Introduction
The Gordon reflex is a pathologic plantar reflex used to assess the integrity of the corticospinal tract and identify upper motor neuron lesions. Clinicians elicit this reflex by firmly compressing the calf muscles while observing for dorsiflexion of the great toe, with or without fanning of the other toes. This extensor plantar response indicates dysfunction of descending motor pathways and is considered abnormal in adults. The Gordon reflex is one of several Babinski-equivalent reflexes (eg, Chaddock and Oppenheim) and serves as a useful adjunct to the neurologic examination, particularly when traditional plantar stimulation is contraindicated, poorly tolerated, or produces equivocal findings.[1][2] See StatPearls companion topics, "Chaddock Reflex" and "Neuroanatomy, Upper Motor Neuron Signs," for additional discussion on the Chaddock and Oppenheim reflexes.
Assessment of the Gordon reflex requires no specialized equipment and can be performed quickly at the bedside, making it a practical tool in a variety of clinical settings, including outpatient clinics, emergency departments, and inpatient evaluations. Accurate elicitation and interpretation of this reflex can aid in the early detection of neurologic disorders such as stroke, spinal cord injury, multiple sclerosis, brain tumors, and other conditions affecting upper motor neuron pathways. Incorporating the Gordon reflex into routine neurologic examination enhances diagnostic accuracy and supports timely evaluation and management of patients with suspected central nervous system pathology.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The Gordon reflex is elicited by squeezing the calf muscle. The calf comprises the gastrocnemius and soleus muscles, which come together to form the Achilles tendon. Both muscles aid in the plantarflexion of the foot at the ankle. The typical plantar response reflex involves all muscles that shorten the leg, including the gastrocnemius and soleus.[3]
A segmental reflex involving all the leg and foot flexor muscles results in the toes flexing during the plantar reflex.[3][4] When there is a lesion in the pyramidal system, the segmental downward response disappears, and the flexion synergy may become disinhibited to the point where the extensor hallucis longus muscle is recruited into the flexion response of the leg.[3][5] This leads to an upgoing toe with the Gordon, Babinski, Chaddock, and Oppenheim reflexes (see Image. Gordon Reflex).[1][6]
Indications
The Gordon reflex is a useful adjunct to the comprehensive neurologic examination, particularly for evaluating suspected pyramidal tract dysfunction. This may be performed alongside the Babinski reflex and is especially valuable when clinicians cannot reliably assess the Babinski test due to patient noncooperation, plantar wounds, or equivocal responses. Because the Babinski reflex can cause discomfort or pain in patients with sensitive soles, leading to withdrawal and unreliable results, the Gordon reflex provides a practical alternative. Calf compression is generally better tolerated and less likely to provoke withdrawal, allowing for more accurate assessment of upper motor neuron involvement.
Contraindications
Contraindications to performing the Gordon reflex include an open wound on the calf or surrounding area, recent or suspected deep vein thrombosis, and markedly swollen or painful calves, which may occur in conditions such as an exacerbation of congestive heart failure. Caution is also warranted in patients with severe thrombocytopenia, as the firm compression required to elicit the reflex may increase the risk of soft tissue injury, bruising, or hematoma.
Equipment
No specialized equipment is required to perform the Gordon reflex. The patient should be comfortable in the supine position with both legs extended, ideally in an environment that allows proper support and relaxation during the examination.
Personnel
Any properly trained healthcare professional can perform the Gordon reflex. Physicians, medical students, physician assistants, nurses, and other trained clinical staff can conduct the examination. Individuals with limited experience should first observe an experienced practitioner or review instructional materials demonstrating proper technique before performing the test independently. Continued practice and experience improve proficiency and increase the accuracy of eliciting and interpreting the reflex.
Preparation
Minimal preparation is required to perform the Gordon reflex. Position the patient supine on an examination table with both legs extended and relaxed.[3] Ensure the lower extremities are fully exposed from the knee to the foot by having the patient wear a hospital gown without shoes or restrictive clothing. Perform proper hand hygiene before beginning the examination. The practitioner may sit or stand beside the patient in a comfortable position that allows easy access to the calf while clearly observing the toes for the reflex response.
Technique or Treatment
The clinician places a hand beneath the patient’s calf to support the leg and uses the other hand to support the ankle. They firmly squeeze the calf muscle while observing the toes on the same side. A positive (abnormal) Gordon reflex occurs when the great toe extends upward, often accompanied by fanning of the other toes, indicating an extensor plantar response.[3] A negative (normal) reflex does not move the toes during calf compression. Repeat the test as needed to confirm the response. Additional supporting tests are the Babinski, Chaddock, or Oppenheim reflexes to support the presence of an extensor plantar response.[2][6]
Complications
Although complications from the Gordon reflex are uncommon, firm compression of the calf muscle may cause temporary discomfort, bruising, or soreness.
Clinical Significance
The Babinski sign itself demonstrates mild to moderate sensitivity but high specificity for upper motor neuron-associated myelopathy. While the Gordon sign indicates the same pathology, its lower interobserver reliability makes it less suitable as a primary diagnostic tool. The clinical utility of the Gordon sign lies primarily in its use as a complementary test when the standard Babinski reflex is equivocal or difficult to elicit. The combination of the Babinski and Chaddock reflexes is most reliable in clinical practice, suggesting that Gordon's reflex may be most useful as part of a comprehensive assessment rather than as a standalone test.[3]
All variants, including Gordon, Chaddock, and Oppenheim, work by expanding the reflexogenic zone in patients with upper motor neuron lesions, thereby allowing clinicians to elicit the pathological extensor response from different anatomical locations.[3] When present, the Gordon reflex signifies a lesion somewhere along the corticospinal pathway, from the motor cortex through the subcortex, brainstem, or spinal cord.[7] Like the Babinski sign, it represents disinhibition of the primitive flexion withdrawal reflex due to loss of descending pyramidal tract control over spinal motoneurons.
The presence of the Gordon sign has high specificity. However, low sensitivity for detecting pyramidal tract dysfunction, similar to other extensor plantar responses.[7][8] This means that when present, it strongly suggests upper motor neuron pathology. However, its absence does not exclude the presence of such pathology.
The most likely cause of an abnormal response is degenerative cervical myelopathy, the most common cause of spinal cord dysfunction in adults older than 55. Affected patients present with neck pain and stiffness, gait disturbance, hand clumsiness, and upper motor neuron signs below the level of the lesion. MRI shows cervical cord compression with T2 hyperintensity.[7][9] Additional causes may be ischemic or hemorrhagic stroke, multiple sclerosis, motor neuron disease, cauda equina syndrome, transverse myelitis, acute myelopathy, and acute spinal cord compression.[10][11] Cardinal features of acute spinal cord impression include relatively symmetric paralysis, urinary retention or incontinence, sensory level, and localized back or neck pain.
Enhancing Healthcare Team Outcomes
The Gordon reflex is a pathologic plantar reflex used to help identify upper motor neuron lesions involving the corticospinal tract. Clinicians elicit the reflex by firmly squeezing the patient’s calf muscle while observing the ipsilateral toes for an extensor plantar response, characterized by dorsiflexion of the great toe with or without fanning of the other toes. This finding is similar to the Babinski sign and supports the presence of central nervous system dysfunction. The Gordon reflex is a useful adjunct to the neurologic examination, particularly when Babinski testing is not feasible or yields equivocal results. Proper technique, patient positioning, and awareness of contraindications are essential to ensure accurate assessment and patient safety.
Effective use of the Gordon reflex requires coordinated interprofessional collaboration to optimize diagnostic accuracy and patient outcomes. Physicians and advanced practitioners integrate reflex findings into the overall neurologic assessment and determine the need for further diagnostic evaluation. Nurses assist with patient positioning, monitoring, and early recognition of abnormal neurologic findings. Pharmacists contribute by reviewing medications that may affect neurologic function or contribute to underlying conditions. Clear communication among healthcare team members ensures accurate documentation, timely recognition of neurologic abnormalities, and appropriate referral or intervention. Coordinated care and shared clinical decision-making enhance patient-centered care, improve patient safety, support accurate diagnosis of upper motor neuron pathology, and strengthen overall team performance.
Media
(Click Image to Enlarge)
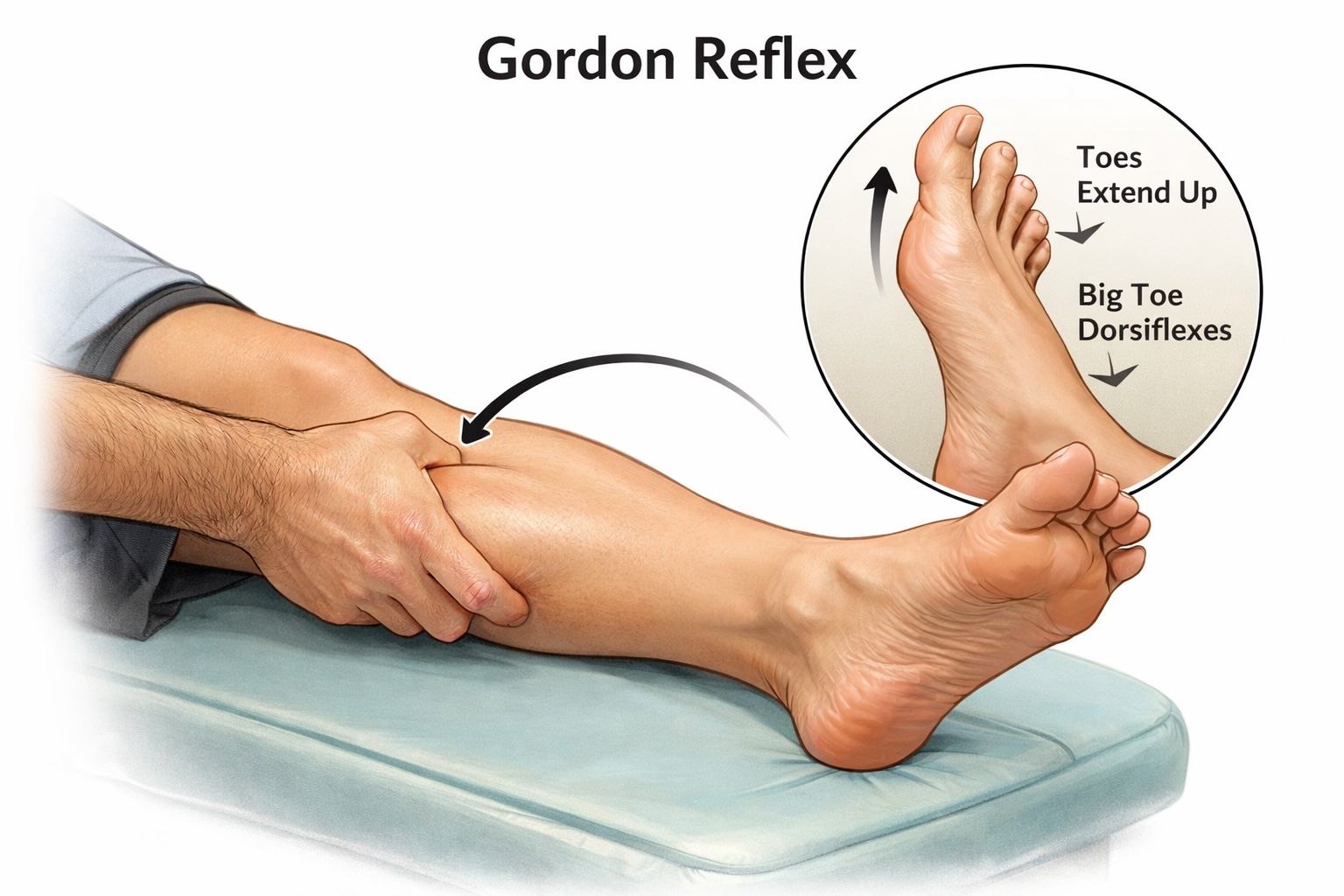
Gordon Reflex. Demonstration of calf muscle compression eliciting an extensor plantar response (dorsiflexion of the great toe, often with fanning of the other toes). This pathologic reflex indicates an upper motor neuron lesion and is considered a Babinski-equivalent sign.
Contributed by Julie Bohlen, MBA-HCM, ELS.
References
Singerman J, Lee L. Consistency of the Babinski reflex and its variants. European journal of neurology. 2008 Sep:15(9):960-4. doi: 10.1111/j.1468-1331.2008.02219.x. Epub 2008 Jul 10 [PubMed PMID: 18637037]
Tashiro K. [Reverse Chaddock sign]. Brain and nerve = Shinkei kenkyu no shinpo. 2011 Aug:63(8):839-50 [PubMed PMID: 21817175]
van Gijn J. The Babinski reflex. Postgraduate medical journal. 1995 Nov:71(841):645-8 [PubMed PMID: 7494766]
Acharya AB, Jamil RT, Dewey JJ. Babinski Reflex. StatPearls. 2026 Jan:(): [PubMed PMID: 30085551]
Lohia A, McKenzie J. Neuroanatomy, Pyramidal Tract Lesions. StatPearls. 2025 Jan:(): [PubMed PMID: 31082020]
Emos MC, Rosner J. Neuroanatomy, Upper Motor Nerve Signs. StatPearls. 2025 Jan:(): [PubMed PMID: 31082126]
Kane SF, Abadie KV, Willson A. Degenerative Cervical Myelopathy: Recognition and Management. American family physician. 2020 Dec 15:102(12):740-750 [PubMed PMID: 33320508]
Isaza Jaramillo SP, Uribe Uribe CS, García Jimenez FA, Cornejo-Ochoa W, Alvarez Restrepo JF, Román GC. Accuracy of the Babinski sign in the identification of pyramidal tract dysfunction. Journal of the neurological sciences. 2014 Aug 15:343(1-2):66-8. doi: 10.1016/j.jns.2014.05.028. Epub 2014 May 21 [PubMed PMID: 24906707]
Theodore N. Degenerative Cervical Spondylosis. The New England journal of medicine. 2020 Jul 9:383(2):159-168. doi: 10.1056/NEJMra2003558. Epub [PubMed PMID: 32640134]
Emos MC, Agarwal S. Neuroanatomy, Upper Motor Neuron Lesion. StatPearls. 2025 Jan:(): [PubMed PMID: 30725990]
Ropper AE, Ropper AH. Acute Spinal Cord Compression. The New England journal of medicine. 2017 Apr 6:376(14):1358-1369. doi: 10.1056/NEJMra1516539. Epub [PubMed PMID: 28379788]