Introduction
Gonorrhea is a sexually transmitted infection (STI) caused by Neisseria gonorrhoeae, a gram-negative diplococcus that primarily targets columnar and transitional epithelium, making the cervix, urethra, rectum, pharynx, and conjunctiva common sites of infection.[1] The natural history of gonorrhea ranges from asymptomatic carriage to symptomatic disease, most commonly characterized by urethritis, cervicitis, or pelvic inflammatory disease (PID). Without treatment, the infection can spread to involve the uterus, fallopian tubes, and ovaries, or it can spread locally to adjacent structures, which can lead to serious sequelae, eg, infertility and ectopic pregnancy. In males, untreated infection can cause epididymitis, prostatitis, and urethral stricture. Hematogenous dissemination occurs in a minority of cases and can lead to arthritis, tenosynovitis, rash, endocarditis, and meningitis. Transmission is highly efficient through sexual contact, and untreated infection significantly increases the risk of partner transmission and coinfection with other STIs.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
N gonorrhoeae is an obligate human pathogen, relying exclusively on the human body for survival, transmission, and reproduction. Gonorrhea only infects humans and most commonly presents as urethritis in men and cervicitis in women.[2] Undiagnosed and untreated gonorrheal urogenital infections can ascend through the upper urogenital tract and cause severe reproductive complications, most commonly but not exclusively in women, eg, endometritis, pelvic inflammatory disease (PID), infertility, and life-threatening morbidity via ectopic pregnancy.[3] In addition, N gonorrhoeae can rarely disseminate, causing septic arthritis, endocarditis, and inflammation of the liver capsule and Fitz-Hugh-Curtis syndrome, which can cause infertility, abdominal adhesions, and chronic abdominal pain in women.[4]
Epidemiology
The World Health Organization (WHO) estimates that 106 million new gonorrhea cases are documented among adults annually worldwide, with many more infections going unreported.[5] Gonorrhea is the second most frequently reported notifiable infection in the United States and the United Kingdom, with more than 1.5 million annual cases in the United States.[6] New cases of gonorrhea are associated with substantial economic and health impacts, resulting in an estimated $323 million in lifetime medical costs and a loss of 386 quality-adjusted life years (QALYs) for females and 12,112 QALYs for males.[7]
Males have higher reported rates of gonorrhea compared to females, with infection rates of approximately 224 cases per 100,000 males compared with 153 cases per 100,000 females. Adolescents and young adults are particularly vulnerable, accounting for over half of all new cases, with 54% of infections occurring in individuals aged 15 to 24.[1][7] Adolescents and young adults are less likely to use condoms, are more likely to have multiple sex partners, and face barriers to accessing STI services, eg, cost.[8][9][10]
Rates of gonorrhea are rising among older adults, who are more likely to report never using condoms, binge drinking, having sex under the influence of alcohol, using cocaine or injection drugs, exchanging sex for money, drugs, or other goods, experiencing sexual assault, and participating in swinging.[11] Additionally, the use of HIV preexposure prophylaxis (PrEP) and birth control has been correlated with a decrease in the use of barrier protection, thus increasing the risk for STI acquisition.[12] Gonorrhea is particularly common in men who have sex with men (MSM).[13] These trends highlight the importance of early recognition, timely diagnosis, and guideline-directed treatment in reducing transmission and preventing complications.[1][7]
STIs disproportionately affect certain populations, including transgender and gender expansive persons, sex workers, and, in the United States and some other countries, people who identify as Black or African American.[14][15][16] Many members of these groups experience social marginalization, and the stigma surrounding STIs can further limit their interaction with healthcare services, reduce public advocacy, and result in inadequate attention from policymakers. These factors contribute to missed opportunities and chronic underfunding for STI prevention, testing, and treatment initiatives.[7] In addition, disparities in the social determinants of health play an important role.[17] Biological differences do not explain why STIs are more prevalent in African Americans compared to Whites in the United States.[18][19]
Pathophysiology
Gonorrhea infection starts with the adhesion of gonococci to epithelial cells, followed by local cellular invasion. N gonorrhoeae has multiple surface proteins that facilitate adhesion. Hair-like appendages, called pili, cover the bacterial surface. N gonorrhoeae utilizes these pili to initiate adhesion to epithelial cells. Their ability to lengthen and retract the pilli allows the bacteria to attach from a distance and move closer to the epithelial cells, promoting cellular invasion. Pili also provide motility and protection.[20] Other surface proteins involved in cellular attachment include opacity-associated proteins (Opa) and lipooligosaccharide. Lipooligosaccharide attaches to sperm cells and likely leads to transmission from males to uninfected sexual partners.[21]
Invasion of cervical epithelium involves bacterial cells interacting with host cell complement receptors type 3 (CR3). This communication is initiated by the binding of pili to CR3.[22] This causes extensive rearrangement of the host cell actin, resulting in large projections called ruffles.[23] Ruffling then allows gonococci to enter host cells in large vacuoles called macropinosomes, and subsequently multiply within infected cells.[24]
N gonorrhoeae induces localized infections at the anatomic site of inoculation, typically the columnar epithelium of the urethra, endocervix, pharynx, or anus in adults, and the eye conjunctiva or pharynx in newborns. However, dissemination can occur.[5] Gonococci are classified as either serum-sensitive or serum-resistant based on their susceptibility to complement-mediated killing; serum-resistant strains have the potential to cause disseminated infection.[25] N gonorrhoeae has evolved multiple mechanisms to evade the innate and adaptive immune defenses of its host organisms.[2]
The mechanisms by which N gonorrhoeae initiates infection differ between males and females. In males, N gonorrhoeae interacts with urethral epithelial cells, triggering the release of pro-inflammatory cytokines and prompting an inflammatory response. Conversely, in the female reproductive tract, N gonorrhoeae is better able to evade the host immune response and does not elicit a strong immune response during uncomplicated genital infections. If N gonorrhoeae ascends the urogenital tract into the uterus and fallopian tubes, inflammation typically results.[26] Thus, uncomplicated urogenital infections tend to be more commonly symptomatic in males compared to females, which in part likely explains why males are more commonly diagnosed with gonorrhea compared to females.
Histopathology
Light microscopy of gram-negative or methylene blue-stained smears of N gonorrhoeae urethral or cervical mucus samples will demonstrate neutrophils with intracellular diplococci. Light microscopy has high sensitivity and specificity for symptomatic males with urethral discharge, although it has a lower sensitivity for diagnosing cervical, pharyngeal, and rectal gonorrhea.[2] A Gram stain of a urethral specimen that demonstrates polymorphonuclear leukocytes and intracellular gram-negative diplococci is considered diagnostic of gonorrhea infection in males (see Images. Gonorrhea Gram Stain and N Gonorrhoeae).
History and Physical
Healthcare practitioners should take sexual histories in a nonjudgmental, trauma-informed manner to accurately assess STI risk while building patient trust. The Centers for Disease Control and Prevention (CDC) recommends using the following 5 “P’s” approach:
- Partners: number, newness, and risk factors
- Practices: types of sexual activity and associated behaviors
- Protection: methods used, including PrEP and vaccines
- Past history: previous STIs or HIV
- Pregnancy: reproductive intentions and contraception
Clinicians should also consider the patient’s gender identity, sexual orientation, and cultural or socioeconomic context, as these factors influence access to care and risk assessment.[1]
Clinical Features in Females
Gonorrhea can present in a range of ways, and up to 90% of individuals who are assigned female at birth with gonorrhea cervicitis have no symptoms.[27] Therefore, relying solely on symptoms will miss the majority of gonorrhea infections.[12] When symptoms do occur, they usually appear within 2 to 10 days after exposure and often correspond to the site of infection. Individuals assigned female at birth commonly develop cervicitis, which may manifest as purulent vaginal discharge, dysuria, pelvic discomfort, or bleeding between menstrual periods. Pain usually only occurs when the infection progresses to the upper genital tract and results in PID, which happens in 10% to 20% of cases. Approximately 40% of PID cases overall are caused by gonorrhea.[12]
In endocervical gonococcal infection, roughly half of patients notice a change or increase in vaginal discharge. About 1 in 4 report lower abdominal discomfort, and pelvic or abdominal tenderness on exam is concerning for PID. Intermenstrual spotting or heavy bleeding is unusual. On pelvic exam, clinicians may observe mucopurulent discharge from the cervix and bleeding that is readily provoked.[28] Gonorrheal infection of the Bartholin’s glands adjacent to the vaginal introitus manifests as labial soft tissue swelling, abscess formation, and pain.[29]
If cervicitis goes undetected and untreated, ascending gonococcal infection can result in upper reproductive tract involvement, eg, salpingitis and PID. PID can lead to infertility and an increased risk of ectopic pregnancy.[6][30] Disseminated infection may result in severe sepsis, morbidity, and death. Gonococcal infections complicating pregnancy can lead to adverse pregnancy outcomes, eg, low birth weight newborns and transmission to newborns, resulting in oropharyngeal or conjunctival infections.[30] The CDC recommends universal prophylaxis with erythromycin eye ointment for newborns because gonococcal conjunctivitis affects about 0.3 per 1000 live births.[1]
Clinical Features in Males
Between 56% and 87% of individuals who are assigned male at birth have asymptomatic gonorrhea infection.[27] Symptoms include urethral discharge or painful urination and typically occur within 2 to 14 days following exposure. The exam can reveal a mucopurulent urethral discharge that is thick and white, yellow, or green. Discharge is typically more frequent and voluminous than from Chlamydia trachomatis infection.
Less commonly, individuals may report testicular or epididymal discomfort, and the exam may show associated unilateral testicular pain and swelling concerning for epididymitis.[28][12] Male urogenital gonococcal complications include orchitis, epididymitis, penile lymphangitis, penile edema, and postinfectious urethral strictures. The prevalence of rectal and pharyngeal gonococcal infections has been increasing in the MSM population.[31]
Disseminated Gonococcal Infection
As with cervicitis, gonococcal infection of the pharynx, rectum, and female urethra often presents asymptomatically or with subtle symptoms. If left untreated, gonorrheal infection of the rectum can manifest with rectal pain, bleeding, discharge, and proctitis.[6] Disseminated gonococcal infection occurs in 0.5% to 3% of gonorrhea cases, manifesting with fever, septicemia, dermatitis, tenosynovitis, arthritis, polyarthralgia, and vasculitis.[30][32] In disseminated gonococcal infection, arthritis most often involves 1 joint but can affect several, with the knee being the most frequent site.
Wrist, ankle, and elbow involvement occurs less often, and tenosynovitis or skin lesions are uncommon. Notably, about half of confirmed cases have negative mucosal gonorrhea tests.[28] Gonorrhea may also cause severe conjunctivitis in adults and adolescents, which may be passed through nonsexual contact. Rarely, N gonorrhoeae can cause endocarditis and meningitis. Endocarditis occurs in 1% to 2% of cases of disseminated gonococcal infection, and meningitis even less commonly.[32]
Evaluation
Diagnostic laboratory assays are essential to confirm the clinical suspicion of gonorrhea. Gonorrhea is diagnosed by identifying N gonorrhoeae at the site of infection, most commonly using microscopy, culture, or nucleic acid amplification.
Screening Recommendations
Clinicians should screen sexually active females younger than 25 years annually, and females 25 years and older who have an increased risk for STIs, with repeat testing recommended 3 months after treatment. Higher-risk patients include those with new or multiple sexual partners, partners who have other partners, inconsistent condom use outside monogamy, engagement in transactional sex, or a history of incarceration. The American College of Gynecology (ACOG) recommends screening pregnant patients aged 24 and younger and those with elevated risk, though many clinicians perform universal screening at the first prenatal visit. Evidence shows that universal screening reduces the risk of PID compared with no screening, highlighting the importance of routine and timely STI testing in improving reproductive health outcomes.[1]
Microscopy
A Gram stain of a urethral specimen that demonstrates polymorphonuclear leukocytes and intracellular gram-negative diplococci is highly specific for N gonorrhoeae and is considered diagnostic of gonorrhea infection in males, with a specificity of around 99%.[30] The sensitivity varies depending on whether symptoms are present and on the site. In symptomatic males, the sensitivity of the urethral swab is around 95%, but it falls to 80% or even lower in asymptomatic males.[33] The sensitivity is even lower, at 40% to 60%, for endocervical swabs.[30] The sensitivity from pharyngeal and rectal swabs is even lower due to the presence of nonpathogenic diplococci, so Gram stain of specimens from these sites is not recommended.
Nucleic Acid Amplification Testing
Nucleic acid amplification testing (NAAT) is the optimal method for diagnosing gonorrhea, particularly from extragenital sites. It can also be used to diagnose coinfections from other pathogens, eg, C trachomatis. For oropharyngeal and rectal infections specifically, NAATs are more sensitive than culture and are highly sensitive (over 95%) in symptomatic and asymptomatic infections. Both self-collected and clinician-collected vulvovaginal swabs yield higher diagnostic accuracy than endocervical swabs and outperform urine testing. For this reason, vulvovaginal swabs are considered the preferred specimen. When disseminated gonococcal infection is a concern, samples from affected sites, eg, synovial fluid, should be collected for both culture and NAAT, and blood cultures should be obtained in all suspected cases. Culture becomes important for antimicrobial susceptibility testing.[28]
Any site potentially exposed to N gonorrhoeae should be tested, so performing a thorough, nonjudgmental sexual history before any STI testing is crucial. For example, individuals who engage in anogenital sex and insertive oral sex should have screening for gonorrhea from the anus and pharynx, in addition to urogenital screening.[31] The routine use of NAATs to screen at-risk asymptomatic patients has shown that pharyngeal and rectal gonococcal infections are not uncommon.[34] NAATs are generally more than 95% sensitive and specific in urethral and cervical swabs and first catch urine of males.[34] Before treatment, anyone diagnosed with urogenital gonorrhea who has engaged in insertive oral sex should have pharyngeal testing performed, since oropharyngeal infection is harder to treat and requires a test-of-cure, unlike uncomplicated urogenital infections.[28]
Testing within 2 weeks of exposure may miss infection, so contacts who are not empirically treated should return for repeat testing after the window period.[28] Repeat laboratory screening after patient and partner treatment for gonococcal infection enhances eradication efforts.[35] Recently, the development of multiplex NAATs has enabled screening of an extensive panel of STIs, in addition to N gonorrhoeae.[30] A complete STI screen should be done in anyone with gonorrhea, since over 20% of patients with gonorrhea will be found to also have chlamydia.[28]
Culture
With the widespread availability of NAAT testing, the most important advantage of culture is its ability to assess antimicrobial susceptibilities. The sensitivity of culture is around 85% to 95% with a specificity of around 100% for symptomatic urethral infections, but the sensitivity falls to 50% to 70% for asymptomatic or chronic infections.[36][30] The sensitivity is even lower for pharyngeal or rectal specimens. Cultures are plated on Thayer-Martin agar, which prevents overgrowth by other flora. The CDC recommends that, in the United States, a gonococcal culture be obtained when treatment failure is suspected or when disseminated gonococcal infection is present.[36]
Point-of-Care Testing
The development of commercially available point-of-care assays for N gonorrhoeae infection has reduced time to results and treatment, with results available within 30 to 90 minutes. Sensitivities range from 97% to 100%, with a specificity of approximately 100%.[37]
Treatment / Management
N gonorrhoeae is highly resistant to penicillin and ciprofloxacin, and resistance to azithromycin is growing. Ceftriaxone has been the sole reliable option for initial treatment of gonorrhea. However, in December of 2025, gepotidacin (an oral pill) and zoliflodacin (granules that dissolve in water) were approved by the Federal Drug Administration (FDA) to treat uncomplicated gonorrhea. These are the first new antibiotics approved for the treatment of gonorrhea in over 30 years. Given the ongoing emergence of antimicrobial resistance, staying informed about local resistance patterns and national guidelines for treating gonorrhea is essential.[12] The following treatment recommendations are per the CDC unless otherwise noted.[38]
Uncomplicated Gonococcal Infection of the Cervix, Urethra, and Rectum
Uncomplicated gonorrhea of the urogenital tract or rectum in adolescents and adults should be treated with ceftriaxone 500 mg intramuscularly in a single dose for persons weighing less than 150 kg. For individuals weighing 150 kg or more, ceftriaxone 1 g should be administered intramuscularly. If chlamydial infection has not been excluded, empirical treatment of chlamydia infection with doxycycline 100 mg orally 2 times a day for 7 days is recommended, unless the individual is pregnant, in which case azithromycin 1 g orally in a single dose should be used. If a severe cephalosporin allergy exists, a single dose of gentamicin 240 mg intramuscularly plus azithromycin 2 g orally may be used. Cefixime 800 mg once orally may be used only if ceftriaxone is unavailable or not feasible. For children weighing less than 45 kg, ceftriaxone 25 to 50 mg/kg as a single intravenous or intramuscular dose is recommended, with a maximum intramuscular dose of 250 mg. For children weighing over 45 kg, the dosage is the same as for adolescents and adults. For uncomplicated urogenital or rectal gonorrhea, repeat testing is not needed when recommended or alternative treatments are used.
As of October 2025, for uncomplicated anogenital and pharyngeal gonorrhea in adults, the British Association for Sexual Health and HIV and the United Kingdom National Guidelines recommend 1 gram of ceftriaxone administered intramuscularly. Cefixime dosing has been updated in response to rising antimicrobial resistance, changing from a single 400 mg dose to 2 doses of 400 mg taken 6 to 12 hours apart. For anogenital infections susceptible to ceftriaxone, a routine test of cure is not necessary following treatment with a 1 g dose. Alternative treatment may be given because of an allergy, severe needle phobia, or other contraindications. In people with penicillin allergy, third-generation cephalosporins, eg, ceftriaxone, have minimal to no cross-activity and may be used, except in people with a history of anaphylaxis to penicillin. Spectinomycin is no longer available in the United Kingdom.[28]
In Canada, a single dose of oral cefixime 800 mg, paired with a single dose of azithromycin 1 g, is recommended for urogenital infections.[5] Of note, 1 g of oral azithromycin and 800 mg of oral cefixime have notable gastrointestinal adverse effects, eg, vomiting.[5] Cefixime does not achieve as high or as sustained bactericidal blood levels as ceftriaxone; therefore, it demonstrates limited efficacy for treating pharyngeal gonorrhea.
In persons with a documented life-threatening allergy to cephalosporins or β-lactam allergy, aztreonam monotherapy can be utilized to treat N gonorrhoeae infections. Aztreonam 1 g administered intravenously treats urogenital gonorrhea and may also have efficacy for pharyngeal and rectal gonococcal infection when using a 2 g dose.[39]
Uncomplicated Gonococcal Infection of the Pharynx
Uncomplicated gonorrhea of the pharynx in adolescents and adults should be treated with ceftriaxone 500 mg intramuscularly in a single dose for persons weighing less than 150 kg. For individuals weighing 150 kg or more, ceftriaxone 1 g should be administered intramuscularly. If chlamydial infection has not been excluded, empirical treatment of chlamydia infection with doxycycline 100 mg orally twice daily for 7 days, unless the individual is pregnant, in which case azithromycin 1 g orally in a single dose should be used. No other reliable treatment options for pharyngeal infection have been identified. Individuals with pharyngeal gonorrhea should have a test of cure 7 to 14 days after treatment.[12]
Gonococcal Conjunctivitis
Gonococcal conjunctivitis in adolescents and adults should be treated with a single intramuscular dose of ceftriaxone 1 g. A 1-time lavage of the infected eye with saline solution should be considered. Neonates up to 4 weeks should be given ceftriaxone 25 to 50 mg/kg intravenously or intramuscularly in a single dose. The dose shouldn't exceed 250 mg. Alternatively, cefotaxime 100 mg/kg as a single intravenous or intramuscular dose can be given. To prevent gonococcal conjunctivitis, erythromycin 0.5% ophthalmic ointment is routinely placed in each eye in a single application at birth.
Complicated Gonococcal infection
For complicated gonococcal infections, including PID, epididymitis, and proctitis, dual therapy with a single intramuscular or intravenous dose of 500 mg of ceftriaxone is paired with oral doxycycline 100 mg twice daily for 7 days, rather than a single 1 g dose of azithromycin, because of doxycycline’s effectiveness against C trachomatis and documented efficacy in treating epididymitis and proctitis.[3] Directly observed therapy, endorsed by the WHO, for gonococcal therapy promotes adherence and limits treatment failures secondary to noncompliance.[40]
Disseminated Gonococcal Infection
Disseminated gonococcal infection in adolescents and adults with arthritis and arthritis-dermatitis syndrome should be treated with ceftriaxone 1 g intramuscularly or intravenously every 24 hours. Alternatively, cefotaxime 1 g intravenously every 8 hours or ceftizoxime 1 g every 8 hours can be given. Guided by antimicrobial susceptibility testing, switching from ceftriaxone to an oral agent can occur 24 to 48 hours after substantial clinical improvement is noted. The total antibiotic duration should be 7 days. If chlamydial infection has not been excluded, treat empirically for chlamydia infection with doxycycline 100 mg orally twice daily for 7 days, unless the individual is pregnant, for which azithromycin 1 g orally in a single dose should be used. For children weighing less than 45 kg, ceftriaxone 50 mg/kg intravenously or intramuscularly is recommended every 24 hours for 7 days. For children over 45 kg, ceftriaxone 1 g intramuscularly or intravenously is recommended every 24 hours for 7 days.
Gonococcal meningitis and endocarditis in adolescents and adults should be treated with ceftriaxone 1 to 2 g intravenously every 12 to 24 hours. If chlamydial infection has not been excluded, empirical treatment of chlamydia infection with doxycycline 100 mg orally twice daily for 7 days, unless the individual is pregnant (azithromycin 1g orally in a single dose should be used).
Infants Born to Mothers Who Have Gonococcal Infection
For neonates up to 4 weeks born to mothers with gonococcal infection who have no signs of gonococcal infection, ceftriaxone 20-50 mg/kg intravenously or intramuscularly should be given in a single dose. The dose should not exceed 250 mg. Ceftriaxone should be administered cautiously in neonates with hyperbilirubinemia. Alternatively, cefotaxime 100 mg/kg as a single intravenous or intramuscular dose can be given.
Empiric therapy for gonococcal infections is often administered during the clinical visit based on a history consistent with possible N gonorrhoeae exposure. In addition, recent sex with a person diagnosed with an STI or a clinical exam suspicious of an STI, eg, penile discharge or abnormal vaginal discharge, should prompt suspicion. If chlamydial infection has not been excluded, empirical treatment of chlamydia infection with doxycycline 100 mg orally twice daily for 7 days, unless the patient is pregnant, for which azithromycin 1 g orally in a single dose should be used.
Antimicrobial Resistance
N gonorrhoeae has evolved antimicrobial resistance since the first use of sulfonamides in the 1930s. In some parts of Asia and Europe, gonococcal isolates exhibiting elevated mean inhibitory concentrations (MICs) to ceftriaxone have been identified, and ceftriaxone treatment failures have been reported. When a high suspicion or confirmation of N gonorrhoeae resistance to standard therapy based on culture and sensitivity results is present, treatment of urogenital infection with a single dose of gentamicin 240 mg IM and a single dose of azithromycin 1 g orally can be administered.[41]
The older oral treatments for gonorrhea have been associated with increasing antimicrobial resistance, resulting in recommendations against the use of fluoroquinolones.[28] Two new oral antibiotics have been developed to treat gonorrhea infection, as noted above. Gepotidacin, a triazaacenaphthylene antibacterial that inhibits bacterial DNA replication, is a newer FDA-approved oral antibiotic for the treatment of uncomplicated urogenital gonorrhea in adolescents and adults. Notably, given the widespread antimicrobial resistance of N gonorrhoeae, which has rendered most antibiotic classes ineffective, ceftriaxone is the primary recommended therapy. Increasing reports of reduced susceptibility to ceftriaxone have raised concern that gonorrhea could become increasingly difficult to treat.[42]
Gepotidacin represents a first-in-class agent that inhibits bacterial DNA replication through a novel mechanism, retaining activity against strains resistant to existing therapies. Clinical trials demonstrated efficacy comparable to standard treatment, supporting its role as an important alternative, particularly when treatment options are limited. However, gepotidacin is approved for use in patients aged 12 years or older who weigh at least 99 pounds (45 kg). This agent is divided into 2 doses of 3000 mg (4 tablets of 750 mg), taken orally 12 hours apart, typically with food to reduce gastrointestinal adverse effects.[43] (A1)
In addition, the FDA has approved zoliflodacin, a spiropyrimidinetrione antibiotic, as another oral agent for the treatment of uncomplicated gonorrhea. The recommended dose of zoliflodacin is 3 grams (1 packet) of granules, dissolved in water, for 1 oral dose. Zoliflodaci is approved for use in people aged 12 and older and weighing at least 35 kg. Together, these approvals mark the first gonorrhea-specific therapeutic advances in decades and represent a meaningful step forward in addressing the growing threat of multidrug-resistant gonorrhea.[44]
If cephalosporin treatment failure is suspected in the United States, clinicians should consult an infectious disease specialist, the STD Clinical Prevention Training Center, their local or state health department, or the CDC for guidance on cultures, susceptibility testing, and treatment. All suspected treatment failures must be reported to the CDC through the local or state health department within 24 hours. Since reinfection is more common than treatment failures, retreatment with the initial regimen of ceftriaxone 500 mg intramuscularly is recommended. When gonorrhea isolates have elevated MICs to cephalosporins, treatment with a single intramuscular dose of gentamicin 240 mg plus oral azithromycin 2 g should be used.[12] If available, 1 of the 2 new oral antibiotics should be considered.
Patient Counseling
Persons treated for gonorrhea should abstain from sexual contact for 7 days after they and their partner have completed treatment.[28] The CDC supports treating sexual partners based on exposure to help identify asymptomatic gonorrhea infections.[38] However, widespread empiric antibiotic use without laboratory confirmation carries a substantial risk of overtreatment and unnecessary antimicrobial exposure. The British Association for Sexual Health and HIV (BASHH) guidelines note that for asymptomatic individuals, postponing epidemiologic treatment until testing is performed at least 14 days after exposure is reasonable. Although this delay may help reduce unnecessary treatment, it also introduces the risk that patients with asymptomatic infections may not return for care after a positive result, allowing continued STI transmission.
In a retrospective cross-sectional review from 2 French clinics that offer free STI testing and treatment, the studied population showed that almost 60% of those given empiric partner treatment ultimately received antibiotics they did not need, while 40% received appropriate treatment. In this study, 94% of patients who tested positive for any STI were successfully contacted and treated. This high rate of follow-up suggests that a test-and-treat strategy can be effective, limiting unnecessary antibiotic use without significantly increasing missed treatment opportunities.[45]
| Pause and Reflect | A 40-year-old man with no significant past medical history presents with a 5-day history of penile discharge and dysuria. He is sexually active with 1 male partner and reports inconsistent condom use. A Gram stain of the discharge reveals gram-negative diplococci. The patient is treated with standard therapy, and symptoms resolve in a few days. However, he returns to the clinic 10 days later with recurrent penile discharge, and Gram stain of the discharge again reveals gram-negative diplococci. What is the most appropriate next step in treatment? |
Differential Diagnosis
Urogenital symptoms caused by gonorrhea can be observed with other STIs, as well as nonsexually transmitted illnesses. Sexually transmitted infections that can cause dysuria, penile discharge, abnormal vaginal discharge, and pelvic pain include C trachomatis, Trichomonas vaginalis, Treponema pallidum, Mycoplasma genitalium, and herpes simplex virus.[31] Urinary tract infections can also present as ureogenital gonorrhea. Although pharyngeal gonorrhea is typically asymptomatic, it can present with symptoms similar to those of viral or bacterial causes of pharyngitis, including streptococcal pharyngitis.
Acute gonococcal infection can impact multiple organ systems. Infectious and noninfectious diseases can cause urethritis, cervicitis, proctitis, conjunctivitis, pharyngitis, and arthritis. Autoimmune, neoplastic, traumatic, and toxicologic etiologies must be considered when evaluating patients presenting with symptoms that raise suspicion of gonorrhea. The gonococcal infection itself can have autoimmune manifestations, eg, reactive arthritis in association with urethritis and conjunctivitis.[6]
Reactive arthritis, Lyme disease, meningococcemia, and acute HIV infection can present like disseminated gonococcal infection. Allergic and viral conjunctivitis are more common than bacterial conjunctivitis, including gonococcal conjunctivitis, in most populations. Viral conjunctivitis is the most frequent cause of infectious "pink eye", accounting for up to 80% of acute cases. Allergic conjunctivitis is also very common, affecting up to 40% of the population. Bacterial conjunctivitis is more common in children than in adults.[46]
Pertinent Studies and Ongoing Trials
As of March 2026, the following clinical trials were ongoing:
- Gonorrhea prevention
- NCT05766904 is a single-center, phase 3, parallel randomized, double-blind, placebo-controlled trial assessing the efficacy of a meningococcal vaccine against Neisseria gonorrhoeae infection among MSM.
- NCT06234943 is a multicenter study to implement and evaluate a novel pilot project involving pharmacy-based management of C trachomatis and N gonorrhoeae, including specimen self-collection (pharyngeal, anorectal, vaginal swabs, and urine samples), assessment, treatment, and linkage to care by community pharmacists in Nova Scotia.
- NCT04415424 is a multicenter, phase 3, double-blinded, randomized placebo-controlled trial evaluating the efficacy of the 4-component meningococcal B vaccine, 4CMenB (Bexsero®), in the prevention of N gonorrhoeae infection.
- NCT06446752 is a multicenter, phase 3, randomized, observer-blind, placebo-controlled study to assess the efficacy of Meningococcal Group B (rMenB+OMV NZ (Bexsero)) for the prevention of gonorrhea in South African cisgender women.
- Gonorrhea diagnostics
- NCT06395675 is a single-center, single-group assignment assessing the performance of the ID NOW™ CT/NG test in male urine, female urine, and self-collected vaginal swabs when tested by intended users (ie, untrained operators). ID NOW™ CT/NG test results will be compared to results from up to 3 FDA-cleared C trachomatis/N gonorrhoeae NAATs for each sample type.
- NCT06234943 is a multicenter study to implement and evaluate a novel pilot project involving pharmacy-based management of C trachomatis and N gonorrhoeae, including specimen self-collection (pharyngeal, anorectal, vaginal swabs, and urine samples), assessment, treatment, and linkage to care by community pharmacists in Nova Scotia.
- NCT06815536 is a multicenter, observational study evaluating whether several investigational tests can accurately detect the gene mutation (mutant allele gyrA 91F) that predicts ciprofloxacin resistance in clinical specimens harboring N gonorrhoeae.
- NCT05286931 is a single-center study evaluating the effectiveness of using the SpeeDx Resistance Plus® GC assay to guide treatment of N gonorrhoeae in a sexual health clinic setting.
Toxicity and Adverse Effect Management
In the United States, clinicians should report any cases of N gonorrhoeae to local or state health departments. Clinicians in England should report cases to GRASP.enquiries@ukhsa.gov.uk. In Wales and Scotland, all cases should be reported to the local Public Health.[28]
Prognosis
Gonorrhea morbidity has risen over the last 20 years, secondary to the progression of antimicrobial resistance.[39] Before the release of the 2 new classes of oral antibiotics for gonorrhea treatment in December 2025, gonorrhea had shown resistance to all antimicrobials that had been used to treat it, creating an urgent global concern.[28] By 2025, resistance was projected to cause almost 70% more deaths compared to 2022. Because of this, antimicrobial resistance should be considered a global health issue.[45]
Complications
Complications from gonorrhea result in substantial morbidity and socioeconomic consequences. If gonorrhea infections are not detected or appropriately treated, they can induce serious complications with reproductive health complications in females, including PID, chronic pelvic pain, infertility, first-trimester abortion, and ectopic pregnancy.[5] Uncommonly, disseminated gonococcal infection can manifest with septic arthritis, endocarditis, and meningitis. Gonorrheal infection can cause male infertility and Fitz-Hugh-Curtis syndrome in females, which is liver capsule inflammation with resultant intra-abdominal adhesions.[1] Without timely treatment, complications of gonorrhea in men include epididymitis, urethral stricture, proctitis, and prostatitis.[43]
Immune-mediated, systemic complications following gonorrhea infection can result in the triad of reactive arthritis, urethritis, and conjunctivitis.[6] Gonorrheal infection can complicate obstetrical delivery by infecting newborns via eye contact with genital secretions during the puerperal period and can result in gonococcal conjunctivitis that can progress to blindness.[7] Gonorrheal infection also increases the risk of sexual transmission of HIV.[6][34]
The development of antimicrobial resistance in N gonorrhoeae is a public health concern with societal implications. Generally, the development of antimicrobial resistance is associated with local, regional, and national antibiotic use. Populations in countries, eg, the Netherlands, with lower utilization of cephalosporins, macrolides, and fluoroquinolones, have a lower incidence of gonococcal resistance than in high-antibiotic-consumption nations.[41]
Consultations
When treating individuals with suspected or confirmed cephalosporin resistance, clinicians are advised to consult an infectious disease specialist and report treatment failure to the CDC within 24 hours of laboratory confirmation of antimicrobial-resistant N gonorrhoeae.[41]
Deterrence and Patient Education
Public health control of gonorrhea relies on effective antimicrobial therapy combined with broad and targeted prevention strategies, accurate diagnostic testing, partner notification, and ongoing surveillance. Treating individuals with appropriate antibiotics is essential to resolving infection, preventing complications, and reducing further transmission.[2]
Patients should avoid sexual activity for at least 1 week after beginning treatment. They should also be advised about the need for microbiologic confirmation of cure when alternative regimens are used, when significant comorbidities, eg, HIV, are present, or when symptoms persist. Repeat testing may identify antibiotic susceptibilities, helping prevent future treatment failures. Individuals with gonorrhea are also at higher risk for acquiring other STIs, including HIV; up to 27% of people diagnosed with HIV have a gonorrhea diagnosis within the preceding 12 months.[47]
In June 2024, the CDC recommended offering doxycycline postexposure prophylaxis (doxyPEP) to males who have sex with males and transgender people assigned female at birth with an STI diagnosis in the prior year, using shared decision-making with healthcare practitioners.[48] DoxyPEP should be administered within 72 hours of condomless oral, vaginal, or anal sex to help reduce the risk of bacterial STIs, gonorrhea, chlamydia, and syphilis, with a recommended dose of 200 mg, and not to exceed 200 mg in 24 hours. Additionally, the CDC notes that evidence is currently insufficient to determine the balance of benefits and harms of doxyPEP for cisgender women.[48]
Pearls and Other Issues
STIs contribute significantly to HIV acquisition by causing mucosal injury and inflammation that recruit HIV-susceptible cells, with prior rectal infections from N gonorrhoeae or C trachomatis conferring an approximately 8-fold increased risk of subsequent HIV infection.[7] Gonorrhea also carries substantial morbidity beyond HIV risk; about half of infants born to mothers with genital infection experience complications, eg, conjunctivitis or pneumonia.[7]
The growing threat of antimicrobial resistance in N gonorrhoeae, including the global spread of strains with high-level ceftriaxone resistance, has heightened public health concern and accelerated interest in new strategies, eg, the potential protective effect of the meningococcal B vaccine and resistance-guided therapy using rapid molecular diagnostics to support alternative regimens and reduce selective pressure.[7] This has led to the development of novel antibiotics and to FDA approval of zoliflodacin and gepotidacin for the treatment of uncomplicated gonorrhea. The economic burden is notable as well. Compounding these challenges, guideline adherence remains suboptimal. In a large convenience sample of United States primary care patients from 2018 to 2022, only slightly more than 38% of individuals diagnosed with gonorrhea received the recommended ceftriaxone treatment.[49]
Enhancing Healthcare Team Outcomes
Gonorrhea is a common sexually transmitted infection caused by Neisseria gonorrhoeae, a gram-negative diplococcus that infects columnar epithelium of the cervix, urethra, rectum, pharynx, and conjunctiva. Infection begins with bacterial adhesion via pili and surface proteins, followed by invasion of the epithelium and local inflammation. Clinical presentation ranges from asymptomatic infection—especially in individuals assigned female at birth—to symptomatic urethritis, cervicitis, or pelvic inflammatory disease, with potential progression to infertility, ectopic pregnancy, or disseminated infection. Diagnosis relies on nucleic acid amplification testing, with site-specific sampling guided by a thorough sexual history. Management includes ceftriaxone-based therapy, consideration of concurrent treatment for chlamydia, and emerging oral agents amid rising antimicrobial resistance. Early detection and treatment are critical to prevent complications and transmission.
Interprofessional collaboration is essential for optimizing outcomes and reducing disease burden. Physicians and advanced practitioners lead diagnostic evaluation and treatment selection, while primary care clinicians ensure appropriate screening and longitudinal care. Nurses support patient education, specimen collection, and adherence monitoring. Pharmacists reinforce antimicrobial stewardship, counsel on medication use, and identify drug interactions. Public health professionals facilitate partner notification and reporting, while all team members engage in shared decision-making, risk-reduction counseling, and coordinated follow-up to prevent reinfection and complications.
Media
(Click Image to Enlarge)
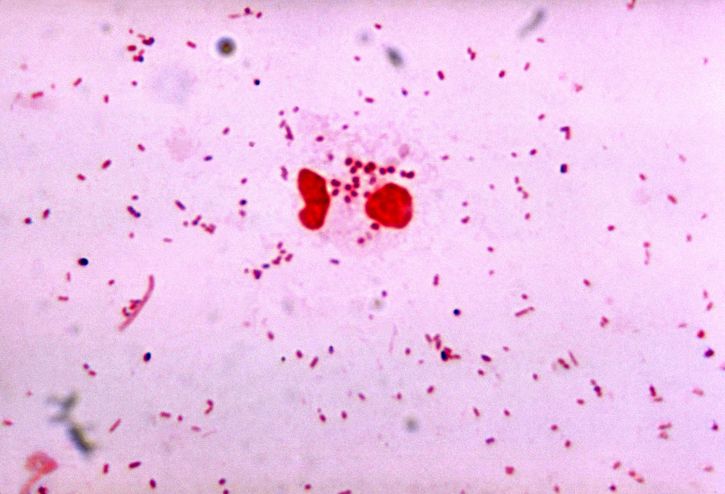
Gonorrhea Gram Stain. Image of gonorrhea diplococcus on a Gram stain.
Dr. James Volk, USCDCP, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
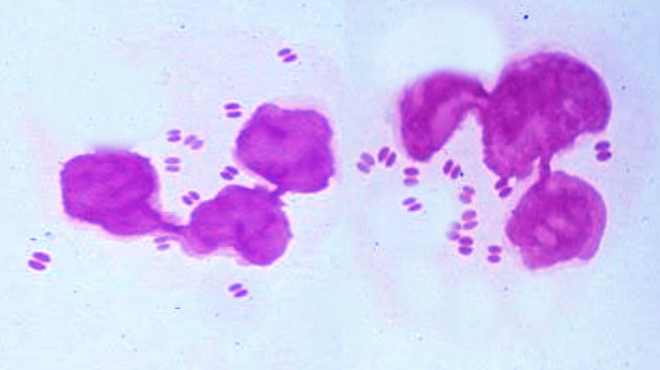
N Gonorrhoeae. Image of N gonorrhoeae; note diplococci.
Contributed by S Bhimji, MD
References
Pyle A, Garner L, Wallace Huff C. Gonorrhea and Chlamydia Infections in Women. Clinical obstetrics and gynecology. 2025 Jun 1:68(2):164-169. doi: 10.1097/GRF.0000000000000931. Epub 2025 Feb 26 [PubMed PMID: 40008679]
Unemo M, Shafer WM. Antimicrobial resistance in Neisseria gonorrhoeae in the 21st century: past, evolution, and future. Clinical microbiology reviews. 2014 Jul:27(3):587-613. doi: 10.1128/CMR.00010-14. Epub [PubMed PMID: 24982323]
Unemo M, Shafer WM. Antibiotic resistance in Neisseria gonorrhoeae: origin, evolution, and lessons learned for the future. Annals of the New York Academy of Sciences. 2011 Aug:1230():E19-28. doi: 10.1111/j.1749-6632.2011.06215.x. Epub [PubMed PMID: 22239555]
Level 3 (low-level) evidenceMahapure K, Singh A. A Review of Recent Advances in Our Understanding of Neisseria gonorrhoeae. Cureus. 2023 Aug:15(8):e43464. doi: 10.7759/cureus.43464. Epub 2023 Aug 14 [PubMed PMID: 37711920]
Level 3 (low-level) evidenceUnemo M. Current and future antimicrobial treatment of gonorrhoea - the rapidly evolving Neisseria gonorrhoeae continues to challenge. BMC infectious diseases. 2015 Aug 21:15():364. doi: 10.1186/s12879-015-1029-2. Epub 2015 Aug 21 [PubMed PMID: 26293005]
Chan PA, Robinette A, Montgomery M, Almonte A, Cu-Uvin S, Lonks JR, Chapin KC, Kojic EM, Hardy EJ. Extragenital Infections Caused by Chlamydia trachomatis and Neisseria gonorrhoeae: A Review of the Literature. Infectious diseases in obstetrics and gynecology. 2016:2016():5758387. doi: 10.1155/2016/5758387. Epub 2016 Jun 5 [PubMed PMID: 27366021]
Allan-Blitz LT, Klausner JD. The Impacts and Consequences of Sexually Transmitted Infections in the United States. Sexually transmitted diseases. 2025 May 1:52(5):285-289. doi: 10.1097/OLQ.0000000000002126. Epub 2024 Dec 23 [PubMed PMID: 39714030]
Saldanha N. STIs in adolescents: Chlamydia, gonorrhea, mycoplasma genitalium, and HPV. Current problems in pediatric and adolescent health care. 2020 Jul:50(7):100835. doi: 10.1016/j.cppeds.2020.100835. Epub 2020 Aug 5 [PubMed PMID: 32768342]
Tao X, Ghanem KG, Page KR, Gilliams E, Tuddenham S. Risk factors predictive of sexually transmitted infection diagnosis in young compared to older patients attending sexually transmitted diseases clinics. International journal of STD & AIDS. 2020 Feb:31(2):142-149. doi: 10.1177/0956462419886772. Epub 2020 Jan 21 [PubMed PMID: 31964236]
Shannon CL, Klausner JD. The growing epidemic of sexually transmitted infections in adolescents: a neglected population. Current opinion in pediatrics. 2018 Feb:30(1):137-143. doi: 10.1097/MOP.0000000000000578. Epub [PubMed PMID: 29315111]
Level 3 (low-level) evidenceKumar B, Kaushal I, Narayanan B, Narang T. Sexually transmitted infections in the elderly: A growing concern in geriatric care. Indian journal of sexually transmitted diseases and AIDS. 2025 Jan-Jun:46(1):16-21. doi: 10.4103/ijstd.ijstd_108_24. Epub 2025 Jun 9 [PubMed PMID: 40546355]
Lee G, Hoffman MF, DuBois Shihabuddin C. Current Challenges in Gonorrhea Management: A Focus on Diagnosis, Treatment, and Antimicrobial Resistance. The Nursing clinics of North America. 2025 Sep:60(3):537-552. doi: 10.1016/j.cnur.2024.10.005. Epub 2025 May 22 [PubMed PMID: 40716812]
Ong JJ, Fethers K, Howden BP, Fairley CK, Chow EPF, Williamson DA, Petalotis I, Aung E, Kanhutu K, De Petra V, Chen MY. Asymptomatic and symptomatic urethral gonorrhoea in men who have sex with men attending a sexual health service. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases. 2017 Aug:23(8):555-559. doi: 10.1016/j.cmi.2017.02.020. Epub 2017 Feb 28 [PubMed PMID: 28257898]
Fein LA, Marbin S, Barnett R, Coudray M. Sexually Transmitted Infection Considerations for Transgender and Gender Expansive Persons. Clinical obstetrics and gynecology. 2025 Jun 1:68(2):213-222. doi: 10.1097/GRF.0000000000000934. Epub 2025 Mar 6 [PubMed PMID: 40045902]
Magee LA, Fortenberry JD, Nelson T, Roth A, Arno J, Wiehe SE. Sexually Transmitted Infections in Association With Area-Level Prostitution and Drug-Related Arrests. Sexually transmitted diseases. 2021 Jul 1:48(7):508-514. doi: 10.1097/OLQ.0000000000001345. Epub [PubMed PMID: 33346589]
Newman LM, Berman SM. Epidemiology of STD disparities in African American communities. Sexually transmitted diseases. 2008 Dec:35(12 Suppl):S4-12. doi: 10.1097/OLQ.0b013e31818eb90e. Epub [PubMed PMID: 18971796]
Barrow RY, Berkel C, Brooks LC, Groseclose SL, Johnson DB, Valentine JA. Traditional sexually transmitted disease prevention and control strategies: tailoring for African American communities. Sexually transmitted diseases. 2008 Dec:35(12 Suppl):S30-9. doi: 10.1097/OLQ.0b013e31818eb923. Epub [PubMed PMID: 18955915]
Banks DE, Hensel DJ, Zapolski TCB. Integrating Individual and Contextual Factors to Explain Disparities in HIV/STI Among Heterosexual African American Youth: A Contemporary Literature Review and Social Ecological Model. Archives of sexual behavior. 2020 Aug:49(6):1939-1964. doi: 10.1007/s10508-019-01609-6. Epub 2020 Mar 10 [PubMed PMID: 32157486]
Level 2 (mid-level) evidenceHenriquez PS, Heimesaat MM. Ethnic disparities in prevalence and screening rates of sexually transmitted infections. European journal of microbiology & immunology. 2025 Oct 7:15(3):164-171. doi: 10.1556/1886.2025.00052. Epub 2025 Oct 3 [PubMed PMID: 41042613]
Swanson J. Studies on gonococcus infection. IV. Pili: their role in attachment of gonococci to tissue culture cells. The Journal of experimental medicine. 1973 Mar 1:137(3):571-89 [PubMed PMID: 4631989]
Harvey HA, Porat N, Campbell CA, Jennings M, Gibson BW, Phillips NJ, Apicella MA, Blake MS. Gonococcal lipooligosaccharide is a ligand for the asialoglycoprotein receptor on human sperm. Molecular microbiology. 2000 Jun:36(5):1059-70 [PubMed PMID: 10844691]
Edwards JL, Brown EJ, Uk-Nham S, Cannon JG, Blake MS, Apicella MA. A co-operative interaction between Neisseria gonorrhoeae and complement receptor 3 mediates infection of primary cervical epithelial cells. Cellular microbiology. 2002 Sep:4(9):571-84 [PubMed PMID: 12390350]
Edwards JL, Brown EJ, Ault KA, Apicella MA. The role of complement receptor 3 (CR3) in Neisseria gonorrhoeae infection of human cervical epithelia. Cellular microbiology. 2001 Sep:3(9):611-22 [PubMed PMID: 11553013]
Level 3 (low-level) evidenceEdwards JL, Shao JQ, Ault KA, Apicella MA. Neisseria gonorrhoeae elicits membrane ruffling and cytoskeletal rearrangements upon infection of primary human endocervical and ectocervical cells. Infection and immunity. 2000 Sep:68(9):5354-63 [PubMed PMID: 10948165]
Rice PA. Molecular basis for serum resistance in Neisseria gonorrhoeae. Clinical microbiology reviews. 1989 Apr:2 Suppl(Suppl):S112-7 [PubMed PMID: 2497955]
Edwards JL, Apicella MA. The molecular mechanisms used by Neisseria gonorrhoeae to initiate infection differ between men and women. Clinical microbiology reviews. 2004 Oct:17(4):965-81, table of contents [PubMed PMID: 15489357]
Tuddenham S, Hamill MM, Ghanem KG. Diagnosis and Treatment of Sexually Transmitted Infections: A Review. JAMA. 2022 Jan 11:327(2):161-172. doi: 10.1001/jama.2021.23487. Epub [PubMed PMID: 35015033]
Fifer H, Ismail MA, Soni S, Nwaosu U, Sadiq ST, Milligan A, Saunders J, Medland N. British Association of Sexual Health and HIV UK National Guideline for the Management of infection with Neisseria gonorrhoeae, 2025. International journal of STD & AIDS. 2025 Oct:36(11-12):826-840. doi: 10.1177/09564624251345195. Epub 2025 May 31 [PubMed PMID: 40448704]
Bhide A, Nama V, Patel S, Kalu E. Microbiology of cysts/abscesses of Bartholin's gland: review of empirical antibiotic therapy against microbial culture. Journal of obstetrics and gynaecology : the journal of the Institute of Obstetrics and Gynaecology. 2010:30(7):701-3. doi: 10.3109/01443615.2010.505672. Epub [PubMed PMID: 20925614]
Meyer T, Buder S. The Laboratory Diagnosis of Neisseria gonorrhoeae: Current Testing and Future Demands. Pathogens (Basel, Switzerland). 2020 Jan 31:9(2):. doi: 10.3390/pathogens9020091. Epub 2020 Jan 31 [PubMed PMID: 32024032]
Workowski KA, Bolan GA, Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports. 2015 Jun 5:64(RR-03):1-137 [PubMed PMID: 26042815]
Said M, Tirthani E. Gonococcal Infective Endocarditis Returns. Cureus. 2021 Sep:13(9):e17955. doi: 10.7759/cureus.17955. Epub 2021 Sep 14 [PubMed PMID: 34660143]
Sherrard J, Barlow D. Gonorrhoea in men: clinical and diagnostic aspects. Genitourinary medicine. 1996 Dec:72(6):422-6 [PubMed PMID: 9038638]
Level 2 (mid-level) evidenceKirkcaldy RD, Harvey A, Papp JR, Del Rio C, Soge OO, Holmes KK, Hook EW 3rd, Kubin G, Riedel S, Zenilman J, Pettus K, Sanders T, Sharpe S, Torrone E. Neisseria gonorrhoeae Antimicrobial Susceptibility Surveillance - The Gonococcal Isolate Surveillance Project, 27 Sites, United States, 2014. Morbidity and mortality weekly report. Surveillance summaries (Washington, D.C. : 2002). 2016 Jul 15:65(7):1-19. doi: 10.15585/mmwr.ss6507a1. Epub 2016 Jul 15 [PubMed PMID: 27414503]
Goggins ER, Chamberlain AT, Kim TG, Young MR, Jamieson DJ, Haddad LB. Patterns of Screening, Infection, and Treatment of Chlamydia trachomatis and Neisseria gonorrhea in Pregnancy. Obstetrics and gynecology. 2020 Apr:135(4):799-807. doi: 10.1097/AOG.0000000000003757. Epub [PubMed PMID: 32168225]
Geraats-Peters CW, Brouwers M, Schneeberger PM, van der Zanden AG, Bruisten SM, Weers-Pothoff G, Boel CH, van den Brule AJ, Harmsen HG, Hermans MH. Specific and sensitive detection of Neisseria gonorrhoeae in clinical specimens by real-time PCR. Journal of clinical microbiology. 2005 Nov:43(11):5653-9 [PubMed PMID: 16272500]
Van Der Pol B, Taylor SN, Mena L, Lebed J, McNeil CJ, Crane L, Ermel A, Sukhija-Cohen A, Gaydos CA. Evaluation of the Performance of a Point-of-Care Test for Chlamydia and Gonorrhea. JAMA network open. 2020 May 1:3(5):e204819. doi: 10.1001/jamanetworkopen.2020.4819. Epub 2020 May 1 [PubMed PMID: 32407506]
Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, Reno H, Zenilman JM, Bolan GA. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports. 2021 Jul 23:70(4):1-187. doi: 10.15585/mmwr.rr7004a1. Epub 2021 Jul 23 [PubMed PMID: 34292926]
Suay-García B, Pérez-Gracia MT. Future Prospects for Neisseria gonorrhoeae Treatment. Antibiotics (Basel, Switzerland). 2018 Jun 15:7(2):. doi: 10.3390/antibiotics7020049. Epub 2018 Jun 15 [PubMed PMID: 29914071]
Walker CK, Workowski KA, Washington AE, Soper D, Sweet RL. Anaerobes in pelvic inflammatory disease: implications for the Centers for Disease Control and Prevention's guidelines for treatment of sexually transmitted diseases. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 1999 Jan:28 Suppl 1():S29-36 [PubMed PMID: 10028108]
Unemo M, Del Rio C, Shafer WM. Antimicrobial Resistance Expressed by Neisseria gonorrhoeae: A Major Global Public Health Problem in the 21st Century. Microbiology spectrum. 2016 Jun:4(3):. doi: 10.1128/microbiolspec.EI10-0009-2015. Epub [PubMed PMID: 27337478]
Keam SJ. Gepotidacin: First Approval. Drugs. 2025 Nov:85(11):1479-1485. doi: 10.1007/s40265-025-02214-9. Epub 2025 Aug 5 [PubMed PMID: 40762778]
Ross JDC, Wilson J, Workowski KA, Taylor SN, Lewis DA, Gatsi S, Flight W, Scangarella-Oman NE, Jakielaszek C, Lythgoe D, Powell M, Janmohamed S, Absalon J, Perry C. Oral gepotidacin for the treatment of uncomplicated urogenital gonorrhoea (EAGLE-1): a phase 3 randomised, open-label, non-inferiority, multicentre study. Lancet (London, England). 2025 May 3:405(10489):1608-1620. doi: 10.1016/S0140-6736(25)00628-2. Epub 2025 Apr 14 [PubMed PMID: 40245902]
Level 1 (high-level) evidenceYurube T, Shigemura K, Kobayashi Y, Maeda T, Nishimura N, Yamada A, Kotani K, Horii S, Yoshida H, Osawa K. Susceptibility of Neisseria gonorrhoeae to Zoliflodacin and Quinolones in Hyogo Prefecture, Japan. Pathogens (Basel, Switzerland). 2025 Aug 21:14(8):. doi: 10.3390/pathogens14080831. Epub 2025 Aug 21 [PubMed PMID: 40872341]
Ben Said L, Conrad A, Souza S, Alfaiate D, Ader F, Batalla AS, Godinot M. Partner treatment strategies for Chlamydia and Gonorrhea: Time for a reappraisal. Infectious diseases now. 2025 May:55(3):105038. doi: 10.1016/j.idnow.2025.105038. Epub 2025 Feb 11 [PubMed PMID: 39947479]
Azari AA, Barney NP. Conjunctivitis: a systematic review of diagnosis and treatment. JAMA. 2013 Oct 23:310(16):1721-9. doi: 10.1001/jama.2013.280318. Epub [PubMed PMID: 24150468]
Level 1 (high-level) evidenceSchwarcz S, Weinstock H, Louie B, Kellogg T, Douglas J, Lalota M, Dickinson G, Torian L, Wendell D, Paul S, Goza G, Ruiz J, Boyett B, McCormick L, Bennett D. Characteristics of persons with recently acquired HIV infection: application of the serologic testing algorithm for recent HIV seroconversion in 10 US cities. Journal of acquired immune deficiency syndromes (1999). 2007 Jan 1:44(1):112-5 [PubMed PMID: 17075386]
Sankaran M, Glidden DV, Kohn RP, Nguyen TQ, Bacon O, Buchbinder SP, Gandhi M, Havlir DV, Liebi C, Luetkemeyer AF, Nguyen JQ, Roman J, Scott H, Torres TS, Cohen SE. Doxycycline Postexposure Prophylaxis and Sexually Transmitted Infection Trends. JAMA internal medicine. 2025 Mar 1:185(3):266-272. doi: 10.1001/jamainternmed.2024.7178. Epub [PubMed PMID: 39761052]
Hao S, Tao G, Pearson WS, Rochlin I, Phillips RL, Rehkopf DH, Kamdar N. Treatment of Chlamydia and Gonorrhea in Primary Care and Its Patient-Level Variation: An American Family Cohort Study. Annals of family medicine. 2025 Mar 24:23(2):136-144. doi: 10.1370/afm.240164. Epub 2025 Mar 24 [PubMed PMID: 40127987]