Introduction
Esthesioneuroblastoma, or olfactory neuroblastoma, is a rare malignant neoplasm of the sinonasal tract that typically arises in the superior nasal cavity and shows olfactory neuroepithelial or neuroblastic differentiation. Since its initial description in 1924 by Luc Berger, more than 1000 cases of esthesioneuroblastoma have been reported in the literature.[1] This condition most often presents with nasal obstruction, epistaxis, headaches, or hyposmia/anosmia, and these common, vague symptoms often lead to more advanced stages at initial presentation.[2] Esthesioneuroblastoma is a locally aggressive neoplasm and metastasizes by both hematogenous and lymphatic routes. The tumor affects both men and women, children and adults, and there are no known geographic or environmental risk factors. Esthesioneuroblastoma and other rare neoplastic lesions should be considered in the differential diagnosis of persistent, unilateral, recurrent, or unexplained sinonasal symptoms.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The exact etiology of esthesioneuroblastoma is still unknown, and no definitive predisposing factors have been identified. The cell of origin remains uncertain. Proposed sources have included the olfactory neuroepithelium, ectodermal olfactory placode, the Jacobson vomeronasal organ, the Loci ganglion, the sphenopalatine ganglion, and the autonomic ganglia within the nasal mucosa; however, available evidence most strongly supports origin from malignant transformation of basal progenitor cells of the olfactory epithelium (malignant globular basal cells).[3][4][5]
Genetic mutations involving tumor protein p53 (TP53), fibroblast growth factor receptor kinase (FRK), notch receptor 3 (NOTCH3), SMARCA4 (SWI/SNF protein family, matrix-associated, actin-dependent regulator of chromatin, subfamily A, member 4), rearranged during transfection (RET), and CTCF (CCCTC-binding factor) have been identified in esthesioneuroblastomas.[6]
Epidemiology
Esthesioneuroblastoma accounts for 2% to 6% of nasal cavity and paranasal sinus cancer cases and 0.3% of all upper aerodigestive tract malignancies, and has an estimated incidence of 0.4 cases per 1 million people.[7] The reported incidence of esthesioneuroblastoma appears to have increased, possibly reflecting improved recognition and reporting. Esthesioneuroblastoma may occur at any age, although most patients present in adulthood. The age distribution has been described as bimodal, with peaks in the 20s and 60s.[8] Men and women are affected equally.[9] In children, it represents the most frequent malignancy of the nasal cavity.
Pathophysiology
Esthesioneuroblastoma is thought to arise from, or show differentiation toward, olfactory neuroepithelium. These cells are normally present in the superior nasal cavity, including the superior nasal septum, superior turbinate, nasal roof, and cribriform plate region of the ethmoid bone.
Molecular and Genetic Profile
Esthesioneuroblastoma exhibits numerous chromosomal copy-number gains and losses, but no consistent recurrent pattern has been established.[10][11] In 1 study, a deletion on chromosome 11 and a gain on chromosome 1p correlated with metastasis and a worse prognosis.[12] Gains are more frequent than losses, and high-stage esthesioneuroblastomas show more alterations than low-stage tumors. Gains in 20q and 13q may be significant in the progression of this neoplasm; these regions may harbor genes with functional relevance in esthesioneuroblastoma. The detection of PTCH1, GL1, and GL2 in 70%, 70%, and 65% of human esthesioneuroblastoma specimens, respectively, suggests that the sonic hedgehog (SHH) signaling pathway may be involved in the pathogenesis of this neoplasm.[13] Recent research has found expression of the OMP and RIC8B genes in esthesioneuroblastomas.[14]
More recent molecular studies suggest that esthesioneuroblastoma is biologically heterogeneous. DNA methylation and multiomic analyses have identified molecular subgroups and have also helped distinguish true olfactory neuroblastoma from mimics such as IDH2-mutant sinonasal carcinoma, SMARCB1-deficient sinonasal carcinoma, and other poorly differentiated sinonasal tumors.[14] At present, these molecular findings are most useful diagnostically and investigationally, and they have not yet replaced histology, immunohistochemistry, Hyams grading, and clinical staging in routine management.
Histopathology
Macroscopic Examination
Esthesioneuroblastomas are usually unilateral, polypoid, glistening, soft, reddish-grey masses with an intact mucosa; the cut surface appears greyish-tan to pinkish-red and hypervascular. The tumors range from under 1 cm in size to large masses involving the nasal cavity and intracranial region. They frequently expand into the adjacent paranasal sinuses, orbit, and anterior cranial fossa.[15]
Macroscopic Examination
Low-grade esthesioneuroblastomas form submucosal, sharply demarcated nests, lobules, or sheets of cells, often separated by richly vascular or hyalinized fibrous stroma. Homer Wright pseudorosettes, with neoplastic cells arranged around a central, delicate fibrillary neural matrix or neuropil, may be seen. The tumor cells are often uniform, with sparse cytoplasm and round or ovoid nuclei with punctate salt-and-pepper chromatin and nucleoli that are either small or absent. Esthesioneuroblastoma characteristically demonstrates a fibrillary background composed of interdigitating neuronal processes, or neuropil. Higher-grade tumors show tumor necrosis, pleomorphism, increased mitotic activity, decreased or absent neuropil, and a less conspicuous lobular growth pattern. The tumor cells can arrange in gland-like rings or tight annular formations with a true lumen (Flexner-Wintersteiner rosettes). Rosettes alone are not diagnostic of esthesioneuroblastoma, although Homer Wright rosettes are nearly pathognomonic in the nasal cavity when accompanied by true neuropil. The mitotic rate is variable, but is usually low, especially in lower-grade tumors. Calcifications (concretion-like or psammomatous) may be seen, less frequently as the grade increases. Melanin pigment, ganglion cells, rhabdomyoblasts, divergent differentiation as islands of true epithelium (squamous pearls or gland formation), and clear-cell change may occasionally be present in esthesioneuroblastoma.[15]
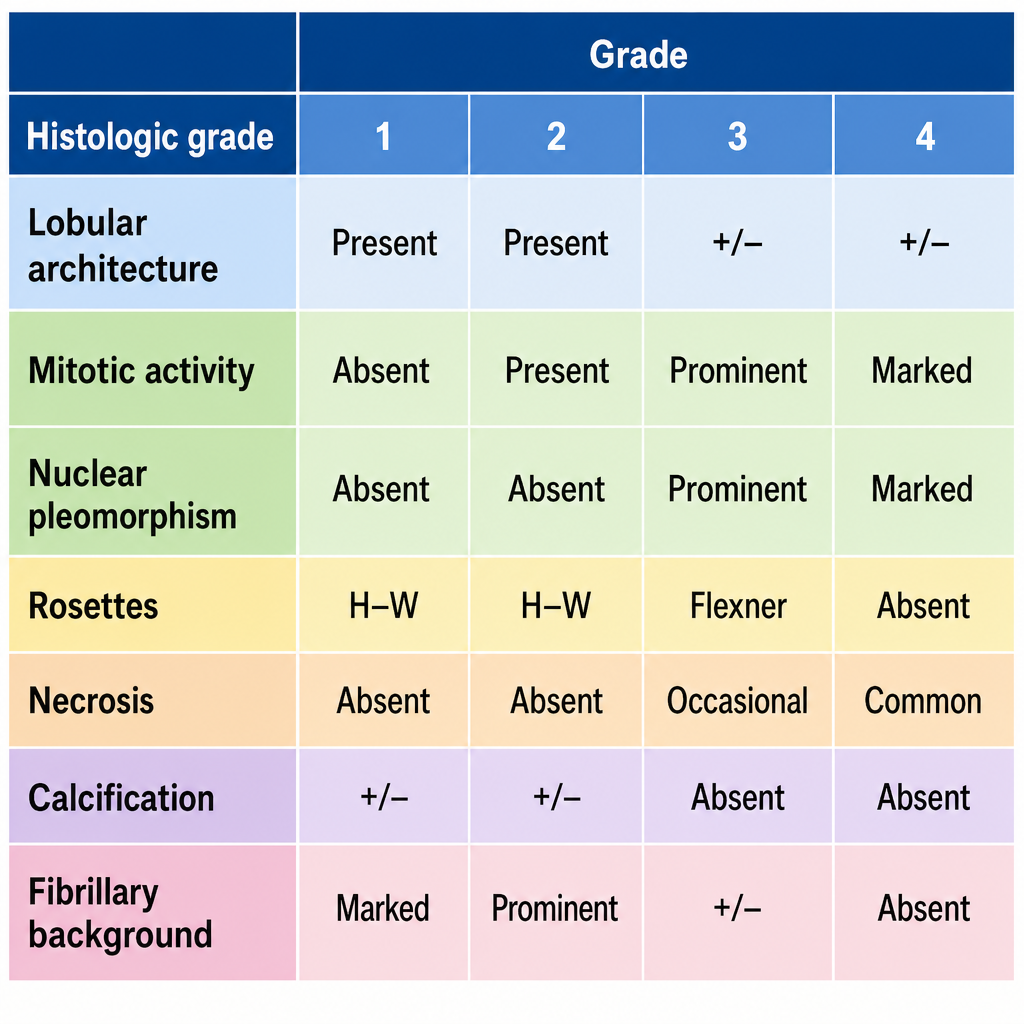
Histopathologic characteristics of esthesioneuroblastoma have been compiled into the Hyams grading system, which correlates with prognosis (see Image. Hyams Grading System for Esthesioneuroblastoma).[16]
Immunohistochemical Profile
The typical immunohistochemical profile includes diffuse staining for neuron-specific enolase, synaptophysin, chromogranin A, CD56 (NCAM), and beta-III tubulin, as well as variable S100 protein reactivity, typically in a sustentacular pattern highlighting cells at the periphery of tumor nests; this pattern may be reduced or absent in higher-grade tumors.[17] INSM1 may also support neuroendocrine differentiation. SSTR2 expression has been described in esthesioneuroblastoma and may have diagnostic, imaging, and therapeutic implications in selected cases. Sustentacular cells may also be GFAP-positive. Calretinin staining (nuclear and cytoplasmic) has been reported in esthesioneuroblastoma but can also be seen in other sinonasal tumors.[18] As many as one-third of esthesioneuroblastomas may also stain focally for cytokeratin (CAM5.2, CK18). Negative markers include CD45RB, CD99, p63, and FLI1. Proliferation marker studies reveal a variable Ki-67 proliferation index (2%-50%), and BCL2 expression increases with tumor grade.[19][20]
History and Physical
Clinically, esthesioneuroblastoma often has a subtle presentation mimicking benign inflammatory or infectious sinonasal disease, and a delay in diagnosis is not uncommon. Nasal obstruction and epistaxis are typical early manifestations; however, other, more specific symptoms may occur depending on the tumor's location and extent.[21] Anosmia can precede the diagnosis of esthesioneuroblastoma by several years.[22] Other symptoms may relate to extension into the paranasal sinuses (facial swelling, medial canthus mass), the orbit (orbital pain, proptosis, epiphora, or visual disturbance), the anterior cranial fossa (headache), or, rarely, to inappropriate antidiuretic hormone secretion.
Initial history should focus on nasal breathing and olfactory symptoms, including the frequency, side, and nature of any rhinorrhea or epistaxis. Clear, positional rhinorrhea is more concerning for an occult cerebrospinal fluid (CSF) leak, whereas recurrent unilateral epistaxis is concerning for neoplasia. Seasonal, alternating, or environmental clear rhinorrhoea or nasal obstruction are more consistent with benign allergic rhinitis. A neurologic history should be obtained, including headache history, visual symptoms, facial pain or weakness, as well as a social and occupational history that could elucidate risk factors for other sinonasal tumors, including tobacco smoking and occupational exposure to wood dust, heavy metals, or aromatic amines.
The physical examination should begin with a head and neck exam, with particular attention to anterior rhinoscopy and a detailed cranial nerve examination. Nasal endoscopy and otoscopy should be performed, as the tumor may obstruct the Eustachian tube. A neck examination should assess for lymphadenopathy that could indicate metastasis.
Evaluation
A thorough physical examination and nasal endoscopic evaluation are essential initially and should be complemented by contrast-enhanced computed tomography (CT) and magnetic resonance imaging (MRI).
CT Scan
Radiographic assessment of esthesioneuroblastoma typically begins with an IV contrast-enhanced computed tomography (CT) scan. Sinus involvement and bony erosion are well depicted on CT, which contributes to initial staging and surgical planning (Figure 2).[15][23][15]
MRI
Esthesioneuroblastoma is typically hypo- to isointense relative to brain gray matter on T1-weighted MRI and usually enhances after gadolinium administration. T2-weighted images show an isointense or hyperintense mass. MRI provides better discrimination between tumor and retained sinus secretions and is superior for evaluating orbital, dural, intracranial, and brain parenchymal involvement.[15] When intracranial extension is present, cysts at the brain-tumor interface may be seen, although this finding is not universal. A dumbbell-shaped transcibrosphenoidal extension is a characteristic imaging feature, but it is not pathognomonic (see Image. Esthesioneuroblastoma).
Nuclear Medicine Imaging
Most of these tumors are metaiodobenzylguanidine (MIBG)-avid, a feature that can help differentiate them from anterior cranial fossa meningiomas.[24] In routine practice, this is rarely required. Fluorodeoxyglucose positron emission tomography (FDG PET)-CT may be useful after histologic diagnosis to evaluate regional or distant metastasis and to assess suspected recurrence. However, esthesioneuroblastoma may show relatively lower FDG avidity than other aggressive sinonasal malignancies. Because many esthesioneuroblastomas express somatostatin receptors, somatostatin receptor imaging with gallium-68 DOTATATE PET-CT or PET-MRI is an emerging adjunct in selected cases, particularly for recurrent, metastatic, or treatment-planning scenarios.[25]
Tumor Biopsy
Endoscopic transnasal biopsy of the sinonasal mass is usually performed to confirm the histologic diagnosis. Biopsy should be performed after imaging studies have been reviewed to assess tumor vascularity, skull base involvement, and the possibility of alternative diagnoses such as vascular lesions or encephalocele.[15]
Treatment / Management
Three modalities are used for the treatment of esthesioneuroblastoma: surgery, external beam radiation, and chemotherapy. Often, the treatment utilizes a combination of these modalities, depending on tumor stage, grade, extent, and resectability.[15][26] (B2)
Surgical resection is advocated as the primary modality whenever possible.[15] This can involve 1 of 2 modalities, depending on the extent of the tumor: Endoscopic resection (usually through an endonasal approach) or open resection (via transfacial, transcranial, or combined craniofacial approaches, often in conjunction with a neurosurgeon).[15][27] Regardless of the resection modality, any resultant skull base defect must then be reconstructed. This can be accomplished with free grafts, such as fascia, bone, or cartilage, or vascularized flaps, such as a pericranial flap or nasoseptal flap.[28][29] The goal is to create a watertight seal to prevent CSF leakage, restore skull base continuity, support intracranial contents, and allow for subsequent radiation therapy.(B2)
Endoscopic craniofacial resection may be used for selected tumors involving the anterior skull base. The approach is tailored to the extent of the tumor and may include removal of the involved cribriform plate, fovea ethmoidalis, anterior skull base bone, and involved dura when required for complete oncologic resection. For tumors involving the frontal sinus or requiring wide access to the rostral anterior skull base, a Draf type III, or modified endoscopic Lothrop, frontal sinusotomy may be performed to create a common frontal sinus cavity and improve surgical exposure. Multilayer skull base reconstruction, often using fascia, fat, graft material, vascularized flaps, and sealant, is used to reduce the risk of postoperative CSF leak.
Orbital involvement should be assessed carefully during treatment planning. Limited periorbital or lacrimal sac involvement may be managed with orbit-preserving surgery and adjuvant therapy in selected patients, whereas extensive intraorbital involvement may require more aggressive treatment.
Many patients who undergo surgery for esthesioneuroblastoma benefit from postoperative radiation therapy, particularly those with higher-stage, higher-grade, margin-positive, or locally advanced disease. Combined surgical resection and postoperative radiation therapy is commonly regarded as the preferred approach for many patients and has been associated with improved local control and survival in retrospective series.[30] Radiation therapy can be delivered via external beam, often using intensity-modulated radiation therapy (IMRT), and proton therapy has become more widely available in recent years as well.[31][32] The advantages of IMRT and proton therapy include precise delivery of radiation to the tumor volume while sparing radiosensitive surrounding structures such as the eyes, optic apparatus, and brain.
Preoperative (neoadjuvant) radiation therapy is an alternative strategy that may yield comparable results in selected patients, particularly those with early-stage Kadish A or B tumors. However, some centers avoid it because it may complicate postoperative tumor-bed mapping (see Image. Kadish Staging for Esthesioneuroblastoma).[15][33][15]
Neoadjuvant chemotherapy may be employed for advanced-stage Kadish C or D tumors or tumors involving structures that cannot be safely resected, such as the optic chiasm or extensive brain parenchymal involvement. Preoperative chemotherapy may be used to reduce tumor volume and facilitate surgical resection while preserving critical structures, followed by surgery and adjuvant radiation therapy when feasible.[34][15][35] Chemotherapy is typically platinum-based, commonly using cisplatin or carboplatin in combination with agents such as etoposide; other agents, including vincristine, doxorubicin, ifosfamide, and cyclophosphamide, have also been used.[36][37][38](B2)
The neck should be evaluated at initial presentation with clinical examination and imaging. Patients with clinically or radiologically evident cervical nodal disease are generally treated with neck dissection, radiation therapy, or both. In clinically node-negative patients, elective neck irradiation or elective neck dissection may be considered for higher-risk tumors, particularly Kadish C or D tumors, high Hyams grade tumors, or tumors with other adverse features; however, the benefit must be balanced against treatment-related morbidity.
Patients with recurrent or widely metastatic disease are candidates for palliative therapy. Depending on disease location, symptom burden, and prior treatment, palliation may include radiation therapy or chemotherapy, with chemotherapy most commonly used.[39][40][36](B3)
Long-term surveillance is required after definitive treatment because esthesioneuroblastoma may recur locally, regionally, or distantly many years after initial therapy. Follow-up generally includes regular nasal endoscopy, clinical examination of the neck, and interval MRI of the sinonasal tract and anterior skull base. Chest imaging or PET-CT may be considered when clinically indicated or in higher-risk disease. Surveillance should be extended beyond the first 5 years.
Differential Diagnosis
Differential diagnoses, particularly other sinonasal small round blue cell tumors and poorly differentiated malignancies, include:
- Extramedullary plasmacytoma
- Extraosseous Ewing sarcoma/Ewing sarcoma family tumor/primitive neuroectodermal tumor (PNET)
- Mesenchymal chondrosarcoma
- Extranodal NK/T-cell lymphoma, nasal type
- Rhabdomyosarcoma
- Sinonasal malignant melanoma
- Sinonasal neuroendocrine carcinoma, including small cell neuroendocrine carcinoma
- Sinonasal undifferentiated carcinoma
- NUT carcinoma
- SMARCB1-deficient sinonasal carcinoma
- SMARCA4-deficient sinonasal carcinoma
- Small cell osteosarcoma
- Synovial sarcoma
- Lymphoepithelial carcinoma [15]
Staging
Hyams et al developed the most widely used grading system for esthesioneuroblastoma (see Image. Hyams Grading System for Esthesioneuroblastoma).[21] This Hyams grading system divides the spectrum of esthesioneuroblastoma maturation into 4 grades, ranging from most differentiated (grade I) to least differentiated (grade IV), based on tumor architecture, mitotic activity, nuclear pleomorphism, fibrillary matrix and rosettes, necrosis, glandular differentiation, and calcifications. This grading scheme has been independently validated as prognostically significant.[21][41]
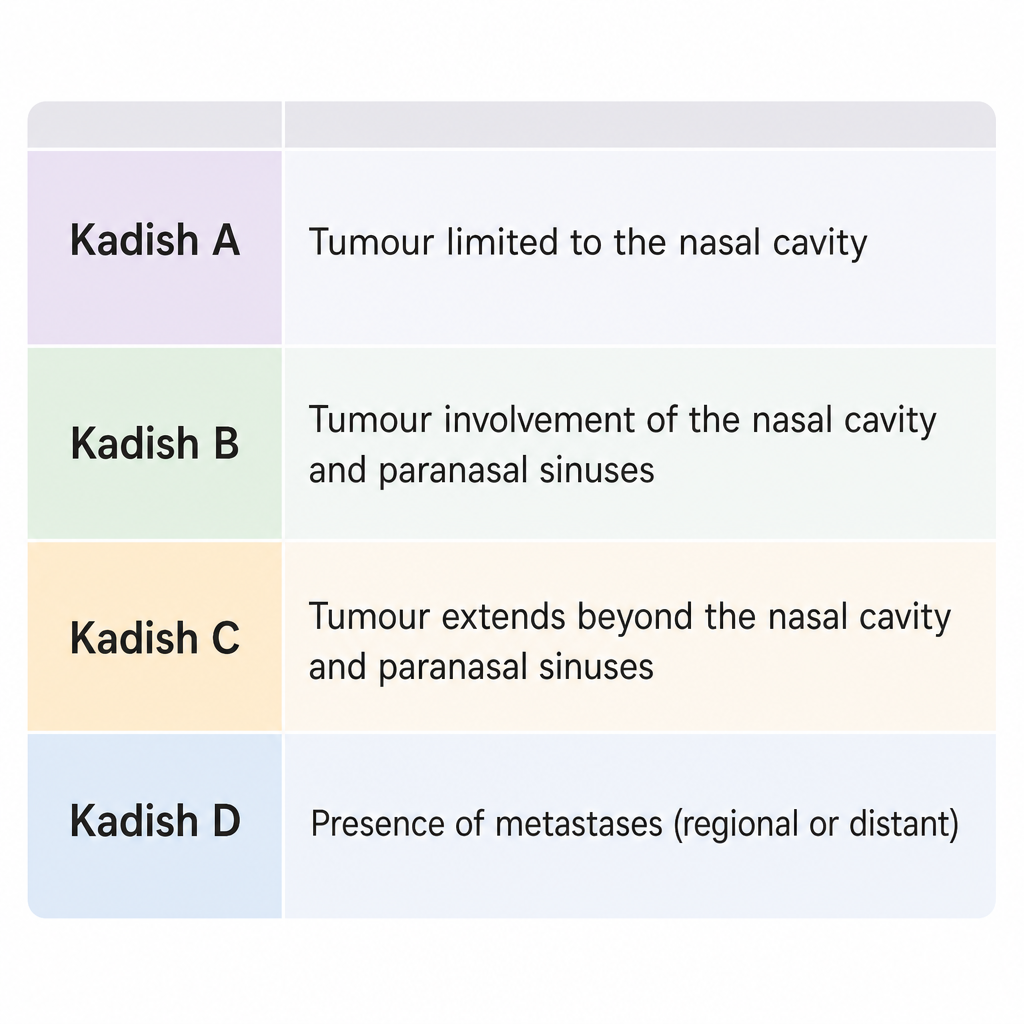
The Kadish staging system is an effective means of predicting disease-free survival and is widely accepted (see Image. Kadish Staging for Esthesioneuroblastoma). This system includes the following groups:
- Group A tumors: limited to the nasal cavity
- Group B tumors: involve the nasal cavity and one or more paranasal sinuses
- Group C tumors: extend beyond the nasal cavity and sinuses, including extension to the orbit, skull base, or intracranial compartment
A modified Kadish system includes group D tumors, defined by cervical nodal or distant metastasis.
Dulguerov proposed a TNM-style staging system that incorporates local tumor extent, nodal disease, and distant metastasis. This system was later reported to correlate closely with survival and recurrence.[4][42]
Prognosis
The prognosis of esthesioneuroblastoma is stage- and grade-dependent. The 5-year survival of stage A tumors is 75% to 90%, whereas stage C has a 45% survival. Similarly, high-grade tumors have been associated with approximately 25% 5-year survival, whereas low-grade tumors have been associated with approximately 80% 5-year survival.[15]
There are several poor prognostic indicators of esthesioneuroblastoma.[15] They include the following:
- Cervical nodal or distant metastasis
- Advanced Kadish or Dulguerov stage
- High-grade tumor
- Age above 50 or below 20 at presentation
- Intracranial spread
- Positive or close surgical margins
- High Ki-67 proliferation index
- Aneuploidy or other adverse cytogenetic features
- Angiopoietin-like 4 (ANGPTL4) expression [43]
Comparative analyses of staging and grading systems have shown variable prognostic performance. In 1 systematic review, predictive accuracy for overall survival was highest for the Kadish system, followed by the Hyams grading system and TNM-based staging.[44]
Complications
Complications of esthesioneuroblastoma may result from local tumor invasion, treatment, or recurrence. Tumor-related complications include anosmia, epistaxis, orbital invasion with proptosis or visual impairment, skull base erosion, intracranial extension, cranial neuropathy, cervical nodal metastasis, distant metastasis, and, rarely, paraneoplastic syndromes such as inappropriate antidiuretic hormone secretion. Treatment-related complications include CSF leak, meningitis, sinonasal crusting, anosmia, epiphora, visual injury, wound complications, osteoradionecrosis, radiation-induced optic neuropathy, hypopituitarism, neurocognitive effects, xerostomia, and chemotherapy-related toxicities.
Recurrence of esthesioneuroblastoma is common, with reported recurrence rates of approximately 30% to 60%, and may occur many years after initial treatment. Metastasis develops in 35% of cases. The cervical lymph nodes are the most common site of regional spread. Distant metastasis occurs in approximately 10% of patients, most commonly involving bone, lung, liver, or skin.[1]
Consultations
The following consultations may need to be obtained:
- Otolaryngologist with expertise in endoscopic skull base surgery
- Neurosurgeon with expertise in skull base surgery
- Radiation oncologist
- Medical oncologist
- Pathologist with expertise in head and neck pathology
- Neuroradiologist or head and neck radiologist
- Ophthalmologist, when orbital involvement is suspected
- Endocrinologist when the syndrome of inappropriate antidiuretic hormone secretion is present
Deterrence and Patient Education
Patients and families should be educated about symptoms that warrant medical evaluation, particularly persistent unilateral nasal obstruction, recurrent epistaxis, hyposmia or anosmia, facial swelling, visual symptoms, or a neck mass. Health education that promotes prompt medical evaluation and early detection may improve outcomes.
Enhancing Healthcare Team Outcomes
Optimal management of esthesioneuroblastoma requires a coordinated, multidisciplinary approach because of the tumor's rarity, proximity to critical neurovascular structures, and potential for local invasion and recurrence. Otolaryngologists, neurosurgeons, medical and radiation oncologists, radiologists, pathologists, advanced practitioners, nurses, pharmacists, and rehabilitation specialists each play essential roles in patient care. Accurate diagnosis depends on careful clinical evaluation, high-quality computed tomography (CT) and magnetic resonance imaging (MRI), endoscopic biopsy, histopathologic grading, and appropriate staging. Collaborative treatment planning is critical to determine the optimal combination of surgery, radiation therapy, and systemic therapy while minimizing treatment-related morbidity and preserving neurologic function and quality of life.
Effective interprofessional communication throughout diagnosis, treatment, and long-term surveillance enhances patient safety and clinical outcomes. Nurses coordinate perioperative care, monitor treatment-related toxicities, provide patient education, and facilitate follow-up. Pharmacists optimize supportive medications, chemotherapy regimens when indicated, and adverse effect monitoring. Radiologists and pathologists provide essential diagnostic information that guides treatment planning. At the same time, rehabilitation specialists, ophthalmologists, and endocrinologists may assist in managing functional deficits resulting from skull base surgery or radiation therapy. Coordinated communication among team members promotes timely intervention, reduces complications, supports shared decision-making, and improves long-term disease control and patient-centered outcomes.
Media
(Click Image to Enlarge)
Hyams Grading System for Esthesioneuroblastoma.
Image generated with assistance from Microsoft Copilot and reviewed for medical accuracy.
Adapted from Gallagher KK, Spector ME, Pepper JP, McKean EL, Marentette LJ, McHugh JB. Esthesioneuroblastoma: updating histologic grading as it relates to prognosis. Ann Otol Rhinol Laryngol. 2014;123(5):353-8358. doi: 10.1177/0003489414526368.
(Click Image to Enlarge)
Kadish Staging for Esthesioneuroblastoma.
Image generated with assistance from Microsoft Copilot and reviewed for medical accuracy.
Adapted from Morita A, Ebersold MJ, Olsen KD, Foote RL, Lewis JE, Quast LM. Esthesioneuroblastoma: prognosis and management. Neurosurgery. 1993;32:706-714. doi: 10.1227/00006123-199305000-00002.
(Click Image to Enlarge)
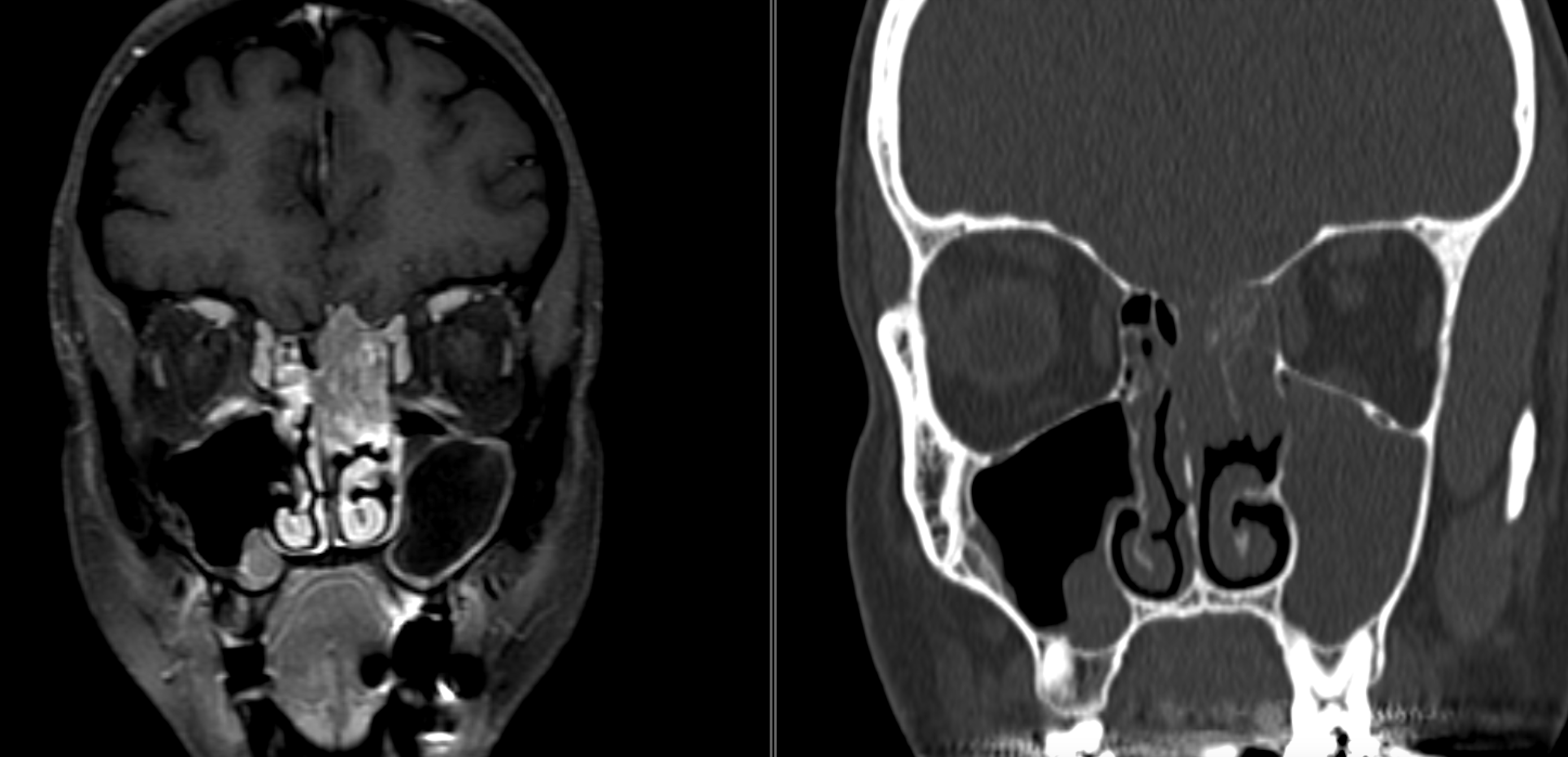
Esthesioneuroblastoma. Magnetic resonance imaging of esthesioneuroblastoma.
Contributed by S Lange, MD
References
Arnold PM, Habib A, Newell K, Anderson KK. Esthesioneuroblastoma metastatic to the thoracic intradural and extradural space. The spine journal : official journal of the North American Spine Society. 2009 May:9(5):e1-5. doi: 10.1016/j.spinee.2008.08.010. Epub 2008 Sep 19 [PubMed PMID: 18805062]
Level 3 (low-level) evidenceSampath P, Park MC, Huang D, Deville C, Cortez S, Chougule P. Esthesioneuroblastoma (olfactory neuroblastoma) with hemorrhage: an unusual presentation. Skull base : official journal of North American Skull Base Society ... [et al.]. 2006 Aug:16(3):169-73 [PubMed PMID: 17268590]
Rao KR, Upadhya IB. A Review on Esthesioneuroblastoma. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India. 2022 Oct:74(Suppl 2):1584-1590. doi: 10.1007/s12070-021-02726-2. Epub 2021 Jul 9 [PubMed PMID: 36452592]
Dulguerov P, Allal AS, Calcaterra TC. Esthesioneuroblastoma: a meta-analysis and review. The Lancet. Oncology. 2001 Nov:2(11):683-90 [PubMed PMID: 11902539]
Level 1 (high-level) evidenceZunitch MJ, Fisch AS, Lin B, Barrios-Camacho CM, Faquin WC, Tachie-Baffour Y, Louie JD, Jang W, Curry WT, Gray ST, Lin DT, Schwob JE, Holbrook EH. Molecular Evidence for Olfactory Neuroblastoma as a Tumor of Malignant Globose Basal Cells. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc. 2023 May:36(5):100122. doi: 10.1016/j.modpat.2023.100122. Epub 2023 Feb 2 [PubMed PMID: 36841178]
Hsia B, Dongre R, Erquizi A, Guerra-Navarro PV, Bitar G, Alshaka SA, Kim JD, Valencia-Sanchez BA, Brandel MG, Sato M, Crawford JR, Levy ML, Patel VA, Polster SP. Molecular Profiling of Olfactory Neuroblastoma Using the AACR Project GENIE Database. Journal of neurological surgery. Part B, Skull base. 2026 Jun:87(3):330-336. doi: 10.1055/a-2639-5690. Epub 2025 Jun 27 [PubMed PMID: 42095028]
Svane-Knudsen V, Jørgensen KE, Hansen O, Lindgren A, Marker P. Cancer of the nasal cavity and paranasal sinuses: a series of 115 patients. Rhinology. 1998 Mar:36(1):12-4 [PubMed PMID: 9569435]
Gandhoke CS, Dewan A, Gupta D, Syal SK, Jagetia A, Saran RK, Meher R, Srivastava AK, Singh D. A rare case report of mixed olfactory neuroblastoma: Carcinoma with review of literature. Surgical neurology international. 2017:8():83. doi: 10.4103/sni.sni_30_17. Epub 2017 May 26 [PubMed PMID: 28607817]
Level 3 (low-level) evidenceLiermann J, Syed M, Held T, Bernhardt D, Plinkert P, Jungk C, Unterberg A, Rieken S, Debus J, Herfarth K, Adeberg S. Advanced Radiation Techniques in the Treatment of Esthesioneuroblastoma: A 7-Year Single-Institution's Clinical Experience. Cancers. 2018 Nov 20:10(11):. doi: 10.3390/cancers10110457. Epub 2018 Nov 20 [PubMed PMID: 30463343]
Holland H, Koschny R, Krupp W, Meixensberger J, Bauer M, Kirsten H, Ahnert P. Comprehensive cytogenetic characterization of an esthesioneuroblastoma. Cancer genetics and cytogenetics. 2007 Mar:173(2):89-96 [PubMed PMID: 17321323]
Level 3 (low-level) evidenceRiazimand SH, Brieger J, Jacob R, Welkoborsky HJ, Mann WJ. Analysis of cytogenetic aberrations in esthesioneuroblastomas by comparative genomic hybridization. Cancer genetics and cytogenetics. 2002 Jul 1:136(1):53-7 [PubMed PMID: 12165452]
Level 2 (mid-level) evidenceBockmühl U, You X, Pacyna-Gengelbach M, Arps H, Draf W, Petersen I. CGH pattern of esthesioneuroblastoma and their metastases. Brain pathology (Zurich, Switzerland). 2004 Apr:14(2):158-63 [PubMed PMID: 15193028]
Mao L, Xia YP, Zhou YN, Dai RL, Yang X, Wang YJ, Duan SJ, Qiao X, Mei YW, Hu B. Activation of sonic hedgehog signaling pathway in olfactory neuroblastoma. Oncology. 2009:77(3-4):231-43. doi: 10.1159/000236047. Epub 2009 Sep 7 [PubMed PMID: 19738389]
Level 2 (mid-level) evidenceDemir E, Montgomery D, Naravetla V, Karsy M. Updated Insights into the Molecular Pathophysiology of Olfactory Neuroblastoma Using Multi-Omics Analysis. Journal of personalized medicine. 2025 Jul 13:15(7):. doi: 10.3390/jpm15070309. Epub 2025 Jul 13 [PubMed PMID: 40710426]
Ow TJ, Bell D, Kupferman ME, Demonte F, Hanna EY. Esthesioneuroblastoma. Neurosurgery clinics of North America. 2013 Jan:24(1):51-65. doi: 10.1016/j.nec.2012.08.005. Epub [PubMed PMID: 23174357]
Gallagher KK, Spector ME, Pepper JP, McKean EL, Marentette LJ, McHugh JB. Esthesioneuroblastoma: updating histologic grading as it relates to prognosis. The Annals of otology, rhinology, and laryngology. 2014 May:123(5):353-8. doi: 10.1177/0003489414526368. Epub 2014 Mar 25 [PubMed PMID: 24668054]
Trojanowski JQ, Lee V, Pillsbury N, Lee S. Neuronal origin of human esthesioneuroblastoma demonstrated with anti-neurofilament monoclonal antibodies. The New England journal of medicine. 1982 Jul 15:307(3):159-61 [PubMed PMID: 7201076]
Level 3 (low-level) evidenceWooff JC, Weinreb I, Perez-Ordonez B, Magee JF, Bullock MJ. Calretinin staining facilitates differentiation of olfactory neuroblastoma from other small round blue cell tumors in the sinonasal tract. The American journal of surgical pathology. 2011 Dec:35(12):1786-93. doi: 10.1097/PAS.0b013e3182363b78. Epub [PubMed PMID: 22020045]
Thompson LD. Olfactory neuroblastoma. Head and neck pathology. 2009 Sep:3(3):252-9. doi: 10.1007/s12105-009-0125-2. Epub 2009 Jul 16 [PubMed PMID: 20596981]
Mills SE. Neuroectodermal neoplasms of the head and neck with emphasis on neuroendocrine carcinomas. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc. 2002 Mar:15(3):264-78 [PubMed PMID: 11904342]
Saade RE, Hanna EY, Bell D. Prognosis and biology in esthesioneuroblastoma: the emerging role of Hyams grading system. Current oncology reports. 2015 Jan:17(1):423. doi: 10.1007/s11912-014-0423-z. Epub [PubMed PMID: 25416317]
Level 2 (mid-level) evidenceKlironomos G, Gonen L, Au K, Monteiro E, Mansouri A, Turel MK, Witterick I, Vescan A, Zadeh G, Gentili F. Endoscopic management of Esthesioneuroblastoma: Our experience and review of the literature. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2018 Dec:58():117-123. doi: 10.1016/j.jocn.2018.09.011. Epub 2018 Oct 16 [PubMed PMID: 30340976]
Korra H, Gandi JB, Nanuvala P, Ardha A. Experiences and Outcomes in Olfactory Neuroblastoma Over A Decade at a Tertiary Cancer Center. South Asian journal of cancer. 2022 Oct:11(4):336-339. doi: 10.1055/s-0041-1739181. Epub 2022 Aug 16 [PubMed PMID: 36756100]
Sasajima T, Kinouchi H, Tomura N, Watarai J, Mizoi K. High uptake of 123I-metaiodobenzylguanidine related to olfactory neuroblastoma revealed by single-photon emission CT. AJNR. American journal of neuroradiology. 2000 Apr:21(4):717-20 [PubMed PMID: 10782784]
Level 3 (low-level) evidencePalmieri DE, Tadokoro KS, Valappil B, Pakala T, Muthukrishnan A, Seethala RR, Snyderman CH. DOTATATE PET Imaging in Olfactory Neuroblastoma and Association with SSTR Expression. Journal of neurological surgery. Part B, Skull base. 2024 Oct:85(5):439-444. doi: 10.1055/a-2096-1802. Epub 2023 Jun 12 [PubMed PMID: 39228885]
Bernier J, Cooper JS, Pajak TF, van Glabbeke M, Bourhis J, Forastiere A, Ozsahin EM, Jacobs JR, Jassem J, Ang KK, Lefèbvre JL. Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head & neck. 2005 Oct:27(10):843-50 [PubMed PMID: 16161069]
Level 2 (mid-level) evidenceChao KS, Kaplan C, Simpson JR, Haughey B, Spector GJ, Sessions DG, Arquette M. Esthesioneuroblastoma: the impact of treatment modality. Head & neck. 2001 Sep:23(9):749-57 [PubMed PMID: 11505485]
Level 2 (mid-level) evidencePalejwala SK, Sharma S, Le CH, Chang E, Erman AB, Lemole GM Jr. Complex Skull Base Reconstructions in Kadish D Esthesioneuroblastoma: Case Report. Journal of neurological surgery reports. 2017 Apr:78(2):e86-e92. doi: 10.1055/s-0037-1601877. Epub [PubMed PMID: 28480156]
Level 3 (low-level) evidenceKarp EE, Gompel JJV, Choby G. Esthesioneuroblastoma (Olfactory Neuroblastoma): Overview and Extent of Surgical Approach and Skull Base Resection. Journal of neurological surgery reports. 2022 Jul:83(3):e80-e82. doi: 10.1055/s-0042-1753519. Epub 2022 Jul 10 [PubMed PMID: 35832684]
Level 3 (low-level) evidenceZeng Q, Tian Y, He Y, Xie Q, Ou L, Wang M, Chen W, Wei R. Long-Term Survival Outcomes and Treatment Experience of 64 Patients With Esthesioneuroblastoma. Frontiers in oncology. 2021:11():624960. doi: 10.3389/fonc.2021.624960. Epub 2021 Mar 4 [PubMed PMID: 33747939]
Bao C, Hu W, Hu J, Dong Y, Lu JJ, Kong L. Intensity-Modulated Radiation Therapy for Esthesioneuroblastoma: 10-Year Experience of a Single Institute. Frontiers in oncology. 2020:10():1158. doi: 10.3389/fonc.2020.01158. Epub 2020 Jul 17 [PubMed PMID: 32766154]
Gordon K, Gulidov I, Smyk D, Semenov A, Golubev K, Lemaeva A, Koryakin S, Jumaniyazova E, Vishnyakova P, Eremina I, Fatkhudinov T, Kaprin A. Upright proton therapy for esthesioneuroblastoma: a single-institution experience. Frontiers in oncology. 2024:14():1348291. doi: 10.3389/fonc.2024.1348291. Epub 2024 Jan 30 [PubMed PMID: 38352894]
Polin RS, Sheehan JP, Chenelle AG, Munoz E, Larner J, Phillips CD, Cantrell RW, Laws ER Jr, Newman SA, Levine PA, Jane JA. The role of preoperative adjuvant treatment in the management of esthesioneuroblastoma: the University of Virginia experience. Neurosurgery. 1998 May:42(5):1029-37 [PubMed PMID: 9588547]
Aljumaily RM, Nystrom JS, Wein RO. Neoadjuvant chemotherapy in the setting of locally advanced olfactory neuroblastoma with intracranial extension. Rare tumors. 2011 Mar 30:3(1):e1. doi: 10.4081/rt.2011.e1. Epub 2011 Mar 30 [PubMed PMID: 21464871]
Nishimura H, Ogino T, Kawashima M, Nihei K, Arahira S, Onozawa M, Katsuta S, Nishio T. Proton-beam therapy for olfactory neuroblastoma. International journal of radiation oncology, biology, physics. 2007 Jul 1:68(3):758-62 [PubMed PMID: 17398027]
Level 2 (mid-level) evidenceThomas SB, Balasubramaniam D, Hiran KR, Dinesh M, Pavithran K. Esthesioneuroblastoma with intracranial extension: A non-surgical approach. Asian journal of neurosurgery. 2016 Jul-Sep:11(3):313. doi: 10.4103/1793-5482.145087. Epub [PubMed PMID: 27366272]
Xiong L, Zeng XL, Guo CK, Liu AW, Huang L. Optimal treatment and prognostic factors for esthesioneuroblastoma: retrospective analysis of 187 Chinese patients. BMC cancer. 2017 Apr 11:17(1):254. doi: 10.1186/s12885-017-3247-z. Epub 2017 Apr 11 [PubMed PMID: 28399835]
Level 2 (mid-level) evidenceSun M, Wang K, Qu Y, Zhang J, Zhang S, Chen X, Wang J, Wu R, Zhang Y, Yi J, Xiao J, Xu G, Huang X, Luo J. Long-term analysis of multimodality treatment outcomes and prognosis of esthesioneuroblastomas: a single center results of 138 patients. Radiation oncology (London, England). 2020 Sep 18:15(1):219. doi: 10.1186/s13014-020-01667-4. Epub 2020 Sep 18 [PubMed PMID: 32948223]
Chamberlain MC. Treatment of intracranial metastatic esthesioneuroblastoma. Cancer. 2002 Jul 15:95(2):243-8 [PubMed PMID: 12124822]
Okai B, Lim J, Jaikumar V, Ghannam M, Mechtler LL, Vakharia K, Siddiqui AH, Levy EI. Revisiting intra-arterial chemotherapy-palliative utility in a case of recurrent esthesioneuroblastoma and literature review. Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences. 2025 Jul 24:():15910199251362087. doi: 10.1177/15910199251362087. Epub 2025 Jul 24 [PubMed PMID: 40702981]
Level 3 (low-level) evidenceTajudeen BA, Arshi A, Suh JD, St John M, Wang MB. Importance of tumor grade in esthesioneuroblastoma survival: a population-based analysis. JAMA otolaryngology-- head & neck surgery. 2014 Dec:140(12):1124-9. doi: 10.1001/jamaoto.2014.2541. Epub [PubMed PMID: 25356502]
Level 2 (mid-level) evidenceDulguerov P, Calcaterra T. Esthesioneuroblastoma: the UCLA experience 1970-1990. The Laryngoscope. 1992 Aug:102(8):843-9 [PubMed PMID: 1495347]
Level 2 (mid-level) evidenceYunyun Y, Yahui L, Yingshi P. ANGPTL4 overexpression is associated with progression and poor prognoses of olfactory neuroblastoma. Diagnostic pathology. 2025 Nov 24:20(1):130. doi: 10.1186/s13000-025-01729-9. Epub 2025 Nov 24 [PubMed PMID: 41286937]
Henson JC, Cutler CC, Cole KL, Lucke-Wold B, Khan M, Alt JA, Karsy M. Immunohistochemical Profiling and Staging in Esthesioneuroblastoma: A Single-Center Cohort Study and Systematic Review. World neurosurgery. 2023 Feb:170():e652-e665. doi: 10.1016/j.wneu.2022.11.094. Epub 2022 Nov 24 [PubMed PMID: 36435382]
Level 1 (high-level) evidence