Introduction
Galactorrhea is milk production from the breast unrelated to pregnancy or lactation. Milk production one year after cessation of breastfeeding is nonlactational and is considered galactorrhea. Various hormones, including prolactin, estrogens, and thyrotropin-releasing hormone (TRH), can affect the production of milk.[1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The various causes of galactorrhea broadly divide into hypothalamic-pituitary causes and non–hypothalamic-pituitary causes.
Hypothalamic-Pituitary Causes
- Prolactinomas: Prolactinomas are prolactin-secreting tumors and are the commonest hormone-secreting tumors of the pituitary glands. Prolactinomas that are less than 1 cm in size are known as microprolactinomas, whereas those greater than 1 cm in size are known as macroprolactinomas. Prolactin levels correlate well with tumor size, with microprolactinomas having levels greater than 200 ng/ml and macroprolactinomas having levels greater than 1000 ng/ml.
- Nonprolactin-secreting pituitary tumor and infiltrative disorders of the pituitary stalk/hypothalamus: These tumors can cause hyperprolactinemia by disrupting the flow of dopamine from the hypothalamus to the anterior pituitary by compressing the pituitary stalk. This disruption decreases prolactin inhibition, leading to mild hyperprolactinemia, usually less than 200 ng/ml.[2]
Non–Hypothalamic-Pituitary Causes
- Hypothyroidism: Elevated levels of TRH in hypothyroidism can stimulate the lactotrophs, resulting in hyperprolactinemia and galactorrhea.
- Medications: Several medications can cause hyperprolactinemia and galactorrhea. In most instances, prolactin levels are less than 200 ng/ml; however, atypical antipsychotics like risperidone are associated with prolactin levels greater than 200 ng/ml, which can be mistaken for a microprolactinoma. Atypical antipsychotics act on the dopamine (D2) receptors in the hypothalamic tuberoinfundibular areas to cause hyperprolactinemia. Risperidone is a combined dopamine-serotonin antagonist, which can significantly raise the prolactin levels. Clozapine, olanzapine, and aripiprazole have both agonist and antagonist properties on the D2 receptor and only transiently raise the prolactin levels. Metoclopramide and domperidone, which are used in the treatment of vomiting, are D2 receptor blockers and cause hyperprolactinemia. Tricyclic antidepressants (especially clomipramine) and monoamine-oxidase inhibitors have been associated with mild hyperprolactinemia. The mechanisms by which these medications cause hyperprolactinemia are unknown. Opioids, by acting through the µ receptors, decrease the release of hypothalamic dopamine and can elevate prolactin levels. Verapamil has also been associated with hyperprolactinemia by decreasing the production of hypothalamic dopamine.[3]
- Renal failure: Hyperprolactinemia in renal failure is due to the failure of the kidneys to clear prolactin. Prolactin levels of greater than 1000 mcg/L have been reported with renal failure. After kidney transplant, the hyperprolactinemia resolves rapidly within a few days.
- Chest wall lesions: Various chest wall lesions, including burns, surgeries, and herpes zoster, have associations with hyperprolactinemia. The hypothesis is that pain signals are transmitted to the hypothalamus via the spinal cord, resulting in decreased dopamine release and hyperprolactinemia.
- Idiopathic hyperprolactinemia: Occasionally, hyperprolactinemia with no known cause has been reported. These could be secondary to small undiagnosed microprolactinomas. The hyperprolactinemia self-resolves in one-third of patients and remains stable in half of the patients.[2]
Epidemiology
Hyperprolactinemia is more common in women. The prevalence of hyperprolactinemia ranges from 0.4% in an unselected normal adult population to as high as 9 to 17% in women with reproductive disorders. The prevalence was as high as 17% among women with polycystic ovary syndrome.[4]
Pathophysiology
Prolactin is responsible for the synthesis and secretion of milk. Prolactin is secreted by the lactotroph cells in the anterior pituitary. Dopamine secreted from the hypothalamus inhibits the secretion of prolactin. TRH and vasoactive intestinal polypeptide can stimulate prolactin secretion. Also, nipple stimulation, renal failure, chest wall lesions, and medications can cause hyperprolactinemia.[1][5]
Estrogens cause hyperprolactinemia by inhibiting hypothalamic dopamine and directly stimulating lactotrophs. In pregnancy, the high levels of estrogen cause lactotroph hyperplasia and can even result in the growth of a preexisting prolactinoma. Excess secretion of estrogen from ovaries in ovarian hyperstimulation syndrome has also been associated with hyperprolactinemia.[6][7]
History and Physical
Careful assessment of hyperprolactinemic-related symptoms, including menstrual irregularities, decreased libido, galactorrhea, erectile dysfunction, infertility, and gynecomastia, should be performed. Detailed medication history is important when considering medication-induced hyperprolactinemia. If a pituitary lesion is suspected, then evaluation for headaches and visual deficits is in order.
For assessing galactorrhea on physical exam, the patient needs to be sitting and leaning forward. The areola needs to be squeezed toward the nipple. The galactorrhea is usually bilateral and can be white or green. Bloody discharge could be due to breast tumors and will need further workup in that direction. A Sudan IV stain for fat droplets can confirm whether the discharge is milk.[2]
Evaluation
Prolactin levels should be measured at least once during the evaluation of hyperprolactinemia. Prolactin levels are measured using a sandwich ELISA assay, in which prolactin binds to both a capture and a detection antibody. Rarely, the hook effect may be seen in large prolactinomas with an extremely high prolactin level. Due to the extremely high prolactin levels, the number of prolactin molecules binding to both the capture and detection antibody is actually low. Diluting the sample to a 1:100 concentration and remeasuring it shows a paradoxical increase in prolactin level. The hook effect needs to be considered in large pituitary adenomas that present with galactorrhea and hypogonadism, but with only mildly elevated prolactin levels.[8][9]
Hormonal assessment of other pituitary hormones should be taken as indicated by the clinical history and exam. Magnetic resonance imaging (MRI) of the pituitary gland may reveal lesions that are responsible for hyperprolactinemia. Visual field assessment should be performed when the tumor contacts the optic chiasma on MRI.[2]
Treatment / Management
After ruling out breast pathologies, the therapy direction is toward the cause of hyperprolactinemia. Hyperprolactinemia is treated if there is a pituitary lesion or hypogonadism with problematic galactorrhea; if not troublesome, it can be monitored without therapy. The mainstay of hyperprolactinemia is treatment with bromocriptine or cabergoline. These are dopamine agonists that act on D2 receptors on lactotrophs and inhibit prolactin production. The doses for bromocriptine and cabergoline are 2.5 to 15 mg once daily and cabergoline 0.25 to 1 mg twice weekly, respectively. They are effective at normalizing prolactin levels and reducing tumor size. Adverse effects include nausea, vomiting, orthostatic hypotension, drowsiness, and headaches. Cardiac valvulopathy has been reported with high doses of cabergoline, and it is recommended to obtain an annual echocardiogram in patients taking more than 3.5 mg/week. In cases of medication-induced hyperprolactinemia, the offending medication should be stopped or changed to a different class. Use of dopamine agonists in these instances has associations with a slight risk of exacerbating the psychiatric disorder.
Normoprolactinemic galactorrhea occurs when the galactorrhea accompanies normal prolactin levels. If symptomatic with troublesome galactorrhea or menstrual cycle irregularities, it can be treated with dopamine agonists to obtain symptomatic relief. The treatment is tapered off once the galactorrhea has resolved.[1][2](A1)
Differential Diagnosis
The differential diagnosis includes:
- Acromegaly
- Breast stimulation
- Bronchogenic carcinoma
- Burns
- Breast surgery
- Craniopharyngioma
- Cushing disease
- Chest wall irritation
- Hypothyroidism
- Idiopathic
- Lymphoma
- Molar pregnancy
- Medications and herbal medications
- Pituitary adenomas
- Renal failure
- Sarcoidosis
- Tuberculosis
Enhancing Healthcare Team Outcomes
Galactorrhea is nonlactational production of milk. Prolactin, estrogens, and TRH all play a role in the production of milk from the breast. The condition is often managed by an interprofessional team consisting of a radiologist, endocrinologist, neurosurgeon, neurologist, and internist. The galactorrhea associated with hyperprolactinemia is often associated with symptoms of hypogonadism (decreased libido, erectile dysfunction, and menstrual irregularities), and thus a thorough medical history and physical exam are needed. Serosanguineous discharge from the breast should prompt further evaluation for breast pathologies. Inquiring of the patient about their current medications is vital. In most cases, treatment with dopamine agonists (cabergoline or bromocriptine) normalizes prolactin levels and results in shrinkage of the tumor.
Media
(Click Image to Enlarge)
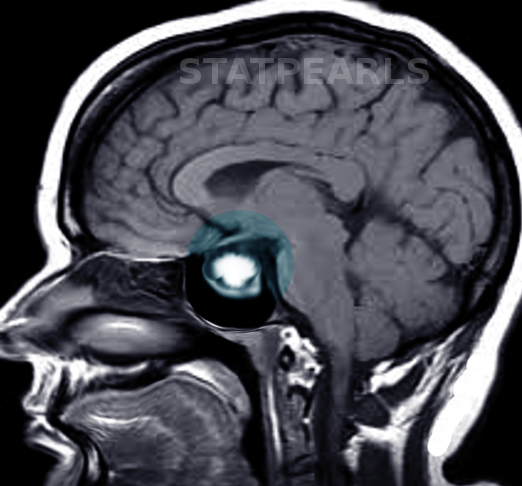
Prolactinoma. Magnetic resonance imaging demonstrates an enhancing lesion in the sella turcica.
Contributed by S Bhimji, MD
References
Huang W, Molitch ME. Evaluation and management of galactorrhea. American family physician. 2012 Jun 1:85(11):1073-80 [PubMed PMID: 22962879]
Melmed S, Casanueva FF, Hoffman AR, Kleinberg DL, Montori VM, Schlechte JA, Wass JA, Endocrine Society. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. The Journal of clinical endocrinology and metabolism. 2011 Feb:96(2):273-88. doi: 10.1210/jc.2010-1692. Epub [PubMed PMID: 21296991]
Level 1 (high-level) evidenceMolitch ME. Drugs and prolactin. Pituitary. 2008:11(2):209-18. doi: 10.1007/s11102-008-0106-6. Epub [PubMed PMID: 18404390]
Level 3 (low-level) evidenceVroonen L, Daly AF, Beckers A. Epidemiology and Management Challenges in Prolactinomas. Neuroendocrinology. 2019:109(1):20-27. doi: 10.1159/000497746. Epub 2019 Feb 7 [PubMed PMID: 30731464]
Freeman ME, Kanyicska B, Lerant A, Nagy G. Prolactin: structure, function, and regulation of secretion. Physiological reviews. 2000 Oct:80(4):1523-631 [PubMed PMID: 11015620]
Level 3 (low-level) evidenceChristin-Maître S, Delemer B, Touraine P, Young J. Prolactinoma and estrogens: pregnancy, contraception and hormonal replacement therapy. Annales d'endocrinologie. 2007 Jun:68(2-3):106-12 [PubMed PMID: 17540335]
Morel GR, Carón RW, Cónsole GM, Soaje M, Sosa YE, Rodríguez SS, Jahn GA, Goya RG. Estrogen inhibits tuberoinfundibular dopaminergic neurons but does not cause irreversible damage. Brain research bulletin. 2009 Dec 16:80(6):347-52. doi: 10.1016/j.brainresbull.2009.08.026. Epub 2009 Sep 8 [PubMed PMID: 19744546]
Level 3 (low-level) evidenceBarkan AL, Chandler WF. Giant pituitary prolactinoma with falsely low serum prolactin: the pitfall of the "high-dose hook effect": case report. Neurosurgery. 1998 Apr:42(4):913-5; discussion 915-6 [PubMed PMID: 9574657]
Level 3 (low-level) evidenceChahal J, Schlechte J. Hyperprolactinemia. Pituitary. 2008:11(2):141-6. doi: 10.1007/s11102-008-0107-5. Epub [PubMed PMID: 18404389]