Introduction
An esophageal hematoma, also known as an intramural hematoma of the esophagus, is a rare manifestation of acute mucosal or submucosal injury, resulting in a blood collection between tissue layers. The condition can occur spontaneously or secondary to trauma from a foreign body, ingestion of toxic substances, or iatrogenic interventions. Patients may present with nonspecific symptoms that mimic acute cardiopulmonary disease or other esophageal conditions. The classic triad of symptoms associated with esophageal hematomas includes acute chest pain, odynophagia or dysphagia, and hematemesis.[1][2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The proposed mechanism involves a rapid alteration in intrathoracic and intraesophageal pressures triggered by events such as vomiting, retching, and coughing, leading to the formation of an intramural hematoma that may rupture into the esophageal lumen. Additional risk factors include the use of anticoagulant or antiplatelet medications and an underlying coagulopathy. In certain cases, esophageal hematomas can occur spontaneously without an identifiable cause.[4][5] Secondary causes of esophageal hematomas include:
- Traumatic ingestion of foreign bodies
- Valsalva maneuver
- Nasogastric tube insertion
- Endotracheal intubation [7]
- Upper gastrointestinal tract endoscopy procedures, including esophagogastroduodenoscopy, esophageal forceps biopsies,[8] endoscopic retrograde cholangiopancreatography,[7] and transesophageal echocardiography [7]
Epidemiology
Esophageal traumatic injuries, including traumatic penetration and perforation, are rare and unpredictable, making the incidence and prevalence of esophageal hematomas difficult to estimate.[9] Most cases are reported in case reports. Results from a large case series showed a bimodal age distribution of esophageal hematomas, with peaks at ages 45 and 75.[10] The younger mode is usually associated with vomiting or trauma, whereas the latter mode appears to be related to either a coagulopathy or the use of anticoagulant or antiplatelet medications.
Esophageal hematomas are approximately twice as common in women as in men for reasons not yet understood. Patients with underlying coagulopathic disorders, such as hemophilia, or those taking antiplatelet or anticoagulant medications, are at a higher risk of developing both spontaneous and secondary esophageal hematomas.[11] Although esophageal hematoma is rare, its recognition is increasing due to the widespread availability of modern endoscopic and radiologic facilities.[12][13]
Pathophysiology
In patients with normal blood clotting, retching or vomiting can lead to a submucosal hematoma, typically in the lower esophagus. Hematoma formation suggests that vomiting-induced pressure can damage the mucosa and submucosal vessels. In one reported case, the esophageal submucosal hematoma was located on the right anterior wall of the distal esophagus, an area prone to increased intra-abdominal pressure. Initially, the hematoma formed in the lower esophagus, likely due to a mucosal laceration, leading to bleeding and local vascular collapse. Bleeding from ruptured submucosal vessels likely extended into the upper esophagus, resulting in a widespread esophageal submucosal hematoma.[14]
A sudden pressure change in the esophagus and an underlying bleeding tendency have been proposed as mechanisms of a spontaneous esophageal hematoma. Secondary esophageal hematomas are thought to result from an acute injury with mechanisms similar to those of a Mallory-Weiss tear and Boerhaave syndrome, with the intramural hematoma representing an intermediate stage. The proposed initiating cause of this condition is sudden bleeding between the mucosa and muscularis propria of the esophageal wall, sometimes involving a long segment of the esophagus. Progressive submucosal dissection from bleeding leads to symptoms ranging from severe chest or upper abdominal pain to signs of esophageal luminal obstruction. Later, a breach of the mucosa containing the hematoma can occur, presenting as hematemesis.[10]
History and Physical
An esophageal hematoma usually presents with sudden-onset chest or retrosternal pain. At least half of patients present with at least 2 symptoms from the classic triads,[15] including retrosternal chest pain (66% to 84%), dysphagia or odynophagia (70%), and hematemesis (26%).[16] When taking the patient’s history, clinicians should inquire about any bleeding diathesis or use of anticoagulants.
A history of violent retching, vomiting, or esophageal instrumentation may also be present, and the patient may experience upper abdominal pain rather than chest pain. Rarely, a history of foreign body ingestion may be present. The presence of dysphagia or odynophagia makes significant cardiac causes of retrosternal pain less likely.[16] Physical examination typically reveals only nonspecific findings, such as tachycardia, hypotension, and pallor.
Evaluation
Multiple modalities have been used to diagnose this condition.[17] The preferred primary investigation is a contrast computed tomography (CT) scan of the chest (with or without the abdomen).[6] A contrast-enhanced CT scan delineates the anatomical relationship between the esophagus, aorta, and mediastinal structures.
The study often demonstrates a thickened esophageal wall with a smooth filling defect within the esophageal lumen. Luminal compression or, in cases of large hematomas, luminal obliteration may be demonstrated. Imaging with oral contrast should be performed when transmural perforation is suspected. Extraluminal extravasation of oral contrast is diagnostic and can localize the mucosal rent. An intraesophageal mass or filling defect may be visualized, sometimes resembling a double-barreled or dual lumen.
MRI can show a mass of intermediate density on T1- and T2-weighted images, distinguishing an esophageal hematoma from other mediastinal pathologies and demonstrating soft tissue planes around the aorta. Endoscopic modalities, such as esophagogastroduodenoscopy and endoscopic ultrasonography, can help diagnose an esophageal hematoma. Endoscopy should be postponed until the integrity of the esophageal wall has been established. Endoscopy reveals a bluish prominence with or without a mucosal tear. Endoscopic ultrasonography is superior to conventional endoscopy because it can demonstrate submucosal lesions and evaluate adjacent structures.
An electrocardiogram, chest radiograph, and cardiac markers are useful in excluding cardiopulmonary diseases that might be mistaken for an esophageal hematoma. The presence of a pneumothorax, pneumomediastinum, or pleural effusion should raise a strong suspicion of a transmural injury to the esophagus and an intramural hematoma. Grading of the degree of luminal involvement by the hematoma is as follows:
- Stage I: Isolated hematoma
- Stage II: Hematoma surrounded by tissue edema
- Stage III: Hematoma causing compression of the esophageal lumen
- Stage IV: Complete obliteration of the esophageal lumen by the hematoma [15]
Treatment / Management
Treatment for esophageal hematomas is usually conservative. Initial treatment involves withholding oral intake, administering intravenous fluids and a proton pump inhibitor, and correcting any associated coagulopathy. Serial CT scans or contrast swallow studies are needed to monitor clinical progress and hematoma resolution. The patient is gradually allowed oral feeding as symptoms improve. In most cases, medical and conservative treatment results in complete patient recovery. This method is suitable for cases in which the muscle layer is unaffected. The hematoma can be absorbed within 1 to 3 weeks, with complete resolution in 2 to 4 weeks.[18] (see Image. Progression and Healing Stages of an Esophageal Hematoma).(A1)
Recurrent bleeding or increased dysphagia should raise suspicion for hematoma leakage into the esophageal lumen or obstruction by an expanding unruptured hematoma, respectively. These situations should be treated as acute emergencies, with hemodynamic resuscitation and airway protection.[5][19] An endoscopic needle knife can be used to incise an obstructing hematoma, allowing drainage.[20] Therapeutic angiography may become necessary in cases of recurrent massive hematemesis to stop bleeding and hematoma expansion via transarterial embolization.[18] A thoracoscopic or open surgical procedure is rarely required and is usually performed only as an emergency in cases of full-thickness perforation.[21](A1)
Differential Diagnosis
Other esophageal etiologies include the following:
- Mallory-Weiss syndrome, a distal esophageal or gastric cardia mucosal tear
- Boerhaave syndrome a transmural esophageal perforation
- Aortoesophageal fistula
- Esophageal variceal rupture
- Esophageal cancer
An esophageal hematoma can be considered an intermediate stage between Mallory-Weiss syndrome and Boerhaave syndrome. Chest radiography may reveal pneumomediastinum, pneumothorax, or pleural effusion in cases of Boerhaave syndrome.
Acute retrosternal chest pain has a cardiopulmonary differential diagnosis, including the following:
- Myocardial infarction
- Aortic dissection
- Pulmonary embolism
Hematemesis, dysphagia, or odynophagia in patients with an esophageal hematoma can help differentiate this condition from other critical conditions when used alongside other diagnostic modalities.[22]
Prognosis
Esophageal hematomas have a generally favorable prognosis when managed promptly and appropriately. Most patients fully recover with conservative treatment, including rest, pain control, and dietary modifications. Patients typically experience significant symptom relief within days to weeks, and the hematoma usually resolves completely within a few weeks. However, clinicians should monitor for signs of deterioration, especially in patients with underlying risk factors or comorbidities. Full-thickness perforation is associated with higher morbidity and mortality.
Complications
Although rare, complications of an esophageal hematoma can be severe and require prompt attention.
The most common complications include:
- Intraluminal bleeding secondary to rupture of the hematoma into the esophageal lumen
- Expansion of the hematoma, causing esophageal luminal obstruction (signaled by progressive dysphagia)
- The most significant complication is esophageal perforation, which can lead to mediastinitis and sepsis and necessitate surgical intervention
Less frequent potential complications include:
- Secondary infection of the hematoma
- Stricture formation due to scar tissue
- Rebleeding, especially in patients with underlying coagulopathies or those taking anticoagulant or antiplatelet therapy
- Aspiration of blood or necrotic tissue into the lungs [23]
Consultations
Patients with an esophageal hematoma often require interdisciplinary consultations to ensure comprehensive treatment and optimal outcomes. A gastroenterologist should be consulted for diagnostic evaluation and endoscopic treatment. Consultation with a cardiothoracic surgeon is essential if there is concern for esophageal perforation or other complications that may require intervention.
The expertise of a radiologist is crucial for interpreting imaging studies such as CT scans and MRI, and for performing angiography when indicated. If the patient has a coagulopathy or is taking anticoagulant or antiplatelet therapy, a hematologist should be consulted. Nurses and dietitians can provide the patient with information about dietary restrictions during recovery.
Deterrence and Patient Education
Patients with an esophageal hematoma must adhere to dietary restrictions and undergo serial imaging follow-up to prevent complications. Clinicians should educate patients about symptoms such as dysphagia, hematemesis, or melena to promote prompt diagnosis of complications. Efforts should be directed toward avoiding activities that can increase intraesophageal pressure or cause trauma, such as Valsalva maneuvers, including heavy lifting, strenuous coughing, and abrupt swallowing of large food boluses, which can exacerbate symptoms and cause complications. Patients taking antiplatelet or anticoagulant medications for other reasons should closely follow up with clinicians regarding the safe resumption of these medications.
Pearls and Other Issues
An esophageal hematoma is a rare but potentially serious acute condition, most often observed in individuals who have undergone esophageal instrumentation, experienced traumatic mucosal injury, or are taking anticoagulants or antiplatelet drugs, although spontaneous cases can also occur. With an aging population at increased cardiovascular risk and increased use of anticoagulants and antiplatelet agents, early recognition and diagnosis of esophageal hematomas are crucial. Misdiagnosing an esophageal hematoma as a cardiopulmonary condition can lead to dangerous complications, particularly if anticoagulation or thrombolytic therapy is administered inappropriately. Accurate diagnosis and appropriate treatment are essential to prevent such outcomes.
Enhancing Healthcare Team Outcomes
Effective treatment of an esophageal hematoma requires a collaborative, interprofessional approach to ensure patient-centered care, enhance outcomes, and promote patient safety. Each healthcare professional plays a critical role, contributing unique skills and perspectives to the team. Clinicians and advanced practice clinicians must possess strong diagnostic skills to promptly identify esophageal hematomas and interpret imaging studies and endoscopic findings. Nurses play a vital role in patient care by closely monitoring vital signs, administering medications, and providing patient education and support. Pharmacists are crucial in treating anticoagulation therapy and recommending alternatives to prevent exacerbation of the condition.[24][25]
Coordinated care involving gastroenterologists, surgeons, radiologists, hematologists, dietitians, and pain treatment specialists is crucial for the comprehensive treatment of this condition. Implementing evidence-based treatment strategies and protocols ensures consistent and effective care. This collaborative approach facilitates timely interventions, continuity of care, and thorough follow-up. Regular training, simulations, and debriefings optimize team performance to address challenges and improve protocols, a critical need given the rarity of this condition. Interprofessional problem-solving and decision-making within the health care team can enhance overall performance and patient care for individuals with esophageal hematomas.
Media
(Click Image to Enlarge)
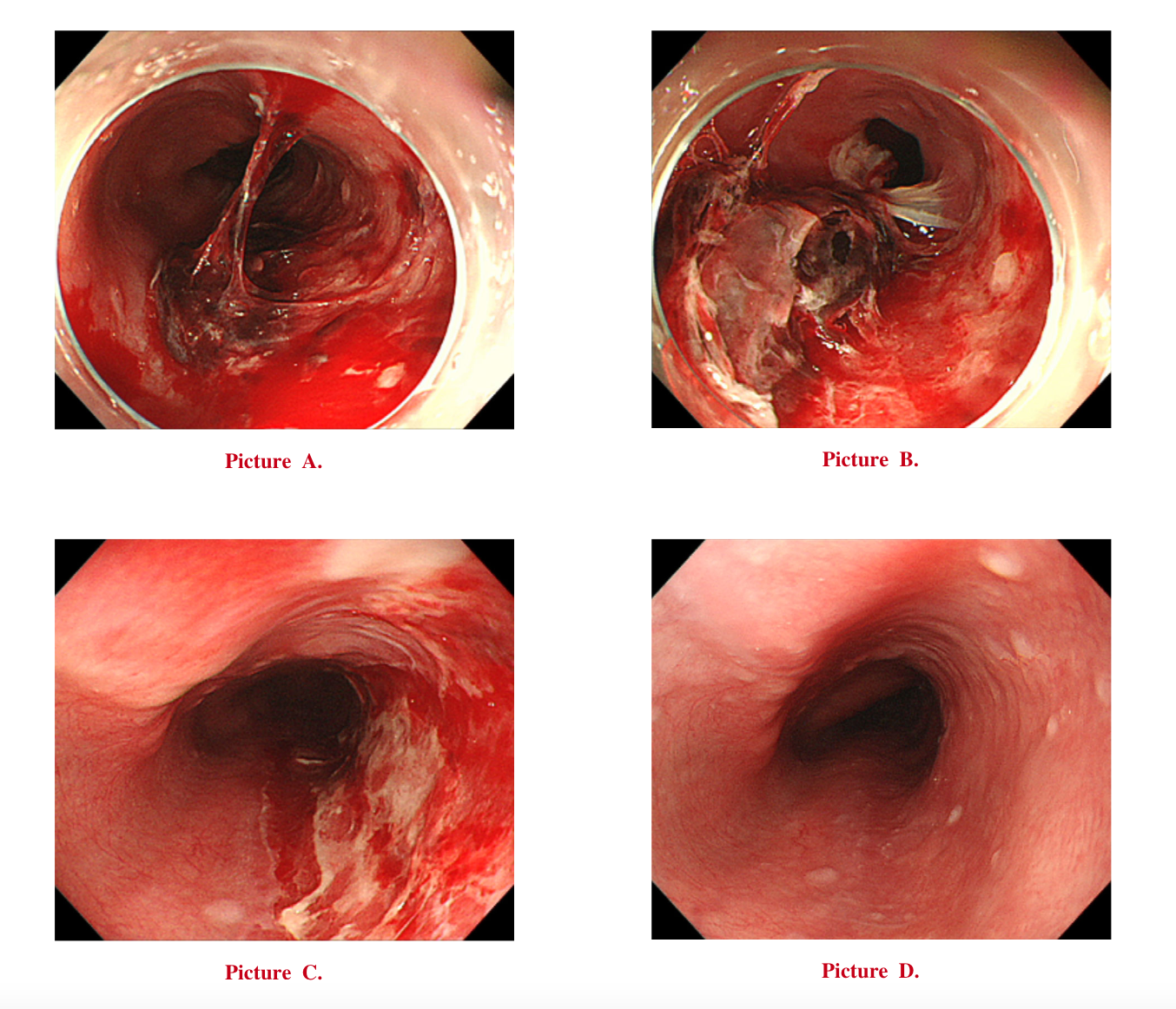
Progression and Healing Stages of Esophageal Hematoma. Images A to D demonstrate the progression of an esophageal hematoma and its subsequent healing stages.
Contributed by Y Hamada, MD
References
Yamada T, Motomura Y, Hiraoka E, Miyagaki A, Sato J. Nasogastric Tubes Can Cause Intramural Hematoma of the Esophagus. The American journal of case reports. 2019 Feb 20:20():224-227. doi: 10.12659/AJCR.914133. Epub 2019 Feb 20 [PubMed PMID: 30783075]
Level 3 (low-level) evidenceMandavdhare HS, Gupta P, Maity P, Sharma V. Image Diagnosis: Esophageal Intramural Hematoma in Sudden-Onset Chest Pain and Dysphagia. The Permanente journal. 2018:23():18-141. doi: 10.7812/TPP/18-141. Epub [PubMed PMID: 30589409]
Chu L, Yang JS, Yu KX, Chen CM, Hao DJ, Deng ZL. Usage of Bone Wax to Facilitate Percutaneous Endoscopic Cervical Discectomy Via Anterior Transcorporeal Approach for Cervical Intervertebral Disc Herniation. World neurosurgery. 2018 Oct:118():102-108. doi: 10.1016/j.wneu.2018.07.070. Epub 2018 Jul 17 [PubMed PMID: 30026139]
Hamada Y, Aota T, Nakagawa H. Intramural Esophageal Hematoma. Internal medicine (Tokyo, Japan). 2024 Oct 1:63(19):2711-2712. doi: 10.2169/internalmedicine.3117-23. Epub 2024 Mar 4 [PubMed PMID: 38432958]
Malhi NS, Grover R, Dhingra JS, Singla N. "Spontaneous Intramural Esophageal Hematoma Associated with Uncontrolled Hypertension: Case Report and Review". International medical case reports journal. 2025:18():1611-1617. doi: 10.2147/IMCRJ.S564041. Epub 2025 Dec 13 [PubMed PMID: 41424750]
Level 3 (low-level) evidenceLei J, Wu L. Esophageal Hematoma After Severe Vomiting. Cureus. 2024 Nov:16(11):e74392. doi: 10.7759/cureus.74392. Epub 2024 Nov 25 [PubMed PMID: 39723264]
Cao DT, Reny JL, Lanthier N, Frossard JL. Intramural hematoma of the esophagus. Case reports in gastroenterology. 2012 May:6(2):510-7. doi: 10.1159/000341808. Epub 2012 Jul 26 [PubMed PMID: 23730267]
Level 3 (low-level) evidenceJeong ES, Kim MJ, Yoo SH, Kim DH, Jung JS, Koo NH, Chang SH. Intramural hematoma of the esophagus after endoscopic pinch biopsy. Clinical endoscopy. 2012 Nov:45(4):417-20. doi: 10.5946/ce.2012.45.4.417. Epub 2012 Nov 30 [PubMed PMID: 23251891]
Ribeiro T, Mascarenhas Saraiva M, Afonso J, Brozzi L, Macedo G. Predicting Factors of Clinical Outcomes in Patients Hospitalized after Esophageal Foreign Body or Caustic Injuries: The Experience of a Tertiary Center. Diagnostics (Basel, Switzerland). 2023 Oct 25:13(21):. doi: 10.3390/diagnostics13213304. Epub 2023 Oct 25 [PubMed PMID: 37958198]
Level 2 (mid-level) evidenceCullen SN, McIntyre AS. Dissecting intramural haematoma of the oesophagus. European journal of gastroenterology & hepatology. 2000 Oct:12(10):1151-62 [PubMed PMID: 11057463]
Sugimura K, Ishii N. Esophageal Hematoma Mimicking a Large Esophageal Polyp: A Diagnostic Clue of Acquired Hemophilia A. Mayo Clinic proceedings. 2019 Oct:94(10):2142-2143. doi: 10.1016/j.mayocp.2019.04.024. Epub [PubMed PMID: 31585586]
Ito S, Iwata S, Kondo I, Iwade M, Ozaki M, Ishikawa T, Kawamata T. Esophageal submucosal hematoma developed after endovascular surgery for unruptured cerebral aneurysm under general anesthesia: a case report. JA clinical reports. 2017:3(1):54. doi: 10.1186/s40981-017-0124-3. Epub 2017 Oct 3 [PubMed PMID: 29457098]
Level 3 (low-level) evidenceRandhawa MS, Rai MP, Dhar G, Bandi A. Large oesophageal haematoma as a result of transoesophageal echocardiogram (TEE). BMJ case reports. 2017 Nov 8:2017():. pii: bcr-2017-223278. doi: 10.1136/bcr-2017-223278. Epub 2017 Nov 8 [PubMed PMID: 29122910]
Level 3 (low-level) evidenceKanamori A, Nadatani Y, Kushiyama N, Nakata A, Higashimori A, Ominami M, Kimura T, Fukumoto S, Fujiwara Y, Watanabe T. Esophageal submucosal hematoma during transnasal endoscopy: A rare case report. DEN open. 2024 Apr:4(1):e366. doi: 10.1002/deo2.366. Epub 2024 Apr 15 [PubMed PMID: 38628503]
Level 3 (low-level) evidenceOuatu-Lascar R, Bharadhwaj G, Triadafilopoulos G. Endoscopic appearance of esophageal hematomas. World journal of gastroenterology. 2000 Apr:6(2):307-309 [PubMed PMID: 11819586]
Long B, Gottlieb M. Emergency medicine updates: Upper gastrointestinal bleeding. The American journal of emergency medicine. 2024 Jul:81():116-123. doi: 10.1016/j.ajem.2024.04.052. Epub 2024 May 3 [PubMed PMID: 38723362]
Gao F, Zhang T, Guo X, Su Z. Embolization of the esophageal branch of intercostal artery for treatment of spontaneous intramural hematoma of the esophagus: a case description. Quantitative imaging in medicine and surgery. 2023 Oct 1:13(10):7417-7422. doi: 10.21037/qims-23-564. Epub 2023 Sep 11 [PubMed PMID: 37869337]
Level 2 (mid-level) evidenceChoi HK, Law S, Chu KM, Wong J. The value of neck drain in esophageal surgery: a randomized trial. Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus. 2017 Nov 1:11(1):40-42. doi: 10.1093/dote/11.1.40. Epub [PubMed PMID: 29040481]
Level 1 (high-level) evidenceNagai T, Torishima R, Nakashima H, Uchida A, Okawara H, Suzuki K, Sato R, Murakami K, Fujioka T. Spontaneous esophageal submucosal hematoma in which the course could be observed endoscopically. Internal medicine (Tokyo, Japan). 2004 Jun:43(6):461-7 [PubMed PMID: 15283180]
Zheng Q, Li M, Zhou Y, Zhao L, Liu J, Liu B. Endoscopic Full Length Mucosa Incision for a Huge Esophageal Hematoma Therapy: The First Clinical Experience. The American journal of gastroenterology. 2022 Nov 1:117(11):1737. doi: 10.14309/ajg.0000000000001849. Epub 2022 Jun 3 [PubMed PMID: 35973154]
Vossler JD, Abdul-Ghani A. Esophageal Hematoma following Acute Esophageal Barotrauma. The American surgeon. 2017 Jun 1:83(6):e213-215 [PubMed PMID: 28637550]
Shim J, Jang JY, Hwangbo Y, Dong SH, Oh JH, Kim HJ, Kim BH, Chang YW, Chang R. Recurrent massive bleeding due to dissecting intramural hematoma of the esophagus: treatment with therapeutic angiography. World journal of gastroenterology. 2009 Nov 7:15(41):5232-5 [PubMed PMID: 19891027]
Level 3 (low-level) evidenceKamphuis AG, Baur CH, Freling NJ. Intramural hematoma of the esophagus: appearance on magnetic resonance imaging. Magnetic resonance imaging. 1995:13(7):1037-42 [PubMed PMID: 8583868]
Level 3 (low-level) evidencePiccione PR, Winkler WP, Baer JW, Kotler DP. Pill-induced intramural esophageal hematoma. JAMA. 1987 Feb 20:257(7):929 [PubMed PMID: 3806873]
Level 3 (low-level) evidenceTrip J, Hamer P, Flint R. Intramural oesophageal haematoma-a rare complication of dabigatran. The New Zealand medical journal. 2017 Jun 2:130(1456):80-82 [PubMed PMID: 28571053]