Introduction
Hip fractures are common injuries, especially seen in the elderly in the emergency setting. These fractures are also seen in young patients who participate in athletics or experience high-energy trauma. Immediate diagnosis and management are required to prevent threatening joint complications.[1] In the United States, the economic burden of hip fractures is among the top 20 most expensive diagnoses, with approximately US $20 billion spent on the management of this injury.[2][3][4] Approximately 300,000 cases of hip fractures are estimated to occur annually in the United States by the year 2030.[5]
Femoral neck fractures are a specific type of intracapsular hip fracture. The femoral neck connects the femoral shaft with the femoral head. The hip joint is the articulation of the femoral head with the acetabulum. The junctional location makes the femoral neck prone to fracture. The blood supply of the femoral head is an essential consideration in displaced fractures, as it runs along the femoral neck.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Femoral neck fractures are associated with low energy falls in the elderly. In younger patients sustaining a femoral neck fracture, the cause is usually secondary to high-energy trauma such as a substantial height or motor vehicle accidents.[6][7] Risk factors for femoral neck fractures include female sex, decreased mobility, and low bone density.[8][9][8]
Epidemiology
Approximately 1.6 million hip fractures occur annually. Seventy percent of all hip fractures occur in women. Hip fracture risk increases exponentially with age and is more common in White women.[7][10]
Pathophysiology
The chief source of vascular supply to the femoral head is the medial femoral circumflex artery, which runs under the quadratus femoris. Displaced fractures of the femoral neck put the blood supply at risk, usually tearing the ascending cervical branches that stem off the arterial ring supply formed by the circumflex arteries. This may compromise fracture healing, inevitably leading to non-union or osteonecrosis.[11] This is most important when considering the younger population that sustains this fracture, for which arthroplasty would be inappropriate.[12] In patients treated via open reduction internal fixation, avascular necrosis is the most common complication.[13]
History and Physical
In the majority of cases, the patient has had recent trauma. In cases of dementia or cognitive impairment, the history may be scant without the report of any trauma. Obtaining an account from the nursing home or health aides is crucial. The nursing aides should be questioned about any recent falls and changes in cognition over the past few days. The patient often reports pain with decreased hip range of motion. In nondisplaced fractures, there may be no deformity. However, displaced fractures may present with a shortened and externally rotated lower limb.
The patient history varies depending on the mechanism of injury. The following should be obtained during the history and physical examination:
- Low-energy trauma: the mechanism is essential, and the events surrounding the fall should be questioned to rule out a possible syncopal cause.
- High energy trauma: Follow the Adult Trauma Life Support protocol when indicated. Assess for any non-orthopedic emergent injuries first and then ipsilateral injuries, including femur fracture or knee injury. For high vertical falls, inspect the ankle for any abnormalities.
- Important pertinent medical history: Baseline function and activity level, use of ambulatory aids before the injury, blood thinners, history of cancer, pulmonary embolism, and deep venous thrombosis.
Evaluation
The clinician should perform a complete neurovascular examination of the affected extremity. The following imaging should be ordered when indicated:
- Plain radiographs: anterior-posterior (AP) pelvis, AP and lateral hip, AP and lateral femur, AP and lateral knee.
- Computed tomography scan: helps classify the fracture pattern or delineate a subtle fracture line. CT is part of the trauma assessment and can be extended to include the femoral neck.
- Magnetic resonance imaging (MRI): not generally used in the acute setting but may be used to evaluate for femoral neck stress fractures.
Medical assessment should include basic labs (complete blood count, basic metabolic panel, and prothrombin time/international normalized ratio, if applicable) as well as a chest radiograph and an electrocardiogram. Older adults with known or suspected cardiac disease may benefit from preoperatively cardiology evaluation. Preoperative medical optimization is vital in the geriatric population.
Many classifications for femoral neck fracture exist, including the most common clinical classifications by Garden and Pauwel, which include the following:
[12]The Garden Classification
- Type I: Incomplete fracture, valgus impacted, nondisplaced
- Type II: Complete fracture, nondisplaced
- Type III: Complete fracture, partially displaced
- Type IV: Complete fracture, fully displaced [12][14]
The Garden classification is the most commonly used system to communicate the type of fracture. For treatment, it is often simplified as nondisplaced (types 1 and 2) versus displaced (types 3 and 4).[14]
Pauwel Classification
The Pauwel classification also includes the inclination angle of the fracture line relative to the horizontal. Higher angles and more vertical fractures exhibit greater instability due to higher shear force. These fractures also have a higher risk of osteonecrosis postoperatively.
- Type I: less than 30°
- Type II: 30° to 50°
- Type III: greater than 50°
Treatment / Management
Nonoperative
Nonoperative management for these fractures is rarely the treatment course. Nonoperative treatment is potentially useful only for non-ambulatory, comfort-care, or extremely high-risk patients.
Operative
Young patients with femoral neck fractures will require treatment with emergent open reduction internal fixation.[6][15] Vertically oriented fractures such as Pauwel III-type fractures are more common in younger and high-energy trauma patients. A sliding hip screw is biomechanically more stable for these fracture patterns. In younger patients with displaced fractures, the goal is to achieve anatomic reduction through emergent open reduction and internal fixation.[15](A1)
Nondisplaced fractures are treated typically with percutaneous cannulated screws or a sliding hip screw. However, there is a higher rate of avascular necrosis with the use of a sliding hip screw (9%) compared to cannulated screws (4%).[16](A1)
With displaced fractures of the femoral neck in older adult patients, the treatment depends on the patient's baseline activity level and age. Less active individuals may receive a hemiarthroplasty.[17] More active individuals are treated with total hip arthroplasty. Total hip arthroplasty is a more durable procedure, but it also carries a higher risk of dislocation compared with a hemiarthroplasty.[15][18][19](A1)
Summary of Operative Methods
Young patients (younger than 60):
- Open-reduction internal fixation
Older adults:
- Nondisplaced
- Percutaneous cannulated screws or sliding hip screw
- Displaced
- Hemiarthroplasty: less active patients
- Total hip arthroplasty: active patients
Differential Diagnosis
The differential diagnosis includes:
- Hip dislocation: displacement of the femoral head from the acetabulum
- Intertrochanteric fracture: the fracture line is more distal and lies between the greater and lesser trochanter
- Subtrochanteric fracture: the fracture line is within 5 cm distal to the lesser trochanter
- Femur fracture: the fracture line is within the femoral diaphysis
- Osteoarthritis: pain that is more chronic. Usually, patients complain of groin pain. Pain that worsens with activity or stairs
Prognosis
After femoral neck fracture, there is a 6% in-house mortality rate. Furthermore, there is a 1-year mortality rate between 20% and 30%, with the highest risk within the first 6 months.[2][20] Overall, with hip fractures, 51% will resume independent ambulation while 22% will remain nonambulatory.[21]
Complications
Complications include:
- Avascular necrosis increased risk factor with increased initial displacement and failure to obtain an anatomical reduction [13]
- Nonunion
- Dislocation is increased with total hip arthroplasty surgery
Postoperative and Rehabilitation Care
Patients treated with a total hip arthroplasty or hemiarthroplasty should be weight-bearing as tolerated postoperatively.[22] They should observe hip precautions depending on the surgical approach used for the procedures. Deep venous thrombosis prophylaxis should be started during the perioperative period and continued for 4 to 6 weeks postoperatively. Physical therapy should begin immediately after surgery.
Deterrence and Patient Education
Preoperatively, patients should be educated on the limitations on hip movements they may have due to the prosthesis. In addition, emphasis should be placed on proper activities of daily living such as sitting on the toilet, climbing stairs, and sitting and standing from a seated position after surgery.
Pearls and Other Issues
Pearls include:
- Young patients with femoral neck fractures should be treated emergently for stabilization via open reduction internal fixation after completion of imaging and the ATLS protocol as needed. With more vertically oriented fractures such as Pauwel III, a sliding hip screw is biomechanically stable.
- Older adults should be seen and evaluated by medical services and optimized as needed.
- Displacement and baseline activity dictate the treatment plan.
- A nondisplaced fracture may have surgical treatment with screws in situ.
- A displaced fracture may be treated with a total hip arthroplasty in active individuals or a hemiarthroplasty in less active individuals.
Enhancing Healthcare Team Outcomes
Most patients with a femoral neck fracture will present to the emergency department. Obtain the proper injury radiographs and history from the patient. With the identification of a femoral neck injury, the patient should immediately become non–weight-bearing. From a triage standpoint, younger patients who benefit from joint-sparing fixation should promptly receive a referral to orthopedics.
For older adults, it is vital to identify medical comorbidities. These patients should be medically optimized before operative treatment. Women often experience painful urination, so the placement of a Foley catheter for comfort within the emergency department may be necessary and discontinued postoperatively with ambulation. In the orthopedic unit, it is essential to note the operative approach used because it dictates the postoperative precautions the patient should maintain. For example, with a posterior approach, the patient typically uses an abduction pillow at night. Posterior precautions also include not crossing the legs, leaning forward while seated, and letting the toes point inward. These precautions help prevent dislocation. Postoperative physical therapy and mobilization are essential to help patients return to function. Patients who experience a femoral neck fracture can benefit from preoperative evaluation and postoperative management of their comorbidities. This interprofessional care team may include orthopedics, geriatrics, internal medicine, trauma surgery, anesthesia, cardiology, operating room and orthopedic nurses, physical therapists, and any other subspecialty that may help manage the patient’s comorbidities.
Media
(Click Image to Enlarge)
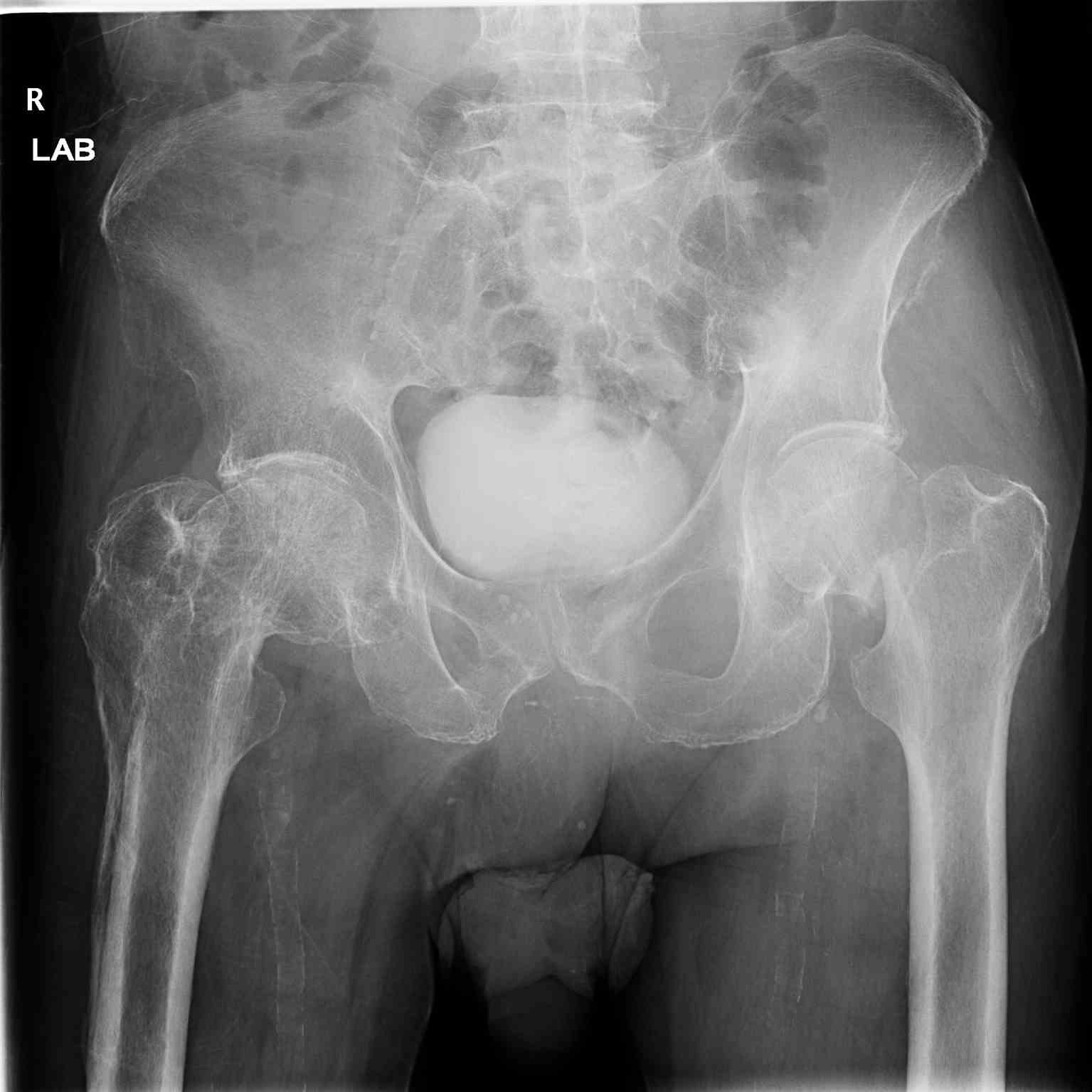
Pelvic Radiograph, Right Hip Fracture.
Contributed by S Dulebohn, MD
(Click Image to Enlarge)

Right Hip Arthroplasty, Pelvic Radiograph.
Contributed by S Dulebohn, MD
(Click Image to Enlarge)
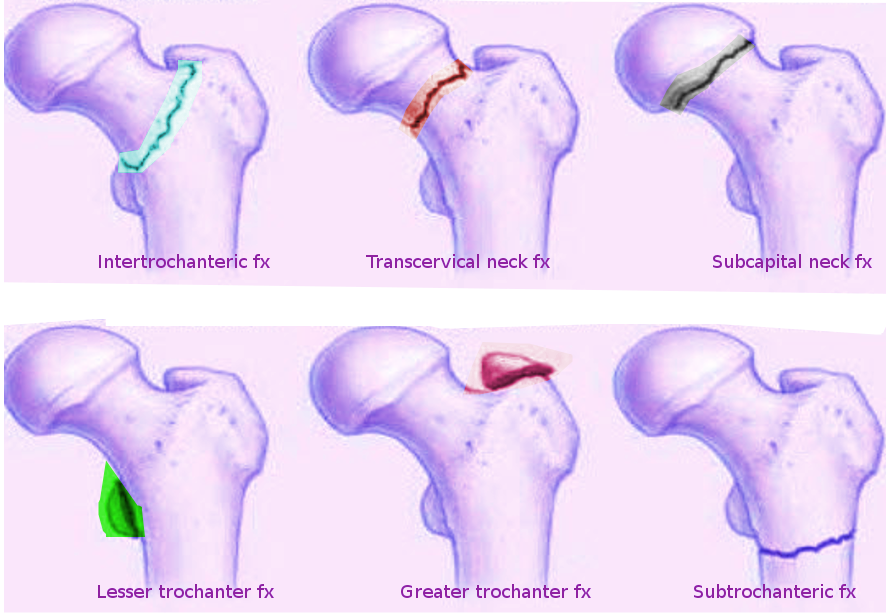
Femoral Hip Fractures. This image shows the different types of extracapsular (intertrochanteric, lesser trochanteric, greater trochanteric, and subtrochanteric) and intracapsular (transcervical and subcapital) fractures.
Contributed by S Bhimji MD
(Click Image to Enlarge)

Femoral Neck fracture Contributed by Jillian Kazley, MD
(Click Image to Enlarge)
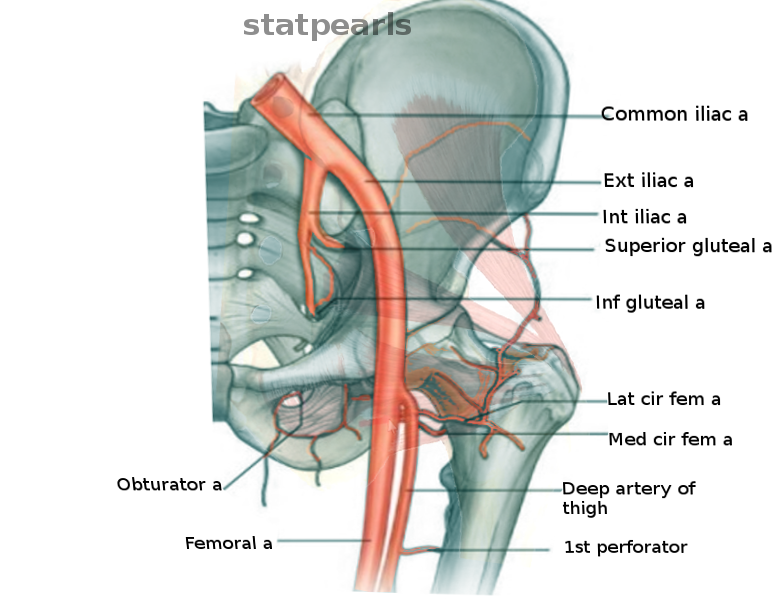
Hip arteries Image courtesy S Bhimji MD
References
Crist BD, Eastman J, Lee MA, Ferguson TA, Finkemeier CG. Femoral Neck Fractures in Young Patients. Instructional course lectures. 2018 Feb 15:67():37-49 [PubMed PMID: 31411399]
Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hip fractures in the United States. JAMA. 2009 Oct 14:302(14):1573-9. doi: 10.1001/jama.2009.1462. Epub [PubMed PMID: 19826027]
Shimizu T, Miyamoto K, Masuda K, Miyata Y, Hori H, Shimizu K, Maeda M. The clinical significance of impaction at the femoral neck fracture site in the elderly. Archives of orthopaedic and trauma surgery. 2007 Sep:127(7):515-21 [PubMed PMID: 17541613]
Level 2 (mid-level) evidenceMiyamoto RG, Kaplan KM, Levine BR, Egol KA, Zuckerman JD. Surgical management of hip fractures: an evidence-based review of the literature. I: femoral neck fractures. The Journal of the American Academy of Orthopaedic Surgeons. 2008 Oct:16(10):596-607 [PubMed PMID: 18832603]
Brox WT, Roberts KC, Taksali S, Wright DG, Wixted JJ, Tubb CC, Patt JC, Templeton KJ, Dickman E, Adler RA, Macaulay WB, Jackman JM, Annaswamy T, Adelman AM, Hawthorne CG, Olson SA, Mendelson DA, LeBoff MS, Camacho PA, Jevsevar D, Shea KG, Bozic KJ, Shaffer W, Cummins D, Murray JN, Donnelly P, Shores P, Woznica A, Martinez Y, Boone C, Gross L, Sevarino K. The American Academy of Orthopaedic Surgeons Evidence-Based Guideline on Management of Hip Fractures in the Elderly. The Journal of bone and joint surgery. American volume. 2015 Jul 15:97(14):1196-9. doi: 10.2106/JBJS.O.00229. Epub [PubMed PMID: 26178894]
Protzman RR, Burkhalter WE. Femoral-neck fractures in young adults. The Journal of bone and joint surgery. American volume. 1976 Jul:58(5):689-95 [PubMed PMID: 932067]
Level 3 (low-level) evidenceJohnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporosis international : a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. 2006 Dec:17(12):1726-33 [PubMed PMID: 16983459]
Cummings SR, Black DM, Nevitt MC, Browner W, Cauley J, Ensrud K, Genant HK, Palermo L, Scott J, Vogt TM. Bone density at various sites for prediction of hip fractures. The Study of Osteoporotic Fractures Research Group. Lancet (London, England). 1993 Jan 9:341(8837):72-5 [PubMed PMID: 8093403]
Level 1 (high-level) evidenceLakstein D, Hendel D, Haimovich Y, Feldbrin Z. Changes in the pattern of fractures of the hip in patients 60 years of age and older between 2001 and 2010: A radiological review. The bone & joint journal. 2013 Sep:95-B(9):1250-4. doi: 10.1302/0301-620X.95B9.31752. Epub [PubMed PMID: 23997141]
Level 2 (mid-level) evidenceKoval KJ, Zuckerman JD. Hip Fractures: I. Overview and Evaluation and Treatment of Femoral-Neck Fractures. The Journal of the American Academy of Orthopaedic Surgeons. 1994 May:2(3):141-149 [PubMed PMID: 10709002]
Level 3 (low-level) evidenceBarney J, Piuzzi NS, Akhondi H. Femoral Head Avascular Necrosis. StatPearls. 2026 Jan:(): [PubMed PMID: 31536264]
Li M, Cole PA. Anatomical considerations in adult femoral neck fractures: how anatomy influences the treatment issues? Injury. 2015 Mar:46(3):453-8. doi: 10.1016/j.injury.2014.11.017. Epub 2014 Nov 26 [PubMed PMID: 25549821]
Dedrick DK, Mackenzie JR, Burney RE. Complications of femoral neck fracture in young adults. The Journal of trauma. 1986 Oct:26(10):932-7 [PubMed PMID: 3773004]
Level 3 (low-level) evidenceKazley JM, Banerjee S, Abousayed MM, Rosenbaum AJ. Classifications in Brief: Garden Classification of Femoral Neck Fractures. Clinical orthopaedics and related research. 2018 Feb:476(2):441-445. doi: 10.1007/s11999.0000000000000066. Epub [PubMed PMID: 29389800]
Bhandari M, Devereaux PJ, Swiontkowski MF, Tornetta P 3rd, Obremskey W, Koval KJ, Nork S, Sprague S, Schemitsch EH, Guyatt GH. Internal fixation compared with arthroplasty for displaced fractures of the femoral neck. A meta-analysis. The Journal of bone and joint surgery. American volume. 2003 Sep:85(9):1673-81 [PubMed PMID: 12954824]
Level 1 (high-level) evidenceFixation using Alternative Implants for the Treatment of Hip fractures (FAITH) Investigators. Fracture fixation in the operative management of hip fractures (FAITH): an international, multicentre, randomised controlled trial. Lancet (London, England). 2017 Apr 15:389(10078):1519-1527. doi: 10.1016/S0140-6736(17)30066-1. Epub 2017 Mar 3 [PubMed PMID: 28262269]
Level 1 (high-level) evidenceRogmark C, Leonardsson O. Hip arthroplasty for the treatment of displaced fractures of the femoral neck in elderly patients. The bone & joint journal. 2016 Mar:98-B(3):291-7. doi: 10.1302/0301-620X.98B3.36515. Epub [PubMed PMID: 26920951]
Avery PP, Baker RP, Walton MJ, Rooker JC, Squires B, Gargan MF, Bannister GC. Total hip replacement and hemiarthroplasty in mobile, independent patients with a displaced intracapsular fracture of the femoral neck: a seven- to ten-year follow-up report of a prospective randomised controlled trial. The Journal of bone and joint surgery. British volume. 2011 Aug:93(8):1045-8. doi: 10.1302/0301-620X.93B8.27132. Epub [PubMed PMID: 21768626]
Level 2 (mid-level) evidenceHedbeck CJ, Enocson A, Lapidus G, Blomfeldt R, Törnkvist H, Ponzer S, Tidermark J. Comparison of bipolar hemiarthroplasty with total hip arthroplasty for displaced femoral neck fractures: a concise four-year follow-up of a randomized trial. The Journal of bone and joint surgery. American volume. 2011 Mar 2:93(5):445-50. doi: 10.2106/JBJS.J.00474. Epub [PubMed PMID: 21368076]
Level 1 (high-level) evidenceEgol KA, Koval KJ, Zuckerman JD. Functional recovery following hip fracture in the elderly. Journal of orthopaedic trauma. 1997 Nov:11(8):594-9 [PubMed PMID: 9415867]
Miller CW. Survival and ambulation following hip fracture. The Journal of bone and joint surgery. American volume. 1978 Oct:60(7):930-4 [PubMed PMID: 701341]
Level 2 (mid-level) evidenceKoval KJ, Friend KD, Aharonoff GB, Zukerman JD. Weight bearing after hip fracture: a prospective series of 596 geriatric hip fracture patients. Journal of orthopaedic trauma. 1996:10(8):526-30 [PubMed PMID: 8915913]