Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is a specialized endoscopic technique that combines endoscopy and fluoroscopy to diagnose and, more commonly, treat disorders of the biliary and pancreatic ducts. Using a side-viewing duodenoscope, the endoscopist advances the instrument into the second portion of the duodenum to access the major or minor papilla, allowing selective cannulation of the common bile duct (CBD) and/or pancreatic duct. Through these channels, contrast material is injected to delineate ductal anatomy under fluoroscopic guidance and to facilitate interventions such as sphincterotomy, stone extraction, stricture dilation, or placement of plastic or metal stents.
Originally developed as a diagnostic modality, ERCP has evolved into a primarily therapeutic procedure, as less invasive imaging methods, such as magnetic resonance cholangiopancreatography (MRCP) and endoscopic ultrasound (EUS), have replaced its diagnostic role. Despite its essential therapeutic value, ERCP carries the highest risk of significant complications among routine endoscopic procedures, including pancreatitis, bleeding, perforation, and infection. Successful performance requires advanced endoscopic training, technical expertise, and careful patient selection to balance clinical benefits against potential risks.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
A detailed understanding of the upper gastrointestinal, biliary, and pancreatic anatomy is essential for performing ERCP safely and effectively. At the start of the procedure, the duodenoscope is advanced through the esophagus, stomach, and pylorus into the second portion of the duodenum, where the major duodenal papilla and the ampulla of Vater are identified along the medial duodenal wall. In approximately 90% of individuals, the CBD and the main pancreatic duct (MPD), also known as the duct of Wirsung, merge at the level of the ampulla and major papilla, draining into the duodenum with flow regulated by the sphincter of Oddi (see Image. Biliary and Pancreatic Ducts). The ducts may unite before entering the papilla or form a common channel that diverges within the duodenal wall. Depending on the indication, radiopaque contrast is injected under low pressure into the biliary or pancreatic ductal systems to delineate ductal anatomy and identify strictures, stones, or other pathology.
Anatomic variants, such as pancreas divisum, occur in approximately 10% of the population and have significant implications for cannulation and therapy. In this variant, the MPD fails to fuse embryologically with the smaller ventral pancreatic duct (duct of Santorini). Instead, the MPD drains through the minor duodenal papilla, located approximately 2 cm proximal to the ampulla of Vater. At the same time, the ventral pancreatic duct joins the duodenal wall at the major papilla.[1] The minor papilla contains its own sphincter, known as the sphincter of Helly. Recognizing these normal and variant ductal configurations is crucial for successful ductal cannulation, appropriate therapeutic intervention, and minimizing procedural complications during ERCP.
Indications
Since the advent of MRCP, ERCP has seldom been used exclusively for diagnostic purposes. ERCP should be used as a diagnostic intervention only in patients with metal implants who cannot undergo magnetic resonance imaging due to contraindications. With ERCP, contrast material is injected into either or both of the CBD and pancreatic duct to identify the anatomy and pathology of the biliary and pancreatic ductal (PD) systems. MRCP is often performed first for these purposes, since it doesn't deliver radiation and is noninvasive; however, additional diagnostic procedures, including taking biopsies, performing brush cytology, and direct cholangiopancreatoscopy, require ERCP.[2] Intraductal biliary ultrasound may also be performed to provide high-resolution imaging of either of the ductal systems, using an ultrasound catheter in the place of a cannulating catheter. ERCP is also used to perform biliary manometry to assess for sphincter of Oddi dysfunction.
Therapeutic procedures commonly performed at ERCP include biliary or pancreatic sphincterotomy, stone removal, stricture dilatation, and biliary and/or pancreatic stent placement.[2] Nasobiliary drain placement and choledochoscopy are procedures that are less frequently performed. Therapeutic indications include:
- Evaluation of obstructive jaundice (benign or malignant) with or without cholangitis
- Gallstone pancreatitis
- Balloon or basket extraction of bile duct stones (choledocholithiasis) or, less often, pancreatic ductal stones
- Management of established benign or malignant biliary strictures
- Management of post-cholecystectomy bile leaks
- Management of biliary sump syndrome following choledochoduodenostomy
- Management of choledochal cysts
- Management of ampullary carcinoma and periampullary adenomas (endoscopic ampullectomy)
- For the performance of cholangioscopy and/or pancreatoscopy for diagnostic and therapeutic interventions
- Minimal role in the management of peripancreatic fluid collections
- Primary drainage of pancreatic pseudocysts and other collections is now mainly done with lumen-apposing metal stents (LAMS) placed with endoscopic ultrasound.[3] ERCP-placed pancreatic stents are used for PD decompression if a fluid collection is being carried into the PD, if additional drainage is needed beyond that provided by the LAMS, or if a LAMS cannot be performed.
- Type I: Typical biliary-type abdominal pain, elevated liver enzymes, and a CBD diameter of at least 12 mm are usually due to fixed papillary stenosis that responds well to biliary sphincterotomy.
- Type II: Typical biliary-type abdominal pain, and either but not both of elevated liver enzymes and a CBD diameter of at least 12 mm, probably due to primary tonic/phasic biliary dyskinesia, are present.[4]
- Evaluation (by biliary manometry) and management of Milwaukee types I and II biliary sphincter of Oddi dysfunction or papillary stenosis.
- Type III: Typical biliary-type abdominal pain, with neither elevated liver enzymes nor CBD dilatation, is rarely due to biliary dyskinesia, and biliary manometry is not recommended because the risk outweighs the potential benefit.[5]
- Primary drainage of pancreatic pseudocysts and other collections is now mainly done with lumen-apposing metal stents (LAMS) placed with endoscopic ultrasound.[3] ERCP-placed pancreatic stents are used for PD decompression if a fluid collection is being carried into the PD, if additional drainage is needed beyond that provided by the LAMS, or if a LAMS cannot be performed.
- Pancreas divisum
- The role of ERCP in patients with recurrent acute pancreatitis and pancreas divisum is controversial, as the association between the 2 conditions remains uncertain because most patients with pancreas divisum are asymptomatic. Pancreas divisum patients with a mutation predisposing to pancreatitis, such as the CFTR gene, and a dilated pancreatic duct, are at increased risk of recurrent acute pancreatitis. ERCP with minor papillotomy has been shown to have a limited benefit in patients with these risk factors; however a prospective randomized sham-controlled clinical trial to evaluate the effectiveness of ERCP and minor papillotomy, the SpHincterotomy for Acute Recurrent Pancreatitis (SHARP) trial, showed no reduction of the risk of recurrent acute pancreatitis, chronic pancreatitis, exocrine dysfunction, or any other adverse events with minor papillotomy.[6][7] No subgroup related to age or sex was found to benefit from the procedure (presented by the principal investigator at Digestive Disease Week, 2025, but final results have not yet been published).
Contraindications
ERCP is contraindicated or not indicated when there is:
- Hemodynamic instability that will not allow the patient to be sedated safely
- Recent perforation or severe stricturing of the pharynx or upper gastrointestinal tract
- Gastric outlet obstruction or a history of prior surgery that would prohibit access to the major papilla (eg, bariatric surgery, Billroth II antrectomy, Roux-en-Y anastomosis)
- A diagnostic indication that can be addressed with a safer diagnostic tool, such as MRCP
- An uncorrected coagulopathy (severe thrombocytopenia or a prolonged international normalized ratio) when a sphincterotomy needs to be performed
- ERCP can be performed in this setting; however, an alternative to sphincterotomy (eg, temporary stent placement, biliary balloon dilatation, or nasobiliary drain placement) can be used.
- When ERCP does not change the action plan [8][9][10]
- Type III sphincter of Oddi dysfunction
Equipment
A side-viewing duodenoscope is used for ERCP in patients with normal anatomy, as it allows an optimal view of the major duodenal papilla, rendering cannulation easier. In surgically altered gastrointestinal anatomy, as in patients after a Billroth II gastrectomy or Roux-en-Y surgery, the afferent loop entrance is hidden, sharply angulated, and elongated, and the papillary position is reversed. In these situations, using a side-viewing duodenoscope may be problematic, and a forward-viewing endoscope facilitates afferent loop intubation and biliary cannulation. Where available, some endoscopists use a double-balloon enteroscope to advance a forward-viewing endoscope through the afferent loop by alternately inflating and deflating the balloons. The duodenoscope features an elevator at its distal tip, which can be raised or lowered to direct the cannula, sphincterotome, balloon, or other accessory into the major or minor papilla, thereby accessing the desired duct and performing the necessary procedures (see Image. Distal Tip of Duodenoscope).
The areas around and beneath the elevator act as a reservoir for bacteria that cannot always be adequately reprocessed with current technology. Reports of serious and life-threatening infections associated with duodenoscopes have led to the design of instruments with replaceable distal tip covers and distal elevator covers, which are used during procedures and for reprocessing (see Image. Duodenoscope with Disposable Distal Cover). Single-use duodenoscopes have also been designed (see Image. Disposable Duodenoscope). While these instruments are designed to reduce or eliminate the risk of this type of infection, concerns remain about additional costs and environmental effects, particularly with single-use scopes. The latter concerns are partly due to the production of nonrecyclable waste and increased carbon dioxide emissions produced by each instrument. Carbon dioxide emissions are approximately 20 times higher with disposable duodenoscopes compared to those with reusable end caps, primarily due to the production process of these devices.[11] As these concerns are addressed over time, it is reasonable to limit their use to patients at an increased risk of infection or with a greater likelihood of morbidity and mortality should this occur. Patients at greater risk include those with:
- A presentation of cholangitis or biliary obstruction
- Cholangiocarcinoma or primary sclerosing cholangitis
- A history of solid organ transplant
- Cancer receiving immunosuppressing chemotherapy
- Other immunosuppressive conditions or those who are receiving immunosuppressive medications
- COVID-19 infection or the flu, who require ERCP
- Diabetes
- A history of methicillin-resistant Staphylococcus aureus, vancomycin-resistant enterococcus, or other multi-drug-resistant organisms [12]
Cannulation, or passage of a catheter through the papillary orifice into either the CBD or pancreatic duct, is done using either a cannula (a catheter exclusively used to access either of the ducts) or a sphincterotome (a cannula equipped with a cutting and cauterizing wire that is also utilized to make an incision in the sphincter of Oddi or either of the pancreatic sphincters). Cannulation is more likely to be successful when a sphincterotome is used. Cholangiopancreatoscopy is done with the use of a cholangioscope (also called a cholangoscope when utilized in the intrahepatic ducts) with distal diameters ranging from 3.1 to 3.5 mm, which have a depth of field of 1.5 to 20 mm, and use narrow band imaging to improve visibility of ductal lesions. Ultraslim endoscopes offer a wide range of angulation, with working lengths ranging from 65 to 110 cm and working channel diameters from 2 to 2.2 mm, enabling the passage of instruments for forceps biopsies, electrohydraulic lithotripsy, and laser lithotripsy.
The biliary tree and pancreatic duct can be visualized directly by passing a cholangioscope through the working channel of the duodenoscope, utilizing a separate light source.[13][14][15][16] These procedures are performed to evaluate and fragment biliary and pancreatic stones, as well as for intraductal cytologic brushing and for tissue biopsies of indeterminate biliary or pancreatic strictures. Tumor ablation and recovery of migrated stents can also be done with a choledochoscope.[17][18] Per-oral cholangioscopy (or pancreatoscopy) can be done by several different techniques, including:
- Mother-baby system (dual operator)
- One endoscopist controls the mother duodenoscope, and the other controls the baby cholangiopancreatoscope. The tip is deflectable only on the vertical plane. The cholangioscope is passed through the therapeutic duodenoscope's working channel over a guidewire into the biliary duct. Several manufacturers produce products of this type.
- SpyGlass technique (single operator)
- This is a catheter-based cholangiopancreatoscopy system. The optical probe is passed through a 4-lumen catheter. The catheter is passed through the working channel of the duodenoscope, and the deflectable tip of the Spyglass can be moved up, down, left, and right. (see Image. SpyGlass Cholangioscope)
- Direct per-oral cholangioscopy (DPOC)
- DPOC uses ultraslim and transnasal endoscopes with digital imaging. These endoscopes are used in dilated CBD cases, as their shaft diameters range from 4.9 to 5.9 mm. To reduce the risk of air embolism, insufflation in these situations should be done using water or carbon dioxide.
Personnel
Required personnel for the performance of ERCP include the following:
- A skilled endoscopist will perform the procedure.
- Gastrointestinal assistants (nurses or technicians) help with the passage of guidewires, deployment of stents, and management of other equipment.
- Either an anesthesiologist or a nurse anesthetist is required if deep sedation with propofol or general anesthesia needs to be administered.
- In some settings, a cytology technician is in the procedure room to prepare endoscopically obtained brushings by applying them to slides and staining them for formal cytological interpretation. The tissue obtained can be immediately assessed for adequacy and for evidence of malignancy.
Preparation
The American Society for Gastrointestinal Endoscopy (ASGE) has issued guidelines for routine laboratory testing before endoscopic procedures.[19] They recommend against routine radiographic, cardiac, or laboratory testing before endoscopy for otherwise healthy individuals, but suggest selective testing based on the patient's and procedure-specific risk factors. A pregnancy test should be performed for all women of childbearing age. Coagulation studies are also indicated in patients with a preprocedural coagulopathy or a history of bleeding. However, a prolonged prothrombin time (PT), International Normalized Ratio (INR), and partial thromboplastin time (PTT) do not predict intraprocedural or postprocedure bleeding.[20]
Patients with biliary disease or biliary obstruction often have a prolonged INR that should be treated before the ERCP if sphincterotomy is to be performed. Other testing should be ordered based on the patient's medical history. Regarding preoperative eating, it is recommended that patients have a meal with fatty foods at least 8 hours before the procedure, avoid light foods for 6 hours, and refrain from clear liquids for the last 2 hours before the procedure.[19][21]
Antibiotic prophylaxis is recommended before ERCP in patients with ascending cholangitis caused by stones and benign or malignant biliary strictures. Due to their immunocompromised state, antibiotics are also prescribed prophylactically to patients who require ERCP after having had a liver transplant. Biliary flora, including enterococci and gram-negative organisms, should be covered, and antibiotics must be continued after ERCP if biliary drainage is incomplete.
Technique or Treatment
The duodenoscope is advanced perorally through the gastric pylorus to the second part of the duodenum to visualize the major duodenal papilla. Access to the CBD and/or the MPD is achieved with either a cannula or a sphincterotome. The recommended technique begins with the passage of a guidewire under fluoroscopic guidance into the CBD or pancreatic duct before deep cannulation or contrast injection. Additional biliary interventions are done with accessories passed over the guidewire.
On the other hand, the standard contrast-assisted method involves contrast material injection after introducing the tapered tip of a cannula or sphincterotome into the major duodenal papillary orifice to ensure proper positioning. Difficult cannulation may be due to a periampullary diverticulum, an impacted biliary stone, bile duct stenosis, or a tumor of the bile duct or pancreatic head. Infrequently, cannulation of the minor papilla with sphincterotomy may be done in cases of idiopathic recurrent acute pancreatitis or in patients with pancreas divisum.
Difficult biliary cannulation does not have a single, confirmed definition; however, the European Society of Gastrointestinal Endoscopy defines it as attempts lasting more than 5 minutes, more than 5 cannulation attempts, or 2 or more unintentional pancreatic duct cannulations or opacifications.[22][23] Cannulation using standard techniques may not be possible. In that case, options include approaching the papilla with the duodenoscope in the long position, using needle-knife and other precut sphincterotomy techniques, the double-wire technique (leaving a wire in the pancreatic duct before attempting to place a second wire into the bile duct or reattempting biliary cannulation), and pancreatic stent placement before sphincterotomy. Techniques used in ERCP include biliary or pancreatic sphincterotomy, endoscopic papillary balloon dilation, balloon or basket stone removal, tissue sampling, placement of biliary and pancreatic stents, cholangiopancreatoscopy, biliary and pancreatic drainage, endoscopic ampullectomy, and sphincter of Oddi manometry.
Common findings at ERCP:
- If bile duct stones are found, a sphincterotomy or balloon dilatation of the sphincter of Oddi is followed by the extraction of the stone(s) with either an air-filled balloon or a wire basket. Stones are generally released into the duodenum and pass harmlessly through the gastrointestinal tract.
- If one or more strictures are found, they may be brushed for cytology or biopsied. The stricture(s) may be dilated using a hydrostatic balloon, and then one or more plastic or metallic self-expanding stents are placed to keep them open. Further management of the strictures depends on their histology, diameter, and elasticity and is beyond the scope of this activity.
- If a mass lesion is found within a duct, it is brushed or biopsied; if it is causing a stricture, a stent can be placed.
- A bile leak may be found in the evaluation of abdominal pain after a cholecystectomy. Common practice is to place a 7-French or 10-French plastic stent into the CBD without a sphincterotomy to eliminate the pressure gradient across the papilla and provide a path of least resistance for bile to drain into the duodenum rather than through the leak. The stent does not need to extend proximal to the leak. After 4 to 6 weeks, the stent is removed by upper endoscopy. No further intervention is generally necessary. If retained bile duct stones are found with a leak, a sphincterotomy is performed to facilitate stone extraction using standard techniques. A stent is then placed to manage the leak.[24] Very minimal leaks can often be managed with a small sphincterotomy and do not necessarily require the placement of a stent.[25]
- Primary sclerosing cholangitis: Dominant strictures, defined as a stenosis of ≤1.5 mm in the CBD and ≤1 mm in the hepatic ducts within 2 cm of the hepatic bifurcation, can be managed endoscopically.[26]
- Ampullary adenoma: Resection of benign adenomas of the papilla that do not show ingrowth of adenomatous tissue 1 cm or more into the CBD or the pancreatic duct is potentially resectable by endoscopic ampullectomy (an extension of ERCP). Patients who are poor surgical candidates who have localized ampullary malignancy or adenoma ingrowth of 1 cm or more into the CBD should also be considered for this procedure.[27] Technical details, complications, and follow-up are beyond the scope of this activity.
Complications
ERCP is the highest-risk regularly performed procedure in gastroenterology.[28] The most common complications are acute post-ERCP pancreatitis (PEP), bleeding, infection, and perforation (see Table. Adverse Events Related to ERCP).[29] More severe complications require endoscopic or surgical intervention, blood transfusion of more than 4 units, or prolonged hospitalization (greater than 10 days). Gastrointestinal bleeding and perforation are primarily related to sphincterotomy. Although perforation is rare, it carries the highest mortality rate among ERCP complications.
Other issues account for 1.3% of total complications. These include cardiovascular and analgesia-related events, such as those in patients with pacemakers and implantable cardioverter-defibrillators, as well as pneumothorax, hepatic hematoma, portal venous air embolism, splenic injury, post-sphincterotomy papillary or ampullary restenosis, duodenal obstruction, stent migration, and impaction of the basket catheter during the removal of biliary stones.
Table. Adverse Events Related to ERCP
| Adverse event | Incidence |
| Acute pancreatitis at first ERCP | 6.5% |
| Acute pancreatitis at subsequent ERCP | 4.6% |
| Bleeding | 1.5% |
| Duodenoscope-related infection | 0.01% [30] |
| Cholangitis | 2.5% |
| Cholecystitis | 0.4% overall, or 1.3% to 1.5% after metallic biliary stent placement [31] |
| Upper gastrointestinal (luminal) or biliary perforation | 0.5% [32] |
| Death | 0.2% |
PEP
PEP is the most commonly encountered complication of ERCP. Despite identifying risk factors and establishing guidelines to reduce its incidence, the incidence of PEP hasn't changed between 2000 and 2023.[29] In 90% of cases, pancreatitis is mild-to-moderate in severity, and early recognition provides the best opportunity to minimize morbidity and mortality.
Diagnosis: The Cotton consensus and the revised Atlanta classification criteria are used to diagnose PEP:
- Cotton consensus criteria
- Pancreatitis-like abdominal pain, elevated pancreatic enzyme levels of lipase or amylase to greater than 3 times the upper limit of normal on the day following ERCP, and an unplanned hospital stay of at least 2 nights.[33]
- Revised Atlanta classification criteria
- Pancreatitis-like abdominal pain, elevated pancreatic enzyme levels of lipase or amylase to greater than 3 times the upper limit of normal on the day following ERCP, and imaging consistent with acute pancreatitis.[34]
Risk factors include patient selection for ERCP, procedure-related issues, and a higher risk associated with less experienced endoscopists and at centers where the procedure is performed less frequently.
- Patient selection
- PEP is more common in younger patients, in females, in people with suspected or confirmed sphincter of Oddi dysfunction, and in people with a history of PEP.
- Procedure-related risk factors
- Difficulty with cannulation [35]
- Delayed decision to perform a precut sphincterotomy
- Balloon dilation of an intact sphincter of Oddi of <1 minute's duration in the absence of a prior biliary sphincterotomy
- Any pancreatic ductal intervention, including wire passage(s) into the pancreatic duct
- Less likely risk factors: intraductal ultrasound and failure to remove bile duct stones
With recognition of risk factors for PEP, measures should be taken to reduce the risk of this complication [36]. These include:
- Use of endoscopic ultrasound or MRCP instead of ERCP unless there is a high likelihood that a therapeutic intervention (sphincterotomy, balloon or basket stone extraction, or stent placement) will need to be performed.
- Referral of patients to tertiary care centers if the risk is high and greater experience is needed.
- Rectal nonsteroidal anti-inflammatory drug (NSAID) administration decreases the incidence of PEP; thus, an indomethacin or diclofenac 100 mg suppository is given immediately before, during, or promptly after the procedure. An NSAID suppository is recommended in all patients except for those in whom the risk of PEP is negligible, such as those with chronic calcific pancreatitis who have had uncomplicated ERCPs in the past or who have had a biliary sphincterotomy and require biliary endotherapy for retained stones, strictures, or bile leaks.
- Aggressive hydration using lactated Ringer solution. This hydration can be achieved with a preprocedural bolus of 1 liter or more in healthy but high-risk individuals. A high-flow infusion should be maintained during and after the procedure. Aggressive hydration is recommended for all patients in the United States who can tolerate it. Still, in Europe, it is limited to those in whom a pancreatic stent hasn't been placed and when rectal NSAIDs cannot be administered.[37][38]
- A pancreatic stent can be placed prophylactically before biliary intervention in patients at an increased risk of PEP. Pancreatic stent placement in conjunction with rectal indomethacin was found to be more effective than indomethacin alone, however in light of the potential risk of pancreatitis due to placement of the stent as well as its cost and requirement of follow-up, its use more recently has been limited to higher risk individuals in whom placement of the stent is not difficult (for example, in cases in which a wire was inadvertently passed into the pancreatic duct during an attempt at biliary cannulation).[39] When a prophylactic stent is placed, a plain abdominal x-ray should be taken 7 to 10 days after placement of a pancreatic stent, and retained stents should be removed endoscopically within 10 days of placement if they haven't passed out of the body spontaneously.
- Coagulopathic individuals with choledocholithiasis have the lowest risk of PEP if a biliary stent is placed and sphincterotomy is delayed until the coagulopathy is corrected. The alternative option is to perform balloon dilatation, which should be maintained for 2 to 5 minutes to reduce PEP.[40]
- Minimizing the number of cannulation attempts and the volume of contrast material injected. The wire-guided technique is recommended for cannulation, rather than attempting to cannulate either duct with the cannula or sphincterotome too deeply. The wire-guided technique has been demonstrated to reduce the risk of PEP by about 50%, and can usually be facilitated by minimal contrast injection when necessary.[41]
- The double-wire technique is used if there is difficulty accessing the CBD and repeated wire passage into the pancreatic duct. This technique leaves a wire in the pancreatic duct to straighten the ductal anatomy, facilitating access to the CBD with a second wire. After the CBD has been accessed, the pancreatic duct wire can be removed unless a pancreatic intervention, such as pancreatic duct stent placement, is planned.
- If a precut sphincterotomy is needed, needle-knife fistulotomy is recommended over other techniques, as it carries fewer complications, including PEP. Alternative maneuvers when cannulation cannot be done easily include biliary cannulation adjacent to a pancreatic stent, placement of a pancreatic duct wire, followed by attempted wire advancement into the bile duct, and pancreatic septotomy.
- Biliary manometry is performed to evaluate the Sphincter of Oddi using a modified triple-lumen perfusion catheter with immediate aspiration or a non-water-perfused micro transducer catheter to reduce the risk of PEP.
Bleeding
This is usually due to sphincterotomy, and bleeding is usually from a vessel at the crest of the sphincterotomy. Risk factors for post-sphincterotomy bleeding include the following:
- Thrombocytopenia (platelet count less than 50,000/µL)
- Use of anticoagulants and direct antiplatelet agents (eg, clopidogrel or prasugrel)
- Cirrhosis (although a prolonged INR in cirrhosis may reflect hypercoagulability rather than a bleeding disorder)
- Chronic renal failure requiring hemodialysis
- Ascending cholangitis
- Periampullary diverticula
Nonsphincterotomy causes of bleeding:
- Hemobilia after intraductal interventions such as biopsies or balloon dilation
- Intraductal photodynamic therapy
- Intraductal radiofrequency ablation
Prevention of bleeding:
- Withhold antiplatelet drugs and anticoagulants before ERCP, with duration differing related to the specific drug, and ideally for 2 to 3 days after ERCP. Aspirin and other NSAIDs can be continued as they do not increase the risk of intraprocedural bleeding.[42]
- If anticoagulation cannot be held or reversed in the setting of ascending cholangitis in the presence of a coagulopathy, there are several options:
- A stent or a nasobiliary drain placed through an intact papilla can temporarily relieve the obstruction and infection. Once the coagulation factors have been normalized, a sphincterotomy and other necessary interventions can be carried out later.
- A small sphincterotomy can be made, then tamponaded with a fully covered metallic stent.
- To further reduce the risk of pancreatitis, balloon dilatation for at least 2 minutes or longer may be necessary.
Control of bleeding:
- Endoscopic application of cauterization at the crest of the sphincterotomy
- Placement of a hemostatic clip, with caution to avoid the pancreatic duct
- Application of polysaccharide hemostatic powder or newer hemostatic gels [43][44]
- Placement of a fully covered metallic stent, trying to avoid obstructing the cystic duct take-off, if other measures are ineffective
- Angiographic embolization of the vessel if all endoscopic measures fail to achieve hemostasis
Infection
Bacterial contamination of duodenoscopes, due to inadequate cleaning in and around the elevator, is caused by the inability to sterilize the instruments during reprocessing. Bacterial biofilm can accumulate beneath and at the elevator channel, and infection outbreaks with MDROs on duodenoscopes have become a problem since 2012. Outbreaks of carbapenem-resistant Enterobacteriaceae (CRE) appeared in the early 2010s.[45] Another outbreak occurred in 2014 in the United States, the Netherlands, and India, with extended-spectrum beta-lactamase-producing Klebsiella pneumoniae.[46] An outbreak of New Delhi metallo-ß-lactamase-producing carbapenem-resistant Escherichia coli occurred in the United States, which only abated after reprocessing was changed from disinfection with ortho-phthalaldehyde to ethylene oxide gas sterilization.[47] An improved reprocessing technique, involving forced-air drying of duodenoscopes, may help reduce such infections.[48] The rate of infections may be reduced with:
- Modified duodenoscopes that can be sterilized
- Readily replaceable channels on reusable scopes
- Availability of disposable duodenoscopes [49][50]
Single-use duodenoscopes may be suitable only for lower-complexity procedures; they are not yet comparable in quality to reusable instruments and significantly increase preprocedure costs.[50] Various newer scopes designed to reduce the risk of infectious disease transmission have been developed and are currently being tested.[49][51] Post-ERCP ascending cholangitis is typically caused by inadequate clearance of ductal obstruction during ERCP or as a consequence of papillary edema following sphincterotomy or complicated stone extraction. Endoscopic accessories and contrast media can carry organisms into the biliary and pancreatic trees, potentially causing infection with inadequate drainage. In this setting, cholangitis can be caused by complicated strictures, such as those resulting from hilar tumors that are challenging to stent, primary sclerosing cholangitis with multiple strictures that can retain contrast, or incompletely cleared choledocholithiasis. Cholangitis may also occur after cholangioscopy, particularly if biopsies are taken and when bacteremia is documented after the procedure.[52] Measures to reduce the risk of cholangitis include the following:
- Attempt to drain the biliary tree entirely during ERCP. Stents or a nasobiliary drain should be placed into undrained ducts that contain contrast until complete drainage can be achieved. If stenting is not possible, percutaneous biliary drainage can be performed.
- Antibiotic prophylaxis is often prescribed when there is concern that complete biliary drainage may be difficult or impossible, as it reduces the risk of bacteremia. However, this has not been proven to reduce the risk of cholangitis, pancreatitis, septicemia, or mortality.[53]
Post-ERCP acute cholecystitis most commonly occurs after placement of uncovered or covered metallic biliary stents that occlude the cystic duct, with the incidence being slightly higher with covered stents; however, a stricture or a retained stone can also be responsible.[44] Symptoms of cholecystitis appear at a median of 5 days after ERCP. If the cystic duct is occluded, antibiotics should be given, and options for gallbladder decompression include:
- Replacement of a metallic stent with 1 or more plastic stents
- Endoscopic transpapillary gallbladder stent placement
- Transmural drainage with EUS guidance
- Percutaneous cholecystostomy drainage
- Cholecystectomy, if indicated
Perforation
Perforations during ERCP can be related to foregut (esophageal, gastric, and proximal duodenal) strictures that prevent the duodenoscope from easily reaching the post-bulbar duodenum, or to steps taken during and after accessing the bile and pancreatic ducts. The latter have been classified into 4 Stapfer types:
- Type I: Duodenal wall free perforation (or jejunal wall perforation after Billroth II gastrectomy)
- Type II: Retroperitoneal duodenal perforation due to periampullary injury; these are the most common and can often be managed endoscopically without requiring surgery [54]
- Type III: Perforation of either the pancreatic duct or the bile duct
- Type IV: Retroperitoneal air without other signs of perforation [55]
Foregut (luminal) full-thickness perforations are rare. Still, morbidity and mortality are high, particularly when perforation is not immediately recognized or cannot be immediately repaired during a procedure at a nonhospital site. Esophageal perforations, for example, have a 13% mortality rate in such settings, as a consequence of infection.[32] Luminal perforations are typically associated with strictures or surgically altered anatomy. Passage of the duodenoscope into the duodenum must be done cautiously to avoid causing perforation in one of those circumstances. A forward-viewing gastroscope is prudent if the anatomy must be clarified before duodenoscopy. If it is available, carbon dioxide should be used for insufflation of the gastrointestinal tract during endoscopy to reduce the risk of perforation. Biliary or pancreatic stents infrequently may penetrate the duodenal wall, which may be asymptomatic or cause stent occlusion.
Sometimes luminal perforations can be closed primarily with endoscopically placed sutures or clips.[32] However, if the lumen is too narrow for the duodenoscope to pass, there will likely be too little room for a primary closure. In those cases, a fully covered esophageal stent can seal the rent if it can be positioned and secured above the major duodenal papilla. If that is not possible due to the type of perforation, if the patient becomes clinically unstable, if the perforation is too large, or if endoscopic expertise is not available to perform a primary closure, surgery may be necessary. In fact, surgery is necessary to repair most esophageal perforations and open gastric or duodenal perforations. When surgery is delayed because of failure of nonoperative therapy, there is greater morbidity and mortality, and hospitalizations are prolonged.[56]
Biliary or pancreatic stents infrequently may penetrate the duodenal wall, which may be asymptomatic or cause stent occlusion. Perforation by a previously placed stent can often be managed by removing the stent. However, antibiotics should be administered, and clip closure should be performed if there is evidence of infection, as indicated by the presence of gas or fluid around the penetrated site. In all cases of luminal perforation, surgical consultation should be considered even if endoscopic closure can be performed successfully during the procedure.
In cases of periampullary or retroperitoneal perforations related to cannulation and additional biliary and pancreatic interventions, sphincterotomy is the intervention that most greatly increases the risk of such perforations, and more so if it is being extended, redone, associated with a sphincteroplasty, or if it is associated with Sphincter of Oddi dysfunction.[57] Difficult cannulations or balloon dilatation of the bile or pancreatic duct also increase the risk of perforation. Guidewires may pass through the duodenal wall, which is recognized by retroperitoneal air. The risk of perforation is minimized by recognition of the anatomical landmarks at the papilla and by choosing a stricture-dilating balloon with a diameter that is not in excess of the size of the duct proximal to it.[57] Management of pancreatic and biliary perforations includes:
- Antibiotic administration should be initiated when a perforation is recognized or suspected.
- The location and extent of the perforation should be confirmed by oral contrast-enhanced computed tomography.
- Perforations due to sphincterotomy or biliary/pancreatic duct leaks are best managed with a fully covered metallic stent, providing the least resistance path through the stent.
- Surgery is indicated if endoscopic management is ineffective or if peritonitis and systemic inflammatory response syndrome (SIRS) are present.
- Guidewire perforation through the duodenal wall is usually clinically inconsequential and rarely requires intervention.
Some perforations cannot be identified immediately or develop gradually after the ERCP, and peritonitis may occur. Such delayed perforations are most frequently due to electrocautery applied during sphincterotomy or sphincteroplasty, and symptoms develop over several days after the procedure. They are typically contained, but may result in peritonitis and SIRS.[58] Delayed luminal perforations without signs of significant morbidity may be managed endoscopically. Still, infection and a systemic inflammatory response necessitate surgery for abdominal washout and external drainage after the defect is closed.[59]
Clinical Significance
ERCP holds major clinical significance as both a diagnostic and, more importantly, a therapeutic intervention for disorders of the biliary and pancreatic systems. The procedure provides direct access to the major duodenal papilla; this enables selective cannulation of the common bile duct or pancreatic duct, allowing for real-time fluoroscopic imaging and interventions such as stone extraction, stent placement, sphincterotomy, and dilation of strictures. ERCP plays a central role in managing choledocholithiasis, malignant or benign biliary strictures, cholangitis, pancreatic ductal obstructions, bile leaks, and certain cases of chronic pancreatitis.
The shift from a primarily diagnostic tool to a predominantly therapeutic procedure underscores its importance in reducing the need for more invasive surgical interventions. By relieving obstructions, restoring ductal patency, and enabling tissue sampling, ERCP directly improves quality of life, prevents recurrent infections, and reduces morbidity and mortality associated with biliary and pancreatic disease. However, ERCP is also the highest-risk endoscopic procedure, with post-ERCP pancreatitis, hemorrhage, perforation, and infection as notable complications. Thus, its clinical significance lies in its therapeutic potential and the demand for high operator expertise, careful patient selection, and multidisciplinary perioperative care. The outcomes for most patients are generally good, and in some cases, life-saving.[14][60][61]
Enhancing Healthcare Team Outcomes
Successful performance of ERCP requires a combination of technical skill, strategic planning, and seamless team coordination. Clinicians must demonstrate advanced endoscopic expertise, precise fluoroscopic interpretation, and the ability to anticipate and manage complications such as post-ERCP pancreatitis, bleeding, or perforation. Advanced clinicians and nurses play a crucial role in patient preparation, sedation monitoring, and postprocedural care, ensuring the early recognition of complications and providing effective patient education on recovery and follow-up. Pharmacists contribute by guiding optimal antibiotic prophylaxis, managing anticoagulation and antiplatelet therapy, and supporting the appropriate use of medication to minimize procedural risks.
Interprofessional communication and structured care coordination are crucial for optimizing patient-centered outcomes in ERCP. Preprocedural planning involves collaboration among the endoscopist, anesthesiologist, nursing staff, and radiology technicians to align on patient-specific risks and procedural strategies. Intraoperatively, real-time communication facilitates the safe navigation of complex anatomy and enables a timely response to complications. Postprocedurally, coordination with primary care clinicians, surgeons, oncologists, or hepatologists ensures continuity of care, particularly in patients requiring long-term stent management or further surgical intervention. This integrated, multidisciplinary approach enhances patient safety, maximizes therapeutic benefit, and strengthens team performance in managing complex biliopancreatic disorders.
Media
(Click Image to Enlarge)
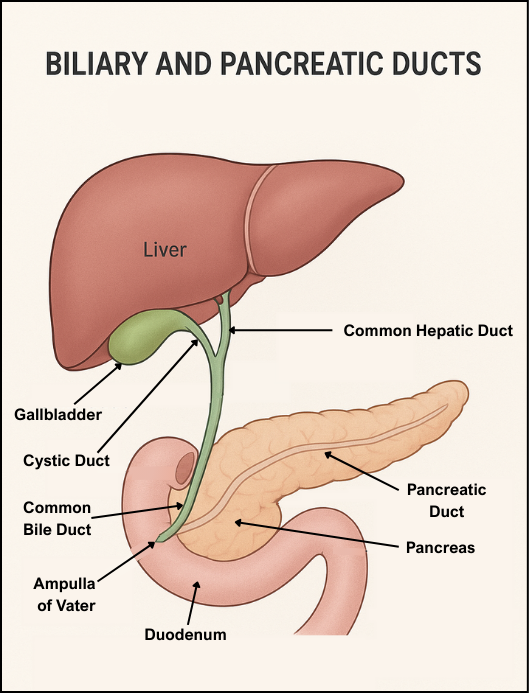
Biliary and Pancreatic Ducts. This image shows the anatomy of the biliary and pancreatic ducts.
Adapted from an image generated by ChatGPT.
(Click Image to Enlarge)
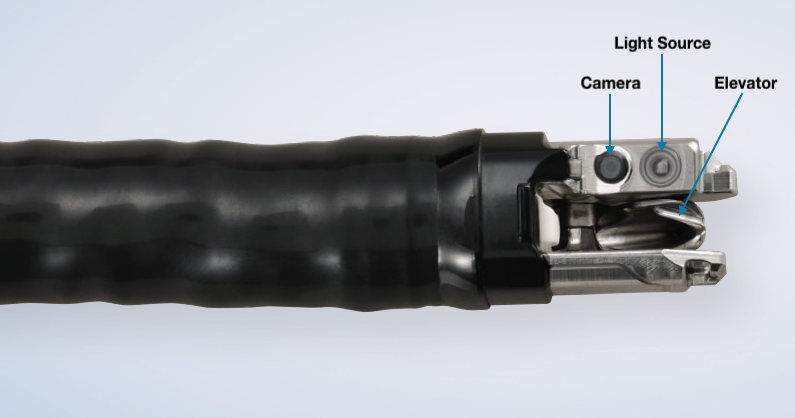
Distal Tip of Duodenoscope. This is an Olympus TJF-Q190V. Pentax Corporation and Fujifilm Corporation have similar endoscopes.
Olympus Corporation of the Americas
(Click Image to Enlarge)
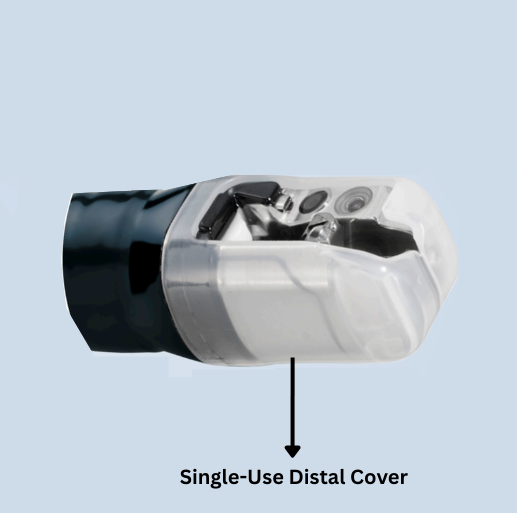
Duodenoscope With Disposable Distal Cover. This image shows the disposable distal cover on the tip of the Olympus TJF-Q190V duodenoscope. The Fujifilm Corporation has a similar product, and the Pentax Corporation incorporates the elevator into a disposable cap.
Olympus Corporation of the Americas
(Click Image to Enlarge)

Disposable Duodenoscope. This image is a Boston Scientific Exalt Model D3 disposable duodenoscope. Ambu Inc. has a comparable product called the Scope Duodeno 2.
Boston Scientific Corporation
(Click Image to Enlarge)

SpyGlass Cholangioscope. This is an image of the Boston Scientific SpyGlass cholangioscope.
Boston Scientific Corporation
References
Gutta A, Fogel E, Sherman S. Identification and management of pancreas divisum. Expert review of gastroenterology & hepatology. 2019 Nov:13(11):1089-1105. doi: 10.1080/17474124.2019.1685871. Epub 2019 Nov 8 [PubMed PMID: 31663403]
ASGE Standards of Practice Committee, Buxbaum JL, Abbas Fehmi SM, Sultan S, Fishman DS, Qumseya BJ, Cortessis VK, Schilperoort H, Kysh L, Matsuoka L, Yachimski P, Agrawal D, Gurudu SR, Jamil LH, Jue TL, Khashab MA, Law JK, Lee JK, Naveed M, Sawhney MS, Thosani N, Yang J, Wani SB. ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis. Gastrointestinal endoscopy. 2019 Jun:89(6):1075-1105.e15. doi: 10.1016/j.gie.2018.10.001. Epub 2019 Apr 9 [PubMed PMID: 30979521]
Bhakta D, de Latour R, Khanna L. Management of pancreatic fluid collections. Translational gastroenterology and hepatology. 2022:7():17. doi: 10.21037/tgh-2020-06. Epub 2022 Apr 25 [PubMed PMID: 35548474]
Hogan WJ, Geenen JE. Biliary dyskinesia. Endoscopy. 1988 Aug:20 Suppl 1():179-83 [PubMed PMID: 3168947]
Cotton PB, Durkalski V, Romagnuolo J, Pauls Q, Fogel E, Tarnasky P, Aliperti G, Freeman M, Kozarek R, Jamidar P, Wilcox M, Serrano J, Brawman-Mintzer O, Elta G, Mauldin P, Thornhill A, Hawes R, Wood-Williams A, Orrell K, Drossman D, Robuck P. Effect of endoscopic sphincterotomy for suspected sphincter of Oddi dysfunction on pain-related disability following cholecystectomy: the EPISOD randomized clinical trial. JAMA. 2014 May:311(20):2101-9. doi: 10.1001/jama.2014.5220. Epub [PubMed PMID: 24867013]
Level 1 (high-level) evidenceKanth R, Samji NS, Inaganti A, Komanapalli SD, Rivera R, Antillon MR, Roy PK. Endotherapy in symptomatic pancreas divisum: a systematic review. Pancreatology : official journal of the International Association of Pancreatology (IAP) ... [et al.]. 2014 Jul-Aug:14(4):244-50. doi: 10.1016/j.pan.2014.05.796. Epub 2014 Jun 11 [PubMed PMID: 25062871]
Level 1 (high-level) evidenceCoté GA, Durkalski-Mauldin VL, Serrano J, Klintworth E, Williams AW, Cruz-Monserrate Z, Arain M, Buxbaum JL, Conwell DL, Fogel EL, Freeman ML, Gardner TB, van Geenen E, Groce JR, Jonnalagadda SS, Keswani RN, Menon S, Moffatt DC, Papachristou GI, Ross A, Tarnasky PR, Wang AY, Wilcox CM, Hamilton F, Yadav D, SHARP Consortium. SpHincterotomy for Acute Recurrent Pancreatitis Randomized Trial: Rationale, Methodology, and Potential Implications. Pancreas. 2019 Sep:48(8):1061-1067. doi: 10.1097/MPA.0000000000001370. Epub [PubMed PMID: 31404020]
Level 1 (high-level) evidenceSalerno R, Mezzina N, Ardizzone S. Endoscopic retrograde cholangiopancreatography, lights and shadows: Handle with care. World journal of gastrointestinal endoscopy. 2019 Mar 16:11(3):219-230. doi: 10.4253/wjge.v11.i3.219. Epub [PubMed PMID: 30918587]
Shih HY, Hsu WH, Kuo CH. Postendoscopic retrograde cholangiopancreatography pancreatitis. The Kaohsiung journal of medical sciences. 2019 Apr:35(4):195-201. doi: 10.1002/kjm2.12040. Epub 2019 Mar 19 [PubMed PMID: 30887733]
Abbarh S, Seleem M, Al Balkhi A, Al Mtawa A, Al Khathlan A, Qutub A, Al Sayari K, Al Otaibi N, AlEid A, Al Ghamdi A, Al Lehibi A. ERCP quality indicators: The experience of a high-volume tertiary care center in Saudi Arabia. Arab journal of gastroenterology : the official publication of the Pan-Arab Association of Gastroenterology. 2019 Mar:20(1):32-37. doi: 10.1016/j.ajg.2019.01.005. Epub 2019 Mar 11 [PubMed PMID: 30872134]
Level 2 (mid-level) evidenceLee T, Enslin S, Kaul V. Single-Use Duodenoscopes for ERCP: Rationale, Feasibility, Cost, and Environmental Impact. Gastroenterology & hepatology. 2022 May:18(5):248-291 [PubMed PMID: 36397752]
Level 2 (mid-level) evidencePeter S, Bang JY, Varadarajulu S. Single-use duodenoscopes: where are we and where are we going? Current opinion in gastroenterology. 2021 Sep 1:37(5):416-420. doi: 10.1097/MOG.0000000000000755. Epub [PubMed PMID: 34010243]
Level 3 (low-level) evidenceDavis J, Sreevastava DK, Dwivedi D, Gadgi S, Sud S, Dudeja P. A Comparison of Stress Response between Insertion of Gastro-laryngeal Tube and Endotracheal Intubation in Patients Undergoing Upper Gastrointestinal Endoscopic Procedures for Endoscopic Retrograde Cholangiopancreatography. Anesthesia, essays and researches. 2019 Jan-Mar:13(1):13-18. doi: 10.4103/aer.AER_9_19. Epub [PubMed PMID: 31031473]
Halász A, Pécsi D, Farkas N, Izbéki F, Gajdán L, Fejes R, Hamvas J, Takács T, Szepes Z, Czakó L, Vincze Á, Gódi S, Szentesi A, Párniczky A, Illés D, Kui B, Varjú P, Márta K, Varga M, Novák J, Szepes A, Bod B, Ihász M, Hegyi P, Hritz I, Erőss B, Hungarian Pancreatic Study Group. Outcomes and timing of endoscopic retrograde cholangiopancreatography for acute biliary pancreatitis. Digestive and liver disease : official journal of the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver. 2019 Sep:51(9):1281-1286. doi: 10.1016/j.dld.2019.03.018. Epub 2019 Apr 25 [PubMed PMID: 31031177]
Tso DK, Almeida RR, Prabhakar AM, Singh AK, Raja AS, Flores EJ. Accuracy and timeliness of an abbreviated emergency department MRCP protocol for choledocholithiasis. Emergency radiology. 2019 Aug:26(4):427-432. doi: 10.1007/s10140-019-01689-w. Epub 2019 Apr 27 [PubMed PMID: 31030393]
Kim JY, Lee HS, Chung MJ, Park JY, Park SW, Song SY, Bang S. Bleeding Complications and Clinical Safety of Endoscopic Retrograde Cholangiopancreatography in Patients with Liver Cirrhosis. Yonsei medical journal. 2019 May:60(5):440-445. doi: 10.3349/ymj.2019.60.5.440. Epub [PubMed PMID: 31016905]
Lee T, Teng TZJ, Shelat VG. Choledochoscopy: An update. World journal of gastrointestinal endoscopy. 2021 Dec 16:13(12):571-592. doi: 10.4253/wjge.v13.i12.571. Epub [PubMed PMID: 35070020]
Navaneethan U, Hasan MK, Lourdusamy V, Njei B, Varadarajulu S, Hawes RH. Single-operator cholangioscopy and targeted biopsies in the diagnosis of indeterminate biliary strictures: a systematic review. Gastrointestinal endoscopy. 2015 Oct:82(4):608-14.e2. doi: 10.1016/j.gie.2015.04.030. Epub 2015 Jun 10 [PubMed PMID: 26071061]
Level 1 (high-level) evidenceASGE Standards of Practice Committee, Pasha SF, Acosta R, Chandrasekhara V, Chathadi KV, Eloubeidi MA, Fanelli R, Faulx AL, Fonkalsrud L, Khashab MA, Lightdale JR, Muthusamy VR, Saltzman JR, Shaukat A, Wang A, Cash B. Routine laboratory testing before endoscopic procedures. Gastrointestinal endoscopy. 2014 Jul:80(1):28-33. doi: 10.1016/j.gie.2014.01.019. Epub 2014 May 15 [PubMed PMID: 24836749]
Segal JB, Dzik WH, Transfusion Medicine/Hemostasis Clinical Trials Network. Paucity of studies to support that abnormal coagulation test results predict bleeding in the setting of invasive procedures: an evidence-based review. Transfusion. 2005 Sep:45(9):1413-25 [PubMed PMID: 16131373]
Kang SH, Hyun JJ. Preparation and patient evaluation for safe gastrointestinal endoscopy. Clinical endoscopy. 2013 May:46(3):212-8. doi: 10.5946/ce.2013.46.3.212. Epub 2013 May 31 [PubMed PMID: 23767028]
Berry R, Han JY, Tabibian JH. Difficult biliary cannulation: Historical perspective, practical updates, and guide for the endoscopist. World journal of gastrointestinal endoscopy. 2019 Jan 16:11(1):5-21. doi: 10.4253/wjge.v11.i1.5. Epub [PubMed PMID: 30705728]
Level 3 (low-level) evidenceTestoni PA, Mariani A, Aabakken L, Arvanitakis M, Bories E, Costamagna G, Devière J, Dinis-Ribeiro M, Dumonceau JM, Giovannini M, Gyokeres T, Hafner M, Halttunen J, Hassan C, Lopes L, Papanikolaou IS, Tham TC, Tringali A, van Hooft J, Williams EJ. Papillary cannulation and sphincterotomy techniques at ERCP: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2016 Jul:48(7):657-83. doi: 10.1055/s-0042-108641. Epub 2016 Jun 14 [PubMed PMID: 27299638]
Gawlik C, Carneval M. A Review of the Management of Bile Leaks. Cureus. 2021 May 10:13(5):e14937. doi: 10.7759/cureus.14937. Epub 2021 May 10 [PubMed PMID: 34123634]
Sandha GS, Bourke MJ, Haber GB, Kortan PP. Endoscopic therapy for bile leak based on a new classification: results in 207 patients. Gastrointestinal endoscopy. 2004 Oct:60(4):567-74 [PubMed PMID: 15472680]
Barkin JA, Levy C, Souto EO. Endoscopic Management of Primary Sclerosing Cholangitis. Annals of hepatology. 2017 November-December,:16(6):842-850. doi: 10.5604/01.3001.0010.5274. Epub [PubMed PMID: 29055922]
Fritzsche JA, Fockens P, Barthet M, Bruno MJ, Carr-Locke DL, Costamagna G, Coté GA, Deprez PH, Giovannini M, Haber GB, Hawes RH, Hyun JJ, Itoi T, Iwasaki E, Kylänpaä L, Neuhaus H, Park JY, Reddy DN, Sakai A, Bourke MJ, Voermans RP. Expert consensus on endoscopic papillectomy using a Delphi process. Gastrointestinal endoscopy. 2021 Oct:94(4):760-773.e18. doi: 10.1016/j.gie.2021.04.009. Epub 2021 Apr 19 [PubMed PMID: 33887269]
Level 3 (low-level) evidenceBarakat M, Saumoy M, Forbes N, Elmunzer BJ. Complications of Endoscopic Retrograde Cholangiopancreatography. Gastroenterology. 2025 Aug:169(2):230-243.e8. doi: 10.1053/j.gastro.2025.03.009. Epub 2025 Mar 20 [PubMed PMID: 40120770]
Bishay K, Meng ZW, Khan R, Gupta M, Ruan Y, Vaska M, Iannuzzi J, O'Sullivan DE, Mah B, Partridge ACR, Henderson AM, Guo H, Samnani S, DeMarco M, Yuan Y, Elmunzer BJ, Keswani RN, Wani S, Smith ZL, Bridges RJ, Heitman SJ, Hilsden RJ, Brenner DR, Leontiadis GI, Forbes N. Adverse Events Associated With Endoscopic Retrograde Cholangiopancreatography: Systematic Review and Meta-Analysis. Gastroenterology. 2025 Mar:168(3):568-586. doi: 10.1053/j.gastro.2024.10.033. Epub 2024 Nov 7 [PubMed PMID: 39515394]
Level 1 (high-level) evidenceKwakman JA, Erler NS, Vos MC, Bruno MJ. Risk evaluation of duodenoscope-associated infections in the Netherlands calls for a heightened awareness of device-related infections: a systematic review. Endoscopy. 2022 Feb:54(2):148-155. doi: 10.1055/a-1467-6294. Epub 2021 Apr 29 [PubMed PMID: 33915575]
Level 1 (high-level) evidenceKhan R, Osman H, Lee S, Chen YI, Singh A, Hookey L, Arya N, Causada Calo N, Grover SC, Tepox-Padrón A, Bass S, Cole M, Lei Y, Li S, Mohamed R, Turbide C, Koury HF, Chau M, Howarth M, Cartwright S, Heitman SJ, Forbes N. Post-ERCP cholecystitis: Incidence, characteristics, and outcomes from a prospective multicenter biliary endoscopy registry. Gastrointestinal endoscopy. 2024 Apr:99(4):633-640. doi: 10.1016/j.gie.2023.12.010. Epub 2023 Dec 11 [PubMed PMID: 38092126]
Biancari F, D'Andrea V, Paone R, Di Marco C, Savino G, Koivukangas V, Saarnio J, Lucenteforte E. Current treatment and outcome of esophageal perforations in adults: systematic review and meta-analysis of 75 studies. World journal of surgery. 2013 May:37(5):1051-9. doi: 10.1007/s00268-013-1951-7. Epub [PubMed PMID: 23440483]
Level 1 (high-level) evidenceCotton PB, Lehman G, Vennes J, Geenen JE, Russell RC, Meyers WC, Liguory C, Nickl N. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointestinal endoscopy. 1991 May-Jun:37(3):383-93 [PubMed PMID: 2070995]
Level 3 (low-level) evidenceBanks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, Tsiotos GG, Vege SS, Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013 Jan:62(1):102-11. doi: 10.1136/gutjnl-2012-302779. Epub 2012 Oct 25 [PubMed PMID: 23100216]
Level 3 (low-level) evidenceHan S, Zhang J, Durkalski-Mauldin V, Foster LD, Serrano J, Coté GA, Bang JY, Varadarajulu S, Singh VK, Khashab M, Kwon RS, Scheiman JM, Willingham FF, Keilin SA, Groce JR, Lee PJ, Krishna SG, Chak A, Slivka A, Mullady D, Kushnir V, Buxbaum J, Keswani R, Gardner TB, Wani S, Edmundowicz SA, Shah RJ, Forbes N, Rastogi A, Ross A, Law J, Yachimski P, Chen YI, Barkun A, Smith ZL, Petersen BT, Wang AY, Saltzman JR, Spitzer RL, Spino C, Elmunzer BJ, Papachristou GI, SVI Study Group. Impact of difficult biliary cannulation on post-ERCP pancreatitis: secondary analysis of the stent versus indomethacin trial dataset. Gastrointestinal endoscopy. 2025 Mar:101(3):617-628. doi: 10.1016/j.gie.2024.10.003. Epub 2024 Oct 9 [PubMed PMID: 39389431]
Buxbaum JL, Freeman M, Amateau SK, Chalhoub JM, Coelho-Prabhu N, Desai M, Elhanafi SE, Forbes N, Fujii-Lau LL, Kohli DR, Kwon RS, Machicado JD, Marya NB, Pawa S, Ruan WH, Sheth SG, Thiruvengadam NR, Thosani NC, Qumseya BJ, (ASGE Standards of Practice Committee Chair). American Society for Gastrointestinal Endoscopy guideline on post-ERCP pancreatitis prevention strategies: summary and recommendations. Gastrointestinal endoscopy. 2023 Feb:97(2):153-162. doi: 10.1016/j.gie.2022.10.005. Epub 2022 Dec 12 [PubMed PMID: 36517310]
Wang RC, Jiang ZK, Xie YK, Chen JS. Aggressive hydration compared to standard hydration with lactated ringer's solution for prevention of post endoscopic retrograde cholangiopancreatography pancreatitis. Surgical endoscopy. 2021 Mar:35(3):1126-1137. doi: 10.1007/s00464-020-07477-9. Epub 2020 Mar 5 [PubMed PMID: 32140860]
Dumonceau JM, Kapral C, Aabakken L, Papanikolaou IS, Tringali A, Vanbiervliet G, Beyna T, Dinis-Ribeiro M, Hritz I, Mariani A, Paspatis G, Radaelli F, Lakhtakia S, Veitch AM, van Hooft JE. ERCP-related adverse events: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2020 Feb:52(2):127-149. doi: 10.1055/a-1075-4080. Epub 2019 Dec 20 [PubMed PMID: 31863440]
Elmunzer BJ, Foster LD, Serrano J, Coté GA, Edmundowicz SA, Wani S, Shah R, Bang JY, Varadarajulu S, Singh VK, Khashab M, Kwon RS, Scheiman JM, Willingham FF, Keilin SA, Papachristou GI, Chak A, Slivka A, Mullady D, Kushnir V, Buxbaum J, Keswani R, Gardner TB, Forbes N, Rastogi A, Ross A, Law J, Yachimski P, Chen YI, Barkun A, Smith ZL, Petersen B, Wang AY, Saltzman JR, Spitzer RL, Ordiah C, Spino C, Durkalski-Mauldin V, SVI Study Group. Indomethacin with or without prophylactic pancreatic stent placement to prevent pancreatitis after ERCP: a randomised non-inferiority trial. Lancet (London, England). 2024 Feb 3:403(10425):450-458. doi: 10.1016/S0140-6736(23)02356-5. Epub 2024 Jan 11 [PubMed PMID: 38219767]
Level 1 (high-level) evidenceLiao WC, Tu YK, Wu MS, Wang HP, Lin JT, Leung JW, Chien KL. Balloon dilation with adequate duration is safer than sphincterotomy for extracting bile duct stones: a systematic review and meta-analyses. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2012 Oct:10(10):1101-9. doi: 10.1016/j.cgh.2012.05.017. Epub 2012 May 27 [PubMed PMID: 22642953]
Level 1 (high-level) evidenceTse F, Liu J, Yuan Y, Moayyedi P, Leontiadis GI. Guidewire-assisted cannulation of the common bile duct for the prevention of post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis. The Cochrane database of systematic reviews. 2022 Mar 29:3(3):CD009662. doi: 10.1002/14651858.CD009662.pub3. Epub 2022 Mar 29 [PubMed PMID: 35349163]
Level 1 (high-level) evidenceAbraham NS, Barkun AN, Sauer BG, Douketis J, Laine L, Noseworthy PA, Telford JJ, Leontiadis GI. American College of Gastroenterology-Canadian Association of Gastroenterology Clinical Practice Guideline: Management of Anticoagulants and Antiplatelets During Acute Gastrointestinal Bleeding and the Periendoscopic Period. The American journal of gastroenterology. 2022 Apr 1:117(4):542-558. doi: 10.14309/ajg.0000000000001627. Epub [PubMed PMID: 35297395]
Level 1 (high-level) evidenceCosta MS, Silva A, Santos L, Almeida N, Gomes D, Figueiredo P. Delayed post-sphincterotomy bleeding: hemostatic powder is a safe and effective option. Revista espanola de enfermedades digestivas. 2024 Oct:116(10):582-583. doi: 10.17235/reed.2024.10161/2023. Epub [PubMed PMID: 38205710]
Ishida Y, Tsuchiya N, Koga T, Kitaguchi T, Matsumoto K, Kuno N, Funakoshi S, Ishibashi H, Ashizuka S, Hirai F. A novel self-assembling peptide hemostatic gel as an option for initial hemostasis in endoscopic sphincterotomy-related hemorrhage: a case series. Clinical journal of gastroenterology. 2022 Dec:15(6):1210-1215. doi: 10.1007/s12328-022-01702-9. Epub 2022 Sep 19 [PubMed PMID: 36121586]
Level 2 (mid-level) evidenceHa J, Son BK. Current Issues in Duodenoscope-Associated Infections: Now Is the Time to Take Action. Clinical endoscopy. 2015 Sep:48(5):361-3. doi: 10.5946/ce.2015.48.5.361. Epub 2015 Sep 30 [PubMed PMID: 26473116]
van der Ploeg K, Severin JA, Klaassen CHW, Vos MC, Bruno MJ, Mason-Slingerland BCGC. Contaminated duodenoscopes in ERCP: sensitivity of detection and risk of underdetection. Gastrointestinal endoscopy. 2025 Jan:101(1):141-148. doi: 10.1016/j.gie.2024.08.004. Epub 2024 Aug 9 [PubMed PMID: 39128530]
Epstein L, Hunter JC, Arwady MA, Tsai V, Stein L, Gribogiannis M, Frias M, Guh AY, Laufer AS, Black S, Pacilli M, Moulton-Meissner H, Rasheed JK, Avillan JJ, Kitchel B, Limbago BM, MacCannell D, Lonsway D, Noble-Wang J, Conway J, Conover C, Vernon M, Kallen AJ. New Delhi metallo-β-lactamase-producing carbapenem-resistant Escherichia coli associated with exposure to duodenoscopes. JAMA. 2014 Oct 8:312(14):1447-55. doi: 10.1001/jama.2014.12720. Epub [PubMed PMID: 25291580]
Thaker AM, Muthusamy VR, Sedarat A, Watson RR, Kochman ML, Ross AS, Kim S. Duodenoscope reprocessing practice patterns in U.S. endoscopy centers: a survey study. Gastrointestinal endoscopy. 2018 Aug:88(2):316-322.e2. doi: 10.1016/j.gie.2018.04.2340. Epub 2018 Apr 21 [PubMed PMID: 29684387]
Level 3 (low-level) evidencevan der Ploeg K, Haanappel CP, Voor In 't Holt AF, de Groot W, Bulkmans AJC, Erler NS, Mason-Slingerland BCGC, Severin JA, Vos MC, Bruno MJ. Unveiling 8 years of duodenoscope contamination: insights from a retrospective analysis in a large tertiary care hospital. Gut. 2024 Mar 7:73(4):613-621. doi: 10.1136/gutjnl-2023-330355. Epub 2024 Mar 7 [PubMed PMID: 38182137]
Level 2 (mid-level) evidenceBang JY, Hawes R, Varadarajulu S. Equivalent performance of single-use and reusable duodenoscopes in a randomised trial. Gut. 2021 May:70(5):838-844. doi: 10.1136/gutjnl-2020-321836. Epub 2020 Sep 7 [PubMed PMID: 32895332]
Level 1 (high-level) evidenceBruno MJ, Beyna T, Carr-Locke D, Chahal P, Costamagna G, Devereaux B, Giovannini M, Goenka MK, Khor C, Lau J, May G, Muthusamy VR, Patel S, Petersen BT, Pleskow DK, Raijman I, Reddy DN, Repici A, Ross AS, Sejpal DV, Sherman S, Siddiqui UD, Ziady C, Peetermans JA, Rousseau MJ, Slivka A, EXALT Single-use Duodenoscope Study Group. Global prospective case series of ERCPs using a single-use duodenoscope. Endoscopy. 2023 Dec:55(12):1103-1114. doi: 10.1055/a-2131-7180. Epub 2023 Jul 18 [PubMed PMID: 37463599]
Level 2 (mid-level) evidenceOthman MO, Guerrero R, Elhanafi S, Davis B, Hernandez J, Houle J, Mallawaarachchi I, Dwivedi AK, Zuckerman MJ. A prospective study of the risk of bacteremia in directed cholangioscopic examination of the common bile duct. Gastrointestinal endoscopy. 2016 Jan:83(1):151-7. doi: 10.1016/j.gie.2015.05.018. Epub 2015 Jun 23 [PubMed PMID: 26116469]
Merchan MFS, de Moura DTH, de Oliveira GHP, Proença IM, do Monte Junior ES, Ide E, Moll C, Sánchez-Luna SA, Bernardo WM, de Moura EGH. Antibiotic prophylaxis to prevent complications in endoscopic retrograde cholangiopancreatography: A systematic review and meta-analysis of randomized controlled trials. World journal of gastrointestinal endoscopy. 2022 Nov 16:14(11):718-730. doi: 10.4253/wjge.v14.i11.718. Epub [PubMed PMID: 36438881]
Level 1 (high-level) evidenceKumbhari V, Sinha A, Reddy A, Afghani E, Cotsalas D, Patel YA, Storm AC, Khashab MA, Kalloo AN, Singh VK. Algorithm for the management of ERCP-related perforations. Gastrointestinal endoscopy. 2016 May:83(5):934-43. doi: 10.1016/j.gie.2015.09.039. Epub 2015 Oct 9 [PubMed PMID: 26439541]
Stapfer M, Selby RR, Stain SC, Katkhouda N, Parekh D, Jabbour N, Garry D. Management of duodenal perforation after endoscopic retrograde cholangiopancreatography and sphincterotomy. Annals of surgery. 2000 Aug:232(2):191-8 [PubMed PMID: 10903596]
Level 2 (mid-level) evidencePatil NS, Solanki N, Mishra PK, Sharma BC, Saluja SS. ERCP-related perforation: an analysis of operative outcomes in a large series over 12 years. Surgical endoscopy. 2020 Jan:34(1):77-87. doi: 10.1007/s00464-019-06733-x. Epub 2019 Mar 11 [PubMed PMID: 30859489]
ASGE Standards of Practice Committee, Chandrasekhara V, Khashab MA, Muthusamy VR, Acosta RD, Agrawal D, Bruining DH, Eloubeidi MA, Fanelli RD, Faulx AL, Gurudu SR, Kothari S, Lightdale JR, Qumseya BJ, Shaukat A, Wang A, Wani SB, Yang J, DeWitt JM. Adverse events associated with ERCP. Gastrointestinal endoscopy. 2017 Jan:85(1):32-47. doi: 10.1016/j.gie.2016.06.051. Epub 2016 Aug 18 [PubMed PMID: 27546389]
Forbes N, Elmunzer BJ, Keswani RN, Hilsden RJ, Hall M, Anderson JT, Arvanitakis M, Chen YI, Duloy A, Elta GH, Maranki JL, Mergener K, Petersen BT, Sethi A, Siersema PD, Smith ZL, Telford JJ, Tse F, Cotton PB, Wani S. Consensus-based development of a causal attribution system for post-ERCP adverse events. Gut. 2022 Jul 11:():. pii: gutjnl-2022-328059. doi: 10.1136/gutjnl-2022-328059. Epub 2022 Jul 11 [PubMed PMID: 35817552]
Level 3 (low-level) evidencePaspatis GA, Arvanitakis M, Dumonceau JM, Barthet M, Saunders B, Turino SY, Dhillon A, Fragaki M, Gonzalez JM, Repici A, van Wanrooij RLJ, van Hooft JE. Diagnosis and management of iatrogenic endoscopic perforations: European Society of Gastrointestinal Endoscopy (ESGE) Position Statement - Update 2020. Endoscopy. 2020 Sep:52(9):792-810. doi: 10.1055/a-1222-3191. Epub 2020 Aug 11 [PubMed PMID: 32781470]
Saito H, Koga T, Sakaguchi M, Kadono Y, Kamikawa K, Urata A, Imamura H, Tada S, Kakuma T, Matsushita I. Safety and Efficacy of Endoscopic Removal of Common Bile Duct Stones in Elderly Patients ≥90 Years of Age. Internal medicine (Tokyo, Japan). 2019 Aug 1:58(15):2125-2132. doi: 10.2169/internalmedicine.2546-18. Epub 2019 Apr 17 [PubMed PMID: 30996182]
Chen Y, Jiang Y, Qian W, Yu Q, Dong Y, Zhu H, Liu F, Du Y, Wang D, Li Z. Endoscopic transpapillary drainage in disconnected pancreatic duct syndrome after acute pancreatitis and trauma: long-term outcomes in 31 patients. BMC gastroenterology. 2019 Apr 16:19(1):54. doi: 10.1186/s12876-019-0977-1. Epub 2019 Apr 16 [PubMed PMID: 30991953]
Level 2 (mid-level) evidence