Introduction
Esophagogastroduodenoscopy (EGD) is a widely utilized diagnostic and therapeutic procedure that enables limited visualization of the oropharynx and detailed examination of the esophagus, stomach, and duodenum. When a longer instrument is used, the distal duodenum and jejunum can also be examined. This procedure plays a central role in the diagnostic evaluation of a wide variety of upper gastrointestinal disorders. In addition to its diagnostic utility, EGD facilitates therapeutic interventions, eg, hemostasis, stricture dilation, variceal ligation, and foreign body removal, making this modality an indispensable tool in modern gastroenterology.
EGD is generally very safe, with major complications occurring in fewer than 2% of cases, although risks such as bleeding, perforation, or sedation-related cardiopulmonary events must be considered. Advances in technology, including high-definition scopes, optical zoom, and single-use disposable gastroscopes, have further enhanced diagnostic accuracy and infection control. Professional guidelines, including those from the American Society for Gastrointestinal Endoscopy (ASGE) and European Society of Gastrointestinal Endoscopy (ESGE), have emphasized the importance of quality indicators, documentation, and biopsy protocols to standardize practice and improve outcomes. As applications of EGD expand across both adult and pediatric populations, continued adherence to evidence-based protocols and interprofessional collaboration remain essential to maximizing the clinical impact of this versatile procedure.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Cricopharyngeal Area
The pharynx and vocal cords can be briefly inspected before the endoscope passes the cricopharyngeus muscle, where the masses pass through the upper esophageal sphincter (UES) and into the proximal esophagus. The UES is typically located 15 to 18 cm from the incisors.
Esophagus
The esophagus lies posterior to the trachea, beginning at the upper esophageal sphincter (UES) and extending to the lower esophageal sphincter (LES), which generally corresponds to the esophagogastric junction (EGJ), where the esophagus meets the gastric cardia. Its diameter ranges from 4 to 6 mm and its length from 9 to 10 cm in a term infant, increasing to approximately 2 cm in diameter and 25 cm in length in an adult. Three physiologic constrictions exist along the esophageal lumen: at the cervical esophagus, at the level of compression by the aortic arch and left bronchus, and at the diaphragm. The squamo-columnar junction usually lies about 40 cm from the incisors. The Z-line, where the mucosal color transitions from pale to reddish-pink, delineates the esophagus from the gastric cardia.
Stomach
The stomach is positioned inferior to the diaphragm, beginning approximately 40 cm distal to the incisors in adults. The onset of gastric rugal folds identifies entry into the gastric cardia, distinct from the flat esophageal mucosa. In Barrett esophagus, the Z-line may lie above the EGJ, and diagnosis requires biopsies demonstrating gastric or intestinal epithelium above the junction. The portion of the stomach immediately distal to the cardia forms the fundus, best visualized endoscopically in a retroflexed view. The majority of the stomach comprises the gastric body, or corpus. Along the lesser curvature, the incisura angularis marks the transition from the gastric body to the antrum, which is also identified endoscopically by the disappearance of rugae and the presence of flat antral mucosa. The pyloric channel serves as the muscular passage between the distal stomach and the duodenal bulb, the first segment of the duodenum.
Duodenum
The duodenum extends from the pylorus to the duodenojejunal junction at the level of the ligament of Treitz. The duodenal bulb lies immediately distal to the pylorus. The second, third, and fourth portions of the duodenum form a C-shaped loop, turning posteriorly and to the right for 2.5 cm, descending inferiorly for 7.5 to 10 cm, and then turning anteriorly and to the left for approximately 2.5 cm before connecting with the jejunum.
Indications
Diagnostic Indications
The following are indications for EGD:
- Persistent upper abdominal pain or pain associated with alarming symptoms, eg, weight loss or anorexia
- Persistent nausea or vomiting of unknown etiology
- Dysphagia or odynophagia
- Chronic gastroesophageal reflux disorder (GERD), persistent or unresponsive to therapy
- Screening for and surveillance of Barrett's esophagus
- Evaluation of upper gastrointestinal bleeding presenting with hematemesis, melena, or rectal bleeding
- Examination after caustic ingestion
- Screening for and surveillance of esophageal varices in patients with documented portal hypertension
- Surveillance for mucosal healing of esophagitis, eosinophilic esophagitis, or gastric ulcers
- Iron deficiency anemia when an upper gastrointestinal source of bleeding is suspected, when colonoscopy is nondiagnostic in the evaluation of gastrointestinal bleeding, or when iron malabsorption is suspected
- Chronic diarrhea or malabsorption
- Surveillance for malignancy in patients with premalignant conditions, eg, Barrett's esophagus, polyposis syndromes, previous caustic ingestion, atrophic gastritis, or gastric intestinal metaplasia (GIM) [1][2]
- To follow up radiologic demonstration of a lesion (suspected ulcer, stricture, obstruction, or mass)
Therapeutic Indications
Therapeutic indications for EGD include:
- Control of upper gastrointestinal bleeding
- Foreign body removal
- Biopsies
- Removal of polyps
- Placement of feeding or draining tubes: Percutaneous endoscopic gastrostomy (PEG), percutaneous endoscopic gastrostomy/jejunostomy (PEG/J), or percutaneous endoscopic jejunostomy (PEJ)
- Endo-bariatric therapy
- Management of stenotic lesions with dilating catheters or balloon dilation
- Management of achalasia with pneumatic balloon dilation, endoscopic myotomy, injection of botulinum toxin, or peroral endoscopic myotomy (POEM) [3]
- Endoscopic eradication of Barrett's esophagus (eg, radiofrequency ablation or endoscopic mucosal resection for dysplasia, or endoscopic submucosal dissection for early malignancy [4]
- Palliative stenting across a stenosing luminal neoplasm of the esophagus, stomach, or duodenum
- Esophageal variceal band ligation or sclerotherapy
- Intra-operative evaluation and treatment of anastomotic reconstruction (eg, anastomotic leaks, pouch evaluation during bariatric surgery) [5][6]
- Third-space endoscopy (TSE) procedures, including:
- Per oral endoscopic myotomy (POEM) for achalasia [7]
- Endoscopic submucosal dissection (ESD) [8]
- Zenker's diverticulotomy (Z-POEM) [7]
- Endoscopic gastric pyloromyotomy (GPOEM) for gastroparesis [9]
- Submucosal tunneling endoscopic resection (STER) for the resection of submucosal tumors [10]
- Tunneling recanalization of the esophagus (POETRE) to create a tunnel or passage through or bypassing obstructed areas of the esophagus due to cancer or radiation [8]
Details of third-space endoscopy procedures are beyond the scope of this activity.
Contraindications
Absolute Contraindications
Absolute contraindications of EGD include:
- Suspected or known perforated viscus
- Severe cardiopulmonary instability (eg, recent myocardial infarction, decompensated congestive heart failure, respiratory failure)
- History of a bleeding disorder (eg, hemophilia, von Willebrand's disease) without factor prophylaxis
- Toxic megacolon and clinical instability
- Uncooperative patient
- Inability to get informed consent
Relative Contraindications
EGD is relatively contraindicated for the following conditions:
- Severe neutropenia
- Coagulopathy (severe thrombocytopenia or significantly prolonged INR) [11]
- Patients receiving anticoagulation or antiplatelet drugs (except aspirin) who are having procedures, including planned polypectomy, stricture dilatation, laser ablation, and coagulation, with a bleeding risk that outweighs the cardiovascular benefit of the medicines (Please refer to the Technique or Treatment section for more information on percutaneous feeding tube placement)
- Untreated severe hemodynamic shock
- Increased risk of perforation (recent bowel surgery or megacolon)
- Unstable aortic aneurysm
- Patients with altered anatomy
Equipment
Gastroscopes
Standard gastroscopes measure 10 mm in diameter, have a 2.8 mm instrument channel, and are usually 100 cm long. For children weighing less than 10 kg, endoscopes with a diameter of less than 6 mm are recommended for routine endoscopy. Gastroscopes with larger operating channels (3.8 to 4.2 mm) or with 2 channels (one for suction and the other for irrigation and passage of accessories) are preferred for therapeutic procedures, while high-definition models with optical zoom are valuable for screening premalignant gastric or duodenal lesions.
Accessories
Biopsy forceps (pediatric, standard, and jumbo) are primarily used to obtain mucosal biopsies. They may be spiked, nonspiked, or serrated, and are available with outer diameters ranging from 1.2 to 3 mm. Different companies make similar products with varying characteristics.[12]
For retrieval of a foreign body during EGD, rat tooth forceps, alligator forceps, a retrieval net, a polypectomy snare, overtubes of esophageal and gastric lengths, and a foreign body protector hood should be available. Additional equipment may be required for anticipated therapeutic procedures or third-space endoscopy.[12][13][14][12]
Single-Use Gastroscope
Single-use disposable gastroscopes are sterile, flexible endoscopes designed for single-use to eliminate cross-contamination risks and reduce the transmission of infections during upper gastrointestinal procedures.[15]
Personnel
The following personnel are typically involved during EGD procedures:
- Endoscopist
- Gastroenterologist or trained surgeon
- Performs the procedure and interprets findings
- Endoscopy nurse or technician
- Assists with patient preparation and education
- Monitors vital signs and supports the endoscopist during the procedure
- Prepares and assists by managing accessories inserted through the scope channel
- Anesthesiologist or certified registered nurse anesthetist (CRNA)
- Administers sedation or anesthesia
- Monitors cardiorespiratory status during and after the procedure
- Recovery room nurse
- Provides postprocedure care
- Monitors recovery from sedation and ensures discharge readiness
Preparation
Routine endoscopy in children and adults is typically performed in an outpatient setting, using either parenteral or general anesthesia. In the hospital setting, EGD can be performed at the bedside in the ICU or emergency room with moderate sedation.
Diet
Preparation for the elective upper endoscopy procedure involves fasting. According to the American Society of Anesthesiologists (ASA) guidelines, patients should fast for at least 2 hours after consuming clear liquids and 6 hours after eating light meals.[16] In emergencies or in conditions where gastric emptying is impaired, the potential for pulmonary aspiration of gastric contents must be considered to determine the following:
- level of sedation
- whether endotracheal intubation should be considered to protect the airway
- whether the procedure should be delayed
Medications
Most medications can be continued and are usually taken with a small sip of water before the endoscopy. However, diabetes medications need to be adjusted due to the fasting period before the procedure.
Antithrombotic Drugs
The decision to continue or discontinue anticoagulants depends on whether the procedure is low-risk (eg, diagnostic EGD with or without biopsy) or high-risk (eg, polypectomy or endoscopic mucosal resection). This decision also varies by clinical context, specifically between elective and urgent indications. In general, continuing aspirin and clopidogrel for primary or secondary cardiovascular prophylaxis is considered safe for low-risk procedures. The ASGE or ESGE guidelines should be consulted to assess both procedural and patient-related bleeding and thrombotic risks, guiding the management of antithrombotic therapy.[17][18] A 2025 report and literature review by the ASGE recommends that percutaneous endoscopic gastrostomy (PEG) or percutaneous endoscopic jejunostomy (PEJ), or PEG/J tube placement can be performed without discontinuing antiplatelet drugs, and the decision about continuing or discontinuing anticoagulants before percutaneous tube placement in a patient with a clear indication for these drugs (eg, soon after a stroke) should be made by a interprofessional panel that can weigh the risks of bleeding from the procedure versus the cardiovascular benefits of the drugs.[19]
Antibiotics
According to ASGE and ESGE recommendations, routine antibiotic prophylaxis is not recommended outside of these specific scenarios.[20] Antibiotic prophylaxis is indicated for the following patient populations undergoing EGD:
- Those undergoing PEG orPEJ due to the risk of peristomal infection
- Patients with cirrhosis and active gastrointestinal bleeding should be treated to reduce the risk of bacteremia and spontaneous bacterial peritonitis
- Individuals with high-risk cardiac conditions or with established gastrointestinal infections in whom enterococci are suspected as the causative organisms
Risk Stratification and Sedation Planning
Before a planned procedure, the patient should undergo an evaluation to assess comorbidities and predict periprocedural risks. The ASA Physical Status Classification is commonly used in practice, and collaborative assessment by anesthesiologists and anesthetists is essential to ensure the procedure is planned safely.[21]
Informed Consent
Informed consent is a voluntary agreement between a patient with decision-making capacity and the healthcare practitioner, acknowledging the patient's understanding of the proposed procedure, its associated risks, benefits, and potential complications.
Sedation and Monitoring
Sedation is used in most patients not only to minimize discomfort but also to provide relaxation and amnesia for the procedure. All patients undergoing upper endoscopy require preprocedural evaluation to assess their risk for sedation and to manage potential problems related to preexisting health conditions. The choice of sedation varies from conscious sedation delivered by the proceduralist or monitored anesthesia care provided by an anesthesiologist or nurse anesthetist, and preferences for one type of sedation over another are largely based on training and available local resources. For routine upper endoscopies, many endoscopists use intravenous sedation with propofol. For therapeutic endoscopic procedures such as foreign body removal or complex therapeutic procedures (eg, endoscopic submucosal dissection), general anesthesia may be required.[22][23]
Time Out Procedures
A "time-out" is a mandatory pause before the procedure to review the procedure while the patient is awake and alert, so they are involved in the process. The time-out includes confirmations of the following:
- That the patient understands the nature and details of the planned procedure and sedation
- The patient's name and statement of the procedure
- Indications, goals, possible limitations, and steps to be carried out
- All required equipment is available and fully functional
- Monitoring equipment is ready and operational, including IV access, pulse oximetry, blood pressure, and cardiac monitoring as appropriate for the level of anesthesia to be provided
- Proper patient positioning
- Determining whether additional steps are required before starting the procedure [24]
Technique or Treatment
Patient Position and Preparation
The patient is preferably positioned in the left lateral decubitus position with the neck flexed. A bite guard is placed to protect the teeth and the scope. Monitoring devices are attached along with nasal prongs (or a mask) for oxygenation (see Image. Upper Endoscopy). The supine position, with the head of the bed elevated at least 30 degrees, is used for PEG tube placement.
Handling the Endoscope
The control section of the endoscope should rest comfortably in the palm of the left hand. The thumb controls the up or down movement of the tip of the endoscope using a large wheel. The index and middle fingers control the suction, air, and water valves. The right hand is used to advance and withdraw the insertion section of the endoscope, control its axial rotation, and to insert instruments such as biopsy forceps, cytology brushes, needles for injection, hemostatic clips, polypectomy snares, foreign body retrieval instruments, and syringes for irrigation via the biopsy channel.
Esophageal Intubation
The endoscope is introduced into the mouth and to the base of the tongue under direct visualization. The tip of the scope is then gently deflected downward until the vocal cords, epiglottis, both piriform sinuses, and cricoarytenoid cartilages are visualized. The scope is then passed behind and to the right of the arytenoid cartilage towards the upper esophageal sphincter. The upper esophageal sphincter is passed under direct visualization, often with gentle pressure applied while insufflating air.
Esophagus and Esophagogastric Junction
The endoscope is advanced down the esophagus while simultaneously examining the mucosa for any inflammation, ulcerations, furrowing, varices, narrowing, or strictures (see Image. Endoscopy of the Esophagus). The location of the esophagogastric junction should be noted. The squamocolumnar junction, also referred to as the Z-line, is the area where the squamous epithelial lining of the esophagus (pale pink colored) meets the columnar lining mucosa (salmon-colored) of the stomach (see Image. Endoscopy of the Z-Line). The level of the Z-line should also be noted, and whether it corresponds to the start of the gastric rugal folds.
Stomach
The stomach is entered after passing the esophagogastric junction. Once the stomach is entered, any residual gastric secretions should be suctioned, and air or carbon dioxide is insufflated to improve visualization. The endoscope is then advanced while torquing to the right (see Image. Endoscopy of the Stomach). The endoscope is advanced along the lesser curvature towards the pyloric channel (see Image. Endoscopy of the Antrum). To pass through the pylorus, the endoscope is positioned in front of the pylorus, and insufflation and gentle pressure should be applied against the orifice.
Duodenum
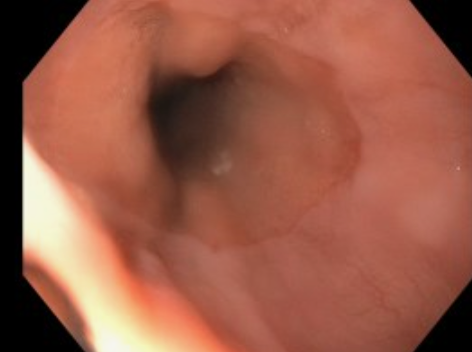
After passing through the pylorus, the endoscope enters the first part of the duodenum (the bulb). The bulb should be examined on endoscope insertion, as passage of the instrument can cause possible mucosal changes (see Image. Endoscopy of the Duodenum). After all 4 quadrants of the bulb are inspected, the scope is advanced to the posterior aspect of the bulb; here, the duodenum turns sharply to the right and then takes a downward course. To enter the second part of the duodenum, the instrument is advanced using the dials and shaft torque, usually down and to the right, followed by an upward spin of the dial.
The distal part of the second portion of the duodenum is reached by straightening the endoscope, in other words, pulling the endoscope slowly backward while maintaining the view of the lumen. This maneuver reduces the loop along the greater curvature of the stomach and, paradoxically, advances the endoscope into the distal duodenum. The duodenum distal to the bulb has distinctive circular rings called valvulae conniventes. The ampulla of Vater (at the major duodenal papilla) is found in the second portion of the duodenum, as is the minor papilla 2 cm proximal to it. They are typically examined during endoscope withdrawal, although they are best visualized with a side-viewing duodenoscope.
After careful examination of the duodenum, pylorus, and antrum, the endoscope is retroflexed to visualize the gastric cardia and fundus. The endoscope is then returned to a neutral position. Once the stomach has been thoroughly inspected and, if necessary, biopsies obtained, the endoscope is withdrawn. Before leaving the stomach, it should be deflated. The esophagus is again examined on withdrawal of the endoscope. The average duration of a diagnostic EGD is 6 to 10 minutes under optimal sedation conditions.
Tissue Sampling
Tissue sampling is obtained from suspicious lesions during EGD. Obtaining biopsies, brushings, or duodenal aspirates from apparently normal-appearing mucosa when pathology is suspected but not macroscopically evident is also appropriate. Examples of this include:
- Barrett's esophagus
- Gastric intestinal metaplasia
- To confirm or rule out celiac or Whipple disease (which may or may not be visually apparent)
- To obtain duodenal biopsies and a duodenal aspirate to look for evidence of Giardiasis or small intestinal bacterial overgrowth
- To obtain a duodenal aspirate for biliary microlithiasis
Specimens obtained include biopsies, mucosal brushings, and polypectomies. Submucosal biopsies are obtained with endoscopic submucosal dissection or by using the tunnel biopsy ("bite-on-bite") technique with standard or jumbo endoscopic biopsy forceps by taking multiple bites directly over one another at the same site. The latter technique improves the diagnostic yield for small lesions such as lipomas and leiomyomas. Specimens are sent for histological, cytological, or microbiological analysis based on the type of the sample and clinical situation.
Third-Space Procedures
Details of the performance of these procedures are beyond the scope of this activity. (Please refer to the Indications section for more information on these procedures.)
Quality Indicators for Esophagogastroduodenoscopy
A joint task force from the ASGE and American College of Gastroenterology (ACG) recently updated the quality indicators for upper gastrointestinal endoscopy (EGD), emphasizing foundational steps across pre-, intra-, and postprocedural phases—including proper indication documentation, thorough photo-documentation, and condition-specific biopsy protocols—with most metrics targeting a success rate of over 98% to ensure consistently high-quality care.[5]
Complications
Complications following EGD are rare, occurring in less than 2% of patients. These could be related to sedation, the endoscopy itself, or complications arising from diagnostic or therapeutic maneuvers.
Sedation-Related Complications
The most frequent and severe complications of sedation are cardiopulmonary; these account for as much as 60% of EGD-related adverse events.[25] These events include hypoxemia, hypoventilation, hypotension, airway obstruction, arrhythmias, and aspiration.[26]
Procedure-Related Complications
The complications following diagnostic EGD include bleeding, perforation, duodenal hematoma, and infection. The risk of bleeding following EGD with biopsy is 0.3%. Bleeding presents with hematemesis or bloody output from the gastrostomy tube. Bleeding following mucosal biopsy can occur as intraluminal hemorrhage or intraluminal hematoma. Duodenal hematoma is an uncommon complication, typically occurring after mucosal biopsies.
Bowel perforation occurs in fewer than 0.3% of cases, and infection is rarely reported. Complications are typically identified within the first 24 hours after the procedure. Perforation is suspected in patients with fever, tachycardia, abdominal pain, or discomfort. An abdominal x-ray should be done to reveal extraluminal air. Conservative therapy with bowel rest and antibiotics is the typical treatment, although some patients might require surgical repair. With ongoing advancement in third-space endoscopy, the risk of adverse events, particularly that of bleeding and perforation, is elevated.[27][28]
Clinical Significance
EGD has become a central component in the diagnosis and management of esophageal, gastric, and small-bowel disorders. Accepted indications include evaluation of dysphagia, gastrointestinal bleeding, peptic ulcer disease, medically refractory gastroesophageal reflux disease, esophageal strictures, celiac disease, and unexplained diarrhea. During EGD, clinicians may obtain diagnostic biopsies while performing therapeutic interventions, eg, hemostasis and dilation, for clinically significant strictures.
When performed according to established standards, EGD remains a safe and well-tolerated procedure. The availability and utilization of EGD in the pediatric population have expanded, reflecting its growing clinical role. Decision-making regarding appropriate indications and optimal timing for EGD in children continues to rely heavily on clinical judgment rather than standardized criteria. Ongoing critical evaluation of pediatric EGD practices remains necessary to optimize diagnostic yield while minimizing procedural risk.
Enhancing Healthcare Team Outcomes
In the context of EGD, an interprofessional team approach is essential to optimize patient-centered care, safety, efficiency, cleanliness of the working area, outcomes, and overall team performance. Physicians, particularly gastroenterologists or surgeons performing the procedure, must demonstrate technical proficiency in scope handling, mucosal inspection, recognition of pathology, and therapeutic interventions, while ensuring adherence to evidence-based quality measures, such as those outlined by the ASGE. Advanced practitioners, including nurse practitioners and physician assistants, play a vital role in preprocedure and postprocedure evaluations, patient education, and follow-up care, helping to streamline care and address patient concerns effectively.
Nurses and endoscopic assistants (technicians) are central to procedural safety through patient preparation, sedation monitoring, and recovery care, and their roles frequently overlap. Their roles include preparing the endoscopy room and equipment, assisting with the management of endoscopes and accessories during procedures, monitoring vital signs (if an anesthesia professional is not present), collecting and managing tissue and fluid specimens, and instrument sterilization. Their role in recognizing early signs of complications and ensuring sterile technique directly impacts patient outcomes. Pharmacists contribute by managing sedation protocols, assessing drug interactions, and advising on periprocedural medication adjustments, especially in patients on antithrombotics or other high-risk medications. Clear communication among team members regarding indications, findings, complications, and follow-up care promotes patient-centered management, minimizes procedural risk, and strengthens overall team performance and quality of care.
Media
(Click Image to Enlarge)
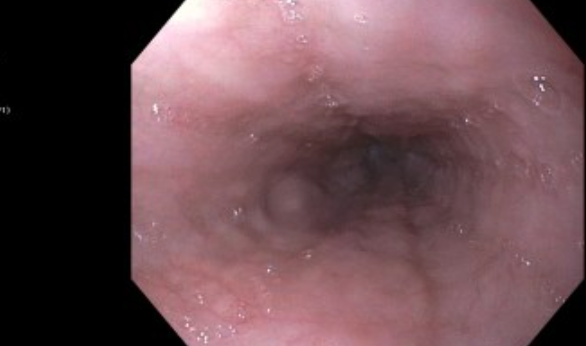
Endoscopy of the Esophagus. Endoscopic image of the esophagus showing smooth, pale-pink mucosa.
Contributed by A Hudgi, MD
(Click Image to Enlarge)
Endoscopy of the Z-Line. The endoscopic image of the gastroesophageal junction, also known as the Z-line, is a sharp, regular line located at the squamocolumnar junction.
Contributed by A Hudgi, MD
(Click Image to Enlarge)

Endoscopy of the Stomach. Endoscopic image of the body of the stomach revealing smooth, pink mucosa with visible rugal folds.
Contributed by A Hudgi, MD
(Click Image to Enlarge)

Endoscopy of the Antrum. Normal endoscopic image of the antrum with smooth and pink mucosa. The pylorus is noted to be round and patent.
Contributed by A Hudgi, MD
(Click Image to Enlarge)

Endoscopy of the Duodenum. Normal endoscopic image of the duodenum, noting velvety mucosa and intact with a normal villous pattern.
Contributed by A Hudgi, MD
(Click Image to Enlarge)
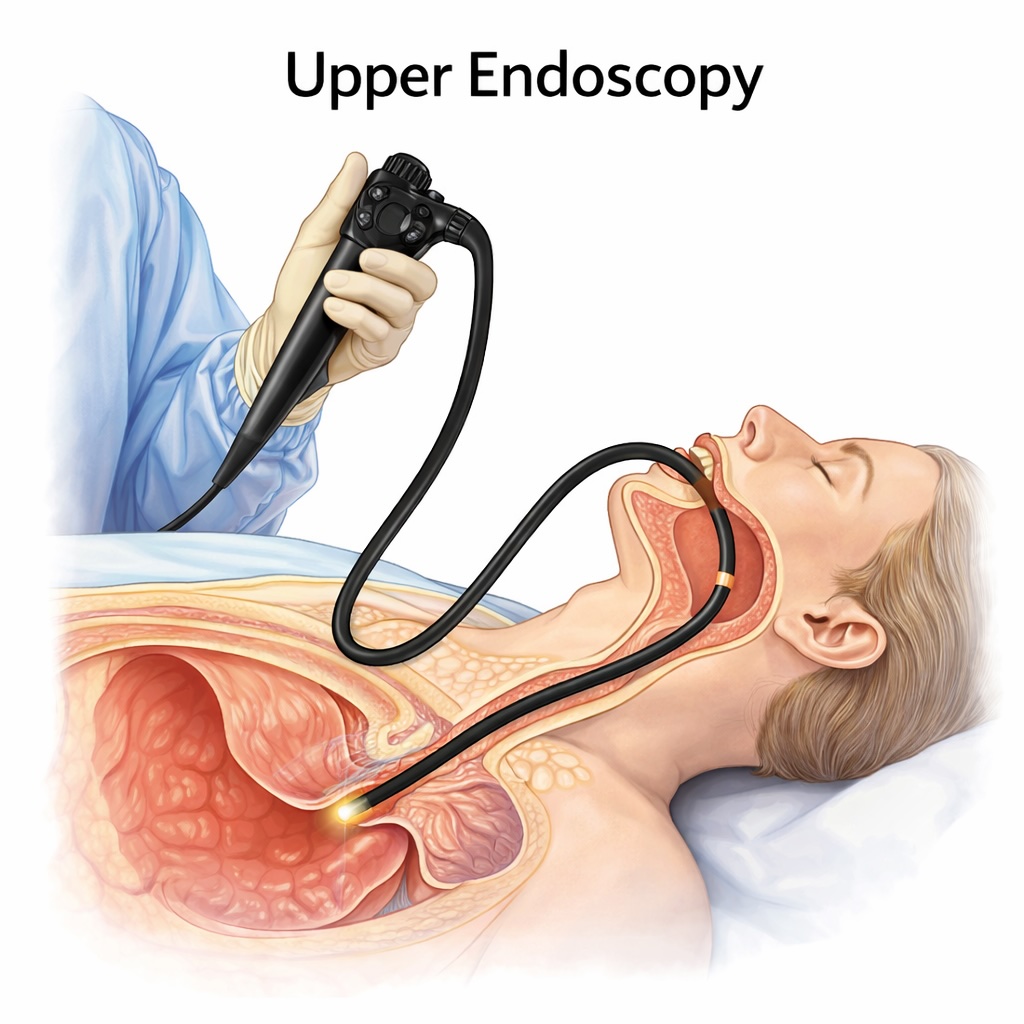
Upper Endoscopy. The image depicts an upper endoscopy in progress, with a flexible endoscope inserted through the patient’s mouth to visualize the esophagus, stomach, and proximal duodenum.
Contributed by StatPearls.
References
Iyer PG, Chak A. Surveillance in Barrett's Esophagus: Challenges, Progress, and Possibilities. Gastroenterology. 2023 Apr:164(5):707-718. doi: 10.1053/j.gastro.2023.01.031. Epub 2023 Feb 4 [PubMed PMID: 36746210]
Morgan DR, Corral JE, Li D, Montgomery EA, Riquelme A, Kim JJ, Sauer B, Shah SC. ACG Clinical Guideline: Diagnosis and Management of Gastric Premalignant Conditions. The American journal of gastroenterology. 2025 Apr 1:120(4):709-737. doi: 10.14309/ajg.0000000000003350. Epub 2025 Mar 12 [PubMed PMID: 40072510]
Khashab MA, Vela MF, Thosani N, Agrawal D, Buxbaum JL, Abbas Fehmi SM, Fishman DS, Gurudu SR, Jamil LH, Jue TL, Kannadath BS, Law JK, Lee JK, Naveed M, Qumseya BJ, Sawhney MS, Yang J, Wani S. ASGE guideline on the management of achalasia. Gastrointestinal endoscopy. 2020 Feb:91(2):213-227.e6. doi: 10.1016/j.gie.2019.04.231. Epub 2019 Dec 13 [PubMed PMID: 31839408]
Rubenstein JH, Sawas T, Wani S, Eluri S, Singh S, Chandar AK, Perumpail RB, Inadomi JM, Thrift AP, Piscoya A, Sultan S, Singh S, Katzka D, Davitkov P. AGA Clinical Practice Guideline on Endoscopic Eradication Therapy of Barrett's Esophagus and Related Neoplasia. Gastroenterology. 2024 Jun:166(6):1020-1055. doi: 10.1053/j.gastro.2024.03.019. Epub [PubMed PMID: 38763697]
Level 1 (high-level) evidenceYadlapati R, Early D, Iyer PG, Morgan DR, Sengupta N, Sharma P, Shaheen NJ. Quality Indicators for Upper GI Endoscopy. The American journal of gastroenterology. 2025 Feb 1:120(2):290-312. doi: 10.14309/ajg.0000000000003252. Epub 2025 Jan 14 [PubMed PMID: 39808581]
Level 2 (mid-level) evidenceNguyen VX, Le Nguyen VT, Nguyen CC. Appropriate use of endoscopy in the diagnosis and treatment of gastrointestinal diseases: up-to-date indications for primary care providers. International journal of general medicine. 2010 Nov 1:3():345-57. doi: 10.2147/IJGM.S14555. Epub 2010 Nov 1 [PubMed PMID: 21116340]
Ahmed K, Rauf SA, Hussain T, Siddiqui A, Ahmed R, Khan NA, Shah HH, Haque MA. Evolving therapeutic approaches in achalasia: a comprehensive review of peroral endoscopic myotomy (POEM) vs. Heller's myotomy. Annals of medicine and surgery (2012). 2025 May:87(5):2855-2867. doi: 10.1097/MS9.0000000000003271. Epub 2025 Apr 10 [PubMed PMID: 40337384]
Dalal I, Andalib I. Advances in endoscopic resection: a review of endoscopic submucosal dissection (ESD), endoscopic full thickness resection (EFTR) and submucosal tunneling endoscopic resection (STER). Translational gastroenterology and hepatology. 2022:7():19. doi: 10.21037/tgh-2020-10. Epub 2022 Apr 25 [PubMed PMID: 35548477]
Level 3 (low-level) evidenceKhashab MA, Wang AY, Cai Q. AGA Clinical Practice Update on Gastric Peroral Endoscopic Myotomy for Gastroparesis: Commentary. Gastroenterology. 2023 Jun:164(7):1329-1335.e1. doi: 10.1053/j.gastro.2023.02.027. Epub 2023 Apr 20 [PubMed PMID: 37086247]
Level 3 (low-level) evidenceDu C, Chai NL, Ling-Hu EQ, Li ZJ, Li LS, Zou JL, Jiang L, Lu ZS, Meng JY, Tang P. Submucosal tunneling endoscopic resection: An effective and safe therapy for upper gastrointestinal submucosal tumors originating from the muscularis propria layer. World journal of gastroenterology. 2019 Jan 14:25(2):245-257. doi: 10.3748/wjg.v25.i2.245. Epub [PubMed PMID: 30670913]
Abraham NS, Barkun AN, Sauer BG, Douketis J, Laine L, Noseworthy PA, Telford JJ, Leontiadis GI. American College of Gastroenterology-Canadian Association of Gastroenterology Clinical Practice Guideline: Management of Anticoagulants and Antiplatelets During Acute Gastrointestinal Bleeding and the Periendoscopic Period. The American journal of gastroenterology. 2022 Apr 1:117(4):542-558. doi: 10.14309/ajg.0000000000001627. Epub [PubMed PMID: 35297395]
Level 1 (high-level) evidenceYang D, Xiao Y, Draganov PV. Novel devices for third-space endoscopy procedures. Digestive endoscopy : official journal of the Japan Gastroenterological Endoscopy Society. 2024 May:36(5):521-532. doi: 10.1111/den.14690. Epub 2023 Oct 25 [PubMed PMID: 37737067]
Chung H. Endoscopic Accessories Used for More Advanced Endoluminal Therapeutic Procedures. Clinical endoscopy. 2017 May:50(3):234-241. doi: 10.5946/ce.2017.079. Epub 2017 May 31 [PubMed PMID: 28609821]
Choi S, El-Hayek K. Endoscopic Equipment-From Simple to Advanced. The Surgical clinics of North America. 2020 Dec:100(6):993-1019. doi: 10.1016/j.suc.2020.08.002. Epub 2020 Oct 10 [PubMed PMID: 33128892]
van der Ploeg K, de Jonge PJF, Lammers WJ, Koch AD, Vos MC, Paulsen V, Aabakken L, Bruno M. Performance of a single-use gastroscope for esophagogastroduodenoscopy: Prospective evaluation. Endoscopy international open. 2024 Mar:12(3):E428-E434. doi: 10.1055/a-2271-2303. Epub 2024 Mar 18 [PubMed PMID: 38504741]
ASGE Standards of Practice Committee, Early DS, Lightdale JR, Vargo JJ 2nd, Acosta RD, Chandrasekhara V, Chathadi KV, Evans JA, Fisher DA, Fonkalsrud L, Hwang JH, Khashab MA, Muthusamy VR, Pasha SF, Saltzman JR, Shergill AK, Cash BD, DeWitt JM. Guidelines for sedation and anesthesia in GI endoscopy. Gastrointestinal endoscopy. 2018 Feb:87(2):327-337. doi: 10.1016/j.gie.2017.07.018. Epub 2018 Jan 3 [PubMed PMID: 29306520]
Veitch AM, Vanbiervliet G, Gershlick AH, Boustiere C, Baglin TP, Smith LA, Radaelli F, Knight E, Gralnek IM, Hassan C, Dumonceau JM. Endoscopy in patients on antiplatelet or anticoagulant therapy, including direct oral anticoagulants: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guidelines. Gut. 2016 Mar:65(3):374-89. doi: 10.1136/gutjnl-2015-311110. Epub [PubMed PMID: 26873868]
Veitch AM, Radaelli F, Alikhan R, Dumonceau JM, Eaton D, Jerrome J, Lester W, Nylander D, Thoufeeq M, Vanbiervliet G, Wilkinson JR, Van Hooft JE. Endoscopy in patients on antiplatelet or anticoagulant therapy: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guideline update. Gut. 2021 Sep:70(9):1611-1628. doi: 10.1136/gutjnl-2021-325184. Epub [PubMed PMID: 34362780]
ASGE Standards of Practice Committee, Kohli DR, Abidi WM, Cosgrove N, Machicado JD, Desai M, Forbes N, Marya NB, Thiruvengadam NR, Thosani NC, Alipour O, Ngamruengphong S, Elhanafi SE, Sheth SG, Ruan W, Fang JC, McClave SA, Zvavanjanja RC, Kamel AY, Qumseya BJ. American Society for Gastrointestinal Endoscopy guideline on gastrostomy feeding tubes: summary and recommendations. Gastrointestinal endoscopy. 2025 Jan:101(1):25-35. doi: 10.1016/j.gie.2024.08.044. Epub 2024 Nov 7 [PubMed PMID: 39520459]
ASGE Standards of Practice Committee, Khashab MA, Chithadi KV, Acosta RD, Bruining DH, Chandrasekhara V, Eloubeidi MA, Fanelli RD, Faulx AL, Fonkalsrud L, Lightdale JR, Muthusamy VR, Pasha SF, Saltzman JR, Shaukat A, Wang A, Cash BD. Antibiotic prophylaxis for GI endoscopy. Gastrointestinal endoscopy. 2015 Jan:81(1):81-9. doi: 10.1016/j.gie.2014.08.008. Epub 2014 Nov 11 [PubMed PMID: 25442089]
Kang SH, Hyun JJ. Preparation and patient evaluation for safe gastrointestinal endoscopy. Clinical endoscopy. 2013 May:46(3):212-8. doi: 10.5946/ce.2013.46.3.212. Epub 2013 May 31 [PubMed PMID: 23767028]
Dossa F, Megetto O, Yakubu M, Zhang DDQ, Baxter NN. Sedation practices for routine gastrointestinal endoscopy: a systematic review of recommendations. BMC gastroenterology. 2021 Jan 7:21(1):22. doi: 10.1186/s12876-020-01561-z. Epub 2021 Jan 7 [PubMed PMID: 33413147]
Level 1 (high-level) evidenceSidhu R, Turnbull D, Haboubi H, Leeds JS, Healey C, Hebbar S, Collins P, Jones W, Peerally MF, Brogden S, Neilson LJ, Nayar M, Gath J, Foulkes G, Trudgill NJ, Penman I. British Society of Gastroenterology guidelines on sedation in gastrointestinal endoscopy. Gut. 2024 Jan 5:73(2):219-245. doi: 10.1136/gutjnl-2023-330396. Epub 2024 Jan 5 [PubMed PMID: 37816587]
Cherciu Harbiyeli IF, Burtea DE, Serbanescu MS, Nicolau CD, Saftoiu A. Implementation of a Customized Safety Checklist in Gastrointestinal Endoscopy and the Importance of Team Time Out-A Dual-Center Pilot Study. Medicina (Kaunas, Lithuania). 2023 Jun 16:59(6):. doi: 10.3390/medicina59061160. Epub 2023 Jun 16 [PubMed PMID: 37374363]
Level 3 (low-level) evidenceASGE Standards of Practice Committee, Ben-Menachem T, Decker GA, Early DS, Evans J, Fanelli RD, Fisher DA, Fisher L, Fukami N, Hwang JH, Ikenberry SO, Jain R, Jue TL, Khan KM, Krinsky ML, Malpas PM, Maple JT, Sharaf RN, Dominitz JA, Cash BD. Adverse events of upper GI endoscopy. Gastrointestinal endoscopy. 2012 Oct:76(4):707-18. doi: 10.1016/j.gie.2012.03.252. Epub [PubMed PMID: 22985638]
Amornyotin S. Sedation-related complications in gastrointestinal endoscopy. World journal of gastrointestinal endoscopy. 2013 Nov 16:5(11):527-33. doi: 10.4253/wjge.v5.i11.527. Epub [PubMed PMID: 24255744]
Jang JM, Park SB, Yoon JY, Kwak MS, Cha JM. Gastrointestinal and non-gastrointestinal complication rates associated with diagnostic esophagogastroduodenoscopy under sedation. Medicine. 2022 May 13:101(19):e29266. doi: 10.1097/MD.0000000000029266. Epub 2022 May 13 [PubMed PMID: 35583537]
Waddingham W, Kamran U, Kumar B, Trudgill NJ, Tsiamoulos ZP, Banks M. Complications of diagnostic upper Gastrointestinal endoscopy: common and rare - recognition, assessment and management. BMJ open gastroenterology. 2022 Dec:9(1):. doi: 10.1136/bmjgast-2021-000688. Epub [PubMed PMID: 36572454]