Introduction
Glasgow Coma Scale (GCS) offers an objective method for describing the extent of impaired consciousness in patients with acute medical conditions or trauma.[1] This is one of the most widely used clinical scales in neuroscience and one of the most-cited articles in the medical literature.[2] Since 1974, publications referencing the GCS have increased globally at an average annual rate of 16.7%, with citations now exceeding 37,000.[3] The scale evaluates 3 aspects of responsiveness: eye-opening, verbal, and motor responses. Reporting each component separately allows clinicians to convey a clear, detailed picture of the patient’s neurologic status. Individual findings from each component are aggregated into a total GCS, offering a concise summary of overall severity.[4]
GCS has stood the test of time since its publication in The Lancet in 1974. Graham Teasdale (chief resident) and Bryan Jennett at Queen Elizabeth Hospital, Glasgow, formulated the scoring system to ease and standardize communication about patients' level of consciousness. All 13 scales referred to by Jennett and Teasdale included motor response. Nine out of ten had incorporated verbal performance, whereas only half of them had included the eye response. Miller Fisher, Plum, and Posner's insights were also pivotal in formulating this scoring system.[2] In 1977, the original total score of 14 was increased to 15 points to include the withdrawal response. Scores of zero for each component were excluded to avoid confusion from missing information during data computation.[5]
Early adaptability and word-of-mouth about its merits from the nursing body and trainees were critical to its widespread appraisal. Furthermore, this was adopted by the "International Data Bank," with ties to centers in Rotterdam, Groningen, and Los Angeles.[2] The 1978 Journal of Neurosurgery (JNS) editorial by Tom Langfitt and the inclusion in Advanced Trauma Life Support (ATLS) provided a pivotal impetus for its global recognition.[2][5] In 1988, the World Federation of Neurosurgical Societies (WFNS) incorporated it into its grading scale for subarachnoid hemorrhage.[6] The GCS has since become embedded in numerous clinical guidelines and scoring systems for trauma and critical illness, extending across all age groups, including preverbal children. Required by the National Institute of Health (NIH) Common Data Elements for head injury studies and included in the ICD-11, the GCS is now used in over 75 countries.[7][8][9]
Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Function
Scoring and Parameters:
The GCS evaluates the following 3 parameters of responsiveness: best eye response (E), best verbal response (V), and best motor response (M). The levels of response in the components of the GCS are scored from 1 (no response) up to normal values of 4 (eye-opening response), 5 (verbal response), and 6 (motor response), respectively. The total GCS score ranges from 3 to 15, with 3 being the lowest and 15 being the highest.
The score is the sum of the individual elements' scores. For example, a score of 10 might be expressed as GCS10 = E3V4M3. Clinicians should denote any untestable component of the GCS as "NT" (not testable) and avoid using the total score when a component is not testable. The following scores are assigned for each response parameter:
- Best eye response
- No eye-opening
- Eyes opening to pain
- Eyes opening to command
- Eyes open spontaneously
- Best verbal response
- No verbal response
- Incomprehensible sounds
- Inappropriate words
- Confused
- Orientated
- Best motor response
- No motor response
- Abnormal extension to pain
- Abnormal flexion to pain
- Withdrawal from pain
- Localizing pain
- Obeys commands
Application of the Glasgow Coma Scale in Pediatric Patients
The GCS can be used in children older than 5 years without modification. However, younger children and infants are unable to provide the necessary verbal responses for a clinician to use the scale to assess their orientation or obey commands to evaluate their motor response. Since the pediatric GCS was initially described in Adelaide, several modifications have been made, but no single method has become universally accepted.[10] The following versions are derived from those of James and the Pediatric Emergency Care Applied Research Network in preverbal children younger than 2 years and verbal children older than 2 years (see Table. Modified Pediatric Glasgow Coma Scale).[11]
Table. Modified Pediatric Glasgow Coma Scale
| Children Younger Than 2 Years (Preverbal) | Children Older Than 2 Years (Verbal) | |
| Best Eye Response |
|
|
| Best Verbal Response |
|
|
| Best Motor Response |
|
|
Neuroanatomical Correlations
Eye-opening response
The basal ganglia are involved in the Fixed Action Patterns (FAPs) of motor movements (action selection) to spoken language (E3).[12] The area ventral to the peri-aqueductal grey matter governs eyelid closure, while the area dorsal to the peri-aqueductal grey matter mediates eye opening to painful stimulus (E2).[13]
Motor response
The "neuromatrix", or nociception, activates "Aδ" (A-delta) fibers (fast, sharp pain) and "C" fibers (persisting, slow-burning pain) that relay to the main relay station, which is the thalamus. The insula governs pain intensity and the mapping of the pain generator. The ventroposterolateral (VPL) and ventromedial thalamic nuclei then relay well-localized pain signals (M5) to the primary somatosensory cortex.[14]
The rubrospinal tract helps to flex the upper limb, leading to decorticate posturing (M3). Please see StatPearls' companion resource, "Decorticate Posturing," for further information. The vestibulospinal tract, on the other hand, causes extension of both the upper and the lower limbs, leading to decerebrate posturing (M2). Please see StatPearls' companion resource, "Neuroanatomy Decerebrate Rigidity" and "Decerebrate and Decorticate Posturing," for further information. Lesion below the vestibular nucleus leads to flaccid paralysis of all the extremities (M1).
The development of motor activity is highly adaptive for survival during growth and evolution and is reflected in the progression of the following motor responses:
- Antigravity postures generated by central pattern generators in the brainstem and spinal cord through disinhibition (M2)
- Programmed patterns, including feeding and locomotion (M3)
- Purposeful extremity movement, such as targeting and grasping (M5)
- Skilled digit movements involving dexterity and manipulation, including following commands (M6)
Verbal response
Speech "codes" first relay on the inferior colliculus. Lesion here leads to incomprehensible speech (V2). Early auditory processing and word recognition take place in the inferior temporal region ("what" pathway).[15] Lesion here leads to inappropriate speech (V3).
The basal ganglia play a role in sequence processing, which can result in syntax deficits.[16] The left basal ganglia monitor the semantic and lexical aspects of language. Putamen engages in cortical initiation, while the cerebellum amplifies and refines this signal for oriented language behavior (lesion leads to disorganized speech; V4). As additional sensory clues that guide the arcuate fasciculus and the ganglion for oriented language behavior are absent, this results in disorganized speech.[17] At the cortical level, speech is produced and continuously monitored by sensory input and subcortical centers, resulting in oriented verbal responses (V5).
Issues of Concern
Factors That May Interfere With GCS Assessment
Preexisting factors
Language barriers, intellectual or neurologic deficits, hearing loss, and speech impairment may limit reliable evaluation. Application in pediatric populations can also be challenging due to developmental variability.
Physiologic and metabolic confounders
Alcohol, seizures, hypothermia, hypoxia, hypotension, and drug intoxication can alter mental status and lead to falsely low scores. Sedatives, particularly benzodiazepines and polysubstance use, may significantly depress GCS, with scores increasing on reassessment. Screening for intoxication is recommended when clinically appropriate.[18]
Injury-related, polytrauma, and treatment-related factors
Maxillofacial trauma and intubation limit verbal scoring, periorbital injury may impair eye assessment, and spinal cord injury affects motor evaluation. In intubated patients, the verbal component is recorded as "V–ET." When the verbal score is unobtainable, the eye–motor sum may be used to estimate overall severity and maintain prognostic accuracy.
Hypotension and hypoxia introduce significant confounding bias and may independently depress GCS scores. Scoring of individual components may also be limited by injury patterns: the verbal (V) component is impaired in maxillofacial trauma or intubated patients, the eye (E) component may be affected by periorbital swelling (eg, raccoon eyes), and the motor (M) component may be limited in spinal cord injury.
In intubated patients who are unable to speak, assessment relies on eye-opening and motor responses, with the suffix "ET" added to indicate intubation. When the verbal component cannot be assessed, commonly due to intubation or sedation, an imputation strategy using the eye–motor score can estimate severity: add 1 point for scores 2 to 6, add 2 points for 7, add 4 points for 8 or 9, and add 5 points for 10. This method preserves prognostic accuracy and supports consistent communication when the verbal component is not testable.[19] In stroke patients with aphasia or intubation, the eye–motor sum alone predicts early mortality comparably to the full GCS. Sedation or pharmacologic paralysis may further confound assessment.[19]
Limitations of the Glasgow Coma Scale
Timing of initial assessment
In trauma patients, the first GCS in the emergency department should ideally be obtained once the patient is hemodynamically stable to minimize confounding effects from hypoxia and hypotension.
Interobserver variability and reproducibility
The motor component is the most challenging to interpret, particularly when distinguishing between withdrawal (M4), abnormal flexion (M3), and localization (M5).[20] Definitions of M3 vary across the literature, contributing to inconsistency. The use of standardized criteria and cognitive aids may reduce errors.
M5 is scored when, following a supraorbital stimulus, the hand crosses the chin, or after a nail-bed stimulus, the contralateral hand crosses the midline to remove the stimulus.[21] In M4, the hand moves above the clavicle in response to supraorbital stimulation but does not reach toward the stimulus site. Variability exists in defining M3. Teasdale and Jennett differentiated M4 from M3 based on shoulder movement—abduction in M4 versus adduction in M3—and described M3 as a slower, stereotyped response.[1] Van der Naalt defined M3 by the presence of at least 2 features, including forearm extension or internal rotation, thumb adduction, maximal wrist flexion, or associated lower extremity extension and internal rotation.[21] Matis and Birbilis described M3 as arm adduction with flexion at the elbow, wrist, and fingers, along with leg extension and plantar flexion.[22] They further characterized M2 by arm adduction and pronation with leg extension and plantar flexion. Use of structured cognitive aids may help reduce interpretation errors.[23]
Variation in noxious stimulus application
Considerable variability exists in the anatomical sites used to apply painful stimuli, including the nail bed, trapezius, pectoralis, earlobe, sternum, supraorbital ridge, mandible, and styloid process. The selection of these sites often reflects training backgrounds, peer observations, and institutional policies. Some methods, eg, sternal rub and earlobe pinch, are associated with higher complication rates. Similarly, bruises and fractures (sternum stimulus), loss of nails (nail bed stimulus), and exacerbation of intracranial or ocular injury (supraorbital stimulus) invariably occur and can lead to charges accounting for an "assault," "battery," or other potential medicolegal implications.
Teasdale and Jennett initially recommended nail-bed pressure but later favored fingertip pressure as a safer peripheral stimulus. Central stimuli include trapezius pinch and supraorbital pressure. Regardless of the site, all stimuli ultimately activate the primary somatosensory cortex. Current guidance recommends beginning with peripheral stimulation (fingertip or nail bed), followed by applying firm pressure to either the trapezius muscle or the supraorbital notch if no response is elicited (see Image. Glasgow Coma Scale Responses).[GCS AID]
Duration of stimulus application
Because nociception involves transduction, transmission, modulation, and perception, painful stimuli should be applied for at least 30 seconds to allow adequate assessment.
Assessment challenges
Eye opening is typically assessed first or concurrently. In the absence of a response, clinicians often escalate the stimuli or seek expert input.[24]
Physiologic and neurologic limitations
GCS does not assess brainstem reflexes, pupillary responses, respiratory patterns, or concurrent eye movement disorders.[20] The total score is also skewed toward the motor component, which may disproportionately influence overall interpretation.
Interpretation limitations
Patients with the same total GCS score but different subscale combinations can have markedly different mortality rates; for example, a GCS of 4, composed of 1+1+2, predicts a mortality rate of 48%, whereas 2+1+1 predicts a mortality rate of 19%.
Clinical utility limitations
GCS may underestimate the need for early surgical intervention in mild to moderate head injury and is a limited predictor of functional outcomes, despite its utility in mortality prognostication. The total score may also misclassify the level of consciousness, as identical scores can represent different clinical states. A GCS of 8 may correspond to a vegetative state, minimally conscious state, or posttraumatic confusional state, and scores of 7 to 11 encompass multiple distinct disorders of consciousness.[25]
Additionally, the GCS may underestimate the need for timely referral or surgical intervention in mild to moderate head injury, particularly in cases, eg, depressed skull fracture and pneumocephalus.[26] Although useful for mortality stratification, the GCS remains a poor predictor of long-term functional outcomes.[27]
Adjuncts to Improve GCS Prognostication and Stratification
Additional systems that can be used to enhance GCS prognostication include:
- The Full Outline of UnResponsiveness (FOUR) score (an alternative validated scoring system) [20]
- Short-form GCS incorporating only motor and pupillary responses (has the same predictive value as the GCS)
- Neurological Pupil Index
- Rotterdam and Marshal CT scoring system [28]
- Serum biomarkers, such as glial fibrillary acidic protein (GFAP) [29]
- Concurrent assessment of intracranial pressure (ICP) waveforms [30]
- Optic nerve sheath diameter (ONSD) measurement [31]
Clinical Significance
Assessment of responsiveness and the level of consciousness with the GCS is widely used to guide early management of patients with a head injury or other kind of acute brain injury. Decisions for more severely impaired patients include emergent management (eg, securing the airway) and triage to determine appropriate management algorithms. Decisions in less severely impaired patients include the need for neuroimaging, admission for observation, or discharge. Serial GCS assessments are also crucial for monitoring a patient's clinical course and guiding management adjustments.
The information gained from the 3 components of the GCS varies across the spectrum of responsiveness (see Image. Glasgow Coma Scale Responses).[32] Changes in motor response are the predominant factor in patients with more severe impairments, whereas eye and verbal responses are more useful in those with less severe impairments. For individual patients, the clinical findings in the 3 components should therefore be reported separately. The total score provides a useful overall summary index, though it omits other necessary information, such as pupillary size and reactivity.
In both preverbal and verbal pediatric patients, the GCS is an accurate marker for clinically significant traumatic brain injury (ie, those requiring neurosurgical intervention, intubation for over 24 hours, hospitalization for more than 2 nights, or causing death).[9] The GCS has been incorporated into numerous guidelines and assessment scores, including trauma guidelines (eg, Advanced Trauma Life Support), Brain Trauma Foundation guidelines for severe traumatic brain injury, intensive care scoring systems (eg, APACHE II, SOFA), and Advanced Cardiac Life Support.
Classification of Severity of Traumatic Brain Injury
The relationship between the GCS score and outcome is the basis for the following common classification of acute traumatic brain injury:
- Severe: GCS 3 to 8
- Moderate: GCS 9 to 12
- Mild: GCS 13 to 15
In pediatric head injury, a GCS threshold of 5 or less identifies the severe injury more accurately than the adult cutoff of 8, because pediatric traumatic brain injury patients with scores of 3 to 5 exhibit markedly higher mortality and morbidity.[33]
Glasgow Coma Scale Pupils Score
The Glasgow Coma Scale Pupils Score (GCS-P) was described by Paul Brennan, Gordon Murray, and Graham Teasdale in 2018 as a strategy to combine the 2 key indicators of the severity of traumatic brain injury into a single, simple index.[34][35] The GCS-P score is calculated by subtracting the Pupil Reactivity Score (PRS) from the total GCS score: GCS-P = GCS – PRS. The PRS reflects the number of unreactive pupils in response to light as follows:
-
Both pupils unreactive: PRS = 2
-
One pupil unreactive: PRS = 1
-
Both pupils are reactive: PRS = 0
The GCS-P score ranges from 1 to 15, extending the range over which early severity is shown to relate to outcomes, including mortality and independent recovery. GCS-P scores between 1 and 8 indicate a severe injury.
The MOST (mortality score for traumatic brain injury) integrates the GCS components, pupillary reactivity, and age. Specifically, MOST assigns weights to each component, and, based on the sum of these values, a conversion table predicts mortality risk. The area under the curve (AUC) of the model in the United States trauma population was 0.875, outperforming CRASH-Basic (AUC = 0.837) and IMPACT-Core (AUC = 0.821) models.[36]
Dichotomizing Clinical Outcomes
A positive correlation between progressive decline in GCS and subsequent mortality is often noted. The findings for the eye, verbal, and motor responses also relate to the outcome, but in distinctive ways, so that assessing each separately yields more information than the aggregated total score.[32]
Although widely recognized as one of the most powerful clinical prognostic indicators, the GCS score, or any single clinical feature, should not be used in isolation to predict an individual patient's outcome. Several factors influence the prognostic value of the GCS score, including the underlying diagnosis, the mechanism of injury in trauma cases, and the presence of extracranial injuries.[37] Patient-specific variables, eg, age, pupillary abnormalities, and imaging results, also affect outcome predictions. The multifactorial prognostic models, eg, those developed in the International Mission on Prognosis and Clinical Trial Design in TBI (IMPACT) and Corticosteroid Randomization after significant head injury (CRASH) trials, have also integrated these clinical indicators.[37][38]
Classifying the Disorders of Consciousness
GCS serves as a tool for classifying disorders of consciousness. A decision tree based on sequential evaluation of GCS subscores enables systematic categorization. This approach designates a recovered posttraumatic confusional state (rPTCS) when the verbal score (V) equals 5 (oriented) and a posttraumatic confusional state (PTCS) when V equals 4 (confused). A minimally conscious state with preserved language (MCS+) is assigned when V equals 3 or motor score (M) equals 6, while a minimally conscious state without preserved language (MCS−) is assigned when M equals 5, and V is less than 3. When none of these criteria apply, the classification assigns a vegetative state/unresponsive wakefulness syndrome if V equals 2 or if eye opening (E) exceeds 1. In the absence of these findings, a coma is designated.[25] Ideally, GCS should be termed as the Consciousness Scale, with coma assigned only for cohorts with a GCS score less than 9.[29]
Other Issues
The reliability of the GCS has been extensively studied. Although its reproducibility has been questioned in a small number of reports, these have proved to be exceptions. A 2016 systematic review of all 53 published studies found that 85% of findings in higher-quality studies demonstrated substantial reliability, defined by a kappa statistic greater than 0.6.[39] The reproducibility of the total GCS score was also high, with a kappa greater than 0.6 in 77% of observations. An apparent beneficial effect on reliability was observed as a result of education and training. To promote this initiative, a standardized, structured assessment approach has been established.[8]
Alternatives to the GCS have been proposed, typically by simplifying its components or incorporating additional features. The Simplified Motor Scale, for example, recognizes only 3 levels of motor response. While this may suffice for binary clinical decisions, eg, whether to intubate, in prehospital and emergency settings, it does not outperform the GCS in predicting early mortality.[40][41] Scales with fewer components inevitably provide less information. They cannot match the GCS or GCS-P in distinguishing degrees of early severity, tracking individual patient progress, or correlating with diverse long-term outcomes.
More complex alternatives include the FOUR score, developed for neurological intensive care.[42] In addition to eye and motor responses adapted from the GCS, the FOUR score incorporates brainstem and respiratory components. While pupil reactivity, part of the brainstem evaluation, is a well-established prognostic indicator, the contributions of corneal and cough reflexes remain unclear. The respiratory subscale assesses breathing patterns but lacks consistency due to extracranial factors, sedation, and ventilatory technique. A systematic review has not compared the reliability and prognostic yield of the FOUR Score and the GCS score. Nevertheless, most studies have not shown a significant difference, and adding pupil response information to the GCS is expected to improve its performance relative to the FOUR score.[41][43] However, FOUR provides a more comprehensive neurological assessment, particularly in intubated patients in intensive care units.[44]
The Glasgow Coma Scale-Pupils-Age (GCS-PA) or Glasgow Coma Scale-Pupils-Age-CT (GCS-PA-CT) charts combine prognostic information from the GCS, pupil response, imaging findings, and the patient's age into a simple, easy-to-understand visual format.[42] They provide a user-friendly predictive tool that balances the simplicity and limited information of a "score" with the precision but greater complexity of multivariate models.
The GCS does not assess brainstem reflexes, which may delay recognition of herniation syndromes and brainstem injury. Subjectivity in the application of painful stimuli and the equal weighting of component scores can obscure critical neurologic changes. Awareness of these limitations can prompt supplemental assessments and training to improve reliability and patient safety.[29]
The GCS demonstrates face validity by formalizing responsiveness assessments that clinicians routinely perform in practice. Criterion validity remains lacking, as no universally accepted reference standard exists to confirm its accuracy; in fact, the GCS often serves as the reference against which other scales are compared. The scale shows moderate construct validity, evidenced by consistent correlations with both mortality and functional recovery outcomes. However, its content validity is limited, as the GCS does not capture the full range of central nervous system functions.[45]
Enhancing Healthcare Team Outcomes
Effective use of the GCS in clinical settings demands coordinated interprofessional strategies, clearly defined responsibilities, and consistent communication among healthcare professionals. Physicians, advanced practitioners, nurses, pharmacists, emergency medical technicians, and allied health staff all play critical roles in patient-centered care, especially when managing noncommunicative patients. Variability in pain stimulus techniques and inconsistent reporting formats compromise the reliability of GCS scores. International surveys have shown that at least 5 different painful stimuli are commonly used to assess motor responses, reducing comparability across assessments. Standardizing these practices through interprofessional education significantly enhances inter-rater reliability and clinician confidence in GCS use, thereby improving patient safety and outcome tracking.[46]
Every team member must understand the GCS and its clinical implications. Emergency medical technicians assess and communicate initial scores, setting the stage for urgent decision-making. Nurses and advanced practitioners document the eye, verbal, and motor components individually, followed by the total score, and record all findings in the electronic health record, including the date and time, for trend monitoring. Physicians interpret patterns, correlate GCS trends with diagnostic findings, and initiate appropriate airway, imaging, and transfer protocols. Pharmacists may contribute by advising on sedation regimens that could influence consciousness levels. Routine and consistent scoring facilitates timely neurosurgical consultations, escalates care when necessary, and facilitates discussions with patients’ families about prognosis. This collaborative, protocol-driven approach not only enhances team performance but also ensures safe, transparent, and patient-centered care.
Media
(Click Image to Enlarge)
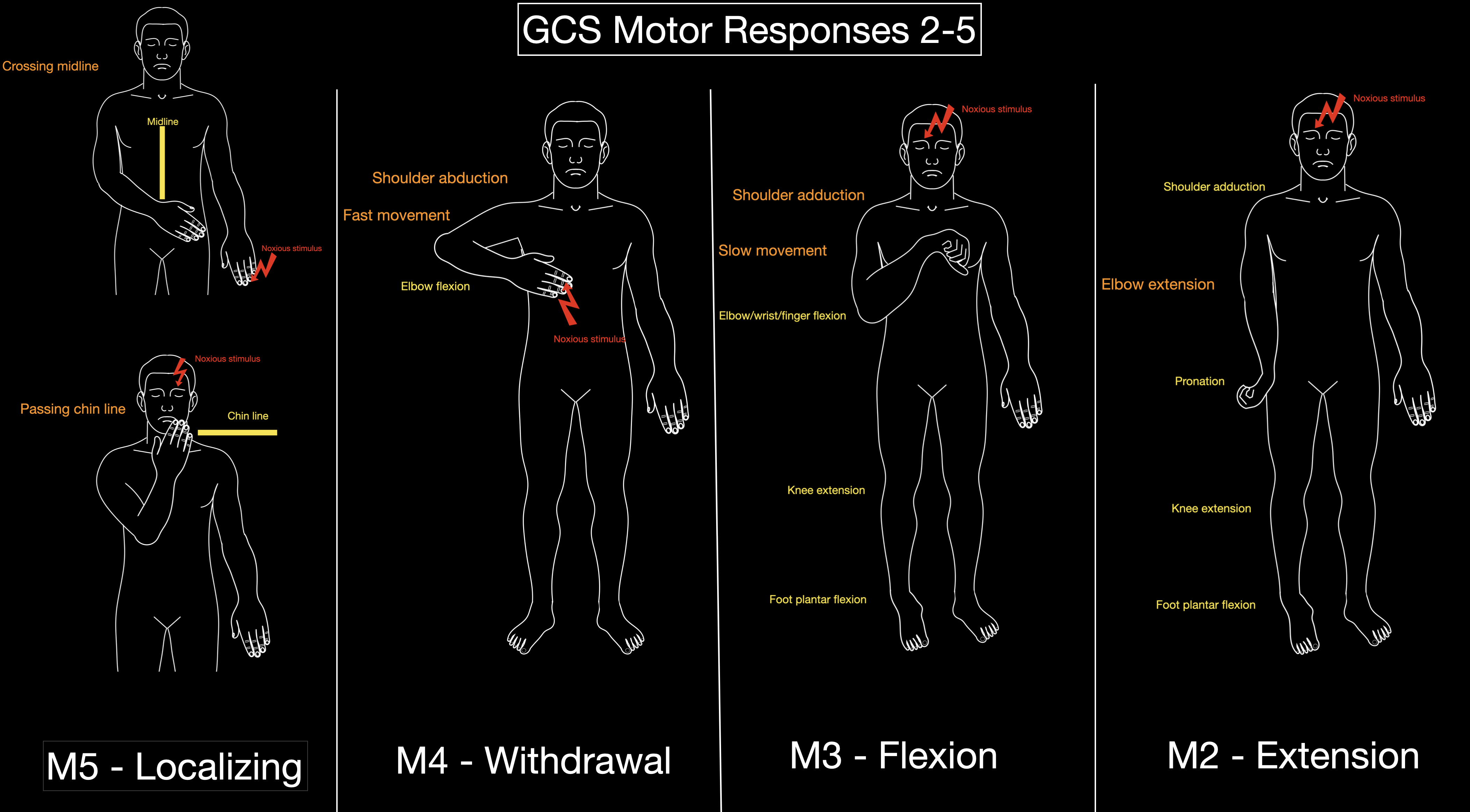
Glasgow Coma Scale Responses. Text in orange denotes key points to differentiate between the different GCS motor responses.
Contributed by K Margetis, MD, PhD
References
Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet (London, England). 1974 Jul 13:2(7872):81-4 [PubMed PMID: 4136544]
Mattei TA, Teasdale GM. The Story of the Development and Adoption of the Glasgow Coma Scale: Part I, The Early Years. World neurosurgery. 2020 Feb:134():311-322. doi: 10.1016/j.wneu.2019.10.193. Epub 2019 Nov 8 [PubMed PMID: 31712114]
Zhang JK, Dinh TU, Teasdale G, Mercier P, Mattei TA. The Message of the Glasgow Coma Scale: A Comprehensive Bibliometric Analysis and Systematic Review of Clinical Practice Guidelines Spanning the Past 50 years. World neurosurgery. 2024 May:185():393-402.e27. doi: 10.1016/j.wneu.2024.02.139. Epub 2024 Mar 2 [PubMed PMID: 38437980]
Level 1 (high-level) evidenceTeasdale G, Murray G, Parker L, Jennett B. Adding up the Glasgow Coma Score. Acta neurochirurgica. Supplementum. 1979:28(1):13-6 [PubMed PMID: 290137]
Wells AJ, Reilly PL. 50 Years of the Glasgow Coma Scale: A historical perspective. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2025 Mar:133():110994. doi: 10.1016/j.jocn.2024.110994. Epub 2025 Jan 5 [PubMed PMID: 39756098]
Level 3 (low-level) evidenceTeasdale GM, Drake CG, Hunt W, Kassell N, Sano K, Pertuiset B, De Villiers JC. A universal subarachnoid hemorrhage scale: report of a committee of the World Federation of Neurosurgical Societies. Journal of neurology, neurosurgery, and psychiatry. 1988 Nov:51(11):1457 [PubMed PMID: 3236024]
Level 3 (low-level) evidenceGrinnon ST, Miller K, Marler JR, Lu Y, Stout A, Odenkirchen J, Kunitz S. National Institute of Neurological Disorders and Stroke Common Data Element Project - approach and methods. Clinical trials (London, England). 2012 Jun:9(3):322-9. doi: 10.1177/1740774512438980. Epub 2012 Feb 27 [PubMed PMID: 22371630]
Teasdale G, Maas A, Lecky F, Manley G, Stocchetti N, Murray G. The Glasgow Coma Scale at 40 years: standing the test of time. The Lancet. Neurology. 2014 Aug:13(8):844-54. doi: 10.1016/S1474-4422(14)70120-6. Epub [PubMed PMID: 25030516]
Borgialli DA, Mahajan P, Hoyle JD Jr, Powell EC, Nadel FM, Tunik MG, Foerster A, Dong L, Miskin M, Dayan PS, Holmes JF, Kuppermann N, Pediatric Emergency Care Applied Research Network (PECARN). Performance of the Pediatric Glasgow Coma Scale Score in the Evaluation of Children With Blunt Head Trauma. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2016 Aug:23(8):878-84. doi: 10.1111/acem.13014. Epub 2016 Aug 1 [PubMed PMID: 27197686]
Reilly PL, Simpson DA, Sprod R, Thomas L. Assessing the conscious level in infants and young children: a paediatric version of the Glasgow Coma Scale. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 1988 Feb:4(1):30-3 [PubMed PMID: 3135935]
James HE. Neurologic evaluation and support in the child with an acute brain insult. Pediatric annals. 1986 Jan:15(1):16-22 [PubMed PMID: 3951884]
Schall JD. Neural basis of deciding, choosing and acting. Nature reviews. Neuroscience. 2001 Jan:2(1):33-42 [PubMed PMID: 11253357]
Esteban A, Traba A, Prieto J. Eyelid movements in health and disease. The supranuclear impairment of the palpebral motility. Neurophysiologie clinique = Clinical neurophysiology. 2004 Feb:34(1):3-15 [PubMed PMID: 15030796]
Garland EL. Pain processing in the human nervous system: a selective review of nociceptive and biobehavioral pathways. Primary care. 2012 Sep:39(3):561-71. doi: 10.1016/j.pop.2012.06.013. Epub 2012 Jul 24 [PubMed PMID: 22958566]
Nobre AC, Allison T, McCarthy G. Word recognition in the human inferior temporal lobe. Nature. 1994 Nov 17:372(6503):260-3 [PubMed PMID: 7969469]
Zenon A, Olivier E. Contribution of the basal ganglia to spoken language: is speech production like the other motor skills? The Behavioral and brain sciences. 2014 Dec:37(6):576; discussion 577-604. doi: 10.1017/S0140525X13004238. Epub [PubMed PMID: 25514965]
Booth JR, Wood L, Lu D, Houk JC, Bitan T. The role of the basal ganglia and cerebellum in language processing. Brain research. 2007 Feb 16:1133(1):136-44 [PubMed PMID: 17189619]
DiGiorgio AM, Wittenberg BA, Crutcher CL 2nd, Kennamer B, Greene CS, Velander AJ, Wilson JD, Tender GC, Culicchia F, Hunt JP. The Impact of Drug and Alcohol Intoxication on Glasgow Coma Scale Assessment in Patients with Traumatic Brain Injury. World neurosurgery. 2020 Mar:135():e664-e670. doi: 10.1016/j.wneu.2019.12.095. Epub 2019 Dec 24 [PubMed PMID: 31881342]
Brennan PM, Murray GD, Teasdale GM. A practical method for dealing with missing Glasgow Coma Scale verbal component scores. Journal of neurosurgery. 2021 Jul 1:135(1):214-219. doi: 10.3171/2020.6.JNS20992. Epub 2020 Sep 8 [PubMed PMID: 32898843]
Chendke P, Shah L, Badave A, Tamboli AA. Interobserver Variability of Both Glasgow Coma Scale and Full Outline of Unresponsiveness Scores in Forecasting the Results of Critically Ill Patients with Altered Sensorium. The Journal of the Association of Physicians of India. 2026 Feb:74(2):86-90. doi: 10.59556/japi.74.1360. Epub [PubMed PMID: 41818078]
van der Naalt J. [Physical diagnosis--the Glasgow coma scale for the measurement of disturbances of consciousness]. Nederlands tijdschrift voor geneeskunde. 2004 Mar 6:148(10):472-6 [PubMed PMID: 15042892]
Matis G, Birbilis T. The Glasgow Coma Scale--a brief review. Past, present, future. Acta neurologica Belgica. 2008 Sep:108(3):75-89 [PubMed PMID: 19115670]
Hession E, Broderick C, Foley J. Don't guess the GCS: a systems-based approach to safer neurological assessment in the emergency department. Irish journal of medical science. 2026 Feb 16:():. doi: 10.1007/s11845-026-04279-1. Epub 2026 Feb 16 [PubMed PMID: 41692919]
Cook NF, Braine ME, Trout R. Nurses' understanding and experience of applying painful stimuli when assessing components of the Glasgow Coma Scale. Journal of clinical nursing. 2019 Nov:28(21-22):3827-3839. doi: 10.1111/jocn.15011. Epub 2019 Sep 5 [PubMed PMID: 31343105]
Level 3 (low-level) evidenceBodien YG, Barra A, Temkin NR, Barber J, Foreman B, Vassar M, Robertson C, Taylor SR, Markowitz AJ, Manley GT, Giacino JT, Edlow BL, TRACK-TBI Investigators. Diagnosing Level of Consciousness: The Limits of the Glasgow Coma Scale Total Score. Journal of neurotrauma. 2021 Dec:38(23):3295-3305. doi: 10.1089/neu.2021.0199. Epub [PubMed PMID: 34605668]
Sewnarain K, Misser SK, Maharajh J, Nadvi SS. Score to scan: Is there a link between Glasgow Coma Scale score and CT neuroimaging findings in trauma? SA journal of radiology. 2026:30(1):3304. doi: 10.4102/sajr.v30i1.3304. Epub 2026 Feb 20 [PubMed PMID: 41810165]
Jiang Z, Ma J, Guo Z, Feng Q, Yuan H. Machine learning-based mortality prediction models for emergency department patients: a comparative analysis. Frontiers in medicine. 2026:13():1721101. doi: 10.3389/fmed.2026.1721101. Epub 2026 Jan 30 [PubMed PMID: 41695176]
Level 2 (mid-level) evidenceMunakomi S. A comparative study between Marshall and Rotterdam CT scores in predicting early deaths in patients with traumatic brain injury in a major tertiary care hospital in Nepal. Chinese journal of traumatology = Zhonghua chuang shang za zhi. 2016:19(1):25-7 [PubMed PMID: 27033268]
Level 2 (mid-level) evidenceAndraos C, Siddiqi A, Brazdzionis J, Siddiqi J. Limitations of the Glasgow Coma Scale: Challenges and Considerations. Cureus. 2025 Feb:17(2):e78900. doi: 10.7759/cureus.78900. Epub 2025 Feb 12 [PubMed PMID: 40091938]
Level 2 (mid-level) evidenceMegjhani M, Li Y, Grassi G, Alalqum T, Kwon SB, Zhou Z, Lau B, Jr ESC, Velazquez A, Ghoshal S, Roh DJ, Agarwal S, Claassen J, Park S. ICP-WAVES: Intracranial Pressure Waveform Analysis and Visualization for Enhanced Signal Processing. IEEE transactions on bio-medical engineering. 2026 Mar 3:PP():. doi: 10.1109/TBME.2026.3669377. Epub 2026 Mar 3 [PubMed PMID: 41774667]
Syed F, Hendi MF, Ghouse Mohammed N, Faoor Medhat Alrais Z, Sheikh W. Optic Nerve Sheath Diameter as a Prognostic Tool for Mortality in Intensive Care Unit Patients. Cureus. 2026 Jan:18(1):e100659. doi: 10.7759/cureus.100659. Epub 2026 Jan 3 [PubMed PMID: 41635345]
Reith FCM, Lingsma HF, Gabbe BJ, Lecky FE, Roberts I, Maas AIR. Differential effects of the Glasgow Coma Scale Score and its Components: An analysis of 54,069 patients with traumatic brain injury. Injury. 2017 Sep:48(9):1932-1943. doi: 10.1016/j.injury.2017.05.038. Epub 2017 Jun 1 [PubMed PMID: 28602178]
Ghaffarpasand F, Razmkon A, Dehghankhalili M. Glasgow Coma Scale Score in Pediatric Patients with Traumatic Brain Injury; Limitations and Reliability. Bulletin of emergency and trauma. 2013 Oct:1(4):135-6 [PubMed PMID: 27162843]
Brennan PM, Murray GD, Teasdale GM. Simplifying the use of prognostic information in traumatic brain injury. Part 1: The GCS-Pupils score: an extended index of clinical severity. Journal of neurosurgery. 2018 Jun:128(6):1612-1620. doi: 10.3171/2017.12.JNS172780. Epub 2018 Apr 10 [PubMed PMID: 29631516]
Reith FC, Van den Brande R, Synnot A, Gruen R, Maas AI. The reliability of the Glasgow Coma Scale: a systematic review. Intensive care medicine. 2016 Jan:42(1):3-15. doi: 10.1007/s00134-015-4124-3. Epub 2015 Nov 12 [PubMed PMID: 26564211]
Level 1 (high-level) evidenceKarabacak M, Jagtiani P, Dams-O'Connor K, Legome E, Hickman ZL, Margetis K. The MOST (Mortality Score for TBI): A novel prediction model beyond CRASH-Basic and IMPACT-Core for isolated traumatic brain injury. Injury. 2025 Jan:56(1):111956. doi: 10.1016/j.injury.2024.111956. Epub 2024 Oct 15 [PubMed PMID: 39428266]
Steyerberg EW, Mushkudiani N, Perel P, Butcher I, Lu J, McHugh GS, Murray GD, Marmarou A, Roberts I, Habbema JD, Maas AI. Predicting outcome after traumatic brain injury: development and international validation of prognostic scores based on admission characteristics. PLoS medicine. 2008 Aug 5:5(8):e165; discussion e165. doi: 10.1371/journal.pmed.0050165. Epub [PubMed PMID: 18684008]
Level 1 (high-level) evidenceMRC CRASH Trial Collaborators, Perel P, Arango M, Clayton T, Edwards P, Komolafe E, Poccock S, Roberts I, Shakur H, Steyerberg E, Yutthakasemsunt S. Predicting outcome after traumatic brain injury: practical prognostic models based on large cohort of international patients. BMJ (Clinical research ed.). 2008 Feb 23:336(7641):425-9. doi: 10.1136/bmj.39461.643438.25. Epub 2008 Feb 12 [PubMed PMID: 18270239]
Level 2 (mid-level) evidencePrasad K, Menon GR. Comparison of the three strategies of verbal scoring of the Glasgow Coma Scale in patients with stroke. Cerebrovascular diseases (Basel, Switzerland). 1998 Mar-Apr:8(2):79-85 [PubMed PMID: 9548004]
Haukoos JS, Gill MR, Rabon RE, Gravitz CS, Green SM. Validation of the Simplified Motor Score for the prediction of brain injury outcomes after trauma. Annals of emergency medicine. 2007 Jul:50(1):18-24 [PubMed PMID: 17113193]
Level 1 (high-level) evidenceTeasdale GM, Stocchetti N, Maas AI, Murray GD. Predicting Mortality in Critically Ill Patients. Critical care medicine. 2015 Oct:43(10):e471-2. doi: 10.1097/CCM.0000000000001153. Epub [PubMed PMID: 26376275]
Murray GD, Brennan PM, Teasdale GM. Simplifying the use of prognostic information in traumatic brain injury. Part 2: Graphical presentation of probabilities. Journal of neurosurgery. 2018 Jun:128(6):1621-1634. doi: 10.3171/2017.12.JNS172782. Epub 2018 Apr 10 [PubMed PMID: 29631517]
Ghelichkhani P, Esmaeili M, Hosseini M, Seylani K. Glasgow Coma Scale and FOUR Score in Predicting the Mortality of Trauma Patients; a Diagnostic Accuracy Study. Emergency (Tehran, Iran). 2018:6(1):e42 [PubMed PMID: 30584558]
Brun FK, Fagertun VH, Larsen MH, Solberg MT. Comparison of Glasgow Coma Scale and Full Outline of UnResponsiveness score to assess the level of consciousness in patients admitted to intensive care units and emergency departments: A quantitative systematic review. Australian critical care : official journal of the Confederation of Australian Critical Care Nurses. 2025 Jan:38(1):101057. doi: 10.1016/j.aucc.2024.03.012. Epub 2024 May 22 [PubMed PMID: 38777642]
Level 1 (high-level) evidenceGill MR, Reiley DG, Green SM. Interrater reliability of Glasgow Coma Scale scores in the emergency department. Annals of emergency medicine. 2004 Feb:43(2):215-23 [PubMed PMID: 14747811]
Reith FC, Brennan PM, Maas AI, Teasdale GM. Lack of Standardization in the Use of the Glasgow Coma Scale: Results of International Surveys. Journal of neurotrauma. 2016 Jan 1:33(1):89-94. doi: 10.1089/neu.2014.3843. Epub 2015 Aug 12 [PubMed PMID: 25951090]
Level 3 (low-level) evidence