity. In younger children, the history may be nonspecific, and decreased spontaneous use of the extremity may be the only clinical clue.[21]
Age, sex, anatomic location, soft tissue involvement (open versus closed injury), and mechanism of injury are important components of the history. Physical examination should assess fracture location, soft tissue involvement, and neurovascular status. The joints proximal and distal to the injury should also be evaluated for occult or multiple fractures. History taking should also address handedness, prior fracture history, analgesic use, and concerning contextual features, including an inconsistent mechanism, delayed presentation, and recurrent injuries.[22]
Physical examination most commonly demonstrates point tenderness over the involved bone and localized swelling, sometimes accompanied by bruising. Visible angulation or deformity may be present, particularly in more unstable incomplete fractures. A complete assessment includes inspection for skin compromise and documentation of distal neurovascular status, evaluating pulses, capillary refill, sensation, and motor function at presentation and after any immobilization or manipulation, with vigilance for evolving compartment syndrome.[23]
Evaluation
Greenstick fractures are diagnosed clinically and confirmed with imaging (see Image. Greenstick Fracture of the Ulna). Routine laboratory testing is not required for an otherwise healthy child with an isolated injury that has a clear traumatic mechanism. Plain radiography is the standard initial imaging study for suspected greenstick fractures. At least 2 orthogonal views, usually anteroposterior and lateral, of the injured bone are obtained. Imaging should include the joints proximal and distal to the injury to avoid missing associated injuries (see Image. Distal Tibia and Fibula Greenstick Fracture). Repeat studies should confirm alignment before discharge when manipulation or reduction is performed.[24][25]
The most definitive radiographic finding is cortical disruption on the tension side of the bone.[26] The compression side remains intact but appears bent or curved, reflecting failure of the bone to return to its original shape after the force is removed.
Treatment / Management
Initial treatment prioritizes neurovascular assessment, pain control, and temporary immobilization. The injured limb is typically immobilized with a well-molded splint or cast.[27] Most greenstick fractures are treated with cast immobilization after swelling is controlled and alignment is acceptable. Closed reduction is performed when angulation exceeds age- and location-dependent tolerance, commonly under procedural sedation or anesthesia, followed by cast immobilization. High-quality cast application is essential to minimize the risk of further displacement.[28]
Early planned follow-up with repeat radiographs is commonly recommended because greenstick fractures can remain unstable and continue to displace, often within 7 to 14 days or earlier for borderline alignment.[29] Immobilization typically lasts 3 to 6 weeks, depending on age, fracture location, and stability, with earlier return of motion in younger children. Operative treatment is uncommon and reserved for fractures with unacceptable alignment despite initial nonoperative management, loss of reduction or progressive displacement, open injury, or neurovascular compromise.[30] Published British Orthopaedic Association Standards for Trauma (BOAST) guidelines emphasize timely assessment, appropriate analgesia, early manipulation or reduction when indicated, high-quality cast application, and structured follow-up for pediatric forearm fractures.(A1)
Differential Diagnosis
Differential diagnoses include Salter-Harris fractures, torus fractures, toddler fractures (nondisplaced spiral fractures of the distal tibia), spiral fractures, open fractures, pathologic fractures, nondisplaced fractures, and plastic deformities.[31] Fractures resulting from nonaccidental trauma should also be considered when the clinical history or injury pattern raises concern.
Prognosis
The prognosis for greenstick fractures is generally excellent because the thick, biologically active pediatric periosteum facilitates rapid healing and substantial remodeling potential. Clinical stability is often achieved within 3 to 6 weeks because of the intact compression cortex and the high metabolic activity of the periosteum. Residual angulation is typically corrected through normal skeletal growth. Most patients achieve a full return to preinjury activity levels without long-term functional deficits, provided initial angulation is managed appropriately.[32][33] Secondary displacement is associated with greater initial displacement and poor cast quality.[34]
Complications
Loss of reduction is the most common complication of greenstick fractures, which are less stable than comparable buckle fractures and can continue to angulate after initial immobilization. Remanipulation or recasting is sometimes required to maintain acceptable alignment. Malunion can occur when residual angulation or rotational deformity is not corrected or is allowed to progress. Malalignment, particularly in diaphyseal fractures, can result in functional limitations despite children's substantial remodeling potential.[35] Refracture is another potential complication, often occurring when callus is present but cortical strength and remodeling remain incomplete.[36][37]
Immobilization-related complications require careful monitoring. These adverse events include skin breakdown, pressure sores, thermal injury during casting, cast tightness with pain, and inadequate cast molding or padding.[38] Severe complications are uncommon. Acute compartment syndrome can follow fracture or overly tight casting. Early warning signs include escalating pain, often with passive stretch, and increasing analgesic requirements.[39] Posttraumatic radioulnar synostosis rarely develops but can cause profound loss of forearm rotation.[40]
Postoperative and Rehabilitation Care
Rehabilitation protocols after a pediatric greenstick fracture primarily consist of early protected motion followed by progressive return to normal function after immobilization ends. Priorities during splint or cast treatment include limb elevation to reduce swelling, active finger motion several times daily for upper extremity fractures, and maintenance of range of motion in adjacent joints to minimize stiffness and functional decline.[41]
Stiffness and weakness are common after cast removal but typically resolve with time. Functional limitations may persist at 3 months in a subset of children. Persistent functional limitations warrant a home exercise program and selective referral for rehabilitation when needed. Rehabilitation begins with gentle range-of-motion exercises performed several times daily. Low-impact functional activities, such as writing and eating, are added as tolerated. Progression to strengthening begins after comfortable passive and active motion is achieved. Strength recovery may lag behind symptom improvement and extend over several months.[42] Return to sports is typically staged. Low-risk activities resume first when pain is minimal and functional motion is largely restored. Higher-risk activities, including contact sports, are commonly delayed longer.[43]
Consultations
Orthopedic surgery consultation is appropriate for any child with unacceptable angulation or translation, suspected rotational deformity, both-bone forearm fractures, open fracture, associated dislocation, neurovascular compromise, or failure to maintain alignment in a well-molded splint or cast. Pediatric consultation, child abuse pediatrician consultation, or child protection consultation is indicated when the history is inconsistent with the injury, concerning associated findings are present, or medical evaluation has been delayed.[44]
Deterrence and Patient Education
Most greenstick fractures occur after low-height falls or sports activities, so prevention focuses on reducing fall impact and avoiding high-risk mechanisms.[45] School- and community-based injury prevention studies show that impact-attenuating playground surfaces are associated with lower injury rates and fewer arm fractures.[46] Trampolines are strongly associated with pediatric extremity fractures, including those of the forearm. Family education regarding trampoline safety recommendations and avoidance of high-risk trampoline use, such as in the performance of multiple simultaneous jumpers, can reduce trampoline-related injuries.[47] Protective equipment, including wrist guards, is associated with meaningful reductions in upper extremity injuries for activity-related risks, such as skating.[48]
Education should establish expectations for the typical recovery course. Families should understand that greenstick fractures can displace during the first 1 to 2 weeks. The importance of attending scheduled follow-up visits and obtaining repeat radiographs when recommended should be emphasized. Clear cast and splint care instructions reduce avoidable complications. Recommendations include keeping the cast dry, avoiding insertion of objects for itching, elevating the affected extremity during the first 24 to 72 hours, encouraging frequent finger motion, and returning promptly for increasing pain, tightness, numbness or tingling, finger discoloration, or inability to move the fingers.[49]
Pearls and Other Issues
Additional clinical considerations include the following:
- Some experienced providers intentionally complete the fracture during reduction by breaking the intact cortex. Fracture completion converts a greenstick fracture into a complete fracture, which is easier to maintain in a neutral, reduced position.
- Greenstick fractures are the most common type of neonatal skull fracture.[50]
- Although greenstick fractures occur predominantly in children, adult cases have also been reported.[51]
These additional considerations highlight the broader clinical spectrum of greenstick fractures. Familiarity with uncommon presentations and alternative treatment approaches helps prevent diagnostic uncertainty and supports appropriate management.
Enhancing Healthcare Team Outcomes
Greenstick fractures are common pediatric long-bone injuries caused by bending forces that produce an incomplete cortical break with partial structural continuity. Optimal outcomes require coordinated involvement of emergency medicine, primary care, orthopedic surgery, outpatient clinicians, and caregivers.
Physicians and advanced practitioners evaluate for manifestations, such as deformity, swelling, distal perfusion, and neurologic function, and identify the fracture mechanism. The assessment also determines reduction thresholds, guides selection of an immobilization strategy, and ensures appropriate follow-up. Orthopedic surgery consultation is important for defining acceptable alignment, performing or guiding reduction when indicated, and establishing follow-up intervals. Outpatient orthopedic management is essential because these fractures can lose alignment after initial treatment. Follow-up visits should cover repeat clinical assessment, the use of interval radiographs when indicated, evaluation of cast fit and pressure-related complications, reassessment of pain and function, and guidance regarding activity restrictions, return to school or sports, and expected healing timelines.
Nurses perform frequent neurovascular assessments, provide cast and splint care education, reinforce return precautions, and recognize early warning signs that require immediate reassessment. Nursing communication is especially important during transitions from emergency care to outpatient orthopedic follow-up to ensure families understand when and where reassessment should occur.[52] Pharmacists optimize pain control and counsel caregivers on safe opioid and nonopioid medication use.[53] Other health professionals, including radiology technicians, cast technicians, social workers, physical and occupational therapists, and child protection teams, contribute to imaging quality, immobilization safety, and functional recovery.
Ethical responsibilities of the interprofessional team include trauma-informed communication, informed consent for reduction and sedation, and vigilance when the history or findings raise concern for nonaccidental trauma. Coordination with social work, pediatrics or child protection teams, and radiology is essential when nonaccidental trauma is suspected.
Media
(Click Image to Enlarge)

Greenstick Fracture of the Ulna. This anteroposterior x-ray of the forearm demonstrates an incomplete greenstick fracture along the midshaft of the ulna. The adjacent radius appears intact.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
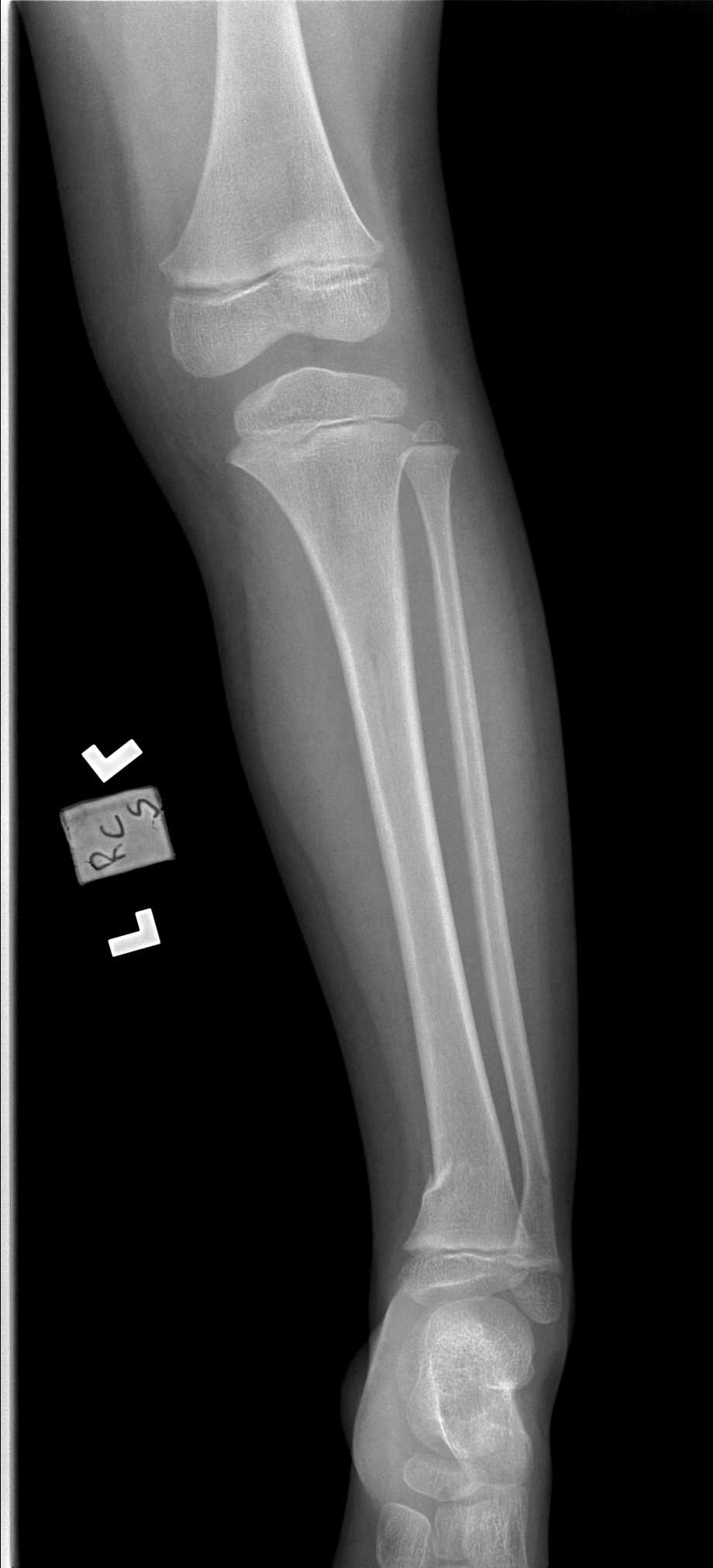
Distal Tibia and Fibula Greenstick Fracture. This anteroposterior radiograph of the lower leg demonstrates a greenstick fracture affecting the distal shafts of the tibia and fibula. The alignment shows characteristic cortical buckling without complete displacement.
Contributed by S Dulebohn, MD
References
Ağırdil Y. The growth plate: a physiologic overview. EFORT open reviews. 2020 Aug:5(8):498-507. doi: 10.1302/2058-5241.5.190088. Epub 2020 Sep 10 [PubMed PMID: 32953135]
Level 3 (low-level) evidenceAsokan A, Kheir N. Pediatric Torus Buckle Fracture. StatPearls. 2026 Jan:(): [PubMed PMID: 32809469]
Szabo E, Rimnac C. Biomechanics of immature human cortical bone: A systematic review. Journal of the mechanical behavior of biomedical materials. 2022 Jan:125():104889. doi: 10.1016/j.jmbbm.2021.104889. Epub 2021 Oct 8 [PubMed PMID: 34736022]
Level 1 (high-level) evidenceLindaman LM. Bone healing in children. Clinics in podiatric medicine and surgery. 2001 Jan:18(1):97-108 [PubMed PMID: 11344982]
Caruso G, Caldari E, Sturla FD, Caldaria A, Re DL, Pagetti P, Palummieri F, Massari L. Management of pediatric forearm fractures: what is the best therapeutic choice? A narrative review of the literature. Musculoskeletal surgery. 2021 Dec:105(3):225-234. doi: 10.1007/s12306-020-00684-6. Epub 2020 Oct 14 [PubMed PMID: 33058085]
Level 3 (low-level) evidenceKorup LR, Larsen P, Nanthan KR, Arildsen M, Warming N, Sørensen S, Rahbek O, Elsoe R. Children's distal forearm fractures: a population-based epidemiology study of 4,316 fractures. Bone & joint open. 2022 Jun:3(6):448-454. doi: 10.1302/2633-1462.36.BJO-2022-0040.R1. Epub [PubMed PMID: 35658607]
Kemp AM, Dunstan F, Harrison S, Morris S, Mann M, Rolfe K, Datta S, Thomas DP, Sibert JR, Maguire S. Patterns of skeletal fractures in child abuse: systematic review. BMJ (Clinical research ed.). 2008 Oct 2:337():a1518. doi: 10.1136/bmj.a1518. Epub 2008 Oct 2 [PubMed PMID: 18832412]
Level 1 (high-level) evidenceYang G, Lee WYW, Hung ALH, Tang MF, Li X, Kong APS, Leung TF, Yung PSH, To KKW, Cheng JCY, Lam TP. Association of serum 25(OH)Vit-D levels with risk of pediatric fractures: a systematic review and meta-analysis. Osteoporosis international : a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. 2021 Jul:32(7):1287-1300. doi: 10.1007/s00198-020-05814-1. Epub 2021 Mar 11 [PubMed PMID: 33704541]
Level 1 (high-level) evidenceWako M, Hagino T, Hagino T, Ichikawa J, Haro H. Correlation between fracture pattern and chronological age and skeletal maturity in distal radial fractures in children. Journal of orthopaedic science : official journal of the Japanese Orthopaedic Association. 2026 Jul:31(4):799-803. doi: 10.1016/j.jos.2026.01.006. Epub 2026 Feb 18 [PubMed PMID: 41708378]
Selvakumaran G, Williams N. Buckled, bent or broken? A guide to paediatric forearm fractures. Australian journal of general practice. 2020 Nov:49(11):740-744. doi: 10.31128/AJGP-10-19-5132. Epub [PubMed PMID: 33123705]
Abbott A, Swertfager K, Bloom S, Jackson NJ, Goldman J. Pediatric Fracture Epidemiology in an Orthopaedic Urgent Care Setting. Journal of the Pediatric Orthopaedic Society of North America. 2025 Aug:12():100216. doi: 10.1016/j.jposna.2025.100216. Epub 2025 May 31 [PubMed PMID: 40704086]
Mamoowala N, Johnson NA, Dias JJ. Trends in paediatric distal radius fractures: an eight-year review from a large UK trauma unit. Annals of the Royal College of Surgeons of England. 2019 Apr:101(4):297-303. doi: 10.1308/rcsann.2019.0023. Epub 2019 Mar 11 [PubMed PMID: 30855170]
Randsborg PH. Fractures in children: aspects on health service, epidemiology and risk factors. Acta orthopaedica. Supplementum. 2013 Apr:84(350):1-24. doi: 10.3109/17453674.2013.789731. Epub [PubMed PMID: 23597144]
Sinikumpu JJ, Nietosvaara Y. Treatment of Distal Forearm Fractures in Children. Scandinavian journal of surgery : SJS : official organ for the Finnish Surgical Society and the Scandinavian Surgical Society. 2021 Jun:110(2):276-280. doi: 10.1177/1457496920983104. Epub 2020 Dec 29 [PubMed PMID: 33372581]
Randsborg PH, Sivertsen EA. Distal radius fractures in children: substantial difference in stability between buckle and greenstick fractures. Acta orthopaedica. 2009 Oct:80(5):585-9. doi: 10.3109/17453670903316850. Epub [PubMed PMID: 19916694]
Level 2 (mid-level) evidencePatel J, Mangal RK, Stead TS, Wanchu R, Ganti L. Greenstick Fractures of the mid- Radial and Ulnar Diaphysis with Volar Angulation. Orthopedic reviews. 2022:14(4):57620. doi: 10.52965/001c.57620. Epub 2022 Dec 26 [PubMed PMID: 36589510]
Currey JD, Butler G. The mechanical properties of bone tissue in children. The Journal of bone and joint surgery. American volume. 1975 Sep:57(6):810-4 [PubMed PMID: 1158919]
Malizos KN, Papatheodorou LK. The healing potential of the periosteum molecular aspects. Injury. 2005 Nov:36 Suppl 3():S13-9 [PubMed PMID: 16188544]
Marsell R, Einhorn TA. The biology of fracture healing. Injury. 2011 Jun:42(6):551-5. doi: 10.1016/j.injury.2011.03.031. Epub 2011 Apr 13 [PubMed PMID: 21489527]
Claes LE, Heigele CA, Neidlinger-Wilke C, Kaspar D, Seidl W, Margevicius KJ, Augat P. Effects of mechanical factors on the fracture healing process. Clinical orthopaedics and related research. 1998 Oct:(355 Suppl):S132-47 [PubMed PMID: 9917634]
Level 3 (low-level) evidenceWebster AP, Goodacre S, Walker D, Burke D. How do clinical features help identify paediatric patients with fractures following blunt wrist trauma? Emergency medicine journal : EMJ. 2006 May:23(5):354-7 [PubMed PMID: 16627835]
Arora R, Fichadia U, Hartwig E, Kannikeswaran N. Pediatric upper-extremity fractures. Pediatric annals. 2014 May:43(5):196-204. doi: 10.3928/00904481-20140417-12. Epub [PubMed PMID: 24877490]
Kyriakides J, Peeters W, Ahluwalia AK, Elvey M. Paediatric forearm fractures: assessment and initial management. British journal of hospital medicine (London, England : 2005). 2022 Sep 2:83(9):1-9. doi: 10.12968/hmed.2021.0564. Epub 2022 Sep 22 [PubMed PMID: 36193916]
Expert Panel on Musculoskeletal Imaging:, Torabi M, Lenchik L, Beaman FD, Wessell DE, Bussell JK, Cassidy RC, Czuczman GJ, Demertzis JL, Khurana B, Klitzke A, Motamedi K, Pierce JL, Sharma A, Walker EA, Kransdorf MJ. ACR Appropriateness Criteria(®) Acute Hand and Wrist Trauma. Journal of the American College of Radiology : JACR. 2019 May:16(5S):S7-S17. doi: 10.1016/j.jacr.2019.02.029. Epub [PubMed PMID: 31054760]
British Orthopaedic Association Trauma Committee. British Orthopaedic Association Standard for Trauma (BOAST): Early Management of Paediatric Forearm Fracture. Injury. 2021 Aug:52(8):2052. doi: 10.1016/j.injury.2021.07.043. Epub [PubMed PMID: 34416974]
Colaris JW, Allema JH, Reijman M, Biter LU, de Vries MR, van de Ven CP, Bloem RM, Verhaar JA. Risk factors for the displacement of fractures of both bones of the forearm in children. The bone & joint journal. 2013 May:95-B(5):689-93. doi: 10.1302/0301-620X.95B5.31214. Epub [PubMed PMID: 23632683]
Liu DS, Bauer AS. Upper Extremity Cast Application. Journal of the Pediatric Orthopaedic Society of North America. 2025 Aug:12():100240. doi: 10.1016/j.jposna.2025.100240. Epub 2025 Jul 3 [PubMed PMID: 40799459]
Singh S, Bhatia M, Housden P. Cast and padding indices used for clinical decision making in forearm fractures in children. Acta orthopaedica. 2008 Jun:79(3):386-9. doi: 10.1080/17453670710015292. Epub [PubMed PMID: 18622843]
Noonan KJ, Price CT. Forearm and distal radius fractures in children. The Journal of the American Academy of Orthopaedic Surgeons. 1998 May-Jun:6(3):146-56 [PubMed PMID: 9689186]
Handoll HH, Elliott J, Iheozor-Ejiofor Z, Hunter J, Karantana A. Interventions for treating wrist fractures in children. The Cochrane database of systematic reviews. 2018 Dec 19:12(12):CD012470. doi: 10.1002/14651858.CD012470.pub2. Epub 2018 Dec 19 [PubMed PMID: 30566764]
Level 1 (high-level) evidenceChasm RM, Swencki SA. Pediatric orthopedic emergencies. Emergency medicine clinics of North America. 2010 Nov:28(4):907-26. doi: 10.1016/j.emc.2010.06.003. Epub [PubMed PMID: 20971397]
Zimmermann R, Gschwentner M, Kralinger F, Arora R, Gabl M, Pechlaner S. Long-term results following pediatric distal forearm fractures. Archives of orthopaedic and trauma surgery. 2004 Apr:124(3):179-86 [PubMed PMID: 14986025]
Roth KC, Musters L, Diederix LW, Edomskis P, van Bergen CJA, Eygendaal D, Colaris JW. Secondary Displacement of Forearm Fractures in Children: When to Anticipate Remodeling and When to Intervene? Children (Basel, Switzerland). 2026 Jan 9:13(1):. doi: 10.3390/children13010098. Epub 2026 Jan 9 [PubMed PMID: 41597106]
Tahririan MA, Soltani Farsani A, Najafi MM, Mirghaderi P. Redisplacement after Closed Reduction in Pediatric Both-Bone Forearm Fractures: The Role of Initial Fracture Angulation and Cast Index. Advanced biomedical research. 2025:14():145. doi: 10.4103/abr.abr_277_25. Epub 2025 Nov 28 [PubMed PMID: 41640661]
Li TP, Wollstein A, Sabharwal S, Nayar SK, Sabharwal S. Malunion of Pediatric Forearm Shaft Fractures: Management Principles and Techniques. Current reviews in musculoskeletal medicine. 2022 Dec:15(6):427-437. doi: 10.1007/s12178-022-09783-2. Epub 2022 Jul 25 [PubMed PMID: 35876970]
Tisosky AJ, Werger MM, McPartland TG, Bowe JA. The Factors Influencing the Refracture of Pediatric Forearms. Journal of pediatric orthopedics. 2015 Oct-Nov:35(7):677-81. doi: 10.1097/BPO.0000000000000355. Epub [PubMed PMID: 25436481]
Bhanushali A, Axelby E, Patel P, Abu-Assi R, Ong B, Graff C, Kraus M. Re-fractures of the paediatric radius and/or ulna: A systematic review. ANZ journal of surgery. 2022 Apr:92(4):666-673. doi: 10.1111/ans.17191. Epub 2021 Sep 22 [PubMed PMID: 34553474]
Level 1 (high-level) evidenceMcGraw-Heinrich JA, Wall JC, Rosenfeld SB. Common Cast Complications. Journal of the Pediatric Orthopaedic Society of North America. 2025 Aug:12():100244. doi: 10.1016/j.jposna.2025.100244. Epub 2025 Jul 3 [PubMed PMID: 40791972]
Gresh M. Compartment Syndrome in the Pediatric Patient. Pediatrics in review. 2017 Dec:38(12):560-565. doi: 10.1542/pir.2016-0114. Epub [PubMed PMID: 29196511]
Kell DM, Chang B, Shah AS, Williams BA. Distal Radioulnar Synostosis Following Greenstick Fracture of the Ulnar Diaphysis: A Case Report. JBJS case connector. 2024 Oct 1:14(4):. doi: 10.2106/JBJS.CC.24.00299. Epub 2024 Oct 31 [PubMed PMID: 39480957]
Level 3 (low-level) evidenceHepping AM, Barvelink B, Ploegmakers JJW, van der Palen J, Geertzen JHB, Bulstra SK, Harbers JS, Stevens M. Functional recovery after reduced pediatric fractures of the forearm with respect to perceived limitations, common post-traumatic symptoms, range of motion, and dexterity: a prospective study. Disability and rehabilitation. 2023 Oct:45(21):3560-3566. doi: 10.1080/09638288.2022.2131006. Epub 2022 Oct 10 [PubMed PMID: 36214289]
Hepping AM, Barvelink B, Ploegmakers JJW, van der Palen J, Geertzen JHB, Bulstra SK, Harbers JS, Stevens M. Recovery of strength after reduced pediatric fractures of the forearm, wrist or hand; A prospective study. PloS one. 2020:15(4):e0230862. doi: 10.1371/journal.pone.0230862. Epub 2020 Apr 1 [PubMed PMID: 32236117]
Bhanushali A, Bright R, Xu L, Cundy P, Williams N. Return to sport after forearm fractures in children: A scoping review and survey. Journal of children's orthopaedics. 2023 Apr:17(2):164-172. doi: 10.1177/18632521231156434. Epub 2023 Mar 10 [PubMed PMID: 37034195]
Level 2 (mid-level) evidenceFlaherty EG, Perez-Rossello JM, Levine MA, Hennrikus WL, American Academy of Pediatrics Committee on Child Abuse and Neglect, Section on Radiology, American Academy of Pediatrics, Section on Endocrinology, American Academy of Pediatrics, Section on Orthopaedics, American Academy of Pediatrics, Society for Pediatric Radiology. Evaluating children with fractures for child physical abuse. Pediatrics. 2014 Feb:133(2):e477-89. doi: 10.1542/peds.2013-3793. Epub 2014 Jan 27 [PubMed PMID: 24470642]
Sherker S, Ozanne-Smith J, Rechnitzer G, Grzebieta R. Out on a limb: risk factors for arm fracture in playground equipment falls. Injury prevention : journal of the International Society for Child and Adolescent Injury Prevention. 2005 Apr:11(2):120-4 [PubMed PMID: 15805443]
Mott A, Rolfe K, James R, Evans R, Kemp A, Dunstan F, Kemp K, Sibert J. Safety of surfaces and equipment for children in playgrounds. Lancet (London, England). 1997 Jun 28:349(9069):1874-6 [PubMed PMID: 9217759]
Black GB, Amadeo R. Orthopedic injuries associated with backyard trampoline use in children. Canadian journal of surgery. Journal canadien de chirurgie. 2003 Jun:46(3):199-201 [PubMed PMID: 12812242]
Chong AL, Sunner PS, Deshpande SR. Wrist guards in in-line and conventional roller-skating injuries. The Medical journal of Australia. 1995 Apr 17:162(8):444 [PubMed PMID: 7746189]
Nguyen S, McDowell M, Schlechter J. Casting: Pearls and pitfalls learned while caring for children's fractures. World journal of orthopedics. 2016 Sep 18:7(9):539-45. doi: 10.5312/wjo.v7.i9.539. Epub 2016 Sep 18 [PubMed PMID: 27672566]
Cho SM, Kim HG, Yoon SH, Chang KH, Park MS, Park YH, Choi MS. Reappraisal of Neonatal Greenstick Skull Fractures Caused by Birth Injuries: Comparison of 3-Dimensional Reconstructed Computed Tomography and Simple Skull Radiographs. World neurosurgery. 2018 Jan:109():e305-e312. doi: 10.1016/j.wneu.2017.09.168. Epub 2017 Oct 5 [PubMed PMID: 28989045]
Casey PJ, Moed BR. Greenstick fractures of the radius in adults: a report of two cases. Journal of orthopaedic trauma. 1996:10(3):209-12 [PubMed PMID: 8667114]
Level 3 (low-level) evidencePeterson K, Laboy C. Pediatric fractures: A nursing perspective. Nursing. 2026 Jan 1:56(1):15-22. doi: 10.1097/NSG.0000000000000315. Epub 2025 Dec 22 [PubMed PMID: 41437463]
Level 3 (low-level) evidenceDrendel AL, Gorelick MH, Weisman SJ, Lyon R, Brousseau DC, Kim MK. A randomized clinical trial of ibuprofen versus acetaminophen with codeine for acute pediatric arm fracture pain. Annals of emergency medicine. 2009 Oct:54(4):553-60. doi: 10.1016/j.annemergmed.2009.06.005. Epub 2009 Aug 19 [PubMed PMID: 19692147]
Level 1 (high-level) evidence