Introduction
Erb palsy most commonly results from an upper brachial plexus birth injury involving the C5–C6 nerve roots, with occasional extension to C7, leading to flaccid weakness or paralysis of the affected upper extremity. Among neonatal brachial plexus palsy (NBPP) patterns, Erb palsy represents the most common presentation and accounts for approximately 90% of cases. NBPP is the preferred contemporary term and encompasses upper plexus (Erb), lower plexus (Klumpke), and total plexus injuries.
Although birth injury remains the most frequent cause, Erb palsy may also develop in older children and adults following trauma that forcefully increases the angle between the neck and shoulder. Common mechanisms include falls, motor vehicle collisions, sports-related traction injuries, prolonged heavy backpack use, and iatrogenic stretch injuries sustained during surgical procedures. Early recognition and coordinated interprofessional management support optimal functional recovery and improve outcomes for affected infants and their families.[1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Erb palsy results from a birth injury involving the cervical spinal nerves C5 and C6, which form the upper trunk of the brachial plexus. The brachial plexus arises from nerve roots C5 through T1 and is organized into upper (C5–C6), middle (C7), and lower (C8–T1) trunks. The ventral rami of C5 and C6 join to form the upper trunk, which then divides into anterior and posterior divisions that ultimately contribute to the lateral, posterior, and medial cords and terminal peripheral nerves, including the musculocutaneous, axillary, radial, median, and ulnar nerves (see Image. Erb Palsy-Brachial Plexus).[2][3]
The level of plexus involvement classifies neonatal brachial plexus injuries. Erb palsy involves the upper trunk (C5–C6), whereas extended Erb palsy includes C7. Klumpke palsy affects the lower trunk (C8–T1), and total brachial plexus palsy involves the entire plexus from C5 through T1 and is the most severe form.[2][4]
The term NBPP encompasses all injury patterns, including upper-, lower-, and total-plexus palsy. Injury to the upper trunk disrupts motor and sensory function to the shoulder and upper arm and represents the most common pattern of NBPP, accounting for approximately 90% of cases.[5] The typical mechanism of causation is traction on the fetal neck and shoulder during delivery, which stretches the brachial plexus. The strongest associated risk factors for NBPP are shoulder dystocia and fetal macrosomia (birth weight >4000 g).[6] Additional risk factors include maternal diabetes, operative vaginal delivery (vacuum or forceps), abnormal labor patterns (prolonged or precipitous second stage), multiparity, and maternal obesity.[6][4] Although cesarean delivery reduces risk, brachial plexus injury may still occur.[7] Please see StatPearls' companion resource, "Brachial Plexus Injuries," for further information.
However, approximately 50% of NBPP cases occur in otherwise uncomplicated deliveries without identifiable obstetric trauma. Some infants affected by NBPP have a normal birth weight and no recognized intrapartum complications. In such cases, an in utero mechanism has also been proposed, supported by findings, eg, muscle atrophy and osseous demineralization of the affected extremity.[8][9]
Epidemiology
The pooled global incidence of NBPP is approximately 1.74 per 1,000 live births, based on a systematic review of 22 studies encompassing more than 29 million births.[6] In the United States, the reported incidence has declined over time, from about 1.7 per 1,000 live births in 1997 to 0.9 to 1.1 per 1,000 in more recent series, with rates largely plateauing.[7][10] Similar declines have been observed internationally, including a reduction in Germany from 0.28 to 0.15 per 1,000 live births between 2005 and 2018 and in Sweden from 3.1 to 1.0 per 1,000 vaginal cephalic deliveries between 1997 and 2019.[11][12]
In the United States, an estimated 5,000 cases of NBPP occur annually, with approximately 580 to 1,050 resulting in permanent deficits.[13] Erb palsy, the most common subtype involving the upper brachial plexus, has been reported to have an incidence of approximately 0.9 to 2.6 per 1,000 live births.[12]
Temporal trends in NBPP incidence closely parallel changes in obstetric practice, particularly the rise in cesarean delivery rates. Cesarean delivery is consistently associated with a reduced risk of NBPP (OR 0.13–0.16), with the strongest protective effect observed among macrosomic infants.[6][7][10] Despite this association, NBPP has also declined in settings where shoulder dystocia rates have risen, suggesting that improved intrapartum management may also contribute to lower injury rates.[12]
Pathophysiology
NBPP results from a traction injury to the brachial plexus during childbirth. The classic mechanism occurs during shoulder dystocia, an obstetric emergency in which the fetal anterior shoulder becomes impacted behind the maternal pubic symphysis after delivery of the head. Attempts to deliver the infant may place traction on the neck and shoulder, stretching the upper brachial plexus, particularly the C5–C6 nerve roots.[14] Fetal macrosomia is a major risk factor for shoulder dystocia and subsequent brachial plexus injury. However, approximately half of NBPP cases occur without clinically recognized shoulder dystocia, suggesting that the pathophysiology is more complex than that explained by clinician-applied traction alone.
Both endogenous and exogenous forces may contribute to injury. Endogenous maternal forces, including uterine contractions and maternal pushing, may generate sufficient traction on the brachial plexus even in the absence of obstetric maneuvers.[14] In some infants, anatomic factors such as cervical ribs, aberrant scalene muscle attachments, or variant plexus branching patterns may increase susceptibility to injury by narrowing the supraclavicular space and lowering the threshold for nerve stretch injury.[15]
The severity of nerve injury ranges from mild stretch injury to complete nerve root avulsion.[4] Neuropraxia is the mildest form and results from transient nerve stretching with intact axonal integrity; recovery is typically spontaneous and complete. Axonotmesis involves the disruption of the axon while preserving the surrounding connective tissue structures, and recovery may take several months. Neurotmesis, including nerve root avulsion, represents complete disruption of the nerve and carries the worst prognosis.[16]
History and Physical
Clinical History
The birth history is central to the evaluation of infants with Erb palsy. Important historical features include the mode of delivery (vaginal versus cesarean), occurrence of shoulder dystocia, use of vacuum or forceps assistance, prolonged or augmented labor, fetal presentation, and birth weight.[5][17] Shoulder dystocia is the strongest recognized risk factor, and fetal macrosomia, maternal diabetes, instrumental delivery, and breech presentation are also associated with increased risk. However, many affected infants are born after otherwise uncomplicated deliveries without identifiable obstetric risk factors.[17]
Erb palsy is typically recognized shortly after birth due to asymmetric upper-extremity movement. Parents may report decreased spontaneous movement of 1 arm, or nurses may notice an asymmetric Moro reflex with preservation of hand grasp. The timing and circumstances surrounding the recognition of weakness should be documented carefully, as they may have prognostic and medicolegal significance.[18]
Clinical evaluation should include an inquiry into associated findings that suggest a more extensive injury. Respiratory difficulty may indicate phrenic nerve involvement with diaphragmatic paralysis, whereas ptosis and miosis may suggest Horner syndrome from sympathetic chain injury.[19][20] Historical features associated with persistent deficits and incomplete spontaneous recovery include cephalic presentation, induction or augmentation of labor, birth weight greater than 4 kg, and associated clavicular fracture.[5]
Physical Examination
The hallmark physical examination finding in Erb palsy is asymmetric upper-extremity weakness, with impaired active range of motion but preserved passive range of motion in the affected limb. Physical examination remains the cornerstone of diagnosis.[5] Infants with Erb palsy classically hold the affected arm in the "waiter's tip" position, characterized by shoulder adduction and internal rotation, elbow extension, forearm pronation, and wrist flexion.[19][21]
These findings reflect weakness of muscles innervated by the C5–C6 roots, including the deltoid, supraspinatus, infraspinatus, biceps, and brachialis. The Moro reflex is typically absent or asymmetric on the affected side, whereas the grasp reflex remains intact because C8–T1 function is preserved in isolated upper plexus injuries.[19] The biceps reflex is also absent on the affected side. In extended Erb palsy involving C7, additional weakness of elbow, wrist, and finger extension may be present. The affected arm may appear limp with diminished spontaneous movement.[22]
A comprehensive neuromuscular examination should assess posture, spontaneous movement, muscle strength, reflexes, and active and passive range of motion. The contralateral extremity should also be examined to exclude bilateral involvement.[23] The examination should assess for findings suggestive of more severe injury or nerve root avulsion. Ptosis and miosis indicate Horner syndrome due to sympathetic chain involvement and are associated with a poorer prognosis.[19] Asymmetric chest expansion or respiratory distress may indicate phrenic nerve injury and hemidiaphragm paralysis.[20]Scapular winging suggests long thoracic nerve involvement. The infant should also be evaluated for associated perinatal clavicular fractures or shoulder dislocations, as well as joint contractures and subluxations that may develop over months.[20][5]
Evaluation
Erb palsy is a clinical diagnosis, and serial physical examinations remain the cornerstone of evaluation. The goals of assessment are to localize the neurologic injury, determine the severity, identify associated injuries, and monitor for spontaneous recovery.[5] Evaluation includes a detailed neuromuscular examination, assessing posture, spontaneous movement, reflexes, strength, and active and passive range of motion (see Image. Erb Palsy Physical Examination). Associated findings, eg, Horner syndrome, asymmetric chest expansion due to phrenic nerve involvement, clavicular fracture, shoulder dislocation, and early joint contractures, should also be evaluated.[18][5]
Several functional assessment tools aid in evaluating and predicting recovery.[5] The Active Movement Scale (AMS) is commonly used to quantify upper extremity movement in infants. At approximately 3 months of age, the Toronto Test Score may help predict recovery; scores below 3.5 are associated with poor spontaneous recovery and may indicate the need for surgical evaluation. In older infants and children, functional assessments, eg, the cookie test, towel test, and Modified Mallet Classification, may be used to evaluate upper-extremity function.[24]
Chest radiography is recommended to evaluate possible associated clavicular or humeral fractures and diaphragmatic paralysis.[4] Advanced imaging is reserved for suspected severe injury, particularly nerve root avulsion, and for surgical planning.[19][25] Magnetic resonance imaging (MRI), including MR myelography, is generally preferred because it can identify pseudomeningoceles and root avulsions without ionizing radiation or intrathecal contrast.[26] Computed tomography (CT) myelography may also detect nerve root avulsion but requires lumbar puncture, intrathecal contrast, and radiation exposure.[5]
Electrodiagnostic studies, including electromyography and nerve conduction studies, may help characterize the severity and chronicity of injury. However, their utility in neonates is debated because findings may not correlate fully with clinical examination. These studies are not universally considered part of the standard of care, but they may assist with prognostication and surgical decision-making in selected cases.[5]
Treatment / Management
The majority of cases of Erb palsy are managed with supportive care. Recommended treatment includes early physical and occupational therapy with motion active and passive motion exercises.[4][19]
Recovery Assessment
Serial clinical examinations are important for assessing recovery, as nerve injuries of varying severity can present with similar clinical features.[20] Immobilization of the affected limb is not recommended in the absence of a fracture. Family members should be trained to perform passive stretching at home to enhance the effectiveness of therapy. Biceps muscle strength assessment is considered the easiest and most reliable measure of recovery.[19]
Incomplete recovery at 1 month of age correlates with a more severe injury, beyond neuropraxia, and referral should be made to an interprofessional team managing brachial plexus injuries. Early consultation facilitates timely intervention, prevents contractures and deformities, supports recovery monitoring, and provides education for families.[20][27] An interprofessional team, including a physical therapist, an occupational therapist, and a pediatric surgical team (plastic surgeon, orthopedic surgeon, neurosurgeon) for nerve reconstruction, is optimal for comprehensive care.[20][27]
Surgical Management
Approximately 20% to 30% of infants with neonatal brachial plexus palsy are potential candidates for surgical consultation and possible intervention if not improving by 3 to 6 months.[28] Surgical intervention is typically indicated for severe Erb palsy cases that show minimal or no functional recovery despite appropriate physical and occupational therapy. Procedures include nerve grafting and nerve decompression, with nerve grafting generally offering the highest likelihood of functional improvement.[29][30] Postoperative rehabilitation with physical and occupational therapy is a cornerstone of management, aimed at maintaining joint mobility, preventing contractures, and optimizing functional recovery.
Brachial plexus nerve wrapping may improve pain and function in selected patients, but requires further studies to document its benefits.[31] The timing of surgery remains controversial; however, surgery is generally recommended between 3 and 6 months after severe injuries to reduce motor end-plate loss.[19] Other recommendations suggest primary nerve repair between 3 and 12 months of age. A few children require secondary surgical management, eg, tendon transfer, arthrodesis, or osteotomies, in the presence of residual dysfunction following primary repair.[23] (A1)
Ancillary Therapies
Additionally, various complementary techniques exist for treating neonatal brachial plexus palsy, including electrostimulation, botulinum toxin injection, thermoplastic splints, and temporary splints for physiological positioning and to improve motor function.[32] However, the randimized controlled trilas evidence for these techniques is limited, with most interventions supported primarily by retrospective cohort studies, case series, and small trials rather than large, high-quality RCTs.[33][34](A1)
Differential Diagnosis
Erb palsy should be differentiated from other forms of NBPP, eg, lower plexus injuries, eg, Klumpke palsy and total plexus palsy. The following neonatal conditions that cause upper extremity weakness or decreased movement may mimic Erb palsy and should be distinguished from brachial plexus birth injury:
- Klumpke palsy primarily affects the intrinsic muscles of the hand and the flexors of the wrist and fingers, resulting in weakness in the forearm and hand. Affected infants may demonstrate a characteristic "claw hand" deformity caused by an imbalance between the intrinsic and extrinsic hand muscles. Horner syndrome may also be present because of involvement of the T1 sympathetic fibers.
- Clavicular fractures can cause pseudoparalysis, which mimics a brachial plexus injury.
- Cervical ribs can result in Erb palsy due to the nerves stretching around the affected rib.
- Osteomyelitis of the humerus or clavicle can cause brachial plexus injury.
- Septic arthritis of the shoulder can cause brachial plexus injury.
- Arthrogryposis multiplex congenita may present with decreased upper extremity movement and fixed joint contractures that can mimic Erb palsy.
Prognosis
Erb palsy has a favorable prognosis, especially when the affected arm begins to recover within the first month. 80% to 90% of affected infants completely recover within a few months to 1 year.[4] In one study, only 3% had residual longer-term neurological deficits.[35] Although many experience spontaneous recovery, residual weakness of the affected extremity may persist, with functional impairment, skeletal deformities, eg, contractures and limb-length discrepancy, and cosmetic deformities.[36][20]
Surgical intervention for brachial plexus injuries improves functional outcomes, particularly shoulder and elbow mobility.[37] Approximately 10% of infants with NBPP fail to gain functional recovery and may require resection of a neuroma-in-continuity (NIC) and surgical nerve reconstruction.[38] The Narakas classification describes the severity of brachial plexus injury, assessed clinically 2 to 3 weeks after birth, based on nerve root involvement (see Table. Narakas Classification). About 25% of cases are Narakas class III or IV.[39][40][20]
Table. Narakas Classification
| Narakas Classification | Nerve Roots involved | Clinical Features and Prognosis |
| Narakas I | C5, C6 | Best prognosis, with clinical improvement in weeks (>80% spontaneous recovery) |
| Narakas II | C5, C6, and C7 | Function of the hand affected with late recovery (spontaneous recovery in >60%) |
| Narakas III | C5, C6, C7, C8, and T1 | A global/total palsy. Recovery of the shoulder/arm is 30-50%, with hand function present. |
| Narakas IV . | C5, C6, C7, C8, and T1 with Horner syndrome | Most severe, with the worst prognosis. Total palsy with Horner syndrome usually requires surgery. |
Complications
Complications of Erb palsy can be categorized into musculoskeletal, neurologic, growth-related, and psychosocial domains.
Musculoskeletal Complications
Among children with persistent weakness or residual dysfunction, shoulder contractures are common, occurring in approximately half of cases in some series. Glenohumeral dysplasia is the most common secondary skeletal complication and results from chronic muscle imbalance, in which unopposed internal rotators overpower weakened external rotators. This imbalance leads to posterior humeral head subluxation and progressive glenoid deformity. Osseous deformities are reported in approximately one-third of cases and may occur even in children with substantial neurologic recovery. The Mallet classification system is commonly used to assess and monitor shoulder function in older children, particularly for abnormalities in abduction and external rotation.[41][42][43]
Other musculoskeletal sequelae include elbow flexion contractures and forearm supination deformities, which may become fixed over time due to persistent imbalance of agonist and antagonist muscle groups. Limb length discrepancy and muscle atrophy may also develop secondary to impaired innervation, with reduced muscle growth and fatty degeneration affecting the involved extremity.[44][45]
Neurologic Complications
Aberrant reinnervation may cause co-contraction, in which opposing muscles activate simultaneously, leading to stiff, poorly coordinated movement and a limited range of motion that often does not improve with therapy alone.[46] If reinnervation is delayed, irreversible muscle changes can occur within 12 to 24 months, after which meaningful recovery is unlikely even with surgery.[5]
Psychosocial and Developmental Complications
Persistent weakness can significantly impact the quality of life in affected children.[44][45] One multicenter study demonstrated reduced health-related quality of life compared with the general population, with psychosocial factors and pain playing a larger role than physical impairment. Emotional functioning, peer relationships, and family dynamics were strongly associated with better outcomes, whereas pain interference and stigma were associated with worse quality of life.[47]
Children with a history of unresolved NBPP may also demonstrate higher rates of internalizing and externalizing behavioral problems, and caregivers may experience increased psychological distress. In addition, gross motor developmental milestones, eg, head control, midline crossing, and rolling may be delayed, with the severity of delay correlating with the extent of nerve injury.[48]
Deterrence and Patient Education
Early recognition and management of Erb palsy are important for optimizing functional recovery and minimizing long-term complications. Prenatal counseling and appropriate glycemic control in pregnant patients with diabetes may help reduce the risk of fetal macrosomia, shoulder dystocia, and associated brachial plexus birth injuries. Parents and caregivers should receive education regarding the clinical presentation, expected course of recovery, therapeutic exercises, prognosis, and available treatment options, including indications for surgical evaluation in persistent or severe cases. Families may also experience significant emotional distress and benefit from psychosocial support. Interprofessional brachial plexus clinics that include physicians, therapists, social workers, and psychologists can provide comprehensive family-centered care and improve coordination of rehabilitation and long-term follow-up.[19]
Enhancing Healthcare Team Outcomes
Optimal management of Erb palsy requires coordinated interprofessional care focused on early recognition, timely intervention, rehabilitation, and long-term follow-up to improve functional outcomes and reduce disability. Neonatologists, pediatricians, nurses, and primary care clinicians play key roles in early identification through careful newborn examination and recognition of asymmetric arm movement, abnormal reflexes, or weakness after delivery. Nurses are often among the first healthcare professionals to recognize impaired upper extremity movement or parental concerns during the neonatal period and are essential in facilitating prompt evaluation and referral.
Pediatricians and primary care clinicians coordinate longitudinal care, perform serial neurologic and musculoskeletal assessments, monitor recovery, and counsel families regarding prognosis and treatment expectations. Early consultation with pediatric neurologists, orthopedic surgeons, plastic surgeons, and neurosurgeons is important in infants with severe injury, incomplete recovery, or persistent deficits to guide further evaluation and determine the need for surgical intervention.
Physical and occupational therapists are essential for maintaining range of motion, preventing contractures, promoting motor recovery, and educating caregivers regarding positioning and home exercise programs. Prenatal counseling and optimal management of maternal diabetes may help reduce risk by decreasing fetal macrosomia and shoulder dystocia. Because prolonged recovery and residual deficits can have substantial psychosocial effects, social workers and mental health professionals provide emotional support, facilitate access to community resources, and assist families with long-term care needs. Close communication among interprofessional team members and continued outpatient monitoring are critical to optimizing patient-centered outcomes.
Media
(Click Image to Enlarge)
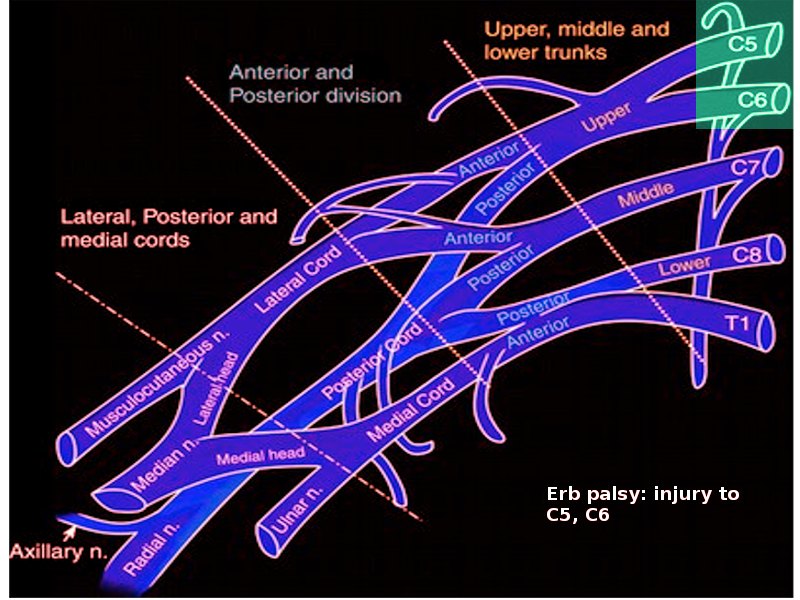
Erb Palsy-Brachial Plexus. Erb palsy results from a birth injury involving the cervical spinal nerves C5 and C6, which form the upper trunk of the brachial plexus.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
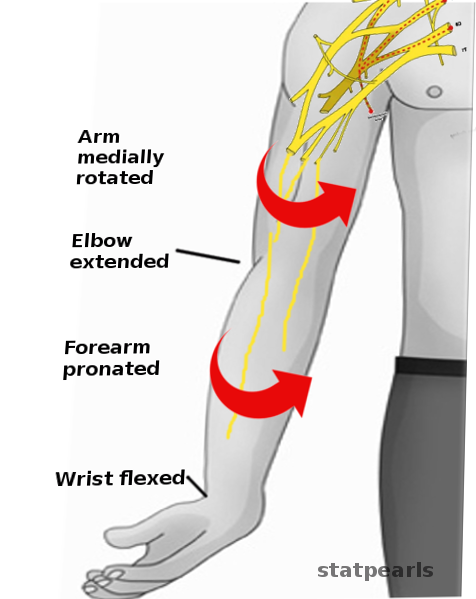
Erb Palsy Physical Examination. Evaluation includes a detailed neuromuscular examination, assessing posture, spontaneous movement, reflexes, strength, and active and passive range of motion.
Contributed by S Bhimji, MD
References
Evans-Jones G, Kay SP, Weindling AM, Cranny G, Ward A, Bradshaw A, Hernon C. Congenital brachial palsy: incidence, causes, and outcome in the United Kingdom and Republic of Ireland. Archives of disease in childhood. Fetal and neonatal edition. 2003 May:88(3):F185-9 [PubMed PMID: 12719390]
Ashworth WR, Kelford-Matthews E. Brachial Plexus Birth Injury: Current Concepts in Its Assessment and Management. British journal of hospital medicine (London, England : 2005). 2026 Mar 20:87(3):52085. doi: 10.31083/BJHM52085. Epub [PubMed PMID: 41913992]
Leinberry CF, Wehbé MA. Brachial plexus anatomy. Hand clinics. 2004 Feb:20(1):1-5 [PubMed PMID: 15005376]
Chater M, Camfield P, Camfield C. Erb's palsy - Who is to blame and what will happen? Paediatrics & child health. 2004 Oct:9(8):556-560 [PubMed PMID: 19680484]
Smith BW, Daunter AK, Yang LJ, Wilson TJ. An Update on the Management of Neonatal Brachial Plexus Palsy-Replacing Old Paradigms: A Review. JAMA pediatrics. 2018 Jun 1:172(6):585-591. doi: 10.1001/jamapediatrics.2018.0124. Epub [PubMed PMID: 29710183]
Van der Looven R, Le Roy L, Tanghe E, Samijn B, Roets E, Pauwels N, Deschepper E, De Muynck M, Vingerhoets G, Van den Broeck C. Risk factors for neonatal brachial plexus palsy: a systematic review and meta-analysis. Developmental medicine and child neurology. 2020 Jun:62(6):673-683. doi: 10.1111/dmcn.14381. Epub 2019 Oct 31 [PubMed PMID: 31670385]
Level 1 (high-level) evidenceDeFrancesco CJ, Mahon SJ, Desai VM, Pehnke M, Manske MC, Shah AS. Epidemiology of Brachial Plexus Birth Injury and the Impact of Cesarean Section on Its Incidence. Journal of pediatric orthopedics. 2025 Jan 1:45(1):43-50. doi: 10.1097/BPO.0000000000002800. Epub 2024 Aug 27 [PubMed PMID: 39187951]
Arslan O, Giray B, Tuğ N. Obstetric brachial plexus injury: risk factors and clinical follow-up results. Journal of the Turkish German Gynecological Association. 2025 Sep 3:26(3):204-211. doi: 10.4274/jtgga.galenos.2025.2025-3-3. Epub 2025 Aug 22 [PubMed PMID: 40843939]
Level 2 (mid-level) evidenceGraham EM, Forouzan I, Morgan MA. A retrospective analysis of Erb's palsy cases and their relation to birth weight and trauma at delivery. The Journal of maternal-fetal medicine. 1997 Jan-Feb:6(1):1-5 [PubMed PMID: 9029377]
Level 2 (mid-level) evidenceDeFrancesco CJ, Shah DK, Rogers BH, Shah AS. The Epidemiology of Brachial Plexus Birth Palsy in the United States: Declining Incidence and Evolving Risk Factors. Journal of pediatric orthopedics. 2019 Feb:39(2):e134-e140. doi: 10.1097/BPO.0000000000001089. Epub [PubMed PMID: 29016426]
Sargut TA, Ferdowssian K, Mark-Sargut CS, Huscher D, Alsolivany J, Früh A, Bahm J, Thomale UW, Dengler NF. Epidemiology and surgical management of obstetric brachial plexus injury: a national cohort study. Journal of neurosurgery. Pediatrics. 2025 Jul 1:36(1):119-126. doi: 10.3171/2025.1.PEDS24626. Epub 2025 May 2 [PubMed PMID: 40315612]
Mollberg M, Ladfors LV, Strömbeck C, Elden H, Ladfors L. Increased incidence of shoulder dystocia but a declining incidence of obstetric brachial plexus palsy in vaginally delivered infants. Acta obstetricia et gynecologica Scandinavica. 2023 Jan:102(1):76-81. doi: 10.1111/aogs.14481. Epub 2022 Nov 8 [PubMed PMID: 36345990]
Chauhan SP, Blackwell SB, Ananth CV. Neonatal brachial plexus palsy: incidence, prevalence, and temporal trends. Seminars in perinatology. 2014 Jun:38(4):210-8. doi: 10.1053/j.semperi.2014.04.007. Epub [PubMed PMID: 24863027]
Doumouchtsis SK, Arulkumaran S. Are all brachial plexus injuries caused by shoulder dystocia? Obstetrical & gynecological survey. 2009 Sep:64(9):615-23. doi: 10.1097/OGX.0b013e3181b27a3a. Epub [PubMed PMID: 19691859]
Level 2 (mid-level) evidenceBeaumont HO, Wiberg A, Brown H, Quick TJ. Anatomical predisposition and neurological vulnerability to brachial plexus birth injury: a contemporary narrative review. The Journal of hand surgery, European volume. 2026 Jul:51(7):961-966. doi: 10.1177/17531934261443088. Epub 2026 May 4 [PubMed PMID: 42080466]
Level 3 (low-level) evidenceKhabyeh-Hasbani N, O'Brien DM, Meisel EM, Koehler SM. Current Concepts in Brachial Plexus Birth Injuries: A Comprehensive Narrative Review. Plastic and reconstructive surgery. Global open. 2024 Aug:12(8):e6083. doi: 10.1097/GOX.0000000000006083. Epub 2024 Aug 22 [PubMed PMID: 39175516]
Level 3 (low-level) evidenceLin JS, Samora JB. Brachial Plexus Birth Injuries. The Orthopedic clinics of North America. 2022 Apr:53(2):167-177. doi: 10.1016/j.ocl.2021.11.003. Epub 2022 Mar 5 [PubMed PMID: 35365261]
. Executive summary: Neonatal brachial plexus palsy. Report of the American College of Obstetricians and Gynecologists' Task Force on Neonatal Brachial Plexus Palsy. Obstetrics and gynecology. 2014 Apr:123(4):902-4. doi: 10.1097/01.AOG.0000445582.43112.9a. Epub [PubMed PMID: 24785634]
Govindan M, Burrows HL. Neonatal Brachial Plexus Injury. Pediatrics in review. 2019 Sep:40(9):494-496. doi: 10.1542/pir.2018-0113. Epub [PubMed PMID: 31477594]
Shah V, Coroneos CJ, Ng E. The evaluation and management of neonatal brachial plexus palsy. Paediatrics & child health. 2021 Dec:26(8):493-497. doi: 10.1093/pch/pxab083. Epub 2021 Dec 27 [PubMed PMID: 34992702]
Dodds SD, Wolfe SW. Perinatal brachial plexus palsy. Current opinion in pediatrics. 2000 Feb:12(1):40-7 [PubMed PMID: 10676773]
Level 3 (low-level) evidenceEl-Sayed AA. Intermediate Type of Obstetric Brachial Plexus Palsy. Journal of child neurology. 2016 Dec:31(14):1628-1630 [PubMed PMID: 27655471]
Mahrouck H, Almatrafi N, Tamboosi M. Early Conservative Physical Therapy Management of Babies With Obstetric Brachial Plexus Injury to Facilitate Spontaneous Recovery. Pediatric physical therapy : the official publication of the Section on Pediatrics of the American Physical Therapy Association. 2025 Jan 1:37(1):100-108. doi: 10.1097/PEP.0000000000001161. Epub 2024 Oct 30 [PubMed PMID: 39495595]
Greenhill DA, Lukavsky R, Tomlinson-Hansen S, Kozin SH, Zlotolow DA. Relationships Between 3 Classification Systems in Brachial Plexus Birth Palsy. Journal of pediatric orthopedics. 2017 Sep:37(6):374-380. doi: 10.1097/BPO.0000000000000699. Epub [PubMed PMID: 26633814]
Expert Panel on Neurologic Imaging:, Bykowski J, Aulino JM, Berger KL, Cassidy RC, Choudhri AF, Kendi AT, Kirsch CFE, Luttrull MD, Sharma A, Shetty VS, Than K, Winfree CJ, Cornelius RS. ACR Appropriateness Criteria(®) Plexopathy. Journal of the American College of Radiology : JACR. 2017 May:14(5S):S225-S233. doi: 10.1016/j.jacr.2017.02.002. Epub [PubMed PMID: 28473078]
Bauer AS, Van Heest AE, Manske MC, Shen PY, Asis MJ, Chang J, Taylor S, James MA. Early MRI Can Predict the Indication for Surgery in Brachial Plexus Birth Injury: Results of the NAPTIME Study. The Journal of bone and joint surgery. American volume. 2025 Mar 19:107(6):e18. doi: 10.2106/JBJS.24.00561. Epub 2025 Jan 29 [PubMed PMID: 39879284]
Duff SV, DeMatteo C. Clinical assessment of the infant and child following perinatal brachial plexus injury. Journal of hand therapy : official journal of the American Society of Hand Therapists. 2015 Apr-Jun:28(2):126-33; quiz 134. doi: 10.1016/j.jht.2015.01.001. Epub 2015 Jan 16 [PubMed PMID: 25840493]
Socolovsky M, Costales JR, Paez MD, Nizzo G, Valbuena S, Varone E. Obstetric brachial plexus palsy: reviewing the literature comparing the results of primary versus secondary surgery. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2016 Mar:32(3):415-25. doi: 10.1007/s00381-015-2971-4. Epub 2015 Nov 28 [PubMed PMID: 26615411]
Raducha JE, Cohen B, Blood T, Katarincic J. A Review of Brachial Plexus Birth Palsy: Injury and Rehabilitation. Rhode Island medical journal (2013). 2017 Nov 1:100(11):17-21 [PubMed PMID: 29088569]
Price A, Tidwell M, Grossman JA. Improving shoulder and elbow function in children with Erb's palsy. Seminars in pediatric neurology. 2000 Mar:7(1):44-51 [PubMed PMID: 10749513]
Thuau F, Gadbled G, Lahmar T, Perrot P, Lancien U. Surgical nerve wrapping for brachial plexus neuropathy: A systematic review. JPRAS open. 2026 Mar:48():163-183. doi: 10.1016/j.jpra.2025.11.005. Epub 2025 Nov 11 [PubMed PMID: 41438880]
Level 1 (high-level) evidenceFrade F, Gómez-Salgado J, Jacobsohn L, Florindo-Silva F. Rehabilitation of Neonatal Brachial Plexus Palsy: Integrative Literature Review. Journal of clinical medicine. 2019 Jul 5:8(7):. doi: 10.3390/jcm8070980. Epub 2019 Jul 5 [PubMed PMID: 31284431]
Boetto V, Markova A, Malgrati F, Bongiovanni I, Bassetto A, Pavese C, Nardone A, Massazza G, Colò G, Titolo P. Conservative Treatment of Neonatal Brachial Plexus Palsy: A Narrative Review. Journal of clinical medicine. 2024 Dec 21:13(24):. doi: 10.3390/jcm13247826. Epub 2024 Dec 21 [PubMed PMID: 39768749]
Level 3 (low-level) evidenceMartínez-Carlón-Reina M, Hareau-Bonomi J, Rodríguez-Pérez MP, Huertas-Hoyas E. Systematic Review and Meta-Analysis of Intervention Techniques in Occupational Therapy for Babies and Children with Obstetric Brachial Plexus Palsy. Journal of clinical medicine. 2024 Oct 17:13(20):. doi: 10.3390/jcm13206186. Epub 2024 Oct 17 [PubMed PMID: 39458134]
Level 1 (high-level) evidenceFogel I, Katz A, Sela HY, Lebel E. Brachial plexus birth palsy: incidence, natural-course, and prognostic factors during the first year of life. Journal of perinatology : official journal of the California Perinatal Association. 2021 Jul:41(7):1590-1594. doi: 10.1038/s41372-021-00972-4. Epub 2021 Mar 31 [PubMed PMID: 33790402]
Caron E, Gienapp AJ, Files H, Ridley-Pryor T. Brachial Plexus Birth Injury: A Single-Center Study. Clinical pediatrics. 2023 Dec:62(12):1489-1496. doi: 10.1177/00099228231163698. Epub 2023 Mar 25 [PubMed PMID: 36964689]
Pires JAP, Martins IC, Ohannesian VA, Ribeiro BDL, Marçola Ishizuka B, Ferreira JSN, Cabral MA, Brenner LBO, Menezes LHF, Dibai Filho AV, Lu VM, Sakata RK, Moura ECR, Leal PDC. Long-term outcomes and effectiveness of interventions in neonatal brachial plexus palsy: A systematic review. Medicine. 2025 Sep 12:104(37):e44508. doi: 10.1097/MD.0000000000044508. Epub [PubMed PMID: 40958300]
Level 1 (high-level) evidencevan Vliet AC, Tannemaat MR, van Duinen SG, Verhaagen J, Malessy MJ, De Winter F. Human Neuroma-in-Continuity Contains Focal Deficits in Myelination. Journal of neuropathology and experimental neurology. 2015 Sep:74(9):901-11. doi: 10.1097/NEN.0000000000000229. Epub [PubMed PMID: 26226133]
Foad SL, Mehlman CT, Foad MB, Lippert WC. Prognosis following neonatal brachial plexus palsy: an evidence-based review. Journal of children's orthopaedics. 2009 Dec:3(6):459-63. doi: 10.1007/s11832-009-0208-3. Epub 2009 Nov 3 [PubMed PMID: 19885693]
Danisman M, Emet A, Kocyigit IA, Hassa E, Uzumcugil A. Examination of Upper Extremity Length Discrepancy in Patients with Obstetric Brachial Plexus Paralysis. Children (Basel, Switzerland). 2023 May 13:10(5):. doi: 10.3390/children10050876. Epub 2023 May 13 [PubMed PMID: 37238424]
Schmieg S, Nguyen JC, Pehnke M, Yum SW, Shah AS. Team Approach: Management of Brachial Plexus Birth Injury. JBJS reviews. 2020 Jul:8(7):e1900200. doi: 10.2106/JBJS.RVW.19.00200. Epub [PubMed PMID: 32618739]
Fawcett EB, Bosh KB, Saul KR, Cole JH. Changes in Glenohumeral Musculoskeletal Development Following Brachial Plexus Birth Injury. Journal of orthopaedic research : official publication of the Orthopaedic Research Society. 2025 Aug:43(8):1367-1377. doi: 10.1002/jor.26104. Epub 2025 Jun 8 [PubMed PMID: 40483597]
Al-Qattan MM, El-Sayed AA. Obstetric brachial plexus palsy: the mallet grading system for shoulder function--revisited. BioMed research international. 2014:2014():398121. doi: 10.1155/2014/398121. Epub 2014 Jan 5 [PubMed PMID: 24527447]
Nikolaou S, Peterson E, Kim A, Wylie C, Cornwall R. Impaired growth of denervated muscle contributes to contracture formation following neonatal brachial plexus injury. The Journal of bone and joint surgery. American volume. 2011 Mar 2:93(5):461-70. doi: 10.2106/JBJS.J.00943. Epub [PubMed PMID: 21368078]
Terzis JK, Kokkalis ZT. Bone discrepancy as a powerful indicator for early surgery in obstetric brachial plexus palsy. Hand (New York, N.Y.). 2010 Dec:5(4):386-96. doi: 10.1007/s11552-010-9270-z. Epub 2010 May 18 [PubMed PMID: 22131921]
Anguelova GV, de Vlugt E, Vardy AN, van Zwet EW, van Dijk JG, Malessy MJA, de Groot JH. Cocontraction measured with short-range stiffness was higher in obstetric brachial plexus lesions patients compared to healthy subjects. Journal of biomechanics. 2017 Oct 3:63():192-196. doi: 10.1016/j.jbiomech.2017.08.015. Epub 2017 Aug 24 [PubMed PMID: 28844723]
Bauer AS, Manske MC, Dorich JM, Miller PE, Aguiar R, Al-Muhtaseb T, Allgier A, Miller M, Davidge KM, Cornwall R. Children's Health-Related Quality of Life After Brachial Plexus Birth Injury. JAMA network open. 2026 May 1:9(5):e2610237. doi: 10.1001/jamanetworkopen.2026.10237. Epub 2026 May 1 [PubMed PMID: 42065889]
Level 2 (mid-level) evidenceAlyanak B, Kılınçaslan A, Kutlu L, Bozkurt H, Aydın A. Psychological adjustment, maternal distress, and family functioning in children with obstetrical brachial plexus palsy. The Journal of hand surgery. 2013 Jan:38(1):137-42. doi: 10.1016/j.jhsa.2012.09.036. Epub 2012 Dec 4 [PubMed PMID: 23218557]