 Anatomy, Bony Pelvis and Lower Limb: Foot and Ankle
Anatomy, Bony Pelvis and Lower Limb: Foot and Ankle
Introduction
The foot is a complex anatomical structure composed of numerous bones, joints, ligaments, muscles, and tendons that enable the coordinated movements required for gait and maintenance of an upright posture (see Image. Lateral Aspect of the Right Foot and Ankle). By definition, the foot is the portion of the lower extremity distal to the ankle joint, also known as the tibiotalar joint. The ankle joint is formed by the articulation of the talus with the mortise created by the distal tibia and fibula.
The foot contains 26 bones, including the tarsals, metatarsals, and phalanges, which are subdivided into 3 groups: the hindfoot, midfoot, and forefoot. The hindfoot is composed of the talus and calcaneus and serves as the primary weight-bearing component of the foot. The midfoot consists of the navicular, cuboid, and cuneiform bones. The forefoot contains the metatarsals and phalanges. Articular surfaces are covered by articular cartilage. Joint capsules and ligaments support the joints and provide stability.
The foot contains 19 intrinsic muscles, while additional extrinsic muscles originating in the leg contribute to foot and ankle movement. Tendons attach these muscles to the osseous structures. Innervation and vascular supply are similarly complex. Major arterial structures include the anterior tibial, posterior tibial, and fibular (peroneal) arteries. Each artery gives rise to numerous branches.
Major nerves supplying the foot and ankle include the tibial nerve, which gives rise to the medial (MPN) and lateral (LPN) plantar nerves, as well as the deep and superficial fibular (peroneal), sural, and saphenous nerves, each with multiple branches. Subcutaneous fat, fascia, and skin complete the anatomical components of the foot and ankle.
Acute trauma, chronic repetitive injury, and degenerative or inflammatory arthropathies are common causes of presentation to emergency departments and primary care providers. Inadequate treatment may result in chronic disability.[1][2][3]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The ankle, or tibiotalar joint, forms the junction between the lower leg and the foot. Osseous components of the ankle joint include the distal tibia, distal fibula, and talus. Together, the distal tibia and fibula form an osseoligamentous recess, commonly referred to as the "ankle mortise," which receives the trochlea (talar dome) of the talus.
The distal tibia contributes to the tibial plafond, the horizontal articular surface that articulates with the superior surface of the talus. The medial malleolus, a projection of the distal tibia, forms the medial wall of the ankle mortise. In contrast, the distal fibula forms the lateral malleolus, which stabilizes the lateral aspect of the ankle joint. The talar dome constitutes the superior articular surface of the talus and fits within the mortise formed by the tibia and fibula.
Ligamentous structures and joint capsules provide substantial stability to the ankle joint. Medial ligaments are collectively referred to as the "deltoid ligament complex," which consists of superficial and deep components. The superficial layer includes the tibionavicular, tibiocalcaneal, tibiospring, and superficial posterior tibiotalar ligaments, whereas the deep layer contains the anterior and posterior tibiotalar ligaments. The deltoid ligament complex stabilizes the medial ankle and resists excessive eversion.
The distal tibiofibular syndesmosis lies superior to the ankle joint and is composed of the anterior inferior and posterior inferior tibiofibular ligaments, the interosseous ligament, and the interosseous membrane. Injury to these structures results in a so-called "high ankle sprain." Lower lateral ligaments include the anterior talofibular, posterior talofibular, and calcaneofibular ligaments. Lower lateral ligaments, particularly the anterior talofibular and calcaneofibular ligaments, are injured more frequently.[4][5][6]
Anatomical structures distal to the ankle joint comprise the foot, which contains 26 bones: 7 tarsals, 5 metatarsals, and 14 phalanges. Structurally, the foot is divided into 3 regions: the hindfoot, midfoot, and forefoot.
The hindfoot, comprising the posterior portion of the foot, consists of the talus and calcaneus, 2 of the 7 tarsal bones. These bones articulate at the subtalar joint, which includes anterior, middle, and posterior facets between the talus and calcaneus. The posterior subtalar articulation constitutes the largest component of this joint. The subtalar joint permits inversion and eversion of the hindfoot, movements essential for adaptation to uneven surfaces during gait.[7]
The midfoot consists of 5 tarsal bones: navicular, cuboid, and the medial, intermediate, and lateral cuneiforms. Articulation between the hindfoot and midfoot forms the transverse tarsal (Chopart) joint, composed of the talonavicular and calcaneocuboid joints. The navicular articulates distally with the 3 cuneiform bones, whereas the cuboid articulates distally with the bases of the 4th and 5th metatarsals. The plantar calcaneonavicular (spring) ligament complex, together with the tibialis posterior tendon, contributes substantially to the stability of the medial longitudinal arch (MLA). The spring ligament complex comprises 3 components: the superomedial, medial plantar oblique, and inferior plantar longitudinal ligaments.[8][9]
The forefoot is the most anterior region of the foot and includes the metatarsals, phalanges (toes), and sesamoid bones. Each digit generally contains 1 metatarsal and 3 phalanges in the absence of developmental fusion anomalies, except for the great toe, which contains only 2 phalanges. Articulation between the midfoot and forefoot forms the Lisfranc joint. The 3 cuneiforms articulate with the bases of the 1st, 2nd, and 3rd metatarsals, whereas the cuboid articulates with the bases of the 4th and 5th metatarsals. The intermediate cuneiform is the smallest cuneiform, allowing keystone interlocking of the 2nd metatarsal at the Lisfranc joint and contributing to stability.
The Lisfranc ligament complex consists of 3 components—dorsal, interosseous, and plantar—which connect the base of the 2nd metatarsal to the medial cuneiform. Injury to the Lisfranc ligament complex may result in midfoot instability and, if left untreated, chronic deformity with progression to a neuropathic joint. In addition to the Lisfranc ligament complex, intertarsal and intermetatarsal ligaments contribute to the stability of the midfoot and forefoot.
Structurally, the foot is often described as consisting of medial and lateral columns. The medial column includes the talus, navicular, cuneiforms, and 1st through 3rd metatarsals. This column demonstrates greater mobility, contributing to shock absorption. The lateral column is composed of the calcaneus, cuboid, and the 4th and 5th metatarsals and provides greater structural stability during stance and propulsion. Metatarsophalangeal (MTP) joints play a critical role in balance, weight-bearing, and propulsion during gait. Plantar aspects of these joints are reinforced by fibrocartilaginous structures known as plantar plates, which contribute to joint stability. Injury to the capsuloligamentous structures of the 1st MTP joint is commonly referred to as "turf toe."[10]
Muscles and tendons are primarily responsible for coordinated movement of the osseous structures of the foot and ankle and serve a secondary role in stabilizing osseous and ligamentous anatomy. Muscles and tendons are discussed in greater detail in a later section. The complex anatomy of the foot and ankle, together with the remainder of the lower limb, functions to support body weight and enable locomotion efficiently. The foot serves as a platform for stance, a shock absorber during gait impact, and a lever for propulsion during stepping.
Gait consists of repetitive cycles divided into a stance phase, during which the foot remains in contact with the ground, and a swing phase, during which the foot advances through the air. The stance phase typically includes initial contact, loading response, midstance, terminal stance, and pre-swing, whereas the swing phase consists of initial swing, mid-swing, and terminal swing. During running, a flight (float) phase occurs in which neither foot contacts the ground.[11]
At initial contact, the heel typically strikes the ground with the foot in a relatively supinated position, creating a more rigid structure that facilitates controlled load acceptance. The foot pronates during the loading response and midstance phases, allowing increased mobility at the subtalar and midtarsal joints, enabling adaptation to the supporting surface and shock absorption.
The foot progressively resupinates during terminal stance and pre-swing, converting into a rigid lever for propulsion. The transverse tarsal (Chopart) joint becomes more stable with subtalar supination, whereas the tarsometatarsal (Lisfranc) joint complex provides structural stability with limited motion. MTP joints, particularly the hallux, dorsiflex during push-off and contribute to the windlass mechanism, tightening the plantar fascia and elevating the MLA.
Load shifts primarily to the medial forefoot during propulsion, particularly the 1st metatarsal and hallux, which play key roles in forward propulsion. The lateral column of the foot, including the calcaneus, cuboid, and 4th and 5th metatarsals, contributes to stability during stance and assists in load distribution. Coordinated interaction of the midfoot, tarsometatarsal joints, and MTP joints enables the foot to function as an efficient lever for propulsion during gait.[12]
Embryology
Development of the appendicular skeleton occurs primarily between weeks 4 and 8 of gestation. Limb development begins with the appearance of limb buds, which form as swellings on the ventrolateral body wall. Limb buds arise from proliferating mesenchyme derived from the somatic layer of the lateral plate mesoderm and are covered by ectoderm. Limb outgrowth is regulated by signaling from the apical ectodermal ridge and mediated largely through fibroblast growth factors, which direct growth in a proximal-to-distal sequence. Lower limb buds appear shortly after upper limb buds, around the end of the 4th week of development. The distal portion of the limb bud expands to form the foot plate by approximately 4.5 weeks of gestation. Shortly thereafter, digital rays develop within the foot plate, marking the future toes.
Cartilaginous bone models arise from mesenchymal condensations, representing the early stage of skeletogenesis. Initially, developing skeletal elements consist of hyaline cartilage models formed through chondrification of mesenchymal tissue. These cartilage templates subsequently undergo endochondral ossification, during which bone gradually replaces cartilage to form the mature skeletal structures of the foot. Separation of the toes occurs through programmed cell death (apoptosis) within the interdigital tissue, producing distinct digits. Major skeletal components of the foot and ankle are established by the end of the 8th week of development, although ossification and further morphological refinement continue throughout fetal development and into postnatal life.[13][14]
Blood Supply and Lymphatics
The arterial supply of the foot is derived primarily from the anterior and posterior tibial arteries. After crossing the ankle joint, the anterior tibial artery continues as the dorsalis pedis artery, which supplies the dorsum of the foot. The dorsalis pedis gives rise to several branches, including the lateral tarsal, medial tarsal, and arcuate arteries. The arcuate artery courses laterally across the dorsum of the foot and gives rise to dorsal metatarsal arteries, which subsequently divide into dorsal digital arteries supplying the toes.
On the plantar aspect of the foot, the posterior tibial artery divides into the medial and lateral plantar arteries after passing posterior and inferior to the medial malleolus (see Image. Arteries and Muscles of the Plantar Surface). The lateral plantar artery courses across the sole of the foot and forms the plantar arterial arch, which is completed by the deep plantar branch of the dorsalis pedis artery. From this arch arise the plantar metatarsal arteries, which divide into plantar digital arteries supplying the toes.
The fibular artery, a branch of the tibiofibular trunk, courses within the deep posterior compartment of the leg along the fibula and contributes to the vascular supply of the ankle and hindfoot. Near the distal tibiofibular syndesmosis, the fibular artery gives rise to a perforating branch that passes to the anterior aspect of the ankle and anastomoses with branches of the anterior tibial artery. Additional branches include the lateral malleolar and calcaneal branches, which contribute to the arterial network supplying the lateral ankle and heel.[15]
Lymphatic drainage of the foot occurs through superficial and deep lymphatic systems. Superficial lymphatic vessels drain the skin and subcutaneous tissues and generally accompany the superficial veins. Medial foot lymphatics follow the great saphenous vein and drain into the superficial inguinal lymph nodes, whereas lateral foot lymphatics accompany the small saphenous vein and typically drain first into the popliteal lymph nodes before reaching the deep inguinal nodes. Deep lymphatic vessels accompany the anterior tibial, posterior tibial, and fibular arteries, draining deeper structures of the foot and ankle into the popliteal lymph nodes, with subsequent drainage to the deep inguinal and external iliac lymph nodes.[16]
Nerves
The nerves supplying the foot and ankle arise primarily from branches of the tibial, common fibular, femoral, and sciatic nerves. Principal nerves of the foot include the saphenous, superficial and deep fibular, medial and lateral plantar, sural, and calcaneal nerves.
The saphenous nerve, a terminal branch of the femoral nerve, provides cutaneous innervation to the medial ankle and medial border of the foot, extending distally to approximately the level of the 1st MTP joint. The superficial fibular nerve, a branch of the common fibular nerve, supplies motor innervation to the fibularis longus and brevis muscles in the leg and provides cutaneous innervation to most of the dorsum of the foot and dorsal surfaces of the toes. Sensation in the 1st interdigital cleft (between the hallux and 2nd toe) is supplied by the deep fibular nerve. The deep fibular nerve, also arising from the common fibular nerve, supplies the extensor digitorum brevis and extensor hallucis brevis muscles on the dorsum of the foot and provides sensory innervation to the skin of the 1st dorsal web space.[17]
The tibial nerve divides within the tarsal tunnel, beneath the flexor retinaculum, into the MPN and LPN, which provide primary innervation to the plantar foot. The MPN travels deep to the abductor hallucis muscle and divides into the common and proper plantar digital nerves. The nerve's motor fibers supply the abductor hallucis, flexor hallucis brevis (FHB), flexor digitorum brevis (FDB), and the 1st lumbrical. The sensory fibers provide cutaneous innervation to the medial plantar foot and the medial 3-1/2 digits. The LPN courses obliquely across the sole between the FDB and quadratus plantae and divides into superficial and deep branches. The nerve's motor branches supply the abductor digiti minimi (ADM), flexor digiti minimi brevis (FDMB), quadratus plantae, adductor hallucis, the lateral 3 lumbricals, and the plantar and dorsal interossei. Sensory innervation includes the lateral plantar surface of the foot and the lateral 1-1/2 digits.
The sural nerve, formed from contributions of the tibial and common fibular nerves, provides cutaneous innervation to the posterolateral leg, the lateral ankle, and the lateral aspect of the foot. Calcaneal nerves supply the skin of the heel. Medial calcaneal branches arise from the tibial nerve, whereas lateral calcaneal branches arise from the sural nerve.[18]
Muscles
Muscles acting on the foot are classified as extrinsic and intrinsic. Approximately 29 muscles contribute to foot movement, including 10 extrinsic muscles originating in the leg and 19 intrinsic muscles located entirely within the foot. Extrinsic muscles generate the primary movements of the ankle and foot, whereas intrinsic muscles contribute mainly to fine motor control, stabilization of the arches, and toe movements.
Extrinsic Muscles
The extrinsic muscles originate in the leg and act on the foot through long tendons (see Image. Tendons of the Extrinsic Foot Muscles). The organization of these muscles follows the compartments of the leg.
The anterior compartment contains the primary dorsiflexors of the ankle, including the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and fibularis (peroneus) tertius. These muscles produce ankle dorsiflexion and assist in toe extension.
The lateral compartment contains the fibularis (peroneus) longus and brevis. These muscles primarily evert the foot and contribute weakly to ankle plantarflexion.
The deep posterior compartment includes the tibialis posterior, flexor digitorum longus (FDL), and flexor hallucis longus. These muscles pass posterior to the medial malleolus beneath the flexor retinaculum and contribute to plantarflexion and inversion of the foot, while also assisting with toe flexion and supporting the MLA. The space along the posteromedial ankle, deep to the flexor retinaculum, is commonly referred to as the "tarsal tunnel."
The superficial posterior compartment contains the gastrocnemius, soleus, and plantaris muscles. These muscles unite to form the calcaneal (Achilles) tendon, which inserts on the posterior surface of the calcaneus (calcaneal tubercle). These muscles provide the primary force for ankle plantarflexion during gait and propulsion.
Intrinsic Muscles
Intrinsic muscles originate and insert within the foot. Primary functions include fine motor control of the toes and stabilization of the arches.
Muscles of the hallux
Muscles associated with the hallux (great toe) include the abductor hallucis, FHB, and adductor hallucis. The abductor hallucis originates from the medial process of the calcaneal tuberosity and the plantar aponeurosis and inserts on the medial aspect of the base of the proximal phalanx of the hallux. Functions include abduction of the great toe and support of the MLA. The FHB originates from the cuboid and lateral cuneiform bones and inserts via 2 tendons on the base of the proximal phalanx of the hallux, with sesamoid bones often embedded within the tendons. Function includes flexion of the MTP joint of the hallux.
The adductor hallucis consists of 2 heads (see Image. Plantar Foot Anatomy, Third Layer). The oblique head originates from the bases of the 2nd through 4th metatarsals, whereas the transverse head arises from the plantar ligaments of the lateral MTP joints. Both heads insert on the lateral aspect of the base of the proximal phalanx of the hallux, producing adduction of the great toe and stabilization of the transverse arch of the foot. Distal tendinous expansions of these muscles contribute to the plantar plate.
Muscles of the central toes
Intrinsic muscles associated with the central digits include the lumbricals, quadratus plantae, FDB, and the dorsal and plantar interossei. The lumbricals originate from the tendons of the FDL and insert into the extensor expansions of digits 2 through 5. The functions of these muscles include flexion of the MTP joints and extension of the interphalangeal joints. The quadratus plantae originates from the medial and lateral surfaces of the calcaneus and inserts into the tendon of the FDL, assisting toe flexion by redirecting the pull of the FDL tendon. The FDB originates from the medial process of the calcaneal tuberosity and inserts onto the middle phalanges of digits 2 through 5, producing flexion at the proximal interphalangeal joints. The dorsal and plantar interossei originate from the metatarsals. Dorsal interossei abduct the toes (DAB), whereas plantar interossei adduct the toes (PAD) relative to the 2nd digit. Additionally, these muscles assist in MTP flexion and interphalangeal extension.
Muscles of the little toe
Muscles associated with the 5th digit include the ADM, FDMB, and opponens digiti minimi. The ADM originates from the calcaneal tuberosity and plantar aponeurosis and inserts on the base of the proximal phalanx of the 5th digit, producing abduction of the little toe. The FDMB originates from the base of the 5th metatarsal and inserts on the base of the proximal phalanx of the 5th digit, producing flexion at the MTP joint. The opponens digiti minimi, when present, originates from the long plantar ligament and cuboid and inserts along the 5th metatarsal, contributing to stabilization and slight opposition of the 5th digit.
Physiologic Variants
Numerous anatomic variants of the foot and ankle have been described. Many of these variants are incidental findings of limited clinical significance, whereas others may predispose to pain, deformity, or biomechanical dysfunction. Variants commonly involve accessory ossicles, accessory muscles, and variations in skeletal alignment. Familiarity with these variations is essential to avoid misinterpretation as pathological conditions and identify variants that may contribute to disease.
Accessory Ossicles
An ongoing debate exists regarding the origin of accessory ossicles. Some evidence suggests that many are congenital developmental variants, whereas others may arise from ununited secondary ossification centers or remote traumatic events.
Common accessory ossicles of the foot and ankle include the os trigonum, accessory navicular (os naviculare), os peroneum, os supranaviculare, and os intermetatarseum. The os trigonum, located posterior to the talus, may contribute to posterior ankle impingement (os trigonum syndrome), particularly during repetitive plantarflexion activities such as ballet dancing, soccer, sprinting, or basketball.
The accessory navicular is classified into 3 recognized types, as follows:
- Type I: A small sesamoid bone within the posterior tibialis tendon
- Type II: A larger ossicle connected to the navicular by fibrocartilage; the most commonly symptomatic variant, often associated with posterior tibial tendon dysfunction
- Type III: A fused or enlarged navicular tuberosity.
Surgical excision of the accessory ossicle may be considered in cases where symptoms persist despite conservative treatment. An additional, less commonly discussed variant is a fibrocartilaginous node, which is a nonossified variant of the os naviculare that may be identified on magnetic resonance imaging (MRI) and mistaken for tendinosis.
The os peroneum is located within the fibularis longus tendon along the plantar lateral aspect of the cuboid in the region of the cuboid tunnel and may be associated with fibularis longus tendinopathy or tendon tears. Painful pathology in this region is referred to as "painful os peroneum syndrome," encompassing disorders related to the os peroneum, including avascular necrosis, fracture, and diastasis.
Other accessory ossicles may mimic fractures on imaging. The os intermetatarseum may be mistaken for the fleck sign associated with Lisfranc injury, whereas the os supranaviculare may resemble a dorsal capsular avulsion fracture of the navicular.[19][20][21][22]
Sesamoid Bones
Sesamoid bones differ from accessory ossicles in that they are embedded within tendons and function to modify tendon biomechanics, reduce friction, and increase mechanical advantage. The most prominent sesamoids are the medial and lateral sesamoid bones of the hallux, located within the tendons of the FHB at the 1st MTP joint. These sesamoids are present in nearly all individuals. Sesamoids associated with the lesser MTP joints occur less frequently. Hallux sesamoids may appear bipartite or multipartite, representing a normal anatomical variant that must be distinguished from sesamoid fractures or fragmentation associated with avascular necrosis.[23][24][25]
Accessory Muscles
Accessory muscles of the foot and ankle most commonly occur around the ankle and hindfoot. Frequently described variants include the fibularis quartus, accessory soleus, and flexor digitorum accessorius longus. The fibularis quartus muscle lies within the retromalleolar region adjacent to the fibular tendons and may cause crowding within the fibular tendon sheath. Although typically asymptomatic, the fibularis quartus may be mistaken for fibular tendon tears on imaging or contribute to tendon pathology through mass effect. The accessory soleus muscle, when present, occupies the posteromedial ankle region and may produce swelling or pain, particularly in young athletes. The flexor digitorum accessorius longus passes through the tarsal tunnel beneath the flexor retinaculum and may compress the tibial nerve, contributing to tarsal tunnel syndrome, a compressive neuropathy characterized by pain, paresthesia, and burning sensations along the medial ankle and plantar surface of the foot.[26][27]
Osseous Variants and Bipartite Bones
Osseous variants may occur as tarsal coalitions or bipartite bones. The most common tarsal coalitions include the talocalcaneal and calcaneonavicular coalitions. These structures may be fibrous, cartilaginous, or osseous. Fibrous and cartilaginous coalitions may function as pseudoarticulations and may produce pain or restricted motion. Osseous coalitions may alter hindfoot biomechanics and lead to rigid flatfoot deformity or early degenerative changes. Radiographic signs have been described for these conditions. The “C-sign” on lateral radiographs may indicate a talocalcaneal coalition involving the middle subtalar facet. Incomplete or fibrous coalitions may be difficult to detect on plain radiographs and are often better visualized using computed tomography (CT) or MRI. A calcaneonavicular coalition may present with an elongated anterior process of the calcaneus articulating or fusing with the navicular. The characteristic radiographic appearance is the “anteater sign,” most clearly seen on oblique foot radiographs.
Bipartite bones result from the incomplete fusion of ossification centers during development. The bipartite medial cuneiform is a common example and is usually an incidental and asymptomatic finding.[28][29]
Variations in Foot Alignment
Variations in foot alignment may be congenital or acquired. Common examples include pes cavus (high arch), pes planus (flatfoot), hindfoot valgus, and hallux valgus. Acquired pes planus and midfoot collapse are frequently associated with posterior tibial tendon dysfunction and insufficiency of the spring (plantar calcaneonavicular) ligament, both of which play important roles in the maintenance of the MLA. Hallux valgus represents malalignment of the 1st ray, characterized by lateral deviation of the hallux and medial deviation of the 1st metatarsal. This deformity may lead to forefoot widening, altered weight distribution, bunion formation, and degenerative joint disease.
Clinical Significance
Tarsal Tunnel Syndrome
Tarsal tunnel syndrome is a compressive neuropathy of the tibial nerve or its branches within the tarsal tunnel, located along the posteromedial aspect of the ankle. Clinical presentation typically includes pain, numbness, or paresthesia involving the heel, plantar surface of the foot, and toes. Physical examination may demonstrate a positive Tinel sign, characterized by paresthesias elicited by percussion over the tibial nerve within the tarsal tunnel.
The tarsal tunnel is bounded by the flexor retinaculum (roof) and the medial surfaces of the talus, calcaneus, and distal tibia (floor). Structures traversing the tunnel include the tibialis posterior tendon, FDL tendon, posterior tibial artery and veins, tibial nerve, and flexor hallucis longus tendon.
Although many cases are idiopathic, secondary causes include ganglion cysts, varicosities, tenosynovitis, tumors, accessory muscles, and fracture deformities. Initial management typically involves conservative treatment, including anti-inflammatory medications, physical therapy, orthotics, and image-guided injections. Surgical decompression may be considered in refractory cases, particularly when a structural cause of nerve compression is identified.[30]
Os Trigonum Syndrome
Os trigonum syndrome is also referred to as "posterior ankle impingement syndrome." The condition is classically described in ballet dancers but may occur in any individual performing repetitive plantarflexion, including soccer players. Os trigonum syndrome is usually unilateral, although bilateral cases have been reported. Clinical presentation typically includes posterior ankle pain exacerbated by plantarflexion. Predisposing factors include an elongated Stieda process, an os trigonum, prior fracture of the posterior process of the talus, or posterior talar process morphology variants. Most patients respond to conservative management, including rest, ice, anti-inflammatory medication intake, or injections.[31][32]
Lisfranc Injury
Lisfranc injuries involve fracture-dislocations of the tarsometatarsal joints, forming the junction between the midfoot and forefoot. These injuries are frequently associated with disruption of the Lisfranc ligament, the strong interosseous ligament connecting the medial cuneiform to the base of the 2nd metatarsal. These injuries most commonly result from indirect trauma, such as axial loading applied to a plantarflexed foot, although direct crush injuries may also occur. Lisfranc injuries may progress to chronic instability, deformity, and posttraumatic arthritis if unrecognized or untreated
Lisfranc injuries are commonly classified as homolateral, divergent, or isolated. Homolateral injuries involve the lateral displacement of multiple metatarsals in the same direction. Divergent injuries involve medial displacement of the 1st metatarsal and lateral displacement of the remaining metatarsals. Isolated injuries involve the displacement of 1 or 2 metatarsals without involvement of the entire tarsometatarsal complex.
Radiographic evaluation should assess alignment of the tarsometatarsal joints on anteroposterior and oblique radiographs. On lateral radiographs, dorsal displacement or a step-off at the tarsometatarsal joint may indicate injury. Since overlapping structures may obscure fractures, CT imaging often reveals more extensive injury than plain radiographs. An important radiographic finding is the “fleck sign,” representing a small avulsion fracture fragment between the bases of the 1st and 2nd metatarsals and indicating disruption of the Lisfranc ligament.[33]
Stress Injury
Stress injuries of the foot and ankle are common in athletes and military recruits and result from repetitive submaximal loading of normal bone, producing microfractures when bone remodeling cannot keep pace with mechanical stress. These injuries are similar in presentation to insufficiency fractures, which occur when weakened bone is subjected to normal physiological stress. Predisposing conditions for insufficiency fractures include osteoporosis, metabolic bone disease, endocrine disorders, chronic corticosteroid use, collagen vascular disease, and alcoholism.
Common locations for stress fractures in the foot include the posterior calcaneus, navicular, cuboid near the tarsometatarsal joints, anterior talus, bases of the 1st through 3rd metatarsals, and necks of the 2nd through 4th metatarsals. Early radiographs may appear normal. Later findings may include periosteal reaction, cortical sclerosis, or a visible fracture line. MRI or nuclear medicine bone scanning is often used for early detection when clinical suspicion remains high despite unremarkable radiographic findings.[34]
Media
(Click Image to Enlarge)
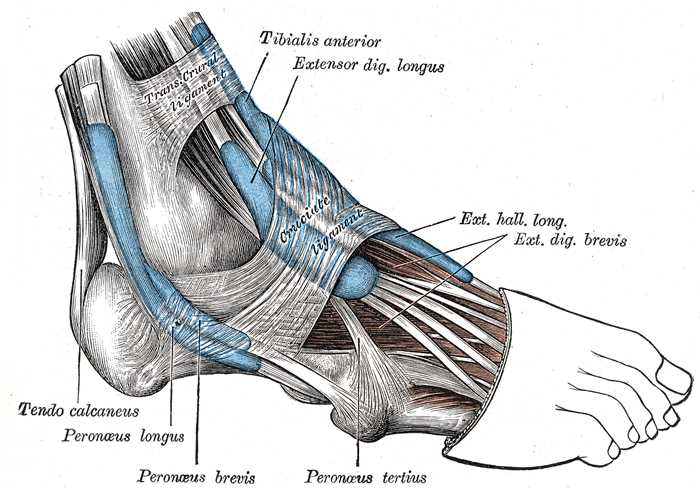
Lateral Aspect of the Right Foot and Ankle. This anatomical diagram details the major musculature and connective tissues of the lower leg and foot. Visible structures include the tibialis anterior, extensor digitorum longus, extensor hallucis longus, extensor digitorum brevis, and fibularis (peroneus) tertius. The fibular (peroneal) group is represented by the fibularis (peroneus) longus and brevis, while the tendo calcaneus (Achilles tendon) is shown inserting into the heel. The tendons are secured by the transverse crural ligament and the cruciate ligament.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
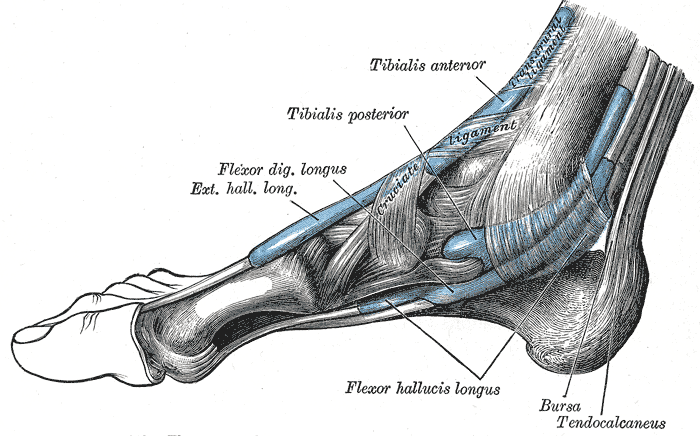
Tendons of the Extrinsic Foot Muscles. This medial view of the right foot shows the tendons of the tibialis anterior, tibialis posterior, flexor digitorum longus, extensor hallucis longus, and flexor hallucis longus. The retrocalcaneal bursa, tendo calcaneus (Achilles tendon), and transcrural and cruciate ligaments are also shown.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)

Plantar Foot Anatomy, Third Layer. This illustration displays the 3rd muscular layer of the foot sole. Labeled anatomical structures include the adductor hallucis (oblique and transverse heads), flexor hallucis brevis, plantar aponeurosis, tibialis posterior tendon, sheath of peroneus longus tendon, flexor digiti quinti brevis, and the sesamoid bone location. The diagram highlights muscles, tendons, and supporting connective tissues that contribute to hallux stability, lateral toe flexion, and foot arch structure. Structures are clearly identified for orientation and instructional reference.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
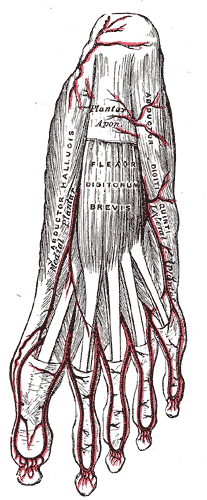
Arteries and Muscles of the Plantar Surface. The illustration highlights the superficial arterial supply and musculature of the sole of the foot. The image identifies the medial and lateral plantar arteries branching into various digital vessels. The labeled muscles and tissues include the abductor hallucis, flexor digitorum brevis, abductor digiti quinti, and the plantar aponeurosis.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Khan IA, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb, Foot Talus. StatPearls. 2026 Jan:(): [PubMed PMID: 31082130]
Stirling P, MacKenzie SP, Maempel JF, McCann C, Ray R, Clement ND, White TO, Keating JF. Patient-reported functional outcomes and health-related quality of life following fractures of the talus. Annals of the Royal College of Surgeons of England. 2019 Jul:101(6):399-404. doi: 10.1308/rcsann.2019.0044. Epub 2019 Jun 3 [PubMed PMID: 31155885]
Level 2 (mid-level) evidenceDe Boer AS, Schepers T, Panneman MJ, Van Beeck EF, Van Lieshout EM. Health care consumption and costs due to foot and ankle injuries in the Netherlands, 1986-2010. BMC musculoskeletal disorders. 2014 Apr 12:15():128. doi: 10.1186/1471-2474-15-128. Epub 2014 Apr 12 [PubMed PMID: 24725554]
Level 2 (mid-level) evidenceShamrock AG, Byerly DW. Talar Neck Fractures. StatPearls. 2026 Jan:(): [PubMed PMID: 31194455]
Manganaro D, Alsayouri K. Anatomy, Bony Pelvis and Lower Limb: Ankle Joint. StatPearls. 2026 Jan:(): [PubMed PMID: 31424742]
Colucci PG, Gao MA, Davenport KL, Conti MS, Sofka CM. Imaging findings of foot and ankle injuries in dancers. Skeletal radiology. 2026 May 4:():. doi: 10.1007/s00256-026-05229-9. Epub 2026 May 4 [PubMed PMID: 42080902]
Brockett CL, Chapman GJ. Biomechanics of the ankle. Orthopaedics and trauma. 2016 Jun:30(3):232-238 [PubMed PMID: 27594929]
Massen FK, Baumbach SF, Herterich V, Böcker W, Waizy H, Polzer H. Fractures to the anterior process of the calcaneus - Clinical results following functional treatment. Injury. 2019 Oct:50(10):1781-1786. doi: 10.1016/j.injury.2019.06.008. Epub 2019 Jun 3 [PubMed PMID: 31178146]
Arain A, Harrington MC, Rosenbaum AJ. Progressive Collapsing Foot Deformity. StatPearls. 2026 Jan:(): [PubMed PMID: 31194335]
Nery C, Fonseca LF, Gonçalves JP, Mansur N, Lemos A, Maringolo L, Fonseca LF. First MTP joint instability - Expanding the concept of "Turf-toe" injuries. Foot and ankle surgery : official journal of the European Society of Foot and Ankle Surgeons. 2020 Jan:26(1):47-53. doi: 10.1016/j.fas.2018.11.009. Epub 2018 Nov 22 [PubMed PMID: 30509556]
Han K, Bae K, Levine N, Yang J, Lee JS. Biomechanical Effect of Foot Orthoses on Rearfoot Motions and Joint Moment Parameters in Patients with Flexible Flatfoot. Medical science monitor : international medical journal of experimental and clinical research. 2019 Aug 8:25():5920-5928. doi: 10.12659/MSM.918782. Epub 2019 Aug 8 [PubMed PMID: 31393860]
Yetman Q, Welte L, Shimizu A, Rainbow MJ. Reconciling how positive foot power drives the arch recoil mechanism. Journal of the Royal Society, Interface. 2026 Feb 4:23(235):. pii: 20250532. doi: 10.1098/rsif.2025.0532. Epub [PubMed PMID: 41633524]
Card RK, Bordoni B. Anatomy, Bony Pelvis and Lower Limb, Foot Muscles. StatPearls. 2026 Jan:(): [PubMed PMID: 30969527]
Wu S, Kondo K, Matsushita Y. Spatiotemporal Regulation and Lineage Specification in Embryonic Endochondral Ossification. International journal of molecular sciences. 2026 Jan 16:27(2):. doi: 10.3390/ijms27020926. Epub 2026 Jan 16 [PubMed PMID: 41596573]
Lezak B, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb, Foot Veins. StatPearls. 2026 Jan:(): [PubMed PMID: 31194435]
Lezak B, Wehrle CJ, Summers S. Anatomy, Bony Pelvis and Lower Limb: Posterior Tibial Artery. StatPearls. 2026 Jan:(): [PubMed PMID: 30725666]
Tang A, Bordoni B. Anatomy, Bony Pelvis and Lower Limb, Foot Nerves. StatPearls. 2026 Jan:(): [PubMed PMID: 30725977]
Desai SS, Cohen-Levy WB. Anatomy, Bony Pelvis and Lower Limb: Tibial Nerve. StatPearls. 2026 Jan:(): [PubMed PMID: 30725713]
Gomes MDR, Pinto AP, Fabián AA, Gomes TJM, Navarro A, Oliva XM. The Os Peroneum incidence - A cadaveric study. Foot and ankle surgery : official journal of the European Society of Foot and Ankle Surgeons. 2020 Apr:26(3):325-327. doi: 10.1016/j.fas.2019.04.009. Epub 2019 Apr 27 [PubMed PMID: 31084989]
Preinl M, Osiowski A, Osiowski M, Baran K, Stolarz K, Jasiewicz B, Taterra D. Clinical aspects and epidemiology of os peroneum: a meta-analysis. Anatomical science international. 2026 Jan:101(1):80-90. doi: 10.1007/s12565-025-00838-1. Epub 2025 Apr 27 [PubMed PMID: 40289243]
Level 1 (high-level) evidencePlakias A, Triantafyllou G, Samolis A, Tsakotos G, Olewnik Ł, Ruzik K, Piagkou M. Prevalence and orthopaedic relevance of the supranavicular bone: a systematic review with meta-analysis. Folia morphologica. 2025 Oct 13:():. doi: 10.5603/fm.108381. Epub 2025 Oct 13 [PubMed PMID: 41081646]
Level 1 (high-level) evidenceOsiowski A, Preinl M, Osiowski M, Baran K, Jasiewicz B, Taterra D. The prevalence and clinical considerations of Os Vesalianum Pedis: A meta-analysis. Foot and ankle surgery : official journal of the European Society of Foot and Ankle Surgeons. 2025 Oct:31(7):612-618. doi: 10.1016/j.fas.2025.04.002. Epub 2025 Apr 8 [PubMed PMID: 40268623]
Level 1 (high-level) evidenceGuo S, Yan YY, Lee SSY, Tan TJ. Accessory ossicles of the foot-an imaging conundrum. Emergency radiology. 2019 Aug:26(4):465-478. doi: 10.1007/s10140-019-01688-x. Epub 2019 Apr 8 [PubMed PMID: 30963314]
Stein CJ, Sugimoto D, Slick NR, Lanois CJ, Dahlberg BW, Zwicker RL, Micheli LJ. Hallux sesamoid fractures in young athletes. The Physician and sportsmedicine. 2019 Nov:47(4):441-447. doi: 10.1080/00913847.2019.1622246. Epub 2019 Jun 5 [PubMed PMID: 31109214]
Lyrtzis C, Mpei D, St John K, Paraskevas G, Lazaridis N. A Less Common Anatomical Variant of Bilateral Multiple Lesser Metatarsal Sesamoids With Radiologic and Clinical Correlation. Cureus. 2025 May:17(5):e84771. doi: 10.7759/cureus.84771. Epub 2025 May 25 [PubMed PMID: 40433024]
Aparisi Gómez MP, Aparisi F, Bartoloni A, Ferrando Fons MA, Battista G, Guglielmi G, Bazzocchi A. Anatomical variation in the ankle and foot: from incidental finding to inductor of pathology. Part I: ankle and hindfoot. Insights into imaging. 2019 Jul 31:10(1):74. doi: 10.1186/s13244-019-0746-2. Epub 2019 Jul 31 [PubMed PMID: 31363861]
Aparisi Gómez MP, Aparisi F, Bartoloni A, Ferrando Fons MA, Battista G, Guglielmi G, Bazzocchi A. Anatomical variation in the ankle and foot: from incidental finding to inductor of pathology. Part II: midfooot and forefoot. Insights into imaging. 2019 Jul 31:10(1):69. doi: 10.1186/s13244-019-0747-1. Epub 2019 Jul 31 [PubMed PMID: 31363862]
Farid A, Faber FWM. Bilateral Triple Talocalcaneal, Calcaneonavicular, and Talonavicular Tarsal Coalition: A Case Report. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons. 2019 Mar:58(2):374-376. doi: 10.1053/j.jfas.2018.08.047. Epub [PubMed PMID: 30850104]
Level 3 (low-level) evidenceSwensen SJ, Otsuka NY. Tarsal Coalitions--Calcaneonavicular Coalitions. Foot and ankle clinics. 2015 Dec:20(4):669-79. doi: 10.1016/j.fcl.2015.08.001. Epub [PubMed PMID: 26589085]
Neary KC, Chang E, Kreulen C, Giza E. Tarsal Tunnel Syndrome Secondary to Accessory Musculature: A Case Report. Foot & ankle specialist. 2019 Dec:12(6):549-554. doi: 10.1177/1938640019863277. Epub 2019 Aug 13 [PubMed PMID: 31409132]
Level 3 (low-level) evidenceRussell TG, Byerly DW. Talus Fracture. StatPearls. 2026 Jan:(): [PubMed PMID: 30969509]
Vosseller JT, Dennis ER, Bronner S. Ankle Injuries in Dancers. The Journal of the American Academy of Orthopaedic Surgeons. 2019 Aug 15:27(16):582-589. doi: 10.5435/JAAOS-D-18-00596. Epub [PubMed PMID: 30789380]
Moracia-Ochagavía I, Rodríguez-Merchán EC. Lisfranc fracture-dislocations: current management. EFORT open reviews. 2019 Jul:4(7):430-444. doi: 10.1302/2058-5241.4.180076. Epub 2019 Jul 2 [PubMed PMID: 31423327]
Ruddick GK, Lovell GA, Drew MK, Fallon KE. Epidemiology of bone stress injuries in Australian high performance athletes: A retrospective cohort study. Journal of science and medicine in sport. 2019 Oct:22(10):1114-1118. doi: 10.1016/j.jsams.2019.06.008. Epub 2019 Jun 29 [PubMed PMID: 31307905]
Level 2 (mid-level) evidence