Introduction
In contrast to other techniques, the deep plane facelift, initially described by Dr. Sam Hamra in 1990, utilizes a composite skin and fascial flap raised in a plane below the superficial musculoaponeurotic layer of the midface.[1] This technique improves the vascularity of the flap, permits repositioning of the malar fat pads to address deep nasolabial folds, and allows direct lysis of key facial retaining ligaments. The result is a mid- and lower facelift with a low risk of skin complications and maximum mobilization of the superficial soft tissues. By placing suspension sutures only at the level of the fascia, the deep plane technique creates a tension-free skin closure and ensures long-term results.
Additionally, the deep plane technique provides access to address the pseudo-herniated buccal fat that contributes to jowling. Although the debate continues regarding which of the myriad rhytidectomy options is most appropriate for a given patient, a properly executed deep-plane facelift can produce dramatic and sustainable rejuvenation of the lower and midface (see Image. Deep-Plane Facelift).[2][3]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
A successful deep-plane rhytidectomy without operative complications can be performed only if the surgeon has a thorough understanding of facial anatomy and the physiology of facial aging. Understanding the process of facial aging informs the maneuvers the surgeon performs during facelifting, while knowledge of facial anatomy is essential to ensure access to the regions requiring correction while avoiding inadvertent injury to nerves, blood vessels, salivary glands, muscles, and other structures.
Fascial Planes of the Face
The most important anatomical principle to grasp when undertaking facial surgery is that of the relationship of the fascial planes to one another (see Image. Fascial Planes of the Face). Beneath the skin lies the superficial musculoaponeurotic system (SMAS), first described in 1976 by Mitz and Peyronie, which provides the primary soft-tissue support in the lateral mid- and lower face.[4] The SMAS has been the target of most facelift techniques since the 1970s, as its repositioning and suspension into a more youthful position typically provide the enduring rejuvenation that rhytidectomy aims to achieve.
This layer is contiguous with the superficial cervical fascia and the platysma in the neck and lower face, the muscles of facial expression in the medial midface, and the temporoparietal fascia and frontalis muscle in the upper face. The parotidomasseteric fascia underlies the SMAS and is contiguous with the deep cervical fascia in the neck, enveloping the parotid gland, the facial nerve, the masseter muscle, and the buccal fat pad. Because the facial nerve lies within the parotidomasseteric fascia, it can be reliably encountered deep to the SMAS and deep to the muscles of facial expression. However, this plane can be challenging to identify in the medial midface, where the fascial landmarks largely give way to adipose tissue. Here, a nerve stimulator can be an invaluable aid to the surgeon.
Facial Innervation
Owing to their deeper location within the face, the mentalis, buccinator, and levator anguli oris muscles are innervated from their superficial surfaces, while the other muscles controlled by the facial nerve are innervated from their deep surfaces.[5] Buccal branches of the facial nerve run superficial to the masseter muscle and the buccal fat pad; injury to these nerves will affect the elevators of the oral commissure and upper lip, resulting in less movement when smiling and potential droop of the corner of the mouth. Injury to the marginal mandibular or cervical branches of the facial nerve will weaken the oral commissure and lower lip depression, making the lower lip appear crooked during smiling or protrusion.
If the frontal branch of the facial nerve is injured, it will cause weakness of the ipsilateral forehead and decreased brow elevation with potential brow ptosis. Zygomatic branch injury most notably results in slow or incomplete eye closure. Despite the presence of multiple facial nerve branches within the plane of dissection, the nerve most commonly injured during rhytidectomy is the great auricular nerve, which runs in a subplatysmal plane roughly 1 cm posterior to the external jugular vein and crosses the sternocleidomastoid muscle approximately 6.5 cm inferior to the external auditory canal.[6] The "deep plane," whose dissection is fundamental to this facelift technique, is located between the SMAS and the parotidomasseteric fascia in the lateral midface, but superficial to the muscles of facial expression medially.
Facial Aging Physiology
During facial aging, sagging affects select muscles of facial expression, including the orbicularis oculi, which contributes to festoons, and the platysma, which produces vertical neck bands; however, the most prominent visible changes arise from fat atrophy and descent, leading to tear troughs, deep nasolabial folds, and jowls, along with progressive bony resorption.[7][8] Involutional changes of the facial skeleton, although not routinely addressed during aging face surgery, include bone loss at the inferolateral and superomedial orbit that creates a hollowed ocular appearance, reduction in maxillary prominence and height that deepens nasolabial folds, thins the upper vermilion, lengthens the upper cutaneous lip, and contributes to nasal tip ptosis, and loss of mandibular angle definition that diminishes jawline contour.[9]
Deep Plane Facelift Maneuvers
The deep plane facelift repositions the SMAS and malar fat pads and provides access for reduction of the buccal fat pads, thereby reversing several prominent soft-tissue manifestations of aging. Additional midfacial rejuvenation follows reduction and repositioning of the lower eyelid fat and muscle, frequently performed concurrently with the deep-plane facelift in the composite facelift described by Hamra.[10][11] Optimal mobilization of facial soft tissues depends on the release of the osteocutaneous retaining ligaments that tether the dermis to the periosteum. The zygomatic ligament, the strongest of these structures, along with the maxillary, masseteric, and mandibular ligaments, must be divided during rhytidectomy.[12] Failure to release these ligaments severely limits correction of nasolabial folds, marionette lines, tear troughs, and jowls.[13][14] Please see StatPearls' companion resource, "Rhytidectomy," for further information on facial anatomy and the physiology of facial aging.
Indications
Areas of the face that the deep-plane facelift technique can address include:
- Malar fat pad descent
- Nasolabial folds
- Jowling, due to pseudo-herniated buccal fat and descent of the SMAS just posterior to the mandibular retaining ligaments
- Festoons (malar mounds); hammocks of lax skin and orbicularis oculi muscle below the orbital rim may be reduced with a composite facelift
- Facial dimples caused by fascial bands from the zygomaticus major muscle (minor dimple) or a bifid zygomaticus major muscle (major dimple)
Contraindications
Increased Risk of Hematoma
Factors that increase the risk of hematoma include:
- Patients taking anticoagulants, antiplatelet agents, and nonsteroidal anti-inflammatory drugs
- Patients taking herbal medications and supplements (eg, chondroitin, ephedra, echinacea, glucosamine, ginkgo biloba, goldenseal, milk thistle, ginseng, kava, turmeric, and garlic)
- Men are twice as likely to experience a hematoma as women (up to 8%)
- Poorly controlled hypertension, which can be problematic intraoperatively and postoperatively [14]
Active Smokers
Skin flap necrosis has historically been more common in smokers undergoing facelifting than in nonsmokers; however, this does not appear to be a significant problem with the deep plane technique, given the increased thickness and improved vascularity of the flap compared with SMAS flap techniques.[15]
Body Dysmorphic Disorder
Body dysmorphic disorder is a psychiatric condition classified as an obsessive-compulsive–related disorder, wherein patients exhibit abnormal preoccupation with perceived cosmetic defects that are either minute or absent to the examiner. Moreover, patients with body dysmorphic disorder tend to have poor satisfaction following surgery and a higher rate of aggression and litigation toward surgeons. The prevalence of body dysmorphic disorder may be as high as 13% in patients who present for facial plastic surgery consultation.[16][17] When the severity of the patient's aesthetic concerns seems disproportionately large compared to the surgeon's perception of the deficit, or if the patient has tried to convince multiple surgeons to operate on the reported problems, a psychiatry consultation should be strongly considered.
Equipment
Preoperative Equipment
Local anesthesia (eg, a 1:1 mix of 1% lidocaine with 1:100,000 epinephrine and 0.5% bupivacaine with 1:200,000 epinephrine) can be injected into the planned incision lines. Tumescent anesthesia may be an option in the areas of proposed skin flap elevation. An example recipe for tumescent solution is 1 L of normal saline, to which are added 50 cc of plain 1% lidocaine, 50 cc of plain 0.5% bupivicaine, 50 cc of 8.4% sodium bicarbonate, 1 g of tranexamic acid, and 1 cc of 1:1000 epinephrine. This solution may be injected using a large syringe and a blunt cannula, or with a purpose-built pump.
Topical antiseptic (eg, povidone-iodine paint or chlorhexidine), depending on surgeon preference and patient allergies
Intraoperatively
Intraoperative equipment includes:
- Bipolar cautery
- Scalpel (#15 and #10 blades)
- Multi-prong retractors (Padgett, Freeman, Joseph)
- Facelift scissors (Gorney-Freeman, Castañares, Goldman-Fox)
- Forceps (Adson-Brown, Castroviejo, DeBakey)
- Needle holders (Mayo-Hegar, Halsey, Webster, Castroviejo)
- Trepsat dissector
- Lighted retractor (Ferreira)
- Closed suction drains with bulbs
- Suture for SMAS suspension (3-0 or 4-0 polydioxanone or polyglactin) and skin closure (4-0 and 5-0 nylon or polypropylene, poliglecaprone for optional deep dermal sutures)
- Stapler (may be used for closure of hair-bearing scalp)
Postoperatively
Equipment utilized postoperatively includes:
- Antibiotic ointment (bacitracin or similar)
- Compressive dressing material
Personnel
Team members who are typically involved in a deep plane facelift procedure include:
- Surgeon
- Anesthesiologist
- Surgical scrub technician
- Operating room nurse (circulator)
- A surgical assistant (useful for retracting, managing intraoperative bleeding, and cutting suture, but is not mandatory)
Preparation
Before a deep plane facelift is performed, several steps should be undertaken, including optimizing the patient's medical status, identifying preoperative facial anatomic structures and surgical incision sites, and ensuring appropriate anesthesia.
Medical Clearance
Risk stratification and medical optimization for general anesthesia are essential for patient safety. Patients with a history of depression should be counseled that depression may recur or worsen during the postoperative period.[18]
Neurological Examination
Trigeminal and facial nerve function should be documented preoperatively. Patients will often experience temporary, self-limited facial hypesthesia postoperatively. Postoperative numbness of the auricular lobule or weakness of the face is abnormal.
Preoperative Photography
Images in frontal, three-quarter, and lateral views will document ear position and shape, facial asymmetries, and hairline contour. Photographs taken with facial expressions are used to establish preoperative facial nerve function. The "chin-down" position is very useful for assessing the effectiveness of a facelift on the cervicomental angle and the neck in general.
Patient Marking
The incisions are planned to run within or just beneath the temporal hair tuft, down along the anterior edge of the root of the helix, and then either just medial to the free margin of the tragus, for women, or anterior to the auricle, for men (see Images. Blair Rhytidectomy and Deep Plane Rhytidectomy).
The male incision trades some scar camouflage to prevent hair-bearing skin from the beard being advanced onto the tragus, which would appear unnatural. The incision proceeds around the lobule and up onto the posterior auricle, roughly one-third of the distance from the postauricular sulcus to the helical rim, so that the scar contracts into the depth of the sulcus with healing. The incision then runs across the shortest distance between the posterior border of the auricle and the hair-bearing scalp, typically at the level of Darwin's tubercle. The final segment of the incision may travel along the posterior hairline or within the hair-bearing scalp itself (see Image. Blair Rhytidectomy Incision).
Important landmarks are identified, including the trajectory of the frontal branch of the facial nerve (following a line running from a point 0.5 cm inferior to the tragus to a point 1.5 cm superior to the lateral brow) and the deep plane entry line (a diagonal line from angle of the mandible to lateral canthus) (see Images. Pitanguy Line and Rhytidectomy Incisions).[19]
Anesthesia
Although the deep plane facelift may be performed entirely under local anesthesia, general anesthesia or intravenous adjuncts (eg, propofol) are helpful to maintain patient comfort. Muscle relaxants are avoided to allow intraoperative monitoring or stimulation of the facial nerve. Local anesthesia is infiltrated along the proposed incision lines, and tumescent solution is infiltrated beneath the planned subcutaneous dissection area.
Prophylaxis
A single preoperative dose of intravenous antibiotics that cover skin flora should be given (eg, 1 g of cefazolin). Intravenous steroids (eg, 8 mg of dexamethasone) may reduce early postoperative swelling as well as postoperative nausea and vomiting.[20] Tranexamic acid, an antifibrinolytic drug, has also been reported to reduce bleeding, drainage output, and bruising, whether administered intravenously or injected as a component of the tumescent solution.[21]
Technique or Treatment
Since the original description of the deep plane rhytidectomy, several modifications have been described by various authors to improve rejuvenation of the midface, jawline, and neck.[7][22][23][24][25][13][26][27][28][29] Therefore, understanding the basic surgical principles for performing a safe, reproducible facelift using the contemporary deep-plane technique is essential.
The incisions described above are typically made with a #15 blade scalpel, although a #11 blade may be used if a fine zigzag pattern is desired along the temporal hair tuft. A subcutaneous flap is then developed with the knife and elevated with scissors, eg, Gorney-Freeman or Kaye facelift scissors, out to the deep-plane entry line between the malar eminence and the angle of the mandible (see Image. Facial Flap Development). Subcutaneous elevation should leave a thin layer of fat on the underside of the dermis and maintain a uniform thickness, which is facilitated with the use of a multiprong retractor to provide tension on the flap, an assistant to provide direct counter-tension, and transillumination of the skin to ensure uniform flap thickness and avoid perforation (see Image. Facial Flap Elevation). The skin of the preauricular area, the temporal region, the postauricular area, and the upper neck are all elevated in this manner.
Care is taken to avoid injury to the great auricular nerve and the external jugular vein just anterior to it, as they cross over the sternocleidomastoid muscle (see Image. Great Auricular Nerve). If a necklift accompanies the facelift, the subcutaneous plane may be used for it as well. However, some surgeons propose a benefit to limited subcutaneous elevation in the neck, instead preferring subplatysmal dissection. This technique is often referred to as a "preservation" rhytidectomy.[30]
The deep plane is then entered by incising the SMAS sharply, often with a #10 blade scalpel, along a line running from just above the angle of the mandible to the malar eminence (see Image. Rhytidectomy Incisions.). The composite skin/SMAS flap is then carefully elevated off the parotidomasseteric fascia using a combination of blunt and sharp dissection (see Image. Deep Plane Entry). The aforementioned scalpel and scissors are often employed alongside a Trepsat facelift elevator, the back end of a Bard-Parker scalpel handle, cotton-tipped applicators, and the surgeon's fingertip. A natural glide plane exists between the SMAS and the parotidomasseteric fascia.
The masseteric cutaneous ligaments, located at the anterior border of the masseter, are released sharply, and dissection is carried anteriorly towards the oral commissure until the surgeon reaches the nasolabial fold. Care must be taken to ensure that facial nerve branches, which lie along and within the floor of this dissection, are neither inadvertently elevated into the flap nor injured via traction, cautery, or division. The marginal mandibular branch runs in close proximity to the facial vein; if this vessel is injured, only extremely cautious application of cautery - if any - should be used. Direct pressure or a topical hemostatic agent may be safer options.
Elevation of the deep plane proceeds superiorly by developing a pocket superficial to the lateral orbicularis oculi muscle. Dissection continues inferomedially to identify the zygomaticus major muscle, which is then followed along its superficial surface to elevate the malar fat pad up into the flap and release the zygomatic cutaneous ligaments, also known as the patch of McGregor (see Image. Deep Plane Rhytidectomy). This maneuver not only protects the facial nerve branches that innervate the zygomaticus major from its deep surface but also produces midfacial lifting when the flap is suspended, thus effacing the nasolabial folds. Dissection continues inferiorly along the zygomatic muscles to the nasolabial fold, inferior to which the surgeon releases the mandibular retaining ligament, taking care to avoid injury to the marginal mandibular nerve and completing the midface release. Release of the mandibular retaining ligament is critical for the reduction of the jowls.
Furthermore, if excessive jowling is caused by buccal fat pseudo-herniation, it can be addressed at this time. With an assistant applying pressure to the buccal fat pad transorally, a conservative amount of buccal fat is then teased out and excised using bipolar cautery. Care is taken to avoid injury to the buccal branches of the facial nerve, which course over the superficial surface of the fat pad (see Image. Buccal Fat Pad Reduction).
Patients who desire periorbital rejuvenation may undergo a composite facelift, which adds upper- and lower-eyelid maneuvers to the deep-plane rhytidectomy. With this technique, a subciliary approach to lower blepharoplasty permits release of the arcus marginalis and fat transposition with the overlying orbital septum across the inferior orbital rim to efface the junction of the cheek and lower eyelid. The orbicularis oculi and zygomaticus major muscles are dissected away from the overlying and underlying tissues, keeping their innervation intact as well as the zygomaticus' origin and insertion. The muscles can then be suspended superiorly with the rest of the middle and lower facial soft tissues during the lift, using a transcanthal canthopexy, which suspends the lateral orbicularis oculi muscle to the lateral orbital periosteum via the lateral aspect of an upper blepharoplasty incision.[31] Composite rhytidectomy is a full-face rejuvenation procedure that typically includes browlifting and a necklift.
The SMAS flap is then suspended, working inferiorly to superiorly, with several half-mattress sutures (4-0 or 3-0 nylon, polypropylene, polydioxanone, or polyglactin) placed along the cuff of SMAS at the deep plane entry point and anchored to the parotid fascia and deep temporal fascia in a vertically oblique vector of about 60 degrees.[32]
After resuspension of the SMAS, the redundant skin is conservatively excised and suspended in a similar vector to the deep-plane flap, allowing for a tension-free skin closure (see Image. Face Lift Flap Tailoring). A combination of deep (4-0 polyglactin) and superficial (5-0 nylon or polypropylene) sutures is used for closure, with attention paid to preserving the continuity of the hairline, everting the skin edges, and excising bunched skin. Staples may be used to close the portions of the incision located within the hair-bearing scalp. A natural appearing preauricular hollow and tragus is created by thinning the skin before redraping the tragus and debulking the SMAS anterior to the tragal cartilage. A pixie ear deformity is avoided by ensuring a tension-free closure inferior to the lobule.
Before final skin closure, a small drain is inserted through a stab incision posterior to the occipital hairline and secured to a bulb suction. Alternatively, hemostatic nets may be used to control or minimize unwanted fluid collections.[33] Antibiotic ointment is applied to the incision line, and a compressive facelift dressing is placed to complete the procedure.
Complications
The well-vascularized flap created by deep-plane dissection decreases the risk of rhytidectomy-related healing complications; however, several complications may still arise.[34]
Hematomas
Hematomas occur in less than 2% of cases and must be addressed promptly to prevent infection, flap necrosis, skin expansion, or clinically significant blood loss (see Image. Upper Neck Hematoma). Prevention of hematomas requires meticulous intraoperative hemostasis as well as effective postoperative pain and nausea control, which will help to prevent hypertension and bleeding. Maintaining postoperative systolic blood pressure below 140 mm Hg has been shown to reduce the risk of hematoma formation.[35] Seromas occur in 4% of cases with deep-plane facelifts. Both hematomas and seromas require removal of the fluid, often with needle aspiration, and application of a pressure dressing. Recurrent or expanding hematomas are best managed in the operating room, where definitive hemostasis can be achieved more easily.
Skin Ischemia
Skin ischemia and sloughing occur in less than 1% of cases, most commonly in the preauricular region, which represents the distal aspect of the facial flap (see Image. Full-Thickness Skin Flap Necrosis). The rate of skin ischemia with deep-plane facelift is lower than with SMAS flap techniques, presumably because the deep-plane technique provides better flap vascularity. This complication is best managed with conservative wound care and minimal debridement, as necessary. Skin resurfacing may be required to reduce visible scarring, though this technique is often unnecessary.
Infections and Nerve Injury
Infections occur in less than 1% of deep-plane facelift cases but slightly over 1% in composite facelift cases. Facial nerve injury occurs in less than 1% of deep-plane facelifts, with permanent injury extremely uncommon (see Image. Rhytidectomy Complications). Despite the deep plane dissection, rates of motor nerve injury are largely consistent across facelifting techniques, with a slightly higher risk for composite rhytidectomy. In the vast majority of cases, no intervention is required, although contralateral botulinum toxin injection into the functional depressor labii inferioris muscle may improve lower lip symmetry during recovery.[36]
If facial nerve weakness is encountered immediately upon emergence from anesthesia, it may represent a nerve transection injury; however, facial nerve weakness is more likely the result of prolonged local anesthetic effect and should be given 12 to 24 hours to resolve before considering electrodiagnostic testing or facial nerve exploration and repair. Please see StatPearls' companion resource, "Facial Nerve Trauma," for further information. Furthermore, injury to the great auricular nerve occurs in up to 7% of cases. Great auricular nerve injury causes numbness in the inferior aspect of the auricle and the lobule, as well as the superolateral neck below and behind the pinna. These injuries may be permanent, but typically resolve spontaneously over a few weeks to a few months.
Pixie Ear Deformity
Pixie ear deformity is caused by excessive tension on the lobule during skin closure (see Image. Pixie Ear Deformity). Repairing a pixie ear deformity can be challenging, often requiring significant skin and soft-tissue rearrangement, with care taken to reposition the lobule superiorly and to avoid tension on the closure completely.[37]
Alopecia
Alopecia may be prevented with beveled incisions within hair-bearing areas and avoidance of cautery near hair follicles.
First Bite Syndrome
First bite syndrome is uncommon but may result from injury to and aberrant regrowth of sympathetic nerve fibers in and around the parotid gland. Botulinum toxin injections into the parotid gland may be helpful, although most instances of first bite syndrome are self-limited.[38]
Clinical Significance
The deep-plane facelift is a powerful surgical approach for restoring a youthful, rested appearance to the aging face, particularly when combined with neck lifting, as commonly performed in comprehensive facial rejuvenation (see Neck Rejuvenation). Compared with SMAS plication rhytidectomy, this approach is more invasive but offers the potential for more pronounced and durable aesthetic improvement in experienced hands, especially among older patients with significant soft-tissue descent.[39]
Successful outcomes with the deep plane facelift depend on careful patient evaluation and precise execution of a meticulous surgical technique. Adherence to sound anatomic principles and thoughtful operative planning supports safe, reliable, and satisfactory results for most patients undergoing this procedure.[40]
Enhancing Healthcare Team Outcomes
The deep plane facelift represents an advanced facial rejuvenation technique that elevates a composite skin and fascial flap beneath the superficial musculoaponeurotic system to address midface and lower face aging. By releasing key retaining ligaments and repositioning descended fat pads, this approach corrects nasolabial folds, jowling, and malar descent while preserving flap vascularity and allowing tension-free skin closure. Durable aesthetic improvement depends on precise anatomic knowledge, careful technique, and appropriate patient selection, particularly in older patients with significant soft tissue descent.
Optimal outcomes require coordinated interprofessional care before, during, and after surgery. Surgeons experienced in deep plane rhytidectomy lead operative planning and execution, while general practitioners and anesthesiologists assess perioperative risk factors and ensure medical fitness for anesthesia. Advanced practitioners, nurses, and surgical assistants support intraoperative safety and postoperative monitoring, enabling early detection of hematoma or facial nerve dysfunction.[41] Pharmacists contribute by reviewing medications that increase bleeding risk and advising on perioperative drug management. Ongoing communication among team members facilitates patient education, adherence to postoperative restrictions, and timely intervention for wound healing concerns, including consideration of adjunctive hyperbaric oxygen therapy when indicated, thereby enhancing patient safety, satisfaction, and team performance.
Nursing, Allied Health, and Interprofessional Team Interventions
Pain and nausea control is critical, as lower pain and nausea levels may help to keep blood pressure levels lower as well, which decreases the risk of bleeding complications. Patients generally report peri-incisional pain for 3 to 4 days postoperatively, and the pressure dressing may exacerbate the discomfort. Opioid medications, scheduled acetaminophen, long-acting local anesthetics, and cold compresses are all effective means of reducing pain.
To minimize edema and ecchymosis, the patient should wear the facelift dressing continuously for the first 24 hours, sleep with the head elevated for 1 week, and avoid strenuous activity for 2 weeks. The patient may be given a low-dose corticosteroid taper, Arnica montana (an herbal pain medication), or bromelain to help reduce bruising and swelling; however, definitive data on their efficacy are lacking.[14] Patients are asked to return at 1 day postoperatively for drain and dressing removal, and again at 1 week for wound assessment and suture removal. Photographic documentation should occur 6 to 12 months postoperatively.
Media
(Click Image to Enlarge)

Deep-Plane Facelift. The image shows the results after a deep-plane facelift. Note the revolumization of the midface with improvement in malar eminence projection, jowl enhancement with appropriate platysmal and SMAS repositioning, and buccal fat pad reduction.
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)
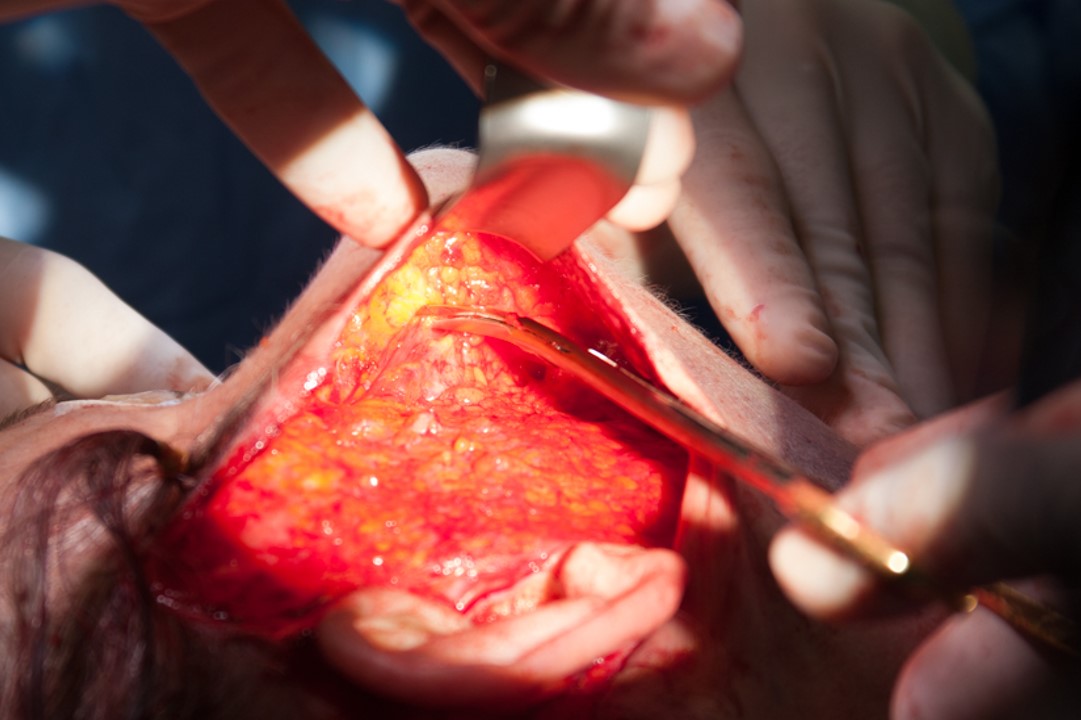
Deep Plane Rhytidectomy. The tips of the scissors point to the medial end of the zygomaticus major muscle. The malar fat pad is the yellow adipose tissue up and to the left of the tips of the scissors.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
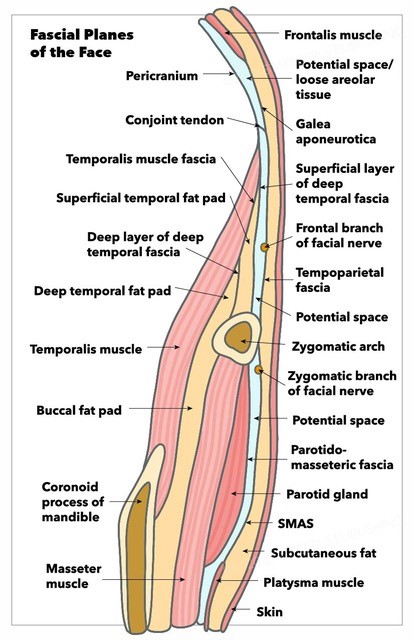
Fascial Planes of the Face. This illustration depicts the facial fascial planes, highlighting the continuity of the frontalis muscle, galea aponeurotica, temporoparietal fascia, superficial musculoaponeurotic system, platysma, and the location of the facial nerve.
Contributed by K Humphreys and MH Hohman, MD, FACS
(Click Image to Enlarge)

Upper Neck Hematoma. An upper neck hematoma is centered just posterior to the angle of the mandible, on postoperative day 1 following rhytidectomy in a 60-year-old male with hypertension. This location is a common site for post-rhytidectomy hematoma, although the size of this hematoma is significantly larger than typically observed.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)

Pixie Ear Deformity. Pixie ear deformity following facelifting, caused by downward traction on the lobule due to excessive tension during closure, likely resulting from over-resection of skin.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)

Rhytidectomy Complications. The image depicts lower lip asymmetry after rhytidectomy due to injury to the nerve that controls the depressor labii inferioris muscle. The left side (arrow) is affected; the patient cannot depress her lower lip on that side.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)

Blair Rhytidectomy Incision. Image demonstrating the postauricular aspect of the incision.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)

Rhytidectomy Incision Patterns. Green: A common configuration that follows the inferior margin of the temporal hair tuft. White: An alternative that hides the temporal segment of the scar within the hair and permits more removal of temporal skin, but may elevate the temporal hair tuft and move it posteriorly. Red: This denotes the posttragal incision, typically used in women. Blue: The line marks the pretragal incision used in men to avoid advancing hair-bearing skin onto the tragus. Purple: The line of entry into the sub-SMAS plane for a deep-plane facelift. Pink: The region of flap elevation in the deep plane. Dotted lines represent incisions placed posterior to portions of the auricle.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)

Great Auricular Nerve. The great auricular nerve crosses over the sternocleidomastoid muscle.
Contributed by M Hohman, MD, FACS
(Click Image to Enlarge)

Facial Flap Development. A #15 blade scalpel is used to make the Blair rhytidectomy incision and then enter the subcutaneous plane.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
Facial Flap Elevation. The surgeon uses Gorney–Freeman facelift scissors to elevate a subcutaneous flap while applying traction with a 2-pronged Joseph skin hook. The assistant provides countertension to facilitate dissection and monitors for facial twitching, which may indicate impending facial nerve injury or inadequate depth of anesthesia.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
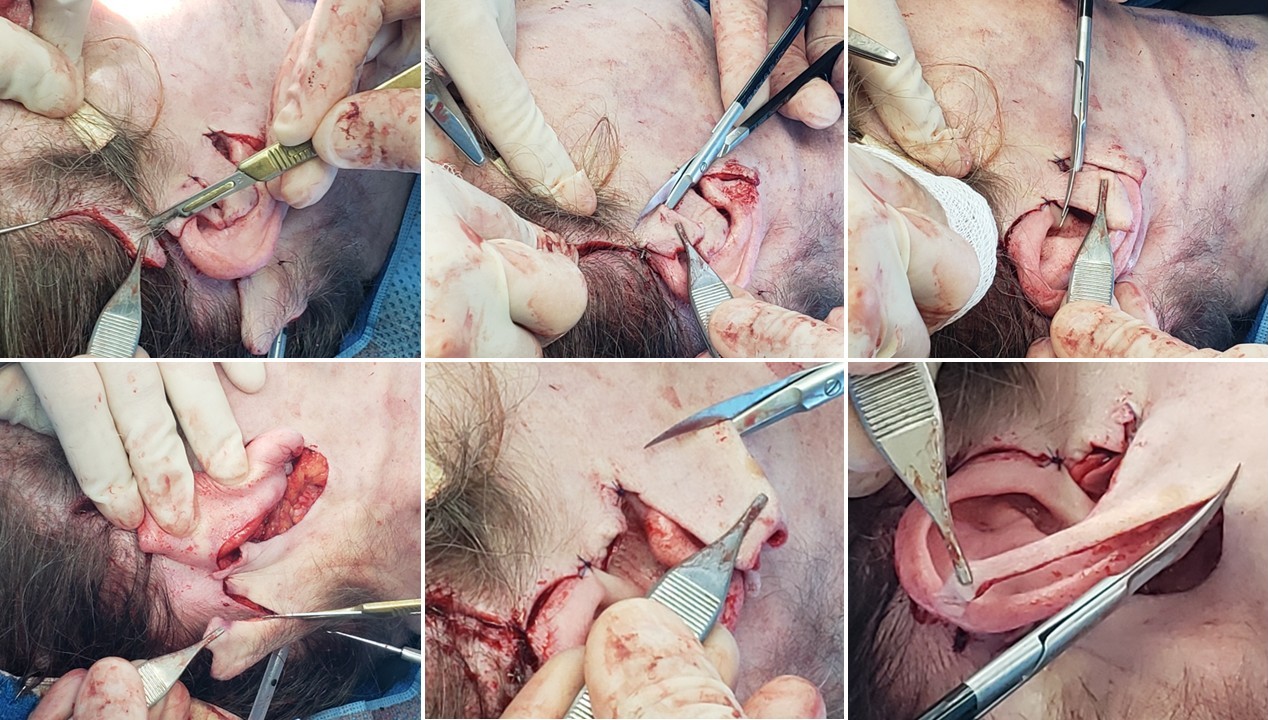
Facelift Flap Tailoring. Clockwise from the upper left, this image demonstrates removal of excess temporal skin following the curve of the helical root; conservative trimming of the skin overlying the tragus; trimming of the posterior skin flap along the helix; contouring of the skin around the lobule with care to preserve sufficient tissue for a tension-free closure and avoidance of a pixie ear deformity; and trimming of the posterior hair-bearing scalp.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)

Deep Plane Entry. A line is marked running between the angle of the mandible and the malar eminence, and the superficial musculoaponeurotic system (SMAS) layer is incised along it. Elevation beneath the SMAS exposes the masseter muscle, facial nerve branches, and the buccal fat pad.
Contributed by MH Hohman, MD, FACS, and CM Llewellyn, MD
(Click Image to Enlarge)

Buccal Fat Pad Reduction. The buccal fat pad, also known as the boule of Bichat, may be accessed through an intraoral or external approach. In this image, the buccal fat pad is reduced during a deep-plane facelift. Careful dissection is required because the buccal branches of the facial nerve course over the fat pad and may be stretched or injured. The buccal fat pad is readily identifiable by its smoother, less lobulated appearance and its ease of separation from surrounding fat.
Contributed by MH Hohman, MD, FACS, and CM Llewellyn, MD
(Click Image to Enlarge)

Full-Thickness Skin Flap Necrosis. Skin ischemia and sloughing occur in less than 1% of cases, most commonly in the preauricular region, which represents the distal aspect of the facial flap.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
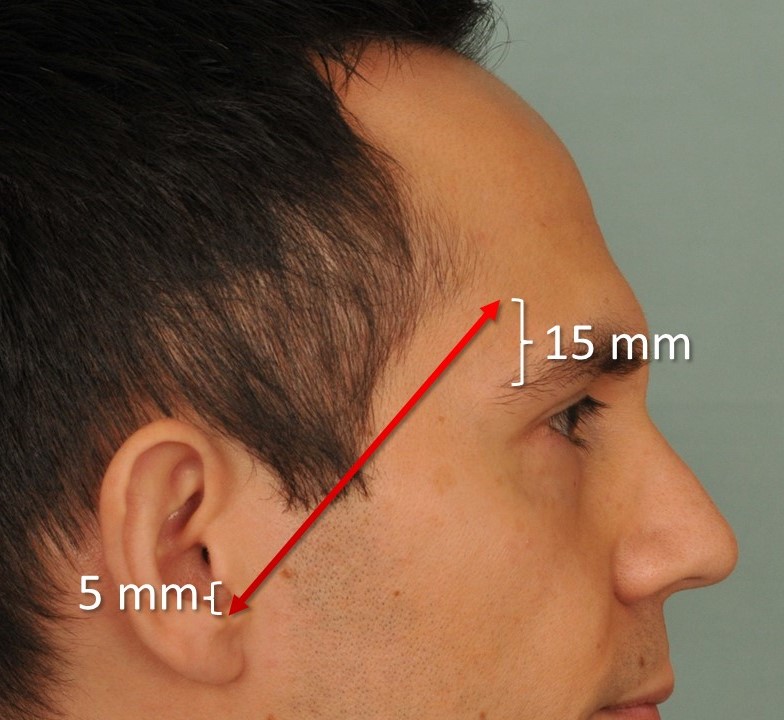
Pitanguy Line. This image illustrates the Pitanguy line, which runs from a point 5 mm inferior to the tragus to a point 15 mm superior to the lateral brow. This line approximates the course of the frontal branch of the facial nerve.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)

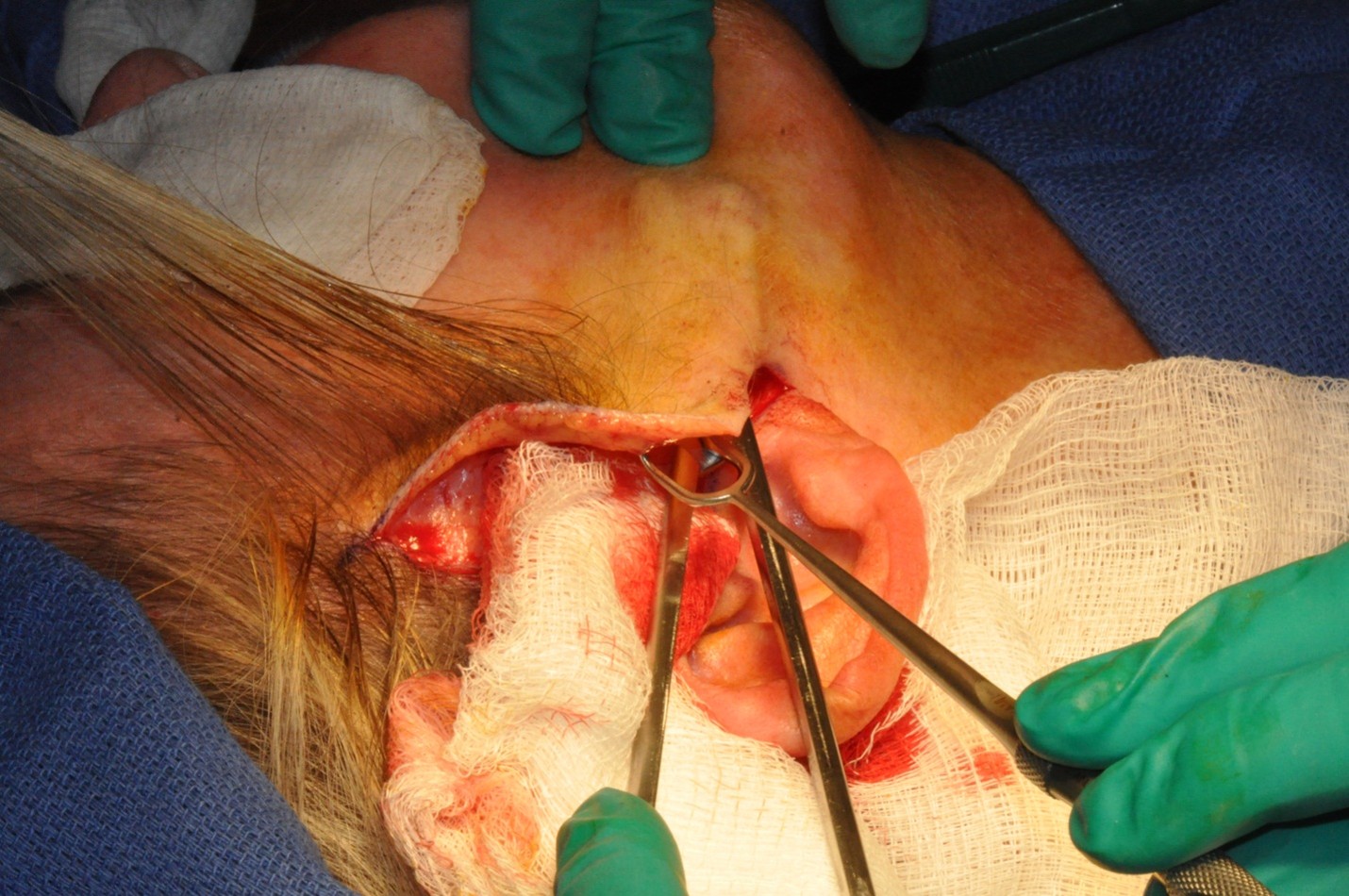
Blair Rhytidectomy. Image demonstrating the posttragal approach in a female patient.
Contributed by MH Hohman, MD, FACS
References
Hamra ST. The deep-plane rhytidectomy. Plastic and reconstructive surgery. 1990 Jul:86(1):53-61; discussion 62-3 [PubMed PMID: 2359803]
Wulu JA, Spiegel JH. Is deep plane rhytidectomy superior to superficial musculoaponeurotic system plication facelift? The Laryngoscope. 2018 Aug:128(8):1741-1742. doi: 10.1002/lary.27065. Epub 2017 Dec 27 [PubMed PMID: 29280491]
Wei B, Duan R, Xie F, Gu J, Liu C, Gao B. Advances in Face-Lift Surgical Techniques: 2016-2021. Aesthetic plastic surgery. 2023 Apr:47(2):622-630. doi: 10.1007/s00266-022-03017-z. Epub 2022 Jul 26 [PubMed PMID: 35882647]
Level 3 (low-level) evidenceMitz V, Peyronie M. The superficial musculo-aponeurotic system (SMAS) in the parotid and cheek area. Plastic and reconstructive surgery. 1976 Jul:58(1):80-8 [PubMed PMID: 935283]
Baker DC, Conley J. Avoiding facial nerve injuries in rhytidectomy. Anatomical variations and pitfalls. Plastic and reconstructive surgery. 1979 Dec:64(6):781-95 [PubMed PMID: 515227]
Lefkowitz T, Hazani R, Chowdhry S, Elston J, Yaremchuk MJ, Wilhelmi BJ. Anatomical landmarks to avoid injury to the great auricular nerve during rhytidectomy. Aesthetic surgery journal. 2013 Jan:33(1):19-23. doi: 10.1177/1090820X12469625. Epub [PubMed PMID: 23277616]
Gordon NA, Adam SI 3rd. Deep plane face lifting for midface rejuvenation. Clinics in plastic surgery. 2015 Jan:42(1):129-42. doi: 10.1016/j.cps.2014.08.009. Epub [PubMed PMID: 25440750]
Fitzgerald R, Graivier MH, Kane M, Lorenc ZP, Vleggaar D, Werschler WP, Kenkel JM. Update on facial aging. Aesthetic surgery journal. 2010 Jul-Aug:30 Suppl():11S-24S. doi: 10.1177/1090820X10378696. Epub [PubMed PMID: 20844296]
Swift A, Liew S, Weinkle S, Garcia JK, Silberberg MB. The Facial Aging Process From the "Inside Out". Aesthetic surgery journal. 2021 Sep 14:41(10):1107-1119. doi: 10.1093/asj/sjaa339. Epub [PubMed PMID: 33325497]
Hamra ST. Composite rhytidectomy. Plastic and reconstructive surgery. 1992 Jul:90(1):1-13 [PubMed PMID: 1615067]
Choucair RJ, Hamra ST. Nuances of the Composite Face-lift Technique. Seminars in plastic surgery. 2009 Nov:23(4):247-56. doi: 10.1055/s-0029-1242183. Epub [PubMed PMID: 21037860]
Rossell-Perry P, Paredes-Leandro P. Anatomic study of the retaining ligaments of the face and applications for facial rejuvenation. Aesthetic plastic surgery. 2013 Jun:37(3):504-12. doi: 10.1007/s00266-012-9995-x. Epub 2012 Oct 24 [PubMed PMID: 23093328]
Jacono A, Bryant LM. Extended Deep Plane Facelift: Incorporating Facial Retaining Ligament Release and Composite Flap Shifts to Maximize Midface, Jawline and Neck Rejuvenation. Clinics in plastic surgery. 2018 Oct:45(4):527-554. doi: 10.1016/j.cps.2018.06.007. Epub [PubMed PMID: 30268241]
Derby BM, Codner MA. Evidence-Based Medicine: Face Lift. Plastic and reconstructive surgery. 2017 Jan:139(1):151e-167e. doi: 10.1097/PRS.0000000000002851. Epub [PubMed PMID: 28027252]
Parikh SS, Jacono AA. Deep-plane face-lift as an alternative in the smoking patient. Archives of facial plastic surgery. 2011 Jul-Aug:13(4):283-5. doi: 10.1001/archfacial.2011.39. Epub [PubMed PMID: 21768564]
Level 3 (low-level) evidenceJoseph AW, Ishii L, Joseph SS, Smith JI, Su P, Bater K, Byrne P, Boahene K, Papel I, Kontis T, Douglas R, Nelson CC, Ishii M. Prevalence of Body Dysmorphic Disorder and Surgeon Diagnostic Accuracy in Facial Plastic and Oculoplastic Surgery Clinics. JAMA facial plastic surgery. 2017 Jul 1:19(4):269-274. doi: 10.1001/jamafacial.2016.1535. Epub [PubMed PMID: 27930752]
Dey JK, Ishii M, Phillis M, Byrne PJ, Boahene KD, Ishii LE. Body dysmorphic disorder in a facial plastic and reconstructive surgery clinic: measuring prevalence, assessing comorbidities, and validating a feasible screening instrument. JAMA facial plastic surgery. 2015 Mar-Apr:17(2):137-43. doi: 10.1001/jamafacial.2014.1492. Epub [PubMed PMID: 25654334]
Goin MK, Burgoyne RW, Goin JM, Staples FR. A prospective psychological study of 50 female face-lift patients. Plastic and reconstructive surgery. 1980 Apr:65(4):436-42 [PubMed PMID: 7360810]
Pitanguy I, Ramos AS. The frontal branch of the facial nerve: the importance of its variations in face lifting. Plastic and reconstructive surgery. 1966 Oct:38(4):352-6 [PubMed PMID: 5926990]
Aldhabaan SA, Hudise JY, Obeid AA. A meta-analysis of pre- and postoperative corticosteroids for reducing the complications following facial reconstructive and aesthetic surgery. Brazilian journal of otorhinolaryngology. 2022 Jan-Feb:88(1):63-82. doi: 10.1016/j.bjorl.2020.05.015. Epub 2020 Jun 20 [PubMed PMID: 32605829]
Level 1 (high-level) evidenceLocketz GD, Lozada KN, Bloom JD. Tranexamic Acid in Aesthetic Facial Plastic Surgery: A Systematic Review of Evidence, Applications, and Outcomes. Aesthetic surgery journal. Open forum. 2020 Sep:2(3):ojaa029. doi: 10.1093/asjof/ojaa029. Epub 2020 Jun 14 [PubMed PMID: 33791652]
Level 1 (high-level) evidenceSykes JM, Liang J, Kim JE. Contemporary deep plane rhytidectomy. Facial plastic surgery : FPS. 2011 Feb:27(1):124-32. doi: 10.1055/s-0030-1270426. Epub 2011 Jan 18 [PubMed PMID: 21246463]
Baker SR. Deep plane rhytidectomy and variations. Facial plastic surgery clinics of North America. 2009 Nov:17(4):557-73, vi. doi: 10.1016/j.fsc.2009.06.003. Epub [PubMed PMID: 19900662]
Choucair RJ, Hamra ST. Extended superficial musculaponeurotic system dissection and composite rhytidectomy. Clinics in plastic surgery. 2008 Oct:35(4):607-22, vii. doi: 10.1016/j.cps.2008.05.014. Epub [PubMed PMID: 18922313]
Level 3 (low-level) evidenceAckerman BM, Savalia NB. Systematic Approach to Deep Plane Facelift. Aesthetic plastic surgery. 2025 Aug:49(16):4579-4586. doi: 10.1007/s00266-025-04793-0. Epub 2025 Mar 25 [PubMed PMID: 40133535]
Level 1 (high-level) evidenceJacono AA. A Novel Volumizing Extended Deep-Plane Facelift: Using Composite Flap Shifts to Volumize the Midface and Jawline. Facial plastic surgery clinics of North America. 2020 Aug:28(3):331-368. doi: 10.1016/j.fsc.2020.03.001. Epub [PubMed PMID: 32503718]
Van Pham T, Truong KHTN. Short or Minimum Incision Deep Plane/Extended Deep Plane Facelift/Rhytidectomy. Facial plastic surgery : FPS. 2020 Aug:36(4):376-385. doi: 10.1055/s-0040-1714118. Epub 2020 Aug 31 [PubMed PMID: 32866975]
Gordon NA, Lockwood DB. Advanced Deep-Plane Rhytidectomy: Advantages for Neck Treatment and Volumization of the Midface. Facial plastic surgery : FPS. 2024 Mar 28:():. doi: 10.1055/s-0044-1785452. Epub 2024 Mar 28 [PubMed PMID: 38547912]
Gordon NA, Sawan TG. Deep-Plane Approach to the Vertical Platysma Advancement: Technical Modifications and Nuances over 25 Years. Facial plastic surgery : FPS. 2020 Aug:36(4):358-375. doi: 10.1055/s-0040-1713842. Epub 2020 Aug 31 [PubMed PMID: 32866974]
Roskies M, Bray D, Gordon NA, Gualdi A, Nayak LM, Talei B. Limited Delamination Modifications to the Extended Deep Plane Rhytidectomy: An Anatomical Basis for Improved Outcomes. Facial plastic surgery & aesthetic medicine. 2024 Nov-Dec:26(6):657-664. doi: 10.1089/fpsam.2024.0018. Epub 2024 Jul 29 [PubMed PMID: 39072376]
Hamra ST. The zygorbicular dissection in composite rhytidectomy: an ideal midface plane. Plastic and reconstructive surgery. 1998 Oct:102(5):1646-57 [PubMed PMID: 9774027]
Jacono AA, Ransom ER. Patient-specific rhytidectomy: finding the angle of maximal rejuvenation. Aesthetic surgery journal. 2012 Sep:32(7):804-13. doi: 10.1177/1090820X12455826. Epub [PubMed PMID: 22942107]
Abi-Rafeh J, Bassiri-Tehrani B, Nahai F. Hemostatic Net Versus Surgical Drain After Deep Plane Facelift Surgery: A Prospective Randomized Controlled Trial. Aesthetic plastic surgery. 2025 Nov:49(21):6196-6197. doi: 10.1007/s00266-025-04997-4. Epub 2025 May 22 [PubMed PMID: 40404849]
Level 1 (high-level) evidenceJacono AA, Alemi AS, Russell JL. A Meta-Analysis of Complication Rates Among Different SMAS Facelift Techniques. Aesthetic surgery journal. 2019 Aug 22:39(9):927-942. doi: 10.1093/asj/sjz045. Epub [PubMed PMID: 30768122]
Level 1 (high-level) evidenceStewart CM, Bassiri-Tehrani B, Jones HE, Nahai F. Evidence of Hematoma Prevention After Facelift. Aesthetic surgery journal. 2024 Jan 16:44(2):134-143. doi: 10.1093/asj/sjad247. Epub [PubMed PMID: 37540899]
Haykal S, Arad E, Bagher S, Lai C, Hohman M, Hadlock T, Zuker RM, Borschel GH. The role of botulinum toxin a in the establishment of symmetry in pediatric paralysis of the lower lip. JAMA facial plastic surgery. 2015 May-Jun:17(3):174-8. doi: 10.1001/jamafacial.2015.10. Epub [PubMed PMID: 25742503]
Vaccari S, Fondrini R, Ragaini E, Lozito A, Andreoletti S, Capuano SM, Klinger F, Vinci V. The pixie ear: How to prevent and correct it-a review of the literature. Surgery. 2024 Oct:176(4):1247-1255. doi: 10.1016/j.surg.2024.06.017. Epub 2024 Jul 15 [PubMed PMID: 39013675]
Gunter AE, Llewellyn CM, Perez PB, Hohman MH, Roofe SB. First Bite Syndrome Following Rhytidectomy: A Case Report. The Annals of otology, rhinology, and laryngology. 2021 Jan:130(1):92-97. doi: 10.1177/0003489420936713. Epub 2020 Jun 21 [PubMed PMID: 32567395]
Level 3 (low-level) evidenceBecker FF, Bassichis BA. Deep-plane face-lift vs superficial musculoaponeurotic system plication face-lift: a comparative study. Archives of facial plastic surgery. 2004 Jan-Feb:6(1):8-13 [PubMed PMID: 14732637]
Level 2 (mid-level) evidencePascali M, Savani L, Gratteri M, Marchese G, Persichetti P. Combining Deep Plane Face and Neck Lift with Periorbital Rejuvenation and Ancillary Surgical Procedures of the Face: A Critical Evaluation of Over 434 Consecutive Cases. Aesthetic plastic surgery. 2025 Aug:49(15):4163-4175. doi: 10.1007/s00266-025-04814-y. Epub 2025 Apr 3 [PubMed PMID: 40180645]
Level 3 (low-level) evidenceNeel OF, Mousa AH, Al-Terkawi RA, Bakr MM, Mortada H. Assessing the Efficacy of Hyperbaric Oxygen Therapy on Facelift Outcomes: A Case-Control Study Comparing Outcomes in Patients With and Without Hyperbaric Oxygen Therapy. Aesthetic surgery journal. Open forum. 2023:5():ojad065. doi: 10.1093/asjof/ojad065. Epub 2023 Jul 14 [PubMed PMID: 37529413]
Level 2 (mid-level) evidence