Introduction
Enophthalmos is defined as the posterior displacement of the globe within the anteroposterior plane of the orbit, producing the clinical impression of a sunken eye (see Image. Orbit, Anterior View). The condition represents a descriptive clinical finding rather than a diagnosis, indicating an underlying imbalance among orbital structures. Under normal conditions, the globe occupies a stable position within the orbital cavity, maintained by equilibrium among the bony orbital walls, orbital fat, extraocular muscles, connective tissue septae, and vascular components. Disruption of this anatomical harmony—whether from trauma, inflammation, infection, congenital anomalies, or degenerative processes—can result in globe displacement. Recognition of enophthalmos provides a significant clinical clue to local and systemic pathologies affecting the orbit.
Differentiation from pseudo-enophthalmos, which reflects an apparent posterior position of the globe due to structural asymmetry or ocular abnormalities, is essential.[1] Common causes of pseudo-enophthalmos include microphthalmos, phthisis bulbi, and anophthalmic socket, in which a small or absent globe produces a deceptive impression of posterior displacement. Globe malpositions, such as hyperglobus, hypoglobus, esoglobus, or exoglobus, as well as contralateral proptosis, can also simulate enophthalmos. Accurate distinction between true and pseudo-enophthalmos is critical for appropriate diagnosis and management.[2]
Clinically, enophthalmos manifests as a posteriorly displaced globe, often accompanied by a deep superior sulcus (superior sulcus deformity) and a hollowed periorbital contour. Eyelid position may be variably affected, including ptosis, retraction, or lagophthalmos, and severe cases can result in functional disturbances such as diplopia, restricted ocular motility, or impaired eyelid closure.[3][4] The opposite clinical finding is proptosis (exophthalmos), defined by anterior displacement of the globe. While proptosis is often more overt due to its cosmetic prominence, enophthalmos typically develops gradually and may remain unnoticed until functional or aesthetic complications arise.
From an anatomical perspective, the orbit is a pyramidal cavity formed by the frontal, zygomatic, maxillary, ethmoid, lacrimal, sphenoid, and palatine bones. The orbital cavity contains the globe, extraocular muscles, adipose tissue, neurovascular structures, and fascial septae, which collectively cushion and stabilize the eyeball. Approximately 40% of the orbital volume consists of fat, a critical determinant of globe position. The integrity of the orbital walls and the volume of soft tissue together define ocular projection.
The pathophysiology of enophthalmos can be classified into 3 principal mechanisms: loss or atrophy of orbital fat, structural expansion of the bony orbit, and fibrosis or scarring of orbital soft tissues that retract the globe posteriorly. Posttraumatic enophthalmos is one of the most common acquired forms, typically resulting from blowout fractures of the orbital floor or medial wall. Herniation of orbital fat into adjacent sinuses increases the effective orbital volume, displacing the globe posteriorly. Chronic maxillary sinusitis, also referred to as “silent sinus syndrome,” can similarly produce progressive inward bowing of the orbital floor, resulting in spontaneous enophthalmos in the absence of overt trauma.[5][6]
Inflammatory and infectious processes can also alter orbital anatomy. Chronic granulomatous disease, orbital pseudotumor, and postinflammatory fibrosis may lead to contracture of periorbital tissues and scarring, tethering the globe. Iatrogenic causes include radiotherapy-induced fat atrophy and fibrosis, often observed after orbital irradiation for malignancies such as retinoblastoma or nasopharyngeal carcinoma. Progressive hemifacial atrophy (Parry-Romberg syndrome) and scleroderma can produce localized orbital tissue loss, contributing to unilateral enophthalmos.
Congenital and developmental anomalies also contribute to enophthalmos. Microphthalmos and craniofacial malformations, such as Crouzon or Apert syndromes, may result in asymmetric globe positioning. In these cases, the apparent enophthalmos arises from dysmorphic orbital bones or reduced globe size rather than true posterior displacement. Postsurgical and postenucleation socket contracture can similarly simulate enophthalmos due to inadequate prosthetic support or soft tissue scarring.[7]
The natural history of enophthalmos is largely determined by its underlying etiology. Traumatic cases may become apparent weeks to months after the initial injury, as edema resolves and tissue remodeling occurs. Inflammatory or degenerative causes typically progress gradually, with slow orbital fat loss or fibrosis resulting in increasing asymmetry. Early recognition and intervention are critical, as chronic enophthalmos can lead to secondary changes, including fibrosis of the extraocular muscles, restrictive strabismus, and orbital volume distortion, which complicate reconstructive efforts.[8]
Clinical assessment requires careful inspection of facial symmetry in multiple gaze positions and measurement using exophthalmometry. A difference greater than 2 mm between both eyes is generally considered significant. Palpation of orbital rims may reveal step deformities in posttraumatic cases, while ocular motility assessment evaluates extraocular muscle involvement. Imaging, particularly high-resolution computed tomography (CT), provides detailed information regarding orbital wall integrity, fat distribution, and muscle morphology. Magnetic resonance imaging (MRI) offers superior soft-tissue resolution, facilitating differentiation between fat atrophy, fibrosis, and infiltrative lesions.[9]
A detailed understanding of orbital anatomy is essential for correlating clinical findings with radiologic evidence. The inferior orbital wall, thin and adjacent to the maxillary sinus, is the most common site of trauma-induced defects. The medial wall, composed of the lamina papyracea of the ethmoid bone, is also susceptible. Expanding these walls increases the volume of the orbital cavity, and even minor volumetric changes can substantially alter the globe's position due to the confined orbital space. Conversely, reduction of retrobulbar soft tissue volume, particularly adipose tissue, produces posterior displacement of the globe without skeletal alteration.[10]
Orbital pathology influencing enophthalmos varies widely. Inflammatory and infectious processes may extend from adjacent sinuses, particularly the maxillary and ethmoidal sinuses, causing osteolysis and remodeling of the orbital walls. Malignant lesions, such as metastatic carcinoma or orbital lymphoma, may induce bone resorption and fibrosis, indirectly contributing to enophthalmos. Infiltrative processes that primarily expand orbital tissues, such as thyroid-associated orbitopathy, typically cause proptosis but may also produce secondary enophthalmos during the fibrotic phase.[11]
Enophthalmos has substantial functional and aesthetic consequences. The sunken appearance of the eye, combined with asymmetrical eyelid contour, can lead to psychological distress and self-consciousness. Functionally, altered globe position impairs binocular vision, restricts ocular motility, and disrupts tear film dynamics, predisposing to exposure keratopathy. Lagophthalmos and incomplete lid closure exacerbate ocular surface compromise, particularly when associated with facial nerve dysfunction or cicatricial lid changes.[12][13]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Enophthalmos may be classified as congenital or acquired based on onset and clinical presentation. Management strategies differ according to etiology and the specific structural or functional abnormalities present.[14]
Congenital Enophthalmos
Congenital enophthalmos frequently occurs in association with craniofacial syndromes or conditions involving facial bony dysplasia. Syndromes such as Treacher-Collins, Crouzon, Apert, and Goldenhar often feature hypoplasia of the zygomatic or maxillary bones, resulting in facial asymmetry and ipsilateral enophthalmos. Bony dysplasia affecting nonfacial cranial bones, such as sphenoid wing dysplasia in neurofibromatosis 1, can also contribute. Disorders of globe development, including congenital microphthalmos without cyst, cryptophthalmos, and anophthalmia, are commonly associated with pseudo-enophthalmos.
Acquired Enophthalmos
Acquired enophthalmos results from alterations in orbital anatomy or physiology. The 3 primary mechanisms include enlargement of the bony orbit, reduction in the volume of orbital contents, and shrinkage or contracture of existing orbital tissues. Enlargement of the orbit may result from defects or displacement of 1 or more orbital walls. Common causes include orbital fractures, involutional changes in orbital structure, and silent sinus syndrome. Reduction of orbital contents arises from age-related fat atrophy, systemic lipodystrophy, linear (localized) scleroderma, Parry-Romberg syndrome, or drug-induced lipoatrophy. Additional contributors include long-standing orbital varix, radiotherapy, orbital surgery, and prior orbital trauma. Shrinkage or contracture of orbital tissues may result from metastatic orbital disease, as seen in scirrhous breast cancer; fibrosis of extraocular muscles, as in congenital fibrosis of extraocular muscles and Duane retraction syndrome; or sequelae of orbital trauma.
Specific Mechanisms and Clinical Associations
Traumatic causes of enophthalmos result from increased orbital volume due to fracture or displacement of the bony walls, often accompanied by herniation of orbital fat into adjacent sinuses. Common examples include blowout fractures of the orbital floor or medial wall, zygomaticomaxillary complex fractures, and late posttraumatic fibrosis or atrophy. Key distinguishing features comprise a history of trauma, step deformity of the infraorbital rim, restricted ocular motility, a positive forced duction test, and CT demonstrating orbital wall defects or fat herniation.
Postsurgical and iatrogenic enophthalmos arises from orbital volume changes or fat loss following surgical or therapeutic interventions. Representative conditions include overcorrection in orbital decompression for thyroid eye disease, excessive fat removal during blepharoplasty producing a “hollowed eye,” postenucleation socket contracture, and orbital irradiation for tumors. Clinical clues include a history of prior surgery or radiation, gradual development of hollowing, and periorbital scarring, cicatrix formation, or socket contracture.
Inflammatory and infectious disorders induce fibrosis and scarring of orbital tissues secondary to chronic inflammation or infection, leading to globe retraction. Examples include chronic orbital cellulitis, granulomatous conditions such as Wegener granulomatosis and sarcoidosis, sclerosing orbital pseudotumor, and chronic sinusitis, including silent sinus syndrome. Distinguishing features consist of progressive onset, tenderness or evidence of prior inflammation, associated sinus pathology, and CT demonstrating inward bowing of the orbital floor with sinus opacification.
Neoplastic causes of enophthalmos result from local invasion, fibrosis, or bone resorption caused by tumor infiltration, leading to posterior displacement of the globe. Examples include metastatic carcinoma (breast, prostate), scirrhous orbital tumors, lymphoma with fibrosing response, and posttreatment fibrosis following radiotherapy. Key distinguishing features include slowly progressive unilateral enophthalmos, often painless; a firm orbital mass; and CT or MRI evidence of an infiltrative lesion with fat replacement.
Congenital and developmental anomalies involve a small or malformed orbital cavity or globe, or abnormal orbital bone growth. Clinical associations include microphthalmos, Crouzon, Apert, or Pfeiffer craniofacial syndromes, and congenital anophthalmos or hypoplastic orbit. Presentation occurs at birth or early childhood, is often bilateral in syndromic cases, and is accompanied by craniofacial deformities. Degenerative and atrophic conditions arise from loss of orbital fat volume due to lipodystrophy or senile atrophy, or from soft tissue degeneration. Examples include age-related fat atrophy (senile enophthalmos), progressive hemifacial atrophy (Parry-Romberg syndrome), scleroderma, and postinflammatory or postradiation atrophy. Onset is gradual and insidious, presenting with periorbital hollowing that may involve the entire hemiface, with normal orbital walls on imaging.
Infectious sinus pathology may cause enophthalmos through chronic disease, leading to maxillary sinus collapse and descent of the orbital floor. Silent sinus syndrome and chronic maxillary sinusitis with osteolysis represent common associations. Clinical features include spontaneous onset without trauma, enophthalmos with hypoglobus, and CT evidence of inward displacement of the orbital floor with sinus opacification.
Postinflammatory fibrosis, or cicatricial changes, results from fibroconnective tissue contraction within the orbit following severe inflammation or injury. Clinical associations include orbital cellulitis sequelae, chemical or thermal burns, and cicatricial changes postsurgery or infection. Key features include globe restriction, periorbital scarring, reduced retropulsion, and a typically nonprogressive course once fibrosis stabilizes.
Systemic and metabolic disorders cause enophthalmos through fat loss or redistribution secondary to systemic metabolic imbalance. Examples include HIV-related lipodystrophy, cachexia from malignancy or chronic illness, corticosteroid withdrawal, and generalized lipoatrophy syndromes. The clinical presentation includes bilateral, symmetrical enophthalmos, a hollowed facial appearance, and a history of chronic disease or medication use.
Neurologic or vasculopathic causes lead to denervation- or ischemia-induced atrophy of orbital fat and muscles. Associations include sympathetic denervation (Horner syndrome with orbital atrophy) and chronic ischemic orbital disease. Key distinguishing features comprise ptosis, miosis, anhidrosis, unilateral mild enophthalmos, and confirmation through neurologic testing. Idiopathic enophthalmos arises in the absence of identifiable structural, inflammatory, or metabolic causes. Examples include spontaneous idiopathic fat atrophy and early or limited forms of connective tissue disorders. Diagnosis is by exclusion, with slow progression and normal imaging except for reduced fat volume.
Epidemiology
The normal position of the globe varies by sex, age, and ethnicity. Enophthalmos occurs more frequently in males than in females.[15] The most common cause is oculofacial trauma and its sequelae. Compared with proptosis, enophthalmos is relatively uncommon, and its true prevalence is difficult to determine because of its varied etiologies and often subtle presentation. Enophthalmos represents a manifestation of multiple orbital pathologies—traumatic, inflammatory, degenerative, or iatrogenic—rather than a single disease entity. Therefore, epidemiologic data are typically reported according to the underlying cause rather than enophthalmos itself.
In the United States and Europe, trauma remains the leading cause of acquired enophthalmos, accounting for up to 40% to 60% of reported cases. Orbital floor and medial wall blowout fractures are widespread among young men aged 20 to 40 years, consistent with higher exposure to road traffic accidents, sports injuries, and interpersonal violence. Male patients predominate in this subgroup, with a male-to-female ratio of approximately 3:1. Late posttraumatic enophthalmos often develops several weeks to months after injury as orbital edema resolves and herniated orbital fat undergoes fibrosis or atrophy.[16]
In contrast, involutional and degenerative causes demonstrate a clear female preponderance and typically occur later in life. Senile enophthalmos, resulting from age-related orbital fat atrophy and skeletal remodeling, is particularly frequent in postmenopausal women due to hormonal influences on fat distribution. This physiologic orbital hollowing contributes to the characteristic sunken-eye appearance of aging and is often bilateral, although asymmetric fat loss can produce unilateral presentation.
Silent sinus syndrome, a relatively rare but increasingly recognized cause of enophthalmos, predominantly affects middle-aged adults without a strong sex predilection. The condition arises from chronic maxillary sinus atelectasis, producing inward bowing of the orbital floor. Epidemiologic studies from the United States and Europe estimate the annual incidence of this condition at approximately 2 to 3 per 100,000, although underdiagnosis is common due to the insidious onset.
In Asia and developing countries, traumatic and infectious causes dominate the epidemiologic profile. Chronic sinusitis-related orbital remodeling and postinflammatory fibrosis remain significant contributors in tropical and subtropical regions, where delayed access to surgical repair and recurrent infection increase the risk of late orbital deformities. Iatrogenic causes, such as orbital irradiation for retinoblastoma, nasopharyngeal carcinoma, or Graves orbitopathy, are more frequent in populations with higher rates of head and neck malignancies, particularly in East and Southeast Asia.
Although rare, neoplastic causes of enophthalmos display distinct demographic patterns. Metastatic breast carcinoma is the most frequent malignant cause in adults, especially among middle-aged and older women. Scirrhous infiltration and fibrosis of orbital fat result in gradual, painless posterior displacement of the globe. Study results report that up to 10% to 20% of women with orbital metastases from breast cancer present with enophthalmos as a key clinical feature. Other malignancies, including prostate carcinoma and lymphoma, contribute smaller proportions, more often affecting older men.
Congenital and developmental forms of enophthalmos, including those associated with craniofacial dysostoses (Apert, Crouzon, Pfeiffer syndromes) or microphthalmos, are primarily observed in pediatric and adolescent populations. These cases frequently coexist with additional craniofacial anomalies, complicating epidemiologic differentiation. The overall incidence is exceedingly low, estimated at less than 1 per 100,000 live births for syndromic craniosynostoses with orbital dysmorphia.
Iatrogenic enophthalmos following orbital or eyelid surgery has gained attention with the increasing popularity of cosmetic blepharoplasty. Overaggressive fat removal or scarring from prior procedures can produce secondary hollowing of the orbit. In Western cosmetic surgery data, mild-to-moderate enophthalmos after upper or lower lid blepharoplasty occurs in 2% to 4% of patients, predominantly among women aged 40 to 65 years. Postorbital decompression enophthalmos may develop in 5% to 10% of cases treated for thyroid eye disease due to overcorrection of proptosis.
Geographic variation in the frequency of enophthalmos causes is notable. In developed countries, trauma, age-related atrophy, and iatrogenic factors account for most cases, reflecting advanced healthcare systems and higher rates of elective orbital and cosmetic surgery. In developing regions, delayed management of sinus infections, orbital cellulitis, and fractures increases the incidence of secondary or postinflammatory enophthalmos. Radiation-induced atrophy remains a significant contributor in areas with limited access to tissue-sparing oncologic therapy.
The age distribution of enophthalmos is bimodal. The first peak occurs in young adults (aged 20–40) and is primarily trauma-related. In contrast, the second occurs in older adults (aged 55 and older) and is associated with degenerative and iatrogenic causes. Pediatric enophthalmos is uncommon and typically arises from congenital causes, silent sinus syndrome, or postinfectious scarring. Unilateral enophthalmos predominates, usually following localized pathology such as trauma, tumor, or sinus disease. Bilateral involvement occurs more frequently in systemic or degenerative conditions, including senile fat atrophy or scleroderma. Mild enophthalmos (1–2 mm) is often underrecognized but may be cosmetically significant in symmetric faces, while severe displacement (>3 mm) frequently produces diplopia or orbital volume imbalance.[17]
Globally, the estimated prevalence of clinically significant enophthalmos (posterior globe displacement ≥2 mm) is 0.1% to 0.3% of ophthalmic outpatient visits, with most cases attributable to prior trauma or surgery. True prevalence is likely higher due to underreporting of subtle cases and the presence of diverse etiologies. Sex distribution varies by cause. Trauma-related enophthalmos shows a male predominance, whereas senile and iatrogenic forms predominate in female individuals. No definitive racial predilection exists, although orbital anatomy and craniofacial morphology may influence clinical detection thresholds.
Enophthalmos is an uncommon but clinically significant finding across all age groups and geographic regions. The frequency of this condition is greatest among men with orbital trauma and women with degenerative fat atrophy or prior surgical history. Global trends indicate a gradual shift toward iatrogenic and involutional causes as trauma-related enophthalmos declines with improved safety measures and orbital reconstruction techniques. Awareness of these epidemiologic patterns facilitates identification of at-risk populations, early diagnosis, and the development of preventive and rehabilitative strategies.[18]
Pathophysiology
The pathophysiology of enophthalmos varies depending on the etiology. These mechanisms are explained below.
Facial Trauma and Sequelae
The sequence of events typically begins with orbital trauma. Orbitofacial damage may occur during sports activities, road traffic accidents, physical assault, or endonasal surgery. The most common injury is a blowout fracture, particularly involving the orbital floor. An isolated blowout fracture expands the orbital cavity along the medial or inferior walls. Herniation of orbital contents, including fat, muscle, and the globe, frequently results in enophthalmos. The inferomedial strut of the orbit, formed by the palatine bone's orbital plate, serves as a critical landmark. Injury to the strut, located at the junction of the medial and inferior orbital walls, can cause globe luxation or hypoglobus.
Maxillofacial injuries, such as zygomaticomaxillary complex disruptions and Le Fort type II and III fractures, are also associated with enophthalmos. Isolated lateral wall or roof fractures rarely produce significant enophthalmos because inward displacement of fragments results in a blow-in configuration. However, extensive lateral wall fractures may lead to fat loss into the temporal fossa, resulting in enophthalmos. Immediately after trauma, patients often present with periorbital edema, eyelid ecchymosis, chemosis, and ptosis, which can mask enophthalmos. Enophthalmos typically becomes evident as periorbital swelling resolves, usually within 1 to 3 weeks posttrauma. Large fractures exceeding 150 mm2 are highly likely to result in significant enophthalmos.[19]
Beyond 3 weeks, some patients develop secondary orbital changes that cause progressive enophthalmos over subsequent months. Posttraumatic orbital ischemia can lead to fat atrophy, producing gradual globe retraction. Compression of orbital contents from periorbital swelling may also induce lipoatrophy, hollowness, and skeletonization of periorbital features. Severe orbital trauma, particularly with hemorrhage or hematoma, can cause orbital fat loss and enophthalmos, even in the absence of facial fractures.
Involutional Changes in the Orbit
Advancing age is associated with enlargement of the orbital cavity due to resorption of the inner table of the orbital bones, resulting in horizontal and oblique orbital expansion. This transformation produces enophthalmos, hypoglobus, deep superior sulcus, and facial skeletonization. Soft-tissue changes include lipoatrophy, typically beginning in the third decade and progressing gradually with age.[20] Loss of orbital fat reduces supportive elements within the orbit, contributes to volume loss in the temples and cheeks, and causes posterior displacement of the globe.
Specific named entities are associated with senile enophthalmos. Giant fornix syndrome arises from the gradual weakening of the levator aponeurosis and orbital septum, deepening the fornices, promoting tear stagnation, and occasionally leading to superimposed infections. These infections, together with enophthalmos and lagophthalmos, often compromise the ocular surface.[21] Senile sunken-eye syndrome is another variant, in which lipoatrophy deepens the superior sulcus, alters upper eyelid position through ptosis or retraction, and results in lagophthalmos.[22]
Pathologies within the Orbit
Congenital orbital pathologies, including microphthalmos, congenital cystic eye, anophthalmos, and cryptophthalmos, may be associated with bony socket contracture, resulting in pseudo-enophthalmos. Acquired orbital lesions are classified as either periodically expansile and collapsible masses, such as orbital varices, or fibrosing etiologies, including congenital fibrosis of the extraocular muscles (CFEOM) and orbital metastases and Duane retraction syndrome (DRS). Orbital varices typically present with pain or proptosis that fluctuates with head position and the Valsalva maneuver. Repeated expansion and contraction of the venous anomaly may lead to orbital fat atrophy and subsequent enophthalmos. Orbital metastasis, accounting for 1% to 13% of orbital tumors, can produce enophthalmos, particularly in metastatic scirrhous breast cancer, in contrast to the proptosis usually seen with metastatic lesions.[23] Fibrotic infiltration of orbital soft tissues results in globe retraction, while replacement of orbital adipocytes by metastatic cells and fat necrosis leads to collagen deposition and contraction of orbital tissues.
CFEOM is a nonprogressive, bilateral congenital disorder characterized by restrictive ophthalmoplegia, strabismus, severe ptosis, a chin-up head position due to eyes fixed in downgaze, and enophthalmos. The condition arises from hypoplasia of the extraocular muscles secondary to congenital oculomotor nerve affliction. DRS has a similar mechanism, involving congenital denervation of the lateral rectus muscle with misinnervation by the oculomotor nerve, producing cocontraction of the medial and lateral recti and enophthalmos on attempted adduction.
Pathologies Around the Orbit
Pathologies of the sinuses, cranial bones, and soft tissues of the upper and midface can alter the position of the globe, resulting in enophthalmos. Variations in orbital anatomy, tissue elasticity, and chronicity of the pathology determine the severity and clinical presentation. Maxillary sinus aplasia, observed historically in the Middle Ages, may present with enophthalmos. Silent sinus syndrome typically presents with painless, progressive unilateral enophthalmos, vertical diplopia, mild-to-moderate facial asymmetry, lagophthalmos, and hypoglobus. The mechanism involves a vacuum effect resulting from the disruption of maxillary sinus drainage into the middle meatus. The most common trigger is lateralization of the middle turbinate, which blocks the maxillary sinus ostium and leads to fluid accumulation. Gradual reabsorption of this fluid generates negative pressure and a downward force on the orbital floor.[24]
Developmental dysplasia of the greater wing of the sphenoid in neurofibromatosis type 1 (NF-1) syndrome results in orbital expansion and enophthalmos. An associated frontal meningocoele or encephalocoele may cause transient pulsatile proptosis, exacerbated by coughing or straining. Plexiform neurofibroma in NF-1 can chronically compress the globe, inducing lipoatrophy and enophthalmos. Localized scleroderma, an inflammatory autoimmune condition, is characterized by sclerosis of the skin and subcutaneous tissue. Morphea en coup de sabre produces linear lesions on the frontoparietal scalp and forehead, resembling a sword strike. Progressive, painless enophthalmos, restriction of upgaze, and diplopia are common clinical features. Parry-Romberg syndrome is characterized by hemifacial lipodystrophy with loss of dermal and subcutaneous fat. The condition primarily affects adolescent girls and progresses slowly. Clinical presentations include thin facial skin with hyperpigmentation, mouth deviation, and ocular manifestations such as enophthalmos, ptosis, restrictive strabismus, coloboma, heterochromia, and uveitis.
Systemic Diseases
Specific congenital syndromes affecting the first branchial arch cause hypoplasia of the maxillary and zygomatic bones, resulting in orbital maldevelopment and either proptosis or enophthalmos. Frequently encountered syndromes include Goldenhar, Apert, Crouzon, and Treacher-Collins. Systemic lipodystrophy syndromes involve abnormal fat distribution, producing patchy lipoatrophy. These conditions are often accompanied by insulin resistance, diabetes mellitus, pancreatitis, hepatic cirrhosis, proteinuria, renal failure, or drug-induced changes from anti-retroviral therapy.[25]
Iatrogenic Causes
Radiotherapy, orbital surgeries, and drug-induced reactions are established causes of enophthalmos. Among children receiving radiation therapy to the head for malignancies such as rhabdomyosarcoma or retinoblastoma, loss of facial fat and enophthalmos occurs in 30% to 35% of cases. Etiologies include osseous hypoplasia of irradiated bones, vascular atrophy of the orbital contents, and hemifacial changes due to soft-tissue atrophy, such as loss of temporal fullness, temporalis muscle atrophy, deep superior sulci, and hypotelorism. Bilateral facial radiotherapy can produce bilateral facial deformities, resulting in an hourglass facial appearance, facial skeletonization, and sunken eyes.
Orbital surgeries, including fracture repair, decompression, and orbitotomy, can induce inflammation and subsequent orbital ischemia. Long-term follow-up often reveals enophthalmos and hypoglobus in these patients. Prostaglandin analogs used as anti-glaucoma medication can alter fat cell metabolism, causing facial fat loss, enophthalmos, deep superior sulci, hollowing of the lower eyelid–cheek junction, prominence of the inferior orbital rim, ptosis, inferior scleral show, prominent eyelid vessels, and eyelid tightness. This constellation of findings is termed "prostaglandin-associated periorbitopathy."[26]
Primary Mechanisms of Enophthalmos
Enophthalmos results from a complex interplay of anatomical, biomechanical, and tissue-level changes that disrupt the equilibrium between orbital contents and bony orbital volume. The globe maintains its forward position through balanced support from orbital fat, extraocular muscles, connective tissue septae, and vascular structures confined within the rigid orbital cavity. Reduction in soft-tissue volume or expansion of the orbital space produces posterior displacement of the globe along the anteroposterior axis.
The underlying pathophysiologic mechanism of enophthalmos can be conceptualized as an orbital volume–content mismatch. This mismatch arises from 3 principal processes: an increase in bony orbital volume, typically due to trauma or chronic sinus disease; loss or atrophy of orbital soft tissue due to fat resorption, fibrosis, or denervation; and cicatricial or fibrotic contracture, which pulls the globe posteriorly via connective tissue scarring.[27] At the cellular level, these mechanisms involve changes in adipocyte morphology, fibroblast activation, and extracellular matrix remodeling, often driven by ischemia, inflammation, or radiation injury.
At the microscopic level, orbital fat plays a pivotal role in maintaining globe projection. This tissue consists primarily of mature adipocytes surrounded by a delicate fibrovascular network. Fat loss occurs through adipocyte apoptosis and fibrosis mediated by activated myofibroblasts. In radiation-induced or postinflammatory cases, fibroblasts secrete excessive amounts of collagen types I and III, resulting in a dense extracellular matrix that contracts over time. This scarring exerts a mechanical pull, displacing the globe posteriorly.
Chronic inflammatory or autoimmune conditions, such as scleroderma or Parry-Romberg syndrome, cause vascular compromise and immune-mediated destruction of adipose tissue, resulting in progressive atrophy. Decreased orbital perfusion over time further promotes ischemic changes in extraocular muscles and connective tissue septae. Traumatic or sinus-related causes increase orbital cavity volume through bony expansion. Even a 1-mL increase in orbital volume can produce a 1- to 1.5-mm posterior shift of the globe, illustrating the sensitivity of ocular position to structural changes.[28]
The quantitative relationship between orbital volume changes and the resulting degree of enophthalmos is illustrated in Table. Quantitative Correlation Between Volume Change and Enophthalmos Severity below, providing a measurable framework for clinical assessment. This table helps predict the severity of globe displacement based on orbital expansion or tissue loss, guiding diagnosis, monitoring progression, and planning surgical or rehabilitative interventions.
Table. Quantitative Correlation Between Volume Change and Enophthalmos Severity
|
Orbital Volume Increase (mL) |
Globe Displacement (mm) |
Clinical Interpretation |
|
0.5 |
0.5–1.0 |
Minimal, often subclinical |
|
1.0 |
1.0–1.5 |
Mild, noticeable on inspection |
|
2.0 |
2.0–3.0 |
Moderate, clinically significant |
|
>3.0 |
>3.0 |
Severe, functionally impairing |
Histopathology
Histopathological features of enophthalmos are diverse and directly reflect the underlying etiology. Although enophthalmos represents a clinical manifestation rather than a distinct disease, microscopic evaluation of affected orbital tissue provides insight into mechanisms of posterior globe displacement. Histologic changes can be broadly grouped into 3 categories: orbital fat atrophy and fibrosis, bony remodeling and sinus-related alterations, and inflammatory or neoplastic infiltration.
Orbital Fat Atrophy and Fibrosis
The most consistent histopathologic finding in enophthalmos, regardless of etiology, is orbital adipose tissue atrophy and fibrosis. Under normal conditions, orbital fat consists of mature unilocular adipocytes surrounded by a delicate network of collagen fibers and capillaries. In involutional or senile enophthalmos, progressive reduction in adipocyte size and lipid content occurs, accompanied by thickening of fibrous septa.
Microscopically, adipocytes appear small, shrunken, and irregularly contoured with condensed cytoplasmic remnants. Collagen types I and III are deposited between fat lobules, often with mild chronic inflammatory infiltrates of lymphocytes and plasma cells. Fibroblast proliferation is evident, and myofibroblastic transformation may develop in advanced cases. Myofibroblasts express α-smooth muscle actin, contributing to tissue contraction and posterior traction on the globe.
Histologic changes are more pronounced in radiation-induced or postinflammatory enophthalmos. Standard fat architecture is obliterated by dense collagenization and hyalinization of connective tissue septa. Capillary endothelial proliferation, vascular occlusion, and ischemic adipocyte necrosis are common and reflect radiation- or inflammatory microangiopathy. Transforming growth factor β1 (TGF-β1), platelet-derived growth factor, and connective tissue growth factor are upregulated, driving fibrosis through extracellular matrix accumulation. Over time, this fibrosis tethers orbital contents, mechanically retracting the globe. In autoimmune or sclerodermatous causes, such as progressive hemifacial atrophy (Parry-Romberg syndrome), perivascular lymphoplasmacytic infiltration and endothelial cell swelling precede widespread adipocyte loss. Affected tissue shows thickened basement membranes and deposition of amorphous eosinophilic material resembling collagen sclerosis, resulting in irreversible fat resorption and enophthalmos on the affected side.
Bony and Sinus-Related Histopathologic Changes
In traumatic and sinus-related enophthalmos, histopathology primarily reflects bony remodeling, mucosal atrophy, and resorption at the sinus–orbit interface rather than primary fat degeneration. Posttraumatic specimens from the orbital floor or medial wall show fibroosseous repair, including immature woven bone, endochondral ossification, and fibrous callus formation. Over time, disorganized trabeculae mature into lamellar bone with osteoblastic rimming and intervening fibrovascular tissue. Resorption lacunae lined by osteoclasts may be present, especially where orbital fat herniates into the maxillary sinus. Chronic sinus exposure contributes to mucosal metaplasia and ciliary atrophy, leading to maxillary sinus atelectasis and orbital floor descent characteristic of silent sinus syndrome.
Microscopically, silent sinus syndrome demonstrates fibrotic thickening of sinus mucosa, reduced glandular elements, and chronic inflammatory infiltration. Advanced disease may show osteoclastic bone resorption and cortical thinning of the orbital plate, promoting orbital expansion. Adjacent orbital fat often develops secondary ischemic atrophy and fibroblast activation, reducing volume support for globe projection. In cases associated with osteomyelitis or long-standing infection, bone sections may show necrotic trabeculae, inflammatory granulation tissue, and bacterial colonies. Surrounding orbital fat demonstrates organizing inflammation with foamy macrophages and granulation tissue consistent with chronic postinfectious cicatrization.[29]
Inflammatory and Neoplastic Causes
Histopathological evaluation is critical for identifying infiltrative diseases that cause enophthalmos, including metastatic carcinoma, sclerosing orbital pseudotumor, and idiopathic orbital inflammation. Metastatic carcinoma, particularly of breast origin, induces a characteristic desmoplastic (scirrhous) reaction within orbital tissues. Dense fibrosis infiltrated by malignant epithelial cells forms a contracting mass that reduces orbital fat volume. Tumor cells are typically arranged in small pleomorphic clusters or cords embedded within hyalinized collagen bundles. Immunohistochemical staining frequently demonstrates cytokeratin, gross cystic disease fluid protein 15, or estrogen or progesterone receptor positivity, supporting the diagnosis of metastatic breast carcinoma. This desmoplastic fibrosis serves as the principal histologic basis for metastatic enophthalmos.
Sclerosing orbital pseudotumor demonstrates extensive collagen deposition with entrapment of atrophic extraocular muscle fibers and scattered chronic inflammatory cells. Lymphocytes, plasma cells, and eosinophils are dispersed throughout the fibrotic stroma, and some specimens exhibit features of vasculitis or obliterative phlebitis. Plasma cells positive for immunoglobulin G4 (IgG4) may be increased, implicating a subset in IgG4-related disease. Progressive collagen maturation and contraction yield a rigid, retracted orbit with enophthalmos and restrictive ophthalmoplegia. Idiopathic orbital fibrosis displays similar collagen-dense, avascular tissue with limited cellularity, lacking a specific antigenic or neoplastic driver. Myofibroblast-rich zones indicate sustained fibrogenic activity and account for gradual posterior traction on the globe.[30]
Extraocular Muscle and Connective Tissue Changes
Extraocular muscles affected by enophthalmos often demonstrate secondary atrophic changes driven by disuse, denervation, or ischemia. Histologic examination reveals variation in muscle fiber size, with angular atrophic fibers scattered among preserved fibers. Endomysial fibrosis and capillary lumen narrowing are common features. Radiation-related cases show more severe alterations, including vacuolar degeneration, loss of cross-striations, and progressive fibrous replacement of muscle fibers. The Tenon capsule and orbital septae exhibit thickened collagen bundles with hyaline degeneration. Elastic fibers become fragmented and reduced in number, diminishing orbital tissue compliance. The periorbita frequently develops dense fibrotic adhesion to underlying bone, restricting the mobility and dynamic positioning of orbital structures.[31]
Special Stains and Immunohistochemistry
Special histochemical and immunohistochemical studies support etiologic differentiation in enophthalmos. The Masson trichrome stain demonstrates dense collagen deposition surrounding atrophic adipocytes, confirming fibrosis. Oil Red O staining on frozen sections highlights loss of lipid content, indicating adipocyte depletion, whereas α-smooth muscle actin immunoreactivity identifies myofibroblast activation within contracting fibrotic tissue.
CD34 or factor VIII staining evaluates vascularity and typically shows reduced microvascular density in chronic ischemic or radiation-associated cases. Positive staining for the estrogen or progesterone receptor, cytokeratin 7, or gross cystic disease fluid protein 15 confirms metastatic breast carcinoma contributing to a desmoplastic orbital process. IgG4 immunostaining shows increased IgG4-positive plasma cells—often exceeding 50 per high-power field—supporting the diagnosis of IgG4-related orbital disease with fibrosis. Histopathologic changes in enophthalmos converge on fat atrophy, fibrosis, and altered orbital volume, resulting in insufficient structural support for normal globe projection. Identifying whether the process is active and inflammatory or dense and fibrotic informs prognosis and directs management toward reversible or reconstructive interventions.[32]
Toxicokinetics
Enophthalmos is not primarily a toxicologic condition. However, toxicokinetics influences the development of this condition in specific clinical contexts. Chemical and pharmacologic agents that disrupt orbital vascular supply, alter adipocyte metabolism, or impair connective tissue integrity can trigger structural changes within the orbit that reduce volume support and promote posterior displacement of the globe. Relevant mechanisms include radiation-related microangiopathy and fibrosis, medication-induced orbital fat atrophy, chronic systemic corticosteroid exposure that reduces adipose volume, and antimetabolite- or chemotherapeutic-induced injury to orbital soft tissues.
Radiation-Induced Toxicokinetics and Fibrosis
Radiation therapy to the head and neck, orbit, or paranasal sinuses constitutes the most well-established toxicokinetic pathway leading to enophthalmos. Ionizing radiation induces radiolysis of water, generating reactive oxygen species, including hydroxyl radicals and superoxide anions. These free radicals initiate lipid peroxidation and DNA injury in adipocytes, fibroblasts, and vascular endothelial cells.
Early effects (days to weeks) include microvascular endothelial damage, capillary dilation, and increased permeability. Transient edema gradually evolves into progressive capillary loss and ischemia. Chronic hypoxia stimulates fibroblast proliferation and differentiation into myofibroblasts, mediated by elevated expression of transforming growth factor-β1, platelet-derived growth factor, and vascular endothelial growth factor. Excessive collagen deposition, hyalinization, and fat necrosis subsequently occur, resulting in irreversible fibrotic contraction of orbital tissues. The progression unfolds over months to years. Higher cumulative radiation doses (>50 Gy) strongly correlate with fibrosis severity and the risk of enophthalmos. Once reparative pathways exceed normal collagen turnover capacity, a persistent “toxic steady state” of remodeled, noncompliant orbital soft tissue emerges, permanently reducing orbital volume support.[33]
Corticosteroid-Induced Fat Redistribution
Corticosteroids exhibit complex pharmacokinetic and toxicokinetic behavior that directly influences orbital tissue composition. Effects on adipose metabolism are dose-dependent and linked to both magnitude and duration of systemic exposure. Early in treatment, corticosteroids enhance lipogenesis in central fat depots while promoting catabolism and lipolysis in peripheral regions, including periorbital and facial fat.
Mechanistically, increased hormone-sensitive lipase activity drives triglyceride breakdown, while suppression of local lipoprotein lipase limits lipid uptake by orbital adipocytes. The result is progressive orbital fat loss and atrophic remodeling. At the cellular level, corticosteroids induce adipocyte apoptosis, inhibit preadipocyte differentiation, and disrupt maintenance of the extracellular matrix.
Prolonged exposure, whether systemic, topical, or periocular, produces cumulative structural changes expressed clinically as orbital hollowing and superior sulcus deformity, thereby mimicking or exacerbating enophthalmos. These changes highlight how steroid tissue retention, receptor affinity, and lipid solubility can reshape orbital morphology over time.[34]
Chemotherapeutic and Antimetabolite Toxicity
Specific cytotoxic agents and antimetabolites can produce secondary orbital toxicity by disrupting fibroblast, endothelial, and adipocyte function. Drugs such as 5-fluorouracil, cisplatin, and methotrexate impair DNA synthesis and cell proliferation, limiting the regenerative capacity of orbital connective tissues. Systemic accumulation leads to chronic microangiopathy and oxidative stress by endothelial apoptosis and reduced perfusion. Fibroblast dysfunction disrupts extracellular matrix turnover, creating an imbalance between collagen deposition and degradation that progresses to atrophic fibrosis. Local exposure, particularly from periocular or intralesional use of antimetabolites such as mitomycin C during ocular surface procedures, can penetrate orbital soft tissues and cause focal fat necrosis and scarring—an iatrogenic mechanism predisposing to localized enophthalmos.
Environmental and Occupational Toxins
Long-term exposure to environmental toxins, including organic solvents, heavy metals (lead, mercury), and hydrocarbon vapors, induces oxidative stress and mitochondrial dysfunction in adipose tissue. These lipophilic agents accumulate in orbital fat, impair mitochondrial β-oxidation, and trigger adipocyte apoptosis. The toxicokinetic hallmark of such exposures is slow elimination, with half-lives extending over months, resulting in cumulative fat toxicity and progressive structural degeneration. Chronic lead exposure additionally compromises vascular smooth muscle contractility and diminishes nitric oxide–mediated vasodilation, exacerbating ischemic atrophy of orbital contents. Toxicokinetic mechanisms, including radiation, steroids, and chemotherapeutic agents, modify orbital tissues, leading to chronic enophthalmos. Awareness of cumulative doses, careful monitoring, and recognition of fibrosis guide prevention and reconstructive planning, influencing graft selection and timing of interventions.[35]
History and Physical
Patient History
The onset and progression of enophthalmos provide important diagnostic clues. Acute enophthalmos often indicates orbital floor blowout fracture or sudden orbital fat necrosis following trauma or surgery. Gradual onset typically reflects chronic processes, including silent sinus syndrome, radiation-induced fibrosis, sclerosing orbital inflammation, or progressive fat atrophy. Intermittent enophthalmos may occur with orbital varices, which are influenced by postural changes. Relevant history includes prior trauma, sinus disease, orbital or periorbital surgery, radiation exposure, weight loss, and systemic disorders such as scleroderma or metastatic carcinoma, particularly breast cancer in women.[36]
Common presenting complaints reflect underlying structural or functional changes. Facial asymmetry arises from loss of orbital volume or expansion of the bony orbit. Droopy eyelid or ptosis results from mechanical displacement, levator dehiscence, or fibrosis. Deep upper sulcus deformity corresponds to orbital fat atrophy or scarring of the orbital septum. Diplopia can originate from restrictive myopathy or altered globe alignment, whereas difficulty with depth perception reflects changes in binocular vision geometry; epiphora or ocular dryness results from altered lid-globe apposition or lagophthalmos. Dull orbital pain or pressure often signifies posttraumatic fibrosis or inflammatory infiltration.
Ophthalmological Examination
Evaluation of enophthalmos requires a comprehensive ophthalmic and periocular assessment. Basic visual acuity, refraction, pupil and anterior chamber examination, intraocular pressure, and fundus evaluation are essential to exclude concurrent intraocular pathology. Assessment of facial symmetry, globe and eyelid position, extraocular movements, and periocular tissue integrity provides critical clues to the underlying etiology.
In unilateral cases, orbital asymmetry is apparent, with the deep-set globe often associated with superior sulcus deformity, relative ptosis, entropion, lagophthalmos, and reduced vertical palpebral fissure height in primary gaze. The Hirschberg test may reveal hyperglobus, hypoglobus, esoglobus, or exoglobus. Optimal inspection for enophthalmos is performed in the chin-up position (worm’s-eye or dog’s-eye view), allowing direct comparison of corneal apex positions.
Orthophoric alignment of the eyes is a prerequisite, as ocular deviation can mask enophthalmos (see Image. Enophthalmos Examination). Bilateral cases require systematic orbital evaluation with exophthalmometry. Progressive conditions and orbitofacial trauma cases benefit from sequential follow-up with photographic documentation to monitor globe position. Trauma with severe periocular ecchymosis, edema, or ptosis warrants repeat assessment after resolution of swelling.[37]
Ocular examination findings
Ocular evaluation requires a structured assessment to delineate visual, anatomic, and functional changes. Investigations should include the determination of visual acuity and refraction to rule out concurrent amblyopia or refractive error; pupillary reactions and anterior segment examination to detect associated uveitis or trauma sequelae; intraocular pressure measurement to ascertain reduction due to orbital volume expansion or elevation from fibrosis compressing episcleral veins; and fundus examination to identify choroidal folds or optic disc tilt secondary to globe displacement.
External and orbital signs provide additional diagnostic information. Posterior globe displacement of 2 mm or more compared to the fellow eye is a hallmark of enophthalmos. Superior sulcus deformity, characterized by a deep upper lid crease, typically reflects fat loss or postsurgical changes. Eyelid malpositions, including entropion, ptosis, or retraction, arise from cicatricial processes, while conjunctival chemosis or injection often accompanies inflammation. Lagophthalmos denotes incomplete lid closure and is commonly associated with fibrosis. An abnormal Hirschberg reflex may reveal vertical or horizontal displacement of the globe, distinguishing true enophthalmos from pseudo-enophthalmos; restricted ocular motility, observed in posttraumatic or fibrotic cases, signals extraocular muscle involvement.
Specialized measurements provide an objective assessment of enophthalmos and guide clinical management. Exophthalmometry using Hertel or Naugle devices quantifies globe projection relative to the lateral orbital rim; enophthalmos is defined as a difference greater than 2 mm compared with the fellow eye. CT-based volumetry enables precise evaluation of orbital fat and bony volumes, thereby aiding surgical planning. Three-dimensional photographic analysis tracks facial asymmetry over time, allowing monitoring of progression or postsurgical outcomes. Worm’s-eye view inspection, performed with the chin-up position, offers a rapid bedside screening method by comparing corneal apex positions.
Clinical variants of enophthalmos demonstrate distinctive findings corresponding to the underlying etiology. Traumatic enophthalmos presents with step deformity, infraorbital hypesthesia, restricted upgaze, and palpable rim defects. Silent sinus syndrome typically presents with a deep superior sulcus and hypoglobus, without motility limitation. Postradiation cases exhibit firm periorbital tissue, cicatricial eyelids, and restricted globe movement. Sclerosing orbital inflammation typically presents with tenderness, movement limitation, and imaging evidence of fibrosis. Metastatic enophthalmos typically presents as painless, progressive globe retraction, with palpable orbital masses uncommon and often in patients with a history of carcinoma. Involutional or senile enophthalmos is usually bilateral and symmetric, with deep superior sulci and preserved ocular motility.
Systemic evaluation
A detailed systemic examination is essential in congenital syndromes, trauma cases, and acquired systemic disorders. In suspected congenital syndromes, a meticulous head-to-toe assessment may reveal additional manifestations, such as café-au-lait spots in NF-1. Evaluation of the face and oral cavity is crucial in first-arch syndromes to detect maldevelopment or malalignment of teeth, cleft lip or palate, high-arched palate, and uvula anomalies.
Oculofacial trauma cases must follow trauma management protocols, prioritizing patient stabilization and assessment of concurrent cranial or limb injuries before orbital and facial fractures. Systemic disorders may present with ocular complaints, including enophthalmos, before other disease manifestations, as seen in breast carcinoma metastasis. Examination of the body to identify primary tumors in the breast, lungs, or prostate is critical in suspected orbital metastasis.
Systemic clues can provide important insight into the etiology of enophthalmos. Chronic sinusitis or allergic disease suggests silent sinus syndrome. Cutaneous sclerosis or hemifacial atrophy points toward autoimmune involvement. A history of breast carcinoma or prior mastectomy indicates possible metastatic fibrosis. Cachexia or malnutrition may underlie generalized orbital fat loss.
Sinus pathologies require consultation with otorhinolaryngology for further management. Localized lipoatrophy disorders, such as scleroderma or Parry-Romberg syndrome, may necessitate systemic evaluation to exclude broader autoimmune involvement affecting periocular tissues. Clinical presentation varies with etiology, chronicity, and associated orbital pathology. Comprehensive history-taking and detailed ocular and systemic examination are essential for establishing the diagnosis, identifying the underlying cause, and assessing functional and cosmetic deformity.[38]
Follow-up and Documentation
Serial photographic documentation, exophthalmometry, and CT orbital imaging are essential in progressive enophthalmos, particularly in posttraumatic or fibrosing conditions. Acute trauma may mask subtle globe displacement due to edema, necessitating reevaluation once swelling resolves, typically after 2 to 3 weeks.[39] Clinical assessment correlates closely with etiology:
- Traumatic cases often present with a history of orbital fracture, step deformity, diplopia, or hypesthesia.
- Postinflammatory cases typically result from prior infection, radiation, or autoimmune disease and present with a firm orbit and restricted motility.
- Neoplastic cases exhibit progressive retraction and fibrosis, usually with a history of breast, sinus, or nasopharyngeal malignancy.
- Silent sinus syndrome manifests with nasal obstruction, chronic sinusitis, painless enophthalmos, and hypoglobus.
- Involutional cases in older adults demonstrate gradual, bilateral deepening of the superior sulcus and symmetric changes.
Evaluation
Enophthalmos is objectively defined as a posterior displacement of the globe of 2 mm or more compared with the fellow eye along the anteroposterior axis, measured from the lateral orbital rim to the apex of the cornea.[40] This measurement presumes normal baseline globe alignment for the individual patient.
Clinical Assessment of Enophthalmos
Clinical assessment of enophthalmos relies on reference to the patient’s orbital margins. Measurement of the anteroposterior position of the globe, known as exophthalmometry, facilitates diagnosis and monitoring of globe displacement. Several exophthalmometers are available, each with its own advantages and limitations (see Image. Types of Exophthalmometers).
The Hertel exophthalmometer consists of a horizontal device supported at the lateral orbital rims to measure the distance from the rim to the corneal apex. This device is relatively easy to use, but accuracy depends on the integrity of the lateral orbital rim. Cases involving loss or recession of the rim, such as orbitozygomatic fractures, lateral orbitotomy with bone window creation, or lateral wall decompression, exhibit substantial interobserver variability. Prisms and parallax adjustment help reduce these discrepancies.[41]
The Naugle exophthalmometer functions similarly but uses a horizontally oriented bar between the lateral canthi to achieve 4-point fixation of the superior and inferior orbital margins. Black markers along its length allow precise identification of the pupil midpoint, facilitating reproducible measurements. Compared with the Hertel device, the Naugle exophthalmometer provides more reliable readings in cases of orbitozygomatic fractures or lateral orbital rim disruption.[42]
The Leudde prism exophthalmometer employs a prism as a ruler, positioned on the lateral orbital rim to eliminate parallax error during binocular observation, allowing accurate assessment of enophthalmos or exophthalmos. The Mourits exophthalmometer combines the use of prisms with a graduated metal frame, similar to the Hertel device, and demonstrates greater reliability than both the Leudde and Hertel instruments.
Clinical Examination of Hypoglobus
Enophthalmos frequently coexists with hypoglobus, particularly in orbital floor fractures, silent sinus syndrome, and postorbital decompression cases.[43] Hypoglobus must be differentiated from hypotropia, in which the central corneal reflex is displaced superiorly. Vertical dystopia and hypoglobus should be measured and documented separately. The 2-scale method provides optimal estimation of hypoglobus, while the Hirschberg test and prism bar cover tests assist in evaluating associated hypotropia and limitations in downward gaze.
Radiological Assessment of Enophthalmos
CT scanning provides high-resolution imaging of orbital bones and contents, making it the modality of choice in orbitofacial trauma. The lateral orbital rim serves as a standard landmark; when lateral rim fractures are present, the nasal septum or mirror imaging of the unaffected orbit is used.[44] Additional reference points, such as the styloid and posterior clinoid processes, enable precise quantification of enophthalmos.[45] Axial images are most informative for measuring globe displacement and making serial comparisons, while coronal and sagittal views assess fracture extent and estimate orbital volume loss from herniated contents. The volume of herniated tissue correlates significantly with the degree of enophthalmos. In congenital anomalies such as microphthalmos, cryptophthalmos, or congenital cystic eye, orbital ultrasound assists in evaluating intraocular structures and guiding management planning.
Systemic Assessment
A comprehensive systemic evaluation is mandatory before planning any intervention for enophthalmos. Trauma cases require imaging tailored to the extent of injury, including radiographs or CT of the head, chest, and affected limbs, with abdominal ultrasound as indicated. Sinus disease assessment typically includes endoscopy to evaluate septal deviation and radiologic evaluation of orbital floor remodeling. Suspected orbital metastasis necessitates an extensive search for the primary tumor, often aided by whole-body positron emission tomography-CT. Localized autoimmune disorders such as scleroderma require antibody testing, including anti-nuclear, anti-topoisomerase (Scl-70), and anti-histone antibodies, and scoring with the Localized Scleroderma Assessment Tool to quantify disease activity and damage.[46][47]
Treatment / Management
Management of Oculofacial Trauma
Management of oculofacial trauma depends on injury severity and timing. Conservative management is appropriate for superficial abrasions, ecchymosis, mild enophthalmos, or undisplaced fractures, as well as for circumstances where surgery is declined or fracture size is small and asymptomatic.[48] Immediate surgical intervention is indicated for open lacerations, complex orbitofacial fractures, significant enophthalmos, or globe luxation. Pediatric individuals with white-eye trapdoor fractures or persistent oculocardiac reflex—manifesting as vomiting, bradycardia, or syncope—require urgent repair. Entrapment of the inferior rectus in floor fractures or the medial rectus in medial wall blowout fractures must be released to preserve extraocular motility and prevent secondary enophthalmos. Delayed surgical intervention is recommended for cases with severe periorbital edema, large undisplaced fractures, or concurrent globe injuries. A 2- to 4-week period allows edema to resolve and reduces the risk of orbital compartment syndrome and sight-threatening complications.[49]
Management of Hypotropia
Hypotropia associated with enophthalmos requires definitive surgical correction. Restrictive strabismus caused by a fibrosed inferior rectus muscle may benefit from recession of the affected muscle.
Cosmetic Correction of Enophthalmos
Cosmetic surgical correction of enophthalmos is indicated when there is apparent posterior displacement of the globe on inspection, the need to address concurrent conditions such as ptosis or entropion, and gross facial disfigurement requiring correction. Surgical options include repair of the underlying pathology, such as orbital fractures or sinus abnormalities, replacement of lost orbital fat, and augmentation of periorbital soft-tissue volume. Surgical management of orbital fractures is guided by CT imaging, using the "enophthalmos estimate line," a virtual line drawn from the most distal part of the fractured segment to its original position.[50] This line provides an indirect estimate of resultant enophthalmos. The primary goals of fracture repair are restoration of ocular motility and resolution of diplopia.[51] Techniques typically include open reduction with external fixation using metal plates or placement of orbital floor implants to support orbital contents. Navigation-based orbital surgery allows precise localization of bony landmarks, facilitating near-total reduction of displaced contents and accurate implant placement.[52](B3)
In cases of silent sinus syndrome, endoscopic evaluation with endonasal maxillary antrostomy and uncinectomy is preferred to restore sinus drainage, decompress the sinus system, and reestablish aeration. Sinus surgery alone can improve enophthalmos by up to 2 mm within 6 months.[53] Orbital floor reconstruction is required in approximately one-fifth of cases, providing acceptable correction of enophthalmos and hypoglobus in most patients.[54] Implants typically consist of titanium plates with spacers, and the advent of customized 3D-printed implants enables patient-specific optimization. Management of lipoatrophy due to systemic causes is more challenging, with volume replacement or augmentation achieved via autologous microfat or nanofat transfer or hyaluronate fillers.(A1)
Cases of pseudo-enophthalmos associated with shrunken globes, including phthisis bulbi, microphthalmos, cryptophthalmos, or congenital cystic eye with no visual potential, may benefit from globe volume restoration via evisceration and placement of a large implant. Customized prostheses with serial conformer expansion are required. Severe anophthalmic sockets with contracture may necessitate extensive reconstruction using dermis-fat and mucous membrane grafts. Surgical correction of globe malpositions, strabismus, eyelid malpositions, lagophthalmos, entropion, or superior sulcus deformity should be planned in a staged approach following enophthalmos repair.
Differential Diagnosis
True enophthalmos must be differentiated from pseudo-enophthalmos, in which the anteroposterior globe position remains normal despite the appearance of posterior displacement.[55] Exophthalmometry may be misleading when axial globe length is shortened, producing a false impression of enophthalmos. Differential considerations include contralateral proptosis, where unilateral forward displacement of one globe creates the illusion of enophthalmos on the opposite side, and facial asymmetry, such as hemifacial microsomia—congenital or acquired—which may mimic Parry-Romberg syndrome. Associated congenital torticollis or Sprengel deformity can exaggerate peribulbar atrophy, while bony hypoplasia or recession of the lateral orbital rim may alter exophthalmometric measurements.[56][57]
Phthisis bulbi results from globe shrinkage following intraocular infections, ruptured globe injuries, or repeated intraocular surgeries and is frequently associated with socket contracture, ptosis, entropion, and pseudo-enophthalmos. These changes reflect orbital volume loss and reduced posterior eyelid support rather than true posterior displacement of the globe (see Image. Phthisis Bulbi).[58] Microphthalmos is a congenital malformation characterized by reduced ocular volume and a small eye, often with a smaller corneal diameter than the contralateral eye, and is commonly associated with hemifacial microsomia (see Image. Microphthalmos).[59]
Anisometropia, particularly unilateral myopia, can produce proptosis of the myopic eye, whereas asymmetric hypermetropia or nanophthalmos may mimic enophthalmos.[60] Horner syndrome presents with ptosis, miosis, anhidrosis, and loss of the ciliospinal reflex. Paresis of the sympathetically innervated Müller muscle produces ptosis, which can simulate enophthalmos despite symmetrical exophthalmometry.[61] Congenital or acquired ptosis often deepens the superior sulcus, giving the clinical impression of enophthalmos.
Postenucleation socket syndrome, also termed the "anophthalmic socket," results from loss of the globe and is characterized by decreased orbital volume, ptosis, deep superior sulcus, lower lid laxity, entropion, and, occasionally, relative upper lid retraction with lagophthalmos. Prosthetic eye placement in a primary sitting may produce the appearance of enophthalmos. Management typically involves a staged approach, beginning with volume-restoration surgery, followed by socket reconstruction, fitting of a custom-made prosthesis, and eyelid procedures to achieve optimal cosmetic results.
Severe orbitofacial trauma can cause total disruption of the orbital floor, medial wall, and inferomedial strut, resulting in luxation or dislocation of the globe into the maxillary or ethmoidal sinuses or nasal cavity. Avulsion or laceration of extraocular muscles and the optic nerve can occur, producing an anophthalmic socket–like appearance with apparent enophthalmos. A small or ill-fitting prosthetic eye in such a socket may further accentuate this appearance, necessitating assessment of prosthetic fit, comfort, and motility, with management ranging from volume replacement surgeries to custom-made prosthetic shells.[62]
Pertinent Studies and Ongoing Trials
Extensive study of enophthalmos has clarified its pathophysiology, diagnostic evaluation, and management, especially in posttraumatic, postradiation, and silent sinus syndrome cases. Contemporary clinical and imaging research has enhanced the understanding of orbital volumetric loss, tissue remodeling, and outcomes of reconstructive interventions.
Radiologic and Volumetric Studies
Results from recent quantitative imaging studies using high-resolution CT and MRI have clarified the relationship between orbital volume expansion and globe displacement. Whitehouse et al (1994) demonstrated that a 1 cm³ increase in orbital volume corresponds to approximately 0.8 mm of enophthalmos in patients with blowout fractures.[63] Volumetric CT studies with 3D reconstruction have improved risk stratification for late enophthalmos and enabled differentiation of true globe displacement from pseudoptosis.[64] Current research employs artificial intelligence-driven orbital morphometry to develop predictive models for surgical planning and posttraumatic enophthalmos assessment.
Posttraumatic Enophthalmos Trials
Posttraumatic orbital fracture repair has been extensively studied, with patient-specific orbital implants (PSIs) designed using 3D planning and manufacturing techniques demonstrating improved anatomical restoration and orbital volume symmetry. Kittichokechai et al (2022) reported that custom titanium mesh reduced the orbital volume and globe position difference between affected and unaffected orbits by approximately 2.9 mm (P < 0.001). A 2021 systematic review noted that although PSIs enhance fit and contour, clinical outcomes such as late enophthalmos and diplopia may not yet be statistically superior to well-performed conventional implants, underscoring the need for multicenter randomized trials comparing materials (eg, titanium versus porous polyethylene) and evaluating long-term functional outcomes.[65]
Definitive long-term randomized trials comparing absorbable and nonabsorbable implants remain limited. A retrospective study by Polacco et al (2019) found no significant difference in postoperative enophthalmos or ocular motility between absorbable implants (poly-L-lactic acid, polyglycolic acid, polydioxanone) and nonabsorbable implants (titanium, porous polyethylene) in moderate-sized orbital floor fractures.[66] Implant selection should be individualized, and prospective trials are necessary to evaluate volume retention, motility outcomes, and late enophthalmos in larger orbital wall defects.
Silent Sinus Syndrome Studies
Silent sinus syndrome, a common nontraumatic cause of enophthalmos, has been extensively investigated in both retrospective and prospective studies. Results from a retrospective series of 18 patients treated with endoscopic maxillary antrostomy alone, 14 (78%) achieved complete resolution of enophthalmos and hypoglobus, while an additional 3 (17%) showed partial improvement without orbital floor reconstruction.[67] Lee et al (2022, Am J Rhinol Allergy) proposed a 2-stage protocol combining functional endoscopic sinus surgery with delayed orbital reconstruction, demonstrating superior orbital alignment compared to simultaneous procedures. Ongoing clinical investigations are evaluating image-guided, navigation-assisted reconstruction to reduce residual deformities.[67]
Postradiation and Fibrosis-Associated Enophthalmos
Radiation-induced enophthalmos is a recognized delayed complication of orbital or nasopharyngeal irradiation. Radiotherapy to the head and neck can produce soft-tissue changes, including fat atrophy and fibrosis, resulting in orbital and facial volume loss. Imaging studies indicate that higher cumulative doses and smaller fractionation schedules correlate with more pronounced tissue atrophy and volumetric decline.[68] Although high-quality randomized trials of antifibrotic agents in postradiation orbital fibrosis are lacking, evidence from other irradiated soft tissues supports this therapeutic approach. For example, pentoxifylline combined with vitamin E improves tissue compliance in chronic radiation-induced fibrosis. Prospective studies are required to evaluate volume loss, fibrosis progression, and prevention of enophthalmos using agents such as pirfenidone or pentoxifylline.[69]
Fat Atrophy and Volume Restoration Studies
The introduction of autologous fat grafting, free flap transfer, and stem cell–assisted volumetric restoration has transformed the management of enophthalmos. Results from a small series have reported significant improvement in posttraumatic enophthalmos using autologous fat grafting. For instance, Chen H et al (2018) observed sustained improvement in globe projection and upper-lid contour in 9 patients over 8 to 24 months.[70]
Results from a randomized trial by Wufuer et al (2024) demonstrated that stromal vascular fraction–enriched fat grafts achieved higher retention at 6 and 24 weeks compared with conventional fat (74.5% ± 9.99% vs 66.6% ± 13.8% at 6 weeks, P < 0.025; 71.3% ± 10.4% vs 62.0% ± 13.5% at 24 weeks, P < 0.012).[71] Current regenerative medicine trials are exploring adipose-derived stem cell scaffolds for long-term orbital soft-tissue reconstruction, showing promising results in early pilot studies.
Artificial Intelligence and Imaging-Based Predictive Modeling
AI-assisted radiomics and 3D simulation platforms are increasingly transforming diagnostic and surgical workflows in orbital management. Deep-learning and radiomics techniques applied to orbital trauma imaging have shown preliminary feasibility in predicting posttraumatic enophthalmos with high accuracy. Ongoing trials in Europe and Japan are integrating AI-guided 3D orbital implant planning to optimize volumetric correction and minimize postoperative asymmetry.[72]
Emerging Research Directions
Emerging strategies in enophthalmos management include 3D bioprinting of orbital scaffolds, enabling development of bioresorbable, patient-specific implants seeded with autologous fibroblasts and adipose-derived stem cells. Molecular pathway inhibitors, such as antagonists of transforming growth factor beta and connective tissue growth factor, are under investigation to prevent fibrosis in postinflammatory or radiation-induced cases. Longitudinal studies are evaluating functional outcomes, integrating oculomotor performance and binocular depth perception recovery with reconstructive results.
Treatment Planning
Treatment planning for enophthalmos requires precise characterization of etiology, chronicity, degree of globe displacement, and associated functional and cosmetic deficits. Therapeutic objectives include restoration of orbital symmetry, preservation or improvement of ocular motility, prevention of exposure keratopathy, and maintenance of orbital volume. An interprofessional approach incorporating oculoplastic surgeons, maxillofacial surgeons, otolaryngologists, and radiologists is essential for optimal outcomes, particularly in complex posttraumatic or postradiation cases.[73]
Diagnostic Workup and Preoperative Assessment
Accurate quantification of enophthalmos forms the foundation of treatment planning. Exophthalmometry allows measurement of relative globe displacement, with a difference of 2 mm or greater compared to the fellow eye considered clinically significant. CT orbital imaging provides 3D volumetric assessment of orbital walls, fat, and muscle compartments, identifying bone resorption, fat atrophy, or sinus expansion. Functional evaluation, including ocular motility testing, diplopia charting, and forced duction testing, determines the presence of restrictive pathology. Photographic and 3D facial analysis supports preintervention and postintervention documentation as well as surgical simulation. Counseling should address the potential for undercorrection or overcorrection, particularly when chronic scarring or fibrosis limits orbital expansion.
Etiology-Specific Management Framework
Management of enophthalmos depends on etiology and involves a combination of primary and adjunctive strategies. Posttraumatic enophthalmos is addressed through orbital floor or wall reconstruction using titanium mesh, porous polyethylene, or 3D patient-specific implants. Early repair within 14 days minimizes fibrosis, while delayed cases may require fat graft augmentation. Silent sinus syndrome is treated with functional endoscopic sinus surgery to reexpand the maxillary sinus and restore orbital floor position, with secondary orbital reconstruction reserved for residual deformity.
Postradiation fibrosis is managed with antifibrotic therapy, including pentoxifylline, tocopherol, or pirfenidone, and delayed soft tissue augmentation, while artificial tears and lid support mitigate exposure symptoms. Involutional or senile enophthalmos is corrected with autologous fat grafting or dermal fat grafts, and hyaluronic acid fillers may address minor asymmetry. Metastatic or neoplastic causes require systemic therapy or local tumor excision, followed by delayed orbital volume restoration and ongoing oncologic surveillance with imaging follow-up. Postinflammatory fibrosis is treated with systemic or local corticosteroids or immunosuppressants, with surgical decompression reserved for severe cases, ensuring underlying inflammation is controlled before reconstruction.
Reconstructive and Surgical Planning
Surgical planning requires precise assessment of defect size, orbital volume loss, and soft-tissue atrophy to guide implant selection and placement. Surgical intervention is indicated for enophthalmos greater than 2 mm, restricted ocular motility, or pronounced aesthetic deformity.
Orbital reconstruction
Orbital reconstruction utilizes porous polyethylene, titanium mesh, resorbable plates, or custom computer-aided design and computer-aided manufacturing implants generated from preoperative 3D CT images. The operative approach is selected based on the defect location, using transconjunctival, subciliary, or endoscopy-assisted routes. Reconstruction centers on reestablishing orbital bony contour and volume while preventing entrapment of the periorbita or extraocular muscles.
Soft tissue augmentation
Soft-tissue augmentation is indicated when fat atrophy or fibrosis results in volume loss in the absence of a significant bony defect. Available techniques include autologous fat transfer, dermal fat grafting, and vascularized free flaps such as radial forearm or temporal fascia flaps. Stem cell–enriched fat grafting is gaining prominence as a long-term strategy for maintaining volume.[74]
Secondary and revision procedures
Secondary and revision procedures are frequently required to address residual asymmetry or contour defects, particularly in posttraumatic or irradiated orbits. Navigation-guided orbital reconstruction and 3D printing–assisted volume restoration provide high reproducibility and improved symmetry.[75]
Nonsurgical and Supportive Measures
Mild or early enophthalmos may be managed conservatively with orbital prosthetics in anophthalmic sockets to maintain socket volume; lubrication and eyelid protection to prevent exposure keratopathy; prism therapy for minor diplopia; and observation with serial imaging in stable, nonprogressive presentations. In postradiation or autoimmune etiologies, steroids, immunomodulators, or antifibrotic agents may slow progression before surgical intervention is planned.[76]
Timing of Intervention
The timing of the intervention depends on the disease course and underlying pathology. Acute trauma warrants repair within 2 weeks to prevent fibrosis, whereas chronic enophthalmos requires delayed correction until soft tissue remodeling stabilizes over approximately 3 to 6 months. Silent sinus syndrome involves treatment of the sinus pathology first, with orbital reconstruction performed only after restoration of sinus ventilation. Reconstruction in radiation fibrosis is typically deferred for at least 6 to 12 months after therapy to minimize complications associated with active tissue necrosis.
Postoperative Follow-Up and Monitoring
Postoperative follow-up focuses on confirming structural stability and identifying early complications. Imaging with CT or MRI verifies orbital symmetry and implant positioning, while serial exophthalmometry allows objective assessment of correction stability. Rehabilitation typically includes ocular motility exercises and scar massage to preserve muscle elasticity and prevent restrictive adhesions. Complications such as overcorrection, diplopia, or implant exposure may require timely revision surgery.[77]
Emerging and Experimental Modalities
Emerging and experimental modalities continue to expand reconstructive options for enophthalmos. AI-assisted 3D orbital planning applies machine-learning algorithms to predict optimal implant shape and volume, with pilot studies demonstrating approximately 95% accuracy in achieving postoperative symmetry. Stem cell–enriched grafting seeks to improve graft survival and limit resorption, with phase II clinical trials reporting encouraging outcomes.
The development of 3D-bioprinted orbital scaffolds aims to produce personalized implants that replicate native bone elasticity, with ongoing work in Europe and Japan. Endoscopic transantral repair offers a minimally invasive alternative that avoids cutaneous incisions while providing excellent cosmetic results and rapid recovery. Fat hydrogel composites function as injectable scaffolds that mimic orbital fat, with early preclinical investigations demonstrating promise for reliable volume restoration.
Prognostic Indicators
Final cosmetic and functional outcomes depend on the underlying etiology, the chronicity of volume loss, the timing and precision of surgical intervention, the quality of soft tissue and implant materials, and adherence to postoperative rehabilitation. Fibrotic or irradiated tissues demonstrate reduced elastic recoil and often require staged correction. In contrast, early intervention in traumatic or sinus-related etiologies offers the greatest likelihood of optimal anatomic and functional recovery.
Toxicity and Adverse Effect Management
Management of enophthalmos, whether medical, surgical, or reconstructive, may have adverse effects that can affect functional and cosmetic outcomes. Understanding and mitigating such complications remains integral to comprehensive care. Adverse effects may arise from pharmacologic agents, operative techniques, implant materials, or radiation-related fibrosis and require preventive strategies, vigilant monitoring, and early interprofessional management to limit long-term morbidity and optimize restoration of orbital volume and symmetry.
Toxicity Due to Pharmacological Treatment
Medical therapy provides supportive benefit rather than definitive correction in enophthalmos, yet several pharmacologic agents used for associated inflammation, fibrosis, or radiation injury carry risks of systemic or local toxicity. Systemic corticosteroids used for posttraumatic or postinflammatory fibrosis may trigger hyperglycemia, hypertension, ocular hypertension, cataract formation, or avascular necrosis. Management relies on intraocular pressure monitoring, dose tapering, and use of topical or periocular routes when feasible. Antifibrotic agents, such as pentoxifylline, tocopherol, or pirfenidone, mitigate radiation-induced fibrosis but may cause gastrointestinal upset, dizziness, hepatotoxicity, or fatigue. Baseline liver function testing, gradual dose escalation, and symptomatic treatment reduce complication rates.
Immunosuppressants, including methotrexate or mycophenolate, support control of autoimmune orbital inflammation but can cause bone marrow suppression, hepatotoxicity, and increased infection risk, warranting monitoring of complete blood count and liver function and avoidance of live vaccines. Topical lubricants and steroids provide ocular surface protection but may induce steroid-related glaucoma or epithelial thinning, requiring preservative-free artificial tears and strict limitation of steroid duration. Hyaluronic acid fillers offer temporary correction for mild enophthalmos but carry risks of nodule formation, vascular occlusion, or, rarely, blindness—injection under imaging guidance and the availability of hyaluronidase support safe use.
Surgical and Implant-Related Adverse Effects
Orbital reconstruction and soft-tissue augmentation remain cornerstone treatments for enophthalmos but carry specific procedural risks. The complexity of orbital anatomy and the proximity to critical structures increase the likelihood of mechanical or neurovascular complications. Overcorrection resulting in exophthalmos may occur due to excessive implant volume or malposition, manifesting as globe protrusion and exposure keratopathy. Management involves early revision or implant adjustment. Undercorrection or residual enophthalmos results from inadequate orbital volume restoration, producing persistent asymmetry, and may require secondary surgery or autologous fat grafting. Diplopia or restrictive strabismus can result from entrapment of extraocular muscles or implant impingement, presenting as double vision and gaze restriction, and managed by forced duction testing and early surgical release.
Implant extrusion or infection may result from inadequate sterilization or tissue reaction, presenting with pain, discharge, or extrusion. Management includes intravenous antibiotics, implant removal, and delayed reconstruction. Orbital hemorrhage from intraoperative vessel injury produces pain, proptosis, and vision loss, necessitating emergency decompression and intravenous steroids. Optic neuropathy may develop from overpacking or direct trauma, causing decreased vision and relative afferent pupillary defect, requiring urgent decompression and high-dose intravenous steroids.
Fat Grafting and Tissue Augmentation Complications
Autologous fat transfer is a valuable, minimally invasive option for soft-tissue augmentation; however, complications may arise from graft resorption, necrosis, or migration. Partial resorption, which may reach up to 40%, is managed with repeat micrografting after 6 to 12 months. Fat necrosis and cyst formation may be minimized using the microdroplet technique with layered injection. Contour irregularities are addressed through secondary refinements or hyaluronic acid fillers. Infection or granuloma formation requires treatment with antibiotics or corticosteroid infiltration.[78] Emerging stem-cell–enriched fat grafting exhibits lower resorption rates and improved biocompatibility, reducing long-term complications.
Postradiation and Fibrosis-Associated Toxicity
Postradiation enophthalmos presents unique challenges due to chronic fibrosis, reduced vascularity, and delayed wound healing. Orbital fibrosis and contracture contribute to progressive globe retraction and lid stiffness. Tissue necrosis may develop in high-dose radiation fields exceeding 60 Gy. Secondary infection or osteoradionecrosis requires early antibiotic prophylaxis and, when indicated, hyperbaric oxygen therapy. Preventive strategies include initiating antifibrotic therapy, combining pentoxifylline and vitamin E, and doing so early in the postradiation phase. Reconstructive surgery should be delayed for 6 to 12 months to allow tissue stabilization. The use of vascularized flaps, such as temporalis fascia, in reconstruction enhances healing and reduces postoperative complications.
Anesthesia and Systemic Risks
Retrobulbar hemorrhage during orbital anesthesia can exacerbate enophthalmos or threaten vision. Systemic reactions to local anesthetics, such as lidocaine toxicity, may manifest as tremor, arrhythmia, or seizures and are managed with intravenous lipid emulsion therapy and supportive care. General anesthesia for orbital reconstruction carries standard perioperative risks, including airway compromise, thromboembolism, and anesthetic sensitivity.[79]
Preventive and Monitoring Protocols
Preventive and monitoring protocols for enophthalmos management span preoperative, intraoperative, postoperative, and long-term phases. Preoperatively, comorbidities such as diabetes and thyroid disease should be optimally controlled, patients counseled regarding expectations, and imaging obtained. Baseline assessments include exophthalmometry, visual acuity, and CT scanning. Intraoperative measures focus on avoiding overpacking, ensuring implant sterilization, and maintaining hemostasis, with continuous monitoring of the oculocardiac reflex.
Postoperative strategies aim at early detection of pain, swelling, or diplopia, with prophylactic antibiotics and steroids administered as indicated. Monitoring entails weekly evaluations for 1 month, followed by follow-up imaging at 3 to 6 months. Long-term management addresses fibrosis and soft-tissue atrophy through follow-up interventions, including annual imaging and functional ocular motility testing.
Emerging Strategies for Toxicity Reduction
Emerging strategies for toxicity reduction include the use of bioresorbable implants, which decrease chronic inflammation and lower the risk of extrusion. Three-dimensional navigation during surgery minimizes entrapment of extraocular muscles and undercorrection. Antioxidant and anti-transforming growth factor beta therapies demonstrate potential in mitigating radiation-induced fibrosis. AI–assisted implant design reduces intraoperative trial-and-error, enhancing long-term anatomical stability.
Staging
Although enophthalmos lacks a universally accepted formal staging system, classification often considers severity, etiology, and effects on ocular function and facial aesthetics. Staging informs clinical decision-making, particularly for surgical reconstruction and timing of intervention. The system integrates objective measurements obtained with exophthalmometry with subjective assessments and radiologic findings to evaluate disease progression and guide management.
Clinical Staging Based on Severity
Enophthalmos can be categorized into 3 stages based on posterior globe displacement, clinical features, functional impact, and suggested management.
- Stage I, mild enophthalmos, involves 1 to 2 mm displacement, barely perceptible asymmetry, subtle deepening of the superior sulcus, and minimal cosmetic concern. Function remains normal, and management is typically conservative, including observation or fillers for cosmetic correction.
- Stage II, moderate enophthalmos, includes 3 to 4 mm of displacement with readily visible posterior globe position, superior sulcus deformity, pseudoptosis, and eyelid malposition. Functional interference, such as tearing or lid lag, may occur, and medical management combined with minor surgical correction, including autologous fat or alloplastic implants, is recommended.
- Stage III, severe, presents with more than 5 mm of displacement, marked asymmetry, deep superior sulcus, lagophthalmos, diplopia, and restricted ocular motility. Significant functional disability and psychosocial distress are common, warranting major orbital reconstruction using customized 3D implants or grafts.
Etiology-Based Staging
Etiology-based staging of enophthalmos incorporates functional and structural considerations. Posttraumatic cases arise from orbital wall fractures with associated fat atrophy or fibrosis, typically presenting with delayed onset after fracture healing. These cases are often progressive and require imaging-guided reconstruction. Postinflammatory or infectious enophthalmos, resulting from chronic sinusitis or sclerosing orbital inflammation, is characterized by fibrosis and tissue retraction. Medical management is preferred, with reconstruction deferred until disease quiescence.
Postirradiation enophthalmos results from radiation-induced fibrosis and fat atrophy, which progress slowly as tissue stiffness increases. Surgery should be delayed, and antifibrotic therapy is indicated. Congenital or developmental forms, such as those associated with craniofacial anomalies or microphthalmos, present as early asymmetry with structural defects and are often static, with cosmetic management sufficient. Atrophic or degenerative enophthalmos, caused by age-related orbital fat loss and connective tissue laxity, is usually bilateral and symmetric. Correction with fillers or fat grafts is effective and carries low surgical risk.
Radiologic Staging
Radiologic staging using CT or MRI provides a quantitative and anatomical assessment of orbital volume and structural damage.
- Grade I corresponds to a less than 5% increase in orbital volume, with mild fat resorption and intact orbital walls, and is associated with mild enophthalmos of less than 2 mm.
- Grade II involves a 5% to 15% increase in orbital volume, characterized by medial or inferior wall bowing and minor defects, resulting in moderate displacement of 2 to 4 mm.
- Grade III indicates more than a 15% increase in orbital volume, with significant bony defects and fat herniation into the sinuses, resulting in severe enophthalmos exceeding 5 mm.
Functional Staging
Functional staging of enophthalmos based on oculomotor limitation and ocular surface compromise stratifies patients according to motility, corneal health, and surgical implications.
- Stage A is characterized by complete extraocular movements and a healthy ocular surface, indicating that cosmetic correction alone is sufficient.
- Stage B involves mild limitation in 1 to 2 gaze directions, accompanied by mild lagophthalmos or dry eye, necessitating combined functional and cosmetic reconstruction.
- Stage C is characterized by severe motility restriction and exposure keratopathy or ulceration, requiring urgent orbital decompression or reconstruction.
Proposed Comprehensive Clinical-Radiologic Staging System
The hypothetical Gurnani-Kaur model is a proposed comprehensive clinical-radiologic staging system. This framework integrates globe displacement, orbital volume change, functional impact, and treatment recommendations.
- Stage I is defined by less than 2 mm of globe displacement and less than 5% increase in orbital volume, with no functional impairment. Management consists of observation and conservative care.
- Stage II encompasses 2 to 4 mm of displacement and 5% to 10% increase in volume, with mild diplopia or ptosis. Minor reconstruction or filler therapy is recommended.
- Stage III involves 4 to 6 mm of displacement and 10% to 20% increase in volume, associated with moderate ocular motility restriction and cosmetic deformity. Treatment includes 3D-planned implants or autologous grafts.
- Stage IV is characterized by more than 6 mm of globe displacement and an increase of more than 20% in orbital volume, resulting in severe motility restriction and exposure keratopathy. A complex, possibly staged, reconstruction with volume replacement is indicated.
Natural History and Progression
Enophthalmos may evolve gradually over weeks to years, with progression dependent on etiology. Posttraumatic cases typically manifest within 2 to 6 weeks after injury due to fat atrophy and orbital remodeling. Postradiation enophthalmos progresses insidiously over months. Congenital forms are usually static but may become more pronounced with growth asymmetry. Early recognition of progressive cases permits timely surgical intervention, preventing secondary ocular surface complications and irreversible fibrosis.
Prognosis
The prognosis for enophthalmos varies primarily with the etiology. Surgical repair of orbital fractures in younger individuals generally yields excellent outcomes, with predictable correction of globe displacement. Residual enophthalmos and limited extraocular motility may persist depending on fracture dimensions, volume of herniated orbital tissue, and rounding of inferior rectus margins.[80] Sinus-related cases have favorable outcomes following antrostomy. However, correction of enophthalmos after isolated sinus surgery varies and may require additional orbital floor reconstruction.
Early follow-up after orbital volume augmentation procedures demonstrates excellent correction, though long-term maintenance is variable. Fat transplantation may result in secondary lipoatrophy, leading to recurrent enophthalmos. Targeted treatment of enophthalmos is rarely indicated in orbital metastatic disease, as management prioritizes primary tumor control and systemic therapy. Neoadjuvant chemotherapy, radiotherapy, and targeted therapies are often considered before orbital exenteration.
The prognosis for enophthalmos varies widely depending on the underlying etiology, timing of diagnosis, and appropriateness of intervention. As a secondary manifestation rather than a primary disease, outcomes depend on effective management of the root cause, including trauma, chronic inflammation, fibrosis, or postradiation changes. Early identification and timely intervention generally yield the best functional and cosmetic results. Mild enophthalmos typically remains stable and may be managed conservatively with observation or cosmetic correction. Moderate-to-severe cases often progress and may result in permanent orbital deformity, restriction of ocular motility, or exposure keratopathy if left untreated.
Prognostic Determinants
The prognosis for enophthalmos varies by underlying cause. Posttraumatic cases have a good prognosis when orbital reconstruction occurs within 2 to 3 weeks. Delayed interventions often require secondary reconstruction complicated by scarring and fibrosis. Postinflammatory or postinfectious enophthalmos depends on the resolution of the primary inflammatory process; in long-standing conditions such as sclerosing orbital pseudotumor, this process may be incomplete, potentially leading to irreversible tissue contracture.
Postradiation enophthalmos is frequently progressive and refractory due to ongoing fibrosis and fat atrophy. Reconstructive procedures may achieve partial correction but rarely complete symmetry. Congenital and developmental forms are generally stable, with favorable cosmetic outcomes achievable via prosthetic or surgical approaches. Senile or involutional atrophy is typically bilateral, with an excellent prognosis for cosmetic rehabilitation using fillers or fat grafting.
The timing of intervention influences outcomes. Early correction within 4 weeks restores orbital volume and globe projection more effectively, minimizing diplopia and lid deformity. In contrast, late intervention after 3 months is associated with poorer function due to fibrosis, implant malposition, or muscle contracture. The severity of the condition further guides prognosis. Mild enophthalmos carries minimal impact and excellent conservative outcomes. Moderate enophthalmos can be corrected with predictable results using autologous fat or alloplastic implants. Severe enophthalmos often requires complex reconstruction with a persistent risk of asymmetry or diplopia.
Associated ocular and systemic conditions influence recovery from enophthalmos. Coexisting orbital floor fractures, sinus disease, or fibrotic conditions such as thyroid eye disease may complicate outcomes. Connective tissue disorders or prior radiation damage slow healing and increase the risk of recurrence. Surgical factors significantly affect reconstructive accuracy and aesthetic results. Advances in 3D imaging, intraoperative navigation, and patient-specific implants have improved precision. Use of biocompatible materials, including porous polyethylene, titanium mesh, and polyetheretherketone, reduces the risk of infection and extrusion, thereby enhancing long-term stability. However, revision surgeries carry a higher risk of implant displacement, infection, or persistent asymmetry.
Functional and cosmetic outcomes are key indicators of success. Functional goals include restoring ocular alignment and motility and preventing exposure keratopathy. Cosmetic goals focus on improving facial symmetry and correcting superior sulcus deformity, thereby enhancing psychological and social well-being. In experienced hands, 70% to 85% of patients achieve clinically acceptable correction, with less than 1 mm residual asymmetry.
Long-Term Outlook
The long-term prognosis for enophthalmos is favorable with timely diagnosis and individualized management. Functional and cosmetic stability is typically achieved within 6 to 12 months postreconstruction. Secondary procedures may be necessary to correct undercorrection or overcorrection. Radiation-induced and fibrotic enophthalmos requires lifelong follow-up to monitor delayed atrophy or implant migration. Early rehabilitation, including ocular physiotherapy, lubrication, and periocular massage, enhances recovery. Interprofessional care involving ophthalmologists, oculoplastic surgeons, and radiologists optimizes outcomes.
Complications
Surgical management of enophthalmos carries potential complications, including facial asymmetry, residual or persistent diplopia, limitations of extraocular muscle motility, traumatic optic neuropathy, and central retinal artery occlusion following volume augmentation procedures. Additional risks include cheek anesthesia from infraorbital nerve injury, lid and lash malposition such as entropion or ectropion, and iatrogenic worsening of enophthalmos due to secondary ischemia of orbital fat or lipoatrophy.
These complications stem from both the underlying disease and interventions employed for correction. Anatomical, functional, and cosmetic adverse effects can occur at any stage of diagnosis, conservative management, or surgical reconstruction. Early recognition and prompt management are essential to minimize morbidity and optimize functional and aesthetic outcomes.
Disease-Related Complications
Disease-related complications of enophthalmos include cosmetic deformity, ocular surface compromise, and diplopia with ocular motility restriction. Tear film instability and sinus-related issues are also common complications. Cosmetic deformity results from progressive posterior displacement of the globe, producing facial asymmetry and a deep superior sulcus deformity, which can cause psychological distress and reduced self-esteem. Management includes cosmetic fillers, fat grafting, or surgical correction. Ocular surface compromise arises from lagophthalmos and poor lid-globe congruity, leading to persistent irritation, epithelial breakdown, or corneal ulceration. Treatment consists of lubrication, tarsorrhaphy, and surgical realignment. Diplopia and motility restriction occur secondary to fibrotic entrapment or extraocular muscle imbalance, producing visual confusion and functional disability. Prism correction or muscle release surgery may be required.
Tear film instability develops from altered eyelid apposition or punctal malposition, resulting in epiphora or dry eye syndrome. Management includes lubricants and punctal repositioning. Sinus-related complications that occur after orbital floor fractures or sinusitis-induced volume loss can lead to chronic sinus infection or orbital cellulitis. Systemic antibiotics or sinus surgery are indicated.
Surgery-Related Complications
Surgical management–related complications of enophthalmos arise from various mechanisms and can manifest with functional or cosmetic deficits. Overcorrection or undercorrection of orbital volume may cause asymmetric globe projection and aesthetic dissatisfaction, which can be managed with secondary revision or implant adjustment. Inadequate orbital wall repositioning or entrapment of extraocular muscles can result in diplopia in specific gaze positions, which may be treated with prism correction or reoperation. Scarring, fibrosis, or mechanical restriction from the implant may result in ocular movement restriction and diplopia, which can be managed with physiotherapy or surgical release.
Intraoperative compression or direct trauma can lead to sudden postoperative visual loss, requiring high-dose steroids and urgent decompression. Elevated intraocular pressure during volume augmentation may cause sudden, painless visual loss with an afferent pupillary defect, which can be managed with ocular massage, intraocular pressure reduction, and acetazolamide. Direct injury during orbital floor surgery can result in cheek or upper lip anesthesia, typically resolving over weeks to months.
Scarring or improper tension during lid reconstruction can cause ocular irritation and exposure; these complications are treated surgically. Secondary fat atrophy or ischemia following overdissection may deepen the superior sulcus and worsen asymmetry, necessitating secondary augmentation or autologous fat grafting. Poor asepsis or a foreign-body reaction can lead to swelling, discharge, and implant exposure, necessitating antibiotics and possible implant removal or replacement.
Long-Term and Delayed Complications
Long-term and delayed complications of enophthalmos management include implant-related issues, scarring and fibrosis, postradiation effects, and psychological consequences. Implant-related complications such as migration, infection, or extrusion may occur months to years after surgery and typically require surgical revision. Chronic scarring and fibrosis can tether orbital tissues, resulting in restrictive diplopia and cosmetic deformity, which are difficult to reverse. Postirradiation effects, including fat necrosis and vascular insufficiency, lead to progressive worsening of enophthalmos and are often irreversible. Psychological consequences, such as cosmetic dissatisfaction and anxiety, can affect quality of life and may necessitate counseling or cosmetic revision.
Preventive Measures and Risk Reduction
Preventive measures and risk reduction in enophthalmos management begin with meticulous preoperative planning using high-resolution CT or MRI to assess orbital volume and defect. Atraumatic dissection techniques minimize manipulation of orbital fat, reducing the risk of ischemic lipoatrophy. Intraoperative 3D navigation ensures symmetric volume restoration, whereas careful implant selection using biocompatible materials, such as polyetheretherketone or porous polyethylene, reduces the risk of complications. Postoperative monitoring includes regular exophthalmometry and photographic documentation. Early recognition and management of complications, such as diplopia, motility limitation, or visual symptoms, require prompt reassessment.
Postoperative and Rehabilitation Care
Postoperative and rehabilitation care following enophthalmos surgery is a crucial phase that determines the long-term cosmetic, functional, and visual outcomes. The primary goals are to promote healing, maintain implant position, prevent infection, restore ocular motility, and ensure patient satisfaction with both appearance and function. Effective interprofessional coordination among ophthalmologists, oculoplastic surgeons, physiotherapists, and rehabilitation specialists is vital for comprehensive recovery.
Immediate Postoperative Phase
The immediate postoperative phase (days 0–7) focuses on pain control, edema management, and infection prevention. Head-end elevation at 30° to 45° helps reduce periorbital edema, while cold compresses for 10 to 15 minutes every few hours during the first 48 hours are beneficial. Broad-spectrum antibiotics (topical and systemic), anti-inflammatory agents, and lubricating eye drops are routinely prescribed. The surgical site must remain clean and dry, with nonabsorbable sutures removed after 5 to 7 days. Ocular protection with a moisture chamber or eye shield prevents accidental trauma or exposure keratopathy. Activity restriction avoids heavy lifting, bending, or straining to prevent orbital hemorrhage or implant displacement. Daily monitoring of proptosis, diplopia, pupillary reactions, and signs of retrobulbar hemorrhage is essential.[81]
Early Rehabilitation Phase
During the early rehabilitation phase (weeks 2–6), assessment of visual and cosmetic outcomes is performed as edema resolves. Exophthalmometry measurements are compared with preoperative values to confirm the desired globe projection. Supervised ocular motility exercises begin to prevent restrictive fibrosis. Key components include gentle horizontal and vertical gaze exercises to maintain extraocular muscle elasticity, eyelid stretching and blink training to prevent lagophthalmos and retraction, and frequent use of preservative-free lubricants for corneal protection. Scar management with silicone gel and gentle massage helps prevent hypertrophic scarring in lower lid incisions. Psychological counseling addresses cosmetic concerns and adjusts patient expectations for symmetry.
Intermediate Rehabilitation Phase
During the intermediate rehabilitation phase (months 2–6), monthly assessments monitor implant position, ocular motility, diplopia, and cosmetic outcomes. Residual asymmetry greater than 2 mm may warrant secondary interventions, including autologous fat grafting, hyaluronic acid filler injection, or minor implant adjustments. Radiologic evaluation with CT or MRI can confirm orbital volume adequacy and implant placement. Persistent motility restriction may require scar lysis or extraocular muscle rebalancing surgery. In orbits affected by radiation or fibrosis, ongoing physical therapy and soft tissue expansion can enhance long-term volume retention.
Long-Term Maintenance
Long-term maintenance after 6 months focuses on preserving surgical results and preventing relapse. Follow-up at 6-month intervals monitors implant integration, orbital volume stability, ocular surface integrity, and tear film dynamics. Delayed complications, including lipoatrophy or implant migration, are identified and addressed, and cosmetic refinements such as fat grafting, fillers, or lid contour correction are planned as needed. Patients receive counseling on UV protection, adequate hydration, and avoidance of trauma to the reconstructed orbit. Regular ocular lubrication is essential in cases with partial lagophthalmos or reduced blinking frequency to prevent late lipoatrophy or implant displacement.[82]
Consultations
Most patients with enophthalmos require multispecialty care. Orbitofacial trauma cases necessitate the expertise of oculofacial plastic surgeons, maxillofacial surgeons, and, at times, neurosurgeons during fracture repair. Sinus disorders require coordination among otolaryngologists, maxillofacial surgeons, and oculoplasty surgeons. Systemic disorders causing lipoatrophy demand consultation with physicians and rheumatologists to diagnose and treat underlying autoimmune involvement before local cosmetic correction can be planned.
Orbital metastatic disease similarly requires an interprofessional team for diagnosis and management planning, including oncologists, oncosurgeons, radiation oncologists, radiologists, nuclear medicine specialists, and orbit surgeons. The ocularist plays an essential role in designing customized prostheses during rehabilitation for anophthalmic and microphthalmic sockets. Management of enophthalmos, particularly when secondary to trauma, chronic inflammation, or surgical sequelae, also necessitates an interprofessional approach involving multiple specialties. The complexity arises from multifactorial etiology, including orbital volume loss and fat atrophy, and requires expertise in imaging, reconstructive surgery, ocular motility, and cosmetic rehabilitation. Early consultation with appropriate specialists ensures accurate diagnosis, comprehensive care, and optimal functional and aesthetic recovery.
Ophthalmologists and oculoplastic surgeons serve as the primary coordinators of care, evaluating globe displacement, eyelid malposition, ocular motility, and visual function. Responsibilities include performing exophthalmometry, motility assessment, and fundus evaluation; planning and executing corrective procedures such as orbital reconstruction, volume augmentation, and lid realignment; and providing long-term follow-up to ensure implant stability and cosmetic symmetry. Referral should occur immediately for all confirmed cases of posttraumatic or progressive enophthalmos.
Maxillofacial and craniofacial surgeons are critical for orbital wall reconstruction and management of midface or zygomatic fractures. Tasks include reconstructing bony orbital defects, restoring normal orbital volume, employing 3D reconstruction and intraoperative navigation for precision, and managing associated facial asymmetry or malocclusion in extensive trauma cases. Radiologists are essential for diagnostic evaluation and postoperative monitoring. Responsibilities include performing CT and MRI scans to assess orbital volume loss, fat atrophy, and muscle displacement, providing 3D volumetric analysis to guide reconstructive planning, and monitoring implant positioning and postsurgical healing. Key imaging findings include increased orbital volume, posterior globe displacement, floor or medial wall discontinuity, and fat herniation or fibrosis.
Neurologists and neuro-ophthalmologists evaluate optic nerve involvement and associated cranial neuropathies. Responsibilities include assessing traumatic optic neuropathy or orbital apex syndrome, managing diplopia from muscle paresis or neuropathy, and initiating neuroprotective or steroid therapy when indicated. Plastic and reconstructive surgeons focus on cosmetic rehabilitation and soft-tissue restoration in chronic or disfiguring conditions. Duties include performing fat grafting, dermal filler injection, or flap procedures to correct soft-tissue asymmetry; coordinating with oculoplastic surgeons to achieve combined structural and cosmetic outcomes; and addressing sequelae such as cicatricial ectropion or superior sulcus deformity.[83]
Physiotherapists and occupational therapists facilitate functional recovery and rehabilitation of ocular motility and periocular muscles. Responsibilities include guiding ocular movement exercises and eyelid rehabilitation, implementing facial massage techniques to reduce postoperative stiffness, and assisting in restoring binocular coordination and depth perception.[84] Psychiatrists and psychologists address psychological distress related to facial asymmetry and disfigurement. Responsibilities include providing counseling and cognitive-behavioral support, assisting with adjustment to postoperative appearance and body image, and evaluating for posttraumatic stress in injury-related cases.[85]
Optometrists and orthoptists support visual rehabilitation and binocular balance. Duties include assessing refraction, binocular vision, and convergence insufficiency, prescribing prisms or occlusion therapy for residual diplopia, and participating in long-term follow-up to restore visual function. Anesthesiologists and pain specialists optimize perioperative safety and manage chronic postoperative pain. Responsibilities include providing anesthesia tailored to orbital and facial reconstruction and managing postoperative infraorbital nerve pain or sensory neuropathy.[86] Optimal management of enophthalmos requires coordinated care by an interprofessional team integrating diagnostic precision, reconstructive expertise, and long-term rehabilitation. The condition’s diverse etiologies necessitate collaboration among oculoplastic surgeons, ophthalmologists, radiologists, maxillofacial specialists, optometrists, psychologists, and rehabilitation therapists to achieve both functional restoration and cosmetic symmetry.
Deterrence and Patient Education
Essential patient education for new enophthalmos emphasizes the potential impact on vision and daily activities, including driving and work, particularly when diplopia is present. In cases involving orbital fractures, patients must avoid nose blowing to prevent orbital emphysema. Education focuses on preventing avoidable causes, promoting early recognition, and ensuring adherence to rehabilitation and follow-up protocols. Given that enophthalmos may result from trauma, infection, iatrogenic factors, or chronic disease, patient awareness regarding ocular safety, symptom monitoring, and postoperative care is critical to minimizing complications and improving long-term outcomes.[87]
Preventive counseling and risk awareness should include guidance on the etiological diversity of enophthalmos and the importance of prompt evaluation for facial trauma, orbital swelling, or visual changes. Trauma prevention involves the use of protective eyewear in high-risk occupations such as construction, welding, and sports. Iatrogenic risk reduction includes discussion of potential volume loss, fat atrophy, or scarring in patients undergoing sinus or orbital surgery, highlighting the importance of experienced surgical care. Infectious and inflammatory control requires adherence to treatment in chronic sinusitis, scleroderma, or autoimmune orbital disease to prevent progressive tissue loss. Radiation-related precautions for oncology patients involve regular ophthalmic monitoring to detect radiation-induced fibrosis and lipoatrophy.
Early detection and patient self-monitoring are essential for prompt recognition of enophthalmos progression. Key warning signs include a sunken eye or facial asymmetry, double vision or restricted ocular movement, progressive eyelid malposition or drooping, and altered depth perception, tearing, or foreign body sensation. Mirror-based symmetry checks and comparison with previous photographs can aid in identifying subtle globe displacement. In trauma cases, early imaging and ophthalmic evaluation within 48 to 72 hours can prevent late-stage enophthalmos caused by fibrosis or bone resorption.[88]
Postoperative education is critical for maintaining surgical results and preventing secondary complications. Regular follow-up should occur monthly during the first 6 months and biannually thereafter. Patients must avoid trauma, pressure, or manipulation over the reconstructed orbit and maintain adequate ocular lubrication, reporting symptoms such as diplopia, redness, or pain promptly. Final cosmetic symmetry may require several months to achieve, with secondary procedures such as fillers or fat grafting occasionally necessary for refinement. Realistic expectations regarding functional and aesthetic recovery should be emphasized. Provision of written instructions, postoperative photographs, and visual rehabilitation handouts enhances compliance and confidence.[89]
Psychosocial education and support are integral to comprehensive enophthalmos management. Facial asymmetry and altered appearance can induce significant emotional distress, anxiety, or social withdrawal. Early psychological counseling promotes body image acceptance and fosters effective coping strategies. Group counseling or peer support programs, particularly for trauma survivors, reduce isolation and facilitate long-term adjustment. Family counseling ensures caregivers understand patient limitations and follow-up requirements.[90]
Lifestyle modifications further optimize outcomes. Smoking cessation and nutritional optimization enhance wound healing and protect orbital fat vascularity. Adequate hydration and sun protection minimize postradiation fibrosis and skin thinning. Avoidance of rapid weight loss is important, as it can exacerbate orbital fat atrophy and worsen enophthalmos.[91]
Patient education benefits from reinforcement by all members of the interprofessional care team. The oculoplastic surgeon explains the disease process, surgical options, and realistic outcomes. The ophthalmologist provides vision-related counseling and strategies for ocular protection. Optometrists and physiotherapists guide eye exercises, visual adaptation, and coordination therapy. Nurse educators or rehabilitation specialists reinforce wound care, hygiene, and medication adherence. Psychologists or counselors offer long-term emotional support and strategies for mental well-being.[92]
Patient education materials enhance understanding and compliance. Illustrated pamphlets should describe why the eye appears sunken and how orbital reconstruction helps. Preoperative and postoperative diagrams depict expected healing timelines. Quick response code–linked videos demonstrate ocular exercises and safety measures. Written guidelines for postorbital surgery home care outline signs of infection, instructions for contacting the physician, and the importance of ocular lubrication.[93]
Pearls and Other Issues
Enophthalmos remains a clinically significant yet frequently underdiagnosed orbital condition that demands a high index of suspicion and comprehensive evaluation. Early recognition of subtle presentations and accurate differentiation between true and pseudo-enophthalmos are crucial to ensure appropriate management and prevent long-term deformity or functional compromise. Key considerations during evaluation and management of this condition include the following:
- Differentiate true vs pseudo-enophthalmos early. True enophthalmos reflects loss of orbital volume or enlargement of the bony orbit, while pseudo-enophthalmos arises from eyelid malposition, microphthalmos, or contralateral proptosis. Accurate distinction prevents misdirected surgical planning.
- Early imaging prevents late deformity. In posttraumatic presentations, CT or MRI within 48 to 72 hours identifies orbital wall defects, fat herniation, or early displacement before fibrosis develops. Timely diagnosis supports appropriate reconstruction and reduces secondary volume loss.
- Quantify, do not estimate. Hertel exophthalmometry or digital 3D volumetric CT analysis provides an objective measurement of globe position and orbital asymmetry. Even mild displacement (<2 mm) may produce clinically and cosmetically meaningful changes.
- Volume assessment is essential, not only the bony contour. Focusing solely on skeletal reconstruction without evaluating orbital fat atrophy or fibrosis often results in persistent enophthalmos. Soft tissue augmentation frequently must accompany bony correction to achieve symmetry.
- Avoid overcorrection. Excessive implant volume or filler augmentation risks secondary exophthalmos, diplopia, or pressure-related optic neuropathy. Target symmetry under physiologic gaze rather than intraoperative over-projection.
- Recognize superior sulcus deformity as a diagnostic indicator. A deep superior sulcus frequently reflects involutional or postsurgical orbital fat loss. Early identification directs evaluation toward soft tissue or implant-related etiologies rather than isolated bony defects.
- Prioritize functional restoration alongside cosmetic outcomes. Management success hinges on the recovery of binocular vision, depth perception, and ocular motility. Diplopia, muscle imbalance, and visual comfort should be addressed throughout all treatment phases.[94]
Critical pitfalls encountered in the evaluation and management of this condition include the following:
- Delayed diagnosis in chronic cases: Gradual-onset enophthalmos associated with radiation injury, scleroderma, or chronic sinus disease may remain subtle for extended periods, resulting in late presentation and suboptimal reconstructive outcomes.
- Underestimating fat atrophy: Postinflammatory or postsurgical orbital fat atrophy may progress for several months. Regular volumetric assessment is necessary before finalizing reconstructive timing to prevent undercorrection or overcorrection.
- Ignoring the contralateral eye: Symmetry assessment must incorporate contralateral orbital measurements. Reconstruction performed without reference to the unaffected side risks persistent asymmetry despite anatomically adequate repair.
- Neglecting psychological impact: Facial asymmetry and altered orbital contour can produce considerable psychosocial distress. Early counseling and structured expectation management form essential components of comprehensive care.
- Failure to coordinate interprofessional care: Insufficient communication among radiology, oculoplastic, and maxillofacial teams may result in incomplete correction of combined osseous and soft tissue deficits, reducing overall functional and cosmetic success.
Important considerations in preventing enophthalmos include the following:
- Use of protective equipment in high-risk sports and occupational settings significantly reduces orbital trauma incidence, the leading preventable cause of enophthalmos.
- Adoption of meticulous surgical technique during orbital and sinus procedures minimizes fat necrosis, scarring, and neurovascular injury, thereby lowering the likelihood of delayed orbital volume loss.
- Scheduling of periodic follow-up imaging after major facial trauma or sinus surgery enables early detection of evolving orbital volume changes that may progress to enophthalmos.
- Timely treatment of sinus infections and autoimmune disorders limits chronic orbital inflammation and fibrosis, reducing the risk of progressive tissue loss and late enophthalmos development.[95]
Long-term management after enophthalmos correction requires ongoing surveillance, particularly in cases associated with trauma, prior radiation, or systemic disease. Reconstructed orbital volume, both implant position and residual fat, should be assessed annually with CT or MRI to ensure stability and to identify evolving asymmetry. Minor postoperative volume discrepancies may be addressed with minimally invasive adjuncts such as autologous fat grafting or hyaluronic acid filler augmentation. Optimal outcomes are achieved when functional recovery aligns with cosmetic restoration, underscoring the value of individualized planning and consistent interprofessional coordination.
Enhancing Healthcare Team Outcomes
Enophthalmos can present subtly while substantially affecting visual function and facial aesthetics. Etiologies include trauma, orbital fat atrophy, inflammatory or infectious processes, congenital anomalies, and iatrogenic changes. Accurate detection requires clinical assessment, including exophthalmometry, and advanced imaging, such as CT or MRI, to quantify orbital volume loss and soft-tissue alterations. Differentiating true enophthalmos from pseudo-enophthalmos, resulting from globe malposition or orbital asymmetry, is critical for accurate diagnosis and management. Management of enophthalmos requires a coordinated interprofessional approach that integrates clinical, surgical, rehabilitative, and psychosocial expertise.
Oculoplastic surgeons oversee surgical recovery, cosmetic outcomes, and any necessary secondary procedures. Coordination between oculoplastic and maxillofacial surgeons ensures that orbital reconstruction restores bone volume in alignment with soft-tissue correction. Ophthalmologists monitor visual acuity, ocular surface integrity, and extraocular motility.
Physicians, advanced practitioners, and nurses perform patient evaluation, perioperative care, and longitudinal monitoring. Radiologists provide imaging interpretation for surgical planning, while optometrists and orthoptists support visual function and binocular coordination. Nursing staff maintain continuity of postoperative care, enforce wound hygiene, reinforce patient education, and enable early detection of complications, including implant migration or infection.[96] Physiotherapists and rehabilitation specialists facilitate ocular and periocular muscle rehabilitation, providing guided motility exercises and facial physiotherapy to reduce stiffness and optimize functional outcomes.
Pharmacists ensure medication safety, and rehabilitation specialists facilitate the recovery of ocular and facial mobility. Psychologists address appearance-related anxiety and promote adherence to treatment plans. Structured interprofessional communication and shared decision-making enable coordinated care, enhance patient safety, and improve functional and aesthetic outcomes, supporting a patient-centered approach that maximizes quality of life. Regular interprofessional case discussions using shared digital platforms or clinical review boards facilitate consensus on surgical timing, imaging interpretation, and patient progress. These discussions minimize duplication of efforts and enhance overall clinical efficiency.
Ethical Considerations and Patient-Centered Care
Ethical practice in the management of enophthalmos emphasizes informed consent, realistic expectation setting, and shared decision-making. Patients must understand the nature of the deformity, the potential limitations of reconstructive procedures, and the long-term implications of the chosen interventions. Transparency regarding surgical risks, including optic nerve injury, undercorrection, or cosmetic asymmetry, is essential. Respect for patient autonomy and empathetic discussion of appearance-related concerns strengthen the therapeutic alliance and improve satisfaction.
Strategies to Improve Team-Based Outcomes
Interprofessional orbital clinics centralize care by bringing together surgeons, radiologists, and optometrists to jointly evaluate patients, enabling same-day imaging, discussion, and procedural planning. Standardized care pathways, including checklists and treatment algorithms for trauma-related and involutional enophthalmos, ensure consistent evaluation and reduce oversight. Shared digital records through cloud-based or AI-supported systems enhance communication and minimize data silos by consolidating imaging and progress documentation.
Simulation and skill workshops, including interprofessional surgical simulations and cadaveric dissections, strengthen understanding of orbital anatomy and procedural expectations. Regular outcome audits foster accountability and continuous quality improvement by providing feedback on surgical success, patient satisfaction, and complication rates. Incorporating patient-reported outcome measures into follow-up assessments enables systematic tracking of visual comfort, cosmetic satisfaction, and psychosocial adjustment.
Enhancing Patient Safety and Long-Term Care
Effective interprofessional team functioning improves patient safety by preventing errors and enabling early detection of complications. Nurses and pharmacists monitor for iatrogenic medication reactions and postoperative infections. Rehabilitation teams identify early implant displacement or fibrosis, facilitating timely reassessment. Psychologists address emotional well-being and support adherence, reducing attrition from follow-up schedules. A coordinated team approach ensures delivery of personalized, evidence-based, and ethically grounded care, enhancing long-term outcomes and minimizing the need for recurrence or revision surgery.
Leadership and Continuous Improvement
Leadership within the care team rotates according to the stage of management: radiologists lead diagnostics, surgeons direct treatment, and rehabilitation specialists oversee recovery. Regular morbidity-mortality meetings and case reviews cultivate transparency and continuous learning, reducing preventable complications. An interprofessional learning model with cross-training in communication, counseling, and shared decision-making enhances empathy, efficiency, and team cohesion.
Key Takeaways
Enophthalmos illustrates a condition in which a coordinated, ethics-driven, interprofessional approach directly impacts visual outcomes, cosmetic results, and overall patient quality of life. Collaborative integration across diagnostics, surgery, rehabilitation, and counseling transforms a potentially disfiguring condition into a successful reconstructive and restorative outcome.[97]
Media
(Click Image to Enlarge)
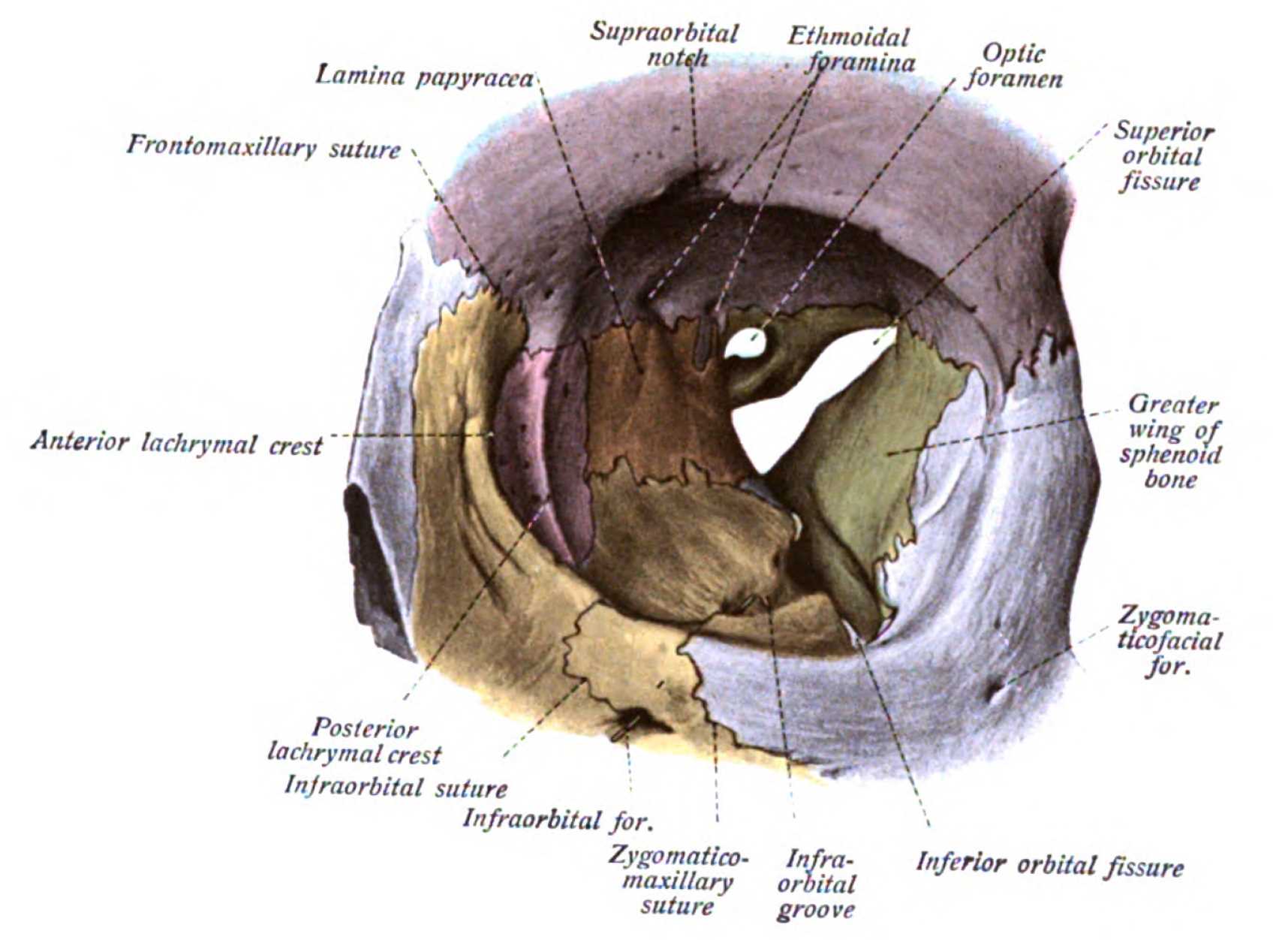
Orbit, Anterior View. Shown in this illustration are the supraorbital notch, ethmoidal foramina, optic foramen, superior orbital fissure (hourglass configuration), greater wing of the sphenoid bone, zygomaticofacial foramen, inferior orbital fissure, infraorbital groove, zygomaticomaxillary suture, infraorbital foramen, infraorbital suture, posterior lacrimal crest, anterior lacrimal crest, frontomaxillary suture, and lamina papyracea. The walls of the orbit include the frontal bone superiorly; ethmoid, frontal, lacrimal, and sphenoid bones medially; maxilla, zygomatic, and palatine bones inferiorly; and zygomatic and sphenoid bones laterally.
Johannes Sobotta, MD, Public Domain, Wikimedia Commons
(Click Image to Enlarge)

Enophthalmos Examination. The chin-up view, also referred to as the "dog’s view" or "lover’s view," allows optimal visual assessment of relative enophthalmos or proptosis. In this patient, left-sided proptosis creates the appearance of right-sided enophthalmos.
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)
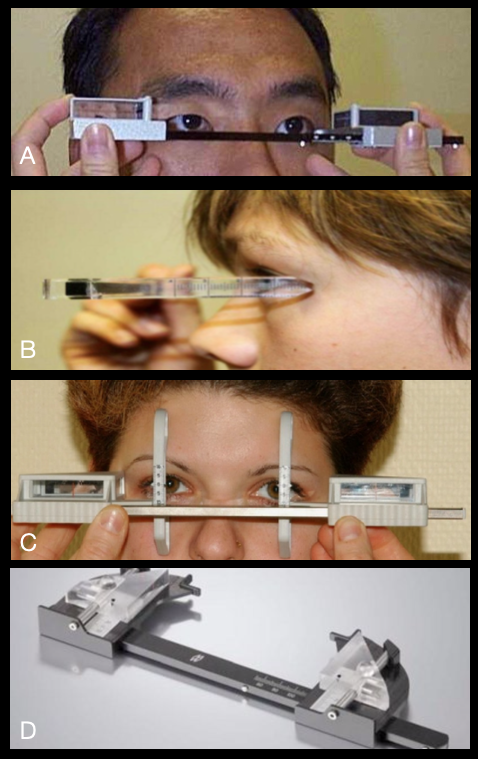
Types of Exophthalmometers. Globe position can be measured using various exophthalmometers: Hertel (A), Leudde (B), Naugle (C), and Mourits (D).
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)

Phthisis Bulbi. The image demonstrates phthisis bulbi of the right eye following intraocular infection. Globe shrinkage creates a sunken appearance that mimics enophthalmos.
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)

Microphthalmos. This condition produces a smaller globe and reduced corneal diameter, creating an apparent sunken appearance that can be mistaken for true enophthalmos.
Contributed by BCK Patel, MD, FRCS
References
Patel BC. In Praise of Precision: Esoglobus and Exoglobus. Ophthalmic plastic and reconstructive surgery. 2017 Jan/Feb:33(1):72-73. doi: 10.1097/IOP.0000000000000817. Epub [PubMed PMID: 27811634]
Farooq S, Bhat MY, Rastogi R, Bansal A, Angel A, Hammannavar R, Chaudhari V. Functional and Aesthetic Outcomes of the Subtarsal Approach in Zygomaticomaxillary Complex Fractures With Orbital Floor Involvement: A Prospective Cohort Study. Cureus. 2025 Sep:17(9):e93604. doi: 10.7759/cureus.93604. Epub 2025 Sep 30 [PubMed PMID: 41179033]
Puri A, Straughan AJ, Klingele CK, Godse NR. Beyond the Maxillary Sinus: A Proposed Classification of Chronic Sinus Atelectasis. The Annals of otology, rhinology, and laryngology. 2025 Nov 5:():34894251388846. doi: 10.1177/00034894251388846. Epub 2025 Nov 5 [PubMed PMID: 41190455]
Joachim MV, Farsio F, Markiewicz MR, Miloro M. Patient-specific Implants in Post-traumatic Orbital Reconstruction: A Systematic Review. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2025 Oct 15:():. pii: S0278-2391(25)00847-X. doi: 10.1016/j.joms.2025.10.003. Epub 2025 Oct 15 [PubMed PMID: 41177522]
Level 1 (high-level) evidenceSheta MS, Elsaadany WH. The accuracy of reconstruction of orbital wall fractures using prebent mesh versus patient specific implants: a randomized clinical trial. BMC oral health. 2025 Nov 1:25(1):1719. doi: 10.1186/s12903-025-07082-z. Epub 2025 Nov 1 [PubMed PMID: 41176602]
Level 1 (high-level) evidenceDjafar JV, Kopecny LR, Yeap I, Pitman A, Francis IC. Forced Duction Testing for Management of Small Orbital Floor Blowout Fractures. Cureus. 2025 Sep:17(9):e93001. doi: 10.7759/cureus.93001. Epub 2025 Sep 23 [PubMed PMID: 41140981]
Lee CYPD, Rees A, Al-Wizni A, Saleki M, Attygalla M, Dharmasena A. Bone grafts versus titanium mesh implants in orbital fracture management: a systematic review and meta-analysis. Orbit (Amsterdam, Netherlands). 2025 Oct 8:():1-10. doi: 10.1080/01676830.2025.2554890. Epub 2025 Oct 8 [PubMed PMID: 41061148]
Level 1 (high-level) evidenceKitsos-Kalyvianakis K, Bontzos G, Kyriazi S, Detorakis ET, Drakonaki EE. Progressive Visual Field Loss in the Setting of Severe Orbital Fat Atrophy. Cureus. 2025 Sep:17(9):e91711. doi: 10.7759/cureus.91711. Epub 2025 Sep 6 [PubMed PMID: 41058829]
Jamal RF, Azariah E, Pandyan D, Chinnaswami R. Validation of Modified Hertel Exophthalmometer. Craniomaxillofacial trauma & reconstruction. 2021 Sep:14(3):174-182. doi: 10.1177/1943387520954625. Epub 2020 Sep 11 [PubMed PMID: 34471472]
Level 1 (high-level) evidenceWhyte A, Boeddinghaus R. The maxillary sinus: physiology, development and imaging anatomy. Dento maxillo facial radiology. 2019 Dec:48(8):20190205. doi: 10.1259/dmfr.20190205. Epub 2019 Aug 13 [PubMed PMID: 31386556]
Wilkins RB, Kulwin DR. Spontaneous enophthalmos associated with chronic maxillary sinusitis. Ophthalmology. 1981 Sep:88(9):981-5 [PubMed PMID: 7301315]
Wang KJ, Li SS, Wang HY. Psychological symptoms in anophthalmic patients wearing ocular prosthesis and related factors. Medicine. 2020 Jul 17:99(29):e21338. doi: 10.1097/MD.0000000000021338. Epub [PubMed PMID: 32702931]
Mayo J, Schubert W. Enophthalmos: Historical Perspective on Definitions, Measurement Devices, and Clinical Significance. Craniomaxillofacial trauma & reconstruction. 2024 Dec:17(4):324-330. doi: 10.1177/19433875241236343. Epub 2024 Feb 23 [PubMed PMID: 39553789]
Level 3 (low-level) evidenceErkoç MF, Öztoprak B, Gümüş C, Okur A. Exploration of orbital and orbital soft-tissue volume changes with gender and body parameters using magnetic resonance imaging. Experimental and therapeutic medicine. 2015 May:9(5):1991-1997 [PubMed PMID: 26136927]
Ahmad Nasir S, Ramli R, Abd Jabar N. Predictors of enophthalmos among adult patients with pure orbital blowout fractures. PloS one. 2018:13(10):e0204946. doi: 10.1371/journal.pone.0204946. Epub 2018 Oct 5 [PubMed PMID: 30289909]
Asiri M, Aldowah O. Ocular Findings in Patients with Orbital Fractures: A 1-Year Prospective Study in a Tertiary Center. Medicina (Kaunas, Lithuania). 2023 Jun 5:59(6):. doi: 10.3390/medicina59061091. Epub 2023 Jun 5 [PubMed PMID: 37374295]
Somogyi R, Smith S, Kark J, Ryu WHA, Yoo J. Age-Based Incidence of Dens Fracture Has Unimodal Distribution Rather Than Commonly Claimed Bimodal Distribution. JB & JS open access. 2024 Jan-Mar:9(1):. doi: 10.2106/JBJS.OA.23.00059. Epub 2024 Jan 11 [PubMed PMID: 38214006]
Corvino S, Corrivetti F, Catapano G, Corazzelli G, Colamaria A, Maghalashvili E, Dallan I, Di Maria D, Di Matteo G, Iaconetta G, de Notaris M. The 4 F (Fat, Fascia, Fibrin, and Fat) Technique for Skull Base Reconstruction in Endoscopic Transorbital Surgery. Acta neurochirurgica. 2025 Sep 29:167(1):258. doi: 10.1007/s00701-025-06667-5. Epub 2025 Sep 29 [PubMed PMID: 41021063]
Basta MN, Rao V, Roussel LO, Crozier JW, Liu PY, Woo AS. Refining Indications for Orbital Floor Fracture Reconstruction: A Risk-Stratification Tool Predicting Symptom Development and Need for Surgery. Plastic and reconstructive surgery. 2021 Sep 1:148(3):606-615. doi: 10.1097/PRS.0000000000008292. Epub [PubMed PMID: 34432690]
Ascher B, Coleman S, Alster T, Bauer U, Burgess C, Butterwick K, Donofrio L, Engelhard P, Goldman MP, Katz P, Vleggaar D. Full scope of effect of facial lipoatrophy: a framework of disease understanding. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 2006 Aug:32(8):1058-69 [PubMed PMID: 16918569]
Level 3 (low-level) evidenceRose GE. The giant fornix syndrome: an unrecognized cause of chronic, relapsing, grossly purulent conjunctivitis. Ophthalmology. 2004 Aug:111(8):1539-45 [PubMed PMID: 15288985]
Level 3 (low-level) evidenceLiang L, Sheha H, Fu Y, Liu J, Tseng SC. Ocular surface morbidity in eyes with senile sunken upper eyelids. Ophthalmology. 2011 Dec:118(12):2487-92. doi: 10.1016/j.ophtha.2011.05.035. Epub 2011 Aug 27 [PubMed PMID: 21872934]
Level 3 (low-level) evidenceNovitskaya E, Rene C. Enophthalmos as a sign of metastatic breast carcinoma. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2013 Sep 17:185(13):1159. doi: 10.1503/cmaj.120726. Epub 2013 Mar 4 [PubMed PMID: 23460637]
Level 3 (low-level) evidenceArikan OK, Onaran Z, Muluk NB, Yilmazbaş P, Yazici I. Enophthalmos due to atelectasis of the maxillary sinus: silent sinus syndrome. The Journal of craniofacial surgery. 2009 Nov:20(6):2156-9. doi: 10.1097/SCS.0b013e3181bf0116. Epub [PubMed PMID: 19884840]
Level 3 (low-level) evidenceFeingold KR, Ahmed SF, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, de Herder WW, Dhatariya K, Dungan K, Hofland J, Kalra S, Kaltsas G, Kapoor N, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrère B, Levy M, McGee EA, McLachlan R, Muzumdar R, Purnell J, Rey R, Sahay R, Shah AS, Singer F, Sperling MA, Stratakis CA, Trence DL, Wilson DP, Akinci B, Gular MC, Oral EA. Lipodystrophy Syndromes: Presentation and Treatment. Endotext. 2000:(): [PubMed PMID: 29989768]
Frankart AJ, Breneman JC, Pater LE. Radiation Therapy in the Treatment of Head and Neck Rhabdomyosarcoma. Cancers. 2021 Jul 16:13(14):. doi: 10.3390/cancers13143567. Epub 2021 Jul 16 [PubMed PMID: 34298780]
Choi JS, Oh SY, Shim HS. Correction of post-traumatic enophthalmos with anatomical absorbable implant and iliac bone graft. Archives of craniofacial surgery. 2019 Dec:20(6):361-369. doi: 10.7181/acfs.2019.00451. Epub 2019 Dec 20 [PubMed PMID: 31914490]
Li C, Gao S, Gao W. Research progress of orbital fat in histology and cytology: A review. Medicine. 2024 Jul 26:103(30):e39040. doi: 10.1097/MD.0000000000039040. Epub [PubMed PMID: 39058805]
Canzi G, Morganti V, Novelli G, Bozzetti A, Sozzi D. Posttraumatic Delayed Enophthalmos: Analogies with Silent Sinus Syndrome? Case Report and Literature Review. Craniomaxillofacial trauma & reconstruction. 2015 Sep:8(3):251-6. doi: 10.1055/s-0034-1399799. Epub 2015 Jan 14 [PubMed PMID: 26269736]
Level 3 (low-level) evidenceFang Y, Shen B, Dai Q, Xie Q, Wu W, Wang M. Orbital inflammatory pseudotumor: new advances in diagnosis, pathogenesis, and treatment. European journal of medical research. 2023 Oct 4:28(1):395. doi: 10.1186/s40001-023-01330-0. Epub 2023 Oct 4 [PubMed PMID: 37794419]
Level 3 (low-level) evidenceTitova A, Nikolaev S, Bilyalov A, Filatov N, Brovkin S, Shestakov D, Khatkov I, Pismennaya E, Bondarev V, Antyuxina M, Shagimardanova E, Bodunova N, Gusev O. Extreme Tolerance of Extraocular Muscles to Diseases and Aging: Why and How? International journal of molecular sciences. 2024 May 3:25(9):. doi: 10.3390/ijms25094985. Epub 2024 May 3 [PubMed PMID: 38732204]
Cohen LM, Habib LA, Yoon MK. Post-traumatic enophthalmos secondary to orbital fat atrophy: a volumetric analysis. Orbit (Amsterdam, Netherlands). 2020 Oct:39(5):319-324. doi: 10.1080/01676830.2019.1691607. Epub 2019 Nov 14 [PubMed PMID: 31726012]
Ramia P, Bodgi L, Mahmoud D, Mohammad MA, Youssef B, Kopek N, Al-Shamsi H, Dagher M, Abu-Gheida I. Radiation-Induced Fibrosis in Patients with Head and Neck Cancer: A Review of Pathogenesis and Clinical Outcomes. Clinical Medicine Insights. Oncology. 2022:16():11795549211036898. doi: 10.1177/11795549211036898. Epub 2022 Jan 30 [PubMed PMID: 35125900]
Level 2 (mid-level) evidencePeckett AJ, Wright DC, Riddell MC. The effects of glucocorticoids on adipose tissue lipid metabolism. Metabolism: clinical and experimental. 2011 Nov:60(11):1500-10. doi: 10.1016/j.metabol.2011.06.012. Epub 2011 Aug 23 [PubMed PMID: 21864867]
Zheng F, Gonçalves FM, Abiko Y, Li H, Kumagai Y, Aschner M. Redox toxicology of environmental chemicals causing oxidative stress. Redox biology. 2020 Jul:34():101475. doi: 10.1016/j.redox.2020.101475. Epub 2020 Apr 18 [PubMed PMID: 32336668]
Ozturker C, Sari Y, Ozbilen KT, Ceylan NA, Tuncer S. Surgical Repair of Orbital Blow-Out Fractures: Outcomes and Complications. Beyoglu eye journal. 2022:7(3):199-206. doi: 10.14744/bej.2022.88156. Epub 2022 Aug 5 [PubMed PMID: 36185982]
Kim S, Park SH, Lee SM. Changes in Intraocular Pressure and Anterior Chamber Parameters Following Cataract Surgery, Vitrectomy, and Combined Surgery. Korean journal of ophthalmology : KJO. 2024 Feb:38(1):23-33. doi: 10.3341/kjo.2023.0072. Epub 2023 Dec 15 [PubMed PMID: 38104596]
Copeland H, Kivuva E, Firth HV, Wright CF. Systematic assessment of outcomes following a genetic diagnosis identified through a large-scale research study into developmental disorders. Genetics in medicine : official journal of the American College of Medical Genetics. 2021 Jun:23(6):1058-1064. doi: 10.1038/s41436-021-01110-3. Epub 2021 Feb 18 [PubMed PMID: 33603196]
Level 1 (high-level) evidenceSadeghi F, Shirkhoda M. Allergy-Related Diseases and Risk of Breast Cancer: The Role of Skewed Immune System on This Association. Allergy & rhinology (Providence, R.I.). 2019 Jan-Dec:10():2152656719860820. doi: 10.1177/2152656719860820. Epub 2019 Jul 22 [PubMed PMID: 31384488]
Bite U, Jackson IT, Forbes GS, Gehring DG. Orbital volume measurements in enophthalmos using three-dimensional CT imaging. Plastic and reconstructive surgery. 1985 Apr:75(4):502-8 [PubMed PMID: 3838589]
Delmas J, Loustau JM, Martin S, Bourmault L, Adenis JP, Robert PY. Comparative study of 3 exophthalmometers and computed tomographic biometry. European journal of ophthalmology. 2018 Mar:28(2):144-149. doi: 10.5301/ejo.5001049. Epub [PubMed PMID: 29108394]
Level 2 (mid-level) evidenceJeon HB, Kang DH, Oh SA, Gu JH. Comparative Study of Naugle and Hertel Exophthalmometry in Orbitozygomatic Fracture. The Journal of craniofacial surgery. 2016 Jan:27(1):142-4. doi: 10.1097/SCS.0000000000002334. Epub [PubMed PMID: 26674913]
Level 2 (mid-level) evidencePidro A, Jovanovic N, Kadribašic E, Barucija N, Leto N, Kahana A. Delayed Management of an Orbital Floor Blow-out Fracture. Beyoglu eye journal. 2021:6(3):249-253. doi: 10.14744/bej.2021.94834. Epub 2021 Sep 27 [PubMed PMID: 35005524]
Zhang Z, Zhang Y, He Y, An J, Zwahlen RA. Correlation between volume of herniated orbital contents and the amount of enophthalmos in orbital floor and wall fractures. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2012 Jan:70(1):68-73. doi: 10.1016/j.joms.2011.02.036. Epub 2011 Jun 12 [PubMed PMID: 21664740]
Level 2 (mid-level) evidenceAfanasyeva DS, Gushchina MB, Gerasimov MY, Borzenok SA. Computed exophthalmometry is an accurate and reproducible method for the measuring of eyeballs' protrusion. Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2018 Mar:46(3):461-465. doi: 10.1016/j.jcms.2017.12.024. Epub 2017 Dec 26 [PubMed PMID: 29325888]
Khatri S, Torok KS, Mirizio E, Liu C, Astakhova K. Autoantibodies in Morphea: An Update. Frontiers in immunology. 2019:10():1487. doi: 10.3389/fimmu.2019.01487. Epub 2019 Jul 9 [PubMed PMID: 31354701]
Kelsey CE, Torok KS. The Localized Scleroderma Cutaneous Assessment Tool: responsiveness to change in a pediatric clinical population. Journal of the American Academy of Dermatology. 2013 Aug:69(2):214-20. doi: 10.1016/j.jaad.2013.02.007. Epub 2013 Apr 4 [PubMed PMID: 23562760]
Level 2 (mid-level) evidenceYoung SM, Kim YD, Kim SW, Jo HB, Lang SS, Cho K, Woo KI. Conservatively Treated Orbital Blowout Fractures: Spontaneous Radiologic Improvement. Ophthalmology. 2018 Jun:125(6):938-944. doi: 10.1016/j.ophtha.2017.12.015. Epub 2018 Feb 3 [PubMed PMID: 29398084]
Boyette JR, Pemberton JD, Bonilla-Velez J. Management of orbital fractures: challenges and solutions. Clinical ophthalmology (Auckland, N.Z.). 2015:9():2127-37. doi: 10.2147/OPTH.S80463. Epub 2015 Nov 17 [PubMed PMID: 26604678]
Ramasamy A, Madhan B, Krishnan B. Comments on "A Straightforward Method of Predicting Enophthalmos in Blowout Fractures Using Enophthalmos Estimate Line". Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2017 Jun:75(6):1094. doi: 10.1016/j.joms.2017.01.045. Epub 2017 Mar 6 [PubMed PMID: 28279685]
Level 3 (low-level) evidenceMcRae M, Augustine HFM, Budning A, Antonyshyn O. Functional Outcomes of Late Posttraumatic Enophthalmos Correction. Plastic and reconstructive surgery. 2018 Aug:142(2):169e-178e. doi: 10.1097/PRS.0000000000004600. Epub [PubMed PMID: 30045183]
DeSerres JJ, Budning A, Antonyshyn OM. Current Management of Late Posttraumatic Enophthalmos. Plastic and reconstructive surgery. 2022 Oct 1:150(4):888e-902e. doi: 10.1097/PRS.0000000000009471. Epub 2022 Sep 28 [PubMed PMID: 36170440]
Raveggi E, Sobrero F, Gerbino G. Patient Specific Implants for Orbital Reconstruction in the Treatment of Silent Sinus Syndrome: Two Case Reports. Journal of personalized medicine. 2023 Mar 25:13(4):. doi: 10.3390/jpm13040578. Epub 2023 Mar 25 [PubMed PMID: 37108964]
Level 3 (low-level) evidenceMichelle L, Du AT, Abiri A, Kuan EC. Clinical manifestations, management, and outcomes of primary silent sinus syndrome: a systematic review. Rhinology. 2023 Aug 1:61(4):297-311. doi: 10.4193/Rhin23.028. Epub [PubMed PMID: 37219052]
Level 1 (high-level) evidenceHamedani M, Pournaras JA, Goldblum D. Diagnosis and management of enophthalmos. Survey of ophthalmology. 2007 Sep-Oct:52(5):457-73 [PubMed PMID: 17719369]
Level 3 (low-level) evidenceKamminga N, Jansonius NM, Pott JW, Links TP. Unilateral proptosis: the role of medical history. The British journal of ophthalmology. 2003 Mar:87(3):370-1 [PubMed PMID: 12598466]
Pattnaik A, Lim A, Sabeti S, Kwon A, Hall K, Lott I, Kimonis V. A unique case of progressive hemifacial microsomia or Parry-Romberg syndrome associated with limb and brain anomalies with normal neurological findings: A review of the literature. European journal of medical genetics. 2021 Sep:64(9):104234. doi: 10.1016/j.ejmg.2021.104234. Epub 2021 Jun 1 [PubMed PMID: 34082156]
Level 3 (low-level) evidenceStefani FH. Phthisis bulbi--an intraocular fluoride proliferative reaction. Developments in ophthalmology. 1985:10():78-160 [PubMed PMID: 3979645]
Llorente-González S, Peralta-Calvo J, Abelairas-Gómez JM. Congenital anophthalmia and microphthalmia: epidemiology and orbitofacial rehabilitation. Clinical ophthalmology (Auckland, N.Z.). 2011:5():1759-65. doi: 10.2147/OPTH.S27189. Epub 2011 Dec 13 [PubMed PMID: 22267908]
Pointer JS, Gilmartin B. Clinical characteristics of unilateral myopic anisometropia in a juvenile optometric practice population. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2004 Sep:24(5):458-63 [PubMed PMID: 15315661]
Kanagalingam S, Miller NR. Horner syndrome: clinical perspectives. Eye and brain. 2015:7():35-46. doi: 10.2147/EB.S63633. Epub 2015 Apr 10 [PubMed PMID: 28539793]
Level 3 (low-level) evidenceRokohl AC, Kopecky A, Trester M, Wawer Matos PA, Pine KR, Heindl LM. Post-enucleation socket syndrome-a novel pathophysiological definition. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2022 Aug:260(8):2427-2431. doi: 10.1007/s00417-022-05648-z. Epub 2022 Apr 2 [PubMed PMID: 35366081]
Whitehouse RW, Batterbury M, Jackson A, Noble JL. Prediction of enophthalmos by computed tomography after 'blow out' orbital fracture. The British journal of ophthalmology. 1994 Aug:78(8):618-20 [PubMed PMID: 7918289]
Sung YS, Chung CM, Hong IP. The Correlation between the Degree of Enophthalmos and the Extent of Fracture in Medial Orbital Wall Fracture Left Untreated for Over Six Months: A Retrospective Analysis of 81 Cases at a Single Institution. Archives of plastic surgery. 2013 Jul:40(4):335-40. doi: 10.5999/aps.2013.40.4.335. Epub 2013 Jul 17 [PubMed PMID: 23898428]
Level 2 (mid-level) evidenceKittichokechai P, Sirichatchai K, Puncreobutr C, Lohwongwatana B, Saonanon P. A Novel Patient-specific Titanium Mesh Implant Design for Reconstruction of Complex Orbital Fracture. Plastic and reconstructive surgery. Global open. 2022 Jan:10(1):e4081. doi: 10.1097/GOX.0000000000004081. Epub 2022 Jan 27 [PubMed PMID: 35186634]
Polacco MA, Kahng PW, Sudoko CK, Gosselin BJ. Orbital Floor Reconstruction: A Comparison of Outcomes between Absorbable and Permanent Implant Systems. Craniomaxillofacial trauma & reconstruction. 2019 Sep:12(3):193-198. doi: 10.1055/s-0038-1651514. Epub 2018 Jun 5 [PubMed PMID: 31428243]
Sivasubramaniam R, Sacks R, Thornton M. Silent sinus syndrome: dynamic changes in the position of the orbital floor after restoration of normal sinus pressure. The Journal of laryngology and otology. 2011 Dec:125(12):1239-43. doi: 10.1017/S0022215111001952. Epub 2011 Aug 11 [PubMed PMID: 21835074]
Kim J, Shin ES, Kim JE, Yoon SP, Kim YS. Neck muscle atrophy and soft-tissue fibrosis after neck dissection and postoperative radiotherapy for oral cancer. Radiation oncology journal. 2015 Dec:33(4):344-9. doi: 10.3857/roj.2015.33.4.344. Epub 2015 Dec 30 [PubMed PMID: 26756035]
Okunieff P, Augustine E, Hicks JE, Cornelison TL, Altemus RM, Naydich BG, Ding I, Huser AK, Abraham EH, Smith JJ, Coleman N, Gerber LH. Pentoxifylline in the treatment of radiation-induced fibrosis. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2004 Jun 1:22(11):2207-13 [PubMed PMID: 15169810]
Chen H, Zhang Q, Qiu Q, Yang Z. Autologous Fat Graft for the Treatment of Sighted Posttraumatic Enophthalmos and Sunken Upper Eyelid. Ophthalmic plastic and reconstructive surgery. 2018 Jul/Aug:34(4):381-386. doi: 10.1097/IOP.0000000000001028. Epub [PubMed PMID: 29369151]
Level 2 (mid-level) evidenceWufuer M, Choi TH, Najmiddinov B, Kim J, Choi J, Kim T, Park Y, Kim JH, Jeon H, Kim BJ. Improving Facial Fat Graft Survival Using Stromal Vascular Fraction-Enriched Lipotransfer: A Multicenter Randomized Controlled Study. Plastic and reconstructive surgery. 2024 Apr 1:153(4):690e-700e. doi: 10.1097/PRS.0000000000010625. Epub 2023 May 2 [PubMed PMID: 37141448]
Level 1 (high-level) evidenceLi Z, Guo X, Zhang J, Liu X, Chang R, He M. Using deep leaning models to detect ophthalmic diseases: A comparative study. Frontiers in medicine. 2023:10():1115032. doi: 10.3389/fmed.2023.1115032. Epub 2023 Mar 1 [PubMed PMID: 36936225]
Level 2 (mid-level) evidencePearl RM. Treatment of enophthalmos. Clinics in plastic surgery. 1992 Jan:19(1):99-111 [PubMed PMID: 1537231]
Issa SA, Jameel ME. Free Dermal Fat Graft for Reconstruction of Soft Tissue Defects in the Maxillofacial Region. Craniomaxillofacial trauma & reconstruction. 2020 Dec:13(4):260-266. doi: 10.1177/1943387520910678. Epub 2020 Apr 8 [PubMed PMID: 33456697]
Whitaker LA, Yaremchuk MJ. Secondary reconstruction of posttraumatic orbital deformities. Annals of plastic surgery. 1990 Dec:25(6):440-9 [PubMed PMID: 2073075]
Paris GL, Spohn WG. Correction of enophthalmos in the anophthalmic orbit. Ophthalmology. 1980 Dec:87(12):1301-8 [PubMed PMID: 7243220]
Strabbing EM, Engin O, Telleman MAJ, Nagtegaal AP, Wolvius EB. Post-traumatic and iatrogenic silent sinus syndrome: a case series. Oral and maxillofacial surgery. 2025 May 22:29(1):106. doi: 10.1007/s10006-025-01391-x. Epub 2025 May 22 [PubMed PMID: 40402305]
Level 2 (mid-level) evidenceVasavada A, Raggio BS. Autologous Fat Grafting for Facial Rejuvenation. StatPearls. 2026 Jan:(): [PubMed PMID: 32491783]
Straub JM, New J, Hamilton CD, Lominska C, Shnayder Y, Thomas SM. Radiation-induced fibrosis: mechanisms and implications for therapy. Journal of cancer research and clinical oncology. 2015 Nov:141(11):1985-94. doi: 10.1007/s00432-015-1974-6. Epub 2015 Apr 25 [PubMed PMID: 25910988]
Choi A, Sisson A, Olson K, Sivam S. Predictors of Delayed Enophthalmos After Orbital Fractures: A Systematic Review. Facial plastic surgery & aesthetic medicine. 2022 Sep-Oct:24(5):397-403. doi: 10.1089/fpsam.2021.0177. Epub 2022 Feb 17 [PubMed PMID: 35179991]
Level 1 (high-level) evidenceHazani R, Yaremchuk MJ. Correction of posttraumatic enophthalmos. Archives of plastic surgery. 2012 Jan:39(1):11-7. doi: 10.5999/aps.2012.39.1.11. Epub 2012 Jan 15 [PubMed PMID: 22783485]
Wang E, Swiekatowski K, Sobol D, Greives M, Hansen-Kiss E. The Great Escape: A Case Series on DDX3X Craniofacial Phenotypes in Females. The Cleft palate-craniofacial journal : official publication of the American Cleft Palate-Craniofacial Association. 2025 Oct 3:():10556656251383776. doi: 10.1177/10556656251383776. Epub 2025 Oct 3 [PubMed PMID: 41042938]
Level 2 (mid-level) evidenceAbu-Ghname A, Perdanasari AT, Reece EM. Principles and Applications of Fat Grafting in Plastic Surgery. Seminars in plastic surgery. 2019 Aug:33(3):147-154. doi: 10.1055/s-0039-1693438. Epub 2019 Aug 2 [PubMed PMID: 31384229]
Aravich D, Troxell L. Clinical Practice Guidelines for Occupational Therapists in the Evaluation and Treatment of Oculomotor Impairment Following Traumatic Brain Injury. Current physical medicine and rehabilitation reports. 2021:9(3):93-99. doi: 10.1007/s40141-021-00310-x. Epub 2021 Jun 2 [PubMed PMID: 34094719]
Level 1 (high-level) evidenceDe Sousa A. Psychological issues in acquired facial trauma. Indian journal of plastic surgery : official publication of the Association of Plastic Surgeons of India. 2010 Jul:43(2):200-5. doi: 10.4103/0970-0358.73452. Epub [PubMed PMID: 21217982]
Conway ML, Shah R, Chapman E, Evans BJW. The Role of Orthoptists in Refraction. The British and Irish orthoptic journal. 2025:21(1):17-35. doi: 10.22599/bioj.384. Epub 2025 Feb 14 [PubMed PMID: 39959347]
Grant MP, Iliff NT, Manson PN. Strategies for the treatment of enophthalmos. Clinics in plastic surgery. 1997 Jul:24(3):539-50 [PubMed PMID: 9246520]
Lin YY, Jiao HR, Peng YQ, Chen X, Lyu F, Liu XT. Eyelid disorders and morphologies among older individuals: a cross-sectional survey in China. International journal of ophthalmology. 2025:18(10):1958-1963. doi: 10.18240/ijo.2025.10.20. Epub 2025 Oct 18 [PubMed PMID: 40994591]
Level 2 (mid-level) evidenceBlöndal K, Sveinsdóttir H, Ingadottir B. Patients' expectations and experiences of provided surgery-related patient education: A descriptive longitudinal study. Nursing open. 2022 Sep:9(5):2495-2505. doi: 10.1002/nop2.1270. Epub 2022 Jun 5 [PubMed PMID: 35666048]
Putri BBK, Noer AH, Purba FD. Psychological Factors Influencing Appearance Anxiety Among Adolescents: A Systematic Literature Review. Psychology research and behavior management. 2025:18():487-503. doi: 10.2147/PRBM.S501547. Epub 2025 Mar 1 [PubMed PMID: 40046607]
Level 1 (high-level) evidenceWinslow E, Bohannon N, Brunton SA, Mayhew HE. Lifestyle modification: weight control, exercise, and smoking cessation. The American journal of medicine. 1996 Oct 8:101(4A):4A25S-31S; discussion 31S-33S [PubMed PMID: 8900334]
Green BN, Johnson CD. Interprofessional collaboration in research, education, and clinical practice: working together for a better future. The Journal of chiropractic education. 2015 Mar:29(1):1-10. doi: 10.7899/JCE-14-36. Epub 2015 Jan 16 [PubMed PMID: 25594446]
Dohlman JC, Yoon MK. Principles of Protection of the Eye and Vision in Orbital Surgery. Journal of neurological surgery. Part B, Skull base. 2020 Aug:81(4):381-384. doi: 10.1055/s-0040-1714077. Epub 2020 Aug 7 [PubMed PMID: 33072480]
Cline RA, Rootman J. Enophthalmos: a clinical review. Ophthalmology. 1984 Mar:91(3):229-37 [PubMed PMID: 6717910]
Ohana O, Alabiad C. Ocular Related Sports Injuries. The Journal of craniofacial surgery. 2021 Jun 1:32(4):1606-1611. doi: 10.1097/SCS.0000000000007618. Epub [PubMed PMID: 33741878]
Susarla SM, Duncan K, Mahoney NR, Merbs SL, Grant MP. Virtual Surgical Planning for Orbital Reconstruction. Middle East African journal of ophthalmology. 2015 Oct-Dec:22(4):442-6. doi: 10.4103/0974-9233.164626. Epub [PubMed PMID: 26692714]
Buljac-Samardzic M, Doekhie KD, van Wijngaarden JDH. Interventions to improve team effectiveness within health care: a systematic review of the past decade. Human resources for health. 2020 Jan 8:18(1):2. doi: 10.1186/s12960-019-0411-3. Epub 2020 Jan 8 [PubMed PMID: 31915007]
Level 1 (high-level) evidence