Introduction
Fetal movements perceived by a pregnant individual are a normal component of fetal development and serve as an important clinical indicator of fetal viability and neurologic integrity. The pregnant individual is typically the first to perceive these movements, which may later be palpable or observable by others. Healthcare professionals routinely advise patients to monitor fetal activity, either through general awareness or through structured methods such as maternal kick counts, which are performed within a defined time frame.
A reduction or alteration in fetal movement patterns may indicate fetal compromise and warrants timely evaluation. Patients should be counseled to promptly notify their healthcare provider if they perceive a significant decrease in movement. Although emerging technologies, including wearable monitoring devices, have been investigated for fetal movement assessment, current obstetric recommendations continue to support maternal kick counts as a simple, low-cost, and effective method for the early identification of abnormal fetal activity that requires further clinical assessment.[1][2][3][4]
Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Function
The initial perception of fetal movement refers to the maternal awareness of subtle movements or pressure exerted by the fetus against the intra-abdominal wall. These movements are believed to reflect early fetal neurologic and motor development. The first recognizable fetal movements, known as quickening, typically occur between 14 and 22 weeks of gestation. These movements are often described as fluttering, bubbling, or tapping sensations that signal the fetus's presence and vitality to the pregnant individual. Multiparous women generally perceive fetal movements approximately 1 week sooner than primigravid women. In rare cases, multiparous women may perceive movement as early as 14 weeks; however, most studies' results indicate that most pregnant individuals first experience quickening between 18 and 20 weeks of gestation. The timing of initial perception varies and may be influenced by factors such as maternal age, body mass index, parity, and placental location, with anterior placentation often associated with delayed perception.
Clinicians typically recommend that pregnant individuals begin monitoring fetal movements during the third trimester, generally around 28 weeks of gestation. This practice may involve maintaining a general awareness of daily fetal activity and noting any reduction in movement. Alternatively, more structured monitoring methods, such as formal fetal movement counting—commonly referred to as kick counts—may be advised. Clinicians often recommend initiating this surveillance at approximately 28 weeks and continuing through the remainder of the pregnancy.
The widely used count-to-10 method instructs the patient to record fetal movements at the same time each day and to contact their healthcare provider if fewer than 10 movements are perceived within 2 hours. Although not all patients require daily fetal movement counting, any noticeable decrease in activity should prompt clinical evaluation. While the effectiveness of kick counting in preventing stillbirth remains uncertain, awareness of fetal movement patterns remains a valuable component of antenatal surveillance and patient engagement in fetal well-being.[5][6][7][8]
Issues of Concern
The primary clinical concern regarding fetal movement centers on perceived or actual decreases in activity. Reduced fetal movement has been associated with adverse outcomes, including stillbirth and intrauterine fetal demise. Educating both patients and healthcare providers to recognize and respond appropriately to changes in fetal movement is intended to promote timely intervention and prevent catastrophic events such as stillbirth. Multiple studies' results have demonstrated that individuals reporting decreased fetal movement are at significantly increased risk for adverse perinatal outcomes. In the United States, stillbirth occurs in approximately 1 in 160 pregnancies, and decreased fetal activity may precede fetal death by several days.
When reduced fetal movement is reported, assessment through noninvasive modalities, such as a nonstress test or biophysical profile, is recommended to evaluate fetal well-being and determine whether delivery is indicated. These evaluations are both low-cost and effective in identifying fetuses at risk. Evidence suggests that decreased fetal movement may result from uteroplacental insufficiency and may reflect a compensatory response to acute or chronic fetal hypoxemia. Although numerous studies have sought to clarify the underlying mechanisms, the precise etiology of decreased fetal movement remains uncertain.[6][9][10][11] Please see StatPearls' companion resource, "Antenatal Fetal Surveillance," for further information.
An unintended consequence of formal fetal movement assessment is the potential for a modest increase in antenatal visits, fetal testing, and interventions, including induction of labor, cesarean delivery, and iatrogenic preterm birth. Conversely, several studies have found that structured fetal movement counting can provide reassurance to pregnant individuals, reduce unnecessary clinical visits, and enhance maternal-fetal bonding. Clinicians should recognize that vigilance in fetal movement monitoring varies among patients and tailor surveillance strategies accordingly, particularly in those with additional risk factors such as obesity, diabetes, or hypertension. Research indicates that fetal movement patterns evolve throughout gestation and can reflect both normal and abnormal development. Although studies suggest that women with obesity perceive fetal movement similarly to those with lower body mass index, the higher prevalence of maternal and fetal complications in this population may contribute to more frequent reports of decreased movement.[12]
Clinical Significance
Any reported decrease in perceived fetal movement should prompt evaluation by the clinician, typically beginning with a nonstress test (NST) (see Image. Nonstress Test). The NST is a noninvasive assessment that evaluates fetal heart rate (FHR) patterns in relation to fetal movements, providing insight into fetal oxygenation and autonomic function. A reactive NST is characterized by the presence of at least 2 FHR accelerations within 20 minutes. For fetuses at or beyond 32 weeks of gestation, each acceleration must be at least 15 bpm above the baseline and last for a minimum of 15 seconds. For fetuses younger than 32 weeks, accelerations of at least 10 bpm above baseline lasting a minimum of 10 seconds are considered appropriate. The baseline FHR should range between 110 and 160 bpm, with moderate variability defined as amplitude fluctuations between 6 and 25 bpm.
A nonreactive NST, characterized by the absence of qualifying accelerations, may reflect either a normal fetal sleep cycle or potential fetal compromise. In such cases, the test is typically extended to allow additional time for accelerations to occur. If the tracing remains nonreactive, further evaluation is warranted, most commonly through a BPP. The BPP utilizes ultrasound to assess 4 parameters of fetal well-being: fetal breathing movements, gross body or limb movements, fetal tone, and amniotic fluid volume. Each parameter is assigned a score of 2 points if present, for a total possible score of 8. A total score of 8 out of 8 is considered reassuring; however, lower scores necessitate individualized management based on gestational age and the overall clinical context.
For a pregnant individual reporting decreased fetal movement after viability, a single episode of antenatal surveillance—such as an NST or biophysical profile—should be performed at the time of symptom reporting. If no recurrent episodes of decreased movement occur and the evaluation is reassuring, repeat antenatal surveillance is generally not required.[6][13] Please see StatPearls' companion resource, "Antenatal Fetal Surveillance," for further information.
Enhancing Healthcare Team Outcomes
Recognition of decreased fetal movement is a critical component of comprehensive prenatal care, serving as a potential early indicator of fetal compromise or distress. Timely identification allows for prompt intervention, which may include enhanced monitoring, modification of antenatal management, or expedited delivery. This proactive approach has the potential to improve both maternal and fetal outcomes. Antenatal monitoring strategies should be individualized, with healthcare professionals maintaining a heightened index of suspicion when patients report changes in fetal activity. Prompt assessment and appropriate clinical action can mitigate the risk of adverse outcomes, including stillbirth.
Effective management requires coordinated efforts within an interprofessional team, with each member fulfilling distinct but complementary roles. Nurses often serve as the first point of contact when a patient reports decreased fetal activity. The ability of nurses to recognize potential warning signs and appropriately escalate care—such as advising an in-person evaluation—is essential. Clinicians then integrate clinical findings to determine the necessity of further testing, which may include an NST, BPP, or ultrasound, and decide whether immediate admission or delivery is warranted, particularly in the presence of significant risk factors. This seamless communication and shared responsibility optimize timely and accurate responses, safeguarding maternal and fetal health.
The most effective care for pregnant individuals is achieved through collaborative, interprofessional practice, involving obstetricians, midwives, nurses, and other relevant healthcare professionals. These clinicians share responsibility for educating patients on self-monitoring fetal movements and recognizing when to report changes. Although various methods exist, such as kick counts and NSTs, evidence supporting their effectiveness in preventing adverse outcomes remains limited. Nevertheless, coordinated evaluation and management in response to decreased fetal movement are essential. Early identification of risk factors and complications, coupled with timely intervention, can reduce neonatal morbidity and mortality. Ongoing research is needed to refine monitoring approaches and establish their long-term impact on perinatal outcomes.[14]
Nursing, Allied Health, and Interprofessional Team Interventions
Nurses play a central role in assessing and managing neonates following maternal reports of decreased fetal movement. Interventions may include advising the patient to undergo further evaluation, applying external fetal heart monitoring, assessing uterine contractions, monitoring maternal vital signs, and evaluating maternal distress. Nurses may also assist during more comprehensive fetal assessments, such as biophysical profile examinations, and serve as a key communicator—relaying findings to the patient, her family, and the primary care clinician.
In the labor and delivery setting, nurses may assist with interventions such as induction of labor or cesarean delivery if fetal assessment results are nonreassuring. Effective communication with patients, their families, and the healthcare team is a critical nursing responsibility. Providing empathy and support during unexpected or emergent changes in the pregnancy or birth process is essential to optimizing outcomes. Through their clinical expertise and patient advocacy, nurses make significant contributions to improving the safety and well-being of both mothers and newborns.
Nursing, Allied Health, and Interprofessional Team Monitoring
Ongoing monitoring by nurses in medical offices that provide care for pregnant individuals should include patient education on fetal movement awareness and timely response to reports of decreased fetal activity. All office personnel who interact with pregnant patients—whether through phone triage or during prenatal visits—must understand the clinical significance of fetal movement monitoring and the importance of attentively responding to patient concerns. Prompt communication of these concerns to the primary care clinician is essential to facilitate further evaluation and treatment. This proactive approach can enhance patient outcomes by facilitating timely assessment and intervention, thereby promoting maternal and fetal well-being.
Media
(Click Image to Enlarge)
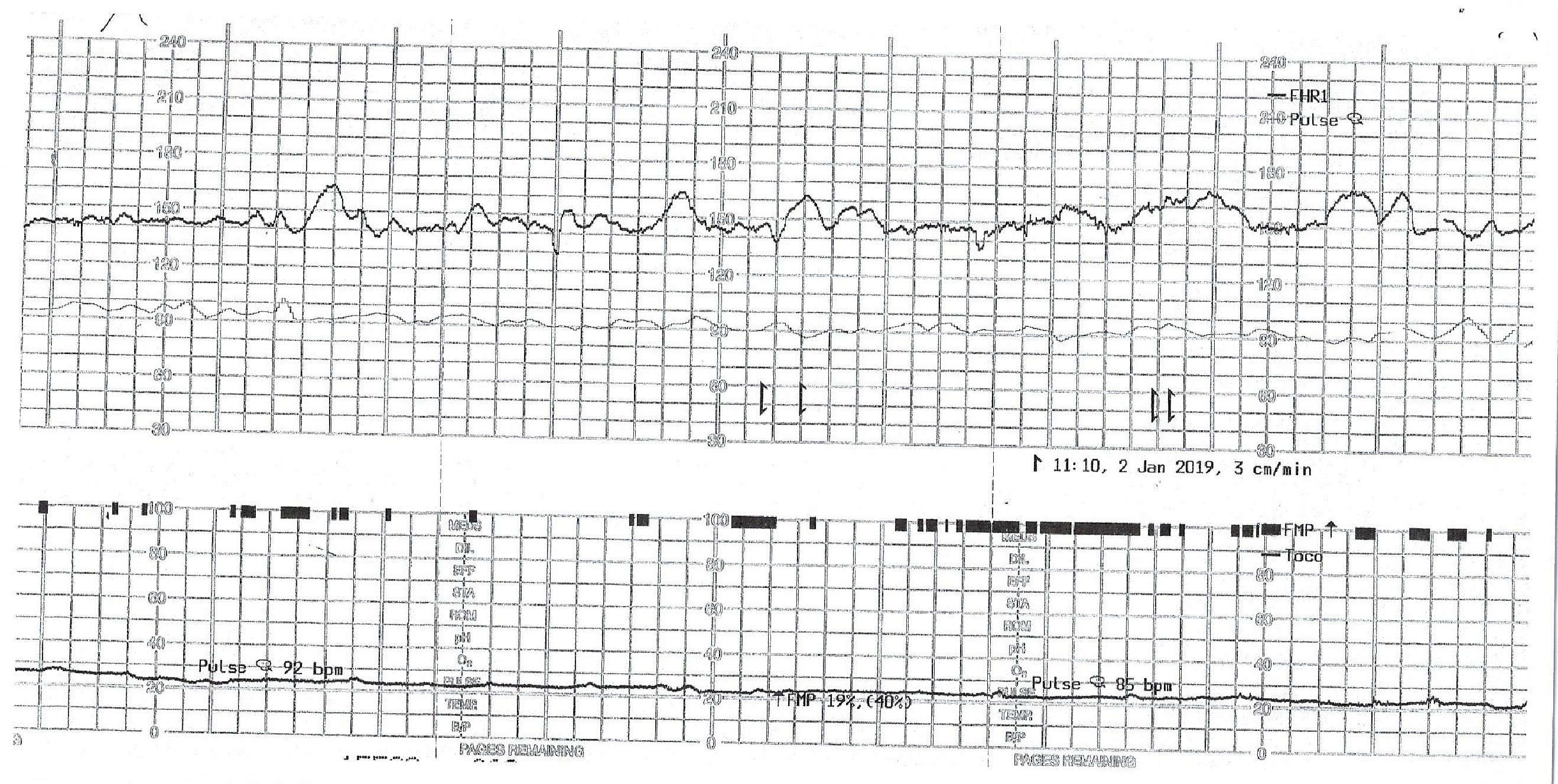
Nonstress Test. Results of a nonstress test reveal fetal heart rate tracing, fetal movement, and contraction tracing.
Contributed by O Umana, MD
References
Qin M, Xu Y, Liang Y, Sun T. A wearable fetal movement detection system for pregnant women. Frontiers in medicine. 2023:10():1160373. doi: 10.3389/fmed.2023.1160373. Epub 2023 Jul 24 [PubMed PMID: 37554507]
Level 2 (mid-level) evidenceDas R, Jana N, Arora N, Sengupta S. Ultrasound assessment of fetal hearing response to vibroacoustic stimulation. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians. 2020 Jul:33(14):2326-2332. doi: 10.1080/14767058.2018.1548600. Epub 2019 Jan 8 [PubMed PMID: 30618302]
Kapaya H, Almeida J, Karouni F, Anumba D. Management of reduced fetal movement: A comparative analysis of two audits at a tertiary care clinical service. European journal of obstetrics, gynecology, and reproductive biology. 2020 May:248():128-132. doi: 10.1016/j.ejogrb.2020.03.040. Epub 2020 Mar 18 [PubMed PMID: 32203823]
Level 2 (mid-level) evidenceNational Guideline Alliance (UK). Fetal movement monitoring: Antenatal care: Evidence review P. 2021 Aug:(): [PubMed PMID: 34524742]
Einspieler C, Prayer D, Marschik PB. Fetal movements: the origin of human behaviour. Developmental medicine and child neurology. 2021 Oct:63(10):1142-1148. doi: 10.1111/dmcn.14918. Epub 2021 May 10 [PubMed PMID: 33973235]
Association of Women’s Health, Obstetric and Neonatal Nurses. Decreased Fetal Movement: AWHONN Practice Brief #20. Nursing for women's health. 2024 Feb:28(1):e1-e3. doi: 10.1016/j.nwh.2023.11.004. Epub 2023 Dec 21 [PubMed PMID: 38127050]
Tsakiridis I, Zerva C, Mamopoulos A, Kalogiannidis I, Athanasiadis A, Dagklis T. Maternal perception of fetal movements: onset and associated factors. Journal of perinatal medicine. 2022 Nov 25:50(9):1174-1179. doi: 10.1515/jpm-2021-0606. Epub 2022 Jul 4 [PubMed PMID: 35779269]
Flenady V, Ellwood D, Bradford B, Coory M, Middleton P, Gardener G, Radestad I, Homer C, Davies-Tuck M, Forster D, Gordon A, Groom K, Crowther C, Walker S, Foord C, Warland J, Murphy M, Said J, Boyle F, O'Donoghue K, Cronin R, Sexton J, Weller M, McCowan L. Beyond the headlines: Fetal movement awareness is an important stillbirth prevention strategy. Women and birth : journal of the Australian College of Midwives. 2019 Feb:32(1):1-2. doi: 10.1016/j.wombi.2018.12.001. Epub 2018 Dec 15 [PubMed PMID: 30563769]
Hayes DJL, Dumville JC, Walsh T, Higgins LE, Fisher M, Akselsson A, Whitworth M, Heazell AEP. Effect of encouraging awareness of reduced fetal movement and subsequent clinical management on pregnancy outcome: a systematic review and meta-analysis. American journal of obstetrics & gynecology MFM. 2023 Mar:5(3):100821. doi: 10.1016/j.ajogmf.2022.100821. Epub 2022 Dec 5 [PubMed PMID: 36481411]
Level 1 (high-level) evidenceWarrander LK, Batra G, Bernatavicius G, Greenwood SL, Dutton P, Jones RL, Sibley CP, Heazell AE. Maternal perception of reduced fetal movements is associated with altered placental structure and function. PloS one. 2012:7(4):e34851. doi: 10.1371/journal.pone.0034851. Epub 2012 Apr 16 [PubMed PMID: 22523561]
Frøen JF. A kick from within--fetal movement counting and the cancelled progress in antenatal care. Journal of perinatal medicine. 2004:32(1):13-24 [PubMed PMID: 15008381]
Bellussi F, Po' G, Livi A, Saccone G, De Vivo V, Oliver EA, Berghella V. Fetal Movement Counting and Perinatal Mortality: A Systematic Review and Meta-analysis. Obstetrics and gynecology. 2020 Feb:135(2):453-462. doi: 10.1097/AOG.0000000000003645. Epub [PubMed PMID: 31923063]
Level 1 (high-level) evidenceMiller DA, Rabello YA, Paul RH. The modified biophysical profile: antepartum testing in the 1990s. American journal of obstetrics and gynecology. 1996 Mar:174(3):812-7 [PubMed PMID: 8633648]
Haws RA, Yakoob MY, Soomro T, Menezes EV, Darmstadt GL, Bhutta ZA. Reducing stillbirths: screening and monitoring during pregnancy and labour. BMC pregnancy and childbirth. 2009 May 7:9 Suppl 1(Suppl 1):S5. doi: 10.1186/1471-2393-9-S1-S5. Epub 2009 May 7 [PubMed PMID: 19426468]
Level 1 (high-level) evidence