Definition/Introduction
Evidence-based medicine (EBM) is an approach to clinical decision making that uses the best current evidence, together with clinical expertise and patient values, to guide care for individual patients.[1] The modern evidence-based medicine movement is closely associated with work at McMaster University and with Gordon Guyatt et al, and the Evidence-Based Medicine Working Group brought it into wider clinical teaching in the early 1990s.[2][3] From the beginning, EBM was intended to bring together 3 elements: the best available research evidence, clinical expertise, and patient values and preferences.[1][4]
EBM is often presented as a repeating cycle. The clinician begins with an answerable question, searches for the best available evidence, critically appraises that evidence, applies it to the patient at hand, and then reassesses the outcome.[1] This cycle remains a useful framework because it keeps attention on real clinical decisions rather than evidence in the abstract ( see Image. Evidence-Based Medicine).
The evidence pyramid is a common teaching tool because it helps learners recognize that different types of evidence do not carry the same weight. In its traditional form, animal and translational studies, case reports, and expert opinion sit near the bottom; observational studies occupy the middle; and randomized controlled trials, systematic reviews, and meta-analyses appear near the top (see Image. Hierarchy of Evidence).[5] Additionally, a central part of EBM is deciding whether the available evidence is applicable to the patient in front of the clinician. Even a strong trial may not translate neatly if the study population differs from the patient in age, comorbidities, baseline risk, or clinical setting.[1][4]
EBM also rests on probabilistic reasoning, especially in diagnosis. Bayes theorem helps clinicians revise the probability of disease as new information becomes available, and likelihood ratios provide a practical way to do this at the bedside.[6][7] Test results do not speak for themselves; their meaning depends on the pretest probability and on whether the new information moves the clinician closer to or farther from a testing or treatment threshold.[6][7]
Probabilistic reasoning remains true in contemporary practice, even as the volume of biomedical literature, clinical data, guidelines, and predictive tools continues to grow. Clinicians are expected to make sense of far more information than any individual can comfortably track by manual reading alone. Machine learning and other artificial intelligence (AI)-assisted tools may help with evidence retrieval, literature screening, organization, and summarization in information-heavy environments.[8] However, these tools should support the EBM process, not replace it. Clinicians must carefully check AI-assisted tool output, especially since large language models can produce inaccurate or fabricated references.[9]
Machine learning models used for diagnosis, prognosis, or clinical decision support should also be viewed through the lens of EBM. These models are not outside the EBM framework. Like other tests and prediction tools, machine learning models require appraisal of validity, discrimination, calibration, applicability, and clinical usefulness before adoption in practice.[10][11] Model output should be interpreted in a clinical context, with attention to pretest probability and disease prevalence, rather than treated as a stand-alone answer.[6][7] Table 1 shows a summary of the Grading of Recommendations Assessment, Development, and Evaluation Framework (GRADE) approach to rating the certainty of evidence and the strength of recommendations.[12]
Table 1. Grading of Recommendations Assessment, Development, and Evaluation Framework
| Element | Category | Plain-language meaning |
| Certainty of evidence | High | Confidence in the estimate is strong, and the true effect is unlikely to be very different. |
| Certainty of evidence | Moderate | Confidence in the estimate is moderate, but the true effect could differ in an important way. |
| Certainty of evidence | Low | Limited confidence; the actual effect could differ substantially from what the data suggest. |
| Certainty of evidence | Very low | Confidence in the estimate is minimal, and the true effect is very uncertain. |
| Strength of recommendation | Strong | The balance of benefits and harms is clear enough that most informed patients would choose the recommended course. |
| Strength of recommendation | Conditional | The balance is less certain, so different choices may be reasonable depending on patient values, clinical context, and resources. |
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
Evidence-based medicine brings together the best available evidence, clinical expertise, and patient values, but also has several limitations.[1][4]
Publication Bias
EBM depends heavily on the published literature, yet published studies are not a neutral sample of all completed research. Positive findings are more likely to be published than negative or inconclusive results, and selective reporting can make benefits appear greater and harms appear less important than they really are. In meta-analyses, funnel plots may provide a visual clue to asymmetry that can suggest publication bias, although they are only one part of the assessment.[13][14][15]
Limitations of Randomized Controlled Trials
Randomized controlled trials are generally regarded as the highest level of primary study evidence, especially for questions of treatment efficacy.[16] Even so, not every important clinical question can be answered by a randomized trial. Rare diseases, ethical constraints, cost, and feasibility may make such studies impractical or inappropriate. Trial populations may also differ in important ways from the patients seen in routine practice, which can limit generalizability. The parachute example remains a useful reminder that not all valuable medical knowledge requires a randomized trial.[1][17]
Lag Time and Information Overload
Keeping current is increasingly difficult because the biomedical literature expands and digital tools multiply. Artificial intelligence (AI)-assisted tools may help with searching, screening, and summarizing the literature, but they can also introduce mistakes, including inaccurate or fabricated citations, and should not replace direct review of key sources.[8][9]
Patient Values and Clinical Judgment
Patient preferences are central to EBM, but they can be overshadowed in practice when clinicians focus too narrowly on protocols, guidelines, or statistically favorable outcomes. Strong evidence does not automatically identify the best choice for every patient. Clinical judgment is still needed to decide whether the evidence applies, and patient values remain essential when weighing burdens, trade-offs, and goals of care.[1][4][18]
Machine Learning as an Object of Evidence-Based Medicine Appraisal
Machine learning tools used for diagnosis, prognosis, triage, or decision support should be judged by the same EBM standards applied to other tests and prediction tools. Table 2 summarizes key questions for appraising clinical machine learning studies. Good performance metrics alone do not show that a model improves care. Validity, calibration, generalizability, and clinical usefulness still matter before a model should influence patient treatment.[10][11] Practical questions clinicians can use when appraising machine learning studies within the evidence-based medicine framework.[10][11]
Table 2. Criteria for Evidence-Based Medicine Evaluation of Clinical Machine Learning Studies
| Domain | Key question | Why it matters |
| Intended use | What clinical task is the model meant to support? | A model should be judged in the role it is expected to fill. |
| Population and setting | Were the development and test populations similar to the patients and setting where the model will be used? | Performance may not carry over well across different populations or practice environments. |
| Reference standard | Was the outcome determined using an appropriate and consistent standard? | Poor or inconsistent labels can make a model look better or worse than it really is. |
| Validation | Was the model tested beyond the original development sample? | Apparent success in the training setting does not prove broader usefulness. |
| Performance | Did the model show acceptable discrimination and calibration? | A useful model should separate risk and estimate it in a clinically meaningful way. |
| Fairness | Did accuracy differ across important patient subgroups? | Uneven performance can worsen bias and inequity in care. |
| Transparency | Were the methods described clearly enough for independent appraisal? | Poor reporting limits trust, critique, and reproducibility. |
| Clinical use | Is there evidence that using the model improves decisions, care, or net benefit? | Good test characteristics alone do not prove that patients have improved outcomes. |
Clinical Significance
Evidence-based medicine is clinically important because it helps clinicians use the best available evidence in ways relevant to individual patients.[1][4] In practice, EBM matters because clinical decisions are rarely made on evidence alone. Diagnosis, prognosis, treatment, and prevention all require judgment about whether the available data fit the patient in front of the clinician. For example, a statistically favorable intervention may still be a poor choice if the patient’s comorbidities, baseline risk, goals, or treatment burden differ from those of the population studied. EBM helps clinicians move beyond habit, anecdote, or authority alone and toward decisions that are more transparent, more consistent, and more patient-centered.[1][18]
EBM is also important beyond the bedside. The framework provides the foundation for clinical practice guidelines, quality improvement efforts, and population-level recommendations. Modern frameworks such as Grading of Recommendations Assessment, Development and Evaluation Framework have improved this process by separating the certainty of evidence from the strength of the recommendation and by considering benefits, harms, patient values, and resource use, rather than study design alone.[12]
The significance of EBM has not diminished in the era of digital medicine and artificial intelligence. Instead, EBM has become more important. Clinicians now face a growing volume of literature, guidelines, prediction tools, and artificial intelligence (AI)-assisted decision-support systems. EBM remains the framework for deciding which of these tools are trustworthy, applicable, and clinically useful. Artificial intelligence may improve the efficiency of evidence retrieval, synthesis, and prediction, but its clinical value still depends on the same core questions: Is the information valid? Does the information apply to this patient? Is the information likely to improve care?[8][10][8][11]
Nursing, Allied Health, and Interprofessional Team Interventions
Evidence-based medicine is not limited to clinicians. Advanced practice clinicians, nurses, pharmacists, therapists, health coaches, athletic trainers, social workers, case managers, and other members of the interprofessional team all help put evidence into practice. Interprofessional team members identify clinical problems, help find and interpret relevant evidence, educate patients, monitor treatment response, and ensure patients’ goals and preferences are heard throughout the care team.[1][4][19]
Interprofessional application of evidence matters at the bedside because evidence rarely applies in exactly the same way to every patient. Nurses and advanced practice clinicians may be the first to notice worsening symptoms, poor treatment tolerance, low health literacy, cost barriers, limited support at home, or other factors that change whether an evidence-based recommendation is realistic. Pharmacists may identify drug interactions, safety concerns, or adherence problems. Therapists and other allied health professionals often add essential functional, behavioral, and practical context that strengthens clinical decision-making. EBM is often most useful when shared across the team rather than carried by a single clinician.[1][4]
The same caution applies to newer digital tools. As artificial intelligence (AI)-assisted prediction models and decision-support systems enter clinical workflows, care team members should interpret them using the same EBM principles applied to other clinical tools. Before prediction models and AI-assisted decision-support systems influence patient treatment, clinicians should ask whether the model was developed and reported transparently, whether it was validated in a relevant population, and whether it is likely to improve care in actual practice rather than simply perform well on paper.[8][10][11]
Nursing, Allied Health, and Interprofessional Team Monitoring
Monitoring closes the EBM cycle: the team assesses whether the chosen plan actually produced the intended outcome for this patient, not merely whether the plan was delivered. Monitoring works best when the team decides in advance what to track and over what interval, then watches for benefits that fail to materialize, harms that surface only with time, and shifts in the patient's condition, goals, or preferences that change which evidence still applies. When the clinical picture changes, the task is not only to adjust the plan but also to reconsider whether the original evidence still fits, including stepping back from an intervention once stronger or contradictory evidence emerges. Prediction models and AI-assisted tools warrant the same longitudinal scrutiny: their performance can drift because patient populations and practice patterns change, so continued accuracy and calibration should be rechecked over time rather than considered settled after adoption.[1][4][10][11][20]
Media
(Click Image to Enlarge)
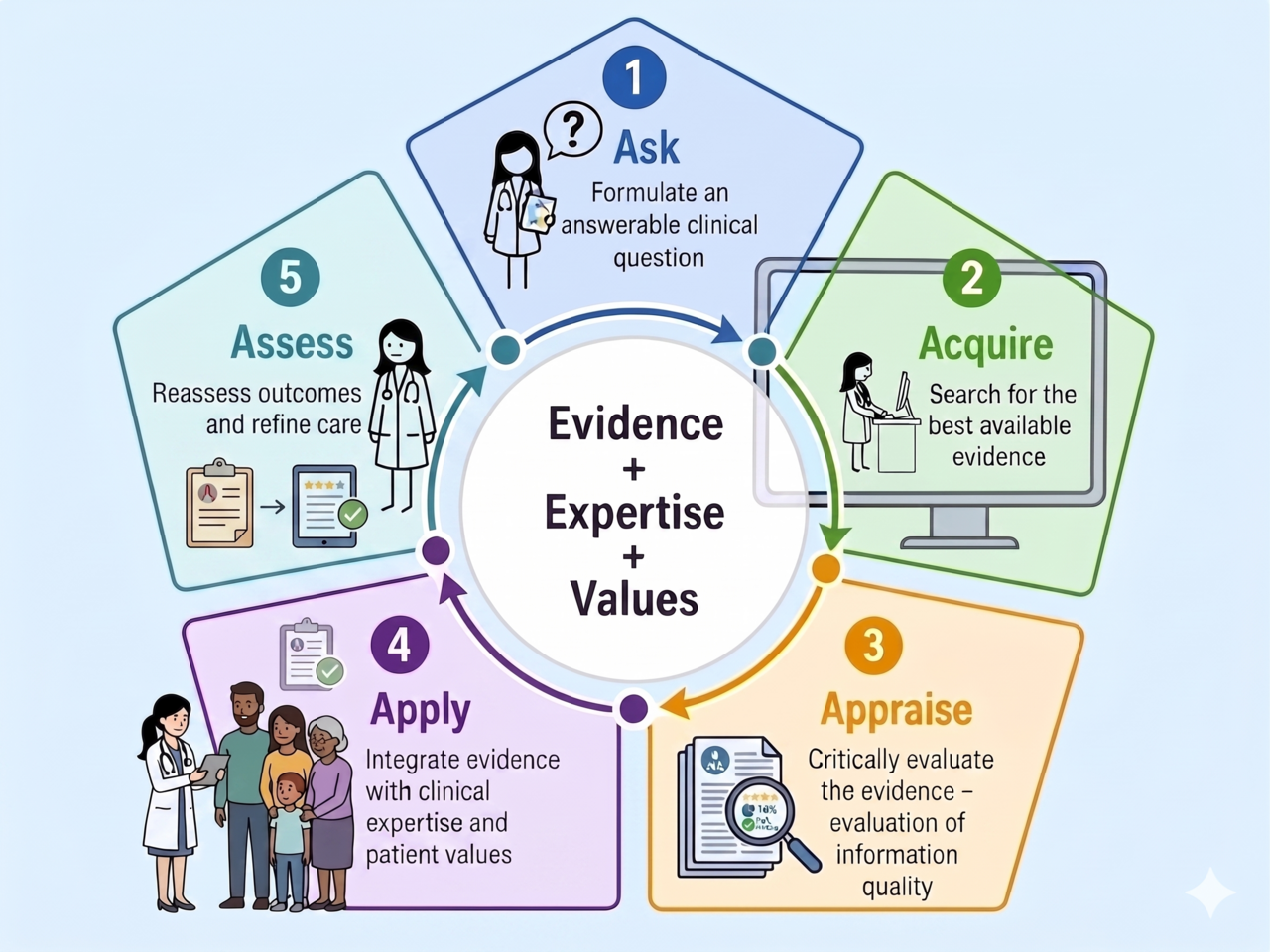
Evidence-Based Medicine Cycle. The five-step model of evidence-based practice: ask, acquire, appraise, apply, and assess, with evidence, expertise, and patient values at the center.
Wiseworker2026, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
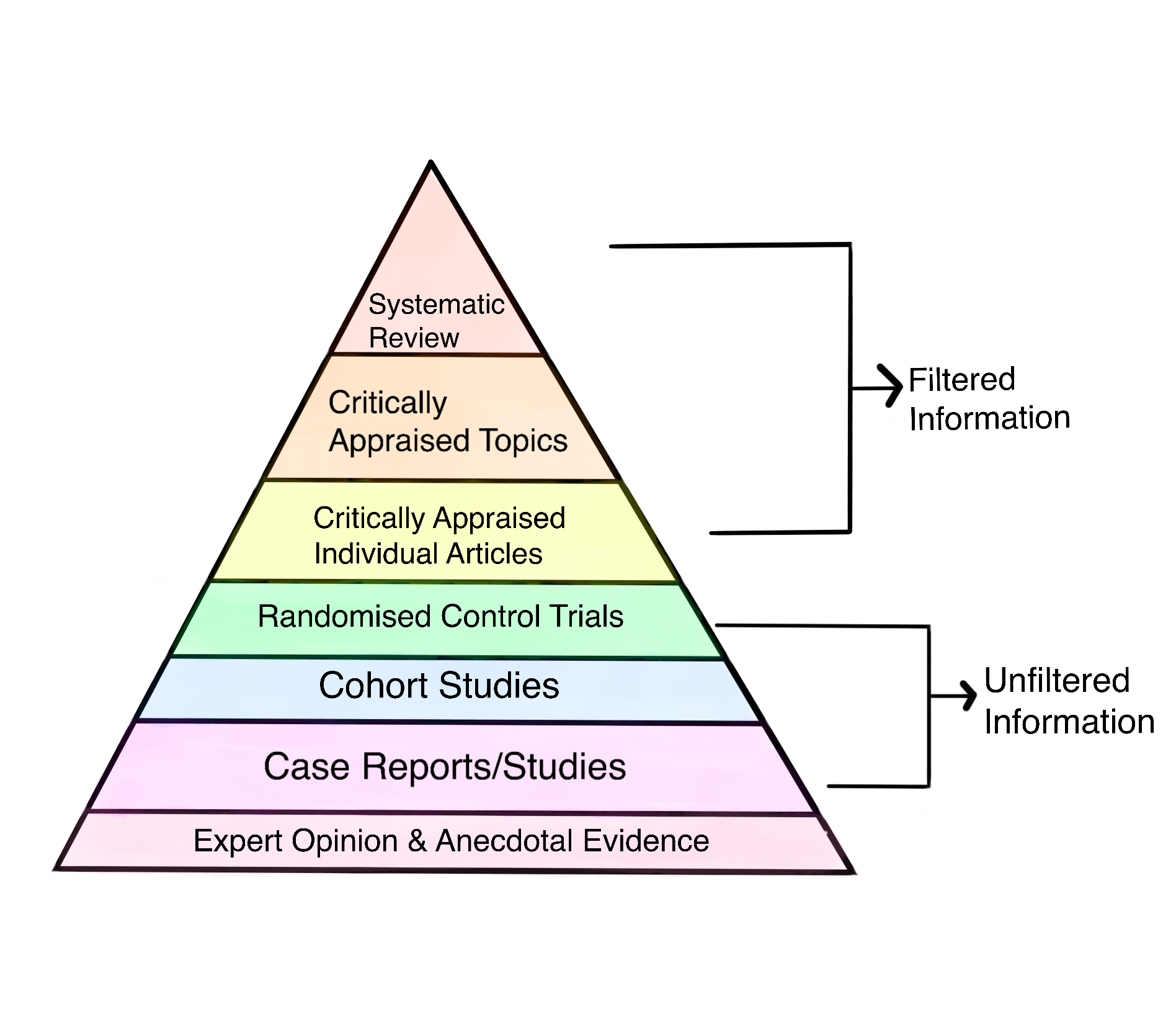
Hierarchy of Evidence. Diagram illustrating common study designs arranged by relative reliability of evidence.
Grandma Gan, Public Domain, via Wikimedia Commons
{kind=link}
References
Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn't. BMJ (Clinical research ed.). 1996 Jan 13:312(7023):71-2 [PubMed PMID: 8555924]
Evidence-Based Medicine Working Group. Evidence-based medicine. A new approach to teaching the practice of medicine. JAMA. 1992 Nov 4:268(17):2420-5 [PubMed PMID: 1404801]
Guyatt G, Cook D, Haynes B. Evidence based medicine has come a long way. BMJ (Clinical research ed.). 2004 Oct 30:329(7473):990-1 [PubMed PMID: 15514320]
Montori VM, Guyatt GH. What is evidence-based medicine and why should it be practiced? Respiratory care. 2001 Nov:46(11):1201-14 [PubMed PMID: 11679142]
Wallace SS, Barak G, Truong G, Parker MW. Hierarchy of Evidence Within the Medical Literature. Hospital pediatrics. 2022 Aug 1:12(8):745-750. doi: 10.1542/hpeds.2022-006690. Epub [PubMed PMID: 35909178]
Diamond GA. The wizard of odds: Bayes theorem and diagnostic testing. Mayo Clinic proceedings. 1999 Nov:74(11):1179-82 [PubMed PMID: 10560608]
Deeks JJ, Altman DG. Diagnostic tests 4: likelihood ratios. BMJ (Clinical research ed.). 2004 Jul 17:329(7458):168-9 [PubMed PMID: 15258077]
Subbiah V. The next generation of evidence-based medicine. Nature medicine. 2023 Jan:29(1):49-58. doi: 10.1038/s41591-022-02160-z. Epub 2023 Jan 16 [PubMed PMID: 36646803]
Chelli M, Descamps J, Lavoué V, Trojani C, Azar M, Deckert M, Raynier JL, Clowez G, Boileau P, Ruetsch-Chelli C. Hallucination Rates and Reference Accuracy of ChatGPT and Bard for Systematic Reviews: Comparative Analysis. Journal of medical Internet research. 2024 May 22:26():e53164. doi: 10.2196/53164. Epub 2024 May 22 [PubMed PMID: 38776130]
Level 1 (high-level) evidenceCollins GS, Moons KGM, Dhiman P, Riley RD, Beam AL, Van Calster B, Ghassemi M, Liu X, Reitsma JB, van Smeden M, Boulesteix AL, Camaradou JC, Celi LA, Denaxas S, Denniston AK, Glocker B, Golub RM, Harvey H, Heinze G, Hoffman MM, Kengne AP, Lam E, Lee N, Loder EW, Maier-Hein L, Mateen BA, McCradden MD, Oakden-Rayner L, Ordish J, Parnell R, Rose S, Singh K, Wynants L, Logullo P. TRIPOD+AI statement: updated guidance for reporting clinical prediction models that use regression or machine learning methods. BMJ (Clinical research ed.). 2024 Apr 16:385():e078378. doi: 10.1136/bmj-2023-078378. Epub 2024 Apr 16 [PubMed PMID: 38626948]
Moons KGM, Damen JAA, Kaul T, Hooft L, Andaur Navarro C, Dhiman P, Beam AL, Van Calster B, Celi LA, Denaxas S, Denniston AK, Ghassemi M, Heinze G, Kengne AP, Maier-Hein L, Liu X, Logullo P, McCradden MD, Liu N, Oakden-Rayner L, Singh K, Ting DS, Wynants L, Yang B, Reitsma JB, Riley RD, Collins GS, van Smeden M. PROBAST+AI: an updated quality, risk of bias, and applicability assessment tool for prediction models using regression or artificial intelligence methods. BMJ (Clinical research ed.). 2025 Mar 24:388():e082505. doi: 10.1136/bmj-2024-082505. Epub 2025 Mar 24 [PubMed PMID: 40127903]
Level 2 (mid-level) evidenceAtkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, Guyatt GH, Harbour RT, Haugh MC, Henry D, Hill S, Jaeschke R, Leng G, Liberati A, Magrini N, Mason J, Middleton P, Mrukowicz J, O'Connell D, Oxman AD, Phillips B, Schünemann HJ, Edejer T, Varonen H, Vist GE, Williams JW Jr, Zaza S, GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ (Clinical research ed.). 2004 Jun 19:328(7454):1490 [PubMed PMID: 15205295]
Level 2 (mid-level) evidenceIoannidis JP. Why most published research findings are false. PLoS medicine. 2005 Aug:2(8):e124 [PubMed PMID: 16060722]
Jefferson T, Doshi P, Boutron I, Golder S, Heneghan C, Hodkinson A, Jones M, Lefebvre C, Stewart LA. When to include clinical study reports and regulatory documents in systematic reviews. BMJ evidence-based medicine. 2018 Dec:23(6):210-217. doi: 10.1136/bmjebm-2018-110963. Epub 2018 Oct 11 [PubMed PMID: 30309870]
Level 1 (high-level) evidenceEgger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ (Clinical research ed.). 1997 Sep 13:315(7109):629-34 [PubMed PMID: 9310563]
Level 1 (high-level) evidenceBurns PB, Rohrich RJ, Chung KC. The levels of evidence and their role in evidence-based medicine. Plastic and reconstructive surgery. 2011 Jul:128(1):305-310. doi: 10.1097/PRS.0b013e318219c171. Epub [PubMed PMID: 21701348]
Smith GC, Pell JP. Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials. BMJ (Clinical research ed.). 2003 Dec 20:327(7429):1459-61 [PubMed PMID: 14684649]
Level 1 (high-level) evidenceHorwitz RI, Charlson ME, Singer BH. Medicine based evidence and personalized care of patients. European journal of clinical investigation. 2018 Jul:48(7):e12945. doi: 10.1111/eci.12945. Epub 2018 Jun 4 [PubMed PMID: 29700817]
Steves R, Hootman JM. Evidence-Based Medicine: What Is It and How Does It Apply to Athletic Training? Journal of athletic training. 2004 Mar:39(1):83-87 [PubMed PMID: 15085215]
Finlayson SG, Subbaswamy A, Singh K, Bowers J, Kupke A, Zittrain J, Kohane IS, Saria S. The Clinician and Dataset Shift in Artificial Intelligence. The New England journal of medicine. 2021 Jul 15:385(3):283-286. doi: 10.1056/NEJMc2104626. Epub [PubMed PMID: 34260843]