Introduction
The middle ear is an air-filled cavity within the petrous portion of the temporal bone, commonly known as the tympanic cavity. The middle ear lies between the tympanic membrane laterally and the oval window medially, connecting the outer and inner ears. The cavity contains the 3 auditory ossicles—the malleus, incus, and stapes—which transmit and amplify sound vibrations from the tympanic membrane to the oval window. Movement of the stapes footplate at the oval window transfers mechanical energy into the fluid-filled inner ear and initiates hearing. The middle ear communicates posteriorly with the mastoid air cell system and anteriorly with the eustachian tube, which provides ventilation and helps equalize pressure within the middle ear space.[1][2][3] The tensor tympani and the stapedius are middle ear muscles that adjust ossicular mobility and activate the acoustic reflex, reducing sound energy transmission to protect cochlear structures from excessive acoustic stimulation.
Arterial supply of the middle ear arises primarily from branches of the external carotid system, with additional contribution from the internal carotid system, including the anterior tympanic, stylomastoid, petrosal, and caroticotympanic arteries. Venous drainage is predominantly via the pterygoid venous plexus. Sensory innervation derives predominantly from the tympanic plexus on the promontory, formed by the tympanic branch of the glossopharyngeal nerve (cranial nerve IX) and caroticotympanic sympathetic fibers. The tensor tympani receives motor innervation from the mandibular division of the trigeminal nerve (cranial nerve V3), whereas the stapedius is supplied by the facial nerve (cranial nerve VII) via the nerve to the stapedius.
Disorders affecting the middle ear frequently impair sound transmission and pressure regulation, resulting in hearing loss, otalgia, tinnitus, vertigo, or recurrent infection. Safe performance of middle ear and mastoid procedures depends on accurate identification of the ossicular chain, facial nerve, chorda tympani, oval window, and surrounding structures. A thorough understanding of middle ear anatomy and physiology assists clinicians in evaluating hearing disorders, interpreting examination findings, and preventing procedure-related complications.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Tympanic Membrane
The tympanic membrane separates the external auditory canal from the middle ear cavity and functions as the primary structure transmitting sound energy into the middle ear. The majority of the tympanic membrane consists of the pars tensa, a taut fibrous region that vibrates in response to sound waves and conducts most sound energy to the ossicular chain. In contrast, the pars flaccida (Shrapnell membrane) is a small, more compliant triangular region located in the superior portion of the tympanic membrane. The relative lack of fibrous support renders the pars flaccida more sensitive to changes in middle ear pressure and allows independent movement from the pars tensa. During otoscopic examination, the pars flaccida is often the first portion of the tympanic membrane to demonstrate retraction or bulging in response to pressure changes. This response occurs when a Valsalva maneuver is performed or when middle ear pressure is increased in association with conditions such as acute otitis media.[4][5]
Auditory Ossicles
The middle ear contains 3 auditory ossicles—the malleus, incus, and stapes—that transmit and amplify sound vibrations from the tympanic membrane to the inner ear. Vibrations of the tympanic membrane transmit first to the malleus, which is firmly attached to the medial surface of the membrane. The malleus articulates with the incus, which connects to the stapes, the smallest bone in the human body. The stapes footplate is secured within the oval window, where movement converts mechanical vibrations into pressure waves within the perilymph of the inner ear. Fluid waves stimulate cochlear sensory structures and initiate auditory perception.[6][7]
The ossicular chain functions as an impedance-matching system, facilitating efficient transfer of sound energy from the air-filled outer and middle ears to the fluid-filled inner ear. Combined effects of the tympanic membrane-to-oval window area ratio and ossicular lever action increase sound pressure at the oval window by approximately 20 to 30 dB. This amplification minimizes energy loss at the air–fluid interface and maintains normal hearing sensitivity.[8]
Muscles
The middle ear contains 2 small muscles that attach to the ossicular chain: the tensor tympani and the stapedius. These muscles dynamically regulate sound transmission within the middle ear and contribute to the acoustic reflex, a protective mechanism that attenuates excessive acoustic stimulation reaching the inner ear.[9][10]
The tensor tympani receives innervation from the mandibular division of the trigeminal nerve via the nerve to the medial pterygoid. The muscle originates from the cartilaginous portion of the eustachian tube, the greater wing of the sphenoid bone, and the adjacent temporal bone, and inserts into the manubrium and neck of the malleus. Contraction of the tensor tympani increases tension on the tympanic membrane and ossicular chain, reducing mobility. Although activation may occur with intense sound, tensor tympani activity more commonly accompanies nonauditory stimuli, such as chewing, swallowing, speaking, and startle responses.
The stapedius receives innervation from the facial nerve via the nerve to the stapedius and inserts into the neck of the stapes. Stapedius contraction serves as the principal effector of the acoustic reflex in humans. Loud sounds stimulate auditory pathways within the brainstem, resulting in bilateral activation of the stapedius muscles. Contraction of the stapedius increases stiffness of the ossicular chain and reduces transmission of sound energy, particularly at lower frequencies, from the middle ear to the cochlea.
The acoustic reflex is typically elicited by sounds approximately 70 to 100 dB above the hearing threshold and produces bilateral stapedius contraction regardless of which ear receives the stimulus. Increased ossicular stiffness attenuates the transmission of excessive acoustic energy to the inner ear. However, reflex latency of approximately 25 to 150 milliseconds limits protection against impulse noises, such as those associated with explosions or gunshots, with greater effectiveness against prolonged loud sounds.[11]
Together, the tensor tympani and stapedius modulate middle ear mechanics by increasing the stiffness of the tympanic membrane and ossicular chain. In addition to a protective role, these muscles may optimize auditory perception in complex acoustic environments by attenuating low-frequency background noise.[12]
Clinical assessment of the acoustic reflex provides valuable information regarding the integrity of the middle ear, cochlea, auditory nerve, brainstem auditory pathways, and facial nerve. Dysfunction of the reflex pathway may occur in disorders affecting any of these structures. Lesions of the facial nerve proximal to the nerve to the stapedius may abolish the acoustic reflex and result in hyperacusis, a condition characterized by increased sensitivity to sound.[13]
Eustachian Tube
The eustachian tube, also known as the auditory or pharyngotympanic tube, connects the middle ear cleft to the nasopharynx and serves as the principal regulator of middle ear ventilation and pressure homeostasis. In adults, the tube measures approximately 36 mm in length and consists of a lateral osseous portion and a medial cartilaginous portion. The cartilaginous segment remains closed under normal conditions, forming a protective barrier between the middle ear and the nasopharynx.[14]
The eustachian tube performs 3 essential functions: ventilation and pressure equalization of the middle ear, clearance of middle ear secretions, and protection of the middle ear from nasopharyngeal pathogens, secretions, and pressure fluctuations. Periodic opening of the tube allows equilibration of middle ear pressure with ambient atmospheric pressure, maintaining optimal mobility of the tympanic membrane and ossicular chain for sound transmission. Opening of the eustachian tube facilitates equalization of ambient air pressure with middle ear pressure. Drainage of middle ear secretions occurs through this pathway (see Image. Tympanic Cavity).[15][16]
Active opening of the eustachian tube occurs primarily through contraction of the tensor veli palatini muscle during pharyngeal activities, such as swallowing, yawning, and chewing. The tensor veli palatini inserts onto the lateral lamina of the cartilaginous eustachian tube and functions as the principal dilator of the tube, facilitating middle ear ventilation and pressure equalization.
The levator veli palatini lies immediately inferior and medial to the cartilaginous eustachian tube. Medial rotation of the cartilaginous framework during swallowing provides a minor contribution to tubal opening, although activity of the tensor veli palatini remains the dominant mechanism of active eustachian tube dilation.
The salpingopharyngeus muscle originates from the inferior aspect of the cartilaginous eustachian tube and descends within the salpingopharyngeal fold to blend with fibers of the palatopharyngeus muscle. This muscle elevates the pharynx and larynx during swallowing and phonation and plays a role in the coordination of pharyngeal and tubal movements. Direct contribution to eustachian tube dilation is limited compared with the tensor veli palatini.[17][18]
The mucosal lining of the eustachian tube is continuous with that of the middle ear and respiratory tract and contains ciliated pseudostratified columnar epithelium. Mucociliary transport directs secretions from the middle ear toward the nasopharynx, facilitating clearance of fluid, debris, and inflammatory products from the middle ear space.[19]
Eustachian tube dysfunction impairs middle ear ventilation and clearance mechanisms, resulting in negative middle ear pressure, tympanic membrane retraction, middle ear effusion, conductive hearing loss, and chronic inflammatory middle ear disease. Persistent dysfunction is a major contributing factor in the pathogenesis of otitis media with effusion, chronic otitis media, tympanic membrane atelectasis, and acquired cholesteatoma. Eustachian tube dysfunction constitutes a lifelong determinant of auditory and vestibular health, contributing to conductive impairment and progressive sensorineural and mixed hearing loss.[20]
Clinical evaluation of eustachian tube function is an essential component of otologic assessment. Aural fullness, pressure sensation, fluctuating hearing, tinnitus, and discomfort during ambient pressure changes commonly characterize dysfunction. Management strategies target underlying causes and aim to restore normal middle ear ventilation and drainage.[21]
Equalization of Pressure
Optimal hearing requires air pressure within the middle ear to closely approximate ambient atmospheric pressure. Under these conditions, the tympanic membrane and ossicular chain vibrate freely, allowing efficient transmission of sound energy to the inner ear. Pressure differences between the middle ear and external environment reduce tympanic membrane compliance, impair ossicular motion, and decrease acoustic transmission, resulting in conductive hearing loss. Severe pressure differentials may produce middle ear barotrauma, tympanic membrane retraction, middle ear effusion, hemotympanum, or tympanic membrane perforation.[22]
The middle ear cleft, which encompasses the tympanic cavity and mastoid air cell system, functions as a single aerated space. Continuous gas exchange across the middle ear mucosa creates a gradual tendency toward negative pressure within the cavity. Periodic ventilation through the eustachian tube maintains pressure equilibrium and preserves normal middle ear function.
The eustachian tube normally remains closed and opens transiently during pharyngeal activities. Tube opening permits airflow between the nasopharynx and the middle ear, equalizing middle ear pressure with ambient atmospheric pressure. Contraction of the tensor veli palatini primarily mediates this process, functioning as the principal dilator of the cartilaginous eustachian tube.[23][24][25]
Failure of normal pressure equalization results in eustachian tube dysfunction and persistent negative middle ear pressure. Chronic impairment of middle ear ventilation contributes to tympanic membrane retraction, otitis media with effusion, conductive hearing loss, and acquired cholesteatoma. Pressure-related symptoms commonly present when altitude changes rapidly, such as during air travel or scuba diving, and ambient pressure fluctuations exceed the capacity of the eustachian tube to equilibrate the middle ear.[26]
Embryology
Tympanic Membrane
The tympanic membrane is a trilaminar structure derived from all 3 germ layers. The tympanic membrane comprises an outer ectodermal layer, an inner endodermal layer, and an intervening fibrous layer derived from mesenchyme of mesodermal and neural crest–derived origin.
The tympanic membrane forms at the junction of the 1st pharyngeal cleft (ectoderm) and the 1st pharyngeal pouch (endoderm) during embryologic development. Ectoderm from the 1st pharyngeal groove and endoderm from the 1st pharyngeal pouch converge to form the epithelial components of the membrane around the 5th week of gestation. The central fibrous layer develops from intervening mesenchyme, which differentiates into connective tissue that provides structural integrity and tensile strength.[27]
Progressive apposition and maturation of these layers produce the definitive trilaminar tympanic membrane, composed of an outer cutaneous ectodermal layer, a middle fibrous layer (lamina propria), and an inner mucosal endodermal layer. This structure establishes the anatomic and functional interface between the external auditory canal and the middle ear.[28]
Tympanic Cavity and Ossicles
The tympanic cavity develops from endoderm of the 1st pharyngeal pouch, which expands laterally toward the developing external auditory structures. This endodermal extension forms the epithelial lining of the middle ear space and contributes to the development of the eustachian tube, tympanic cavity, and mastoid antrum.
The auditory ossicles begin their development during the 6th to 8th weeks of gestation from neural crest–derived mesenchyme within the 1st and 2nd pharyngeal arches. The malleus and incus derive primarily from the Meckel cartilage of the 1st pharyngeal arch. In contrast, the stapes arises from the Reichert cartilage of the 2nd pharyngeal arch, with contributions from neural crest–derived mesenchyme.
Mesenchymal tissue fills the tympanic cavity and surrounds the developing ossicles during early development. Progressive ossification of the ossicles is followed by resorption of this mesenchymal tissue, allowing formation of an air-filled cavity. Postnatally, the middle ear becomes an aerated space, and ossicles remain suspended by ligaments and mucosal folds rather than embedded within tissue. A similar resorption and aeration process occurs in the development of the mastoid air cell system, which arises from the mastoid antrum and progressively pneumatizes during childhood.[29]
Eustachian Tube
The eustachian tube develops from endoderm of the 1st pharyngeal pouch, specifically the tubotympanic recess. This endodermal structure forms the epithelial lining of both the middle ear cavity and the eustachian tube, establishing a connection between the nasopharynx and the middle ear cleft. Surrounding mesenchyme of mesodermal origin contributes to the development of the cartilaginous and supportive structures of the tube. The epithelial lining is continuous with the upper respiratory tract.
Postnatal development involves craniofacial growth with progressive elongation of the eustachian tube and alteration of its orientation. The tube lies relatively horizontal in infancy. In adulthood, the tube assumes a more oblique orientation, angling inferolateral to superomedial. This change in orientation enhances efficiency of middle ear ventilation and clearance.
Clinically, the immature anatomy and function of the pediatric eustachian tube contribute to increased susceptibility to middle ear disease. The horizontal orientation, combined with the relative cartilaginous compliance and less efficient muscular opening, predisposes infants and young children to impaired pressure equalization, fluid retention, and recurrent otitis media. Maturation of tubal function and progressive angulation reduce the frequency of middle ear effusions and infectious episodes.
Eustachian tube dysfunction in any age group disrupts middle ear pressure homeostasis. The condition is a key pathophysiologic mechanism in otitis media with effusion, chronic otitis media, tympanic membrane retraction, and acquired cholesteatoma formation.
The eustachian tube arises as a proximal expansion of the tympanic cavity. This tube develops from endoderm of the 1st pharyngeal pouch and ectoderm of the 1st branchial cleft. Cartilage and muscle associated with the eustachian tube derive from mesoderm.[30]
Muscles
The muscles of the middle ear and surrounding nasopharyngeal region are derived from mesoderm of the pharyngeal (branchial) arches, with innervation patterns reflecting embryologic origin. The tensor tympani and tensor veli palatini arise from mesoderm of the 1st pharyngeal arch and receive innervation from the mandibular division of the trigeminal nerve. The tensor veli palatini functions as the primary muscle responsible for the active opening of the eustachian tube, facilitating middle ear ventilation and pressure equalization. Contraction of the tensor tympani produces low-frequency conductive hearing changes while modulating sound transmission through the middle ear.[31] The stapedius originates from mesoderm of the 2nd pharyngeal arch and receives innervation from the facial nerve. This muscle functions as the principal effector of the acoustic reflex, reducing transmission of excessive sound energy to the inner ear through stiffening of the ossicular chain.[32]
The levator veli palatini is derived from mesoderm of the 4th pharyngeal arch and receives innervation from the vagus nerve (cranial nerve X) via the pharyngeal plexus. This muscle elevates the soft palate and supports eustachian tube function during swallowing. The salpingopharyngeus also originates from the 4th pharyngeal arch and receives innervation from the vagus nerve. This muscle has limited direct contribution to eustachian tube opening despite its anatomical association with the cartilaginous tube.[33]
Clinically, coordinated function of these muscles is essential for maintenance of middle ear pressure homeostasis and protection of cochlear function. Dysfunction of the tensor veli palatini may contribute to eustachian tube dysfunction and middle ear disease. Impairment of the stapedius reflex, such as in facial nerve pathology, may result in hyperacusis due to reduced attenuation of loud sound transmission.[34][35]
Blood Supply and Lymphatics
Arterial Supply
The vascular supply of the middle ear cleft is derived from branches of both the external and internal carotid arterial systems, reflecting complex embryologic development and extensive mucosal surface area. Arterial supply to the middle ear and eustachian tube is characterized by extensive anastomoses between branches of the external and internal carotid systems, providing robust collateral circulation while creating potential pathways for hematogenous spread of infection and inflammation. This vascular network supports mucosal function but contributes to persistent middle ear disease, increased intraoperative bleeding risk during otologic and skull base procedures, and potential vascular spread of middle ear or nasopharyngeal pathology to adjacent intracranial and deep neck structures.
The tympanic membrane receives a dual blood supply. The lateral (cutaneous) surface is supplied primarily by the anterior tympanic artery, a branch of the maxillary artery, with additional contribution from the deep auricular artery. The medial (mucosal) surface receives blood supply from middle ear vascular branches, including contributions from the stylomastoid artery. A smaller contribution arises from the internal carotid artery via the caroticotympanic arteries.[36]
The middle ear cavity is supplied by an anastomotic vascular network derived from multiple arterial sources. Contributors include the tympanic (tubal) branch of the middle meningeal artery, the superior tympanic artery (middle meningeal artery), the petrosal branch of the middle meningeal artery, caroticotympanic branches of the internal carotid artery, and the stylomastoid artery, most commonly arising from the posterior auricular artery. The inferior tympanic artery, a branch of the ascending pharyngeal artery, contributes to perfusion in the medial wall and promontory region.
The eustachian tube receives a mixed arterial supply from nasopharyngeal and middle ear–associated vascular systems, including tympanic branches of the middle meningeal artery, caroticotympanic branches of the internal carotid artery, deep auricular artery, pharyngeal branches of the maxillary artery, ascending palatine artery of the facial artery, and the inferior tympanic artery from the ascending pharyngeal artery. A minor contribution may occasionally arise from the artery of the pterygoid canal (Vidian artery), particularly near the cartilaginous portion and nasopharyngeal junction.
Venous Drainage
Venous drainage of the middle ear cleft parallels the arterial supply and establishes extensive connections with extracranial and intracranial venous systems. The tympanic cavity and tympanic membrane primarily drain into the pterygoid venous plexus. Additional venous outflow occurs through the superior petrosal sinus, providing communication with intracranial venous circulation. The stylomastoid region drains via accompanying venous channels into the posterior auricular and retromandibular venous systems. The eustachian tube drains predominantly into the pterygoid venous plexus, with minor drainage into the pharyngeal venous plexus. These venous connections are clinically relevant pathways for spread of infection between the nasopharynx, middle ear, and intracranial structures.
Lymphatic Drainage
Lymphatic drainage of the middle ear cleft reflects dual relationships with the external ear and nasopharynx. The lateral surface of the tympanic membrane drains primarily to the preauricular (parotid) lymph nodes, while the middle ear cavity and the medial surface of the tympanic membrane drain to the deep cervical lymph nodes, particularly the jugulodigastric group. The eustachian tube drains predominantly to the retropharyngeal lymph nodes, with secondary drainage to the deep cervical lymph node chain. This pattern reflects embryologic origin from the nasopharyngeal endoderm. Clinical relevance includes potential spread of nasopharyngeal infection and inflammatory disease to the middle ear cleft.[37][38]
Nerves
Sensory innervation of the tympanic membrane is divided between external and internal surfaces, reflecting a composite embryologic origin. The external (lateral) surface receives overlapping somatic sensory input from 3 cranial nerves. The posterior-superior region is supplied by the auricular branch of the facial nerve, the posterior-inferior region by the auricular branch of the vagus nerve, and the anterosuperior region by the auriculotemporal nerve. The overlapping distribution contributes to variability and the often poorly localized nature of referred otalgia.
The medial (internal) surface of the tympanic membrane, along with the mucosa of the middle ear cavity, receives primary innervation from the tympanic plexus on the promontory of the middle ear. The tympanic plexus is formed predominantly by the tympanic branch of the glossopharyngeal nerve, with contributions from sympathetic fibers via the carotid plexus. The glossopharyngeal contribution continues as the lesser petrosal nerve and participates in parasympathetic pathways to the otic ganglion.
Sensory innervation of the eustachian tube is similarly mixed. The cartilaginous and nasopharyngeal portion receives sensory fibers primarily from the maxillary nerve (cranial nerve V2) via branches associated with the pterygopalatine ganglion and pharyngeal innervation. The bony portion receives additional sensory input from the tympanic plexus. The dual innervation reflects anatomic and functional continuity between the nasopharynx and middle ear cleft.
The innervation patterns of the middle ear muscles correspond to their pharyngeal arch origins. The tensor tympani is supplied by a branch of the mandibular nerve, reflecting its development from the 1st pharyngeal arch. The stapedius receives innervation from the facial nerve, corresponding to its 2nd pharyngeal arch derivation. These muscles function in the acoustic reflex to regulate ossicular stiffness and attenuate sound transmission.
Muscles associated with the eustachian tube and surrounding pharynx are innervated according to embryologic origin. The tensor veli palatini receives innervation from the mandibular nerve and serves as the primary active dilator of the eustachian tube during swallowing and related pharyngeal movements. The levator veli palatini and salpingopharyngeus receive innervation from the vagus nerve via the pharyngeal plexus and contribute to coordinated elevation of the soft palate and the pharyngeal wall, with secondary roles in supporting eustachian tube function.[39][40][41]
Muscles
The middle ear contains 2 small skeletal muscles that attach to the ossicular chain: the tensor tympani and the stapedius. These muscles are components of the acoustic reflex system and function to modulate sound transmission to the inner ear by increasing stiffness of the ossicular chain and reducing amplitude of sound-induced vibrations.
The tensor tympani attaches to the manubrium and neck of the malleus. Contraction increases tension on the tympanic membrane and reduces ossicular mobility, with preferential limitation of low-frequency sound transmission. The stapedius attaches to the neck of the stapes and stabilizes the stapes footplate at the oval window during contraction, further increasing ossicular chain stiffness. The combined activity of these muscles attenuates excessive acoustic energy reaching the cochlea and demonstrates greater effectiveness for sustained loud sounds due to acoustic reflex latency.
The primary muscle responsible for the active opening of the eustachian tube is the tensor veli palatini (see Image. Anatomical Relationships of the Tensor Veli Palatini and Pharyngeal Orifice). Contraction of this muscle dilates the cartilaginous portion of the eustachian tube during pharyngeal movements, permitting ventilation of the middle ear and equilibration of pressure between the nasopharynx and the middle ear. The levator veli palatini and salpingopharyngeus provide secondary pharyngeal support but do not directly open the eustachian tube.
Clinically, dysfunction of the stapedius reflex, most commonly due to facial nerve pathology proximal to the nerve to the stapedius, results in hyperacusis and increased sensitivity to everyday sound levels. Lesions affecting the acoustic reflex pathway at the level of the cochlea, auditory nerve, or brainstem nuclei similarly disrupt protective attenuation of loud sound.
Abnormal function of the tensor veli palatini is a central mechanism in eustachian tube dysfunction, leading to impaired middle ear ventilation and pressure regulation. The resulting manifestations include aural fullness, development of negative middle ear pressure, tympanic membrane retraction, otitis media with effusion, and, in chronic cases, cholesteatoma formation due to persistent retraction pockets. Pediatric populations demonstrate increased susceptibility due to the developmental immaturity of eustachian tube angulation and muscular efficiency.
Physiologic Variants
Middle ear function exhibits a range of physiological differences arising from variations in developmental anatomy, tissue flexibility, and neuromuscular performance. Variation is particularly evident in eustachian tube mechanics, ossicular chain function, and tympanic membrane compliance, affecting regulation of pressure and transmission of sound. These differences do not necessarily indicate disease.[42]
The eustachian tube demonstrates the greatest physiologic variation relevant to clinical practice.[43] Variation in length, angulation, cartilage stiffness, and mucosal compliance affects efficiency of middle ear ventilation. In infants and young children, a shorter, more horizontal, and more compliant eustachian tube reduces effectiveness of pressure regulation compared with the more oblique adult configuration. Interindividual variation in tensor veli palatini strength also influences tubal opening during swallowing and related pharyngeal movements. These variations may produce transient or situational changes in middle ear pressure, particularly in the setting of rapid environmental pressure shifts, such as during altitude changes, or upper respiratory infections.
Physiological variation also affects ossicular chain mechanics. Minor differences in ligament laxity, joint stiffness at the incudomalleolar and incudostapedial joints, and tympanic membrane flexibility influence sound transmission across different frequencies. These variations remain within normal limits but may produce slight differences in hearing sensitivity among individuals. Hearing loss associated with tympanic membrane perforation correlates with perforation size and the extent of middle ear and mastoid pneumatization, provided middle ear mucosa and ossicular structures are normal. Both perforation size and degree of pneumatization warrant consideration in the management of tympanic membrane perforations.[44][45]
Tympanic membrane compliance depends on structural thickness and connective tissue composition, influencing vibratory efficiency without resulting in conductive hearing loss. Acoustic reflex sensitivity thresholds also vary among individuals while maintaining normal protective function.[46]
Distinction between physiological variation and pathology is essential. Chronic eustachian tube dysfunction, otitis media with effusion, ossicular fixation (including otosclerosis), tympanic membrane retraction, and ossicular discontinuity involve structural or inflammatory abnormalities that produce persistent or progressive impairment of sound transmission or middle ear ventilation. [Source: McCoul, ED. Eustachian Tube Dysfunction: Evidence and Controversies. 2020] Physiological variants are reversible, situational, and part of normal middle ear function. Accurate differentiation in clinical practice prevents overdiagnosis and supports appropriate identification of clinically significant otologic disease.
Surgical Considerations
Tympanostomy
Tympanostomy, or ventilation tube placement, is used to restore airflow and fluid drainage in the middle ear, particularly in otitis media with effusion and recurrent acute otitis media.[47] The procedure involves a myringotomy incision in the anteroinferior or posteroinferior portion of the tympanic membrane, where risk to adjacent structures, such as the ossicular chain, chorda tympani, and major blood vessels, is minimized. Ventilation tubes are then inserted to maintain sustained middle ear aeration and prevent fluid reaccumulation.
Premature extrusion of tympanostomy tubes may occur, particularly during chronic or resolving inflammation. Contributing factors include tympanic membrane thickening, altered compliance, and pressure imbalance between the external auditory canal and middle ear, which may result in displacement of the tube into the external canal before intended removal.
Complications of tympanostomy include persistent tympanic membrane perforation, otorrhea, tympanosclerosis, tube blockage, and premature extrusion. Less common complications include focal atrophy or scarring of the tympanic membrane. Contraindications are mostly relative and include uncontrolled coagulopathy, active external ear infection in selected cases, and inability to safely administer anesthesia when required.
Stapedectomy and Stapedotomy
Stapedectomy and stapedotomy are performed in patients with conductive hearing loss due to stapes fixation, most commonly resulting from otosclerosis. Stapedectomy involves removal of the stapes suprastructure, with prosthesis placement to restore continuity of the ossicular chain at the oval window. Stapedotomy pertains to the creation of a fenestration in the fixed stapes footplate, followed by prosthesis insertion to reestablish ossicular chain continuity at the oval window. The chorda tympani is identified and may be gently mobilized during either procedure to improve access to the oval window.
Both stapedotomy and stapedectomy provide favorable hearing outcomes with low complication rates in patients with otosclerosis. Stapedotomy is the preferred technique. In cases where intraoperative conversion to stapedectomy is required, operative outcomes remain favorable with appropriate surgical execution and technique.[48]
Complications of stapes surgery include vertigo, sensorineural hearing loss, taste disturbance due to chorda tympani injury, prosthesis displacement or migration, perilymphatic fistula, and, in rare cases, profound hearing loss (“dead ear”). Contraindications include active middle ear infection, poor cochlear reserve (with manifestations such as poor speech discrimination or advanced sensorineural hearing loss), and medical conditions precluding safe anesthesia or surgical tolerance.[49]
Bone-Conduction Hearing Devices
Bone-conduction hearing devices are indicated for conductive or mixed hearing loss in which middle ear reconstruction is not feasible or is ineffective. These devices use titanium implants inserted into the mastoid bone to transmit vibrations directly to the cochlea, bypassing the ossicular chain.[50] Active middle ear implants comprise an alternative approach, using transducers attached to the ossicles to enhance mechanical vibration in response to sound.
Newer active transcutaneous systems, including Osia® and Bonebridge™, utilize advanced electronic signal transmission, improve bone-conduction efficiency, and reduce the risk of skin-related adverse effects.[51] Complications of bone-conduction devices include skin irritation or infection at the implant site, device failure, osseointegration failure, soft tissue overgrowth, and the need for revision surgery. Contraindications include insufficient bone quality, active infection at the implantation site, and inability to maintain implant hygiene or adhere to postoperative care requirements.
Balloon Dilation Eustachian Tuboplasty
Balloon dilation eustachian tuboplasty (BDET), also known as eustachian tube balloon dilation, is used to treat chronic obstructive eustachian tube dysfunction. The procedure involves insertion of a balloon catheter through the nasal cavity into the cartilaginous portion of the eustachian tube. The balloon is then inflated under controlled pressure to expand the lumen and promote mucosal remodeling, supporting improved long-term ventilatory function.
BDET aims to prevent, reverse, or halt disease progression through dilation of the cartilaginous eustachian tube and restoration of functional patency. Reported outcomes are generally favorable, supporting broader clinical application in appropriately selected patients with eustachian tube dysfunction.[52]
Complications of BDET include epistaxis, mucosal injury, submucosal dissection, transient otalgia, barotrauma, and, rarely, carotid artery injury due to proximity to the parapharyngeal carotid space. Contraindications include carotid canal dehiscence or aberrant carotid anatomy, active infection of the nasopharynx or middle ear, and inability to safely access the eustachian tube via the transnasal route.
Clinical Significance
Clinical Correlates of Middle Ear Pressure, Sound Transmission, and Pathology
The tympanic membrane is highly responsive to pressure changes from both external and internal sources. Rupture may result from rapid external pressure changes, such as those seen in barotrauma during diving or flying, exposure to loud sounds, or mechanical injury. Internal causes include acute or chronic middle ear infections, in which inflammatory fluid accumulates within the middle ear and exerts sustained positive pressure on the tympanic membrane. Otoscopic examination in acute otitis media may reveal a bulging, convex tympanic membrane due to increased middle ear pressure.
Middle ear pressure regulation depends on intermittent opening of the eustachian tube during pharyngeal activities. Inadequate pressure equalization produces stress on the tympanic membrane, leading to otalgia, conductive hearing loss, or, in severe cases, rupture. Individuals exposed to rapid ambient pressure changes, such as pilots and divers, require effective eustachian tube function to reduce the risk of barotrauma.
Otitis media occurs more frequently in children due to anatomic and functional differences of the eustachian tube. The tube is shorter, more compliant, and more horizontally oriented in pediatric patients, reducing effectiveness of middle ear ventilation and drainage. With craniofacial development, the eustachian tube lengthens and assumes a more oblique inferolateral-to-superomedial orientation. This change improves passive drainage and facilitates active opening, thereby reducing infection risk.
Additional notable middle ear disorders include ossicular chain discontinuity and ossicular fixation. Ossicular chain discontinuity, often resulting from trauma or chronic inflammation with erosion, impairs mechanical transmission of sound from the tympanic membrane to the oval window, resulting in maximal conductive hearing loss. Ossicular fixation, as seen in otosclerosis, restricts ossicular mobility and produces progressively worsening conductive hearing loss, typically with greater involvement of low frequencies.
Chronic middle ear disease may lead to cholesteatoma, a keratinizing epithelial growth that often develops from tympanic membrane retraction pockets, usually secondary to chronic eustachian tube dysfunction. Cholesteatoma demonstrates local destructive potential through enzymatic bone erosion and may involve the ossicles, facial nerve canal, and adjacent temporal bone structures. Progressive disease can result in conductive hearing loss, persistent otorrhea, and complications from extension into surrounding tissues.
Clinical features of tympanic membrane rupture include otalgia, conductive hearing loss, and, occasionally, tinnitus. Most perforations heal spontaneously. However, the healing period carries an increased risk of middle ear contamination and secondary infection. Strict water precautions are recommended, along with avoidance of foreign body insertion into the external auditory canal during recovery.
The Facial Nerve and the Middle Ear Cleft
Facial nerve dysfunction can significantly affect middle ear physiology, as this cranial nerve supplies the stapedius via the nerve to the stapedius. Facial nerve involvement impairs the muscle in Bell palsy, a condition typically caused by idiopathic inflammation associated with reactivation of latent neurotropic viruses, such as herpes simplex virus. Loss of stapedius function results in failure of the acoustic reflex, reduced dampening of ossicular chain movement, and hyperacusis, a heightened sensitivity to sound.
Facial nerve dysfunction may also arise from causes beyond idiopathic Bell palsy, including infection, trauma, inflammation, or iatrogenic injury. Functional impact on the stapedius depends on lesion location. Infectious causes include acute otitis media and mastoiditis, in which inflammation within the temporal bone may involve the facial nerve as it traverses the fallopian (facial) canal. Facial nerve involvement in these settings may indicate severe middle ear or mastoid disease and warrants prompt clinical assessment.
Traumatic facial nerve injury most often occurs in association with temporal bone fractures. Longitudinal fractures occur more frequently and typically involve the external auditory canal and middle ear, often resulting in delayed or partial facial nerve dysfunction. Transverse fractures occur less commonly but tend to involve the otic capsule and produce immediate, severe facial nerve paralysis due to direct nerve injury. In both patterns, involvement of the facial nerve proximal to the nerve to the stapedius results in loss of acoustic reflex attenuation and contributes to hyperacusis.
Iatrogenic facial nerve injury most commonly occurs during otologic and skull base surgery, particularly during drilling of the mastoid or middle ear. Injury may involve exposure or inadvertent damage to the horizontal segment of the facial nerve within the temporal bone. The risk increases when the nerve is dehiscent, displaced, or obscured by chronic inflammation or cholesteatoma. Regardless of etiology, stapedius dysfunction eliminates an important protective mechanism of the middle ear, increasing sound energy transmission to the cochlea and resulting in abnormal auditory sensitivity.
Other Issues
Several clinically relevant considerations arise when interpreting middle ear physiology across the spectrum of normal variation and disease. Physiologic variability in eustachian tube function, ossicular mechanics, and tympanic membrane compliance may overlap with early or mild manifestations of pathology, particularly in pediatric populations or individuals experiencing transient inflammation. A key diagnostic challenge involves distinguishing reversible, situational variations in middle ear pressure regulation from early eustachian tube dysfunction. Temporary impairment of tubal opening due to upper respiratory inflammation or environmental pressure changes may mimic early disease but does not indicate structural failure. Subtle interindividual differences in ossicular chain mechanics or tympanic membrane compliance may also contribute to audiometric variability without clinically significant hearing loss.
Overinterpretation of physiologic variation may lead to unnecessary labeling of disease, particularly in patients with transient symptoms, such as mild aural fullness or short-lived conductive fluctuation. Careful correlation of symptoms with persistence and progression, together with objective findings, is essential to avoid misdiagnosis. Understanding physiologic variability is essential for distinguishing normal functional differences from otologic conditions requiring treatment.
Media
(Click Image to Enlarge)
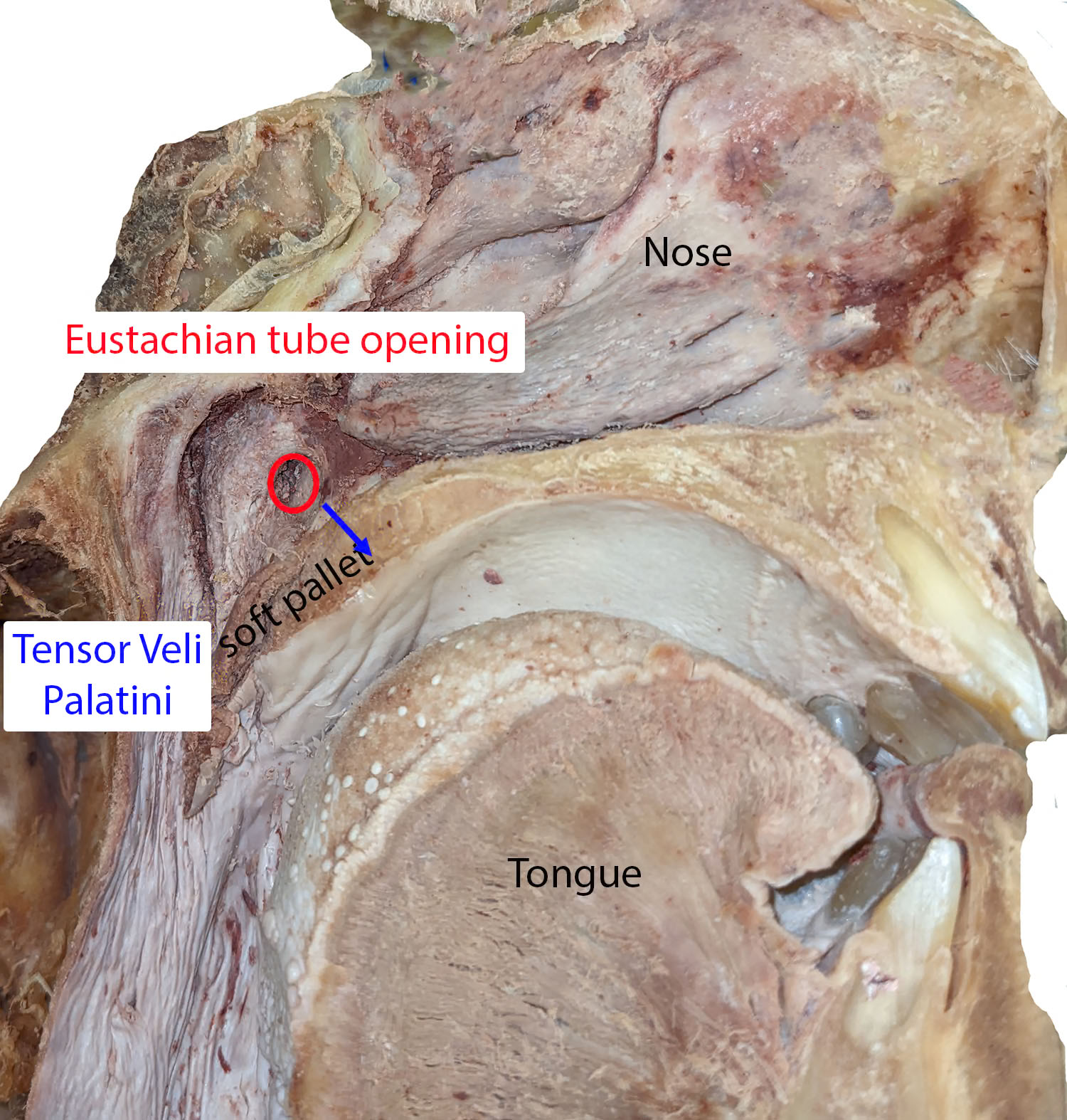
Anatomical Relationships of the Tensor Veli Palatini and Pharyngeal Orifice. This sagittal cadaveric dissection exposes the structural relationships within the nasopharynx and oral cavity. The red circle marks the pharyngeal orifice of the eustachian tube, while the blue arrow indicates its trajectory toward the soft palate. The specimen clearly displays the nose and tongue to provide anatomical context, while delineating the deep muscle fibers of the tensor veli palatini.
Peterson created image for StatPearls article.
(Click Image to Enlarge)
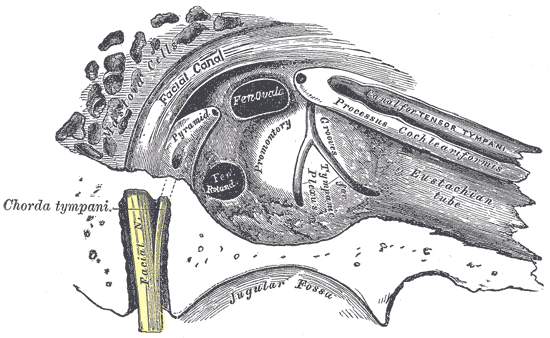
Tympanic Cavity. This image highlights the complex osseous and neural pathways traversing the inner wall of the tympanum. The illustration charts the courses of the facial nerve and its chorda tympani branch relative to central landmarks like the facial canal, pyramid, and promontory. Additional labeled structures index the mastoid cells, fenestra ovale, fenestra rotundum, grooves for the tympanic plexus, processus cochleariformis, canal for the tensor tympani, Eustachian tube, and the adjacent jugular fossa floor.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Alves IS, Martin MDGM. Anatomy and Embryology of the Middle Ear, Labyrinth, and Intracranial Vestibular Pathways. Seminars in ultrasound, CT, and MR. 2024 Oct:45(5):353-359. doi: 10.1053/j.sult.2024.09.002. Epub 2024 Oct 5 [PubMed PMID: 39369828]
Pfaff C, Schultz JA, Schellhorn R. The vertebrate middle and inner ear: A short overview. Journal of morphology. 2019 Aug:280(8):1098-1105. doi: 10.1002/jmor.20880. Epub 2018 Aug 17 [PubMed PMID: 30117612]
Level 3 (low-level) evidenceSundar PS, Chowdhury C, Kamarthi S. Evaluation of Human Ear Anatomy and Functionality by Axiomatic Design. Biomimetics (Basel, Switzerland). 2021 May 19:6(2):. doi: 10.3390/biomimetics6020031. Epub 2021 May 19 [PubMed PMID: 34069537]
Sutton AE, Weimer AD. Tympanic Membrane Perforation. StatPearls. 2026 Jan:(): [PubMed PMID: 32491810]
Job A, Paucod JC, O'Beirne GA, Delon-Martin C. Cortical representation of tympanic membrane movements due to pressure variation: an fMRI study. Human brain mapping. 2011 May:32(5):744-9. doi: 10.1002/hbm.21063. Epub [PubMed PMID: 21484948]
Heine PA. Anatomy of the ear. The Veterinary clinics of North America. Small animal practice. 2004 Mar:34(2):379-95 [PubMed PMID: 15062614]
Level 3 (low-level) evidenceCosset JM, Chabot P, Arriagada R, Socie G, Girinski T, Chavaudra J. Modified bolus technique for the treatment of Kaposi's sarcoma. International journal of radiation oncology, biology, physics. 1988 Aug:15(2):511 [PubMed PMID: 3403331]
Young A, Ng M. Ossiculoplasty. StatPearls. 2026 Jan:(): [PubMed PMID: 33085309]
Oguchi M, Kiyono K, Watanabe T, Sone S, Imai Y, Kawai T, Takei K, Maruyama K, Maruyama Y. [Radiotherapy of nasopharyngeal carcinoma]. Gan no rinsho. Japan journal of cancer clinics. 1987 Oct:33(12):1407-13 [PubMed PMID: 3682192]
Sutton AE, De Jong R, Kwartowitz G. Tensor Tympani Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 30085597]
Trevino M, Zang A, Lobarinas E. The middle ear muscle reflex: Current and future role in assessing noise-induced cochlear damage. The Journal of the Acoustical Society of America. 2023 Jan:153(1):436. doi: 10.1121/10.0016853. Epub [PubMed PMID: 36732247]
Fournier P, Paquette S, Paleressompoulle D, Paolino F, Devèze A, Noreña A. Contraction of the stapedius and tensor tympani muscles explored by tympanometry and pressure measurement in the external auditory canal. Hearing research. 2022 Jul:420():108509. doi: 10.1016/j.heares.2022.108509. Epub 2022 Apr 27 [PubMed PMID: 35568596]
Mukerji S, Windsor AM, Lee DJ. Auditory brainstem circuits that mediate the middle ear muscle reflex. Trends in amplification. 2010 Sep:14(3):170-91. doi: 10.1177/1084713810381771. Epub 2010 Sep 23 [PubMed PMID: 20870664]
Level 3 (low-level) evidenceSzymanski A, Agarwal A. Anatomy, Head and Neck, Ear Eustachian Tube. StatPearls. 2026 Jan:(): [PubMed PMID: 29493963]
Savenko IV, Boboshko MY. [The patulous Eustachian tube syndrome: the current state-of-the-art and an original clinical observation. Second communication]. Vestnik otorinolaringologii. 2018:83(3):77-81. doi: 10.17116/otorino201883377. Epub [PubMed PMID: 29953063]
Tysome JR, Sudhoff H. The Role of the Eustachian Tube in Middle Ear Disease. Advances in oto-rhino-laryngology. 2018:81():146-152. doi: 10.1159/000485581. Epub 2018 Apr 6 [PubMed PMID: 29794454]
Level 3 (low-level) evidenceOkada R, Muro S, Eguchi K, Yagi K, Nasu H, Yamaguchi K, Miwa K, Akita K. The extended bundle of the tensor veli palatini: Anatomic consideration of the dilating mechanism of the Eustachian tube. Auris, nasus, larynx. 2018 Apr:45(2):265-272. doi: 10.1016/j.anl.2017.05.014. Epub 2017 Jun 16 [PubMed PMID: 28625531]
Liu CL, Hsu NI, Shen PH. Endoscopic endonasal nasopharyngectomy: tensor veli palatine muscle as a landmark for the parapharyngeal internal carotid artery. International forum of allergy & rhinology. 2017 Jun:7(6):624-628. doi: 10.1002/alr.21921. Epub 2017 Apr 6 [PubMed PMID: 28383178]
Li Y, Liu H, Li J, Zhang Q, Gong S, He D. Morphology and ciliary motion of mucosa in the Eustachian tube of neonatal and adult gerbils. PloS one. 2014:9(6):e99840. doi: 10.1371/journal.pone.0099840. Epub 2014 Jun 12 [PubMed PMID: 24925141]
Kim HY. Eustachian Tube Dysfunction in Hearing Loss: Mechanistic Pathways to Targeted Interventions. Biomedicines. 2025 Oct 31:13(11):. doi: 10.3390/biomedicines13112686. Epub 2025 Oct 31 [PubMed PMID: 41301779]
Schilder AG, Bhutta MF, Butler CC, Holy C, Levine LH, Kvaerner KJ, Norman G, Pennings RJ, Poe D, Silvola JT, Sudhoff H, Lund VJ. Eustachian tube dysfunction: consensus statement on definition, types, clinical presentation and diagnosis. Clinical otolaryngology : official journal of ENT-UK ; official journal of Netherlands Society for Oto-Rhino-Laryngology & Cervico-Facial Surgery. 2015 Oct:40(5):407-11. doi: 10.1111/coa.12475. Epub [PubMed PMID: 26347263]
Level 3 (low-level) evidenceDoyle WJ. A formal description of middle ear pressure-regulation. Hearing research. 2017 Oct:354():73-85. doi: 10.1016/j.heares.2017.08.005. Epub 2017 Aug 24 [PubMed PMID: 28917121]
Casale J, Shumway KR, Hatcher JD. Physiology, Eustachian Tube Function. StatPearls. 2026 Jan:(): [PubMed PMID: 30335317]
Cantekin EI, Doyle WJ, Reichert TJ, Phillips DC, Bluestone CD. Dilation of the eustachian tube by electrical stimulation of the mandibular nerve. The Annals of otology, rhinology, and laryngology. 1979 Jan-Feb:88(1 Pt 1):40-51 [PubMed PMID: 106759]
Cantekin EI, Phillips DC, Doyle WJ, Bluestone CD, Kimes KK. Effect of surgical alterations of the tensor veli palatini muscle on eustachian tube function. The Annals of otology, rhinology & laryngology. Supplement. 1980 May-Jun:89(3 Pt 2):47-53 [PubMed PMID: 6778348]
Hamrang-Yousefi S, Ng J, Andaloro C. Eustachian Tube Dysfunction. StatPearls. 2026 Jan:(): [PubMed PMID: 32310368]
Toro-Tobon S, Manrique M, Paredes-Gutierrez J, Mantilla-Rivas E, Oh H, Ahmad L, Oh AK, Rogers GF. Pharyngeal Arches, Chapter 1: Normal Development and Derivatives. The Journal of craniofacial surgery. 2023 Oct 1:34(7):2237-2241. doi: 10.1097/SCS.0000000000009374. Epub 2023 Jun 2 [PubMed PMID: 37264513]
Mozaffari M, Jiang D, Tucker AS. Developmental aspects of the tympanic membrane: Shedding light on function and disease. Genesis (New York, N.Y. : 2000). 2020 Mar:58(3-4):e23348. doi: 10.1002/dvg.23348. Epub 2019 Nov 25 [PubMed PMID: 31763764]
Helwany M, Arbor TC, Tadi P. Embryology, Ear. StatPearls. 2026 Jan:(): [PubMed PMID: 32491520]
Anthwal N, Thompson H. The development of the mammalian outer and middle ear. Journal of anatomy. 2016 Feb:228(2):217-32. doi: 10.1111/joa.12344. Epub 2015 Jul 30 [PubMed PMID: 26227955]
Frisdal A, Trainor PA. Development and evolution of the pharyngeal apparatus. Wiley interdisciplinary reviews. Developmental biology. 2014 Nov-Dec:3(6):403-18. doi: 10.1002/wdev.147. Epub 2014 Aug 29 [PubMed PMID: 25176500]
Level 3 (low-level) evidencePrasad KC, Azeem Mohiyuddin SM, Anjali PK, Harshita TR, Indu Varsha G, Brindha HS. Microsurgical Anatomy of Stapedius Muscle: Anatomy Revisited, Redefined with Potential Impact in Surgeries. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India. 2019 Mar:71(1):14-18. doi: 10.1007/s12070-018-1510-5. Epub 2018 Oct 9 [PubMed PMID: 30906706]
Finkelstein Y, Talmi YP, Nachmani A, Hauben DJ, Zohar Y. Levator veli palatini muscle and eustachian tube function. Plastic and reconstructive surgery. 1990 May:85(5):684-92; discussion 693-7 [PubMed PMID: 2326351]
Adams A, Mankad K, Offiah C, Childs L. Branchial cleft anomalies: a pictorial review of embryological development and spectrum of imaging findings. Insights into imaging. 2016 Feb:7(1):69-76. doi: 10.1007/s13244-015-0454-5. Epub 2015 Dec 10 [PubMed PMID: 26661849]
Heyd C, Yellon R. Anatomy, Head and Neck, Pharynx Muscles(Archived). StatPearls. 2026 Jan:(): [PubMed PMID: 30969574]
Pairaudeau C, Mendonca C. Anaesthesia for major middle ear surgery. BJA education. 2019 May:19(5):136-143. doi: 10.1016/j.bjae.2019.01.006. Epub 2019 Mar 6 [PubMed PMID: 33456882]
Susai S, Motwani R, Chandrupatla M. Tracking Lymphatic Drainage Pathways Through Inner Ear Channels: A Systematic Review. Cureus. 2024 Aug:16(8):e66670. doi: 10.7759/cureus.66670. Epub 2024 Aug 12 [PubMed PMID: 39262517]
Level 1 (high-level) evidenceHAMBERGER CA, WERSAELL J. VASCULAR SUPPLY OF THE TYMPANIC MEMBRANE AND THE OSSICULAR CHAIN. Acta oto-laryngologica. Supplementum. 1964:188():SUPPL 188:308+ [PubMed PMID: 14146691]
Widemar L, Hellström S, Schultzberg M, Stenfors LE. Autonomic innervation of the tympanic membrane. An immunocytochemical and histofluorescence study. Acta oto-laryngologica. 1985 Jul-Aug:100(1-2):58-65 [PubMed PMID: 2411101]
Level 3 (low-level) evidenceNaraev BG, Linthicum FH Jr. Traumatic neuroma of the tympanic (Jacobson's) nerve as a possible cause of otalgia. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2008 Jun:138(6):735-7. doi: 10.1016/j.otohns.2008.02.008. Epub [PubMed PMID: 18503845]
Falcon RT, Rivera-Serrano CM, Miranda JF, Prevedello DM, Snyderman CH, Kassam AB, Carrau RL. Endoscopic endonasal dissection of the infratemporal fossa: Anatomic relationships and importance of eustachian tube in the endoscopic skull base surgery. The Laryngoscope. 2011 Jan:121(1):31-41. doi: 10.1002/lary.21341. Epub [PubMed PMID: 21181982]
Ugarteburu M, Withnell RH, Cardoso L, Carriero A, Richter CP. Mammalian middle ear mechanics: A review. Frontiers in bioengineering and biotechnology. 2022:10():983510. doi: 10.3389/fbioe.2022.983510. Epub 2022 Oct 10 [PubMed PMID: 36299283]
Teixeira MS. Understanding Eustachian tube function. Brazilian journal of otorhinolaryngology. 2020 Sep-Oct:86(5):523-524. doi: 10.1016/j.bjorl.2020.02.001. Epub 2020 Feb 28 [PubMed PMID: 32209307]
Level 3 (low-level) evidenceGuan X. A mechanical lumped-element model of the human middle ear for bone conduction hearing. Scientific reports. 2025 Jul 28:15(1):27434. doi: 10.1038/s41598-025-09614-7. Epub 2025 Jul 28 [PubMed PMID: 40721420]
Gottlieb PK, Vaisbuch Y, Puria S. Human ossicular-joint flexibility transforms the peak amplitude and width of impulsive acoustic stimuli. The Journal of the Acoustical Society of America. 2018 Jun:143(6):3418. doi: 10.1121/1.5039845. Epub [PubMed PMID: 29960477]
Park H, Hong SN, Kim HS, Han JJ, Chung J, Suh MW, Oh SH, Chang SO, Lee JH. Determinants of conductive hearing loss in tympanic membrane perforation. Clinical and experimental otorhinolaryngology. 2015 Jun:8(2):92-6. doi: 10.3342/ceo.2015.8.2.92. Epub 2015 May 13 [PubMed PMID: 26045905]
Nagar RR, Deshmukh PT. An Overview of the Tympanostomy Tube. Cureus. 2022 Oct:14(10):e30166. doi: 10.7759/cureus.30166. Epub 2022 Oct 11 [PubMed PMID: 36397911]
Level 3 (low-level) evidenceTeixeira-Marques F, Osório RV, Teixeira M, Rebelo J, Gerós S, Helena D, Almeida AF, Oliveira P. Stapedotomy or Stapedectomy: Does It Really Matter? International archives of otorhinolaryngology. 2025 Jan:29(1):1-5. doi: 10.1055/s-0044-1792086. Epub 2025 Jan 10 [PubMed PMID: 39801896]
Cheng HCS, Agrawal SK, Parnes LS. Stapedectomy Versus Stapedotomy. Otolaryngologic clinics of North America. 2018 Apr:51(2):375-392. doi: 10.1016/j.otc.2017.11.008. Epub 2018 Feb 3 [PubMed PMID: 29397948]
Ellsperman SE, Nairn EM, Stucken EZ. Review of Bone Conduction Hearing Devices. Audiology research. 2021 May 18:11(2):207-219. doi: 10.3390/audiolres11020019. Epub 2021 May 18 [PubMed PMID: 34069846]
Rohani SA, Bartling ML, Ladak HM, Agrawal SK. The BONEBRIDGE active transcutaneous bone conduction implant: effects of location, lifts and screws on sound transmission. Journal of otolaryngology - head & neck surgery = Le Journal d'oto-rhino-laryngologie et de chirurgie cervico-faciale. 2020 Aug 10:49(1):58. doi: 10.1186/s40463-020-00454-1. Epub 2020 Aug 10 [PubMed PMID: 32778163]
Gołota K, Czerwaty K, Dżaman K, Szczepański D, Ludwig N, Szczepański MJ. Balloon Eustachian Tuboplasty: A Systematic Review of Technique, Safety, and Clinical Outcomes in Chronic Obstructive Eustachian Tube Dysfunction. Healthcare (Basel, Switzerland). 2025 Jul 27:13(15):. doi: 10.3390/healthcare13151832. Epub 2025 Jul 27 [PubMed PMID: 40805865]
Level 1 (high-level) evidence