Introduction
Esophageal foreign body impaction is a common clinical problem in emergency and acute care settings. An ingested object becomes lodged in the esophagus, most commonly at physiologic narrowing sites, including the upper esophageal sphincter (UES), the esophageal constriction at the level of the aortic arch, and the lower esophageal sphincter (LES). Although many ingested objects pass spontaneously through the gastrointestinal tract, esophageal impactions require prompt recognition and, in some cases, urgent intervention.
Esophageal foreign body impaction affects both adults and children, although etiologies differ by age group. Accidental ingestion of small objects, such as coins and toys, predominates in children. Food bolus impaction, particularly involving meat, predominates in adults and is frequently associated with underlying esophageal pathology, including strictures, rings, malignancy, or motility disorders.
Clinical presentation ranges from mild discomfort to severe symptoms, including dysphagia, odynophagia, drooling, chest pain, vomiting, and inability to tolerate oral secretions. High-risk objects, including button batteries, sharp objects, and magnets, carry a substantial risk of mucosal injury, perforation, and fistula formation and often require emergent removal. Early diagnosis, appropriate risk stratification, and timely interprofessional management are essential to prevent complications and optimize outcomes.
Though the event is often unwitnessed in young children, most patients present after accidental ingestion of a known object and remain clinically stable with mild symptoms. Diagnostic evaluation becomes more challenging in infants, young children, and individuals with cognitive impairment or psychiatric conditions who cannot or will not provide a reliable history. Broad clinical presentations and the potential for serious complications further complicate diagnosis and management, requiring a high index of suspicion.[1][2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Esophageal foreign body impaction in children most commonly results from accidental ingestion during exploratory behavior. Young children frequently place objects in the mouth, resulting in ingestion of small objects, such as coins, small toys, beads, button batteries, and magnets. Food impaction also occurs, particularly after ingestion of inadequately chewed food or large food boluses. The risk is highest among toddlers and preschool-aged children because of limited coordination, incomplete dentition, and a tendency to swallow without adequate chewing. Additional risk factors include unsupervised play, access to small household objects, and developmental delays or neurobehavioral conditions that impair judgment or oral motor control.
Unlike adults, children are less likely to have intrinsic esophageal disease, although congenital esophageal anomalies, strictures, and eosinophilic esophagitis predispose some children to recurrent impactions. Button batteries and magnets warrant particular concern because of the risk of rapid tissue injury, including pressure necrosis, perforation, fistula formation, and, in the case of button batteries, systemic toxicity. Pediatric esophageal foreign body impaction primarily reflects behavioral risk factors and environmental exposures, with a smaller contribution from underlying structural or inflammatory esophageal disorders than in adults.
The esophagus is a 20- to 25-cm muscular tube extending from the hypopharynx to the stomach (see Image. Digestive and Respiratory Structures Anatomically Related to the Esophagus). The esophageal wall consists of a mucosal lining and an outer muscular layer, with striated muscle proximally and smooth muscle distally. Natural esophageal narrowing predisposes to foreign body impaction, although most ingested objects that reach the stomach pass without intervention. Foreign body types vary by geographic region and dietary habits. For example, fish bones are a frequent cause in parts of East Asia.[4][5][6]
Epidemiology
Children account for approximately 80% of emergency department visits for esophageal foreign bodies.[7] Incidence is highest among older infants and toddlers, reflecting the tendency to place readily accessible objects in the mouth. Peak risk occurs between 6 months and 6 years of age, with most cases affecting children younger than 3 years.[8]
Esophageal foreign body impactions in children are usually accidental and involve small objects, including coins, pins, needles, button batteries, toy parts, crayons, marbles, bones, large food boluses, and jewelry. Coins are the most commonly ingested object.[9] Most affected children have normal esophageal anatomy. However, underlying conditions, including eosinophilic esophagitis, previous esophageal atresia repair, and prior Nissen fundoplication, increase the risk of impaction.[10]
In contrast, esophageal impaction in adults most commonly results from food boluses, particularly meat, with an estimated annual incidence of 13 per 100,000. Most impactions occur in the distal esophagus at sites of preexisting pathology, including diverticula, webs, rings, strictures, tumors, eosinophilic esophagitis, achalasia, scleroderma, and esophageal spasm. Therefore, adults with a history of food impaction should undergo follow-up esophageal evaluation, even after spontaneous symptom resolution.[11] A subset of adults presents after intentional foreign body ingestion related to self-harm or concealment of substances.
Pathophysiology
The esophagus has 3 physiologic points of narrowing where foreign bodies most commonly become impacted. These sites include the following:
- UES, which contains the cricopharyngeus muscle at the C6 level
- Midesophagus at the level of the aortic arch, at approximately the T4 level
- LES at the T10 to T11 level
Approximately 74% of pediatric foreign bodies become impacted at the UES, whereas about 68% of adult impactions occur in the distal esophagus and are frequently associated with underlying structural pathology.[12] The level of the left mainstem bronchus is another common site of impaction.
Complications range from local mucosal damage to life-threatening extraluminal injury. Local complications include mucosal abrasions, lacerations, necrosis, and stricture formation. Severe complications include airway compromise, esophageal perforation, tracheoesophageal fistula, vascular injury such as an aortoesophageal fistula, retropharyngeal abscess, mediastinitis, pericarditis, and vocal cord injury.[13]
Button batteries, multiple magnets, and sharp or pointed objects are associated with particularly high complication rates. Button battery ingestion has increased with the widespread use of batteries in household and recreational products.[14] Esophageal impaction allows electrical current to flow between the battery poles through the surrounding mucosa, causing pressure injury and rapid liquefactive necrosis that may progress to perforation. Leakage of corrosive contents further exacerbates tissue injury because button batteries contain heavy metals, such as lithium, mercury, or silver, as well as strong alkaline agents, such as sodium hydroxide or potassium hydroxide. Sharp foreign bodies carry a substantial risk of perforation and generally require urgent removal. The most commonly ingested sharp objects in children include pins, needles, paper clips, and fish bones.[15]
Magnet ingestion has become an increasingly important pediatric safety concern with the widespread use of small magnets in toys and household products.[16][17] High-powered neodymium magnets used in consumer products pose a particularly high risk because of their strong magnetic force. Ingestion of multiple magnets can result in attraction across adjacent bowel loops, causing tissue compression, pressure necrosis, fistula formation, obstruction, or perforation.[18] Even brief delays in diagnosis substantially increase the risk of serious complications, making early recognition and prompt management essential. More than 90% of severe complications occur in children aged 5 years or younger, particularly after ingestion of button batteries measuring 20 mm or larger. Prolonged esophageal impaction further increases the risk of developing complications.
History and Physical
The assessment of patients with ingested foreign bodies should elicit vital information, including the type and number of objects, the location, the time since ingestion, and the presenting signs and symptoms. These factors determine the need for emergent or urgent retrieval versus observation with follow-up. Most adults and older children can provide a history of foreign body ingestion and symptom onset.
The most common symptoms include foreign body sensation and dysphagia. Symptoms typically develop within minutes to hours. Foreign bodies in the upper esophagus are generally localized accurately, whereas middle or distal esophageal impactions often present as vague discomfort, aching, or chest pain. Additional symptoms include hypersalivation, retrosternal fullness, regurgitation, gagging, choking, hiccups, and retching. Odynophagia may indicate more severe forms of injury, such as esophageal laceration or perforation.
Physical examination may reveal anxiety and discomfort with swallowing. Inability to swallow saliva indicates complete esophageal obstruction and warrants more urgent treatment.
Infants, young children, and individuals with cognitive impairment may be unable to provide a reliable history, thus requiring a high index of suspicion. Presenting symptoms may include unexplained cough, gagging, poor feeding, drooling, or irritability in infants and young children. Esophageal foreign bodies may also compress the trachea, causing wheezing, cough, dyspnea, or stridor. Airway foreign bodies should remain in the differential diagnosis. Initial physical examination should focus on airway patency, vital signs, ability to manage secretions, and evidence of complications, including hematemesis, abnormal breath sounds, tenderness of the neck, chest, or abdomen, and subcutaneous emphysema.
Evaluation
Anteroposterior and lateral chest radiographs are the preferred initial diagnostic studies (see Image. Button Battery in the Upper Esophagus of a Child). Radiographs help identify the foreign body, determine its location, and detect complications. Chest radiographs are usually sufficient, although neck and abdominal radiographs may be indicated based on the clinical presentation.
Flat objects, including coins, bottle caps, and disc batteries, typically align in the coronal plane when lodged in the esophagus and appear round on the frontal (posteroanterior) view. In contrast, tracheal foreign bodies align in the sagittal plane and appear round on the lateral view. Circular radiopaque objects require careful evaluation for a halo or double-ring sign, which identifies a button battery and necessitates emergent removal. Chest radiography differentiates coins from button batteries with approximately 80% sensitivity, specificity, and accuracy.
Food, plastic, wood, and aluminum are radiolucent and are not visible on plain radiographs. Bones and glass may or may not be radiographically visible. Diagnostic endoscopy or computed tomography (CT) should be considered when findings from plain radiographs are unremarkable despite persistent clinical suspicion. CT has high sensitivity for detecting foreign bodies and is useful for identifying complications, such as perforation. The strong association between esophageal food impaction and eosinophilic esophagitis warrants consideration of esophagogastroduodenoscopy with biopsy, particularly in patients with recurrent impactions.[19]
Treatment / Management
Management in patients with a stable airway and no evidence of complications depends on the type and location of the foreign body, degree of obstruction, and duration of impaction. Endoscopic removal is the treatment of choice, achieving success rates exceeding 90% with complication rates below 5%. Endoscopic management is categorized according to the urgency of intervention. Categories include emergent (within 2 hours of presentation), urgent (within 24 hours of presentation), and elective or expectant (24 hours or more after presentation).[20][21][22][23](A1)
Indications for emergent removal include the following:
- Airway compromise or respiratory distress
- Inability to manage oral secretions, which often presents with persistent drooling
- Button battery impaction in the esophagus
- Symptomatic sharp foreign body impaction in the esophagus
- Presence of clinical manifestations of gastrointestinal perforation or obstruction, eg, fever, abdominal pain, or vomiting
Urgent removal is indicated for impaction involving the following foreign bodies:
- Multiple high-powered magnets
- Sharp objects in the stomach
- Button batteries in the stomach that produce symptoms
- Superabsorbent polymers in the esophagus or stomach
Endoscopic intervention should be performed within 24 hours for foreign bodies that are retained in the esophagus or have an unknown duration of impaction. In otherwise asymptomatic children, removal is generally recommended when the object remains in the stomach for more than 4 weeks. Selection of the endoscopic approach depends on the foreign body type and location, duration of impaction, patient age, airway status, and local expertise.[24][25][26](B2)
Flexible endoscopy is generally the 1st-line approach for most esophageal foreign body impactions in children because of its high success rate, minimally invasive nature, and ability to provide complete visualization of the esophagus and stomach. Flexible endoscopy is particularly useful for removing impacted blunt objects, such as food and coins. Rigid endoscopy may be preferred in selected situations, including impaction of sharp or large foreign bodies in the proximal esophagus, development of airway compromise, foreign body entrapment at the UES, and cases requiring enhanced airway protection or procedural control. Flexible endoscopy is generally associated with lower morbidity, less extensive instrumentation, and shorter recovery times. Rigid endoscopy provides superior control for dislodging proximal esophageal foreign bodies, particularly sharp objects, and may offer better airway protection. However, rigid endoscopy typically requires general anesthesia and specialized expertise.
Several medical therapies have been evaluated for esophageal foreign body impaction, although routine pharmacologic management is not recommended in children. Agents intended to relax the LES, particularly glucagon, have been used in attempts to facilitate the passage of smooth, blunt foreign bodies into the stomach. Glucagon is administered at a dose of 0.25 to 2 mg intravenously over 1 to 2 minutes in a sitting patient, followed by oral intake of water or a carbonated beverage after approximately 1 minute to promote esophageal distention and LES relaxation. Associated adverse effects include nausea and vomiting, which may dislodge the foreign body but also increase the risk of esophageal rupture. Available studies demonstrate limited efficacy compared with placebo and are constrained by small sample sizes and methodological limitations.[27]
The use of proteolytic enzymes, including papain, is not recommended for food bolus impaction. Reported complications of this approach include hypernatremia, mucosal injury, perforation, aspiration, and a theoretical risk of esophageal injury.[28]
Impaction of a disc battery in the esophagus constitutes a true emergency and requires immediate intervention. The most serious complication is a potentially fatal aortoesophageal fistula, with highest risk in presentations involving children aged younger than 5 years, ingestion of batteries 20 mm or larger, impaction at the level of the aortic arch, prolonged esophageal impaction, and the occurrence of any degree of hematemesis. In these situations, an interprofessional approach may be required, involving pediatric gastroenterology, pediatric surgery, cardiothoracic surgery, anesthesia, and radiology, with management in the operating room or cardiac catheterization laboratory.
Asymptomatic children with a coin impacted in the esophagus may be observed for up to 24 hours without increased risk of complications. Coin location is an important determinant of spontaneous passage, with 10% of proximal esophageal coins, 26% of midesophageal coins, and 43% of distal esophageal coins passing spontaneously within 16 hours of ingestion.
Adults presenting with esophageal food impaction should undergo evaluation for eosinophilic esophagitis, as esophageal food impaction may be the initial manifestation of the disease. Eosinophilic esophagitis is a chronic immune-mediated disorder believed to result from the combination of genetic susceptibility, environmental exposures, and aberrant immune responses to food antigens and, in some patients, aeroallergens. The incidence and prevalence of this condition have increased substantially over the past several decades.
Clinical manifestations often reflect a prolonged history of esophageal dysfunction that precedes the initial impaction. Patients may report intermittent dysphagia, prolonged meal times, excessive chewing, frequent fluid intake during meals, food avoidance or modification, difficulty swallowing pills, and recurrent food impactions. Personal or family histories of atopic disease or eosinophilic esophagitis further increase the likelihood of the diagnosis. Confirmation of eosinophilic esophagitis should prompt disease-specific management with anti-inflammatory therapy, dietary modification, and, when indicated, endoscopic dilation to reduce the risk of recurrent food impaction.[29]
Differential Diagnosis
Esophageal abrasions may produce a persistent foreign body sensation even after passage of the offending object. Reassessment within 12 to 24 hours is appropriate in stable patients who can tolerate oral intake. Persistent symptoms warrant further evaluation with CT imaging or endoscopy. Conditions that may produce a foreign body sensation in the absence of a retained object include infectious esophagitis due to Candida species, herpes simplex virus, or cytomegalovirus; noninfectious esophagitis, including cases secondary to reflux, pill ingestion, and eosinophilic inflammation; esophageal spasm; and globus pharyngeus (globus hystericus), a sensation of a lump or foreign body in the throat of uncertain etiology. Patients who are stable and able to tolerate oral intake should receive treatment of the underlying condition and appropriate follow-up care.
Prognosis
Approximately 80% to 90% of ingested foreign bodies pass spontaneously within 3 to 7 days. Children with esophageal injury from disc batteries require short- and long-term follow-up to assess for complications related to erosion, perforation, and esophageal stricture formation. Adults with food impactions have underlying abnormalities in 85% to 90% of cases and require evaluation and treatment of the underlying disorder.
Complications
Delayed diagnosis of esophageal foreign body can result in serious complications, including stricture formation. Less commonly, perforation may occur with pneumomediastinum, mediastinitis, pneumonia, or life-threatening hemorrhage secondary to major vascular injury.
Consultations
Consultation needs for patients with esophageal foreign body impaction depend on the type of object, location, timing, and severity of presenting symptoms and complications, as well as the services available at a given facility. Common consultations and management considerations are outlined below.
Pediatric gastroenterology serves as the primary consulting service for most pediatric esophageal foreign bodies requiring endoscopic removal, particularly coins, impacted food pieces, magnets, sharp objects, and items unlikely to pass spontaneously. Pediatric surgery consultation is indicated for suspected perforation, mediastinitis, abscess formation, failed endoscopic retrieval, or complications warranting operative intervention. Pediatric critical care or pediatric intensive care unit consultation is required in cases of airway compromise, respiratory distress, hemodynamic instability, caustic injury, perforation, severe edema, or cases requiring postoperative intensive monitoring.
Otolaryngology consultation is useful for evaluating and managing proximal or cervical esophageal foreign body impaction, airway symptoms, suspected upper esophageal entrapment, or cases that warrant rigid esophagoscopy. As in pediatric patients, general surgery referral is indicated in adults for complications requiring operative treatment, particularly when endoscopic management fails. Cardiothoracic surgery involvement is indicated when major thoracic complications arise, including esophageal perforation near great vessels, mediastinal injury, vascular erosion, or severe disc battery injury. Anesthesiology referral is frequently required for procedural sedation or general anesthesia during endoscopic retrieval, particularly in young children or high-risk airway cases. Pulmonology and respiratory therapy consultations are indicated when aspiration, airway compression, wheezing, or concurrent airway foreign body is suspected. Radiology supports urgent imaging interpretation, localization, fluoroscopic guidance in selected cases, and evaluation of complications (see Image. Pill Retention in the Distal Esophagus).
Poison control and toxicology consultation is recommended for button battery ingestion due to rapid tissue injury and evolving management recommendations. In the US, the National Poison Center provides guidance.
Deterrence and Patient Education
Family education is essential, as many pediatric esophageal foreign body ingestions are preventable, particularly in children younger than 5 years. Counseling and prevention strategies should aim to reduce exposure to high-risk objects. Small objects, including coins, button batteries, magnets, jewelry, small toy parts, marbles, and safety pins, should be kept out of children’s reach. Battery-containing devices, such as remote controls, hearing aids, toys, watches, and key fobs, should be secured, and spare batteries must be stored in locked containers. Toys with small detachable parts should be avoided in young children.
Magnet-specific counseling is also essential. High-powered magnets are particularly dangerous because attraction across tissue planes can result in necrosis, fistula formation, perforation, obstruction, or death. Families may underestimate the risk, as early symptoms can appear mild despite significant underlying injury.
Feeding and behavioral counseling should include avoidance of high-risk foods in young children, including whole grapes, hot dogs, large meat chunks, hard candy, and nuts when developmentally inappropriate. Recommended practices include age-appropriate food preparation, supervised eating, and avoidance of running or talking while eating.
Additional counseling may be required for special populations, including children with developmental delays, autism spectrum disorder, and esophageal disease entities, such as eosinophilic esophagitis or strictures. These groups carry a higher risk of recurrent ingestion.
Postdischarge education should emphasize close monitoring and prompt return for symptoms such as drooling, dysphagia, vomiting, chest pain, fever, neck swelling, hematemesis, respiratory distress, or persistent cough. Delayed complications may occur even after initial clinical improvement.
Button battery education should emphasize several key points for caregivers. Serious injuries can occur within 2 hours of ingestion. Early symptoms may mimic a viral illness, which can delay recognition. Any suspected ingestion requires immediate emergency evaluation.
Prevention at the systems level includes public awareness campaigns, safer battery compartment regulations, use of warning labels, anticipatory guidance during pediatric visits, and education in schools and daycare settings. Still, education alone does not fully prevent ingestions. Many events occur despite supervision due to widespread use of lithium batteries and small magnets in household products. Therefore, effective prevention requires engineering controls, packaging standards, and product safety regulations in addition to caregiver awareness.
Pearls and Other Issues
Key diagnostic challenges and considerations in esophageal foreign body impaction include the following:
- Plain radiographs identify radiopaque materials, such as metallic objects. However, many ingested items, such as plastic, are radiolucent and may require contrast studies (eg, barium swallow) or endoscopy for detection.
- Coins lodged in the esophagus typically appear with the flat surface on the anteroposterior view, whereas tracheal placement demonstrates the flat surface more clearly on the lateral view.
- Differentiation between a coin and a disc battery on radiographs may be challenging, making careful assessment for distinguishing features essential.
- Button battery ingestion warrants immediate localization and emergent removal when the battery is lodged in the esophagus.
Although a clear history of ingestion is often obtained, a substantial proportion of pediatric foreign body ingestions are unwitnessed. Therefore, a high index of suspicion is required for diagnosis, and esophageal foreign body should be considered in any young child presenting with a sudden change in eating behavior.
Enhancing Healthcare Team Outcomes
Management of esophageal foreign bodies requires timely coordination among multiple healthcare professionals through an interprofessional, patient-centered approach. Most patients initially present to the emergency department, where early recognition is essential to prevent complications, such as airway compromise, perforation, mediastinitis, or vascular injury.
Triage nurses play a critical role in identifying concerning symptoms, including drooling, dysphagia, odynophagia, vomiting, chest pain, refusal to eat, stridor, wheezing, and respiratory distress. High-risk ingestions, such as those involving button batteries, magnets, and sharp objects, require immediate prioritization due to the potential for rapid tissue injury. Emergency nurses support ongoing care through close monitoring of airway status, oxygenation, pain, hydration, and evolving symptoms, while maintaining communication with caregivers throughout the evaluation process.
Emergency medicine physicians manage the initial evaluation, imaging studies, and stabilization measures and facilitate timely specialty consultation. Early involvement of the appropriate specialty is recommended once an esophageal foreign body is identified or strongly suspected. Gastroenterology commonly performs endoscopic retrieval, while otolaryngology may assist with proximal esophageal foreign bodies or airway-related concerns. Pediatric or cardiothoracic surgery consultation may be required for perforation, failed endoscopic removal, mediastinal complications, or severe button battery injury. Anesthesiology referral is often required for procedural sedation or airway management, particularly in young children or critically ill patients.
Although many ingested foreign bodies pass spontaneously, a significant subset requires urgent intervention. Foreign bodies lodged in the esophagus are less likely to pass without treatment and may lead to serious complications if management is delayed. Button batteries, multiple magnets, sharp objects, and symptomatic impactions require emergent evaluation and, often, urgent removal.
Patient and caregiver education is an essential component of care prior to discharge. Clinicians, nurses, and other team members should counsel families on prevention strategies, including keeping small objects like coins, batteries, and magnets out of children’s reach and ensuring appropriate supervision during meals and play. Caregivers should also receive education on warning signs that require immediate medical attention, such as persistent drooling, inability to tolerate secretions, vomiting, chest pain, fever, hematemesis, or respiratory symptoms.
Prevention cannot rely solely on parental vigilance. Many injuries occur despite supervision due to the widespread availability of button batteries and high-powered magnets in household products. Therefore, reducing morbidity requires public awareness, product safety measures, and early recognition in healthcare settings. Outcomes for most patients with esophageal foreign body impaction are excellent with prompt diagnosis, coordinated interprofessional care, and timely intervention.[30][31]
Media
(Click Image to Enlarge)

Button Battery in the Upper Esophagus of a Child. This periapical chest radiograph displays the classic “double rim” or “halo” sign, which distinguishes the battery from a coin. The foreign object is lodged near the clavicles.
Contributed by S Dulebohn, MD
(Click Image to Enlarge)
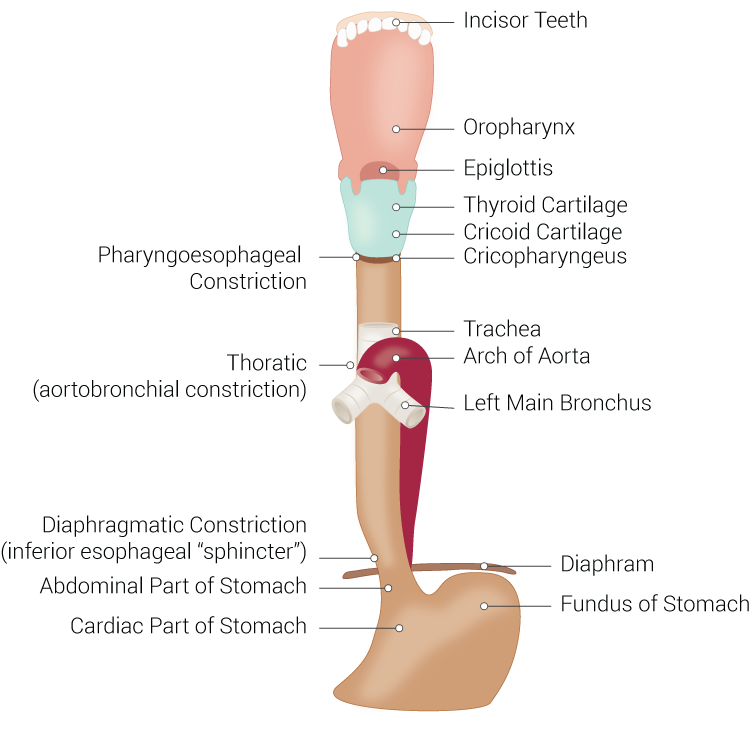
Digestive and Respiratory Structures Anatomically Related to the Esophagus. This illustration shows the esophagus and adjacent digestive and respiratory structures, including the incisors, oropharynx, laryngeal cartilages, trachea, aortic arch, bronchi, diaphragm, stomach, and esophageal constrictions.
Illustrated by B Palmer
(Click Image to Enlarge)

Pill Retention in the Distal Esophagus. This fluoroscopic image shows the lower esophagus and stomach. A pill is located immediately proximal to the gastroesophageal junction.
Contributed by Dr.Dawood Tafti, MD.
References
Anderson KL, Dean AJ. Foreign bodies in the gastrointestinal tract and anorectal emergencies. Emergency medicine clinics of North America. 2011 May:29(2):369-400, ix. doi: 10.1016/j.emc.2011.01.009. Epub [PubMed PMID: 21515184]
Al Lawati TT, Al Marhoobi RM. Timing of Button Battery Removal From the Upper Gastrointestinal System in Children. Pediatric emergency care. 2021 Aug 1:37(8):e461-e463. doi: 10.1097/PEC.0000000000001697. Epub [PubMed PMID: 30601350]
Zhang XR, Li Q. [A case of magnetic pharyngeal foreign body in children]. Lin chuang er bi yan hou tou jing wai ke za zhi = Journal of clinical otorhinolaryngology head and neck surgery. 2018 Sep:32(18):1432-1433. doi: 10.13201/j.issn.1001-1781.2018.18.017. Epub [PubMed PMID: 30550179]
Level 3 (low-level) evidenceMalik SA, Qureshi IA, Muhammad R. Diagnostic Accuracy Of Plain X-Ray Lateral Neck In The Diagnosis Of Cervical Esophageal Foreign Bodies Keeping Oesophagoscopy As Gold Standard. Journal of Ayub Medical College, Abbottabad : JAMC. 2018 Jul-Sep:30(3):386-388 [PubMed PMID: 30465371]
Al Lawati TT, Al Marhoobi R. Patterns and Complications of Ingested Foreign Bodies in Omani Children. Oman medical journal. 2018 Nov:33(6):463-467. doi: 10.5001/omj.2018.86. Epub [PubMed PMID: 30410687]
Shatani N, Alshaibani S, Potts J, Phillips B, Bray H. Chest Radiograph Alone Is Sufficient as the Foreign Body Survey for Children Presenting With Coin Ingestion. Pediatric emergency care. 2021 Sep 1:37(9):e524-e527. doi: 10.1097/PEC.0000000000001688. Epub [PubMed PMID: 30461670]
Level 3 (low-level) evidenceArana A, Hauser B, Hachimi-Idrissi S, Vandenplas Y. Management of ingested foreign bodies in childhood and review of the literature. European journal of pediatrics. 2001 Aug:160(8):468-72 [PubMed PMID: 11548183]
Manfredi MA, Alvarez RP, Arai K, Cheema HA, Darma A, Elawad M, Iglesias C, Homan M, Saadah OI, Walsh CM, de Ridder L. Global insights on the diagnosis, management, and prevention of pediatric ingestions: A report from the FISPGHAN expert panel. JPGN reports. 2025 Aug:6(3):274-287. doi: 10.1002/jpr3.70025. Epub 2025 May 26 [PubMed PMID: 40814587]
Kramer RE, Lerner DG, Lin T, Manfredi M, Shah M, Stephen TC, Gibbons TE, Pall H, Sahn B, McOmber M, Zacur G, Friedlander J, Quiros AJ, Fishman DS, Mamula P, North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition Endoscopy Committee. Management of ingested foreign bodies in children: a clinical report of the NASPGHAN Endoscopy Committee. Journal of pediatric gastroenterology and nutrition. 2015 Apr:60(4):562-74. doi: 10.1097/MPG.0000000000000729. Epub [PubMed PMID: 25611037]
Triadafilopoulos G, Roorda A, Akiyama J. Update on foreign bodies in the esophagus: diagnosis and management. Current gastroenterology reports. 2013 Apr:15(4):317. doi: 10.1007/s11894-013-0317-5. Epub [PubMed PMID: 23435762]
Denney W, Ahmad N, Dillard B, Nowicki MJ. Children will eat the strangest things: a 10-year retrospective analysis of foreign body and caustic ingestions from a single academic center. Pediatric emergency care. 2012 Aug:28(8):731-4. doi: 10.1097/PEC.0b013e31826248eb. Epub [PubMed PMID: 22858742]
Level 2 (mid-level) evidenceGretarsdottir HM, Jonasson JG, Björnsson ES. Etiology and management of esophageal food impaction: a population based study. Scandinavian journal of gastroenterology. 2015 May:50(5):513-8. doi: 10.3109/00365521.2014.983159. Epub 2015 Feb 22 [PubMed PMID: 25704642]
Level 2 (mid-level) evidenceLeinwand K, Brumbaugh DE, Kramer RE. Button Battery Ingestion in Children: A Paradigm for Management of Severe Pediatric Foreign Body Ingestions. Gastrointestinal endoscopy clinics of North America. 2016 Jan:26(1):99-118. doi: 10.1016/j.giec.2015.08.003. Epub [PubMed PMID: 26616899]
Chandler MD, Ilyas K, Jatana KR, Smith GA, McKenzie LB, MacKay JM. Pediatric Battery-Related Emergency Department Visits in the United States: 2010-2019. Pediatrics. 2022 Sep 1:150(3):. pii: e2022056709. doi: 10.1542/peds.2022-056709. Epub [PubMed PMID: 36032018]
Wyllie R. Foreign bodies in the gastrointestinal tract. Current opinion in pediatrics. 2006 Oct:18(5):563-4 [PubMed PMID: 16969173]
Level 3 (low-level) evidenceSeguier-Lipszyc E, Samuk I, Almog A, Silbermintz A, Kravarusic D. Multiple magnet ingestion in children: A problem on the rise. Journal of paediatrics and child health. 2022 Oct:58(10):1824-1828. doi: 10.1111/jpc.16117. Epub 2022 Jul 16 [PubMed PMID: 35841278]
Hayward RK, Saxena AK. Surgical management of pediatric multiple magnet ingestions in the past two decades of minimal access surgery- systematic review of operative approaches. Updates in surgery. 2024 Aug:76(4):1203-1211. doi: 10.1007/s13304-023-01750-x. Epub 2024 Feb 4 [PubMed PMID: 38310610]
Level 1 (high-level) evidenceAlfonzo MJ, Baum CR. Magnetic Foreign Body Ingestions. Pediatric emergency care. 2016 Oct:32(10):698-702 [PubMed PMID: 27749667]
Kamalumpundi V, Saha B, Leggett C. Management of Foreign Body Ingestions and Food Impactions: Advice for General Practitioners. Mayo Clinic proceedings. 2025 Aug:100(8):1411-1419. doi: 10.1016/j.mayocp.2025.03.035. Epub [PubMed PMID: 40754397]
Aiolfi A, Ferrari D, Riva CG, Toti F, Bonitta G, Bonavina L. Esophageal foreign bodies in adults: systematic review of the literature. Scandinavian journal of gastroenterology. 2018 Oct-Nov:53(10-11):1171-1178. doi: 10.1080/00365521.2018.1526317. Epub 2018 Nov 5 [PubMed PMID: 30394140]
Level 1 (high-level) evidenceHuang T, Li WQ, Xia ZF, Li J, Rao KC, Xu EM. Characteristics and outcome of impacted button batteries among young children less than 7 years of age in China: a retrospective analysis of 116 cases. World journal of pediatrics : WJP. 2018 Dec:14(6):570-575. doi: 10.1007/s12519-018-0188-9. Epub 2018 Oct 17 [PubMed PMID: 30328588]
Level 2 (mid-level) evidenceBekkerman M, Sachdev AH, Andrade J, Twersky Y, Iqbal S. Endoscopic Management of Foreign Bodies in the Gastrointestinal Tract: A Review of the Literature. Gastroenterology research and practice. 2016:2016():8520767 [PubMed PMID: 27807447]
Cervi E. Towards evidence based emergency medicine: best BETs from the Manchester Royal Infirmary. BET 3: management of asymptomatic children with a history of coin ingestion. Emergency medicine journal : EMJ. 2010 May:27(5):395-6. doi: 10.1136/emj.2010.094904. Epub [PubMed PMID: 20442177]
Meher BK, Naik S, Mishra SR, Augustus S. Flexible Fiberoptic Bronchoscopy for Esophageal Foreign Body Removal in Children. Indian journal of critical care medicine : peer-reviewed, official publication of Indian Society of Critical Care Medicine. 2025 Apr:29(8):700-703. doi: 10.5005/jp-journals-10071-25023. Epub 2025 Aug 18 [PubMed PMID: 41114395]
Lee SM, Baek SE, Lee CW, Kim YC, Kim MJ. Foreign Body Ingestion: Radiologic Evaluation, Findings, and Management. Korean journal of radiology. 2025 Jul:26(7):638-649. doi: 10.3348/kjr.2025.0118. Epub [PubMed PMID: 40590076]
Liu B, Kuang S, Cao M, Li X. Esophageal foreign bodies: a retrospective analysis of 275 cases. Journal of thoracic disease. 2025 Jun 30:17(6):4136-4144. doi: 10.21037/jtd-2025-758. Epub 2025 Jun 19 [PubMed PMID: 40688279]
Level 2 (mid-level) evidence. BET 1: use of glucagon for oesophageal food bolus impaction. Emergency medicine journal : EMJ. 2015 Jan:32(1):85-8. doi: 10.1136/emermed-2014-204467.1. Epub [PubMed PMID: 25511630]
Al-Haddad M, Ward EM, Scolapio JS, Ferguson DD, Raimondo M. Glucagon for the relief of esophageal food impaction does it really work? Digestive diseases and sciences. 2006 Nov:51(11):1930-3 [PubMed PMID: 17004122]
Dellon ES, Muir AB, Katzka DA, Shah SC, Sauer BG, Aceves SS, Furuta GT, Gonsalves N, Hirano I. ACG Clinical Guideline: Diagnosis and Management of Eosinophilic Esophagitis. The American journal of gastroenterology. 2025 Jan 1:120(1):31-59. doi: 10.14309/ajg.0000000000003194. Epub 2025 Jan 2 [PubMed PMID: 39745304]
Bolton SM, Saker M, Bass LM. Button battery and magnet ingestions in the pediatric patient. Current opinion in pediatrics. 2018 Oct:30(5):653-659. doi: 10.1097/MOP.0000000000000665. Epub [PubMed PMID: 30188872]
Level 3 (low-level) evidenceHam PB 3rd, Ellis MA, Simmerman EL, Walsh NJ, Lalani A, Young M, Hatley R, Howell CG, Hughes CA. Analysis of 334 Cases of Pediatric Esophageal Foreign Body Removal Suggests that Traditional Methods Have Similar Outcomes Whereas a Magnetic Tip Orogastric Tube Appears to Be an Effective, Efficient, and Safe Technique for Disc Battery Removal. The American surgeon. 2018 Jul 1:84(7):1152-1158 [PubMed PMID: 30064579]
Level 3 (low-level) evidence