Indications
Flecainide acetate is an oral Class Ic antiarrhythmic drug that blocks cardiac sodium (Na+) channels and was approved by the US Food and Drug Administration (FDA) in 1984.
FDA-Approved Indications
Flecainide is used to prevent and treat abnormally rapid heart rates, including paroxysmal supraventricular tachycardia, Wolff-Parkinson-White syndrome, atrioventricular nodal reentrant tachycardia, atrioventricular reentrant tachycardia, and atrial fibrillation or atrial flutter in patients without structural heart disease.[1][2] Flecainide is also an option for treating life-threatening ventricular arrhythmias. It is essential to note that treatment with flecainide for sustained ventricular tachycardia should be initiated in a hospital setting. Flecainide acetate is not recommended for patients with less severe ventricular arrhythmias, even if they are symptomatic, because of its proarrhythmic potential. Its use should be reserved for patients in whom the benefits of treatment outweigh the risks. The FDA states that flecainide should not be used in patients with chronic atrial fibrillation or a recent myocardial infarction.
Off-Label Uses
According to the American Heart Association (AHA), the American College of Cardiology (ACC), and the Heart Rhythm Society (HRS), in patients diagnosed with long QT syndrome type 3, medications such as ranolazine, mexiletine, and flecainide are utilized to shorten the QTc interval and may help decrease the recurrence of arrhythmias.[3] Catecholaminergic polymorphic ventricular tachycardia (CPVT) is characterized by exertion-related polymorphic or bidirectional ventricular tachycardia associated with syncope and sudden cardiac arrest. Sudden cardiac arrest or sudden cardiac death occurs in 3% to 13% of patients. Treatment with beta-blockers is associated with a decrease in adverse cardiac events. Some experts prefer nadolol over other beta-blockers. Using a maximally tolerated dose of a beta-blocker is crucial. Flecainide, when combined with a beta-blocker, can reduce ventricular ectopy by up to 76% in patients with CPVT.[3][4][5][6] Andersen-Tawil syndrome type 1 (ATS1) is a rare arrhythmogenic disorder caused by loss-of-function mutations in KCNJ2.[7] Flecainide is effective in the treatment of ATS1, although further research is warranted.[8][9]
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
Flecainide is classified as a Class Ic antiarrhythmic agent according to the Vaughan–Williams classification. Flecainide acts on the fast-inward Na+ ion channel and has a high affinity for activated or open Na+ channels. It prolongs depolarization and increases refractoriness due to slow release from its binding site. It potently acts on the His-Purkinje system. It also works by inhibiting IKr channels, thereby delaying the potassium rectifier current and resulting in the prolongation of action potential duration in both ventricular and atrial muscle fibers. Flecainide blocks ryanodine receptor opening, reducing calcium release from the sarcoplasmic reticulum and leading to afterdepolarizations and triggered activity.[10] Hence, indications for flecainide include CPVT (see Image. Effects of Class Ic Sodium Channel Blockers on Cardiac Action Potential).[5]
Class Ic antiarrhythmic agents exert their effects primarily by potently blocking the fast sodium current (INa). These agents preferentially bind to the open and inactivated states of sodium channels, producing a state-dependent (use-dependent) block with slow dissociation kinetics, thereby prolonging their effects across heart rates. This action markedly reduces the maximal upstroke velocity (dV/dt or Vmax), resulting in slowed conduction velocity, decreased action potential amplitude, and widening of the QRS complex on the electrocardiogram (ECG), with minimal effect on the QT interval.
Pharmacokinetics
Absorption: Following oral administration, flecainide is nearly completely absorbed. Peak plasma levels are reached approximately 3 hours after administration (range 1 to 6 hours). Steady-state levels are attained within 3 to 5 days. Flecainide does not undergo significant presystemic biotransformation, and its absorption is not affected by food or antacids. Milk may inhibit absorption in infants, so reducing the dose when milk is removed from their diet should be considered.[11]
Distribution: Once at steady state, no additional (or unexpected) accumulation of drug in plasma occurs during chronic therapy. The extent of flecainide binding to human plasma proteins is approximately 40% and remains constant across a plasma drug concentration range of 0.015 to approximately 3.4 mcg/mL. Therefore, significant drug interactions due to protein binding are unlikely.
Metabolism: Flecainide is metabolized hepatically via the CYP450 system; flecainide is a CYP2D6 substrate.[12] The extent of metabolism may vary depending on genetic polymorphisms that affect CYP2D6 activity.
Excretion: The elimination half-life of flecainide varies with age. The elimination half-life is age-dependent; in adults, it averages 12 to 24 hours. It is typically shortest in young children (eg, 6 to 8 hours) and prolonged in newborns due to immature clearance mechanisms. Flecainide is excreted primarily in the urine (about 30%) and to a lesser extent in feces (approximately 5%).[13][14][15][16]
Administration
Available Dosage Forms and Strengths
Flecainide is available in 50 mg, 100 mg, and 150 mg tablets.
Adult Dosage
Dosing regimens for specific conditions are as follows:
Paroxysmal atrial fibrillation/paroxysmal supraventricular tachycardia (per ACC/AHA/HRS guidelines):
- 50 to 300 mg daily by mouth, divided into 8- to 12-hour intervals.
- Start with 50 mg orally every 12 hours, then increase by 100 mg per day every 4 days. The maximum recommended daily dose is 300 mg. Dose adjustment is made based on serum levels.
Ventricular arrhythmia prophylaxis:
- 100 to 400 mg daily by mouth, divided into 8- or 12-hour intervals.
- Start with 100 mg orally every 12 hours, and increase the dose by 100 mg per day every 4 days. The maximum recommended daily dose is 400 mg. Dose adjustment is made based on serum levels.
Specific Patient Populations
Hepatic impairment: According to the manufacturer, no dosage adjustment is necessary in patients with liver disease. Dosage adjustment is recommended in patients with severe hepatic impairment, and caution and close monitoring are advised.
Renal impairment: In cases where urinary pH is markedly alkaline (8 or higher), which may occur in rare conditions such as renal tubular acidosis or with a strict vegetarian diet, the elimination of flecainide from plasma occurs at a significantly slower rate. In patients with renal impairment and a creatinine clearance below 35 mL/min/1.73 m², caution must be exercised.
Pregnancy considerations: Using flecainide during pregnancy may pose some risk to the fetus; therefore, clinicians should perform a risk-benefit analysis. Fetal risks include reduced fetal heart rate variability, impaired acceleration, and QT interval abnormalities.[17] Neonates exposed to flecainide in utero have been reported to develop hyperbilirubinemia after birth, although data are limited.
Breastfeeding considerations: Flecainide is present in breast milk; the relative infant dose is 8% when the maternal dosing is 200 mg per day. The relative infant dosing is calculated using the highest average breast milk concentration compared to the maternal dosage. Breastfeeding is considered acceptable as long as the relative infant dose is less than 10%.[17]
Pediatric patients: The FDA has not approved the use of flecainide in children. Its proarrhythmic effects, as previously mentioned, are also relevant in pediatric patients. In children with structural heart disease, flecainide has been associated with cases of cardiac arrest and sudden death. Therefore, initiation of flecainide treatment should occur in a hospital setting with rhythm monitoring. Any administration of flecainide acetate in children must be supervised by a cardiologist experienced in pediatric arrhythmia treatment. Consult institutional guidelines or manufacturer prescribing information for pediatric dosing regimens. Flecainide may be used off-label for the treatment of fetal supraventricular tachycardia; however, additional research is required.[18][19]
Older patients: According to manufacturer labeling, flecainide is eliminated more slowly from plasma in older individuals than in younger individuals. Patients aged 80 and older have been safely treated with standard dosages.
Adverse Effects
Cardiac Toxicity
Flecainide has proarrhythmic effects with an increased incidence of mortality and nonfatal cardiac arrest in patients with a history of myocardial infarction and asymptomatic premature ventricular contractions/non-sustained ventricular tachycardia. Flecainide prolongs depolarization and can slow conduction in the atrioventricular node and the His-Purkinje system. These changes can result in prolonged PR intervals and first-degree and second-degree heart blocks. Preexisting sinus node disease can result in profound bradycardia. It does not affect repolarization, exerting a mild effect on the QT interval.
Flecainide has a negative inotropic effect on cardiac muscles. Therefore, its use is contraindicated in patients with heart failure. Flecainide can convert atrial fibrillation to atrial flutter with 1:1 conduction or provoke ventricular tachyarrhythmias; therefore, a beta-blocker or a calcium channel blocker should be used concurrently.[15][20]
Common reactions to flecainide include dizziness, arrhythmias, dyspnea, visual disturbances, palpitations, chest pain, tremor, asthenia, abdominal pain, and constipation.
Drug-Drug Interactions
Significant drug interactions include ritonavir, cisapride, desipramine, dronedarone, quinidine, saquinavir, and tipranavir. Concurrent use with these agents should be avoided. Flecainide interacts with many other drugs, and therapy modification may be necessary; therefore, thorough medication reconciliation is important, as with all medications.
- Digoxin: Flecainide has been administered to patients receiving digoxin without significant adverse effects; however, during multiple-dose administration, plasma digoxin concentrations may increase, requiring additional monitoring.[13]
- Amiodarone: When amiodarone is added to ongoing flecainide therapy, plasma flecainide levels may increase twofold or more. Therefore, reducing the flecainide dose and carefully monitoring for toxicity are advised.[21]
- Disopyramide/verapamil: The combined use of disopyramide or verapamil with flecainide should be approached cautiously. Since all three medications have negative inotropic effects, they should be used together only if the benefits clearly outweigh the risks.
- Calcium channel blockers: The combination of nifedipine or diltiazem with flecainide has not been studied, and concurrent use is not routinely recommended until further data are available.
- CYP450 enzyme inducers: Enzyme inducers, such as phenytoin, phenobarbital, and carbamazepine, modestly increase flecainide elimination by approximately 30%, potentially necessitating minor dosage adjustments in chronic therapy.
- CYP2D6 inhibitors: CYP2D6 inhibitors such as quinidine may increase plasma flecainide levels by inhibiting its metabolism. Antidepressants such as fluoxetine, paroxetine, and duloxetine are potent CYP2D6 inhibitors, and their coadministration with flecainide has been shown to increase plasma flecainide concentrations by 16% to 28%.[22][23][24]
Contraindications
According to the AHA/ACC/HRS 2017 guidelines, flecainide is contraindicated in patients with structural heart disease.[3] Other contraindications include hypersensitivity, documented second- or third-degree atrioventricular block, sick sinus syndrome, bundle branch block, cardiogenic shock, and acquired or congenital QT prolongation with a history of torsades de pointes.
Box Warnings
Flecainide has an FDA Black Box Warning recommending that its use be restricted to life-threatening ventricular arrhythmias, as data show no survival benefits without such arrhythmias. Proarrhythmic effects may occur in patients with atrial flutter or atrial fibrillation; the drug is not recommended for chronic atrial fibrillation. The warning also notes increased mortality and non-fatal cardiac arrest rates in asymptomatic patients with non–life-threatening ventricular arrhythmias and a prior history of myocardial infarction occurring 6 days to 2 years earlier.[25]
Warnings and Precautions
Caution is also advised in patients with myocardial dysfunction, congestive heart failure, QT prolongation, electrolyte abnormalities, and pacemakers.[26] In patients with a preexisting QRS duration of greater than 130 ms, Class Ic drugs should be prescribed with caution.[27]
Flecainide remains contraindicated in patients with structural heart disease based on the Cardiac Arrhythmia Suppression Trial (CAST trial) data; however, limited observational reports have raised cautious interest in its potential use in highly selected cases, such as stable coronary artery disease without active ischemia and preserved ventricular function. Robust prospective studies are essential before any reconsideration of current safety restrictions can be made.[1][28][29]
Monitoring
Narrow Therapeutic Index
There is an increased response and a steep relationship between dose and concentration. Plasma levels require monitoring in patients with severe renal impairment or hepatic disease. Flecainide overdose could be fatal. The prescriber should adjust the dose based on the clinical response.[13]
Monitoring Parameters
In patients with renal or hepatic impairment, it is prudent to monitor ECG and blood pressure and to obtain periodic serum trough concentrations. The therapeutic trough concentration is between 0.2 and 1 mcg/mL. Lower trough concentration may be sufficient in pediatric patients. Because of its narrow therapeutic index, slight differences in dose or blood concentration can cause serious therapeutic failures or life-threatening adverse drug reactions. Therefore, it is crucial to monitor all hemodynamic parameters, vital signs, ECG, and serum flecainide levels.[30]
Toxicity
Signs and Symptoms of Overdose
There is no specific antidote for flecainide overdose. Ingestion of doses up to 8000 mg has been survived, with reported plasma concentrations as high as 5.3 mcg/mL. Clinical features may include nausea, vomiting, seizures, hypotension, bradycardia, syncope, and pronounced ECG abnormalities such as marked QRS widening, QT and PR prolongation, ventricular tachycardia, atrioventricular block, asystole, bundle branch block, heart failure, or cardiac arrest. Fatal outcomes have occurred following ingestion of as little as 1000 mg, often in the context of co-ingestion with other medications or alcohol. Flecainide plasma levels should be obtained to confirm toxicity.
The therapeutic window for flecainide is narrow, ranging from 0.2 to 1.0 mcg/mL.[30] A patient with atrial tachyarrhythmia and pacemaker therapy developed a wide-QRS tachycardia that mimicked ventricular tachycardia. Pacemaker interrogation confirmed atrial flutter with pacemaker-mediated ventricular pacing, consistent with flecainide toxicity.[31][32] Infrequent cases of suicide by intentional flecainide overdose have been reported in the literature.[33][34][35]
Management of Overdose
Management of an overdose is mainly supportive, and there is no antidote for flecainide overdose. According to the review of literature, the documented mortality rate from overdose of Class Ic Vaughan Williams antiarrhythmics stands at 22.5%. Standard treatments include aggressive fluid resuscitation, administration of hypertonic sodium bicarbonate, and intravenous magnesium.[36] The initial management of toxicity involves administering a sodium bicarbonate infusion to promptly counteract the effects of flecainide, thereby preventing potentially life-threatening arrhythmias. Case reports indicate that sodium bicarbonate can be used as monotherapy and is commonly given as first-line treatment for a QRS duration of greater than 100 ms, in increments of 1 to 2 mEq/kg. Sodium bicarbonate raises serum pH and increases extracellular sodium levels, enabling it to compete with flecainide for sodium channel binding and strengthening the electrochemical gradient across cell membranes.[37] Consult a medical toxicologist and contact the national poison control center for up-to-date information.
Lipid emulsion therapy can also be used in conjunction with sodium bicarbonate for flecainide toxicity. The "lipid sink" theory suggests that it removes lipophilic flecainide from toxicity sites by increasing blood lipid levels.[38] Management is mainly supportive. Prompt gastrointestinal decontamination should be considered to limit absorption. Hemodynamic instability may respond to inotropic or chronotropic agents. Mechanical ventilation may be required in patients with severe cardiac and respiratory depression. Advanced supportive measures, including intra-aortic balloon counterpulsation or transvenous pacing, may be indicated in cases of refractory conduction block or profound hemodynamic compromise.[39] Due to flecainide's prolonged elimination half-life (approximately 12–27 hours) and potential for nonlinear kinetics at toxic concentrations, extended monitoring and supportive care are essential. Hemodialysis does not enhance clearance.
Enhancing Healthcare Team Outcomes
This section discusses the evidence-based use and outcomes of flecainide across various clinical settings.
CAST Trial
Initially, it was thought to be effective in the treatment of premature ventricular contractions and nonsustained ventricular tachycardia after myocardial infarction to reduce the incidence of sudden death. However, in a multicenter randomized placebo-controlled trial on patients after myocardial infarction, the use of flecainide was associated with increased mortality due to fatal arrhythmias. Therefore, flecainide is considered for patients without coronary artery disease and left ventricular dysfunction. Currently, contraindications to flecainide include patients with left ventricular hypertrophy, ischemic heart disease, hypertrophic obstructive cardiomyopathy, high-degree atrioventricular block, and complete heart block.[40]
PITAGORA Trial
A multicenter, single-blind, prospective randomized trial compared amiodarone with Class Ic (propafenone and flecainide) in patients with atrial fibrillation and a pacemaker due to sinus node disease for maintaining sinus rhythm as a goal. Flecainide was found to be noninferior and equally efficacious in preventing episodes lasting more than 10 minutes or those lasting for 1 day.[41]
Pill-in-the-Pocket Approach
According to the NEJM study published in 2004, flecainide is one of the drugs, apart from propafenone, used in outpatient or emergency department settings to treat symptomatic atrial fibrillation. In some patients, oral prophylaxis or catheter ablation may not be feasible; therefore, a single dose of an antiarrhythmic medication at the time of symptom onset is an appropriate option. The dose of flecainide was 300 mg for patients of more than 70 kg or 200 mg otherwise. Around 165 patients were followed for 2 years; 94% were successfully treated after the onset of symptoms within 2 hours. Recurrences were successfully treated in up to 84% of cases. The number of emergency room visits and hospitalizations was significantly lower during the study period compared to the year before the treatment period.[42]
Acute Cardioversion in Emergency Departments
Based on recent meta-analyses, IV flecainide is superior to other antiarrhythmics, such as ibutilide, amiodarone, sotalol, propafenone, and procainamide. Eleven randomized controlled trials were analyzed, and it was found that flecainide was highly effective for cardioversion within 2 hours. There is no statistically significant difference in proarrhythmic behavior compared to placebo or other antiarrhythmics.[43]
Effect on Atrial Remodeling
Structural changes in the atria occur due to atrial fibrillation, leading to myocardial remodeling and mitochondrial dysfunction caused by oxidative stress. During atrial fibrillation, atrial activation rapidly leads to intracellular calcium accumulation via the Na+/Ca2+ exchanger. Flecainide inhibits intracellular Ca2+ accumulation, which reduces atrial remodeling and oxidative stress.[44]
Fetal Tachycardia
Flecainide has been shown to be effective in the transplacental treatment of fetal tachycardia. Flecainide was found to be superior to digoxin and sotalol in the termination of fetal tachycardia, especially supraventricular tachycardia. The placental transfer is not affected in hydrops fetalis.[45]
Catecholaminergic Polymorphic Ventricular Tachycardia
As discussed above, flecainide inhibits cardiac ryanodine receptors in their open state, which are responsible for calcium release and lead to CPVT. Flecainide suppresses 76% of exercise-induced ventricular arrhythmias in 33 genotype-positive patients. It is also efficacious in suppressing ventricular tachyarrhythmias in genotype-negative patients.[46]
Practical Aspects Before and During Initiation of Flecainide
- An exercise stress test should be performed before initiating flecainide therapy to rule out coronary artery disease and repeated during treatment if resting QRS prolongation is observed.
- ECG monitoring is recommended to assess QRS duration. The flecainide dose should be reduced to half the initial dose if the QRS duration increases by 25%.
- Patients should be screened for sinus node dysfunction and atrioventricular node disease prior to treatment initiation.
- Concurrent administration of negative chronotropic agents, such as beta-blockers, is recommended.
While pharmaceutical therapy with flecainide should be initiated only by a cardiologist, it requires an interprofessional team approach, including the patient, other clinicians and specialists, specialty-trained nurses, and pharmacists, all collaborating across disciplines to achieve optimal patient outcomes. As a narrow therapeutic index medication, all healthcare team members must be aware of the patient's therapy, recognize signs of toxicity or inadequate response, and communicate openly with other interprofessional team members regarding treatment progress and adverse events to optimize therapeutic outcomes and improve the patient's condition.
Media
(Click Image to Enlarge)
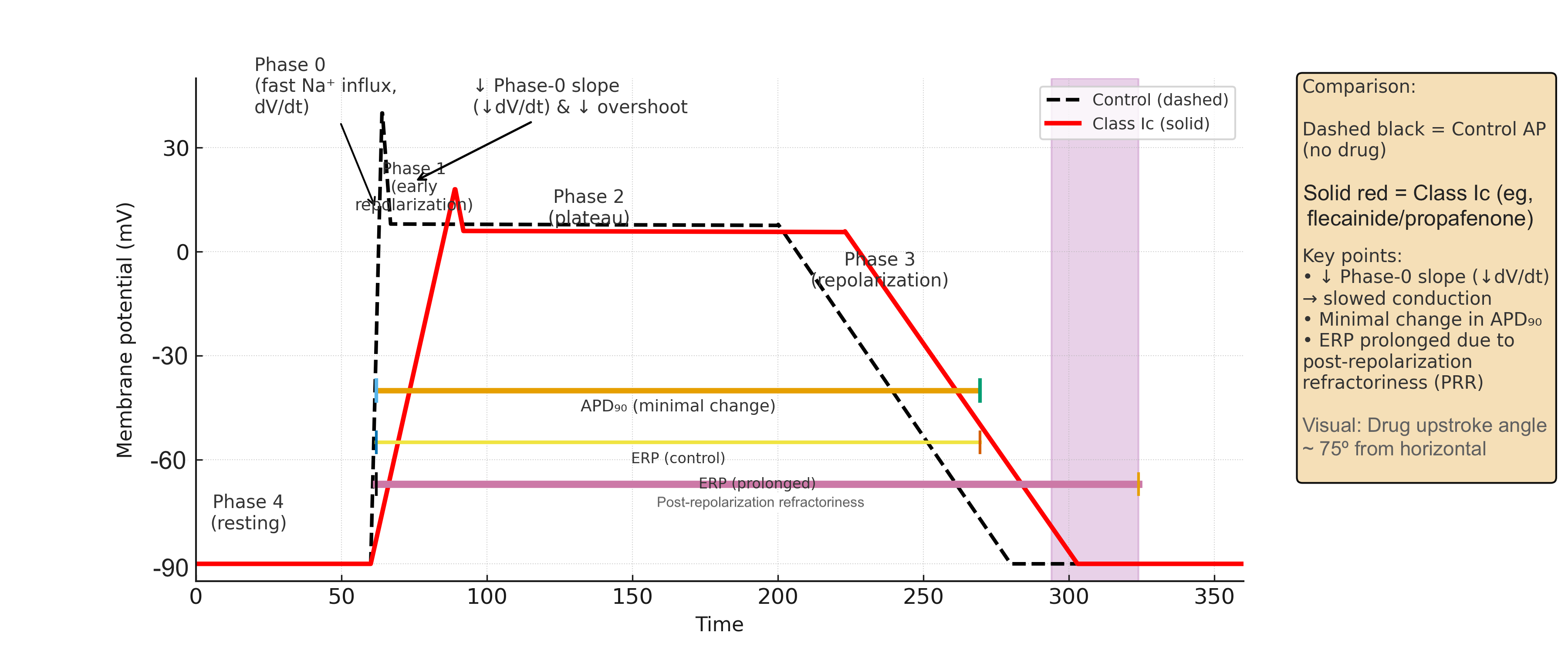
Effects of Class Ic Sodium Channel Blockers on Cardiac Action Potential. Diagram comparing a normal cardiac action potential (AP) with one altered by Class Ic antiarrhythmic drugs (eg, flecainide and propafenone), demonstrating a marked reduction in the phase-0 slope and a prolonged effective refractory period resulting from post-repolarization refractoriness.
Contributed by P Patel, PharmD
References
Genovese D, Salama M, Ruggiero D, Sgarito G, Francia P, Santoro F, Perrotta L, Mugnai G. Flecainide in structural heart diseases: A contemporary reappraisal beyond the CAST. Heart rhythm. 2025 Aug 25:():. pii: S1547-5271(25)02788-2. doi: 10.1016/j.hrthm.2025.08.034. Epub 2025 Aug 25 [PubMed PMID: 40865597]
deSouza IS, Shrestha P, Allen R, Koos J, Thode H Jr. Safety and Effectiveness of Antidysrhythmic Drugs for Pharmacologic Cardioversion of Recent-Onset Atrial Fibrillation: a Systematic Review and Bayesian Network Meta-analysis. Cardiovascular drugs and therapy. 2025 Aug:39(4):903-923. doi: 10.1007/s10557-024-07552-6. Epub 2024 Feb 7 [PubMed PMID: 38324103]
Level 1 (high-level) evidenceAl-Khatib SM, Stevenson WG, Ackerman MJ, Bryant WJ, Callans DJ, Curtis AB, Deal BJ, Dickfeld T, Field ME, Fonarow GC, Gillis AM, Granger CB, Hammill SC, Hlatky MA, Joglar JA, Kay GN, Matlock DD, Myerburg RJ, Page RL. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2018 Sep 25:138(13):e272-e391. doi: 10.1161/CIR.0000000000000549. Epub [PubMed PMID: 29084731]
Level 1 (high-level) evidenceAbbas M, Miles C, Behr E. Catecholaminergic Polymorphic Ventricular Tachycardia. Arrhythmia & electrophysiology review. 2022 Apr:11():e20. doi: 10.15420/aer.2022.09. Epub [PubMed PMID: 36644199]
Wang G, Zhao N, Zhong S, Wang Y, Li J. Safety and efficacy of flecainide for patients with catecholaminergic polymorphic ventricular tachycardia: A systematic review and meta-analysis. Medicine. 2019 Aug:98(34):e16961. doi: 10.1097/MD.0000000000016961. Epub [PubMed PMID: 31441899]
Level 1 (high-level) evidenceKrause U. Management of channelopathies in children. Herzschrittmachertherapie & Elektrophysiologie. 2025 Sep:36(3):186-191. doi: 10.1007/s00399-025-01098-2. Epub 2025 Aug 5 [PubMed PMID: 40762707]
Yu S, Lv H. When the U Wave Tells the Story: Andersen-Tawil Syndrome Unmasked. Annals of noninvasive electrocardiology : the official journal of the International Society for Holter and Noninvasive Electrocardiology, Inc. 2025 Nov:30(6):e70119. doi: 10.1111/anec.70119. Epub [PubMed PMID: 41129324]
Mann TD, Yoruk A, Neves RA, Bergman AT, Bos MJ, van der Werf C, Gollob MH, Roberts JD, Khan H, Sanatani S, Vedantham V, Lee BK, Yesaulov A, Krahn AD, Tadros R, Wilde AA, Ackerman MJ, Scheinman MM. Flecainide for the Treatment of Andersen-Tawil Syndrome. JACC. Clinical electrophysiology. 2025 Jul:11(7):1511-1518. doi: 10.1016/j.jacep.2025.03.020. Epub 2025 May 14 [PubMed PMID: 40372332]
Maffè S, Paffoni P, Bergamasco L, Dellavesa P, Zenone F, Baduena L, Franchetti Pardo N, Careri G, Facchini E, Sansone V, Parravicini U. Therapeutic management of ventricular arrhythmias in Andersen-Tawil syndrome. Journal of electrocardiology. 2020 Jan-Feb:58():37-42. doi: 10.1016/j.jelectrocard.2019.10.009. Epub 2019 Nov 1 [PubMed PMID: 31710873]
Bannister ML, MacLeod KT, George CH. Moving in the right direction: elucidating the mechanisms of interaction between flecainide and the cardiac ryanodine receptor. British journal of pharmacology. 2022 Jun:179(11):2558-2563. doi: 10.1111/bph.15718. Epub 2021 Dec 2 [PubMed PMID: 34698387]
Thompson B, Mangat J, Barton C, Hawcutt DB. Decreased milk drinking causing flecainide toxicity in an older child. BMJ case reports. 2012 Jun 21:2012():. doi: 10.1136/bcr.02.2012.5810. Epub 2012 Jun 21 [PubMed PMID: 22729333]
Level 3 (low-level) evidencePalmen R, Sandritter T, Malloy-Walton L, Follansbee C, Wagner JB. Case report: Use of therapeutic drug monitoring and pharmacogenetic testing as opportunities to individualize care in a case of flecainide toxicity after fetal supraventricular tachycardia. Frontiers in pediatrics. 2023:11():1168619. doi: 10.3389/fped.2023.1168619. Epub 2023 Jun 28 [PubMed PMID: 37449265]
Level 3 (low-level) evidenceTamargo J, Le Heuzey JY, Mabo P. Narrow therapeutic index drugs: a clinical pharmacological consideration to flecainide. European journal of clinical pharmacology. 2015 May:71(5):549-67. doi: 10.1007/s00228-015-1832-0. Epub 2015 Apr 15 [PubMed PMID: 25870032]
Holmes B, Heel RC. Flecainide. A preliminary review of its pharmacodynamic properties and therapeutic efficacy. Drugs. 1985 Jan:29(1):1-33 [PubMed PMID: 3882390]
Level 3 (low-level) evidenceRoden DM, Woosley RL. Drug therapy. Flecainide. The New England journal of medicine. 1986 Jul 3:315(1):36-41 [PubMed PMID: 3520324]
Level 3 (low-level) evidenceConard GJ, Ober RE. Metabolism of flecainide. The American journal of cardiology. 1984 Feb 27:53(5):41B-51B [PubMed PMID: 6364769]
Level 3 (low-level) evidenceTamirisa KP, Elkayam U, Briller JE, Mason PK, Pillarisetti J, Merchant FM, Patel H, Lakkireddy DR, Russo AM, Volgman AS, Vaseghi M. Arrhythmias in Pregnancy. JACC. Clinical electrophysiology. 2022 Jan:8(1):120-135. doi: 10.1016/j.jacep.2021.10.004. Epub 2021 Dec 22 [PubMed PMID: 35057977]
Albrecht MEM, Makabe SF, Bravo-Valenzuela NJ, Araujo Júnior E. Fetal tachyarrhythmias: current knowledge for clinical practice. Translational pediatrics. 2025 Jul 31:14(7):1624-1636. doi: 10.21037/tp-2025-67. Epub 2025 Jul 17 [PubMed PMID: 40800184]
Miyoshi T. Fetal arrhythmias: Current evidence of prenatal diagnosis and management. The journal of obstetrics and gynaecology research. 2025 Mar:51(3):e16256. doi: 10.1111/jog.16256. Epub [PubMed PMID: 40040358]
Andrikopoulos GK, Pastromas S, Tzeis S. Flecainide: Current status and perspectives in arrhythmia management. World journal of cardiology. 2015 Feb 26:7(2):76-85. doi: 10.4330/wjc.v7.i2.76. Epub [PubMed PMID: 25717355]
Level 3 (low-level) evidenceMar PL, Horbal P, Chung MK, Dukes JW, Ezekowitz M, Lakkireddy D, Lip GYH, Miletello M, Noseworthy PA, Reiffel JA, Tisdale JE, Olshansky B, Gopinathannair R, from the American Heart Association Electrocardiography and Arrhythmias Committee of the Council of Clinical Cardiology. Drug Interactions Affecting Antiarrhythmic Drug Use. Circulation. Arrhythmia and electrophysiology. 2022 May:15(5):e007955. doi: 10.1161/CIRCEP.121.007955. Epub 2022 May 2 [PubMed PMID: 35491871]
Trujillo TC, Nolan PE. Antiarrhythmic agents: drug interactions of clinical significance. Drug safety. 2000 Dec:23(6):509-32 [PubMed PMID: 11144659]
Taylor C, Crosby I, Yip V, Maguire P, Pirmohamed M, Turner RM. A Review of the Important Role of CYP2D6 in Pharmacogenomics. Genes. 2020 Oct 30:11(11):. doi: 10.3390/genes11111295. Epub 2020 Oct 30 [PubMed PMID: 33143137]
Lim KS, Cho JY, Jang IJ, Kim BH, Kim J, Jeon JY, Tae YM, Yi S, Eum S, Shin SG, Yu KS. Pharmacokinetic interaction of flecainide and paroxetine in relation to the CYP2D6*10 allele in healthy Korean subjects. British journal of clinical pharmacology. 2008 Nov:66(5):660-6. doi: 10.1111/j.1365-2125.2008.03267.x. Epub 2008 Jul 24 [PubMed PMID: 18754843]
Stolear A, Dulgher M, Bae JY, Kaminsky L, Jeyashanmugaraja GP, Emerenini U. Wide Spectrum of Flecainide Toxicity: A Case Report and Literature Review. Cureus. 2024 Jun:16(6):e62923. doi: 10.7759/cureus.62923. Epub 2024 Jun 22 [PubMed PMID: 39040749]
Level 3 (low-level) evidenceRivner H, Lambrakos LK. Flecainide Toxicity Leading to Loss of Pacemaker Capture and Cardiac Arrest. JACC. Case reports. 2021 Apr:3(4):586-590. doi: 10.1016/j.jaccas.2020.11.030. Epub 2021 Jan 27 [PubMed PMID: 34317582]
Level 3 (low-level) evidenceDan GA, Martinez-Rubio A, Agewall S, Boriani G, Borggrefe M, Gaita F, van Gelder I, Gorenek B, Kaski JC, Kjeldsen K, Lip GYH, Merkely B, Okumura K, Piccini JP, Potpara T, Poulsen BK, Saba M, Savelieva I, Tamargo JL, Wolpert C, ESC Scientific Document Group. Antiarrhythmic drugs-clinical use and clinical decision making: a consensus document from the European Heart Rhythm Association (EHRA) and European Society of Cardiology (ESC) Working Group on Cardiovascular Pharmacology, endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS) and International Society of Cardiovascular Pharmacotherapy (ISCP). Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2018 May 1:20(5):731-732an. doi: 10.1093/europace/eux373. Epub [PubMed PMID: 29438514]
Level 3 (low-level) evidenceMuzzey M, Tellor KB, Ramaswamy K, Schwarze M, Armbruster AL. Flecainide is well-tolerated and effective in patient with atrial fibrillation at 12 months: a retrospective study. Therapeutic advances in cardiovascular disease. 2020 Jan-Dec:14():1753944720926824. doi: 10.1177/1753944720926824. Epub [PubMed PMID: 32633682]
Level 2 (mid-level) evidenceSangpornsuk N, Rungpradubvong V, Tiensantisuk T, Leelapattana P, Chokesuwattanakul R, Prechawat S. Flecainide use in arrhythmic patients who have structural heart disease. Therapeutic advances in drug safety. 2025:16():20420986251316462. doi: 10.1177/20420986251316462. Epub 2025 Feb 12 [PubMed PMID: 39944374]
Level 3 (low-level) evidenceKhatiwada P, Clark L, Khunger A, Rijal BB, Ritter J. A Case Report of Flecainide Toxicity With Review of Literature. Cureus. 2022 Feb:14(2):e22261. doi: 10.7759/cureus.22261. Epub 2022 Feb 15 [PubMed PMID: 35350525]
Level 3 (low-level) evidencePeribáñez S, Martínez-Fleta M, Corredoira PM. Flecainide toxicity in a patient with a pacemaker. Revista portuguesa de cardiologia : orgao oficial da Sociedade Portuguesa de Cardiologia = Portuguese journal of cardiology : an official journal of the Portuguese Society of Cardiology. 2025 Aug:44(8):519-520. doi: 10.1016/j.repc.2025.02.008. Epub 2025 Jun 2 [PubMed PMID: 40466766]
Vattikonda K, Peterson CJ, Anyanwu B, Binder MS, Penmetsa M, May T. Therapeutic Flecainide Toxicity Causing VT Storm. JACC. Case reports. 2025 Jan 15:30(2):102797. doi: 10.1016/j.jaccas.2024.102797. Epub 2025 Jan 15 [PubMed PMID: 39886422]
Level 3 (low-level) evidenceFan S, Norton KN. Flecainide Intoxication: An Unusual Case of Suicide. The American journal of forensic medicine and pathology. 2025 Sep 1:46(3):255-257. doi: 10.1097/PAF.0000000000001026. Epub 2025 Feb 24 [PubMed PMID: 39976590]
Level 3 (low-level) evidenceBen Kilani M, Naccache S, Tlili R, Mbarek D, Longo S, Ben Ameur Y, Boujnah MR. Attempted suicide by Flécainide overdose: A case report. La Tunisie medicale. 2017 Jun:95(6):451-453 [PubMed PMID: 29512803]
Level 3 (low-level) evidenceBologa C, Lionte C, Popescu A, Sorodoc V, Sorodoc L. First Case of Acute Poisoning with Amiodarone and Flecainide in Attempted Suicide Successfully Managed with Lipid Emulsion Therapy in the Emergency Department: Case Report and Literature Review. Healthcare (Basel, Switzerland). 2021 Jun 4:9(6):. doi: 10.3390/healthcare9060671. Epub 2021 Jun 4 [PubMed PMID: 34199756]
Level 3 (low-level) evidenceMukhtar O, Archer JR, Dargan PI, Wood DM. Lesson of the month 1: Acute flecainide overdose and the potential utility of lipid emulsion therapy. Clinical medicine (London, England). 2015 Jun:15(3):301-3. doi: 10.7861/clinmedicine.15-3-301. Epub [PubMed PMID: 26031986]
Gardner Yelton SE, Leonard JB, de la Uz CM, Wadia RS, Barnes SS. Flecainide Toxicity Secondary to Accidental Overdose: A Pediatric Case Report of Two Brothers. Case reports in critical care. 2021:2021():6633859. doi: 10.1155/2021/6633859. Epub 2021 May 13 [PubMed PMID: 34094603]
Level 3 (low-level) evidenceBazoukis G, Efthymiou P, Yiannikourides A, Khattab E, Dimitriades V, Tse G, Pavlou M, Georgiou P, Kapetis L, Patestos D, Tsielepis M, Myrianthopoulos K, Papasavvas E, Christophides T. Flecainide toxicity-Clinical diagnosis and management of an urgent condition. Clinical case reports. 2024 Sep:12(9):e9371. doi: 10.1002/ccr3.9371. Epub 2024 Aug 29 [PubMed PMID: 39219784]
Level 3 (low-level) evidenceTimperley J, Mitchell AR, Brown PD, West NE. Flecainide overdose--support using an intra-aortic balloon pump. BMC emergency medicine. 2005 Dec 12:5():10 [PubMed PMID: 16343338]
Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, Barker AH, Arensberg D, Baker A, Friedman L, Greene HL. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial. The New England journal of medicine. 1991 Mar 21:324(12):781-8 [PubMed PMID: 1900101]
Level 1 (high-level) evidenceGulizia M, Mangiameli S, Chiarandà G, Spadola V, Di Giovanni N, Colletti A, Bulla V, Circo A, Pensabene O, Vasquez L, Vaccaro I, Grammatico A, PITAGORA Study Investigators. Design and rationale of a randomized study to compare amiodarone and Class IC anti-arrhythmic drugs in terms of atrial fibrillation treatment efficacy in patients paced for sinus node disease: the PITAGORA trial. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2006 Apr:8(4):302-5 [PubMed PMID: 16627459]
Level 1 (high-level) evidenceAlboni P, Botto GL, Baldi N, Luzi M, Russo V, Gianfranchi L, Marchi P, Calzolari M, Solano A, Baroffio R, Gaggioli G. Outpatient treatment of recent-onset atrial fibrillation with the "pill-in-the-pocket" approach. The New England journal of medicine. 2004 Dec 2:351(23):2384-91 [PubMed PMID: 15575054]
Level 1 (high-level) evidenceMarkey GC, Salter N, Ryan J. Intravenous Flecainide for Emergency Department Management of Acute Atrial Fibrillation. The Journal of emergency medicine. 2018 Mar:54(3):320-327. doi: 10.1016/j.jemermed.2017.11.016. Epub [PubMed PMID: 29269083]
Iwai T, Tanonaka K, Inoue R, Kasahara S, Motegi K, Nagaya S, Takeo S. Sodium accumulation during ischemia induces mitochondrial damage in perfused rat hearts. Cardiovascular research. 2002 Jul:55(1):141-9 [PubMed PMID: 12062717]
Level 3 (low-level) evidenceAlsaied T, Baskar S, Fares M, Alahdab F, Czosek RJ, Murad MH, Prokop LJ, Divanovic AA. First-Line Antiarrhythmic Transplacental Treatment for Fetal Tachyarrhythmia: A Systematic Review and Meta-Analysis. Journal of the American Heart Association. 2017 Dec 15:6(12):. doi: 10.1161/JAHA.117.007164. Epub 2017 Dec 15 [PubMed PMID: 29246961]
Level 1 (high-level) evidencevan der Werf C, Kannankeril PJ, Sacher F, Krahn AD, Viskin S, Leenhardt A, Shimizu W, Sumitomo N, Fish FA, Bhuiyan ZA, Willems AR, van der Veen MJ, Watanabe H, Laborderie J, Haïssaguerre M, Knollmann BC, Wilde AA. Flecainide therapy reduces exercise-induced ventricular arrhythmias in patients with catecholaminergic polymorphic ventricular tachycardia. Journal of the American College of Cardiology. 2011 May 31:57(22):2244-54. doi: 10.1016/j.jacc.2011.01.026. Epub [PubMed PMID: 21616285]
Level 2 (mid-level) evidence