Introduction
Frontal lobe syndrome is characterized by impairments in executive function, behavior, emotion, motivation, and personality resulting from damage to the frontal lobes, particularly the prefrontal cortex and its associated neural networks.[1][2][3] Although historically described following traumatic brain injury, most famously in the 1848 case of Phineas Gage, frontal lobe syndrome is now recognized as a network-based disorder arising from diverse etiologies, including cerebrovascular disease, neurodegeneration, neoplasms, infection, inflammation, and metabolic or toxic injury.[4][5] Clinical manifestations reflect disruption of frontal–subcortical circuits rather than isolated cortical lesions.
Anatomy
The frontal lobe, the largest cerebral lobe, lies anterior to the central sulcus and comprises the primary motor cortex, the supplementary and premotor cortices, and the prefrontal cortex. Injury to the motor and premotor regions produces contralateral weakness and impaired motor execution. The posteroinferior frontal gyrus of the dominant hemisphere (Broca area, Brodmann areas 44 and 45) mediates expressive language, and lesions result in nonfluent aphasia.[6][7]
The prefrontal cortex (PFC), the anterior-most region of the frontal lobe, serves as the neuroanatomical substrate for higher-order cognitive processes, including working memory, planning, decision-making, behavioral regulation, and social cognition (see Image. Prefrontal Cortex).[7] As a heteromodal association cortex, it integrates convergent input from all sensory modalities and maintains extensive reciprocal connections with limbic structures (eg, amygdala, hippocampus), the basal ganglia, and the thalamus. These interconnected pathways form parallel, functionally segregated frontal–subcortical circuits that support distinct cognitive, behavioral, and motivational domains. Emerging evidence emphasizes the role of frontal–limbic integration in decision-making and adaptive behavior, supporting the conceptualization of frontal lobe syndrome as a disorder of dysfunction in the frontal–subcortical network rather than as an isolated cortical injury.[8][9]
Functional Subdivisions of the Prefrontal Cortex
Key factors of the dorsolateral prefrontal cortex (DLPFC) include:
- The DLPFC originates in the dorsolateral prefrontal cortex and projects to the dorsolateral caudate, globus pallidus, and thalamus.
- Functions of this area include working memory, planning, cognitive flexibility, set-shifting, attention regulation, and problem solving.
- Lesions result in dysexecutive syndrome with impaired planning, reduced verbal fluency, poor working memory, and stimulus-bound behavior (may present with apathy and psychomotor slowing or "pseudo-depressive" syndrome.[10][11][12]
Key factors of the orbitofrontal cortex (OFC) include:
- The OFC receives input from the amygdala, hippocampus, and sensory association cortices and projects to the ventral striatum, mediodorsal thalamus, hypothalamus, and back to limbic structures (including the amygdala).
- Functions of the OFC include impulse control, judgment, social cognition, emotional regulation, and reward-based decision making.
- Lesions result in disinhibition syndrome, manifesting as impulsivity, tactlessness, emotional lability, and socially inappropriate behavior ("pseudo-psychopathic" or "frontal lobe personality").[13][14] Lateral OFC lesions have been correlated with OCD, depression, irritability, and mania.[15][16][14][17]
Key factors of the anterior cingulate cortex (ACC) include:
- The ACC comprises the anterior cingulate gyrus and the supplementary motor area and connects the amygdala, lateral hypothalamus, brainstem centers, hippocampus, and ventral striatum.
- Functions of the ACC include motivation, initiation of goal-directed behavior, error monitoring, emotional processing, and autonomic regulation.
- Lesions result in apathetic/akinetic syndrome, which manifests as profound apathy, abulia (loss of will), reduced spontaneous movement, and speech. Severe bilateral lesions produce akinetic mutism, in which patients are awake but lack voluntary movement or speech.[18][19][20]
Frontal–Subcortical Circuits
Frontal lobe syndrome is best conceptualized as a dysfunction of parallel frontal–subcortical circuits that connect the prefrontal cortex to the striatum, globus pallidus, substantia nigra, and thalamus (see Table 1). Lesions affecting cortical regions, subcortical nuclei, or connecting white matter tracts can produce similar clinical syndromes, explaining why caudate, thalamic, or basal ganglia lesions may mimic primary frontal cortical damage (“subcortical frontal syndrome”).[21][18]
Table 1. Frontal–Subcortical Circuits and Lesion Effects
|
Circuit |
Cortical origin |
Key Relay Structures |
Primary Function |
Lesion Manifestation |
|
Dorsolateral prefrontal |
DLPFC (Brodmann area 9, 46) |
Dorsolateral caudate → globus pallidus interna/substantia nigra pars reticulata → ventral anterior thalamus/mediodorsal thalamus |
Executive function |
Dysexecutive syndrome |
|
Orbitofrontal |
OFC (Brodmann area 11, 12, 47) |
Ventromedial caudate → globus pallidus interna/substantia nigra pars reticulata → mediodorsal thalamus |
Behavioral regulation |
Disinhibition syndrome |
|
Anterior cingulate |
ACC (Brodmann area 24, 32) |
Nucleus accumbens → Ventral pallidum → mediodorsal thalamus |
Motivation |
Apathy/akinetic mutism |
Natural History
The natural history of frontal lobe syndrome is etiology-dependent. Acute insults (stroke, traumatic brain injury, infection) may stabilize or demonstrate gradual improvement with targeted treatment and rehabilitation.[22] Neurodegenerative etiologies, particularly behavioral variant frontotemporal dementia (bvFTD), follow progressive decline over 6 to 11 years from symptom onset to death.[23][24] Tumor-related frontal lobe syndrome trajectories vary with histologic grade, location, and treatment response. Without appropriate intervention, frontal lobe syndrome typically results in progressive functional disability, social isolation, legal and financial complications, and substantial caregiver burden regardless of underlying etiology.[25]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Frontal lobe syndrome results from any process disrupting the prefrontal cortex or its connected circuits, including:
- Traumatic brain injury
- Cerebrovascular disease (ACA or frontal MCA territory infarcts)
- Neurodegenerative disorders (frontotemporal dementia, Alzheimer's disease) [24]
- Intracranial neoplasms (primary or metastatic)
- Idiopathic normal pressure hydrocephalus [26]
- Infectious or inflammatory conditions (eg, HSV encephalitis, neurosyphilis, HIV)
- Frontal lobe epilepsy
- Metabolic or toxic encephalopathies
- Iatrogenic injury (eg, neurosurgical intervention) [1][21][5]
Epidemiology
Because frontal lobe syndrome is a syndrome rather than a discrete disease, prevalence data are derived from underlying etiologies.
- Frontotemporal dementia: prevalence approximately 10 to 30 per 100,000; accounts for an estimated 20% of early-onset dementia (<65 years) [27][28][29]
- Traumatic brain injury: approximately 2.9 to 3.5 million emergency department visits annually in the United States; frontal involvement is common due to anatomical vulnerability [29][30]
- Stroke: frontal lobe involvement occurs in a substantial proportion of ACA and MCA infarcts; poststroke frontal dysfunction affects 20% to 40% of survivors [31][32]
Frontal lobe syndrome affects all age groups but is most commonly identified in middle-aged and older adults due to vascular and neurodegenerative causes.
Pathophysiology
Frontal lobe syndrome results from the disruption of distributed frontal–subcortical networks that mediate executive control, behavioral regulation, motivation, and emotional processing. These networks comprise parallel cortico–striato–pallido–thalamo–cortical loops linking the prefrontal cortex with the striatum, globus pallidus, substantia nigra, and thalamus.[33] Injury may occur at the cortical, subcortical, or white matter level, often producing clinically similar phenotypes through network disconnection rather than focal damage.[34]
Pathophysiologic mechanisms vary by etiology. Neurodegenerative disorders such as behavioral variant frontotemporal dementia involve abnormal protein aggregation (tau in MAPT mutations; TDP-43 in GRN and C9orf72 mutations), leading to progressive neuronal loss and synaptic dysfunction in frontal and anterior temporal regions.[35] Traumatic brain injury causes diffuse axonal injury with secondary inflammatory cascades.[36] Cerebrovascular insults produce ischemic neuronal injury, with strategically located infarcts in frontal–subcortical circuits yielding disproportionate deficits.[37] Neoplasms disrupt networks via mass effect, infiltration, edema, and seizure activity.[38]
Neuroimaging studies demonstrate that clinical manifestations correlate with the extent of network-level disconnection, supporting the view of frontal lobe syndrome as a disorder of distributed neural systems rather than of isolated regional pathology.[39]
Histopathology
The following histopathologic findings vary by etiology:
History and Physical
Clinical History
Patients typically present with behavioral, personality, or cognitive changes noted by family or caregivers. Impaired insight and anosognosia are common; therefore, collateral history is essential.[5]
History should establish baseline functioning and clarify the onset and progression of symptoms. Acute onset suggests vascular events such as stroke, traumatic brain injury, or seizures, whereas subacute progression raises concern for infection, neoplasm, or autoimmune encephalitis. An insidious onset is more consistent with neurodegenerative disease or chronic hydrocephalus.[5][42][43]
Core symptom domains include behavioral disinhibition, manifested by social inappropriateness, tactlessness, impulsivity, hypersexuality, criminal behavior, loss of manners, emotional lability, and irritability. Apathy and loss of motivation may present as reduced initiative, diminished interest in activities, emotional blunting, loss of empathy, and decreased spontaneous speech or movement. Executive dysfunction is common and includes impaired planning and organization, poor judgment, difficulty with multitasking, perseveration, stimulus-bound behavior, and reduced problem-solving ability. Reported memory complaints often reflect impaired encoding due to attentional deficits rather than primary amnestic processes. Language changes may include reduced speech output, echolalia, palilalia, stereotyped utterances, or semantic deterioration, particularly in semantic-variant primary progressive aphasia.[16][1][44]
Functional impact should be assessed through real-world consequences such as occupational decline, deterioration in interpersonal relationships, financial mismanagement, legal problems, driving impairment, and safety concerns. Additional history should include past medical conditions such as prior stroke, head trauma, seizures, psychiatric diagnoses, and substance use, a thorough medication review with attention to polypharmacy and anticholinergic burden, family history of early-onset dementia, psychiatric illness, or movement disorders; and relevant social history, including alcohol use, occupational exposures, and educational background.
Physical Examination
A comprehensive mental status and neurological examination is essential when evaluating suspected frontal lobe syndromes. Clinical manifestations span cognitive, behavioral, language, and motor domains, and may vary depending on the specific frontal–subcortical circuits involved.[1]
Cognitive and executive dysfunction is common and includes impaired planning, organization, and cognitive flexibility. Patients frequently demonstrate poor working memory, difficulty with multitasking, and reduced capacity for abstract reasoning. Executive testing may reveal impaired abstraction, decreased verbal fluency, difficulty with sequential motor tasks (eg, Luria 3-step test), and inaccurate cognitive estimates.[45]
Behavioral and psychiatric manifestations often predominate and may include disinhibition, impulsivity, apathy, or abulia. Patients may exhibit poor social judgment, socially inappropriate behavior, emotional dysregulation, distractibility, impersistence, and environmental dependency, including utilization behavior. Insight into deficits is frequently impaired, and anosognosia is common.[5][8]
Language and motor features depend on lesion laterality and extent. Clinical signs may include reduced speech output, perseveration, echolalia, dysarthria, hypophonia, or apraxia of speech. Expressive aphasia may occur with involvement of the dominant hemisphere. Motor findings can include impaired initiation of voluntary movement, contralateral weakness from primary motor cortex involvement, rigidity or bradykinesia due to subcortical pathology, and gait apraxia with medial frontal lesions. Abnormal eye movements, such as vertical gaze palsy, may suggest specific neurodegenerative etiologies, eg, progressive supranuclear palsy.[46][1]
Primitive (frontal release) reflexes, including the grasp, snout, glabellar (Myerson), and palmomental reflexes, may be present but have limited diagnostic specificity and can be observed in normal aging.[47]
Clinical presentations often overlap but may reflect disruption of distinct frontal-subcortical circuits, resulting in executive dysfunction, emotional or behavioral dysregulation, hypoemotional states characterized by apathy, or distress and anxiety syndromes.[45] A recognized phenomenon is the frontal lobe paradox, in which patients perform adequately on structured neuropsychological testing yet exhibit marked impairment in real-world functioning, reflecting a “knowing–doing dissociation.”[48]
Importantly, the neurological examination may be normal in early disease, particularly in behavioral variant frontotemporal dementia; therefore, an unremarkable physical examination does not exclude frontal lobe pathology.[5]
Evaluation
Diagnosis relies on clinical evaluation demonstrating characteristic executive dysfunction, behavioral disturbances, and personality changes consistent with frontal lobe pathology, supported by findings from neuroimaging and neuropsychological testing.[49]
Neuroimaging
Neuroimaging plays a central role in identifying structural or functional abnormalities associated with frontal lobe syndrome. Brain magnetic resonance imaging (MRI) with or without contrast remains the preferred modality and evaluates patterns of cerebral atrophy, including frontotemporal involvement in behavioral variant frontotemporal dementia and medial temporal atrophy in Alzheimer disease, along with mass lesions, vascular pathology, white matter disease, and hydrocephalus.[50][49]
Head computed tomography (CT) serves as an alternative in acute clinical settings and facilitates rapid identification of intracranial hemorrhage or large infarcts when MRI remains unavailable. Fluorodeoxyglucose positron emission tomography demonstrates frontal or anterior temporal hypometabolism in behavioral variant frontotemporal dementia when structural imaging fails to reveal diagnostic abnormalities.[50]
Neuropsychological Testing
Neuropsychological testing provides an objective assessment of executive dysfunction and functional impairment. Structured evaluation may reveal the “frontal lobe paradox,” in which preserved performance on formal testing contrasts with substantial impairment in real-world functioning.[1] Executive function tests commonly include the Wisconsin Card Sorting Test, Trail Making Test-B, Stroop test, verbal fluency tasks using phonemic or semantic categories, and the Tower of London task.[1]
Screening instruments, eg, the Montreal Cognitive Assessment, Frontal Assessment Battery, and Addenbrooke's Cognitive Examination-III, assist with the detection of cognitive deficits.[51] Behavioral assessment tools include the Frontal Behavioral Inventory, the Neuropsychiatric Inventory, and the Frontal Systems Behavior Scale.[52]
Laboratory Studies
Laboratory studies do not establish a diagnosis of frontal lobe syndrome but assist in identifying reversible or contributory conditions.[53] Routine screening commonly includes complete blood count, comprehensive metabolic panel, thyroid-stimulating hormone with free T4, vitamin B12 with or without methylmalonic acid, folate, rapid plasma reagin or VDRL testing, urinalysis, and urine drug screening. Additional investigations guided by clinical suspicion may include HIV testing, erythrocyte sedimentation rate or C-reactive protein, antinuclear antibodies or neuronal antibodies (eg, NMDA and LGI1), ceruloplasmin with urine copper measurement, very-long-chain fatty acids, and thiamine levels.[54]
Cerebrospinal Fluid
Cerebrospinal fluid analysis does not form part of routine evaluation but supports assessment when infection, inflammatory disease, autoimmune encephalitis, or diagnostic uncertainty arises.[55] Biomarker profiles may aid etiologic differentiation. Alzheimer disease often demonstrates decreased Aβ42 with increased total and phosphorylated tau. Frontotemporal dementia typically shows normal Aβ42 with normal or mildly elevated tau concentrations. Neurofilament light chain functions as a nonspecific biomarker of neurodegeneration.[56]
Genetic Testing
Genetic testing warrants consideration in patients with early disease onset before 65, positive family history, or atypical clinical presentations. Frequently implicated genes include C9orf72, MAPT, GRN, TARDBP, and FUS.[50]
Electroencephalography
Electroencephalography lacks a routine indication but assists in evaluation when seizures or autoimmune encephalitis are included in the differential diagnosis. Results are frequently normal or show nonspecific slowing.[57]
Treatment / Management
Management of frontal lobe syndrome requires an etiology-specific and interprofessional approach that addresses the underlying cause while mitigating cognitive, behavioral, and functional impairments.
Etiology-Specific Treatment
Treatments tailored to specific etiologies include:
- Stroke: reperfusion therapy when appropriate; secondary prevention
- Infections: antimicrobial therapy (acyclovir for HSV encephalitis, penicillin for neurosyphilis)
- Neoplasms: surgical resection, radiation, chemotherapy
- Normal pressure hydrocephalus: ventriculoperitoneal shunting [26]
- Autoimmune encephalitis: immunotherapy (eg, corticosteroids, IVIG, and plasmapheresis)
- Metabolic: thiamine replacement (Wernicke encephalopathy), copper chelation (Wilson disease)
- Neurodegenerative disease: no disease-modifying therapies exist; management focuses on symptomatic treatment.
Pharmacologic Management
Pharmacologic therapy targets predominant behavioral and motivational symptoms. However, no medications have received FDA approval specifically for frontal lobe syndrome. Medications for symptoms include:
- Behavioral symptoms (eg, disinhibition and agitation)
- First-line: SSRIs (sertraline, citalopram, escitalopram) show modest efficacy for behavioral symptoms in frontotemporal dementia [58]
- Second-line: trazodone 25 to 200 mg daily for agitation and sleep disturbance [58]
- Antipsychotics: reserved for severe, refractory symptoms due to limited efficacy and increased mortality risk in dementia; use the lowest dose for the shortest duration (quetiapine 25-100 mg, aripiprazole 2.5-10 mg) [59]
- Apathy
- Methylphenidate: 5-20 mg daily (often divided twice daily) may improve apathy; limited evidence [60]
- Contraindicated
- Cholinesterase inhibitors: may worsen behavioral symptoms in behavioral variant frontotemporal dementia
- Benzodiazepines: avoid due to cognitive worsening and fall risk
- Anticholinergic medications: worsen cognitive function
(A1)
Nonpharmacologic Interventions
Nonpharmacologic interventions form the foundation of management and address behavioral symptoms, safety concerns, and functional decline.[25][50] These therapies include:(A1)
- Behavioral and environmental strategies
- Structured daily routines
- Environmental modification to reduce stimulation and promote safety
- Redirection and distraction techniques
- Positive reinforcement
- Cognitive rehabilitation, eg, goal-directed training focused on compensatory strategies, use of external memory aids (calendars, lists, reminders)
- Physical/occupational therapy to maintain mobility, home safety evaluation, and fall prevention
- Speech-language pathology eg, communication strategies, swallowing evaluation
- Safety and legal considerations
- Driving: Assess driving safety; consider a formal evaluation. Patients with moderate-severe executive dysfunction should stop driving.
- Financial management: Implement protective measures (eg, a power of attorney, a representative payee).
- Advance care planning: Initiate early while the patient retains capacity.
- Caregiver support
- Essential components include education, behavioral management training, respite care, support groups, and connections to community resources
Differential Diagnosis
The differential diagnosis for frontal lobe syndrome is broad and includes:
- Psychiatric disorders: schizophrenia, bipolar disorder, major depression, personality disorders
- Other dementias: Alzheimer disease, dementia with Lewy bodies, vascular dementia
- Movement disorders: Parkinson disease with dementia, progressive supranuclear palsy, Huntington disease
- Structural lesions: subdural hematoma, hydrocephalus
- Infectious/inflammatory: encephalitis, autoimmune encephalitis
- Metabolic/toxic: vitamin deficiencies, thyroid disorders, medication effects, chronic alcohol use
- Other: epilepsy (frontal lobe epilepsy with interictal changes), chronic traumatic encephalopathy
Prognosis
Prognosis depends on etiology. Reversible causes (treated infections, resected tumors, corrected metabolic disorders, shunting for idiopathic normal pressure hydrocephalus) may show significant improvement. Traumatic brain injury recovery varies with injury severity, with younger age predicting better outcomes. Frontal stroke recovery occurs primarily within 3 to 6 months.[22] Frontotemporal dementia median survival is 6 to 11 years from symptom onset, with progressive functional decline.[23] Frontal lobe syndrome substantially impacts quality of life, relationships, and caregiver well-being regardless of etiology.[25]
Complications
Complications of frontal lobe syndromes are cause-specific. Progressive neurodegenerative disorders have social and behavioral complications requiring multifaceted support services for the patients and their families.
Deterrence and Patient Education
The most important aspect of treatment is patient and family education in patients affected by these syndromes. Patients suffer from cognitive, behavioral, and physical symptoms. Patients and their families need to be educated on the importance of providing supportive and safe environments for patients who will likely have a progressive decline in functional and cognitive abilities. Referrals to social work and other supportive services should be made early to help them cope with the changing needs of the patient.
Pearls and Other Issues
Frontal lobe syndrome is due to a broad array of pathologies ranging from trauma to neurodegenerative diseases. The most important clinical feature is the dramatic change in cognitive function (eg, executive processing), language, attention, and behavior.
Enhancing Healthcare Team Outcomes
Frontal lobe syndrome describes a clinical condition characterized by impairments in executive function, behavior, motivation, and personality resulting from disruption of frontal–subcortical networks involving the prefrontal cortex and associated circuits. Diverse etiologies may produce this syndrome, including traumatic brain injury, cerebrovascular disease, neurodegenerative disorders, neoplasms, infection, autoimmune disease, and metabolic or toxic injury. Clinical manifestations commonly include disinhibition, apathy, impaired judgment, executive dysfunction, and socially inappropriate behavior, often leading to significant functional impairment. Diagnosis relies on careful clinical assessment supported by neuroimaging, neuropsychological testing, and targeted laboratory studies. Management focuses on identifying and treating the underlying cause while addressing behavioral symptoms, functional decline, and safety concerns through pharmacologic and nonpharmacologic strategies.
Effective management requires coordinated interprofessional care. Physicians and advanced practitioners apply diagnostic expertise, interpret neuroimaging and cognitive assessments, and develop individualized treatment plans that address underlying etiologies and symptom management. Nurses monitor behavioral and cognitive changes, implement environmental and behavioral interventions, and identify safety concerns. Pharmacists review medication regimens to reduce polypharmacy and optimize pharmacologic treatment of behavioral symptoms. Social workers, therapists, and care coordinators support advance care planning, caregiver education, and access to community resources. Clear communication, shared decision-making, and coordinated care strategies strengthen patient-centered management, improve functional outcomes, reduce caregiver burden, and enhance overall team performance.
Media
(Click Image to Enlarge)
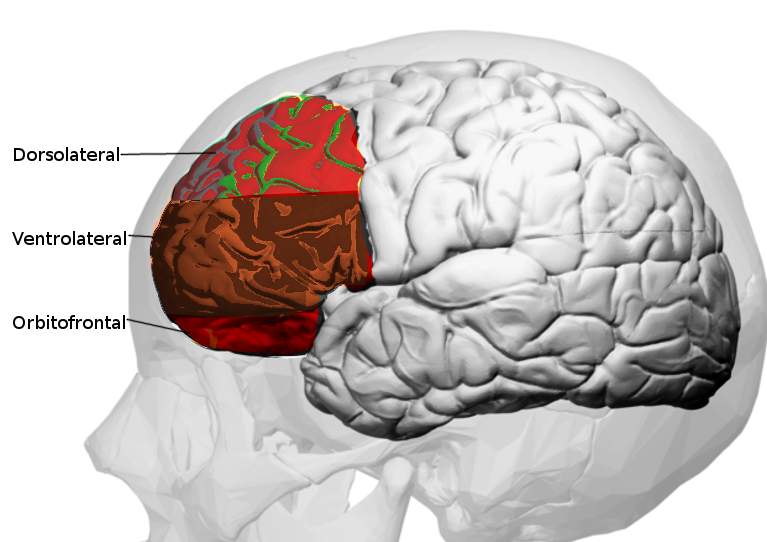
Prefrontal Cortex. The prefrontal cortex (PFC), the anterior-most region of the frontal lobe, serves as the neuroanatomical substrate for higher-order cognitive processes, including working memory, planning, decision-making, behavioral regulation, and social cognition.
Contributed by O Chaigasame, MD
References
. The frontal lobes and neuropsychiatric illness. The Journal of neuropsychiatry and clinical neurosciences. 1994 Fall:6(4):341-477 [PubMed PMID: 7841804]
Cao W, Li H, Luo J. Prefrontal cortical circuits in social behaviors: an overview. Journal of Zhejiang University. Science. B. 2024 Nov 15:25(11):941-955. doi: 10.1631/jzus.B2300743. Epub [PubMed PMID: 39626878]
Level 3 (low-level) evidenceLee S, Williams ZM. Role of Prefrontal Cortex Circuitry in Maintaining Social Homeostasis. Biological psychiatry. 2025 May 15:97(10):953-960. doi: 10.1016/j.biopsych.2024.07.007. Epub 2024 Jul 15 [PubMed PMID: 39019390]
Damasio H, Grabowski T, Frank R, Galaburda AM, Damasio AR. The return of Phineas Gage: clues about the brain from the skull of a famous patient. Science (New York, N.Y.). 1994 May 20:264(5162):1102-5 [PubMed PMID: 8178168]
Rascovsky K, Hodges JR, Knopman D, Mendez MF, Kramer JH, Neuhaus J, van Swieten JC, Seelaar H, Dopper EG, Onyike CU, Hillis AE, Josephs KA, Boeve BF, Kertesz A, Seeley WW, Rankin KP, Johnson JK, Gorno-Tempini ML, Rosen H, Prioleau-Latham CE, Lee A, Kipps CM, Lillo P, Piguet O, Rohrer JD, Rossor MN, Warren JD, Fox NC, Galasko D, Salmon DP, Black SE, Mesulam M, Weintraub S, Dickerson BC, Diehl-Schmid J, Pasquier F, Deramecourt V, Lebert F, Pijnenburg Y, Chow TW, Manes F, Grafman J, Cappa SF, Freedman M, Grossman M, Miller BL. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain : a journal of neurology. 2011 Sep:134(Pt 9):2456-77. doi: 10.1093/brain/awr179. Epub 2011 Aug 2 [PubMed PMID: 21810890]
Dronkers NF, Plaisant O, Iba-Zizen MT, Cabanis EA. Paul Broca's historic cases: high resolution MR imaging of the brains of Leborgne and Lelong. Brain : a journal of neurology. 2007 May:130(Pt 5):1432-41 [PubMed PMID: 17405763]
Level 3 (low-level) evidenceFridriksson J, den Ouden DB, Hillis AE, Hickok G, Rorden C, Basilakos A, Yourganov G, Bonilha L. Anatomy of aphasia revisited. Brain : a journal of neurology. 2018 Mar 1:141(3):848-862. doi: 10.1093/brain/awx363. Epub [PubMed PMID: 29360947]
Levy R, Dubois B. Apathy and the functional anatomy of the prefrontal cortex-basal ganglia circuits. Cerebral cortex (New York, N.Y. : 1991). 2006 Jul:16(7):916-28 [PubMed PMID: 16207933]
Aron AR, Robbins TW, Poldrack RA. Inhibition and the right inferior frontal cortex: one decade on. Trends in cognitive sciences. 2014 Apr:18(4):177-85. doi: 10.1016/j.tics.2013.12.003. Epub 2014 Jan 15 [PubMed PMID: 24440116]
D'Esposito M, Postle BR. The cognitive neuroscience of working memory. Annual review of psychology. 2015 Jan 3:66():115-42. doi: 10.1146/annurev-psych-010814-015031. Epub 2014 Sep 19 [PubMed PMID: 25251486]
Barbey AK, Koenigs M, Grafman J. Dorsolateral prefrontal contributions to human working memory. Cortex; a journal devoted to the study of the nervous system and behavior. 2013 May:49(5):1195-205. doi: 10.1016/j.cortex.2012.05.022. Epub 2012 Jun 16 [PubMed PMID: 22789779]
Joyce MKP, Uchendu S, Arnsten AFT. Stress and Inflammation Target Dorsolateral Prefrontal Cortex Function: Neural Mechanisms Underlying Weakened Cognitive Control. Biological psychiatry. 2025 Feb 15:97(4):359-371. doi: 10.1016/j.biopsych.2024.06.016. Epub 2024 Jun 27 [PubMed PMID: 38944141]
Owens AP, Allen M, Ondobaka S, Friston KJ. Interoceptive inference: From computational neuroscience to clinic. Neuroscience and biobehavioral reviews. 2018 Jul:90():174-183. doi: 10.1016/j.neubiorev.2018.04.017. Epub 2018 Apr 22 [PubMed PMID: 29694845]
Berlin HA, Rolls ET, Kischka U. Impulsivity, time perception, emotion and reinforcement sensitivity in patients with orbitofrontal cortex lesions. Brain : a journal of neurology. 2004 May:127(Pt 5):1108-26 [PubMed PMID: 14985269]
Berthier ML, Starkstein SE, Robinson RG, Leiguarda R. Limbic lesions in a patient with recurrent mania. The Journal of neuropsychiatry and clinical neurosciences. 1990 Spring:2(2):235-6 [PubMed PMID: 2136079]
Hoffmann M. The human frontal lobes and frontal network systems: an evolutionary, clinical, and treatment perspective. ISRN neurology. 2013:2013():892459. doi: 10.1155/2013/892459. Epub 2013 Mar 14 [PubMed PMID: 23577266]
Level 3 (low-level) evidenceGroman SM, Lee D, Taylor JR. Unlocking the reinforcement-learning circuits of the orbitofrontal cortex. Behavioral neuroscience. 2021 Apr:135(2):120-128. doi: 10.1037/bne0000414. Epub [PubMed PMID: 34060870]
Devinsky O, Morrell MJ, Vogt BA. Contributions of anterior cingulate cortex to behaviour. Brain : a journal of neurology. 1995 Feb:118 ( Pt 1)():279-306 [PubMed PMID: 7895011]
Bush G, Luu P, Posner MI. Cognitive and emotional influences in anterior cingulate cortex. Trends in cognitive sciences. 2000 Jun:4(6):215-222 [PubMed PMID: 10827444]
Myers DC, Simon J, Oh J, Kabotyanski KE, Fujimoto S, Oathes DJ, Rudebeck PH, Amemori KI, Sheth SA, Fudge JL. Circuit-Based Approaches to Understanding the Anterior Cingulate Cortex (ACC). The Journal of neuroscience : the official journal of the Society for Neuroscience. 2025 Nov 12:45(46):. doi: 10.1523/JNEUROSCI.1311-25.2025. Epub 2025 Nov 12 [PubMed PMID: 41224651]
Level 3 (low-level) evidenceCummings JL. Frontal-subcortical circuits and human behavior. Archives of neurology. 1993 Aug:50(8):873-80 [PubMed PMID: 8352676]
Cicerone KD, Langenbahn DM, Braden C, Malec JF, Kalmar K, Fraas M, Felicetti T, Laatsch L, Harley JP, Bergquist T, Azulay J, Cantor J, Ashman T. Evidence-based cognitive rehabilitation: updated review of the literature from 2003 through 2008. Archives of physical medicine and rehabilitation. 2011 Apr:92(4):519-30. doi: 10.1016/j.apmr.2010.11.015. Epub [PubMed PMID: 21440699]
Onyike CU, Diehl-Schmid J. The epidemiology of frontotemporal dementia. International review of psychiatry (Abingdon, England). 2013 Apr:25(2):130-7. doi: 10.3109/09540261.2013.776523. Epub [PubMed PMID: 23611343]
Barker MS, Manoochehri M, Huey ED. The Diagnostic Landscape of Behavioral Variant Frontotemporal Dementia. Rhode Island medical journal (2013). 2025 May 1:108(5):17-22 [PubMed PMID: 40300053]
Gitlin LN, Winter L, Dennis MP, Hodgson N, Hauck WW. A biobehavioral home-based intervention and the well-being of patients with dementia and their caregivers: the COPE randomized trial. JAMA. 2010 Sep 1:304(9):983-91. doi: 10.1001/jama.2010.1253. Epub [PubMed PMID: 20810376]
Level 1 (high-level) evidenceIshikawa M, Mori E, Kazui H. Gait and frontal lobe function become associated in patients with idiopathic normal pressure hydrocephalus after shunt surgery. Frontiers in neurology. 2025:16():1647707. doi: 10.3389/fneur.2025.1647707. Epub 2025 Oct 17 [PubMed PMID: 41180522]
Onyike CU, Huey ED. Frontotemporal dementia and psychiatry. International review of psychiatry (Abingdon, England). 2013 Apr:25(2):127-9. doi: 10.3109/09540261.2013.785169. Epub [PubMed PMID: 23611342]
Knopman DS, Roberts RO. Estimating the number of persons with frontotemporal lobar degeneration in the US population. Journal of molecular neuroscience : MN. 2011 Nov:45(3):330-5. doi: 10.1007/s12031-011-9538-y. Epub 2011 May 17 [PubMed PMID: 21584654]
Coyle-Gilchrist IT, Dick KM, Patterson K, Vázquez Rodríquez P, Wehmann E, Wilcox A, Lansdall CJ, Dawson KE, Wiggins J, Mead S, Brayne C, Rowe JB. Prevalence, characteristics, and survival of frontotemporal lobar degeneration syndromes. Neurology. 2016 May 3:86(18):1736-43. doi: 10.1212/WNL.0000000000002638. Epub 2016 Apr 1 [PubMed PMID: 27037234]
Pan X, Chen H, Bickerton WL, Lau JK, Kong AP, Rotshtein P, Guo A, Hu J, Humphreys GW. Preliminary findings on the reliability and validity of the Cantonese Birmingham Cognitive Screen in patients with acute ischemic stroke. Neuropsychiatric disease and treatment. 2015:11():2377-90. doi: 10.2147/NDT.S85698. Epub 2015 Sep 16 [PubMed PMID: 26396522]
Li JM, Long SS, Lu TX, Jiang YC, Zhang XW, Ren YQ. Psychiatric symptoms in stroke patients: Clinical features of depression and anxiety. World journal of psychiatry. 2025 Jun 19:15(6):103888. doi: 10.5498/wjp.v15.i6.103888. Epub 2025 Jun 19 [PubMed PMID: 40574782]
Masuccio FG, Grange E, Di Giovanni R, Rolla M, Solaro CM. Post-Stroke Depression in Older Adults: An Overview. Drugs & aging. 2024 Apr:41(4):303-318. doi: 10.1007/s40266-024-01104-1. Epub 2024 Feb 23 [PubMed PMID: 38396311]
Level 3 (low-level) evidenceHaber SN. Corticostriatal circuitry. Dialogues in clinical neuroscience. 2016 Mar:18(1):7-21 [PubMed PMID: 27069376]
Catani M, Dell'acqua F, Thiebaut de Schotten M. A revised limbic system model for memory, emotion and behaviour. Neuroscience and biobehavioral reviews. 2013 Sep:37(8):1724-37. doi: 10.1016/j.neubiorev.2013.07.001. Epub 2013 Jul 9 [PubMed PMID: 23850593]
Olney NT, Spina S, Miller BL. Frontotemporal Dementia. Neurologic clinics. 2017 May:35(2):339-374. doi: 10.1016/j.ncl.2017.01.008. Epub [PubMed PMID: 28410663]
Mckee AC, Daneshvar DH. The neuropathology of traumatic brain injury. Handbook of clinical neurology. 2015:127():45-66. doi: 10.1016/B978-0-444-52892-6.00004-0. Epub [PubMed PMID: 25702209]
Level 3 (low-level) evidenceCorbetta M, Siegel JS, Shulman GL. On the low dimensionality of behavioral deficits and alterations of brain network connectivity after focal injury. Cortex; a journal devoted to the study of the nervous system and behavior. 2018 Oct:107():229-237. doi: 10.1016/j.cortex.2017.12.017. Epub 2018 Jan 2 [PubMed PMID: 29357980]
Noll KR, Sullaway C, Ziu M, Weinberg JS, Wefel JS. Relationships between tumor grade and neurocognitive functioning in patients with glioma of the left temporal lobe prior to surgical resection. Neuro-oncology. 2015 Apr:17(4):580-7. doi: 10.1093/neuonc/nou233. Epub 2014 Sep 16 [PubMed PMID: 25227126]
Seeley WW. Mapping Neurodegenerative Disease Onset and Progression. Cold Spring Harbor perspectives in biology. 2017 Aug 1:9(8):. doi: 10.1101/cshperspect.a023622. Epub 2017 Aug 1 [PubMed PMID: 28289062]
Level 3 (low-level) evidenceLouis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, Hawkins C, Ng HK, Pfister SM, Reifenberger G, Soffietti R, von Deimling A, Ellison DW. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro-oncology. 2021 Aug 2:23(8):1231-1251. doi: 10.1093/neuonc/noab106. Epub [PubMed PMID: 34185076]
Wardlaw JM, Smith EE, Biessels GJ, Cordonnier C, Fazekas F, Frayne R, Lindley RI, O'Brien JT, Barkhof F, Benavente OR, Black SE, Brayne C, Breteler M, Chabriat H, Decarli C, de Leeuw FE, Doubal F, Duering M, Fox NC, Greenberg S, Hachinski V, Kilimann I, Mok V, Oostenbrugge Rv, Pantoni L, Speck O, Stephan BC, Teipel S, Viswanathan A, Werring D, Chen C, Smith C, van Buchem M, Norrving B, Gorelick PB, Dichgans M, STandards for ReportIng Vascular changes on nEuroimaging (STRIVE v1). Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. The Lancet. Neurology. 2013 Aug:12(8):822-38. doi: 10.1016/S1474-4422(13)70124-8. Epub [PubMed PMID: 23867200]
Bigler ED. Traumatic brain injury, neuroimaging, and neurodegeneration. Frontiers in human neuroscience. 2013:7():395. doi: 10.3389/fnhum.2013.00395. Epub 2013 Aug 6 [PubMed PMID: 23964217]
Fuster de Carulla JM. [Functions and diseases of the frontal lobe]. Anales de la Real Academia Nacional de Medicina. 1998:115(3):639-50 [PubMed PMID: 10208017]
Robert PH, Lafont V, Snowden JS, Lebert F. [Diagnostic criteria for fronto-temporal lobe degeneration]. L'Encephale. 1999 Nov-Dec:25(6):612-21 [PubMed PMID: 10668605]
Bonelli RM, Cummings JL. Frontal-subcortical circuitry and behavior. Dialogues in clinical neuroscience. 2007:9(2):141-51 [PubMed PMID: 17726913]
Level 3 (low-level) evidenceHöglinger GU, Respondek G, Stamelou M, Kurz C, Josephs KA, Lang AE, Mollenhauer B, Müller U, Nilsson C, Whitwell JL, Arzberger T, Englund E, Gelpi E, Giese A, Irwin DJ, Meissner WG, Pantelyat A, Rajput A, van Swieten JC, Troakes C, Antonini A, Bhatia KP, Bordelon Y, Compta Y, Corvol JC, Colosimo C, Dickson DW, Dodel R, Ferguson L, Grossman M, Kassubek J, Krismer F, Levin J, Lorenzl S, Morris HR, Nestor P, Oertel WH, Poewe W, Rabinovici G, Rowe JB, Schellenberg GD, Seppi K, van Eimeren T, Wenning GK, Boxer AL, Golbe LI, Litvan I, Movement Disorder Society-endorsed PSP Study Group. Clinical diagnosis of progressive supranuclear palsy: The movement disorder society criteria. Movement disorders : official journal of the Movement Disorder Society. 2017 Jun:32(6):853-864. doi: 10.1002/mds.26987. Epub 2017 May 3 [PubMed PMID: 28467028]
Plutino A, Baldinelli S, Fiori C, Ranaldi V, Silvestrini M, Luzzi S. Inter-rater reliability of primitive signs in dementia. Clinical neurology and neurosurgery. 2019 Dec:187():105555. doi: 10.1016/j.clineuro.2019.105555. Epub 2019 Oct 11 [PubMed PMID: 31639632]
Chaytor N, Schmitter-Edgecombe M. The ecological validity of neuropsychological tests: a review of the literature on everyday cognitive skills. Neuropsychology review. 2003 Dec:13(4):181-97 [PubMed PMID: 15000225]
Level 2 (mid-level) evidenceSeeley WW, Crawford RK, Zhou J, Miller BL, Greicius MD. Neurodegenerative diseases target large-scale human brain networks. Neuron. 2009 Apr 16:62(1):42-52. doi: 10.1016/j.neuron.2009.03.024. Epub [PubMed PMID: 19376066]
Bang J, Spina S, Miller BL. Frontotemporal dementia. Lancet (London, England). 2015 Oct 24:386(10004):1672-82. doi: 10.1016/S0140-6736(15)00461-4. Epub [PubMed PMID: 26595641]
Goldberg E, Bougakov D. Neuropsychologic assessment of frontal lobe dysfunction. The Psychiatric clinics of North America. 2005 Sep:28(3):567-80, 578-9 [PubMed PMID: 16122567]
Malloy P, Grace J. A review of rating scales for measuring behavior change due to frontal systems damage. Cognitive and behavioral neurology : official journal of the Society for Behavioral and Cognitive Neurology. 2005 Mar:18(1):18-27 [PubMed PMID: 15761273]
Ntymenou S, Tsantzali I, Kalamatianos T, Voumvourakis KI, Kapaki E, Tsivgoulis G, Stranjalis G, Paraskevas GP. Blood Biomarkers in Frontotemporal Dementia: Review and Meta-Analysis. Brain sciences. 2021 Feb 15:11(2):. doi: 10.3390/brainsci11020244. Epub 2021 Feb 15 [PubMed PMID: 33672008]
Level 1 (high-level) evidenceMcCollum L, Karlawish J. Cognitive Impairment Evaluation and Management. The Medical clinics of North America. 2020 Sep:104(5):807-825. doi: 10.1016/j.mcna.2020.06.007. Epub [PubMed PMID: 32773047]
Baldacci F, Mazzucchi S, Della Vecchia A, Giampietri L, Giannini N, Koronyo-Hamaoui M, Ceravolo R, Siciliano G, Bonuccelli U, Elahi FM, Vergallo A, Lista S, Giorgi FS, Hampel H. The path to biomarker-based diagnostic criteria for the spectrum of neurodegenerative diseases. Expert review of molecular diagnostics. 2020 Apr:20(4):421-441. doi: 10.1080/14737159.2020.1731306. Epub 2020 Feb 27 [PubMed PMID: 32066283]
Skillbäck T, Mattsson N, Blennow K, Zetterberg H. Cerebrospinal fluid neurofilament light concentration in motor neuron disease and frontotemporal dementia predicts survival. Amyotrophic lateral sclerosis & frontotemporal degeneration. 2017 Aug:18(5-6):397-403. doi: 10.1080/21678421.2017.1281962. Epub 2017 Feb 6 [PubMed PMID: 28631955]
Jenssen S. Electroencephalogram in the dementia workup. American journal of Alzheimer's disease and other dementias. 2005 May-Jun:20(3):159-66 [PubMed PMID: 16003931]
Tsai RM, Boxer AL. Treatment of frontotemporal dementia. Current treatment options in neurology. 2014 Nov:16(11):319. doi: 10.1007/s11940-014-0319-0. Epub [PubMed PMID: 25238733]
Maust DT, Kim HM, Seyfried LS, Chiang C, Kavanagh J, Schneider LS, Kales HC. Antipsychotics, other psychotropics, and the risk of death in patients with dementia: number needed to harm. JAMA psychiatry. 2015 May:72(5):438-45. doi: 10.1001/jamapsychiatry.2014.3018. Epub [PubMed PMID: 25786075]
Padala PR, Padala KP, Lensing SY, Ramirez D, Monga V, Bopp MM, Roberson PK, Dennis RA, Petty F, Sullivan DH, Burke WJ. Methylphenidate for Apathy in Community-Dwelling Older Veterans With Mild Alzheimer's Disease: A Double-Blind, Randomized, Placebo-Controlled Trial. The American journal of psychiatry. 2018 Feb 1:175(2):159-168. doi: 10.1176/appi.ajp.2017.17030316. Epub 2017 Sep 15 [PubMed PMID: 28945120]
Level 1 (high-level) evidence