Introduction
Basal cell carcinoma (BCC), previously known as basal cell epithelioma, is humans' most common type of skin cancer. This carcinoma typically arises on sun-exposed skin and rarely develops on the mucous membranes, palms, or soles of the feet. BCC is usually a slow-growing tumor with rare metastases, but delayed or inadequate treatment can result in significant local tissue destruction and disfigurement. Clinically, BCC often appears as pink or flesh-colored, pearly papules with overlying ulceration or telangiectatic vessels. Most cases occur on the head or neck, but can also involve the trunk and extremities.[1][2]
The literature describes more than 26 histologic subtypes of BCC. The most common and clinically distinctive types include nodular, micronodular, superficial, morpheaform, infiltrative, and fibroepithelial (also known as fibroepithelioma of Pinkus). Combinations of these types can also occur. While most BCCs are amelanotic, some may contain variable amounts of melanin. The primary treatment for BCC is surgical, including standard excision, electrodesiccation and curettage (EDC), cryosurgery, and Mohs micrographic surgery. These approaches are generally reserved for localized disease and achieve excellent outcomes, with 5-year cure rates exceeding 95%.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The principal etiologic factor in BCC development is exposure to ultraviolet (UV) radiation, particularly UVB wavelengths, although UVA also contributes.[3] Meta-analyses confirm a significantly higher incidence among outdoor workers, with risk increasing at lower latitudes.[4] Among White individuals, Fitzpatrick skin type is a strong predictor, with types I and II carrying the greatest susceptibility.
Cumulative UV dose alone does account for BCC risk; exposure timing and intensity, especially during childhood and adolescence, are critical determinants. Additional contributors include recreational sunlight exposure, blistering sunburns, indoor tanning, and certain phototherapies (particularly high-dose Psoralen plus UVA [PUVA]).[5] Notably, up to 20% of BCCs arise on non–sun–exposed sites, implicating additional risk factors such as prior ionizing radiation, arsenic exposure, immunosuppression, and inherited syndromes (eg, xeroderma pigmentosum, basal cell nevus syndrome, Bazex–Dupré–Christol syndrome, and Rombo syndrome).[6] There is no proven link between diet and BCC, and while some studies ' results suggest smoking may modestly increase risk in women, the evidence remains inconsistent.[7]
Epidemiology
BCC is the most common malignancy in humans, and its incidence continues to rise globally. Over the past 30 years, reported BCC incidence rates have increased by an estimated 20% to 80%. In the United States, approximately 5.4 million cases of basal and squamous cell carcinomas (SCCs) are diagnosed annually, affecting about 3.3 million individuals.[8]
Risk Factors
BCC arises from environmental, genetic, and host-related risk factors. The most significant contributor is UV radiation exposure, though additional risks include the following:
- Age: The risk increases with advancing age, with the median diagnosis occurring at approximately 68 years.
- Gender: Men have a higher incidence of BCC than women, particularly in older age groups.
- Ethnicity: White individuals have a higher lifetime risk compared to other racial groups.
- UV exposure: Chronic exposure to UV radiation is BCC's primary environmental driver.
- Previous skin cancer: A prior diagnosis of BCC or SCC significantly elevates the likelihood of developing subsequent BCCs.
Prognosis and Mortality
BCC is typically a slow-growing tumor with very low metastatic potential. Mortality is rare and occurs most often in immunocompromised individuals. The estimated age-adjusted mortality rate for BCC is 0.12 per 100,000 individuals.[9]
Metastasis
Metastatic BCC is exceedingly rare, with an estimated incidence ranging from 0.0028% to 0.55%.[10] When metastasis occurs, it often involves regional lymph nodes, bone, lungs, and skin.
Pathophysiology
Chronic sun exposure is among the most critical risk factors for developing BCC. There is typically a latency period of 15 to 20 years between UV damage and the clinical onset of BCC.[11] UV radiation promotes BCC formation through direct and indirect DNA damage and immune suppression. UVB directly damages DNA and RNA, producing characteristic C→T or CC→TT transition mutations. UVA generates reactive oxygen species through melanin absorption, resulting in indirect DNA damage. Ultraviolet exposure also causes dose-dependent suppression of the cutaneous immune system, impairing immune surveillance against emerging skin cancer.
Genetic Alterations in BCC
The pathogenesis of BCC is strongly linked to mutations in the Hedgehog (Hh) signaling pathway and other tumor suppressor genes:[12]
- PTCH1 mutations: Inactivating mutations in the PTCH1 gene are present in approximately 70% to 90% of BCCs.
- SMO mutations: Activating mutations in the SMO gene occur in approximately 10% to 20% of BCCs, resulting in aberrant Hh pathway activation.[12]
- TP53 mutations: Mutations in the TP53 gene are the second most common genetic alterations in BCCs, found in approximately 44% to 65% of cases.
- CDKN2A mutations: Mutations in the CDKN2A gene are less common in sporadic BCCs, and variable frequencies have been reported across studies.
Histopathology
The hallmark histopathologic feature of BCCs is the presence of islands or nests of basaloid cells, characterized by peripheral palisading of nuclei and a more disorganized arrangement within the tumor centers. These small pleomorphic cells typically have basophilic nuclei, no discernible nucleoli, and scant cytoplasm. A retraction artifact (clefting) between the tumor and surrounding stroma is commonly observed in paraffin-embedded sections. Additional findings may include mucin deposition within and around the tumor, as well as the presence of mitotic figures. Perineural growth, also known as perineural invasion, can indicate aggressive disease.
The histologic differential diagnosis of BCC includes trichoepithelioma and trichoblastoma. Multiple morphological subtypes of BCC have been described, including nodular (solid), micronodular, superficial, cystic, infiltrating, infundibulocystic, pigmented, adenoid, sclerosing, metatypical, basosquamous, and fibroepitheliomatous (see Image. Pigmented Basal Cell Carcinoma). Mixed patterns of these subtypes are also common.
- The superficial subtype features multiple, small basaloid cell buds descending from the epidermis, without dermal invasion.[13][14]
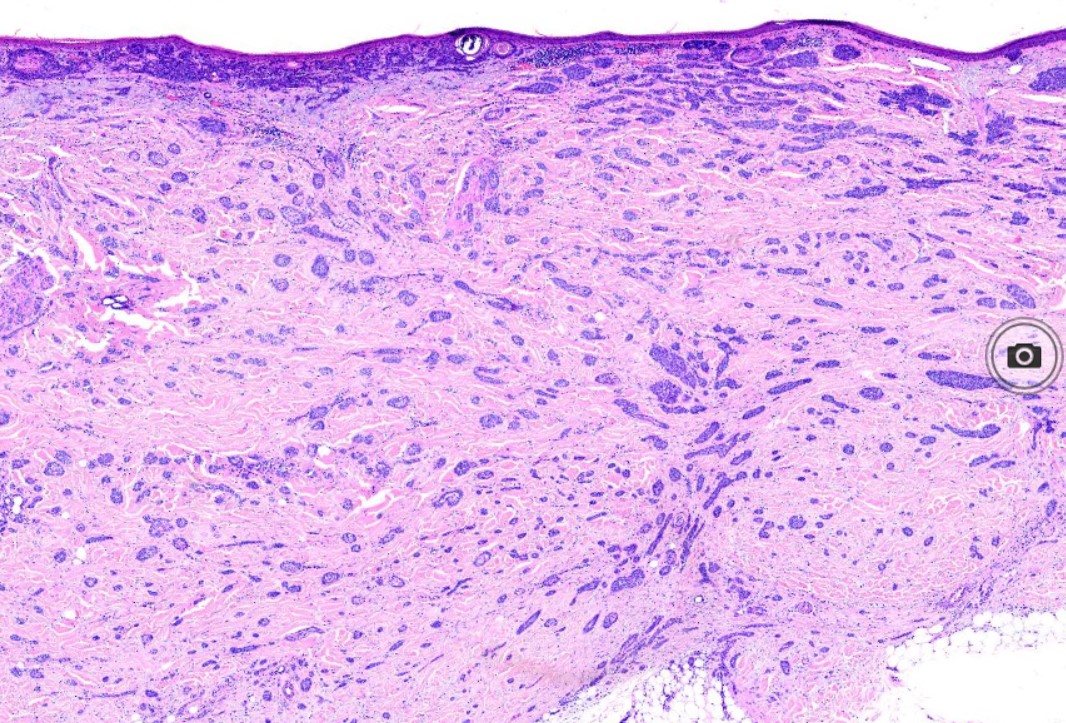
- The nodular variant, which accounts for most cases, consists of islands of basaloid cells with peripheral palisading and a haphazard arrangement of central cells. Ulceration may occur in larger lesions (see Image. Basal Cell Carcinoma, Nodular).[13][14]
- The micronodular subtype resembles nodular BCC but is composed of numerous small nodules. The micronodular type has a significantly higher risk of local recurrence than the solid type (see Image. Micronodular Basal Cell Carcinoma).[13][14]
- The sclerosing (morpheaform) subtype exhibits spiky strands of basaloid cells infiltrating the dermis within a dense fibrous stroma. The histologic differential diagnosis includes microcystic adnexal carcinoma, desmoplastic trichoepithelioma, and metastatic cancer. When most tumor nests show spiky projections, the tumor may invade deeply, an infiltrative BCC (see Image. Basal Cell Carcinoma, Morpheaform).[14]
- The pigmented BCC results from the presence of melanocytes and melanin interspersed among tumor cells, occurring most commonly in superficial, micronodular, or follicular variants (see Image. Basal Cell Cancer).
- The infundibulocystic variant is uncommon and often found on the face, appearing as a small, well-circumscribed tumor composed of anastomosing nests of basaloid cells with minimal stroma. Numerous small infundibular cyst-like structures contain keratinous material and occasional melanin.
- Basosquamous or metatypical BCC shows features of both BCC and SCC. The exact nature of this lesion is controversial; however, the term is generally applied to a rare type of BCC composed of nests and strands of basaloid cells that mature into larger, paler cells lacking peripheral palisading.
- Fibroepithelioma of Pinkus presents as a soft nodular lesion resembling a fibroma or papilloma, commonly on the lower back. These comprise anastomosing strands and aggregates of basaloid cells within a fibrous stroma (see Image. Basal Cell Carcinoma, Fibroepithelioma of Pinkus).[13][14]
History and Physical
Many clinical variants of BCC exist, but the most recognized types are superficial, nodular, and morpheaform BCC. Nodular BCC is the most prevalent (see Image. Nodulocystic Basal Cell Carcinoma). BCC typically presents as a shiny, pink- or flesh-colored papule or nodule with surface telangiectasia. As the lesion enlarges, ulceration may develop, producing the characteristic rolled or "rodent ulcer" borders. Nodular BCC often arises on the face, especially the nose, cheeks, forehead, nasolabial folds, and eyelids. Patients frequently report a history of crusting and recurrent bleeding, prompting medical evaluation. Pigmented nodular BCC is more common in individuals with darker skin tones.
Superficial BCCs are pink to red, and scaly macules or patches may contain telangiectasia (see Image. Superficial Basal Cell Carcinoma). They have a predilection for the shoulders, chest, or back, and multiple lesions may be present. Pigmented variants can also occur (see Image. Pigmented Basal Cell Carcinoma of Temple). Clinically, superficial BCC can resemble inflammatory dermatoses such as eczema or psoriasis; thus, persistent, erythematous, scaly plaques should prompt consideration of superficial BCC. Over time, areas of superficial BCC can evolve into nodular BCC.
The morpheaform subtype is another common clinical variant of BCC. These tumors frequently present as white or flesh-colored with induration and poorly defined borders, often resembling a scar or plaque of morphea. The surface is typically smooth, although it may be crusted with underlying erosions, ulcerations, or superimposed papules, which telangiectasias can sometimes accompany. Morpheaform BCC generally exhibits a more aggressive biologic behavior, with a tendency for extensive local tissue destruction.
Evaluation
A skin biopsy is necessary for definitive diagnosis of BCC. Acceptable techniques include shave, punch, or excisional biopsy, with attention to sampling a portion of the dermis to distinguish superficial from more invasive histologic subtypes. Punch and shave biopsies are about 80% accurate in identifying the various BCC subtypes.[15]
A qualified clinician should perform a comprehensive skin examination, as individuals with 1 skin cancer frequently have additional cancers or precancerous lesions and remain at an elevated risk for other cutaneous malignancies. Photographic or digital documentation of lesion sites is recommended. Clinicians should maintain a low threshold for biopsy in these patients. Preoperative imaging may be warranted when there is concern for involvement of the parotid gland, muscle, deep soft tissue, orbit, bone, or perineural invasion. Patients with a history of BCC require long-term, often lifelong follow-up, particularly those with multiple or high-risk tumors.
Dermoscopy is a valuable tool for experienced clinicians in diagnosing pigmented and nonpigmented BCCs. The hallmark feature is the presence of well-focused arborizing vessels. Additional findings include multiple blue-gray globules, leaf-like structures, large blue-gray ovoid nests, and spoke-wheel areas. BCC lacks the pigment network typically seen in melanocytic lesions.
Treatment / Management
Treatment planning for BCCs depends on patient factors (such as age and gender) and tumor characteristics (including site, size, and histologic subtype). No single approach is universally appropriate for all patients or lesions. A biopsy should be obtained in all suspected cases to confirm the diagnosis and guide management. The primary goals of therapy are: (1) complete tumor removal to prevent recurrence, (2) preservation or restoration of function, and (3) achievement of the best possible cosmetic outcome.[16](A1)
The management of BCC typically involves surgical intervention, although certain cases may be treated with medical or radiation therapies. Surgical approaches include Mohs micrographic surgery (MMS), standard surgical excision, electrodessication and curettage (EDC), and cryosurgery. Nonsurgical options encompass radiation therapy, photodynamic therapy, topical therapies, and systemic medications such as vismodegib. Reported recurrence rates for primary BCC vary by modality: MMS, 1.0%; surgical excision, 10.1%; EDC, 7.7%; radiation therapy, 8.7%; and cryosurgery, 7.5%.[17][18]
Mohs surgery provides the best long-term cure rate of all treatment modalities for BCC and is considered the gold standard for managing high-risk BCCs and recurrent BCCs because of its high cure rate and tissue-sparing benefit. The high cure rate stems from examining 100% of surgical margins compared to standard vertical sectioning, which assesses less than 1% of peripheral and deep margins. By removing thin layers of tissue only from areas with positive tumor margins, MMS minimizes wound size and maximizes the likelihood of a favorable cosmetic outcome.
Postoperative pathologic analysis with permanent sections is standard following surgical excision. A 4 mm margin is typically sufficient for well-circumscribed tumors smaller than 2 cm in diameter. For facial lesions, narrow-margin excision is often inadequate for complete tumor removal. EDC is frequently used for low-risk BCCs, with reported cure rates of 97% to 98% when tumors do not extend into the deep dermis. While EDC is the least expensive and fastest treatment option, wounds heal by second intention, often leaving a white, atrophic scar that may be cosmetically unfavorable.
Radiation therapy is a primary treatment option for BCC or SCC when surgery is contraindicated, and it also serves as an adjuvant treatment in cases where further surgery could risk damage to major nerves or other vital structures, or when perineural invasion is present. The disadvantages of radiation therapy are higher cost, potential for suboptimal cosmetic outcomes, lengthy treatment courses (typically 15-30 sessions), and an increased risk for secondary skin cancers. Unlike surgical scars, which often improve over time, radiation-induced scars may worsen with age. Radiation is relatively contraindicated in those with connective tissue disorders. The NCCN explicitly notes that patients with scleroderma are at elevated risk of severe radiation-induced fibrosis, necrosis, and poor wound healing, making RT a poor choice even when technically feasible.[19](B3)
Cryosurgery is an option for treating low-risk BCCs. The procedure involves the controlled application of liquid nitrogen to the clinically visible tumor and a small margin of surrounding normal-appearing skin. A temperature probe can be inserted at the lateral tumor margin, with the tip positioned obliquely beneath the tumor. Liquid nitrogen is applied until the temperature reaches -60 °C, although temperature monitoring is seldom employed in practice. Cryosurgery is a relatively quick and minimally invasive procedure, making it suitable for patients who wish to avoid traditional surgery. However, the treated area often becomes painful and swollen after thawing, and potential complications include hypertrophic scarring and permanent pigment alteration.
Topical therapy is an additional treatment option for BCC. Topical 5-fluorouracil (5-FU) and imiquimod 5% cream are approved by the Food and Drug Administration (FDA) to manage superficial BCC. especially when the lesion is <2 cm, well-demarcated, and confined to the superficial dermis These agents are useful options in patients with multiple superficial BCCs and in those who are poor surgical candidates. Local application-site reactions are common and may include erythema, pruritus, pain, edema, hypopigmentation, hyperpigmentation, crusting, bleeding, and erosions. A significant limitation of topical therapy is the lack of complete tumor clearance and histologic confirmation.
A more recent option for patients with advanced or metastatic BCC not amenable to conventional therapies is treatment with hedgehog pathway inhibitors (HHI). The FDA approved vismodegib in 2012, followed by sonidegib, indicated for locally advanced lesions that cannot be treated with surgery or radiation.[20] Unlike immunotherapy, HHIs do not rely on immune activation and have not been associated with increased transplant rejection risk. They are considered appropriate for use in solid organ transplant recipients with locally advanced BCC.[21] The adverse effects may result in discontinuation in up to 55% of patients. The most commonly reported adverse effects included nausea, dysgeusia, muscle spasm, alopecia, weight loss, diarrhea, and fatigue. For those who respond well to HHI but stop due to side effects, a drug holiday and restart of the same drug class is a reasonable approach. Cemiplimab is a monoclonal antibody immune checkpoint inhibitor that is indicated as a second-line treatment for locally advanced or metastatic basal cell carcinoma.[22] In specific populations, such as immunosuppressed individuals, older adults, and those with poor baseline functional status, surgery may not be the optimal option. For individuals with metastatic, advanced, recalcitrant, or cosmetically sensitive disease, nonsurgical management may be a preferred alternative.[16](A1)
Differential Diagnosis
The differential diagnosis of BCC includes adnexal tumors with follicular, sweat gland, or sebaceous differentiation and specific subtypes of squamous cell carcinoma (SCC). Nodular BCC may resemble trichoblastoma or trichoepithelioma, while superficial BCC may mimic inflammatory dermatoses such as psoriasis or eczema. Morpheaform BCC may be mistaken for a scar or a plaque of morphea. In such cases, histopathological examination is essential to confirm the diagnosis.
Pertinent Studies and Ongoing Trials
Ongoing clinical trials in BCC are exploring novel therapeutic approaches beyond standard surgical management. Investigational studies include the use of Hh pathway inhibitors, such as vismodegib, in combination with surgery, topical agents like patidegib for Gorlin syndrome, and immune checkpoint inhibitors, such as cemiplimab, for advanced or metastatic BCC following prior Hh inhibitor therapy.[23][24] Prophylaxis for syndromic basal cell includes systemic nicotinamide.[25] Additional trials are examining the safety and efficacy of oncolytic virus therapy (RP1) in patients with advanced cutaneous malignancies, including those with solid organ transplants, as well as photodynamic therapy using BF-200 ALA and Ameluz with the BF-RhodoLED lamp.[26] These studies, designed as randomized controlled, open-label, or multicenter trials, aim to improve treatment efficacy, reduce adverse events, and expand therapeutic options for patients with locally advanced, recurrent, or treatment-resistant BCC. Participation in these trials provides early access to emerging therapies and advances clinical knowledge in managing BCC.
Staging
BCC is primarily staged based on tumor size, location, histologic subtype, and high-risk features. Unlike many other malignancies, formal tumor, node, metastasis (TNM) staging is less commonly applied for BCC due to its very low metastatic potential. High-risk features include tumor diameter greater than 2 cm, location on the central face, ears, or scalp, poorly defined borders, recurrent tumors, aggressive histologic subtypes (morpheaform, infiltrative, micronodular, or basosquamous), and perineural invasion. While regional or distant metastases are exceedingly rare, staging may be considered in advanced or high-risk cases to guide management. Risk stratification informs treatment decisions, including selecting MMS, standard excision with appropriate margins, or adjunctive therapies such as radiation or systemic Hh pathway inhibitors for locally advanced or inoperable disease.
Prognosis
BCC is rarely associated with a fatal outcome. Prognosis is primarily determined by the risk of recurrence after initial therapy, which depends on the tumor's location and its clinical and histopathological features.
- Good prognosis:
- Primary superficial BCC
- Primary nodular BCC <1cm in an intermediate-risk location or,
- <2 cm in a low-risk location
- Intermediate prognosis:
- Recurrent superficial BCC
- Nodular BCC <1 cm in a high-risk location or,
- <2 cm in an intermediate-risk location or,
- >2cm in a low-risk location
- Poor prognosis:
- Nodular BCC >1 cm in a high-risk location (high risk of recurrence)
- Morpheaform, infiltrative, or other histologically aggressive subtypes (very high recurrence risk)
- Recurrent tumors (except superficial BCC), which also carry a very high risk of recurrence
Complications
Treatment of BCC is generally effective but may be associated with complications that vary depending on the treatment modality. The likelihood and severity of these complications depend on factors such as tumor location, size, patient comorbidities, and the specific therapeutic approach chosen. Surgical interventions, including MMS and standard excision, carry risks such as bleeding, infection, delayed wound healing, scarring, and cosmetic or functional deficits, particularly in anatomically sensitive areas such as the face. These risks are generally low but can significantly impact quality of life when lesions occur in cosmetically or functionally critical areas.
Nonsurgical therapies, including radiation, photodynamic therapy, topical agents, and systemic Hh pathway inhibitors (eg, vismodegib), can lead to localized skin reactions, pain, erythema, edema, alopecia, taste disturbances, muscle cramps, and gastrointestinal symptoms. Rarely, systemic therapy may cause more severe adverse effects, such as teratogenicity, weight loss, or fatigue, underscoring the need for careful patient selection, monitoring, and interprofessional management to optimize outcomes and minimize morbidity.
Deterrence and Patient Education
Following excision of a low-risk basal cell carcinoma, persons should undergo a full skin check every 6-12 months for the first 5 years, followed by annual exams. An estimated 30% to 50% of patients with a history of BCC will develop another BCC within 5 years. Continued surveillance is essential even in patients with low-risk histology and/or negative margins.[27]
Pearls and Other Issues
Key facts to keep in mind about BCC include the following:
- Most common skin cancer and most common cancer overall
- Arises from basal keratinocytes in the epidermis
- Strongest risk factor is chronic sun (UVB) exposure, especially in fair-skinned individuals
- Other risks include ionizing radiation, arsenic, immunosuppression, and genetic syndromes (xeroderma pigmentosum, basal cell nevus syndrome)
- Typically occurs on sun-exposed areas of the head and neck
- Classic presentation: Pearly papule or nodule with telangiectasias, which may ulcerate, forming a rolled “rodent ulcer” border
- Usually slow growing, locally invasive, and very rare metastasis
- Histology: Nests of basaloid cells with peripheral palisading and retraction clefts
- Common subtypes: Nodular (most common), superficial, morpheaform/sclerosing (more aggressive), pigmented, micronodular
- Diagnosis requires biopsy (shave, punch, excision)
- Treatment options include surgical excision, Mohs surgery (highest cure rates), EDC, cryotherapy, radiation, topical therapy (imiquimod, 5-FU), and Hh inhibitors for advanced cases
- Systemic therapy is appropriate for patients with recurrent, high-risk BCC where surgery and RT are contraindicated.
- Prognosis is excellent; recurrence risk is higher with aggressive subtypes or lesions in high-risk locations (central face, ears, scalp, recurrent tumors)
Enhancing Healthcare Team Outcomes
BCC is the most common human malignancy, primarily affecting sun-exposed skin and arising from mutations in genes regulating the Hh pathway, including PTCH1, SMO, and TP53. Chronic UV exposure is the principal risk factor, causing direct and indirect DNA damage and impairing immune surveillance. BCC typically has an extended latency period, with clinical manifestations often appearing decades after UV-induced DNA damage. While most BCCs are slow-growing and rarely metastasize, prompt diagnosis and appropriate treatment are essential to prevent local tissue destruction and disfigurement. Management ranges from surgical interventions, including MMS, to nonsurgical modalities for select patients.
Providing optimal patient-centered care for individuals with BCC requires a coordinated, interprofessional approach. Dermatologists, surgeons, primary care clinicians, nurses, pharmacists, pathologists, and other healthcare professionals must collaborate to ensure accurate diagnosis, staging, and individualized treatment planning. Effective collaboration involves clearly defined responsibilities, seamless communication, and shared decision-making with the patient and family.
Nurses and advanced practitioners educate patients about sun protection, lesion monitoring, and treatment adherence, while pharmacists review medications to prevent interactions and support safe perioperative management. Pathologists provide precise histologic assessment to guide surgical margins, and surgeons ensure complete tumor excision, particularly for high-risk or cosmetically sensitive lesions.
Care coordinators streamline follow-up appointments and surveillance schedules, reducing delays and minimizing the risk of recurrence. By flattening hierarchical barriers and leveraging the expertise of each team member, the interprofessional team improves patient outcomes, enhances safety, and delivers high-quality, patient-centered care. This team-based approach ensures patients with BCC receive timely, evidence-based management while fostering education, communication, and shared responsibility across disciplines.[28]
Media
(Click Image to Enlarge)

Nodulocystic Basal Cell Carcinoma. The image shows nodulocystic BCC, a rarer variant that may have more than one dermoscopic face and can appear macroscopically benign.
(Click Image to Enlarge)

Pigmented Basal Cell Carcinoma. The photograph shows a pigmented BCC characterized by melanocytes and melanin intermixed with tumor cells. This variant is more frequently seen in the superficial, micronodular, and follicular subtypes.
(Click Image to Enlarge)

Superficial Basal Cell Carcinoma. Superficial BCCs present as a pink-red, scaly, macule or patch, which may contain telangiectasia. They have a predilection for the shoulders, chest, or back, and multiple lesions may be present.
(Click Image to Enlarge)
Micronodular Basal Cell Carcinoma. Histological image showing BCC with micronodular and morpheaform features.
Contributed by Dipti Anand, MD
(Click Image to Enlarge)
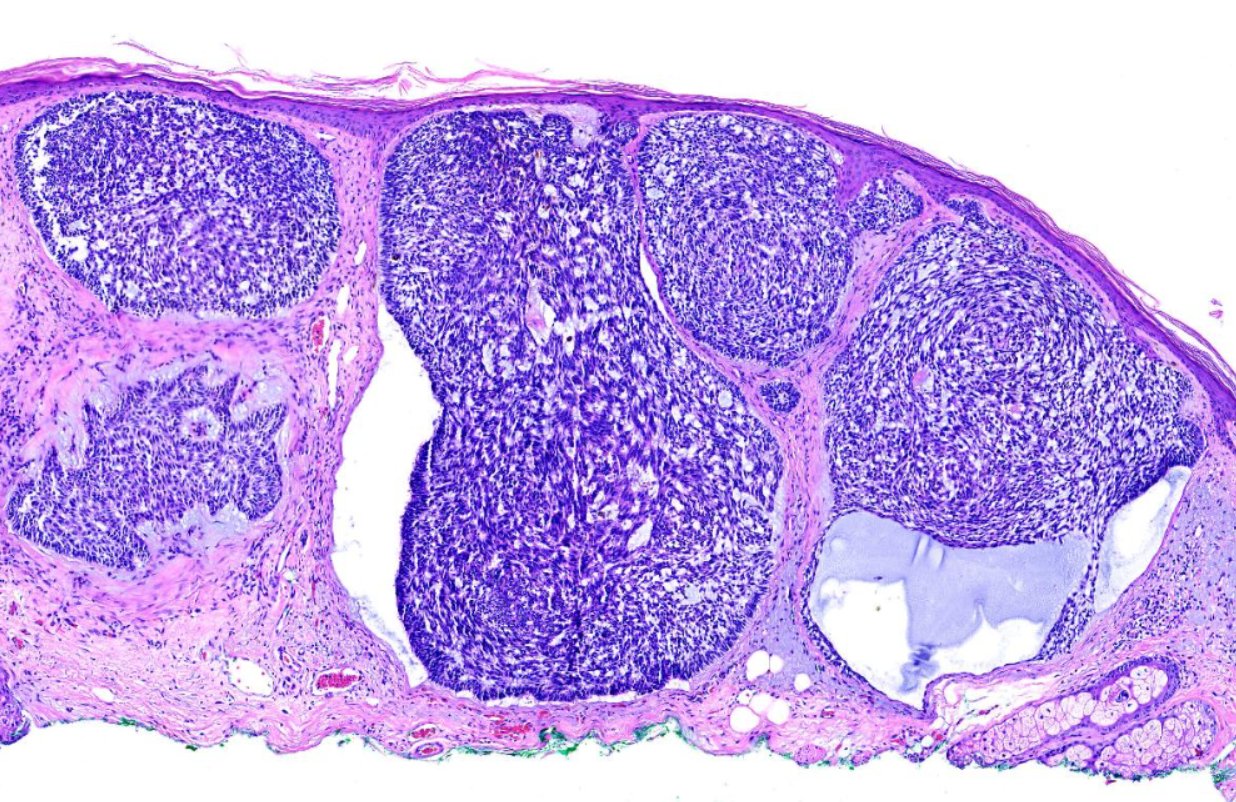
Basal Cell Carcinoma, Nodular. The nodular variant, which accounts for the majority of all cases, consists of islands of basaloid cells with peripheral palisading and a haphazard arrangement of central cells.
Contributed by Dipti Anand, MD
(Click Image to Enlarge)
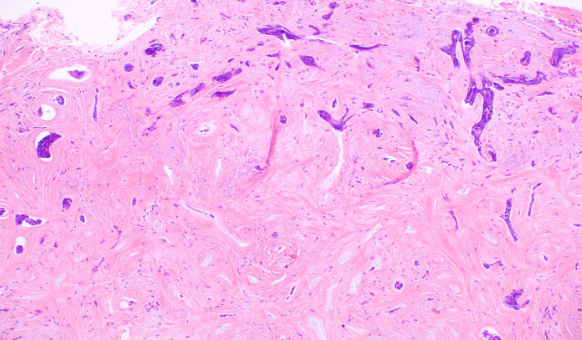
Basal Cell Carcinoma, Morpheaform. The sclerosing (morpheaform) subtype exhibits spiky strands of basaloid cells infiltrating the dermis within a dense fibrous stroma.
Contributed by Dipti Anand, MD
(Click Image to Enlarge)
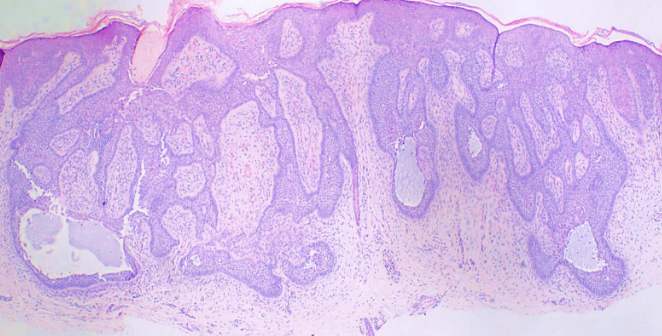
Basal Cell Carcinoma, Fibroepithelioma of Pinkus. Histological findings reveal anastomosing strands and aggregates of basaloid cells within a fibrous stroma.
Contributed by Dipti Anand, MD
(Click Image to Enlarge)
Basal Cell Cancer. Pigmented BCC on the temple, presenting as a darkly pigmented nodule with irregular borders. Pigmentation results from melanin deposition within the tumor cells and adjacent melanocytes, a finding more commonly seen in superficial, micronodular, or follicular variants.
Contributed by Dr. Shyam Verma, MBBS, DVD, FRCP, FAAD, Vadodara, India
(Click Image to Enlarge)

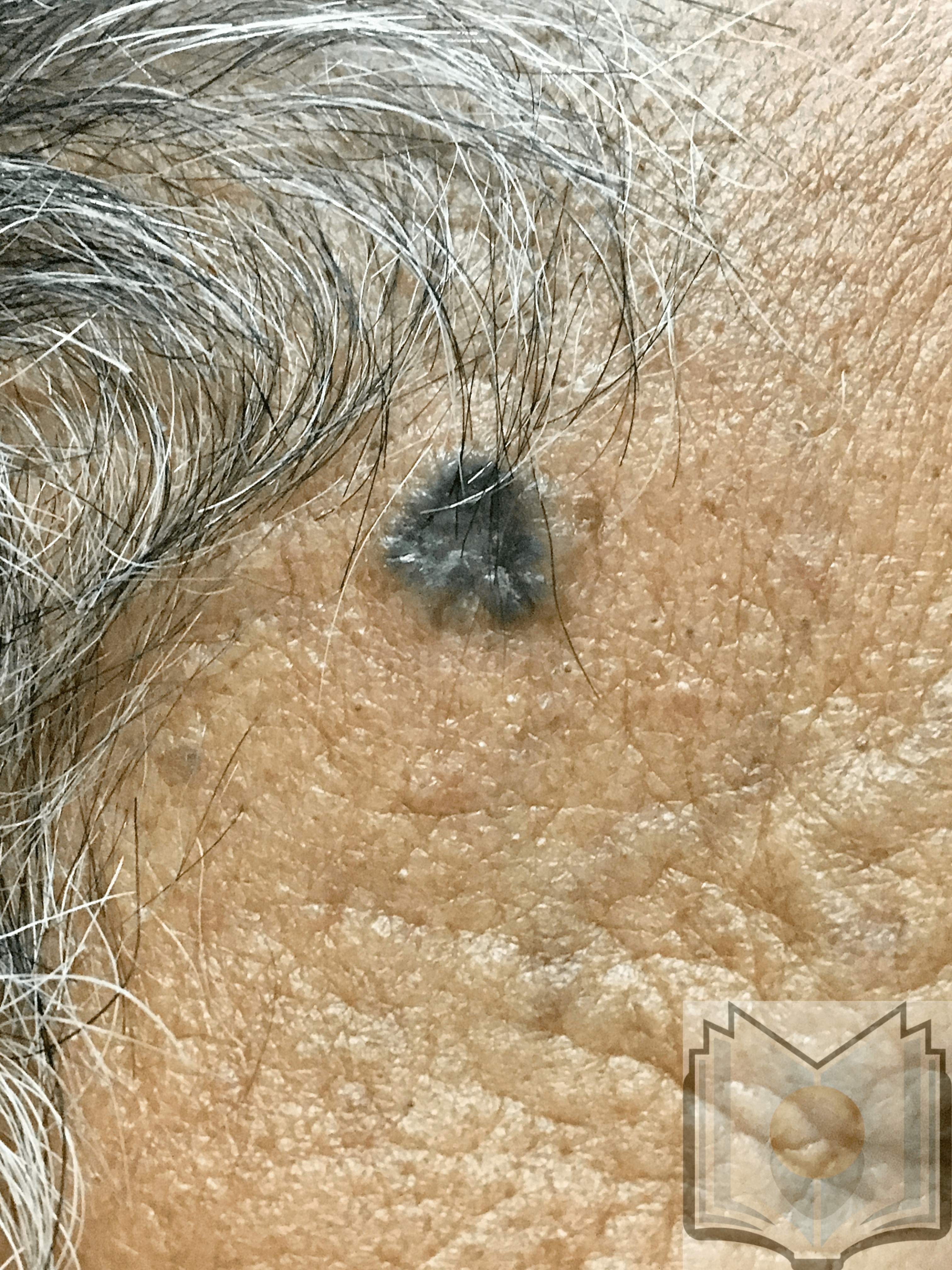
Pigmented Basal Cell Carcinoma of Temple. Pigmented BCC on the temple presenting as a dark, irregularly pigmented nodule with a nodular surface. Pigmentation results from melanin deposition within tumor cells and melanocytes, a feature more often observed in nodular or superficial variants. The clinical presentation can closely resemble melanoma.
Contributed by Dr. Shyam Verma, MBBS, DVD, FRCP, FAAD, Vadodara, India
References
Dai J, Lin K, Huang Y, Lu Y, Chen WQ, Zhang XR, He BS, Pan YQ, Wang SK, Fan WX. Identification of critically carcinogenesis-related genes in basal cell carcinoma. OncoTargets and therapy. 2018:11():6957-6967. doi: 10.2147/OTT.S170504. Epub 2018 Oct 15 [PubMed PMID: 30410353]
De Giorgi V, Savarese I, Gori A, Scarfi F, Topa A, Trane L, Portelli F, Innocenti A, Covarelli P. Advanced basal cell carcinoma: when a good drug is not enough. The Journal of dermatological treatment. 2020 Sep:31(6):552-553. doi: 10.1080/09546634.2018.1542481. Epub 2020 Jan 7 [PubMed PMID: 30388924]
Verkouteren JAC, Ramdas KHR, Wakkee M, Nijsten T. Epidemiology of basal cell carcinoma: scholarly review. The British journal of dermatology. 2017 Aug:177(2):359-372. doi: 10.1111/bjd.15321. Epub 2017 Feb 20 [PubMed PMID: 28220485]
Bauer A, Diepgen TL, Schmitt J. Is occupational solar ultraviolet irradiation a relevant risk factor for basal cell carcinoma? A systematic review and meta-analysis of the epidemiological literature. The British journal of dermatology. 2011 Sep:165(3):612-25. doi: 10.1111/j.1365-2133.2011.10425.x. Epub 2011 Aug 18 [PubMed PMID: 21605109]
Level 1 (high-level) evidenceGandini S, Sera F, Cattaruzza MS, Pasquini P, Picconi O, Boyle P, Melchi CF. Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. European journal of cancer (Oxford, England : 1990). 2005 Jan:41(1):45-60 [PubMed PMID: 15617990]
Level 1 (high-level) evidencePotestio L, Tommasino N, Lauletta G, Salsano A, Lucagnano G, Menna L, Esposito G, Martora F, Megna M. The Impact of Psoriasis Treatments on the Risk of Skin Cancer: A Narrative Review. Advances in therapy. 2024 Oct:41(10):3778-3791. doi: 10.1007/s12325-024-02968-w. Epub 2024 Aug 28 [PubMed PMID: 39196500]
Level 3 (low-level) evidenceUotila I, Siiskonen H, Haimakainen S, Harvima I. Tobacco smoking is associated with cutaneous squamous cell carcinoma but not with basal cell carcinoma or melanoma in adult subjects at risk of skin cancer: A cross-sectional study. Tobacco induced diseases. 2024:22():. doi: 10.18332/tid/185299. Epub 2024 May 14 [PubMed PMID: 38745594]
Level 2 (mid-level) evidenceRogers HW, Weinstock MA, Harris AR, Hinckley MR, Feldman SR, Fleischer AB, Coldiron BM. Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Archives of dermatology. 2010 Mar:146(3):283-7. doi: 10.1001/archdermatol.2010.19. Epub [PubMed PMID: 20231499]
Level 2 (mid-level) evidenceKaria PS, Han J, Schmults CD. Cutaneous squamous cell carcinoma: estimated incidence of disease, nodal metastasis, and deaths from disease in the United States, 2012. Journal of the American Academy of Dermatology. 2013 Jun:68(6):957-66. doi: 10.1016/j.jaad.2012.11.037. Epub 2013 Feb 1 [PubMed PMID: 23375456]
Snow SN, Sahl W, Lo JS, Mohs FE, Warner T, Dekkinga JA, Feyzi J. Metastatic basal cell carcinoma. Report of five cases. Cancer. 1994 Jan 15:73(2):328-35 [PubMed PMID: 8293396]
Level 3 (low-level) evidenceSkoda AM, Simovic D, Karin V, Kardum V, Vranic S, Serman L. The role of the Hedgehog signaling pathway in cancer: A comprehensive review. Bosnian journal of basic medical sciences. 2018 Feb 20:18(1):8-20. doi: 10.17305/bjbms.2018.2756. Epub 2018 Feb 20 [PubMed PMID: 29274272]
Trieu KG, Tsai SY, Eberl M, Ju V, Ford NC, Doane OJ, Peterson JK, Veniaminova NA, Grachtchouk M, Harms PW, Swartling FJ, Dlugosz AA, Wong SY. Basal cell carcinomas acquire secondary mutations to overcome dormancy and progress from microscopic to macroscopic disease. Cell reports. 2022 May 3:39(5):110779. doi: 10.1016/j.celrep.2022.110779. Epub [PubMed PMID: 35508126]
Niculet E, Craescu M, Rebegea L, Bobeica C, Nastase F, Lupasteanu G, Stan DJ, Chioncel V, Anghel L, Lungu M, Tatu AL. Basal cell carcinoma: Comprehensive clinical and histopathological aspects, novel imaging tools and therapeutic approaches (Review). Experimental and therapeutic medicine. 2022 Jan:23(1):60. doi: 10.3892/etm.2021.10982. Epub 2021 Nov 18 [PubMed PMID: 34917186]
Stanoszek LM, Wang GY, Harms PW. Histologic Mimics of Basal Cell Carcinoma. Archives of pathology & laboratory medicine. 2017 Nov:141(11):1490-1502. doi: 10.5858/arpa.2017-0222-RA. Epub [PubMed PMID: 29072946]
Weber P, Tschandl P, Sinz C, Kittler H. Dermatoscopy of Neoplastic Skin Lesions: Recent Advances, Updates, and Revisions. Current treatment options in oncology. 2018 Sep 20:19(11):56. doi: 10.1007/s11864-018-0573-6. Epub 2018 Sep 20 [PubMed PMID: 30238167]
Level 3 (low-level) evidenceDrucker AM, Adam GP, Rofeberg V, Gazula A, Smith B, Moustafa F, Weinstock MA, Trikalinos TA. Treatments of Primary Basal Cell Carcinoma of the Skin: A Systematic Review and Network Meta-analysis. Annals of internal medicine. 2018 Oct 2:169(7):456-466. doi: 10.7326/M18-0678. Epub 2018 Sep 18 [PubMed PMID: 30242379]
Level 1 (high-level) evidencePatel K, Migden M. Mohs Micrographic Surgery: Chemotherapeutic Agents Used in Cutaneous Oncology. StatPearls. 2026 Jan:(): [PubMed PMID: 40334041]
Gupta RK, Parvadiya L, Dudhat K. Advancements in Skin Cancer Prevention and Treatment: Harnessing Technology, Natural Therapies, and Emerging Diagnostic Approaches. Critical reviews in therapeutic drug carrier systems. 2025:42(5):1-54. doi: 10.1615/CritRevTherDrugCarrierSyst.2025053255. Epub [PubMed PMID: 40743615]
Noy MA, Rich BJ, Llorente R, Kwon D, Abramowitz M, Mahal B, Mellon EA, Zaorsky NG, Dal Pra A. Levels of Evidence for Radiation Therapy Recommendations in the National Comprehensive Cancer Network (NCCN) Clinical Guidelines. Advances in radiation oncology. 2022 Jan-Feb:7(1):100832. doi: 10.1016/j.adro.2021.100832. Epub 2021 Oct 29 [PubMed PMID: 34869943]
Level 3 (low-level) evidenceMoreno-Arrones OM, Béa-Ardebol S, Mayo-Martinez F, Pérez-Pastor G, Torres-Navarro I, Bonfill-Ortí M, Deza G, Ruiz-Salas V, Masferrer E, Feal C, Turrión-Merino L, Toll A, Yébenes M, Galiano-Mejías S, Jaka A, Ferrandiz-Pulido C, Florez A, Hernández-Hernández N, Fernández-de-Misa R, Rios-Buceta L, Sanmartin O. Sonidegib as a Locally Advanced Basal Cell Carcinoma Therapy in Real-life Clinical Setting: A National Multicentre Study. Actas dermo-sifiliograficas. 2023 Jul-Aug:114(7):565-571. doi: 10.1016/j.ad.2023.04.022. Epub 2023 Apr 23 [PubMed PMID: 37088285]
Gambini D, Passoni E, Nazzaro G, Beltramini G, Tomasello G, Ghidini M, Kuhn E, Garrone O. Basal Cell Carcinoma and Hedgehog Pathway Inhibitors: Focus on Immune Response. Frontiers in medicine. 2022:9():893063. doi: 10.3389/fmed.2022.893063. Epub 2022 Jun 14 [PubMed PMID: 35775005]
Stratigos AJ, Sekulic A, Peris K, Bechter O, Prey S, Kaatz M, Lewis KD, Basset-Seguin N, Chang ALS, Dalle S, Orland AF, Licitra L, Robert C, Ulrich C, Hauschild A, Migden MR, Dummer R, Li S, Yoo SY, Mohan K, Coates E, Jankovic V, Fiaschi N, Okoye E, Bassukas ID, Loquai C, De Giorgi V, Eroglu Z, Gutzmer R, Ulrich J, Puig S, Seebach F, Thurston G, Weinreich DM, Yancopoulos GD, Lowy I, Bowler T, Fury MG. Cemiplimab in locally advanced basal cell carcinoma after hedgehog inhibitor therapy: an open-label, multi-centre, single-arm, phase 2 trial. The Lancet. Oncology. 2021 Jun:22(6):848-857. doi: 10.1016/S1470-2045(21)00126-1. Epub 2021 May 14 [PubMed PMID: 34000246]
Lear JT, Harwood CA, Hasan Z, Kentley J, Thomson J, Khoo A, Alderman A, DeSouza M, Epstein EH Jr, Kochendoerfer GG, Tang JY. Topical application of the Hedgehog inhibitor patidegib in patients with Gorlin syndrome: a phase II trial. The British journal of dermatology. 2025 Mar 18:192(4):611-617. doi: 10.1093/bjd/ljae444. Epub [PubMed PMID: 39545486]
Cosio T, Di Prete M, Di Raimondo C, Garofalo V, Lozzi F, Lanna C, Dika E, Orlandi A, Rapanotti MC, Bianchi L, Campione E. Patidegib in Dermatology: A Current Review. International journal of molecular sciences. 2021 Oct 3:22(19):. doi: 10.3390/ijms221910725. Epub 2021 Oct 3 [PubMed PMID: 34639065]
Breglio KF, Knox KM, Hwang J, Weiss R, Maas K, Zhang S, Yao L, Madden C, Xu Y, Hartman RI, Wheless L. Nicotinamide for Skin Cancer Chemoprevention. JAMA dermatology. 2025 Nov 1:161(11):1140-1147. doi: 10.1001/jamadermatol.2025.3238. Epub [PubMed PMID: 40960808]
Reinhold U, Dirschka T, Ostendorf R, Aschoff R, Berking C, Philipp-Dormston WG, Hahn S, Lau K, Jäger A, Schmitz B, Lübbert H, Szeimies RM. A randomized, double-blind, phase III, multicentre study to evaluate the safety and efficacy of BF-200 ALA (Ameluz(®) ) vs. placebo in the field-directed treatment of mild-to-moderate actinic keratosis with photodynamic therapy (PDT) when using the BF-RhodoLED(®) lamp. The British journal of dermatology. 2016 Oct:175(4):696-705. doi: 10.1111/bjd.14498. Epub 2016 Jun 25 [PubMed PMID: 26921093]
Level 1 (high-level) evidenceSutrisno CSN, Pramita DH, Dewi IP. Curative or Conservative Approaches: A Systematic Review of Surgical and Nonsurgical Treatments for Basal Cell Carcinoma. Cureus. 2025 Oct:17(10):e95556. doi: 10.7759/cureus.95556. Epub 2025 Oct 28 [PubMed PMID: 41163634]
Level 1 (high-level) evidenceThevissen J, Schmitz MT, Schmid M, Ko YD, Jacobs AH, Jaehde U. Interprofessional, risk-adapted medication management in older patients with cancer (IrMa). Journal of geriatric oncology. 2025 Nov:16(8):102359. doi: 10.1016/j.jgo.2025.102359. Epub 2025 Aug 29 [PubMed PMID: 40884933]