 Anatomy, Abdomen and Pelvis: Foramen of Winslow (Omental Foramen, Epiploic Foramen)
Anatomy, Abdomen and Pelvis: Foramen of Winslow (Omental Foramen, Epiploic Foramen)
Introduction
The foramen of Winslow constitutes the only natural communication between the greater and lesser sacs of the peritoneal cavity. The caudate lobe of the liver marks the superior boundary, and the 1st part of the duodenum forms the inferior border. The hepatoduodenal ligament, the free edge of the lesser omentum containing the hepatic portal vein, hepatic artery, and common bile duct, forms the anterior boundary. The inferior vena cava constitutes the posterior border.[1] Also referred to as the “epiploic foramen” or “omental foramen,” this structure was first described by Jacob Winslow in his 1732 publication, "Exposition anatomique de la structure du corps humain" (see Image. Foramen of Winslow).[2]
Jacob Winslow, born in Denmark and later naturalized as a French citizen, converted to Catholicism. Winslow is regarded alongside William Cheselden in London and Alexander Monro in Edinburgh as a leading anatomist of the 18th century. His publication is notable for reliance solely on direct anatomical observation rather than the opinions of contemporaneous anatomists. Winslow subsequently held the position of professor of anatomy at the Jardin du Roi in Paris.[3][4] He also provided the first description of the foramen spinosum at the skull base.
The foramen of Winslow carries clinical importance as a potential site of internal herniation and an access point for rapid hepatic inflow control. Mastery of the boundaries and adjacent structures of this foramen enables accurate identification during operative and diagnostic procedures. Familiarity with the anatomic relationships surrounding the region enhances surgical safety and improves recognition of pathology.
Embryology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Embryology
The embryonic foregut is suspended from the abdominal wall by ventral and dorsal mesentery. The liver develops within the ventral mesentery. The portion of the ventral mesentery between the liver and abdominal wall persists in the mature fetus as the falciform ligament. The segment of the ventral mesentery between the stomach and liver persists as the lesser omentum, including the hepatogastric and hepatoduodenal ligaments.
The part of the dorsal mesentery attached to the stomach persists as the greater omentum. The stomach shifts to the right during the first 90° of intestinal rotation, carrying the lesser omentum. The right side of the stomach and the lesser omentum lie against the posterior abdominal wall without fusion. The space posterior to the stomach constitutes the lesser sac.
Subsequent counterclockwise rotation of the midgut by 180° occurs around the axis of the superior mesenteric artery. The 3rd portion of the duodenum extends transversely across the peritoneal cavity, posterior to the superior mesenteric artery. This section of the duodenum and the pancreas becomes secondarily retroperitoneal, forming the posterior wall of the lesser sac.
The transverse colon also crosses the peritoneal cavity transversely but lies anterior to the superior mesenteric artery. Attachment of the greater omentum to the transverse colon completes the separation of the lesser sac from the greater sac, leaving only the small window at the free distal margin of the hepatoduodenal ligament, the foramen of Winslow.[5]
Surgical Considerations
Identification of the foramen of Winslow in the operating room is straightforward due to the pliability of viable tissue. Identification in stiff, nonpliable fixed tissue in the dissecting laboratory presents greater difficulty.
Localization of the foramen begins at the hepatogastric ligament. Following the lesser curvature of the stomach distally leads to the pylorus, where the lesser omentum becomes the hepatoduodenal ligament. Tracing the duodenum distally to the termination of the hepatoduodenal ligament permits insertion of a finger along the free edge of the ligament into the foramen of Winslow.
The cystic duct may be followed to the junction with the common hepatic duct, which continues along the course of the common bile duct within the hepatoduodenal ligament toward the foramen of Winslow. Mobilization of the hepatic flexure of the colon allows the 2nd portion of the duodenum to be traced proximally to the 1st portion of the duodenum, forming the inferior boundary of the foramen of Winslow.[6][7]
Clinical Significance
The foramen of Winslow is clinically notable for 2 reasons. First, the foramen constitutes a potential site for internal herniation, although hernias in this location are exceedingly rare.[8][9] Presenting symptoms typically reflect intermittent bowel obstruction and are nonspecific. Prior to the advent of modern imaging, diagnosis was frequently established only during laparotomy, and delays contributed to significant mortality. Computed tomography now facilitates diagnosis. Management consists of hernia reduction, with or without resection of nonviable viscera. Laparoscopic repair has also been reported.
The hepatic artery, portal vein, and common bile duct pass through the hepatoduodenal ligament immediately adjacent to the foramen of Winslow. This proximity allows rapid control of hepatic inflow in cases of uncontrolled hepatic hemorrhage. Insertion of the forefinger through the foramen permits compression of the vessels between the thumb and finger. For increased stability, 1 jaw of a vascular clamp may be placed through the foramen to compress the hepatic artery and portal vein.
Both techniques represent variations of the Pringle maneuver, first described by James Hogarth Pringle in 1908.[10] Pringle, born in Australia of Scottish descent, trained at the University of Edinburgh and was appointed surgeon at the Royal Infirmary of Glasgow in 1896. He gained recognition for the management of fractures, traumatic injuries, and radical amputations. Pringle’s 1908 publication, "Notes on the Arrest of Hepatic Hemorrhage due to Trauma," established him as a pioneer in trauma surgery.
Other Issues
The foramen of Winslow constitutes a distinct anatomical structure. Formation of this feature is readily explained by embryologic development. The foramen represents a rare site of clinical concern for the surgeon and serves as a notable landmark for identification in the dissection laboratory.
Media
(Click Image to Enlarge)
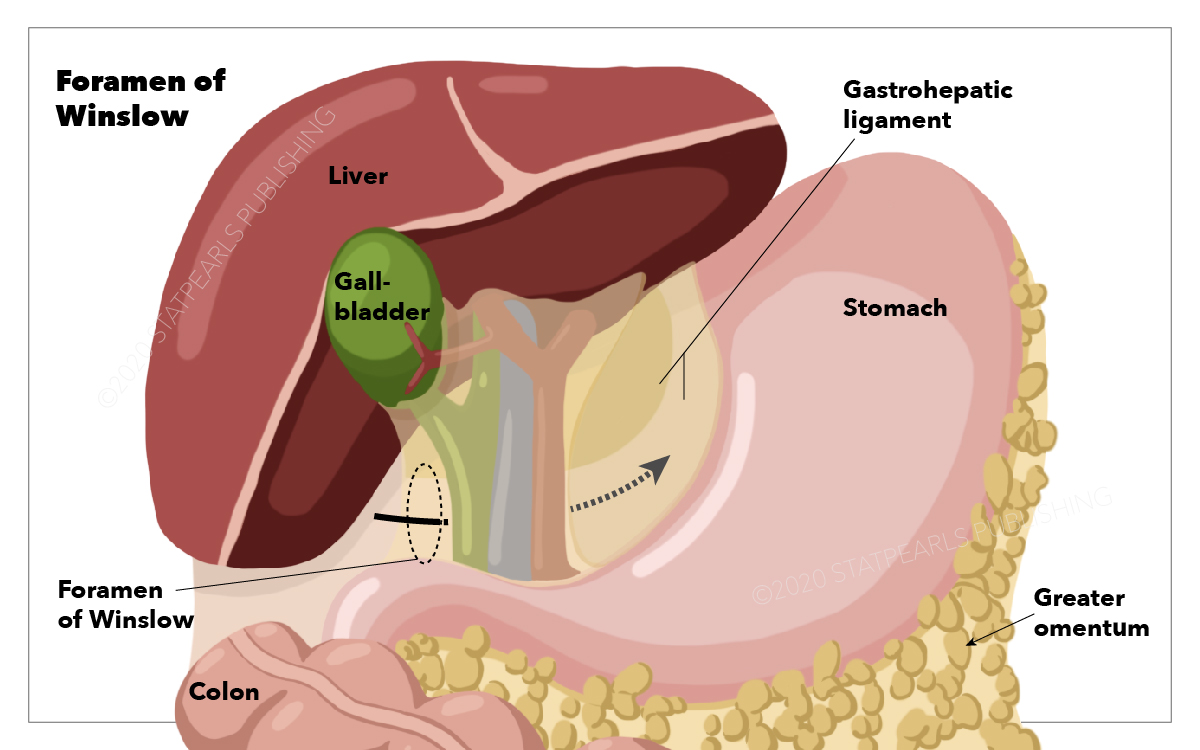
Foramen of Winslow. Relevant abdominal and pelvic structures include the foramen of Winslow, gastrohepatic ligament, greater omentum, gallbladder, liver, colon, and stomach.
StatPearls Publishing Illustration
References
Elmohr MM, Blair KJ, Menias CO, Nada A, Shaaban AM, Sandrasegaran K, Elsayes KM. The Lesser Sac and Foramen of Winslow: Anatomy, Embryology, and CT Appearance of Pathologic Processes. AJR. American journal of roentgenology. 2020 Oct:215(4):843-851. doi: 10.2214/AJR.19.22749. Epub 2020 Aug 12 [PubMed PMID: 32783559]
Saad TC. Jacob Winslow (1669-1760): The surprising legacy of an anatomist. Journal of medical biography. 2021 Aug:29(3):124-131. doi: 10.1177/0967772019858244. Epub 2019 Sep 2 [PubMed PMID: 31475885]
Bellary SS, Walters A, Gielecki J, Shoja MM, Tubbs RS, Loukas M. Jacob B. Winslow (1669-1760). Clinical anatomy (New York, N.Y.). 2012 Jul:25(5):545-7. doi: 10.1002/ca.22033. Epub 2012 Jan 31 [PubMed PMID: 22294452]
Ellis H. Jacob Winslow: distinguished Danish anatomist. British journal of hospital medicine (London, England : 2005). 2019 Apr 2:80(4):232. doi: 10.12968/hmed.2019.80.4.232. Epub [PubMed PMID: 30951411]
Malone JC, Arbor TC, Shah AB. Embryology, Midgut. StatPearls. 2026 Jan:(): [PubMed PMID: 31985949]
Krishnan A, Mackay TG, Iyengar K, Joel A. Unveiling the Foramen of Winslow: A Case Report of Internal Hernia and Its Surgical Implications. Cureus. 2025 Aug:17(8):e90562. doi: 10.7759/cureus.90562. Epub 2025 Aug 20 [PubMed PMID: 40978989]
Level 3 (low-level) evidenceDowns P, Downes N, Zayshlyy E, Esper C, Giuseppucci P. Internal hernia through the foramen of Winslow. Journal of surgical case reports. 2018 Dec:2018(12):rjy329. doi: 10.1093/jscr/rjy329. Epub 2018 Dec 11 [PubMed PMID: 30555674]
Level 3 (low-level) evidenceJansen YJL, Nieboer K, Senesael E, Van Bael K, Allaeys M. Internal herniation through the foramen of Winslow: a case report. Acta chirurgica Belgica. 2020 Apr:120(2):136-138. doi: 10.1080/00015458.2018.1515396. Epub 2018 Oct 4 [PubMed PMID: 30284522]
Level 3 (low-level) evidenceHuh CW, Kim JS, Kim BW. Endoscopic reduction of gastric antrum herniation through the foramen of Winslow into the lesser sac. Digestive endoscopy : official journal of the Japan Gastroenterological Endoscopy Society. 2018 Jan:30(1):122-123. doi: 10.1111/den.12974. Epub 2017 Nov 9 [PubMed PMID: 29055109]
van Gulik TM. James Hogarth Pringle and his time-honored maneuver. Hepatobiliary surgery and nutrition. 2024 Jun 1:13(3):391-392. doi: 10.21037/hbsn-24-271. Epub 2024 May 24 [PubMed PMID: 38911209]