Introduction
Bacterial endophthalmitis represents one of the most vision-threatening emergencies in ophthalmology and is characterized by an acute purulent inflammation of the intraocular cavities, primarily involving the aqueous humor, vitreous body, and adjacent intraocular tissues. The condition is a fulminant infection that can cause profound, irreversible vision loss within hours to days if not promptly recognized and treated. The disease process involves microbial proliferation within the closed ocular environment, leading to an intense inflammatory cascade, breakdown of the blood–ocular barriers, and subsequent structural damage to retinal and choroidal tissues. Unlike sterile postoperative inflammation or immune-mediated uveitis, bacterial endophthalmitis is characterized by the presence of replicating bacteria within the eye. Viral and parasitic intraocular infections are generally classified as uveitis, whereas fungal infections are categorized separately as fungal endophthalmitis, due to differences in pathophysiology and inflammatory mechanisms.[1][2]
Anatomically, the eye is normally protected from infection by several defense mechanisms, including an intact corneal epithelium, conjunctival immune surveillance, tear-film antimicrobial components, and the blood–aqueous and blood–retinal barriers. These barriers maintain ocular immune privilege by limiting infiltration of systemic immune cells. However, when microorganisms enter the intraocular space, the globe's confined architecture paradoxically facilitates rapid microbial replication.
The vitreous cavity, in particular, provides a relatively avascular and immunologically protected environment, allowing bacteria to multiply with minimal early immune containment. Once bacterial proliferation reaches a critical threshold, pathogen-associated molecular patterns (PAMPs) trigger a robust inflammatory response mediated by cytokines, complement activation, and neutrophilic infiltration. This inflammatory cascade contributes substantially to tissue destruction, often exceeding the direct damage caused by the microorganisms themselves.[3]
Bacterial endophthalmitis is broadly classified into exogenous and endogenous forms based on the route of pathogen entry.[4] Exogenous endophthalmitis, the more common subtype, results from direct inoculation of microorganisms into the eye. This breach may occur following intraocular surgery, penetrating trauma, or intravitreal injections.
Postoperative endophthalmitis, particularly after cataract surgery, remains the most common presentation worldwide. Despite advances in aseptic technique and perioperative prophylaxis, a small but significant risk persists due to contamination from ocular surface flora or surgical instruments. The most commonly implicated organisms in postoperative cases include coagulase-negative Staphylococcus species, Staphylococcus aureus, and Streptococcus species, with gram-negative organisms accounting for a smaller proportion but often associated with more aggressive clinical courses.[5]
Traumatic endophthalmitis typically follows open globe injuries, particularly when contaminated with soil or organic matter. In such cases, highly virulent organisms, such as Bacillus cereus, may be involved, leading to rapid clinical deterioration and a poor visual prognosis. Bleb-related endophthalmitis is another important exogenous subtype observed in patients with filtering blebs following glaucoma surgery. Thin, avascular blebs predispose to late-onset infection, often caused by Streptococcus species or Haemophilus influenzae, and are associated with severe inflammatory responses.[6]
In recent decades, the epidemiology of exogenous endophthalmitis has evolved with the widespread use of intravitreal injections for retinal diseases. Following the United States Food and Drug Administration approval of anti-vascular endothelial growth factor agents for neovascular age-related macular degeneration in 2004, the frequency of intravitreal injections increased exponentially. Consequently, some tertiary centers now report post-injection endophthalmitis cases that approach or exceed postoperative cases.[7] Although the absolute risk per injection remains low, the sheer volume of procedures has altered the epidemiological landscape. Organisms implicated in post-injection endophthalmitis frequently include Streptococcus species, which are thought to originate from oral flora, underscoring the importance of mask usage and strict aseptic protocols during injections.[6]
Endogenous bacterial endophthalmitis, in contrast, results from hematogenous dissemination of pathogens during episodes of bacteremia. This subtype is less common but often associated with systemic comorbidities such as diabetes mellitus, immunosuppression, indwelling catheters, intravenous drug use, malignancy, or infective endocarditis. Pathogens seed the highly vascular choroid before breaching the blood–retinal barrier and spreading into the vitreous cavity. Gram-positive cocci remain common etiologic agents, though in certain geographic regions, gram-negative organisms, including Klebsiella pneumoniae, may predominate and are associated with hepatic abscesses. Endogenous cases frequently present bilaterally and may initially manifest with subtle ocular symptoms overshadowed by systemic illness.[8]
The natural history of untreated bacterial endophthalmitis is characterized by rapid progression. Initial symptoms typically include ocular pain, decreased vision, redness, photophobia, and floaters. On examination, clinicians may observe conjunctival injection, corneal edema, anterior chamber cells and flare, hypopyon, vitritis, and reduced fundus visibility. As inflammation intensifies, retinal necrosis, vascular occlusion, and panophthalmitis may ensue. Without timely intervention, permanent visual impairment, phthisis bulbi, or even loss of the eye may occur. Importantly, visual outcomes correlate strongly with the virulence of the infecting organism, the initial visual acuity at presentation, and the rapidity of therapeutic intervention.[9] When diagnosed and treated promptly with appropriate intravitreal antibiotics, visual outcomes may be preserved.[10]
The pattern of intraocular spread typically begins in the posterior segment, particularly in exogenous cases in which organisms are introduced into the anterior chamber during surgery and then migrate posteriorly. In endogenous disease, choroidal seeding precedes vitreous involvement. The inflammatory response leads to breakdown of ocular barriers, increased vascular permeability, and exudation of inflammatory cells into the vitreous cavity. The resulting vitreous opacification impairs visualization and may serve as a reservoir for continued bacterial replication. In severe cases, inflammation extends beyond the globe, resulting in orbital cellulitis or panophthalmitis.[11]
Early recognition and prompt administration of intravitreal broad-spectrum antibiotics remain the cornerstone of management. The time-sensitive nature of bacterial endophthalmitis cannot be overstated; visual prognosis deteriorates rapidly with treatment delay. Advances in microbiological diagnostics, including polymerase chain reaction techniques, have improved pathogen identification rates, while evolving surgical strategies (eg, early pars plana vitrectomy in selected cases) may enhance visual outcomes.[12]
In summary, bacterial endophthalmitis is a fulminant intraocular infection with potentially devastating consequences. This condition's pathogenesis reflects the interplay between microbial virulence and host inflammatory response within the anatomically confined ocular environment. Understanding the anatomical barriers, routes of infection, natural history, and patterns of intraocular spread is essential for early diagnosis and effective intervention. Given the expanding use of intraocular procedures and intravitreal therapies worldwide, vigilance among clinicians remains paramount to preserve vision and prevent irreversible ocular morbidity.[13]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Bacteria are not present in the vitreous or aqueous humor of a healthy eye, but seeding into the eye can occur from an exogenous or endogenous source (see Table 1). The most common cause of bacterial endophthalmitis is exogenous seeding from the exterior ocular surface during penetrating ocular trauma, surgery, or intraocular injections. Although rare, bacterial endophthalmitis can also result from hematogenous spread from infections elsewhere in the body or intravenous drug use (see Image. Etiologic Classification of Bacterial Endophthalmitis).[14]
Risk Factors
Specific risk factors have been associated with preoperative, intraoperative, and postoperative stages:
Preoperative
- Blepharitis or lid abnormalities [15]
- Application of 2% xylocaine gel before povidone-iodine [16]
- Diabetes mellitus [17]
- Advanced age
- Immunocompromised status [18]
Intraoperative
- Poor sterile technique [19]
- Posterior capsular rupture
- Vitreous loss and wound leak
- Use of intracameral miotics/staining dyes and epinephrine
- Contamination during the mixing of compounded medications
Postoperative
- Postoperative wound leak
- Nonsilicon intraocular lens type
The second most common cause of endophthalmitis is post-intravitreal injection, with coagulase-negative staphylococci and streptococci as the primary pathogens. Penetrating eye trauma is the third most common cause and constitutes anywhere from 2% to 15% of all cases of endophthalmitis.[20] Coagulase-negative staphylococci predominate in this category, but other bacteria, such as Bacillus, gram-negative bacilli, and fungi, can cause infection.
Bleb-related endophthalmitis is the fourth most common cause, with bacterial etiology in descending order of S pneumoniae, enterococci, and Haemophilus influenzae. The fifth most common cause of endophthalmitis-keratitis is corneal penetration by infectious organisms. However, 50% of keratitis-related cases are due to fungi, with S aureus, streptococci, and Pseudomonas causing a minority of these infections. Endogenous blood-borne endophthalmitis is the rarest cause, with Klebsiella pneumoniae being the most common pathogen, followed by Candida, Streptococcus, S aureus, and E coli.[10][21]
In postoperative endophthalmitis, most cases (48%–70%) are caused by coagulase-negative staphylococci. Gram-positive bacteria, including S aureus and streptococcal and enterococcal species, have been identified as causative agents in such instances. In the context of ocular trauma, the incidence of endophthalmitis is notably higher, with reported rates between 3% and 17%.[22] The incidence of endophthalmitis following ocular trauma has shifted from coagulase-negative staphylococci to other staphylococcal species and to Bacillus cereus. Notably, B cereus is 10 times more prevalent in post-traumatic endophthalmitis than in post-surgical cases.[23]
Endogenous endophthalmitis, also called metastatic endophthalmitis, emerges from the spread of infectious organisms to the eye from other sites within the body. Although less common than its postoperative or post-traumatic counterparts, accounting for only 2% to 8% of all endophthalmitis cases, endogenous endophthalmitis presents a significant risk of bilateral infection, occurring in 15% to 25% of such cases.
Fungal pathogens cause approximately half of all endogenous endophthalmitis cases, with Candida albicans the primary fungal pathogen, accounting for 75% to 80% of fungal cases. On the other hand, gram-negative bacteria are associated with 32% to 37% of endogenous endophthalmitis cases. Infections caused by gram-negative organisms are concerning due to their association with poor outcomes and their difficulty in treating.[24]
Table 1. Etiologies of Bacterial Endophthalmitis
|
Category |
Subtype/Risk Factor |
Common Causative Organisms |
Key Clinical Notes |
|
Exogenous endophthalmitis |
Post-cataract surgery (acute) |
Coagulase-negative Staphylococcus (most common), Staphylococcus aureus, Streptococcus spp, gram-negative bacilli |
Usually presents within 2 to 7 days postoperatively; variable severity depending on virulence |
|
Post-cataract surgery (chronic/delayed) |
Cutibacterium acnes (formerly Propionibacterium acnes), coagulase-negative staphylococci |
Insidious onset; recurrent inflammation; often associated with capsular plaque |
|
|
Post-intravitreal injection |
Streptococcus spp (eg, oral flora), coagulase-negative Staphylococcus |
Often more aggressive; associated with droplet contamination; mask use critical |
|
|
Post-vitrectomy/other intraocular surgery |
Similar to postoperative spectrum |
Risk increases with wound leak or suture-related issues |
|
|
Post-traumatic (open globe injury) |
Bacillus cereus (highly virulent), Staphylococcus spp, Streptococcus spp, gram-negative bacilli |
Rapid progression; worse prognosis; soil contamination increases Bacillus risk |
|
|
Bleb-related (after glaucoma filtering surgery) |
Streptococcus spp, Haemophilus influenzae, Staphylococcus aureus |
Can occur months to years later; thin avascular blebs predispose |
|
|
Keratitis-associated |
Same organism as the corneal ulcer (eg, Pseudomonas, Streptococcus) |
Secondary spread from severe corneal infection |
|
|
Endogenous endophthalmitis |
Bacteremia/septicemia |
Staphylococcus aureus, Streptococcus spp, Enterococcus spp |
Often unilateral but may be bilateral; systemic source present |
|
Intravenous drug use |
Staphylococcus aureus, gram-negative organisms |
Associated with endocarditis |
|
|
Liver abscess (especially in Asia) |
Klebsiella pneumoniae |
Frequently bilateral; aggressive course |
|
|
Indwelling catheters/Patients in intensive care unit |
Gram-negative bacilli, Enterococcus |
Seen in hospitalized or immunocompromised patients |
|
|
Immunocompromised state (diabetes, malignancy) |
Mixed gram-positive and negative organisms |
Higher risk and worse outcomes |
Cataract surgery is the single most important cause of bacterial endophthalmitis. Approximately 40% to 80% of endophthalmitis cases are caused by cataract surgery; of these cases, 70% are caused by coagulase-negative staphylococci, 10% by Staphylococcus aureus, and 9% by streptococci (see Table 2).
Table 2. Classification of Bacterial Endophthalmitis by Microbial Type
|
Microbial Category |
Examples |
Clinical Implication |
|
Gram-positive cocci |
Coagulase-negative Staphylococcus, S aureus, Streptococcus spp |
Most common overall cause |
|
Gram-negative bacilli |
Pseudomonas, Klebsiella, Enterobacter |
Often more severe inflammation |
|
Highly virulent organisms |
Bacillus cereus, Streptococcus spp |
Rapid vision loss; poor prognosis |
Epidemiology
Cataract surgery and intravitreal injections are the leading causes of endophthalmitis. However, endophthalmitis remains a relatively rare complication in the modern antibiotic era. Among patients undergoing cataract surgery, approximately 0.05% to 0.2% develop postoperative endophthalmitis, with most contemporary large database studies reporting rates closer to 0.03% to 0.1% in centers that use intracameral antibiotics.
Traumatic penetrating eye injury can result in bacterial endophthalmitis in 1% to 18% of patients, depending on the extent of globe disruption, contamination with organic matter, presence of intraocular foreign bodies, and delay in primary wound repair. Hematogenous bacterial endophthalmitis is the rarest form, with reported incidence rates ranging from 0.04% to 0.4%, and is commonly associated with intravenous drug use, diabetes mellitus, immunosuppression, malignancy, prolonged hospitalization, indwelling catheters, or systemic infections requiring intravenous antibiotic therapy.[11] Systemic infections involving the liver, lungs, heart, brain, or urinary tract are the most common.
Epidemiologic trends have evolved alongside changes in ophthalmic practice patterns. In the 1990s, infection rates following cataract surgery were estimated at approximately 0.1% (1 in 1000 surgeries). During the early 2000s, some reports documented a transient increase to approximately 0.2% (1 in 500 surgeries), possibly related to clear corneal incision techniques and increased surgical volume. However, results from more recent studies suggest that rates stabilize or decline with the widespread adoption of intracameral antibiotic prophylaxis. Despite its rarity, cataract surgery remains the largest contributor to the absolute number of postoperative endophthalmitis cases, given the sheer number of procedures performed worldwide.[13]
Globally, postoperative endophthalmitis accounts for approximately 40% to 80% of cases in developed nations, whereas post-traumatic endophthalmitis contributes 2% to 15% in many Western countries. In contrast, post-traumatic cases represent a significantly larger proportion in certain developing regions, ranging from 40% to 60% of all reported endophthalmitis cases, particularly in parts of Egypt, India, and China. This geographic variation reflects differences in occupational hazards, agricultural exposure, access to immediate surgical repair, and variations in healthcare infrastructure.[25]
The epidemiology of endophthalmitis has also shifted due to the exponential increase in intravitreal injections for retinal diseases, including neovascular age-related macular degeneration, diabetic macular edema, and retinal vein occlusion. The per-injection risk of endophthalmitis is low, generally estimated at 0.02% to 0.05%, but the cumulative procedural volume has led to a measurable rise in post-injection cases in tertiary referral centers. In some institutions, post-injection endophthalmitis now rivals or exceeds the number of post-cataract surgery cases. Streptococcal species appear more common in post-injection cases than in postoperative cataract cases, potentially due to contamination from oral flora.[26]
Age distribution varies by etiology. Postoperative endophthalmitis predominantly affects older individuals, reflecting the age demographic undergoing cataract surgery and intravitreal injections. The mean age in postoperative series typically ranges from 65 to 80.
Conversely, post-traumatic endophthalmitis is more common in younger populations, particularly men in the second to fifth decades of life, due to occupational exposure, agricultural injuries, and higher rates of mechanical trauma. Pediatric traumatic endophthalmitis is also reported, particularly in rural settings, where delayed presentation and limited access to care contribute to higher complication rates.[27]
Sex distribution similarly reflects underlying risk exposure. Postoperative endophthalmitis generally demonstrates no significant sex predilection, as cataract surgery is performed across both sexes with comparable frequency in aging populations. However, post-traumatic endophthalmitis shows a marked predominance, often accounting for 70% to 90% of cases in trauma-related series. This bias in men is attributed to occupational and environmental risk factors. Endogenous endophthalmitis does not demonstrate a consistent sex predilection but is more frequent in patients with systemic comorbidities, including diabetes mellitus and intravenous drug use, conditions that may have variable demographic patterns across regions.[3]
Microbiological epidemiology also demonstrates regional variability. In North America and Europe, gram-positive organisms, particularly coagulase-negative Staphylococcus species, remain the most common pathogens in postoperative cases. Streptococcus species and gram-negative bacilli are associated with more severe clinical presentations and worse visual outcomes. In East Asia, particularly in Taiwan and parts of China, Klebsiella pneumoniae is a leading cause of endogenous endophthalmitis, often associated with pyogenic liver abscess. In agricultural regions worldwide, Bacillus cereus is a common pathogen in post-traumatic endophthalmitis and is associated with rapid progression and poor prognosis.[26]
The incidence of endogenous endophthalmitis remains low compared to exogenous forms, accounting for approximately 2% to 15% of all cases in most large case series. However, this proportion may be higher in regions with increased prevalence of systemic infections, liver abscesses, or poorly controlled diabetes. Bilateral involvement is more common in endogenous cases than in exogenous forms.[28]
Temporal trends suggest that while improved aseptic technique and prophylaxis have reduced the relative risk per procedure, the growing number of intraocular interventions globally has maintained the absolute burden of disease. Advances in surgical technology, antibiotic prophylaxis strategies, and sterile technique have improved outcomes, but endophthalmitis continues to pose a significant threat to vision due to its rapid progression and inflammatory sequelae.[29]
In summary, bacterial endophthalmitis is an uncommon but severe ocular infection with epidemiologic patterns that vary by geography, age, sex, and underlying etiology. Postoperative cases predominate in developed countries with high surgical volume, whereas post-traumatic cases account for a larger proportion in developing regions. Older adult populations are primarily affected in postoperative and injection-related cases, while younger males are disproportionately represented in trauma-related disease. Endogenous cases remain rare but are strongly associated with systemic comorbidities. Understanding these epidemiologic patterns is critical for prevention strategies, early recognition, and optimized clinical management worldwide.[30]
Pathophysiology
Exogenous seeding is the most common cause of bacterial endophthalmitis (see Image. Pathogenesis of Bacterial Endophthalmitis). Disease development depends on host and pathogen factors, as well as inoculum size (see Table 3). Pathogen factors play a particularly critical role in the pathogenesis of bacterial endophthalmitis (see Table 4).
Bacteria such as coagulase-negative staphylococci typically colonize the conjunctiva and can be introduced to the inner ocular cavity during surgery, injections, or trauma. After cataract surgery, research results have shown that one-third of patients' aqueous humor samples tested positive for coagulase-negative staphylococci. However, only 0.1% to 0.2% of cataract surgeries result in bacterial endophthalmitis. These numbers highlight how host factors, such as the immune response, can clear a small bacterial inoculum. However, a larger inoculum size has been shown to overload the immune system, leading to infection.[31][32][33]
Bacteremia is a rare cause of bacterial endophthalmitis, but when it does occur, Klebsiella pneumoniae is usually the culprit. The mucoviscosity-associated gene A endows K pneumoniae serotypes K1 and K2 with a mucopolysaccharide capsule that allows hypermucoviscosity. K pneumoniae is a common cause of pyogenic liver abscess in Southeast Asia, in part due to this virulence mechanism. As many as 7% of patients with K1 or K2 Klebsiella pneumoniae liver abscess will experience hematogenous spread to their retina. Experimental mouse models confirm that eyes injected with Klebsiella strains exhibiting the hypermucoviscosity (HMV) phenotype show greater retinal functional loss and inflammation than eyes injected with HMV-negative strains.[34]
Bacillus cereus can cause posttraumatic endophthalmitis, particularly in patients with intravenous drug use. B cereus is a major pathogen that can cause fulminant endophthalmitis. Quorum-sensing by Bacillus initiates toxin release and migration, contributing to the rapid deterioration of the retina and the destructive course of Bacillus endophthalmitis. The virulence factors of Bacillus species that trigger this destruction include membrane-damaging toxins such as hemolysins, sphingomyelinases, and phospholipases. The quorum-sensing–dependent phospholipase C regulator acts as a transcriptional regulator to control virulence factor production. Neutrophil recruitment and C-X-C motif chemokine ligand 1 lead to inflammation and retinal damage in Bacillus endophthalmitis.[35]
In bleb-related endophthalmitis, S pneumoniae is the most common pathogen; this organism can cause severe endophthalmitis. The virulence factors that appear to contribute to pathogenesis include exotoxins and enzymes such as pneumolysin and autolysin, as well as a polysaccharide capsule that prevents phagocytosis. S pneumoniae uses pneumolysin to inhibit host responses involved with antibody synthesis and lymphocyte proliferation. Studies have found that initial tissue damage is less severe when infected with pneumolysin-deficient S pneumoniae vs pneumolysin-producing strains within the first 24 hours of the disease.[36][37] Components of the cell wall of S pneumoniae cause inflammation, resulting in the characteristic clinical symptoms.[38]
Pseudomonas aeruginosa endophthalmitis causes rapid tissue necrosis due to toxins such as pyocyanin, pyoverdin, exotoxin A, and elastase. These toxins disrupt membrane and epithelial barriers, leading to cytotoxicity.[38] This aggressive toxin-mediated damage contributes to rapid clinical deterioration and is associated with poor visual outcomes despite prompt treatment.
Table 3. Pathophysiology of Bacterial Endophthalmitis
|
Stage |
Pathophysiologic Mechanism |
Key Mediators/Processes |
Clinical Correlations and Common Findings |
|
1. Microbial entry |
Bacteria gain access to intraocular space via surgery, trauma, injection, or hematogenous spread |
Direct inoculation (exogenous) or choroidal seeding (endogenous) |
Recent surgery/injection, open globe injury, systemic infection |
|
2. Rapid bacterial proliferation |
Vitreous cavity provides avascular, immune-privileged environment allowing unchecked bacterial multiplication |
High bacterial load; toxin production (eg, Bacillus toxins) |
Rapid onset pain, decreased vision |
|
3. Breakdown of blood–ocular barriers |
Inflammatory cytokines disrupt blood–aqueous and blood–retinal barriers |
IL-1, IL-6, TNF-α, complement activation |
Anterior chamber cells & flare, hypopyon, vitritis |
|
4. Neutrophilic infiltration |
Massive influx of PMNs into vitreous cavity |
Chemokines, complement cascade |
Dense vitreous haze, poor fundus view |
|
5. Cytokine storm and tissue damage |
Host inflammatory response contributes more to tissue damage than bacteria |
Reactive oxygen species, proteolytic enzymes |
Retinal edema, necrosis, vascular occlusion |
|
6. Vitreous opacification |
Accumulation of inflammatory debris and exudates |
Fibrin formation, cellular debris |
Floaters, red reflex loss, B-scan echoes |
|
7. Retinal and choroidal injury |
Direct toxin effect + ischemia + inflammatory destruction |
Vascular thrombosis, retinal infarction |
Severe vision loss, RAPD in advanced cases |
|
8. Advanced spread (panophthalmitis) |
Infection extends to sclera and orbit in severe cases |
Progressive inflammatory extension |
Proptosis, lid edema, orbital cellulitis |
|
9. End-stage changes |
Persistent inflammation leads to structural collapse |
Fibrosis, phthisis bulbi |
Irreversible vision loss |
IL-1, interleukin 1; IL-2, interleukin 2; TNFα, tumor necrosis factor alpha; PMNs, polymorphonuclear leukocytes; RAPD, relative afferent pupillary defect
Table 4. Most Common Pathophysiologic Findings in Bacterial Endophthalmitis
|
Finding |
Mechanism |
|
Hypopyon |
Neutrophil accumulation in anterior chamber |
|
Vitritis |
Inflammatory cells + bacterial load in vitreous |
|
Loss of red reflex |
Dense vitreous opacification |
|
Retinal necrosis |
Toxin-mediated and ischemic injury |
|
Rapid vision loss |
Combined microbial + inflammatory damage |
Histopathology
Histopathologic examination of bacterial endophthalmitis reveals a series of pathological changes within the intraocular tissues. The process begins with bacterial infiltration of the eye, triggering an acute inflammatory response. The key histopathological features observed in cases of bacterial endophthalmitis are as follows:
- Inflammatory infiltrate: The vitreous cavity typically shows an infiltration of polymorphonuclear leukocytes, indicative of an acute inflammatory response. In response to the infection, the retina and choroid may also exhibit infiltration by inflammatory cells, including lymphocytes, macrophages, and plasma cells.[39]
- Suppurative changes: Areas of suppuration may occur with the formation of abscesses within the vitreous body or the retina. Necrotizing inflammation can occur, characterized by tissue destruction and necrotic debris.[40]
- Vascular changes: Endophthalmitis can lead to vasculitis of the choroidal and retinal vasculature. Vascular occlusion and hemorrhages may be present due to the inflammation.[41]
- Fibrin exudation: Fibrin deposition is noted within the vitreous cavity and anterior chamber; this process may progress to a hypopyon, characterized by the layering of white blood cells in the anterior chamber.[42]
- Retinal detachment: Progressive inflammation can lead to separation of the sensory retina from the underlying retinal pigment epithelium.[43]
- Tissue damage and necrosis: Bacterial infection and the host immune response can lead to retinal and uveal tissue damage, with focal-to-confluent areas of necrosis.[44]
- Granulomatous reaction: In some cases, particularly with certain bacteria, a granulomatous response is observed, characterized by the formation of granulomas containing multinucleated giant cells.
- Fibrosis and scarring: Over time, the inflammation can lead to fibrosis and scarring within the eye, which can have long-term effects on vision.[45]
- Infiltration of the optic nerve: In severe cases, the optic nerve may show signs of inflammation and infiltration, potentially leading to optic atrophy.[46]
- Biofilm formation: Some bacteria can form biofilms on intraocular lenses or other implanted devices within the eye; this phenomenon enables resistance to immune cells and antibiotics.[47]
Clinicians should note that the histopathological features of bacterial endophthalmitis can vary with bacterial virulence, the host's immune status, and the duration of infection prior to treatment. Early and effective intervention is crucial in preventing the severe histopathological changes associated with this condition.
Toxicokinetics
The key toxicokinetic features of the bacteria most commonly implicated in bacterial endophthalmitis are outlined below. Understanding these aspects is crucial for effectively managing bacterial endophthalmitis, as they directly influence treatment strategies and outcomes. The goal is to maximize the local concentration of antibiotics to control the infection while minimizing inflammatory damage from bacterial toxins and the immune response.[48]
- Absorption: In bacterial endophthalmitis, bacterial toxins and inflammatory mediators are produced locally in the eye and are not absorbed in the traditional sense but can diffuse into adjacent ocular tissues.[49]
- Distribution: Bacterial toxins are typically confined to the intraocular compartments, particularly the vitreous and aqueous humor. The inflammatory response to these toxins can cause the breakdown of the blood–ocular barrier, leading to potential leakage and more widespread distribution of inflammatory cells and mediators.[45]
- Metabolism: Bacterial toxins are not metabolized in the same way as drugs. Instead, toxins may be neutralized by antibodies or broken down by enzymes in the ocular fluids, or they may persist, contributing to ongoing inflammation and damage.[50]
- Excretion: Bacterial toxins and inflammatory debris are removed from the eye by phagocytosis and possibly through the trabecular meshwork and the canal of Schlemm, which are part of the eye's natural drainage system.
- Local toxicity: The virulence factors of the bacteria damage ocular tissues, leading to the characteristic signs of endophthalmitis, including vitreous clouding, retinal edema, and uveal tract inflammation.[51]
- Pharmacokinetics of antibiotics: Intravitreal injection enables high local drug concentrations while bypassing systemic circulation, thereby reducing systemic toxicity. The half-life of antibiotics in the vitreous may be prolonged due to the vitreous body's relatively avascular nature and the slow turnover of vitreous fluid.[52]
- Response to treatment: The efficacy of antibiotic therapy for endophthalmitis can be influenced by bacterial cell wall permeability, biofilm formation, and antibiotic resistance.[53]
History and Physical
A thorough history and comprehensive ocular examination are fundamental in the early diagnosis and timely management of bacterial endophthalmitis. Because the disease can progress rapidly and lead to irreversible visual loss within hours to days, clinicians must maintain a high index of suspicion, particularly in patients presenting with recent ocular procedures or systemic infection. Early recognition significantly influences visual prognosis.
History
The hallmark symptom of bacterial endophthalmitis is a sudden decrease in vision, reported in nearly all cases (see Image. Approach to History in Suspected Bacterial Endophthalmitis). The visual decline is typically rapid in onset and may progress over hours to 1 to 3 days in acute postoperative or post-traumatic cases. Pain is common in bacterial infections but may vary in intensity depending on the organism's virulence. Redness, photophobia, lid swelling, floaters, and purulent discharge may also occur. However, the absence of severe pain does not exclude the diagnosis.[54]
The timeline of symptom onset provides valuable diagnostic clues.[55] Acute bacterial endophthalmitis typically presents within 2 to 7 days following surgery or injection. Hyperacute presentations (within 24–48 hours) may suggest highly virulent organisms such as Streptococcus or Bacillus. Chronic postoperative endophthalmitis (eg, Cutibacterium acnes) may present weeks to months later with recurrent inflammation. In contrast, fungal endophthalmitis usually demonstrates a subacute course, with gradual vision decline over days to weeks (see Table 5).[26]
A targeted history should include:
- Recent intraocular surgery (especially cataract surgery)
- Recent intravitreal injection
- History of open globe trauma
- Filtering bleb from glaucoma surgery
- Contact lens wear
- Recent antibiotic use
- Systemic infections (endocarditis, liver abscess, pneumonia, urinary tract infection)
- Intravenous drug use
- Diabetes mellitus
- Immunosuppression or malignancy
- Recent hospitalization or indwelling catheters [10]
In endogenous endophthalmitis, systemic symptoms such as fever, malaise, chills, or recent bacteremia are often present, although ocular symptoms may be the initial manifestation.[54]
Physical Examination
A complete ophthalmic examination should be performed urgently (see Table 6).
Visual acuity
Visual acuity often ranges from reduced Snellen vision to light perception or, in severe cases, no light perception. Initial visual acuity is an important prognostic indicator (see Image. Examination-Based Suspicion of Bacterial Endophthalmitis).[56]
External examination
- Eyelid edema
- Conjunctival chemosis
- Diffuse conjunctival injection
- Purulent discharge (occasionally)
Slit lamp examination
- Anterior segment findings include:
- Corneal edema (due to inflammatory endothelial dysfunction)
- Anterior chamber cells and flare
- Hypopyon (layered leukocytes in the anterior chamber)
- Fibrin formation
- Posterior synechiae
- Reduced red reflex [13]
- Posterior segment examination
- Fundus visualization may be limited due to dense vitritis. When visible, findings may include:
- Vitreous haze
- Retinal hemorrhages
- Retinal infiltrates
- Retinal necrosis
- Optic disc hyperemia
- Fundus visualization may be limited due to dense vitritis. When visible, findings may include:
B-scan ultrasonography
If the fundus view is obscured, B-scan ultrasonography is essential and typically reveals:
- Low to moderate reflective echoes within the vitreous cavity
- Membranous strands
- Retinal detachment in advanced cases
- Choroidal thickening [2]
Table 5. Key Historical Features of Endophthalmitis
|
Feature |
Bacterial Endophthalmitis |
Fungal Endophthalmitis |
|
Onset |
Acute (hours–days) |
Subacute (days–weeks) |
|
Pain |
Common, often moderate–severe |
Mild or absent |
|
Vision loss |
Rapid |
Gradual |
|
Recent surgery/injection |
Common |
Possible |
|
Systemic infection |
Less common (unless endogenous) |
More common in endogenous |
Table 6. Physical Examination Findings in Bacterial Endophthalmitis
|
Structure Examined |
Typical Findings |
Clinical Significance |
|
Visual acuity |
Severe reduction |
Prognostic indicator |
|
Conjunctiva |
Injection, chemosis |
Active inflammation |
|
Cornea |
Edema |
Barrier breakdown |
|
Anterior chamber |
Cells, flare, hypopyon |
Acute purulent inflammation |
|
Vitreous |
Dense vitritis |
Diagnostic hallmark |
|
Retina |
Infiltrates, hemorrhages |
Advanced disease |
|
B-scan |
Vitreous echoes |
Used when the fundus is obscured |
Red Flag Findings Suggesting Severe Disease
- Light perception, vision, or worse
- Rapid progression within 24 hours
- Marked hypopyon
- Severe vitritis obscuring the fundus
- Relative afferent pupillary defect
- Associated orbital signs (suggesting panophthalmitis)
Evaluation
Because bacterial endophthalmitis progresses rapidly, evaluation and treatment must occur concurrently rather than sequentially. Bacterial endophthalmitis is primarily a clinical diagnosis, and management should never be delayed while awaiting laboratory confirmation (see Image. Diagnostic Approach to Bacterial Endophthalmitis). However, microbiological, imaging, and systemic investigations are essential to confirm etiology, guide antimicrobial therapy, and evaluate systemic sources in endogenous cases (see Image. Diagnostic Pathway for Suspected Bacterial Endophthalmitis). Timely diagnostic sampling before intravitreal antibiotic administration improves culture yield but must not delay treatment (see Table 7).
Immediate Clinical Evaluation
When endophthalmitis is suspected, immediate clinical evaluation should include:
- Documentation of the best corrected visual acuity
- Slit lamp examination for anterior chamber inflammation and hypopyon
- Dilated fundus examination (if view possible)
- B-scan ultrasonography if the posterior view is obscured
- Immediate vitreous or aqueous sampling [3]
Management decisions are guided by presenting visual acuity, as supported by the Endophthalmitis Vitrectomy Study and American Academy of Ophthalmology Preferred Practice Patterns:
- Patients with vision better than light perception → vitreous tap and inject
- Patients with light perception only → consider immediate pars plana vitrectomy [57]
Table 7. Ocular Diagnostic Investigations for Suspected Bacterial Endophthalmitis
|
Investigation |
Purpose |
Typical Findings |
Clinical Role |
|
Visual acuity |
Baseline and prognosis |
Reduced to counting fingers/light perception /no light perception |
Prognostic indicator |
|
Slit lamp exam |
Assess anterior inflammation |
Hypopyon, fibrin, corneal edema |
Confirms intraocular inflammation |
|
Dilated fundus exam |
Assess the posterior segment |
Vitritis, retinal infiltrates |
Severity assessment |
|
B-scan ultrasonography |
Evaluate the posterior segment if the view is obscured |
Vitreous echoes, membranes, retinal detachment |
Essential when the media is opaque |
|
Intraocular pressure |
Assess ocular perfusion |
Often low or normal |
Helps rule out other causes |
Microbiological Evaluation
Vitreous sampling (gold standard)
Vitreous biopsy provides the highest diagnostic yield (see Table 8). Vitreous samples obtained during vitrectomy have a higher diagnostic yield than needle aspiration.
- Needle aspiration (tap)
- Vitreous cutter sampling during vitrectomy [56]
Aqueous humor sampling
Aqueous sampling has lower sensitivity than vitreous sampling because it is farther from the primary site of infection. However, an aqueous sample may be helpful when a vitreous tap is not feasible.
Guideline recommendations
- Obtain an intraocular specimen before antibiotics when feasible.
- Start empiric intravitreal antibiotics immediately (vancomycin + ceftazidime).
- Consider early vitrectomy if the presenting visual acuity is light perception.[58]
Microbiologic results may provide prognostic information and guide targeted therapy, although initial management is empiric and should not be delayed.
Table 8. Microbiological Testing for Bacterial Endophthalmitis
|
Test |
Specimen |
Purpose |
Yield/Notes |
|
Gram stain |
Vitreous or aqueous |
Rapid organism identification |
Immediate guidance |
|
Culture (aerobic and anaerobic) |
Vitreous preferred |
Definitive organism identification |
50%–70% positivity |
|
Fungal culture |
If suspected |
Identify fungal pathogens |
Slower growth |
|
Polymerase chain reaction |
Vitreous |
Detect bacterial and fungal DNA, even in culture-negative cases |
Higher sensitivity |
|
Antibiotic sensitivity testing |
Positive cultures |
Guide therapy adjustment |
Essential for targeted therapy |
Imaging Evaluation
Imaging plays a complementary role in the evaluation of bacterial endophthalmitis, particularly when clinical examination is limited or when complications are suspected (see Table 9).
B-scan ultrasonography
B-scan ultrasonography is indicated when media opacity prevents visualization of the fundus.
Typical findings:
- Low to medium reflective echoes in vitreous
- Membranous strands
- Retinal detachment
- Choroidal thickening [9]
Orbital computed tomography
Orbital computed tomography is indicated in cases of suspected:
- Trauma
- Intraocular foreign body
- Panophthalmitis [11]
Optical coherence tomography
This is useful when media clarity permits visualization of the posterior segment and detailed assessment of retinal structure.
Typical findings:
- Hyperreflective vitreous opacities (in mild cases)
- Retinal thickening or edema
- Disruption of retinal layers
- Subretinal or intraretinal fluid
- Epiretinal membrane or inflammatory debris
Table 9. Imaging Modalities for Bacterial Endophthalmitis
|
Imaging |
Indication |
Findings |
Clinical Importance |
|
B-scan ultrasound |
No fundus view |
Vitreous echoes |
Confirms vitritis |
|
Computed tomography orbit |
Trauma/ intraocular foreign body |
Foreign body, scleral rupture |
Guides surgical planning |
|
Optical coherence |
Mild cases |
Macular edema |
Rarely useful in acute severe cases |
Systemic Evaluation (Endogenous Cases)
If endogenous endophthalmitis is suspected, systemic workup is mandatory (see Table 10). Blood cultures may be positive in a subset of cases and should be obtained prior to systemic antibiotic administration when feasible (see Image. Evaluation Pathway for Endogenous Bacterial Endophthalmitis).
Recommended investigations:
- Complete blood count
- Blood cultures (2–3 sets)
- Liver function tests
- Urine culture
- Chest x-ray
- Echocardiography (if endocarditis is suspected)
- Abdominal ultrasound or computed tomography (if liver abscess is suspected) [13]
Table 10. Systemic Workup in Suspected Endogenous Endophthalmitis
|
Investigation |
Purpose |
Associated Findings |
|
Blood cultures |
Identify bacteremia |
Positive in ~50% cases |
|
Complete blood count |
Detect leucocytosis |
Elevated WBC |
|
Liver imaging |
Rule out abscess |
Klebsiella association |
|
Echocardiography |
Endocarditis |
Vegetations |
|
Urine culture |
Urinary tract infection source |
Gram-negative bacteria |
National and International Guideline Highlights
American Academy of Ophthalmology
- Immediate intravitreal broad-spectrum antibiotics
- Vitreous sampling before antibiotics, if possible
- Early vitrectomy for light perception vision
- Systemic antibiotics in endogenous cases [59]
Endophthalmitis Vitrectomy Study
- Vitrectomy improves outcomes in cases of light perception.
- Tap-and-inject is acceptable for visual acuity better than LP.[3]
Royal College of Ophthalmologists (United Kingdom)
- Do not delay treatment for microbiology.
- Consider local resistance patterns.
- Intracameral prophylaxis is recommended in cataract surgery.
Key Points in Evaluation
- Endophthalmitis is a clinical emergency.
- Diagnosis is primarily clinical, with microbiologic testing used to confirm etiology.
- Vitreous sampling provides the highest yield.
- B-scan is essential when the fundus is not visible.
- Systemic evaluation is mandatory in cases of suspected endogenous origin.
- Treatment should not be delayed while awaiting laboratory results.[13]
Treatment / Management
Bacterial endophthalmitis necessitates prompt and early management with intraocular antibiotics, often combined with a pars plana vitrectomy. Patients should be hospitalized, and broad-spectrum intravitreal, topical, and potentially intravenous antibiotics should be initiated after appropriate cultures are collected. Intravitreal antibiotics offer higher intraocular concentrations and include ceftazidime 2.2 mg, vancomycin 1 mg, and amikacin 0.4 mg.
The antibiotic of choice should be selected based on the suspected etiology, and once cultures return, the clinician can adjust antibiotic therapy.[60] Patients should receive a topical cycloplegic, such as atropine 1%, twice daily, and topical prednisolone acetate 1% every 1 to 6 hours. PPV is beneficial because it reduces the infective and inflammatory load and provides material for diagnostic studies.[61](B3)
Current Antibiotic Regimen
Contemporary therapeutic protocols for bacterial endophthalmitis typically include direct intravitreal antibiotic administration. Ceftazidime, dosed at 2.2 mg per 0.1 mL, provides broad-spectrum coverage against gram-negative bacteria. Conversely, at a dose of 1.0 mg per 0.1 ml, vancomycin is used for its broad coverage of gram-positive pathogens, with a 99% susceptibility rate among gram-positive organisms implicated in endophthalmitis. However, cases of vancomycin-resistant Enterococcus causing endophthalmitis have been reported, indicating that the effectiveness of traditionally used antibiotics varies with the emergence of resistance.[62] For endogenous endophthalmitis, systemic antibiotic administration is standard.
Ceftazidime, a third-generation cephalosporin, has historically shown complete susceptibility among gram-negative ocular isolates. Nonetheless, resistance has been documented, with a subset of gram-negative endophthalmitis cases exhibiting resistance to amikacin and ceftazidime. Structural advancements within the cephalosporin class have enhanced their efficacy against gram-negative bacteria, with both second- and third-generation cephalosporins demonstrating this improved activity.[63](A1)
Intravitreal ceftazidime is generally regarded as safer compared to aminoglycosides, with toxicity observed only at elevated concentrations. Clinical evidence suggests a significant reduction in the risk of endophthalmitis when cefuroxime, a second-generation cephalosporin, is administered intracamerally as a surgical prophylactic. The synergistic potential of antibiotic combinations, particularly vancomycin paired with either amikacin or ceftazidime, should be considered when managing rapidly progressing infections such as endophthalmitis. However, the necessity is debated because intravitreal injections achieve high local concentrations.[64]
Fluoroquinolones are another promising class for the treatment of endophthalmitis, especially later generations, which exhibit robust activity against a broad spectrum of ocular pathogens. The ability of fluoroquinolones to cross the ocular barrier without intravitreal injection underscores their value in specific clinical scenarios. Although primarily indicated for ocular surface infections, their use for endophthalmitis is considered off-label. Experimental studies have confirmed the safety and effectiveness of intravitreal fluoroquinolones in eliminating intraocular infections, suggesting that intravitreal administration of these and other antibiotics can be effective when immediate, adequate bactericidal concentrations at the site of infection are required.[65]
However, the use of fluoroquinolones for surgical prophylaxis or for the treatment of postoperative endophthalmitis remains contentious. The penetration of fluoroquinolones into ocular tissues varies widely, with moxifloxacin showing superior intraocular penetration compared to gatifloxacin in topical administration. Despite the efficacy of topical moxifloxacin in experimental models, the ability of fourth-generation fluoroquinolones to achieve bactericidal concentrations in the vitreous remains inconsistent.[66] Notably, gatifloxacin has been discontinued for systemic use due to its association with dysglycemia.
Anti-Inflammatory Drugs
Intraocular inflammation, a crucial component of the host defense mechanism against infection, can inflict retinal damage. Intravitreal introduction of bacterial cell wall components provokes a significant inflammatory response within the ocular environment. This reaction typically results in only transient, reversible functional impairment of the retina, but given the potential for the inflammatory response to cause permanent damage within the eye, intravitreal corticosteroids may be administered strategically to mitigate immune-mediated injury. This method can serve as an additional therapeutic strategy alongside antibiotic treatment.[67]
The clinical and experimental literature presents a divergent viewpoint on the utility of intravitreal corticosteroids in the context of endophthalmitis. While the safety profile of dexamethasone following intravitreal injection is well established clinically, with no evidence of retinal toxicity, its efficacy remains a point of contention. Disparate clinical findings have been reported, with some studies suggesting that intravitreal dexamethasone may be beneficial, whereas others argue its utility is negligible.[68]
Experimental investigations into the role of intravitreal steroids in bacterial endophthalmitis have similarly yielded inconsistent outcomes. Some studies' results support the efficacy of combined dexamethasone and antibiotic therapy in managing inflammation, while others report no significant advantage. Furthermore, combinations of intravitreal prednisolone and antibiotics did not reduce inflammation in experimental Bacillus endophthalmitis compared with antibiotic therapy alone. Although a definitive consensus has not been reached, corticosteroids, such as dexamethasone 0.4 mg, are frequently used as adjuncts in the management of endophthalmitis, reflecting a preference for their anti-inflammatory properties in combination with antibiotic regimens.[69]
Role of Vitrectomy
In advanced presentations of endophthalmitis, pars plana vitrectomy is frequently employed to excise necrotic microorganisms, compromised cellular material, and deleterious inflammatory by-products from the vitreous cavity. This intervention enhances optical clarity and diffusion within the posterior segment, expediting the restoration of visual function. Minimally invasive approaches to vitrectomy, such as 23- and 25-gauge systems, have gained favor in recent years. Nonetheless, the inherent complexity of PPV entails certain procedural risks, even with these refined techniques.[1](B3)
The Endophthalmitis Vitrectomy Study led to increased use of vitrectomy for therapeutic purposes in endophthalmitis (see Image. Visual Acuity–Based Treatment Algorithm for Bacterial Endophthalmitis). Early vitrectomy improved visual acuity outcomes for patients with hand motion or light perception deficits. The postulated mechanisms underlying the efficacy of vitrectomy in such scenarios include a breach of the blood–ocular barrier, which may enhance the intraocular penetration of systemic antibiotics. A synergistic approach of immediate intravitreal antibiotics coupled with PPV is recommended for endophthalmitis secondary to ocular trauma with retained intraocular foreign bodies. This strategy, including timely foreign body removal, has been associated with significant visual recovery in most cases, although a subset of patients may experience visible decline after these interventions.[70](B3)
Similarly, the prognosis for endophthalmitis secondary to ocular procedures other than cataract surgery appears to benefit from expeditious vitrectomy, especially when initial conservative management is ineffective. In endogenous endophthalmitis, the temporal aspect of vitrectomy plays a pivotal role, with early surgical intervention correlating with improved outcomes. The consensus within clinical literature increasingly supports immediate vitrectomy alongside appropriate intravitreal antibiotic therapy in severe cases of endophthalmitis, particularly those complicated by IOFBs. This aggressive treatment modality is deemed essential for optimizing recovery.[71]
Exploratory research has focused on the utility of vitrectomy in managing fungal endophthalmitis, but the mechanical debridement of pathogen load, inflammatory mediators, and toxic substances through vitrectomy remains equally pertinent for bacterial infections. Novel office-based sutureless vitrectomy systems show promise, although their use in treating endophthalmitis has yet to be substantiated in clinical practice. The current body of experimental research on the efficacy of vitrectomy for bacterial endophthalmitis is limited, underscoring the need for further investigation into the benefits of this surgical intervention in managing infectious vitritis.[72]
Periocular injections or subtenon injections are options if necessary.[38] Results from a recent study demonstrated the most common isolate in cases of endophthalmitis following evisceration was S pneumoniae, followed by Aspergillus and P aeruginosa.[38] Endophthalmitis can convert to panophthalmitis if the infection spreads to the sclera and the Tenon capsule.[73]
In panophthalmitis, the affected eye requires evisceration or enucleation; studies report an evisceration rate ranging from 14.3% to 23.2%.[73] All isolates were susceptible to ceftazidime and levofloxacin, and the minimum inhibitory concentration values for isolates in the current period were identical to those from 1987 to 2001. Despite early and appropriate treatment, outcomes for panophthalmitis were generally poor, with a high enucleation rate.[74] Patients with intravenous drug use are given aminoglycosides and clindamycin to cover the most likely causative organism, B cereus.
Differential Diagnosis
Bacterial endophthalmitis is an ocular emergency characterized by inflammation and infection within the eye. Differentiating it from other conditions with similar presentations is vital for effective treatment (see Table 11). The differential diagnosis includes:
- Sterile endophthalmitis
- Similar to infectious endophthalmitis, but occurs as a sterile inflammatory response to intraocular agents or surgery and lacks the growth of organisms on culture [75]
- Fungal endophthalmitis
- May present similarly, but has a more indolent course
- Risk factors include systemic immunosuppression, chronic antibiotic use, and IV drug use
- Investigation includes fungal cultures and consideration of intravitreal antifungal therapy [76]
- Viral retinitis
- Commonly due to cytomegalovirus or herpes simplex virus
- Presents with retinal necrosis and hemorrhages
- May have less prominent pain than bacterial endophthalmitis
- Requires polymerase chain reaction testing of ocular fluids for definitive diagnosis [77]
- Noninfectious uveitis
- Inflammatory condition without infection
- May be associated with systemic autoimmune conditions [78]
- Acute retinal necrosis
- Syndrome characterized by peripheral necrotizing retinitis, usually due to viral etiology
- Typically progresses to retinal detachment [79]
- Toxic anterior segment syndrome
- Acute sterile postoperative inflammation following cataract surgery due to a noninfectious substance entering the anterior segment
- Distinguished from endophthalmitis by rapid onset and lack of vitreous involvement [76]
- Panuveitis
- Involves inflammation of all uveal tracts
- May mimic the appearance of endophthalmitis [80]
- Retained intraocular foreign body
- Must differentiate post-traumatic bacterial endophthalmitis from the simple presence of an intraocular foreign body without infection
- Imaging studies, such as computed tomography or B-scan ultrasonography, aid in diagnosis [81]
- Masquerade syndromes (eg, intraocular lymphoma)
- May present with symptoms similar to endophthalmitis, but the underlying mechanism is neoplastic, rather than infectious [82]
- Ocular ischemic syndrome
- Presents with pain and vision loss, but it is due to vascular insufficiency rather than infection [83]
- Retinochoroidal infection
- Infection involves the retina and choroid, mimicking the vitreous haze and retinal lesions in endophthalmitis
- Causative organisms include herpes simplex virus, cytomegalovirus, especially in immunocompromised patients, or toxoplasmosis
- Diagnosis based on serological tests, ocular fluid analysis, and clinical picture [84]
- Noninfectious posterior or intermediate uveitis
- Inflammatory conditions that affect the posterior segment and can resemble the vitritis seen in endophthalmitis
- May be associated with systemic autoimmune diseases or idiopathic causes
- Clinical diagnosis, supported by imaging (eg, optical coherence tomography and fluorescein angiography) and excluded from infectious causes.[85]
- Neoplastic conditions
- Retinoblastoma, uveal melanoma, ocular surface squamous neoplasia, lymphoma, choroidal hemangioma, optic nerve glioma, ciliary body, and iris tumors, among others
- Large cell lymphoma
- May present with vitreous cells and haze, similar to endophthalmitis
- Typically older population
- Vitreous biopsy for cytology is often required for diagnosis
- Retinoblastoma
- Usually occurs in children
- May present with leukocoria and vitreous seeding that may resemble endophthalmitis
- Imaging with ultrasound and MRI, along with clinical examination, is required for diagnosis [86]
Table 11. Differential Diagnosis of Bacterial Endophthalmitis
|
Condition |
Key Distinguishing Features |
Differentiation from Bacterial Endophthalmitis |
Diagnostic Clues |
|
Toxic anterior segment syndrome |
Sterile postoperative inflammation; onset within 12 to 48 hrs after surgery |
No vitritis; minimal pain; sterile cultures |
Clear vitreous; responds to steroids; no infectious organism |
|
Severe noninfectious uveitis |
History of autoimmune disease; recurrent episodes |
Less purulent; usually no hypopyon with fibrin layering |
Systemic inflammatory markers; responds to steroids |
|
Acute angle-closure glaucoma |
Severe ocular pain; headache; halos |
Elevated IOP; mid-dilated pupil; corneal edema without vitritis |
IOP >40 mm Hg; shallow anterior chamber |
|
Sterile postoperative inflammation |
Mild inflammation; improves with steroids |
No rapid deterioration; no dense vitritis |
Negative cultures; stable vision |
|
Retinal detachment |
Flashes and floaters; curtain-like visual loss |
No hypopyon; no anterior chamber reaction |
B-scan shows detached retina without inflammatory echoes |
|
Vitreous hemorrhage |
Sudden vision loss; no significant pain |
No hypopyon; no marked anterior inflammation |
B-scan shows mobile dense echoes without inflammatory debris |
|
Intraocular foreign body |
Trauma history |
May coexist with infection |
Computed tomography orbit identifies foreign body |
|
Orbital cellulitis |
Proptosis; restricted eye movements; systemic symptoms |
Primarily orbital signs; intraocular inflammation less prominent initially |
Computed tomography orbit shows orbital soft tissue involvement |
|
Fungal endophthalmitis |
Subacute onset; mild pain; fluffy vitreous infiltrates |
Slower progression; often endogenous |
Candida “string of pearls” lesions |
|
Masquerade syndromes (eg, intraocular lymphoma) |
Chronic course; minimal pain |
Steroid-responsive initially; no purulent inflammation |
Vitreous biopsy shows malignant cells |
|
Sympathetic ophthalmia |
Bilateral granulomatous uveitis; history of trauma |
Bilateral involvement; no purulence |
Dalen-Fuchs nodules; systemic autoimmune features |
|
Postoperative hyphema |
Blood in anterior chamber |
Red blood cells instead of hypopyon |
History of surgical trauma; visible red blood cell layering |
|
Panophthalmitis |
Extension beyond globe |
Orbital involvement |
Severe lid edema, proptosis |
A thorough history, detailed ocular examination, imaging, and laboratory investigations, including cultures and polymerase chain reaction testing, are essential in diagnosing bacterial endophthalmitis. The correct diagnosis guides targeted therapy, from antibiotics or antivirals to immunosuppressive treatments, depending on the underlying cause (see Table 12).
Table 12. Clinical Differentiation of Bacterial Endophthalmitis, Toxic Anterior Segment Syndrome, and Fungal Endophthalmitis
|
Feature |
Bacterial Endophthalmitis |
TASS |
Fungal Endophthalmitis |
|
Onset |
2 to 7 days (acute) |
12 to 48 hrs |
Days–weeks |
|
Pain |
Moderate–severe |
Minimal |
Mild |
|
Vitritis |
Present |
Absent |
Present |
|
Hypopyon |
Common |
May occur |
Less dense |
|
Culture |
Positive |
Negative |
Fungal growth |
|
Treatment |
Intravitreal antibiotics |
Steroids |
Antifungals |
Red Flags Suggesting Infectious Endophthalmitis
- Rapid visual deterioration
- Hypopyon with vitritis
- Recent intraocular procedure
- Severe ocular pain
- Poor red reflex
- Dense vitreous echoes on B-scan
Pertinent Studies and Ongoing Trials
The management of bacterial endophthalmitis is grounded in pivotal randomized controlled trials (RCTs), prospective cohort studies, and guideline-driven consensus statements. The strongest evidence supporting current recommendations, particularly intravitreal antibiotics and selective PPV, comes from the Endophthalmitis Vitrectomy Study (EVS) and subsequent epidemiologic and interventional studies.[2]
Landmark Randomized Controlled Trial: Endophthalmitis Vitrectomy Study
The EVS remains the most influential RCT guiding treatment of acute postoperative endophthalmitis (see Table 13).
- Population: There were 420 patients with acute postoperative endophthalmitis following cataract surgery or secondary intraocular lens implantation
- Design: Randomized to:
- Immediate pars plana vitrectomy vs vitreous tap/biopsy
- Intravenous antibiotics vs no intravenous antibiotics
- Intervention: All patients received intravitreal vancomycin and amikacin.[87]
Impact on recommended treatment
- Immediate intravitreal antibiotics are the standard of care.
- PPV is recommended for patients with light-perception vision.
- Tap-and-inject is acceptable for patients with vision better than light perception.
- Systemic antibiotics are not routinely required in exogenous postoperative cases.
Table 13. Key Findings from the Endophthalmitis Vitrectomy Study
|
Outcome |
Results |
Clinical Implication |
|
Visual acuity ≥20/40 |
53% overall |
A good prognosis is possible with early treatment |
|
Benefit of pars plana vitrectomy |
Significant only in patients with light perception vision |
PPV recommended if initial visual acuity = light perception |
|
Intravenous antibiotics |
No additional visual benefit |
Routine intravenous antibiotics are not required in postoperative cases |
|
Organism profile |
Mostly gram-positive cocci |
Supports empiric vancomycin coverage |
Intracameral Antibiotic Prophylaxis Studies
Multiple large prospective European studies (eg, European Society of Cataract and Refractive Surgeons [ESCRS] trial) demonstrated:
- Significant reduction in postoperative endophthalmitis with intracameral cefuroxime
- Reduction in infection rates from ~0.3% to less than 0.1%
Clinical implication
These studies support the guideline recommendations for intracameral antibiotic prophylaxis in cataract surgery.[88][89] Additional evidence suggests that procedural factors, including surgical technique and intraocular lens selection, as well as perioperative antimicrobial strategies, influence infection risk, although findings across studies are variable.[90] Prevention remains challenging to study due to the low incidence of endophthalmitis; however, adherence to aseptic technique, appropriate wound construction, and antimicrobial prophylaxis is essential in minimizing risk.[91]
Post-Injection Endophthalmitis Studies
Post-injection endophthalmitis is an uncommon but important complication of intravitreal anti-vascular endothelial growth factor therapy. Evidence from large registries and observational studies has clarified incidence rates, organism profiles, and factors influencing infection risk. These data support best practices in aseptic technique and procedural precautions (see Table 14).
Table 14. Bacterial Endophthalmitis Post-Injection Studies
|
Study Type |
Key Findings |
Clinical Implication |
|
Multicenter injection registries |
Incidence 0.02% to 0.05% per injection |
Confirms low but cumulative risk |
|
Mask usage studies |
Reduced Streptococcus-related cases |
Supports strict aseptic technique |
|
Culture studies |
Higher Streptococcus rates vs postoperative cases |
Emphasizes droplet precautions |
Early Vitrectomy Studies Beyond EVS
Recent retrospective analyses and smaller prospective series suggest:
- Early PPV may improve outcomes in severe cases beyond the EVS light-perception-only criteria.
- Small-gauge vitrectomy techniques allow earlier intervention.
- Possible benefit in highly virulent organisms (eg, Streptococcus, Bacillus).
However, no large modern RCT has definitively replaced EVS recommendations.[92]
Endogenous Endophthalmitis Evidence
Large RCTs for the treatment of endogenous bacterial endophthalmitis do not yet exist. Management is instead based on the following data sources (see Table 15):
- Retrospective case series
- Systemic infection control studies
- Regional organism data (eg, Klebsiella liver abscess studies in Asia)
Evidence supports:
- Combined intravitreal + systemic intravenous antibiotics
- Source control (abscess drainage, catheter removal)
- Early vitrectomy in severe bilateral cases [93]
Table 15. Evidence Supporting Recommended Treatment
|
Recommended Treatment |
Supporting Study |
Level of Evidence |
Key Outcome |
|
Intravitreal vancomycin + ceftazidime |
EVS |
Level I (RCT) |
Improved visual outcomes |
|
PPV for light perception vision |
EVS |
Level I |
Better visual acuity recovery |
|
Intracameral prophylaxis |
ESCRS Trial |
Level I |
Reduced postoperative rates |
|
Tap-and-inject for visual acuity >light perception |
EVS |
Level I |
Comparable outcomes |
|
Systemic antibiotics (endogenous cases) |
Observational studies |
Level II–III |
Reduced systemic morbidity |
EVS, Endophthalmitis Vitrectomy Study; ESCRS, European Society of Cataract and Refractive Surgeons; PPV, pars plana vitrectomy; RCT, randomized controlled trial
Ongoing and Emerging Research Areas
Although no major contemporary RCT equivalent to EVS is currently redefining standard management for bacterial endophthalmitis, ongoing areas of investigation include studies in the following domains (see Table 16).
Table 16. Active Research Areas for Bacterial Endophthalmitis
|
Research Area |
Clinical Focus |
|
Small-gauge early vitrectomy |
Impact of earlier surgery on improving outcomes |
|
Intravitreal corticosteroids |
Role in modulating inflammatory damage |
|
Rapid polymerase chain reaction diagnostics |
Faster organism identification |
|
Newer broad-spectrum antibiotics |
Resistance pattern adaptation |
|
Prophylaxis protocols |
Optimization of injection-room sterility |
Current Evidence Gaps
- Limited modern RCT data incorporating the anti-vascular endothelial growth factor era surgical volumes
- Limited randomized data in endogenous endophthalmitis
- Limited pediatric-specific RCT evidence
- No large trial comparing immediate PPV for all patients vs a selective approach
Summary
The management of bacterial endophthalmitis is primarily supported by high-quality evidence from the EVS, which established intravitreal antibiotics as the cornerstone of therapy and defined surgical indications based on presenting visual acuity. Subsequent epidemiologic and prophylactic studies further refined prevention and management strategies. While newer surgical techniques and diagnostic tools continue to evolve, current recommendations remain strongly rooted in EVS-derived evidence and reinforced by international ophthalmic guidelines.
Treatment Planning
Bacterial endophthalmitis is a true ophthalmic emergency, and treatment must be initiated immediately upon clinical suspicion. Therapy should not be delayed for laboratory confirmation. Management is guided by clinical presentation, visual acuity at diagnosis, etiology (exogenous vs endogenous), organism virulence, and presence of complications such as retinal detachment or panophthalmitis (see Image. Treatment Algorithm for Bacterial Endophthalmitis).[58]
Immediate Treatment Principles
- Prompt vitreous sampling (if feasible)
- Immediate intravitreal broad-spectrum antibiotics
- Consideration of PPV based on visual acuity
- Adjunctive topical therapy
- Systemic antibiotics in endogenous cases
- Close monitoring and repeat intervention if needed [29]
The following intravitreal antibiotic doses are supported by AAO and EVS guidelines (see Table 17).
Table 17. Standard Intravitreal Antibiotic Regimen for Bacterial Endophthalmitis
|
Antibiotic |
Dose (Intravitreal) |
Coverage |
Purpose |
|
Vancomycin |
1.0 mg/0.1 mL |
Gram-positive organisms (including methicillin-resistant Staphylococcus aureus) |
Primary gram-positive coverage |
|
Ceftazidime |
2.25 mg/0.1 mL |
Gram-negative organisms |
Broad gram-negative coverage |
|
Amikacin (alternative) |
0.4 mg/0.1 mL |
Gram-negative |
Used if cephalosporin allergy |
Decision-Making Based on Visual Acuity
The EVS remains the cornerstone for surgical planning (see Table 18).
Table 18. Surgical Planning in Bacterial Endophthalmitis
|
Clinical Scenario |
Recommended Action |
Rationale |
|
Visual acuity better than light perception |
Vitreous tap + inject |
Comparable outcomes to PPV |
|
Visual acuity = light perception |
Immediate PPV + inject |
Improved visual outcomes |
|
Severe streptococcal infection |
Consider early PPV |
Highly virulent organism |
|
Post-traumatic with IOFB |
PPV + foreign body removal |
Reduce infectious load |
|
Endogenous cases |
Intravitreal + systemic antibiotics ± PPV |
Control ocular & systemic source |
IOFB, intraocular foreign body; PPV, pars plana vitrectomy
Pars Plana Vitrectomy
Indications:
- Presenting visual acuity = light perception
- Dense vitreous opacification
- Retinal detachment
- Poor response to initial therapy
- Highly virulent organisms
Goals of PPV:
- Remove infective and inflammatory debris.
- Reduce bacterial load.
- Improve antibiotic penetration.
- Improve visualization for retinal assessment.
Modern small-gauge (23G–27G) vitrectomy systems enable earlier and safer intervention than EVS-era techniques.[54]
Adjunctive Therapies
Intravitreal corticosteroids
- Dexamethasone 0.4 mg/0.1 mL (controversial)
- May reduce inflammatory damage
- Use cautiously; evidence is mixed.
Topical therapy
Topical therapy serves as an adjunct to intravitreal antibiotics in the management of bacterial endophthalmitis, primarily targeting anterior-segment inflammation and improving patient comfort (see Table 19).
Table 19. Topical Therapy for Bacterial Endophthalmitis
|
Medication |
Purpose |
|
Fortified topical antibiotics |
Additional anterior segment coverage |
|
Topical steroids |
Reduce inflammation (after antibiotics are initiated) |
|
Cycloplegics |
Pain relief and prevent synechiae |
Systemic antibiotics
Indications:
- Endogenous endophthalmitis
- Orbital involvement
- Panophthalmitis
- Immunocompromised patients
Common systemic regimens:
- Intravenous vancomycin + intravenous ceftriaxone
- Tailored based on culture results
Systemic antibiotics are not routinely required in exogenous postoperative cases, according to EVS findings.[12]
Monitoring and Re-Treatment
Patients require close daily monitoring initially (see Table 20).
Signs of improvement:
- Reduced hypopyon
- Decreased vitritis
- Improved visual acuity
- Reduced ocular pain
Indications for repeat intravitreal injection:
- Persistent inflammation
- Worsening vision
- Positive culture with a resistant organism
Repeat injections are typically administered 48 to 72 hours after initial treatment if needed.[94]
Table 20. Follow-Up Schedule for Bacterial Endophthalmitis
|
Time Frame |
Assessment Focus |
|
24 hours |
Clinical response, intraocular pressure, inflammation |
|
48–72 hours |
Consider repeat injection |
|
1 week |
Retinal status, complications |
|
Long-term |
Visual rehabilitation |
Management of bacterial endophthalmitis varies by underlying etiology, with differences in microbial virulence, route of infection, and risk of complications influencing treatment planning. Recognizing these distinctions helps guide appropriate procedural and antimicrobial interventions (see Table 21).
Table 21. Management of Bacterial Endophthalmitis by Etiologic Category
|
Type |
Primary Treatment Strategy |
|
Postoperative |
Tap and inject ± PPV |
|
Post-injection |
Same as postoperative |
|
Post-traumatic |
Early PPV is often recommended |
|
Bleb-related |
Aggressive treatment; streptococcal coverage |
|
Endogenous |
Intravitreal + systemic intravenous antibiotics |
Complications of bacterial endophthalmitis can significantly impact visual outcomes and often require targeted interventions beyond initial infection control. Early recognition and appropriate management are essential to minimize long-term morbidity (see Table 22).[6]
Table 22. Complication Management for Bacterial Endophthalmitis
|
Complication |
Management |
|
Retinal detachment |
Surgical repair |
|
Persistent hypotony |
Monitor; treat inflammation |
|
Epiretinal membrane |
Secondary surgery |
|
Phthisis bulbi |
End-stage management |
Key Principles
- Treatment must not be delayed.
- Intravitreal antibiotics are the cornerstone.
- PPV improves outcomes in light perception vision.
- Systemic antibiotics are reserved for endogenous cases.
- Early aggressive management improves prognosis.
Toxicity and Adverse Effect Management
Management of bacterial endophthalmitis requires aggressive antimicrobial therapy and, in some cases, surgical intervention. However, both the infection itself and the therapeutic interventions may result in ocular and systemic adverse effects. Prompt recognition and appropriate management of treatment-related toxicity are critical to preserving visual function and minimizing complications (see Image. Adverse Effect Monitoring Pathway for Bacterial Endophthalmitis).
Adverse effects may arise from:
- Intravitreal antibiotics
- Systemic antibiotics
- Corticosteroids
- Pars plana vitrectomy
- Inflammatory sequelae of infection [2]
Intravitreal Antibiotic Toxicity
Intravitreal antibiotics are administered in high intraocular concentrations and may cause dose-dependent retinal toxicity if improperly prepared or overdosed (see Table 23). Strict adherence to recommended intravitreal dosing is essential to prevent retinal toxicity.
Table 23. Intravitreal Antibiotic Toxicity in Bacterial Endophthalmitis
|
Drug |
Potential Toxicity |
Mechanism |
Clinical Signs |
Management |
|
Vancomycin |
Rare retinal toxicity |
Direct retinal cellular toxicity (high dose) |
Decreased vision, retinal whitening |
Supportive; avoid overdose |
|
Ceftazidime |
Minimal toxicity |
Generally safe at the recommended dose |
Rare macular edema |
Monitor |
|
Amikacin |
Macular infarction (rare but serious) |
Retinal vascular toxicity |
Sudden severe vision loss, central scotoma |
Avoid if possible; prefer ceftazidime |
|
Gentamicin (historical use) |
Severe retinal toxicity |
Retinal necrosis |
Profound vision loss |
No longer recommended |
Hemorrhagic Occlusive Retinal Vasculitis
Hemorrhagic occlusive retinal vasculitis is a rare but severe complication associated with intracameral or intravitreal vancomycin.
Clinical features:
- Delayed onset (1–2 weeks after surgery)
- Retinal hemorrhages
- Vascular occlusion
- Severe visual loss
Management:
- High-dose systemic and intravitreal corticosteroids
- Avoid future vancomycin exposure
- Aggressive retinal ischemia management (anti-vascular endothelial growth factor, panretinal photocoagulation if needed) [5]
Steroid-Related Adverse Effects
Corticosteroids may be used adjunctively but carry risks (see Table 24). Steroids should only be initiated after adequate antimicrobial coverage.[6]
Table 24. Corticosteroid Toxicity in Bacterial Endophthalmitis
|
Route |
Adverse Effect |
Management |
|
Topical |
Elevated intraocular pressure |
Monitor intraocular pressure; add antiglaucoma drops |
|
Intravitreal dexamethasone |
Delayed infection resolution (theoretical) |
Careful patient selection |
|
Systemic steroids |
Hyperglycemia, immunosuppression |
Monitor glucose; taper appropriately |
Systemic Antibiotic Toxicity (Endogenous Cases)
When systemic antibiotics are required for endogenous bacterial ophthalmitis, monitor for systemic side effects (see Table 25).
Table 25. Adverse Effects of Systemic Antibiotics in Endogenous Bacterial Endophthalmitis
|
Drug |
Major Toxicity |
Monitoring |
|
Vancomycin (intravenous) |
Nephrotoxicity, vancomycin infusion reaction (formerly red man syndrome) |
Renal function tests |
|
Ceftriaxone |
Biliary sludge, allergy |
Liver function tests if prolonged |
|
Fluoroquinolones |
QT prolongation, tendon rupture |
Electrocardiogram if high risk |
|
Aminoglycosides |
Nephrotoxicity, ototoxicity |
Renal monitoring |
Surgical Complications (Pars Plana Vitrectomy)
PPV is a key surgical intervention in selected cases of bacterial endophthalmitis but carries inherent procedural risks. Awareness of potential complications and their management is essential for optimizing surgical outcomes (see Table 26).
Table 26. Adverse Effects of Surgery for Bacterial Endophthalmitis
|
Complication |
Mechanism |
Management |
|
Retinal detachment |
Tractional or rhegmatogenous |
Surgical repair |
|
Hypotony |
Ciliary body dysfunction |
Observation or intervention |
|
Iatrogenic retinal tear |
Instrument-related |
Laser retinopexy |
|
Cataract progression |
Lens trauma |
Cataract surgery (later) |
Inflammation-Related Complications
A severe inflammatory response itself may cause:
- Macular edema
- Epiretinal membrane
- Optic nerve damage
- Phthisis bulbi
Management includes:
- Controlled steroid therapy
- Secondary vitreoretinal procedures
- Visual rehabilitation [5]
Table 27 summarizes key toxicity risks associated with treatment modalities for bacterial endophthalmitis, including intravitreal, systemic, surgical, and corticosteroid therapies. Risks range from retinal toxicity and systemic or renal adverse effects to structural surgical complications and intraocular pressure elevation with steroid use, underscoring the need for careful risk-benefit assessment.
Table 27. Bacterial Endophthalmitis Toxicity Risk Stratification
|
Treatment Type |
Complication |
|
Intravitreal |
Retinal toxicity risk |
|
Systemic |
Renal and systemic toxicity |
|
Surgical |
Structural complications |
|
Steroids |
Intraocular pressure elevation |
Prevention of Toxicity
- Strict adherence to recommended dosing
- Accurate drug dilution protocols
- Avoidance of aminoglycosides when safer alternatives exist
- Renal function monitoring in systemic therapy
- Early recognition of hemorrhagic occlusive retinal vasculitis
- Close postoperative follow-up [26]
Key Clinical Pearls
- Most cases of retinal toxicity result from dosing errors.
- Ceftazidime is safer than amikacin for gram-negative coverage.
- Steroids should never precede antibiotic administration.
- Sudden worsening after initial improvement warrants urgent reassessment.
- Early intervention prevents permanent structural damage.
Summary
While aggressive antimicrobial therapy is essential in bacterial endophthalmitis, treatment-related toxicity and inflammatory sequelae must be carefully monitored. Intravitreal antibiotics are generally safe when administered correctly, but retinal toxicity, steroid-induced intraocular pressure elevation, systemic antibiotic complications, and surgical risks must be anticipated. A structured monitoring protocol ensures early detection and optimal visual outcomes.[9]
Staging
Unlike malignancies and chronic inflammatory conditions, bacterial endophthalmitis lacks a universally standardized staging system. However, clinical severity–based staging is highly relevant for treatment decisions, prognostication, and surgical planning (see Image. Staging-Based Management of Bacterial Endophthalmitis). Staging is primarily based on:
- Visual acuity at presentation
- Extent of anterior and posterior segment inflammation
- Presence of complications (retinal detachment, panophthalmitis)
- Systemic involvement (endogenous cases)
The Endophthalmitis Vitrectomy Study (EVS) indirectly established a severity-based classification using presenting visual acuity to guide management (see Image. Clinical Severity Staging of Bacterial Endophthalmitis).[3]
Clinical Staging System for Bacterial Endophthalmitis
This severity-based framework synthesizes clinical findings and visual acuity to support risk stratification and procedural decision-making (see Table 28).
Table 28. Severity-Based Clinical Staging for Bacterial Endophthalmitis
|
Stage |
Clinical Features |
Visual Acuity |
Ocular Findings |
Recommended Management |
|
Stage I = Early/Mild |
Mild pain, redness, reduced vision |
20/40 to 20/200 |
Anterior chamber cells, mild vitritis |
Vitreous tap + intravitreal antibiotics |
|
Stage II = Moderate |
Increased pain, hypopyon present |
20/200 to counting fingers |
Dense anterior chamber reaction, moderate vitritis |
Tap and inject; close monitoring |
|
Stage III = Severe |
Marked pain, significant hypopyon |
Hand movements to light perception |
Dense vitritis, no fundus view |
Consider early pars plana vitrectomy + antibiotics |
|
Stage IV = Advanced |
Profound vision loss |
Light perception or worse |
Total media opacity, possible retinal detachment |
Immediate pars plana vitrectomy |
|
Stage V = Panophthalmitis |
Severe lid edema, proptosis |
No light perception often |
Orbital involvement |
Systemic intravenous antibiotics ± enucleation |
EVS-Based Functional Staging
The EVS simplified staging into two major functional categories (see Table 29). This staging remains widely used in modern clinical decision-making.
Table 29. Endophthalmitis Vitrectomy Study–Based Functional Staging
|
EVS Category |
Definition |
Treatment Recommendation |
|
Better than light perception |
Visual acuity > light perception |
Tap and inject |
|
Light perception only |
Visual acuity = light perception |
Immediate pars plana vitrectomy |
Anatomic Staging
Anatomic classification complements severity-based staging by defining the extent of intraocular and orbital involvement, which has important implications for disease progression and urgency of intervention (see Table 30).
Table 30. Anatomic Spread–Based Staging for Bacterial Endophthalmitis
|
Stage |
Anatomic Involvement |
Clinical Implication |
|
Posterior endophthalmitis |
Vitreous cavity involvement |
Classic presentation |
|
Anterior endophthalmitis |
Anterior chamber inflammation predominates | Rare; early detection possible |
|
Diffuse endophthalmitis |
Anterior + posterior involvement |
Severe infection |
|
Panophthalmitis |
The entire globe + orbit is involved |
Vision-threatening emergency |
Microbiological Severity Correlation
Certain organisms are associated with more aggressive stages at presentation (see Table 31).
Table 31. Microbiologic Correlates of Disease Severity in Bacterial Endophthalmitis
|
Organism |
Typical Stage at Presentation |
Prognosis |
|
Coagulase-negative Staphylococcus |
Stage I–II |
Good with treatment |
|
Streptococcus spp |
Stage III–IV |
Guarded |
|
Bacillus cereus |
Stage IV–V |
Poor |
|
Klebsiella (endogenous) |
Stage III–IV |
Often bilateral; poor |
Early-stage detection significantly improves outcomes (see Table 32). Visual acuity at presentation remains the strongest prognostic indicator.
Table 32. Bacterial Endophthalmitis Prognostic Implications by Stage
|
Stage |
Visual Prognosis |
|
Stage I |
Often recoverable vision |
|
Stage II |
Variable outcome |
|
Stage III |
Guarded |
|
Stage IV |
Poor |
|
Stage V |
Very poor; risk of phthisis |
This simplified grading system translates staging concepts into a practical framework for rapid bedside decision-making and initial management (see Table 33).
Table 33. Proposed Practical Clinical Staging
|
Grade |
Description |
Immediate Action |
|
Grade A |
Mild inflammation, visual acuity >20/200 |
Urgent tap and inject |
|
Grade B |
Hypopyon + moderate vitritis |
Tap & inject ± early pars plana vitrectomy |
|
Grade C |
Visual acuity ≤light perception |
Immediate pars plana vitrectomy |
|
Grade D |
Orbital involvement |
Systemic intravenous therapy + surgical consult |
Key Clinical Points
- A universally standardized staging system does not yet exist, but severity-based classification is clinically useful.
- Visual acuity–based staging guides surgical decisions.
- More virulent organisms correlate with higher stages at presentation.
- Early intervention in Stage I–II dramatically improves prognosis.
- Stage V represents panophthalmitis and may require globe-sacrificing procedures.[2]
Prognosis
The prognosis of bacterial endophthalmitis is variable and hinges on several critical factors. Prompt diagnosis and treatment are paramount for improving outcomes, as delayed therapy can result in rapid deterioration of vision and irreversible ocular damage.
- Pathogen virulence: Infections caused by highly virulent organisms, such as Bacillus species and Pseudomonas aeruginosa, tend to have a poorer prognosis due to rapid progression and extensive ocular damage. Infections caused by Streptococcus pneumoniae are also associated with poor visual outcomes and higher rates of globe loss. Conversely, infections with less aggressive bacteria, such as coagulase-negative staphylococci, may have better visual outcomes with timely and appropriate treatment.[38][95]
- Initiation of therapy: The timing of intervention is crucial; early administration of appropriate intravitreal antibiotics is associated with more favorable visual outcomes.[96]
- Surgical intervention: The need for and timing of vitrectomy both play a role in prognosis. The EVS indicated that immediate vitrectomy benefits cases presenting with a loss of visual acuity to light perception only.[97]
- Host factors: The patient's immune status can significantly influence the prognosis. Immunocompromised individuals or those with diabetes may experience more severe infections and complications, leading to a worse prognosis. Older age has also been associated with poorer outcomes.
- Complications: The development of complications such as retinal detachment, persistent intraocular inflammation, or phthisis bulbi can lead to a poor visual prognosis. Certain clinical scenarios, including endogenous endophthalmitis and concurrent corneal ulceration, are associated with higher rates of evisceration or enucleation.[73]
- Visual acuity at presentation: Patients presenting with better initial visual acuity typically have a more favorable prognosis. Poor presenting visual acuity is one of the strongest predictors of severe outcomes, including the need for globe-sacrificing procedures.
- Rehabilitation potential: Access to and the effectiveness of rehabilitation services, including low-vision aids and occupational therapy, can maximize vision and improve quality of life post-infection.[98]
Despite advances in diagnosis and management, bacterial endophthalmitis remains a condition with a guarded prognosis. Multidisciplinary care involving ophthalmologists, infectious disease specialists, and rehabilitation services is essential for optimizing patient outcomes. Early recognition and aggressive management remain the most important modifiable factors influencing visual outcomes. Continuous research into novel therapeutic strategies and diagnostic tools is also critical to improve the prognostic outlook for this severe ocular infection.
Complications
The following complications pose a significant challenge in the management of bacterial endophthalmitis and may require additional interventions, including surgery. Early recognition and aggressive treatment are critical to minimize the risks.
- Permanent visual impairment: The most feared complication, from partial vision loss to complete blindness.[99]
- Retinal detachment: This complication occurs due to inflammation and traction on the retina, potentially requiring surgical repair.[100]
- Vitreous hemorrhage: Bleeding into the vitreous cavity can obscure vision and complicate infection management.[101]
- Corneal edema and opacification: Inflammation can lead to damage which may become permanent and require corneal transplantation.[102]
- Cystoid macular edema: Fluid accumulation in the macula can lead to distorted central vision.[103]
- Glaucoma: Increased intraocular pressure may develop acutely due to inflammatory debris or chronic trabecular meshwork damage.[104]
- Phthisis bulbi: Severe injury or disease may result in a shrunken, non-functional eye.[105]
- Choroidal effusion: Fluid accumulation in the choroidal space can lead to retinal detachment and decreased vision.[106]
- Endophthalmitis-related uveitis: An inflammatory response in the uveal tract can cause persistent discomfort and photophobia.[107]
- Ocular hypotony: Low intraocular pressure can occur due to ciliary body dysfunction or detachment.[108]
- Epiretinal membrane formation: Scar tissue over the retina can cause visual distortion.[109]
- Optic atrophy: Damage to the optic nerve from severe and prolonged inflammation leads to irreversible vision loss.[110]
- Proliferative vitreoretinopathy: Scar tissue formation can lead to retinal detachment and is challenging to treat.[111]
- Subretinal abscess formation: This complication can occur if the infection extends beyond the vitreous into the retinal tissue.[112]
- Sympathetic ophthalmia: A rare but severe immune-mediated condition affecting the non-infected eye.[113]
- Panophthalmitis: This complication is an extreme form of endophthalmitis that involves all layers and structures of the eye, leading to total loss of vision and a painful, non-functional eye that may necessitate enucleation.[114]
- Corneal ulcer: The infection may progress to involve the cornea, leading to ulceration. Corneal ulcers can be aggressive, leading to perforation and further spread of infection, and may require corneal grafting if structural integrity is compromised.[115]
- Orbital cellulitis: This infection spreads beyond the confines of the eye into the orbital tissues. Orbital cellulitis is a severe condition that can cause pain and swelling and lead to abscess formation, vision loss, and life-threatening complications if the infection spreads to the central nervous system.[102]
Postoperative and Rehabilitation Care
Postoperative Care
- Immediate postoperative period: Patients should be closely monitored for signs of improvement or worsening after intervention. Ocular pain, redness, discharge, and visual acuity should be assessed.
- Intravitreal antibiotics: Depending on the causative organism and the severity of the infection at presentation, follow-up doses may be necessary.
- Anti-inflammatory treatment: Corticosteroids, whether topical, periocular, or intravitreal, should be considered to reduce intraocular inflammation.
- Intraocular pressure monitoring: Patients are at risk for increased and decreased IOP, which should be managed accordingly.
- EVS guidelines: Adherence to EVS guidelines can inform decision-making regarding further surgical interventions, such as repeat vitrectomy.[66]
Rehabilitation Care
- Visual acuity rehabilitation: Low-vision aids and services may be necessary, and patients should be referred to a low-vision specialist for evaluation and management.
- Patient education: Patients should be educated about the symptoms of complications requiring urgent medical attention to ensure timely intervention.
- Psychosocial support: Endophthalmitis is a traumatic experience, and patients may benefit from counseling to cope with the potential loss of vision and the impact on quality of life.
- Physical rehabilitation: In cases with significant vision loss, orientation and mobility training may be needed to ensure patient safety and independence.
- Long-term follow-up: Regular ophthalmic examinations are crucial for monitoring late-onset complications such as cataract formation, retinal detachment, or glaucoma.[66]
The goal of providing comprehensive postoperative and rehabilitation care is to maximize the visual outcome for patients with bacterial endophthalmitis and ensure the best possible quality of life.
Consultations
Early and effective management of bacterial endophthalmitis necessitates a collaborative approach. The following consultations are recommended:
- Ophthalmology: Immediate consultation with a vitreoretinal specialist is paramount for managing suspected bacterial endophthalmitis. If the media are unclear, the ophthalmologist will perform a comprehensive ocular assessment, including slit-lamp examination, indirect ophthalmoscopy, and possibly B-scan ultrasonography.
- Infectious disease: This expertise is crucial for interpreting microbiological results and modifying antimicrobial therapy based on sensitivities and resistance patterns.
- Microbiology: Close collaboration is needed for the timely processing and interpretation of ocular samples. Microbiologists also provide valuable insights into local antibiotic resistance trends, which can inform empirical antibiotic choice.
- Internal or primary care: Coordination with the patient's primary care provider is essential for managing comorbid conditions that may affect treatment, such as diabetes or immunosuppression.
- Pharmacy: A clinical pharmacist can assist with antibiotic dosing, especially in patients with renal impairment, and provide information on drug interactions.
- Emergency medicine: In acute settings, consultations may be necessary for initial stabilization and assessment before definitive ophthalmological intervention.
- Anesthesiology: For patients requiring urgent surgical intervention, such as vitrectomy, consultation with an anesthesiologist is necessary for perioperative management.
- Rheumatology or immunology: Specialists provide valuable input in cases where immune-mediated reactions are suspected; they are also critical in managing steroid therapy in patients with pre-existing autoimmune diseases.[116]
In this interdisciplinary setup, clear communication and a well-coordinated care plan are vital to ensure prompt and effective treatment to preserve visual function and prevent complications. Regular multidisciplinary team meetings can facilitate this process, enabling a seamless flow of information and an integrated care pathway for patients with bacterial endophthalmitis.
Deterrence and Patient Education
Deterrence and patient education are crucial components in preventing and managing bacterial endophthalmitis. The following key points can be addressed in discussions with patients and caregivers.
- Understanding endophthalmitis: Educate patients about the seriousness of bacterial endophthalmitis, its causes, symptoms, and the importance of early detection and treatment.
- Preventive measures: Stress the importance of proper eye protection to prevent trauma, which is a significant risk factor for developing endophthalmitis. Discuss the role of meticulous perioperative antiseptic protocols for those undergoing ocular surgery and emphasize the need for proper contact lens hygiene to reduce the risk of infection.
- Early symptoms recognition: Instruct patients on recognizing early signs of infection, such as redness, pain, vision changes, or discharge, and the necessity of immediate medical attention.
- Postoperative care compliance: Ensure patients understand and adhere to postoperative care instructions following ocular surgery, including the use of prescribed antibiotic eye drops.
- Managing chronic conditions: Patients with chronic ocular surface diseases or those who use topical corticosteroids should be informed about their increased risk of endophthalmitis and the need for regular ophthalmic evaluations.
- Systemic health: Educate patients about the potential for endogenous endophthalmitis arising from systemic infections and the importance of managing systemic health conditions such as diabetes.
- Follow-up and monitoring: Reinforce the need for regular follow-up appointments to monitor for complications after ocular procedures or following the onset of symptoms suggestive of endophthalmitis.
- Patient empowerment: Encourage patients to be proactive in their eye health, including seeking prompt attention for eye injuries or when suspecting an infection.
Educating patients on these aspects aims to reduce the incidence of bacterial endophthalmitis and improve outcomes for those who develop the condition. Patient education should be reinforced by all team members involved in the patient's care.
Pearls and Other Issues
Clinical Pearls
- Early diagnosis: Rapid recognition of symptoms and signs is crucial for prompt treatment to prevent vision loss.
- Microbiological testing: Immediate collection of ocular samples for culture and sensitivity is essential for targeted therapy.
- Antibiotic selection: Empirical broad-spectrum intravitreal antibiotics are the first line of treatment until culture results guide antibiotic therapy.
- Inflammation control: Using corticosteroids to manage intraocular inflammation should be balanced against the risk of exacerbating infection.
- Vitrectomy: Early vitrectomy can benefit cases with dense vitritis by improving drug penetration and removing the infectious load.[116]
Management Challenges
- Resistance patterns: Awareness of local antimicrobial resistance patterns is important for selecting effective empirical therapy.
- Systemic infection: Investigating and managing potential sources of endogenous infection is essential.
- Visual prognosis: Patients should be counseled regarding the potential outcomes and prognosis.
- Therapeutic window: Recognition of the narrow therapeutic window is critical for preserving vision.
- Follow-up: Frequent monitoring and follow-up are required to adjust treatment based on the clinical response and laboratory findings.[117]
Other Issues
- Prevention: Implement strategies in surgical practice to minimize the risk of postoperative endophthalmitis.
- Patient education: Educate patients on the signs of endophthalmitis for early detection, especially after ocular procedures.
- Post-traumatic considerations: Ensure awareness of the special considerations for post-traumatic endophthalmitis, such as the presence of intraocular foreign bodies.
- Multidisciplinary approach: Collaboration with microbiologists, infectious disease specialists, and internists is necessary for complex cases.
- Research advances: Clinicians should keep abreast of advances in diagnostic and therapeutic techniques, including molecular diagnostics and newer antimicrobial agents.[118]
Enhancing Healthcare Team Outcomes
Bacterial endophthalmitis is a time-sensitive ophthalmic emergency that requires rapid diagnosis, coordinated intervention, and meticulous follow-up. Optimal patient outcomes depend not only on the ophthalmologist but also on effective collaboration among a multidisciplinary healthcare team.[3] Structured communication, standardized protocols, early recognition pathways, and coordinated systemic evaluation significantly improve visual prognosis and reduce morbidity.[5]
Interprofessional Team Roles
Effective management requires coordinated input from multiple professionals (see Table 34).[53]
Table 34. Interdisciplinary Team Roles in Managing Bacterial Endophthalmitis
|
Team Member |
Role in Management |
Impact on Outcomes |
|
Ophthalmologist (retina specialist) |
Diagnosis, intravitreal antibiotics, pars plana vitrectomy |
Primary determinant of visual outcome |
|
Emergency physician |
Early recognition and urgent referral |
Reduces delay to treatment |
|
Nursing staff |
Medication preparation, aseptic technique |
Prevents dosing errors and infection spread |
|
Microbiologist |
Culture processing, antibiotic sensitivity |
Guides targeted therapy |
|
Infectious disease specialist |
Systemic management (endogenous cases) |
Improves systemic control |
|
Pharmacist |
Accurate dilution of intravitreal antibiotics |
Prevents retinal toxicity |
|
Radiologist |
Computed tomography imaging in trauma/endogenous cases |
Identifies intraocular foreign body or abscess |
|
Primary care/hospitalist |
Management of comorbidities |
Reduces recurrence risk |
Time-to-Treatment Optimization
Studies consistently demonstrate that a shorter time from symptom onset to intravitreal antibiotic administration correlates with improved visual outcomes (see Image. Rapid Response Algorithm for Bacterial Endophthalmitis). Therefore, the multidisciplinary team should:
- Establish institutional rapid-response protocols.
- Implement emergency triage pathways for postoperative patients.
- Educate staff to treat “red eye + decreased vision post-surgery” as an emergency.[6]
Standardized Clinical Protocols
Hospitals should implement standardized protocols, including:
- Pre-filled intravitreal antibiotic kits
- Dosing checklists to prevent dilution errors
- Emergency access to B-scan ultrasonography
- Clear EVS-based surgical decision guidelines
- Infection control checklists for intravitreal injections
- Standardization reduces medical errors and improves safety [8]
Communication and Documentation
Clear documentation improves continuity of care:
- Record presenting visual acuity (prognostic marker).
- Document the time of symptom onset.
- Record time antibiotics administered.
- Communicate culture results promptly.
- Document systemic findings in endogenous cases.
Interdepartmental communication is especially critical in endogenous endophthalmitis.[58]
Preventive Team Strategies
Surgical prevention
- Intracameral antibiotic prophylaxis during cataract surgery
- Strict sterile technique
- Mask usage during intravitreal injections
- Avoid talking during injections [25]
Patient education
Patients should be instructed to immediately report:
- Sudden vision decrease
- Increasing pain
- Redness after surgery/injection
- Early self-reporting: improves prognosis [6]
Quality Improvement Measures
Healthcare institutions can enhance outcomes through various quality improvement methods (see Table 35).
Table 35. Quality Improvement Strategies for Bacterial Endophthalmitis
|
Strategy |
Outcome Benefit |
|
Routine audit of surgical infection rates |
Early identification of trends |
|
Injection room sterility protocols |
Reduced post-injection cases |
|
Antibiotic dilution training programs |
Prevent toxicity |
|
Postoperative follow-up call systems |
Early symptom detection |
|
Multidisciplinary case reviews |
Continuous improvement |
Managing Endogenous Endophthalmitis
For endogenous cases, coordination between ophthalmology and systemic care teams is essential. Failure to manage the systemic source increases the risk of mortality (see Image. Managing Endogenous Bacterial Endophthalmitis).
Patient Safety Considerations
Key safety practices include:
- Double-check intravitreal drug preparation
- Avoid aminoglycosides if safer alternatives exist
- Monitor IOP after steroid use
- Educate patients on warning signs
- Immediate reassessment if vision worsens [13]
Outcome Metrics for Healthcare Systems
Hospitals can monitor several metrics to ensure optimized care (see Table 36).
Table 36. Healthcare System Outcome Metrics for Bacterial Endophthalmitis
|
Metric |
Goal |
|
Time from presentation to antibiotic injection |
<2 hours |
|
Post-cataract infection rate |
<0.1% |
|
Injection-related infection rate |
<0.05% |
|
Rate of medication preparation errors |
Zero tolerance |
|
Percentage of patients achieving ≥20/40 |
Continuous improvement |
Long-Term Follow-Up and Rehabilitation
Patients recovering from endophthalmitis may require:
- Cataract surgery
- Retinal detachment repair
- Low vision rehabilitation
- Psychological support for vision loss
Involving rehabilitation specialists improves quality-of-life outcomes.[6]
Key Points for Enhancing Outcomes
- Rapid recognition and immediate treatment are critical.
- Interdisciplinary coordination improves both ocular and systemic outcomes.
- Standardized antibiotic protocols prevent toxicity.
- Preventive surgical measures reduce the incidence of bacterial endophthalmitis.
- Quality audits and education sustain long-term improvements.[9]
Summary
Improving outcomes in bacterial endophthalmitis requires a coordinated, protocol-driven, and interprofessional approach. Timely diagnosis, standardized treatment pathways, multidisciplinary communication, and continuous quality improvement initiatives significantly enhance visual prognosis and patient safety. Prevention strategies and patient education further reduce disease burden and healthcare costs.[3]
Media
(Click Image to Enlarge)
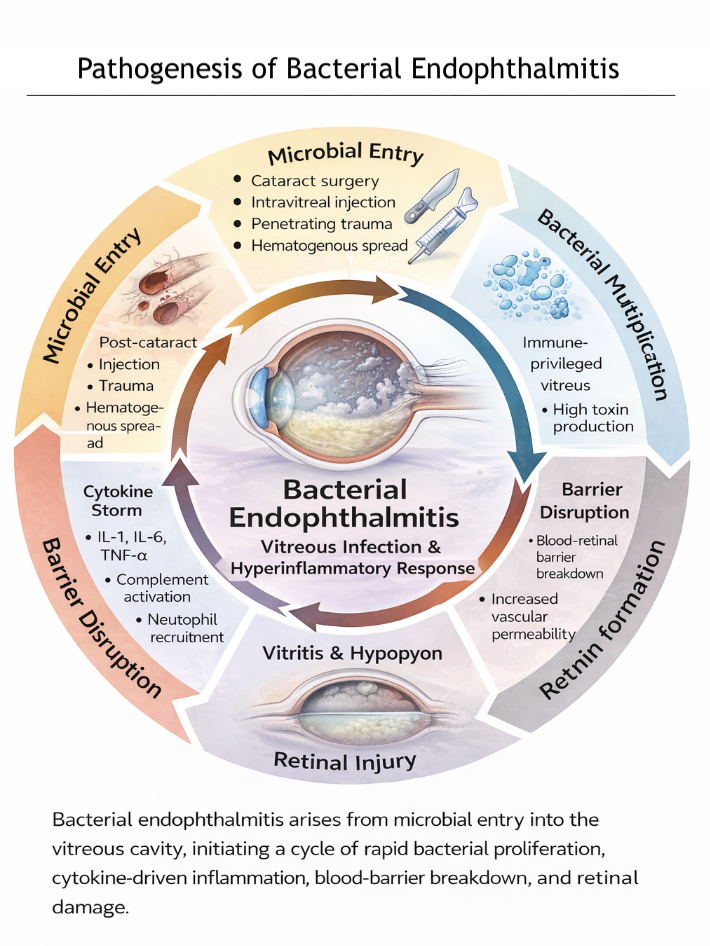
Pathogenesis of Bacterial Endophthalmitis. Infographic illustrating microbial entry (post-cataract surgery, intravitreal injection, penetrating trauma, hematogenous spread), rapid bacterial proliferation within the vitreous, cytokine-mediated inflammation, blood-retinal barrier disruption, and progression to vitritis, hypopyon, and retinal injury.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
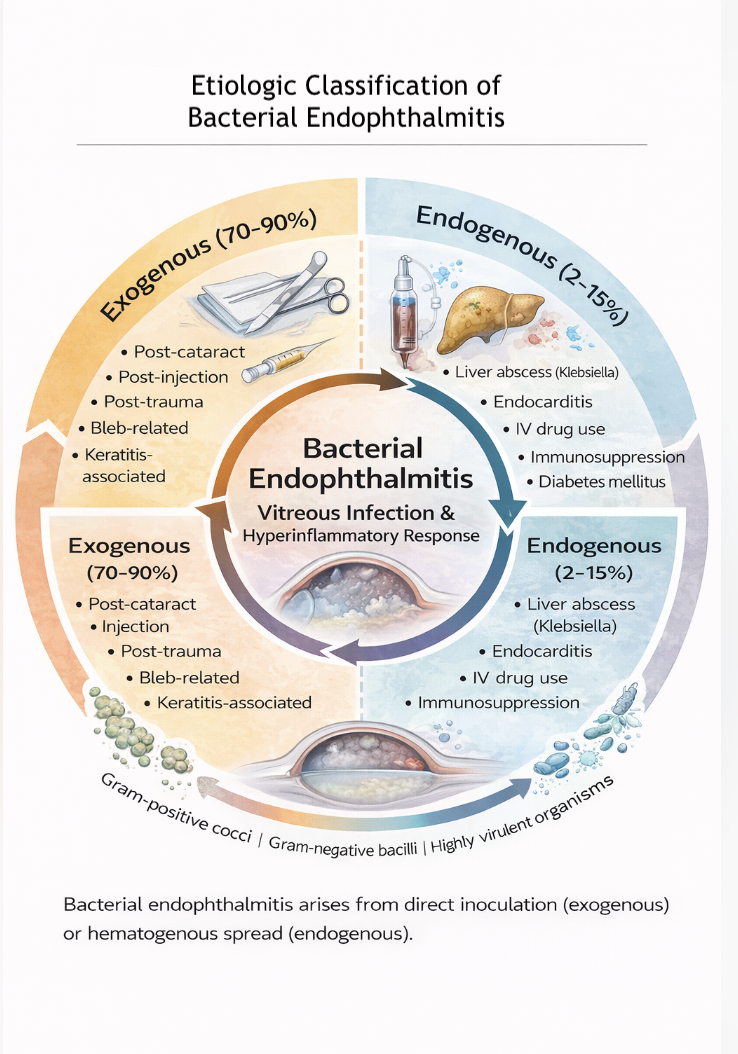
Etiologic Classification of Bacterial Endophthalmitis. Infographic distinguishing exogenous (postoperative, postinjection, post-traumatic, bleb-related, keratitis-associated) and endogenous (hematogenous spread from systemic infection) sources, with representative risk factors and common causative organisms.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
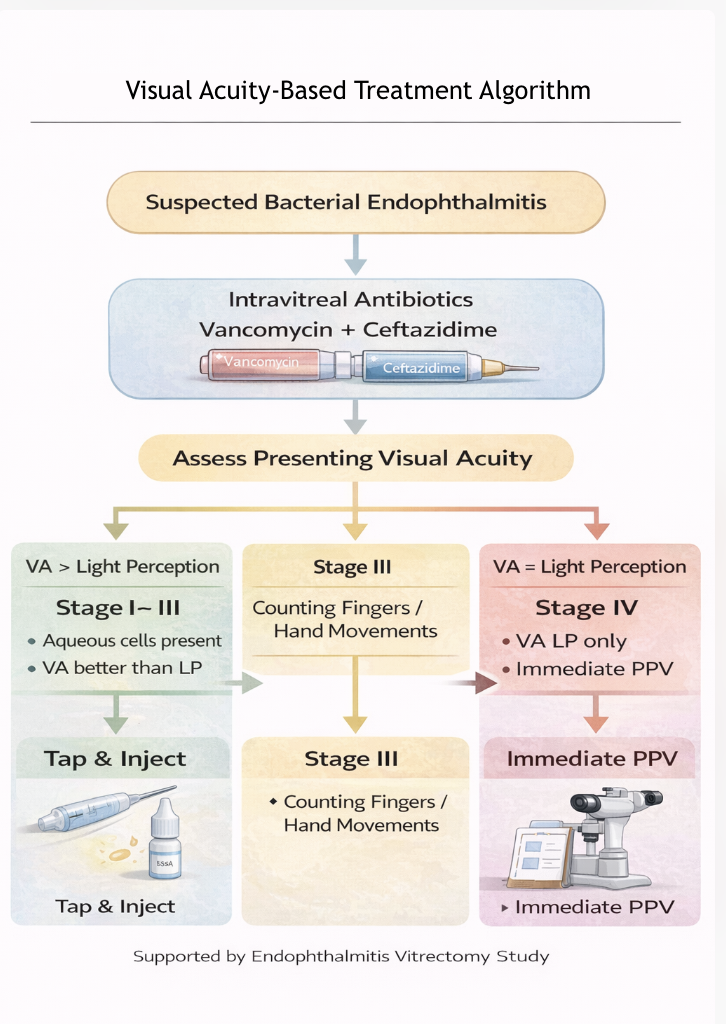
Visual Acuity–Based Treatment Algorithm for Bacterial Endophthalmitis. Flowchart outlining initial intravitreal antibiotic therapy (vancomycin plus ceftazidime) followed by management stratified by presenting visual acuity, including tap-and-inject approaches for better vision and immediate pars plana vitrectomy for light perception–only vision.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
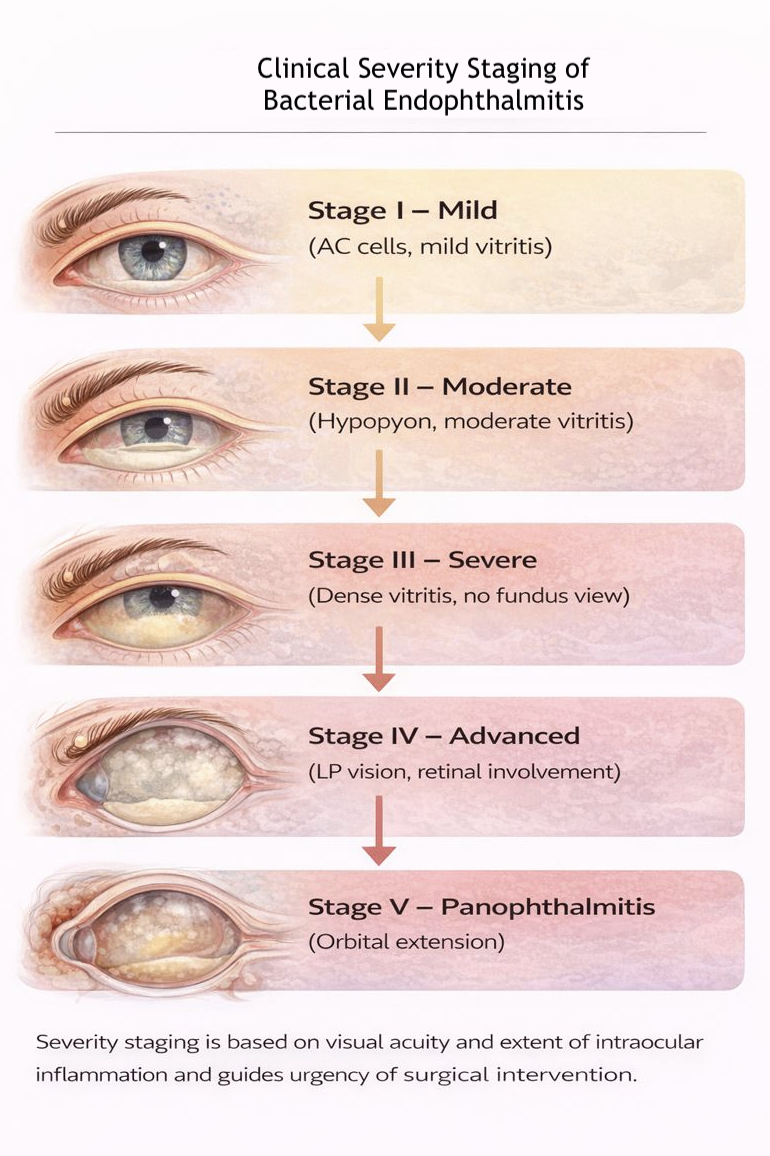
Clinical Severity Staging of Bacterial Endophthalmitis. Infographic depicting progression from mild anterior chamber inflammation to moderate hypopyon, severe vitritis with obscured fundus, advanced disease with light perception vision and retinal involvement, and panophthalmitis with orbital extension.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
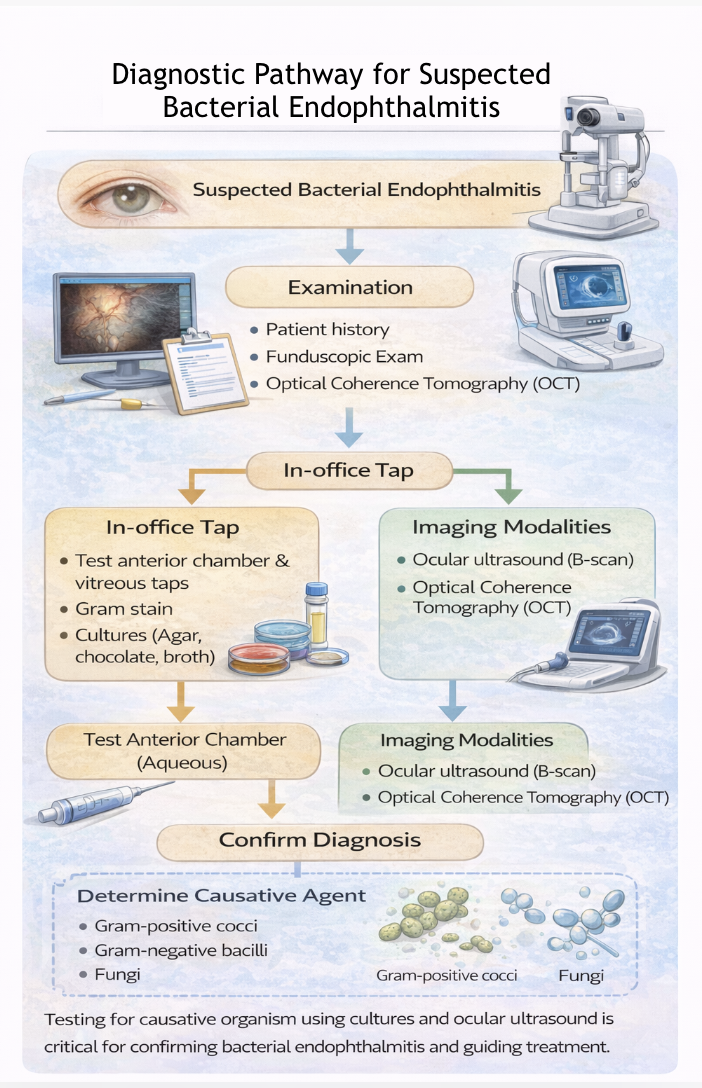
Diagnostic Pathway for Suspected Bacterial Endophthalmitis. Flowchart illustrating clinical evaluation, anterior chamber and vitreous sampling for Gram stain and culture, adjunctive imaging with ocular ultrasound and optical coherence tomography, and identification of causative organisms to guide targeted therapy.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
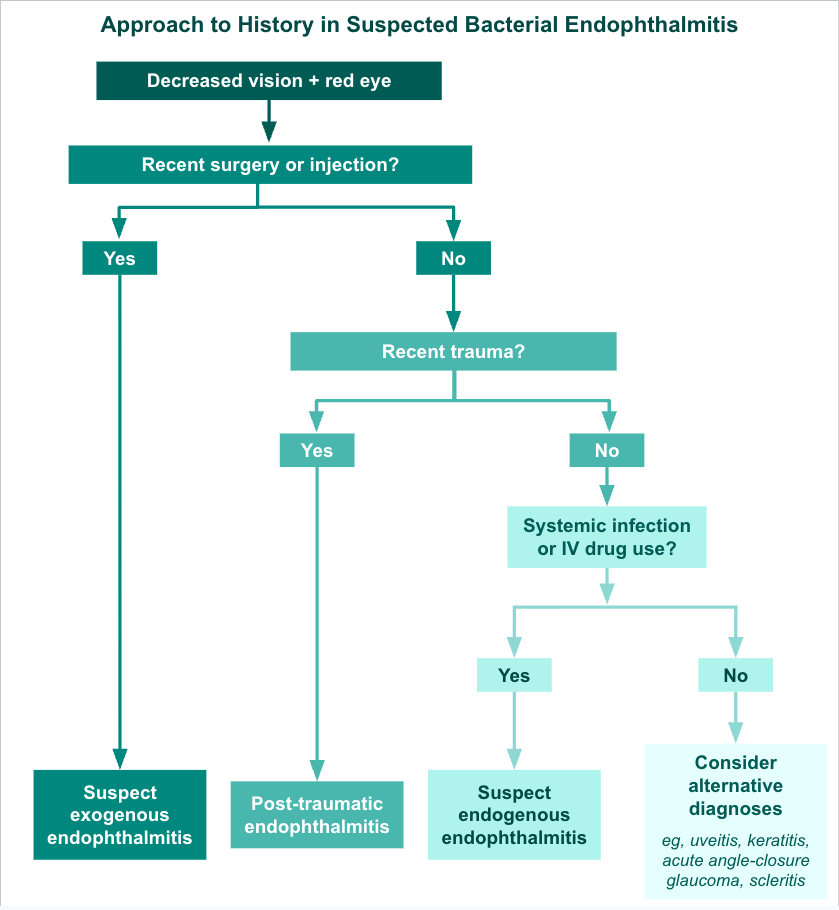
Approach to History in Suspected Bacterial Endophthalmitis. Flowchart outlining a structured history-taking approach for patients presenting with decreased vision and red eye, incorporating recent surgery or intravitreal injection, ocular trauma, and systemic infection or intravenous drug use to differentiate exogenous, post-traumatic, and endogenous endophthalmitis.
Contributed by M Horiates Kerekes, MD
(Click Image to Enlarge)
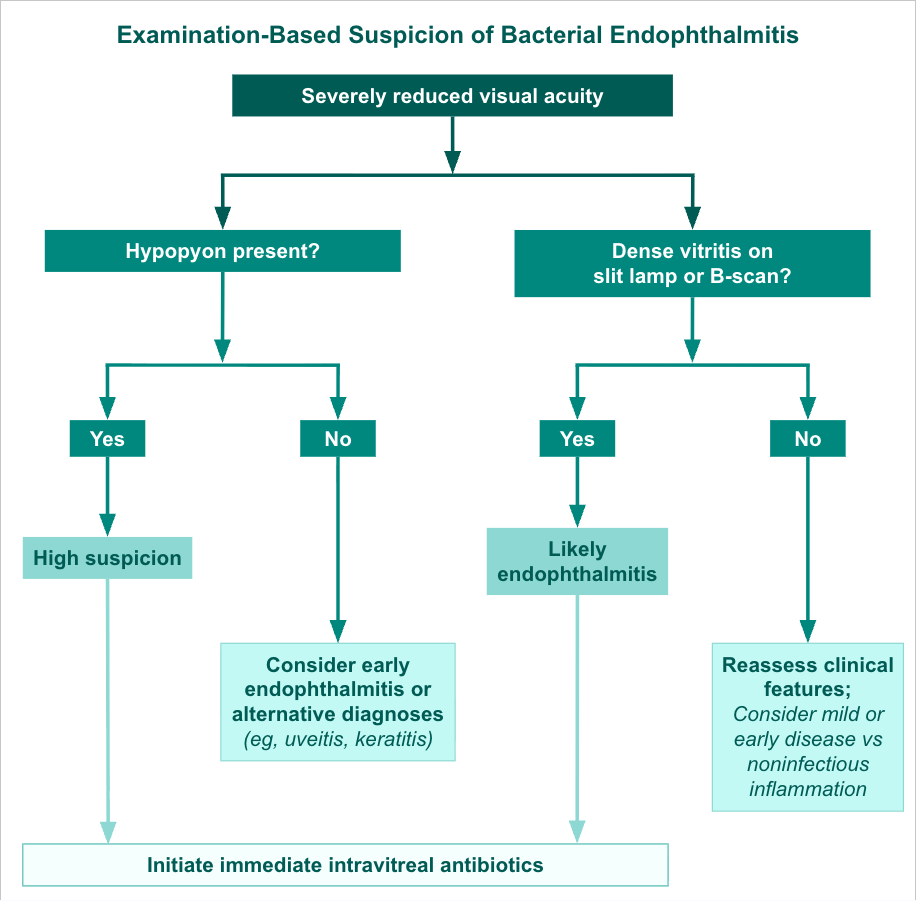
Examination-Based Suspicion of Bacterial Endophthalmitis. Flowchart illustrating an examination-based approach to suspected bacterial endophthalmitis in patients with severely reduced visual acuity and high clinical suspicion, using key findings such as hypopyon and dense vitritis on slit-lamp examination or B-scan to stratify likelihood and guide prompt initiation of intravitreal antibiotics while considering early disease or alternative diagnoses when findings are absent.
Contributed by M Horiates Kerekes, MD
(Click Image to Enlarge)
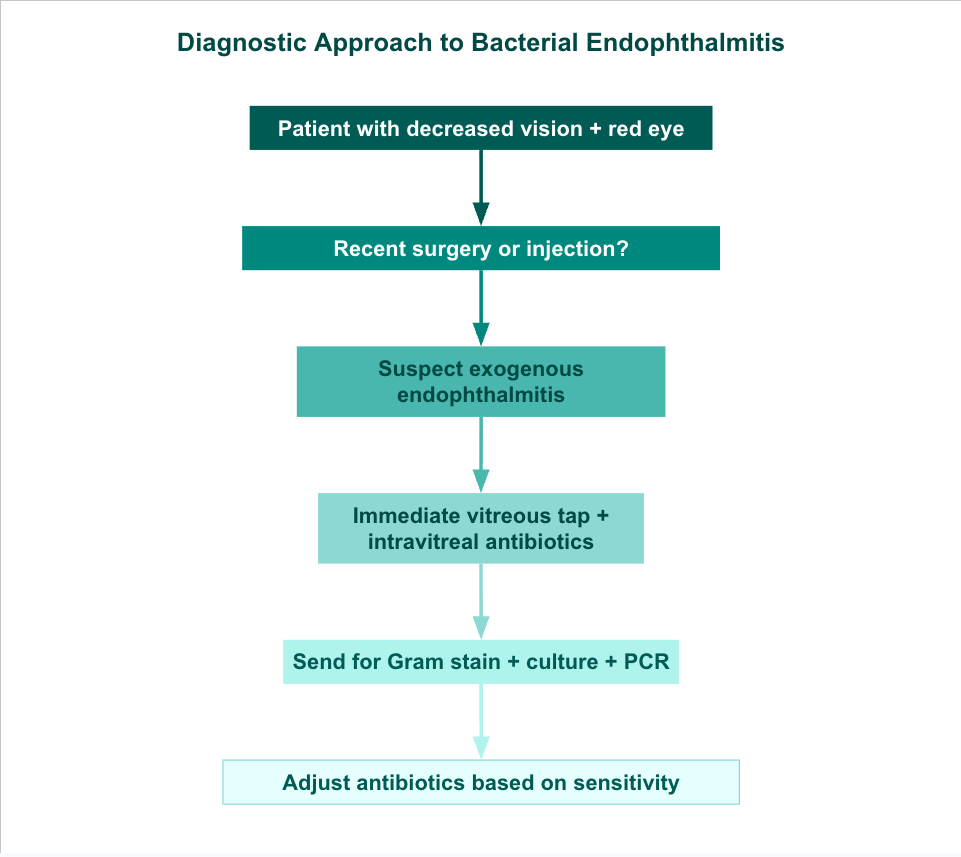
Diagnostic Approach to Bacterial Endophthalmitis. Flowchart outlining the stepwise evaluation and initial management of patients presenting with decreased vision and red eye, emphasizing identification of recent intraocular procedures to suspect exogenous endophthalmitis, prompt vitreous sampling with intravitreal antibiotic administration, microbiologic testing with Gram stain, culture, and polymerase chain reaction, and subsequent antibiotic adjustment based on organism identification and sensitivity results.
Contributed by M Horiates Kerekes, MD
(Click Image to Enlarge)
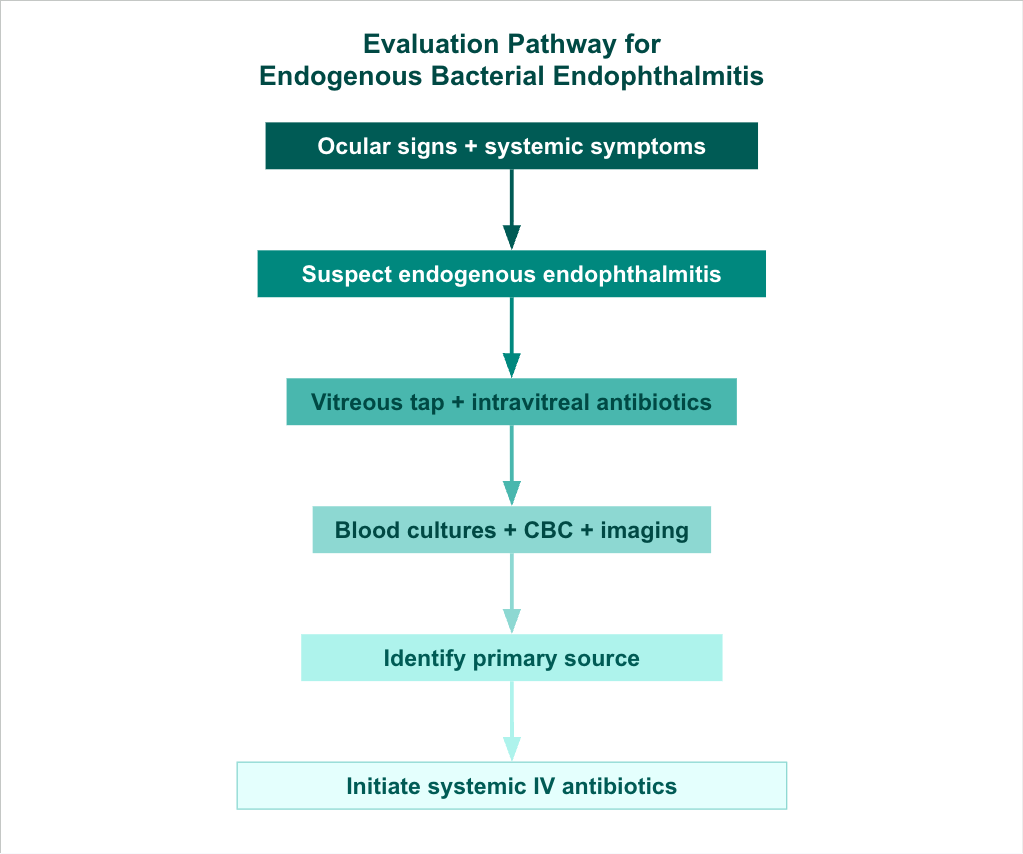
Evaluation Pathway for Endogenous Bacterial Endophthalmitis. Flowchart outlining the diagnostic and management approach for suspected endogenous bacterial endophthalmitis in patients with ocular findings and systemic symptoms, including prompt vitreous sampling with intravitreal antibiotic administration, systemic evaluation with blood cultures, laboratory testing, and imaging, identification of the primary infectious source, and initiation of targeted intravenous antibiotic therapy.
Contributed by M Horiates Kerekes, MD
(Click Image to Enlarge)
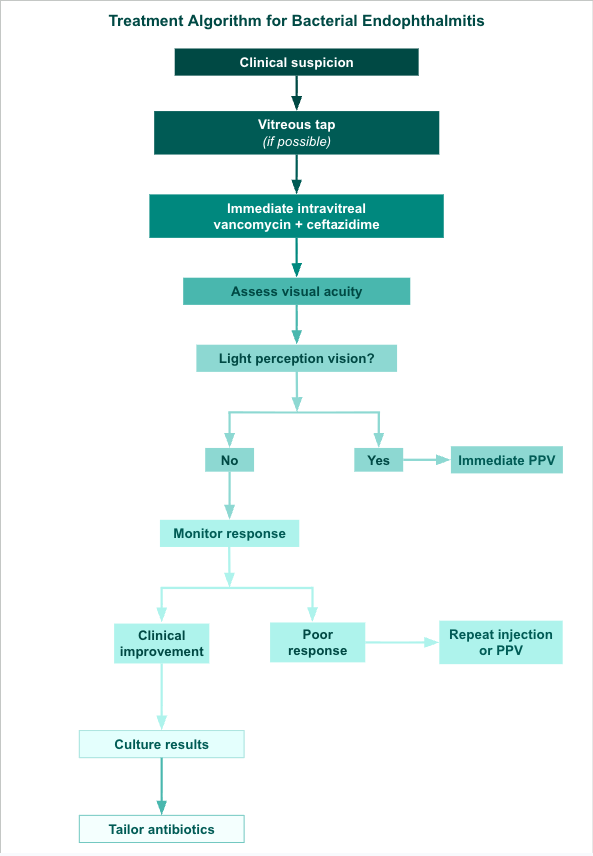
Treatment Algorithm for Bacterial Endophthalmitis. Flowchart outlining the stepwise management of suspected bacterial endophthalmitis, including initial vitreous sampling when feasible, immediate intravitreal antibiotic administration with vancomycin and ceftazidime, visual acuity–based stratification to guide early pars plana vitrectomy, and subsequent management based on clinical response and microbiologic results, with escalation to repeat injection or surgery for poor response and targeted antibiotic therapy following culture identification.
Contributed by M Horiates Kerekes, MD
(Click Image to Enlarge)
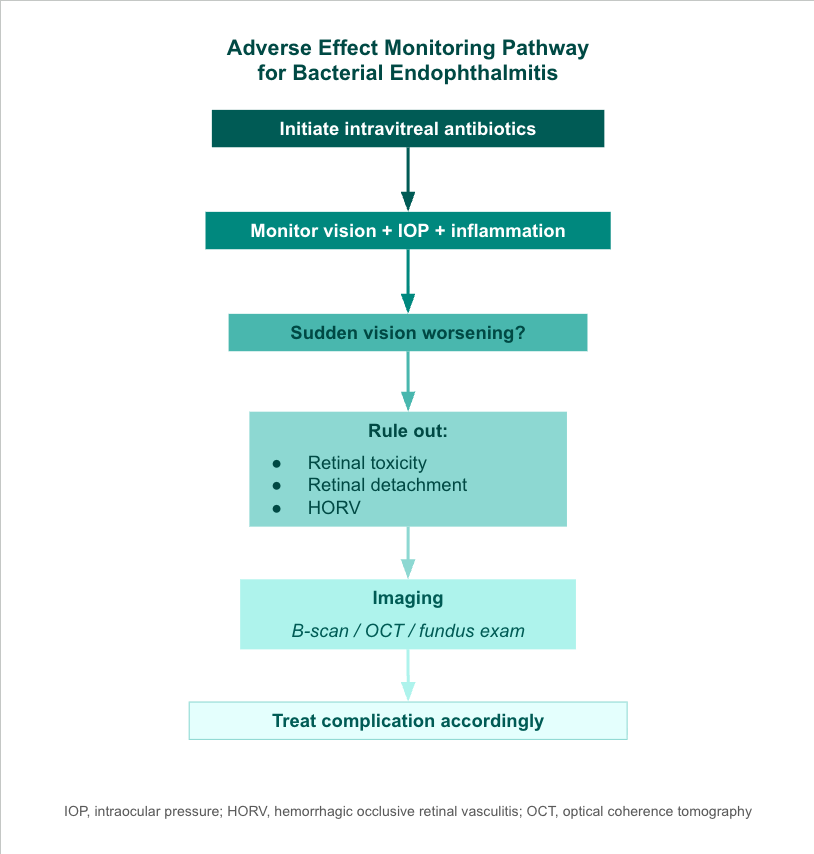
Adverse Effect Monitoring Pathway for Bacterial Endophthalmitis. Flowchart outlining the posttreatment monitoring and evaluation of patients receiving intravitreal antibiotics for bacterial endophthalmitis, emphasizing serial assessment of vision, intraocular pressure, and inflammation, recognition of acute vision worsening, targeted evaluation for complications such as retinal toxicity, retinal detachment, and hemorrhagic occlusive retinal vasculitis, and the use of imaging modalities to guide timely, complication-specific management.
Contributed by M Horiates Kerekes, MD
(Click Image to Enlarge)
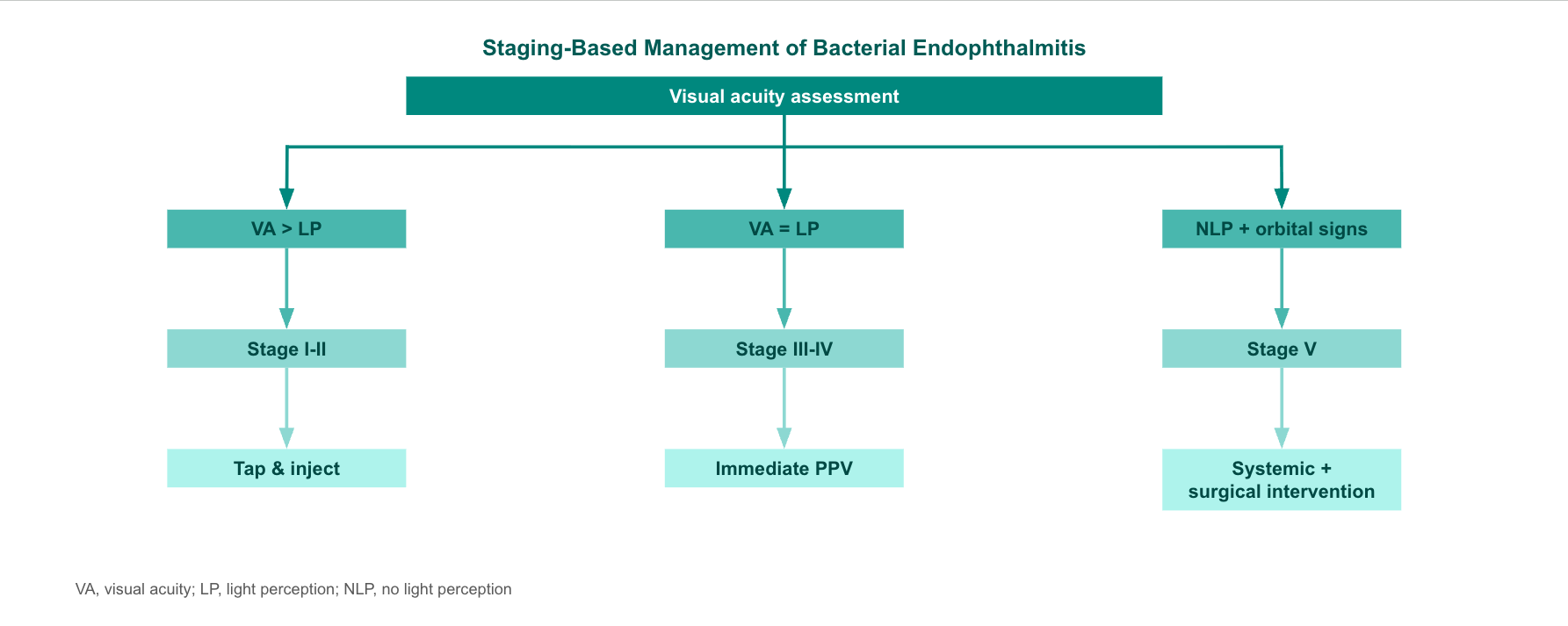
Staging-Based Management of Bacterial Endophthalmitis. Flowchart outlining management stratified by presenting visual acuity in bacterial endophthalmitis, with patients maintaining vision better than light perception managed with vitreous tap and intravitreal antibiotics, those with light perception vision requiring immediate pars plana vitrectomy, and advanced cases with no light perception and orbital involvement necessitating systemic therapy and surgical intervention.
Contributed by M Horiates Kerekes, MD
(Click Image to Enlarge)
Rapid Response Algorithm for Bacterial Endophthalmitis. Flowchart outlining the urgent initial management of patients presenting with red eye and vision loss, emphasizing immediate triage as an ocular emergency, prompt ophthalmology consultation, rapid vitreous sampling with intravitreal antibiotic administration, and close daily follow-up to monitor clinical response and guide further management.
Contributed by M Horiates Kerekes, MD
(Click Image to Enlarge)
Managing Endogenous Bacterial Endophthalmitis. Flowchart outlining the coordinated diagnostic and management approach for endogenous bacterial endophthalmitis, including confirmation of ocular involvement, systemic evaluation with blood cultures and imaging, identification of the primary infectious source, initiation of intravenous antibiotic therapy, and implementation of source control measures such as abscess drainage or catheter removal to optimize outcomes.
Contributed by M Horiates Kerekes, MD
References
Das T, Joseph J, Simunovic MP, Grzybowski A, Chen KJ, Dave VP, Sharma S, Staropoli P, Flynn H Jr. Consensus and controversies in the science of endophthalmitis management: Basic research and clinical perspectives. Progress in retinal and eye research. 2023 Nov:97():101218. doi: 10.1016/j.preteyeres.2023.101218. Epub 2023 Oct 12 [PubMed PMID: 37838286]
Level 3 (low-level) evidenceKang H, Wang Y, Xin L, Jia J, Fan Y, Han S, Liu F, Qi S, Sun S, Yue Z, Huo T, Xu J, Li S, Zhang Y. Integrated analysis of risk factors, visual prognosis, and pathogens in pediatric post-traumatic endophthalmitis: a retrospective cohort study. Frontiers in medicine. 2026:13():1699901. doi: 10.3389/fmed.2026.1699901. Epub 2026 Jan 22 [PubMed PMID: 41658598]
Level 2 (mid-level) evidenceMoon M, Mathews S, Mahjabin F, Karaiskos K, Libre PE. Failure of endophthalmitis prophylaxis: laboratory model comparing antibiotics and bacterial loads. Journal of cataract and refractive surgery. 2026 Jun 1:52(6):602-606. doi: 10.1097/j.jcrs.0000000000001892. Epub [PubMed PMID: 41642980]
Zheng K, Zheng X, Gan D, Zhou X. Successful antibiotic management of Staphylococcus epidermidis endophthalmitis after implantable collamer lens implantation. BMC ophthalmology. 2023 Oct 12:23(1):410. doi: 10.1186/s12886-023-03127-5. Epub 2023 Oct 12 [PubMed PMID: 37828437]
Yan Y, Li F, Huang T, Cheng Y, Liao Y, Liu H. Intraocular infection of Moraxella nonliquefaciens accompanied by secondary angle-closure glaucoma: A case report. The Journal of international medical research. 2026 Jan:54(1):3000605251411736. doi: 10.1177/03000605251411736. Epub 2026 Jan 31 [PubMed PMID: 41618766]
Level 3 (low-level) evidenceAther M, Conrady CD. Emerging Ocular Pathogen Resistance and Clinically Used Solutions: A Problem That Is More than Meets the Eye. Pharmaceuticals (Basel, Switzerland). 2025 Dec 23:19(1):. doi: 10.3390/ph19010031. Epub 2025 Dec 23 [PubMed PMID: 41599633]
Aloqab A, Semidey VA. Postoperative Aspergillus Endophthalmitis With Iris Granuloma: A Case Report. Cureus. 2023 Sep:15(9):e44945. doi: 10.7759/cureus.44945. Epub 2023 Sep 9 [PubMed PMID: 37818509]
Level 3 (low-level) evidenceQuin-Sánchez A, Roche-Fernández K, Campos-Figueroa P, Vazquez-Dorrego X, Sabala-Llopart A, Jarroudi RB, Valentín-Bravo J, Broc Iturralde L. Silicone Punctal Plugs as a Significant Risk Factor for Iatrogenic Endophthalmitis: A Case Report. Ocular immunology and inflammation. 2026 Feb:34(2):428-431. doi: 10.1080/09273948.2026.2613092. Epub 2026 Jan 18 [PubMed PMID: 41548097]
Level 3 (low-level) evidenceHe J, Ma H, Zhang Y, Huang D, Zhou Z, Cheng M, Wang L, Piao Y, Hao X. An injectable dual-drug-loaded hydrogel for the treatment of bacterial endophthalmitis. Biomaterials advances. 2026 May:182():214704. doi: 10.1016/j.bioadv.2026.214704. Epub 2026 Jan 4 [PubMed PMID: 41512470]
Level 3 (low-level) evidenceDurand ML. Bacterial and Fungal Endophthalmitis. Clinical microbiology reviews. 2017 Jul:30(3):597-613. doi: 10.1128/CMR.00113-16. Epub [PubMed PMID: 28356323]
Li XL, Zhang XL, Han JJ, Wan X, Ding HF, Chen HL. [Etiological characteristics, clinical manifestations, and prognosis of patients with endogenous endophthalmitis in 2024: a single-center retrospective cohort study]. [Zhonghua yan ke za zhi] Chinese journal of ophthalmology. 2026 Jan 11:62(1):41-51. doi: 10.3760/cma.j.cn112142-20250403-00170. Epub [PubMed PMID: 41491511]
Level 2 (mid-level) evidenceWisniewski P, Becker YA, Larson DT, Blaylock JM, Butler FK Jr, Cybulski RJ, Deaton TG, Donovan KA, Graf PCF, King JR, Lewandowski LR, Maves R, Neading R, O'Shea MK, Ressner RA, Wallace JD, Weymouth WL, Murray CK. Antibiotics in Tactical Combat Casualty Care 2025: TCCC Change 25-1. Journal of special operations medicine : a peer reviewed journal for SOF medical professionals. 2025 Dec 1:25(4):85-93. doi: 10.55460/SW7X-X8ZP. Epub [PubMed PMID: 41474877]
Kaleem S, Mihalache A, Golrokhian-Sani AA, Lai A, Zajner C, Popovic MM, Kaleem S, Kertes PJ, Muni RH, Wong DT. The association between treatment method, microbiological findings, and visual acuity in endophthalmitis patients: A retrospective, multi-centred study. Eye (London, England). 2026 Feb:40(3):406-411. doi: 10.1038/s41433-025-04125-1. Epub 2025 Dec 19 [PubMed PMID: 41419596]
Level 2 (mid-level) evidenceThompson KN, Alshaikhsalama AM, Wang AL. Evaluation of the Clinical Course of Endogenous Endophthalmitis. Journal of vitreoretinal diseases. 2023 Sep-Oct:7(5):389-396. doi: 10.1177/24741264231191344. Epub 2023 Aug 18 [PubMed PMID: 37706078]
Gurnani B, Kaur K. Inflammatory cytokines in tears of patients with lacrimal duct obstruction. The Indian journal of medical research. 2023 Sep:158(3):317. doi: 10.4103/ijmr.ijmr_1487_22. Epub [PubMed PMID: 37815066]
Gurnani B, Kaur K. Successful management of delayed hyaluronidase hypersensitivity after subtenon's anesthesia during the COVID-19 pandemic: A rare case report. Indian journal of pharmacology. 2023 Jan-Feb:55(1):59-61. doi: 10.4103/ijp.ijp_995_21. Epub [PubMed PMID: 36960522]
Level 3 (low-level) evidenceMorya AK, Ramesh PV, Kaur K, Gurnani B, Heda A, Bhatia K, Sinha A. Diabetes more than retinopathy, it's effect on the anterior segment of eye. World journal of clinical cases. 2023 Jun 6:11(16):3736-3749. doi: 10.12998/wjcc.v11.i16.3736. Epub [PubMed PMID: 37383113]
Level 3 (low-level) evidenceGurnani B, Christy J, Kaur K, Moutappa F, Gubert J. Successful Management of Pythium insidiosum Keratitis Masquerading as Dematiaceous Fungal Keratitis in an Immunosuppressed Asian Male. Ocular immunology and inflammation. 2024 Jul:32(5):583-586. doi: 10.1080/09273948.2023.2179495. Epub 2023 Feb 22 [PubMed PMID: 36812410]
Gurnani B, Kaur K. Contact Lens–Related Complications. StatPearls. 2026 Jan:(): [PubMed PMID: 36512659]
Callegan MC, Engelbert M, Parke DW 2nd, Jett BD, Gilmore MS. Bacterial endophthalmitis: epidemiology, therapeutics, and bacterium-host interactions. Clinical microbiology reviews. 2002 Jan:15(1):111-24 [PubMed PMID: 11781270]
Level 3 (low-level) evidenceRelhan N, Forster RK, Flynn HW Jr. Endophthalmitis: Then and Now. American journal of ophthalmology. 2018 Mar:187():xx-xxvii. doi: 10.1016/j.ajo.2017.11.021. Epub 2017 Dec 5 [PubMed PMID: 29217351]
Uner OE, Lee D, Horesh R, Jewart B, Seebruck C. Lowering the Incidence of Endophthalmitis Following Intravitreal Anti-VEGF Injection: An Analysis of Aseptic Protocol Adjustment. Ophthalmic surgery, lasers & imaging retina. 2023 Sep:54(9):520-525. doi: 10.3928/23258160-20230808-01. Epub 2023 Aug 1 [PubMed PMID: 37642415]
Kelkar AS, Sharma N, Verma L, Chandorkar SA, Saxena R, Mishra D, Kelkar JA, Sengupta S. Antibiotic prophylaxis for cataract surgery - Practice patterns amongst Indian Ophthalmologists. Indian journal of ophthalmology. 2023 Sep:71(9):3235-3241. doi: 10.4103/IJO.IJO_702_23. Epub [PubMed PMID: 37602614]
Rudraprasad D, Gandhi J, Naik P, N Naik M, Naidu C, Kumar Mishra D, Joseph J. A Novel and Low-cost Approach for Intravitreal Injection in an Experimental Model of Endophthalmitis. Journal of ophthalmic & vision research. 2023 Jul-Sep:18(3):272-282. doi: 10.18502/jovr.v18i3.13775. Epub 2023 Jul 28 [PubMed PMID: 37600911]
Shanks RMQ, Romanowski EG, Patel DR, Kadouri DE. Eying up predatory bacteria: living antimicrobials for ocular infections. Current opinion in ophthalmology. 2026 May 1:37(3):244-250. doi: 10.1097/ICU.0000000000001200. Epub 2025 Dec 1 [PubMed PMID: 41330426]
Level 3 (low-level) evidenceSiatkowski RM, Morse CL, Gold RS, Li C, Peng X, Lum F. Major Complications following Strabismus Surgery: Nine-year Data from the IRIS® Registry. Ophthalmology. 2026 Apr:133(4):495-498. doi: 10.1016/j.ophtha.2025.11.007. Epub 2025 Nov 28 [PubMed PMID: 41320133]
Kutlu Uzakgider N, Karaca Adiyeke S. Cefuroxime-related hemorrhagic retinal vasculitis following cataract surgery. BMC ophthalmology. 2025 Nov 25:25(1):662. doi: 10.1186/s12886-025-04479-w. Epub 2025 Nov 25 [PubMed PMID: 41291565]
Abouammoh MA, Younis AS, Alsulaiman SM, Nazer R, Al-Salem R, AlBloushi AF, Almousa AN, AlBalawi ED, Arévalo JF. Visual and Anatomical Outcomes of Microbial Keratitis-Induced Endophthalmitis. Ocular immunology and inflammation. 2025 Dec:33(10):2463-2468. doi: 10.1080/09273948.2025.2584588. Epub 2025 Nov 10 [PubMed PMID: 41213074]
Osei Duah Junior I, Ampong J, Danquah CA. Mechanisms and Evolution of Antimicrobial Resistance in Ophthalmology: Surveillance, Clinical Implications, and Future Therapies. Antibiotics (Basel, Switzerland). 2025 Nov 20:14(11):. doi: 10.3390/antibiotics14111167. Epub 2025 Nov 20 [PubMed PMID: 41301664]
He X, Luo M, Ran J, He H, Wang Y. A case of panophthalmitis with orbital infection of polymicrobial origin. BMC infectious diseases. 2025 Nov 7:25(1):1526. doi: 10.1186/s12879-025-11988-y. Epub 2025 Nov 7 [PubMed PMID: 41204199]
Level 3 (low-level) evidenceValdez-García JE, Climent A, Chávez-Mondragón E, Lozano-Ramírez JF. Anterior chamber bacterial contamination in cataract surgery. BMC ophthalmology. 2014 Apr 30:14():57. doi: 10.1186/1471-2415-14-57. Epub 2014 Apr 30 [PubMed PMID: 24885986]
Srinivasan R, Tiroumal S, Kanungo R, Natarajan MK. Microbial contamination of the anterior chamber during phacoemulsification. Journal of cataract and refractive surgery. 2002 Dec:28(12):2173-6 [PubMed PMID: 12498855]
Lundström M, Wejde G, Stenevi U, Thorburn W, Montan P. Endophthalmitis after cataract surgery: a nationwide prospective study evaluating incidence in relation to incision type and location. Ophthalmology. 2007 May:114(5):866-70 [PubMed PMID: 17324467]
Wiskur BJ, Hunt JJ, Callegan MC. Hypermucoviscosity as a virulence factor in experimental Klebsiella pneumoniae endophthalmitis. Investigative ophthalmology & visual science. 2008 Nov:49(11):4931-8. doi: 10.1167/iovs.08-2276. Epub 2008 Jun 27 [PubMed PMID: 18586871]
Level 3 (low-level) evidenceCallegan MC, Kane ST, Cochran DC, Novosad B, Gilmore MS, Gominet M, Lereclus D. Bacillus endophthalmitis: roles of bacterial toxins and motility during infection. Investigative ophthalmology & visual science. 2005 Sep:46(9):3233-8 [PubMed PMID: 16123424]
Level 3 (low-level) evidenceNg EW, Costa JR, Samiy N, Ruoff KL, Connolly E, Cousins FV, D'Amico DJ. Contribution of pneumolysin and autolysin to the pathogenesis of experimental pneumococcal endophthalmitis. Retina (Philadelphia, Pa.). 2002 Oct:22(5):622-32 [PubMed PMID: 12441729]
Level 3 (low-level) evidenceSanders ME, Norcross EW, Robertson ZM, Moore QC 3rd, Fratkin J, Marquart ME. The Streptococcus pneumoniae capsule is required for full virulence in pneumococcal endophthalmitis. Investigative ophthalmology & visual science. 2011 Feb:52(2):865-72. doi: 10.1167/iovs.10-5513. Epub 2011 Feb 22 [PubMed PMID: 21051708]
Level 3 (low-level) evidenceDave TV, Dave VP, Sharma S, Karolia R, Joseph J, Pathengay A, Pappuru RR, Das T. Infectious endophthalmitis leading to evisceration: spectrum of bacterial and fungal pathogens and antibacterial susceptibility profile. Journal of ophthalmic inflammation and infection. 2019 May 16:9(1):9. doi: 10.1186/s12348-019-0174-y. Epub 2019 May 16 [PubMed PMID: 31098742]
Yang Y, Wong Y, Li Y, Duan F, Ma X, Wong H, Sun R, Zeng J, Liu M, Yuan Z, Lin X. Clinical Features, Antibiotic Susceptibilities, and Outcomes of Endophthalmitis Caused by Streptococcal Infection: Children vs. Adults. Antibiotics (Basel, Switzerland). 2023 May 25:12(6):. doi: 10.3390/antibiotics12060962. Epub 2023 May 25 [PubMed PMID: 37370281]
Ly V, Sallam A. Fungal Endophthalmitis. StatPearls. 2026 Jan:(): [PubMed PMID: 32644683]
Phasukkijwatana N, Jongpipatchai R, Phuksapaisalsilp P, Pharkjaksu S, Ngamskulrungroj P, Prakhunhungsit S. Effect of fenestrated sterile drape and face mask on bacterial dispersion toward the periocular area during intravitreal injection. Scientific reports. 2023 Jun 19:13(1):9878. doi: 10.1038/s41598-023-37091-3. Epub 2023 Jun 19 [PubMed PMID: 37336958]
Myers WG, Chang DF, Shorstein NH, Mah FS, Mamalis N, Miller KM, ASCRS Cataract Clinical Committee. ASCRS clinical advisory on intracameral moxifloxacin injection for infection prophylaxis. Journal of cataract and refractive surgery. 2023 Oct 1:49(10):1068-1070. doi: 10.1097/j.jcrs.0000000000001237. Epub [PubMed PMID: 37290753]
Chawla H, Pahng JN, Benevento JD, Mazzulla DA, Puri S, Eustis HS. Subretinal Abscess Complicated by Post-infectious Retinal Vasculitis Following Strabismus Surgery. Journal of pediatric ophthalmology and strabismus. 2023 May:60(3):e26-e30. doi: 10.3928/01913913-20230222-01. Epub 2023 May 1 [PubMed PMID: 37227991]
Taubenslag KJ, Cherney EF, Patel SN, Law JC, Daniels AB, Kim SJ. Intravitreal triple therapy with vancomycin, ceftazidime, and moxifloxacin for bacterial endophthalmitis: A Twelve-year experience. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2023 Oct:261(10):2813-2819. doi: 10.1007/s00417-023-06112-2. Epub 2023 May 25 [PubMed PMID: 37227476]
Tang Q, He M, Zhang S, Zhang J, Yang L, Shi H. The Diagnostic Value of Triggering Receptor Expressed on Myeloid Cells-1 in Post-Traumatic Bacterial Endophthalmitis. Investigative ophthalmology & visual science. 2023 May 1:64(5):4. doi: 10.1167/iovs.64.5.4. Epub [PubMed PMID: 37129904]
Antaki F, Marchand-Senécal X, Aubin MJ. Endogenous endophthalmitis and bilateral optic neuropathy secondary to Mycobacterium bovis. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2020 Jun:55(3):e88-e91. doi: 10.1016/j.jcjo.2019.10.008. Epub 2019 Dec 23 [PubMed PMID: 31879069]
Lodha D, Karolia R, Sharma S, Joseph J, Das T, Dave VP. Biofilm formation and its effect on the management of culture-positive bacterial endophthalmitis. Indian journal of ophthalmology. 2022 Feb:70(2):472-476. doi: 10.4103/ijo.IJO_1872_21. Epub [PubMed PMID: 35086219]
Kaur K, Gurnani B. Lens Abscess. StatPearls. 2026 Jan:(): [PubMed PMID: 36512661]
Zhou S, Hunt KM, Grewal AS, Brothers KM, Dhaliwal DK, Shanks RMQ. Release of Moxifloxacin From Corneal Collagen Shields. Eye & contact lens. 2018 Nov:44 Suppl 2(Suppl 2):S143-S147. doi: 10.1097/ICL.0000000000000421. Epub [PubMed PMID: 28945653]
Rudraprasad D, Joseph J. Proteomic landscape of extracellular vesicles in human retinal cells infected with Staphylococcus aureus and Pseudomonas aeruginosa: Role in endophthalmitis. Experimental cell research. 2023 Jun 15:427(2):113604. doi: 10.1016/j.yexcr.2023.113604. Epub 2023 Apr 17 [PubMed PMID: 37075825]
Patel SB, Reddy NK, He YG. TOXIC POSTERIOR SEGMENT SYNDROME AFTER DROPLESS CATARACT SURGERY WITH COMPOUNDED TRIAMCINOLONE-MOXIFLOXACIN. Retina (Philadelphia, Pa.). 2020 Mar:40(3):446-455. doi: 10.1097/IAE.0000000000002450. Epub [PubMed PMID: 30689622]
Velez-Montoya R, Monroy-Esquivel L, Ortiz-Guevara R, Quiroz-Mercado H, Fromow-Guerra J, Mexican Endophthalmitis Study Group (Mex-ESG). ALTERNATIVE INTRAVITREAL ANTIBIOTICS: A Systematic Review for Consideration in Recalcitrant or Resistant Endophthalmitis. Retina (Philadelphia, Pa.). 2023 Sep 1:43(9):1433-1447. doi: 10.1097/IAE.0000000000003773. Epub [PubMed PMID: 36893433]
Level 1 (high-level) evidenceGhita AM, Iliescu DA, Ghita AC, Ilie LA. Susceptibility of Ocular Surface Bacteria to Various Antibiotic Agents in a Romanian Ophthalmology Clinic. Diagnostics (Basel, Switzerland). 2023 Nov 9:13(22):. doi: 10.3390/diagnostics13223409. Epub 2023 Nov 9 [PubMed PMID: 37998545]
Velivelli L, Pradeep TG, Reddy SS, Palassery R. Panophthalmitis in a case of Glanzmann thrombasthenia - The dilemma in diagnosis. Romanian journal of ophthalmology. 2025 Jul-Sep:69(3):418-420. doi: 10.22336/rjo.2025.65. Epub [PubMed PMID: 41189778]
Level 3 (low-level) evidenceGurnani B, Kaur K. Endogenous Endophthalmitis. StatPearls. 2026 Jan:(): [PubMed PMID: 35015416]
McCarthy K, Silkiss RZ. Ocular manifestations of vaccine-preventable diseases: A comprehensive review. Vaccine. 2025 Dec 5:68():127900. doi: 10.1016/j.vaccine.2025.127900. Epub 2025 Nov 7 [PubMed PMID: 41205407]
Zhao MY, Kiryakoza LC, Rohowetz LJ, Albini TA, Yannuzzi NA, Miller D, Flynn HW Jr. Endophthalmitis Caused by Enterococcus Gallinarum Following Intravitreal Bevacizumab for Diabetic Macular Edema. Ophthalmic surgery, lasers & imaging retina. 2025 Dec:56(12):756-758. doi: 10.3928/23258160-20250815-01. Epub 2025 Oct 7 [PubMed PMID: 41052358]
Zhang Y, Tian J, Xu Y. Endogenous endophthalmitis secondary to neisseria meningitidis: a case report. BMC ophthalmology. 2026 Jan 10:26(1):16. doi: 10.1186/s12886-026-04612-3. Epub 2026 Jan 10 [PubMed PMID: 41519702]
Level 3 (low-level) evidenceHui W, Hui L, Junfeng P, Yajun X, Yujiao C, Danqi L, Yoo G, In-Chul J, Feng W. Analysis of pathogenic bacteria and predictors of infectious endophthalmitis after cataract surgery. BMC ophthalmology. 2025 Oct 31:25(1):613. doi: 10.1186/s12886-025-04444-7. Epub 2025 Oct 31 [PubMed PMID: 41174521]
Level 2 (mid-level) evidenceRowe LW, McVeigh LG, Hajrasouliha AR. SUBTENON'S VANCOMYCIN INJECTION FOR SUBRETINAL ABSCESS SECONDARY TO METHICILLIN-RESISTANT STAPHYLOCOCCUS AUREUS ENDOGENOUS ENDOPHTHALMITIS: A CASE REPORT AND LITERATURE REVIEW. Retinal cases & brief reports. 2024 May 1:18(3):296-300. doi: 10.1097/ICB.0000000000001398. Epub [PubMed PMID: 36728564]
Level 3 (low-level) evidenceSoleimani M, Masoumi A, Tabatabaei SA, Zamani MH. Citrobacter keratitis: predisposing factors and clinical characteristics. Journal of ophthalmic inflammation and infection. 2023 Jan 31:13(1):3. doi: 10.1186/s12348-022-00322-1. Epub 2023 Jan 31 [PubMed PMID: 36720767]
Al-Khersan H, Nuesi R. Subretinal and Liver Abscesses in Klebsiella Endophthalmitis. American journal of ophthalmology. 2023 Apr:248():e1. doi: 10.1016/j.ajo.2023.01.018. Epub 2023 Jan 25 [PubMed PMID: 36709020]
Tiecco G, Laurenda D, Mulè A, Arsuffi S, Storti S, Migliorati M, Boldini A, Signorini L, Castelli F, Quiros-Roldan E. Gram-Negative Endogenous Endophthalmitis: A Systematic Review. Microorganisms. 2022 Dec 28:11(1):. doi: 10.3390/microorganisms11010080. Epub 2022 Dec 28 [PubMed PMID: 36677371]
Level 1 (high-level) evidenceKim SW, Kim JH, Choi M, Lee SJ, Shin JP, Kim JG, Kang SW, Park KH, Korean Retina Society members. An Outbreak of Fungal Endophthalmitis After Cataract Surgery in South Korea. JAMA ophthalmology. 2023 Mar 1:141(3):226-233. doi: 10.1001/jamaophthalmol.2022.5927. Epub [PubMed PMID: 36656597]
Clauss KD, Kinde B, Berrocal AM. Neonate with Disseminated Pseudomonas Infection Presenting with Endogenous Endophthalmitis, Meningitis, and Subcutaneous Nodules. American journal of ophthalmology. 2023 Mar:247():e4-e5. doi: 10.1016/j.ajo.2022.12.013. Epub 2022 Dec 21 [PubMed PMID: 36565905]
Segretín Gutiérrez EFE, García MM, Bursztyn M, Benavente Defferrari MM, Ortiz-Basso T. Incidence of endophthalmitis post cataract surgery in a Tertiary Hospital of Buenos Aires. Medicina. 2022:82(6):851-855 [PubMed PMID: 36571523]
Li K, Yu L, Ma L, Xia J, Peng J, Hu P, Liu G, Ye J. Surface modification of commercial intraocular lens by zwitterionic and antibiotic-loaded coating for preventing postoperative endophthalmitis. Colloids and surfaces. B, Biointerfaces. 2023 Feb:222():113093. doi: 10.1016/j.colsurfb.2022.113093. Epub 2022 Dec 15 [PubMed PMID: 36542949]
Fabiani C, Agarwal M, Dogra M, Tosi GM, Davis JL. Exogenous Endophthalmitis. Ocular immunology and inflammation. 2023 Sep:31(7):1386-1395. doi: 10.1080/09273948.2022.2152699. Epub 2022 Dec 19 [PubMed PMID: 36534597]
Singh S, Singh PK, Kumar A. Butyrate Ameliorates Intraocular Bacterial Infection by Promoting Autophagy and Attenuating the Inflammatory Response. Infection and immunity. 2023 Jan 24:91(1):e0025222. doi: 10.1128/iai.00252-22. Epub 2022 Dec 14 [PubMed PMID: 36515524]
Rosenberg CR, Gensure RH, Tri Ta Kim D, Yumang M, Suhler EB, Lin P, Flaxel CJ. LATE DIAGNOSIS OF Cutibacterium acnes (FORMERLY Propionibacterium acnes ) ENDOPHTHALMITIS AND THE IMPORTANCE OF DUAL TESTING WITH BACTERIAL CULTURE AND POLYMERASE CHAIN REACTION. Retinal cases & brief reports. 2024 Sep 1:18(5):576-579. doi: 10.1097/ICB.0000000000001458. Epub [PubMed PMID: 37683191]
Level 3 (low-level) evidenceYu J, Yuan G, Sun X, Shan T, Zhang D, Liu C, Zhang J. EFFICACY OF VITRECTOMY COMBINED WITH INTRAVITREAL ANTIBIOTICS FOR SEVERE POST-TRAUMATIC ENDOPHTHALMITIS. Retina (Philadelphia, Pa.). 2023 Nov 1:43(11):2003-2009. doi: 10.1097/IAE.0000000000003887. Epub [PubMed PMID: 37490780]
Ciociola EC, Powell JC, Barnwell E, Zehden JA, Robbins CB, Soundararajan S, Singh P, Zhang AY, Fekrat S, Greven MA. ENDOGENOUS ENDOPHTHALMITIS ASSOCIATED WITH INJECTION DRUG USE COMPARED WITH OTHER ETIOLOGIES. Retina (Philadelphia, Pa.). 2023 Nov 1:43(11):1996-2002. doi: 10.1097/IAE.0000000000003898. Epub [PubMed PMID: 37490751]
Lu X, Ng DS, Zheng K, Peng K, Jin C, Xia H, Chen W, Chen H. Risk factors for endophthalmitis requiring evisceration or enucleation. Scientific reports. 2016 Jun 15:6():28100. doi: 10.1038/srep28100. Epub 2016 Jun 15 [PubMed PMID: 27302573]
Sridhar J, Kuriyan AE, Flynn HW Jr, Miller D. ENDOPHTHALMITIS CAUSED BY PSEUDOMONAS AERUGINOSA: Clinical Features, Antibiotic Susceptibilities, and Treatment Outcomes. Retina (Philadelphia, Pa.). 2015 Jun:35(6):1101-6. doi: 10.1097/IAE.0000000000000469. Epub [PubMed PMID: 25658178]
Shah PN, Mishra DK, Shanmugam MP, Agarwal M, Susvar P, Sen AC, Ramanjulu R, Dave V, Saravanan V, Kannan N, Sinha T, Sindal MD, Singh SR, Rajanna MK, Ayachit AG, Maitray A, Yadav NK, Balakrishnan D, Nigam E, Narula R, Khadar SMA, Atri N, Mittal S, Murthy H, Mahalingam PS, Pillai GS, Nagpal M, Walinjkar J, Gupta V, Kothari A, VRSI Study Group. Incidence of post vitrectomy endophthalmitis in India - A multicentric study by VRSI study Group. Eye (London, England). 2023 Oct:37(14):2915-2920. doi: 10.1038/s41433-023-02430-1. Epub 2023 Feb 8 [PubMed PMID: 36754984]
Dowler KK, Vientós-Plotts A, Giuliano EA, McAdams ZL, Reinero CR, Ericsson AC. Molecular and microbiological evidence of bacterial contamination of intraocular lenses commonly used in canine cataract surgery. PloS one. 2022:17(11):e0277753. doi: 10.1371/journal.pone.0277753. Epub 2022 Nov 21 [PubMed PMID: 36409704]
Level 3 (low-level) evidenceGreen MB, Agranat JS, Davoudi S, Sanayei N, Ness S. Penicillin Responsive Presumed Seronegative Ocular Syphilis in a Patient with Human Immunodeficiency Virus: A Case Report and Review of the Literature. Ocular immunology and inflammation. 2023 Sep:31(7):1320-1327. doi: 10.1080/09273948.2023.2183413. Epub 2023 Mar 10 [PubMed PMID: 36897959]
Level 3 (low-level) evidenceLeveziel L, Knoeri J, Errera MH, Kobal A, Fardeau C, Bouheraoua N, Sahel JA, Baudouin C, Nordmann JP, Baudouin F, Merabet L, Borderie V. Anterior chamber tap cytology in acute postoperative endophthalmitis: a case-control study. The British journal of ophthalmology. 2022 Jun:106(6):807-814. doi: 10.1136/bjophthalmol-2020-317438. Epub 2021 Feb 11 [PubMed PMID: 33574032]
Level 2 (mid-level) evidenceConfalonieri F, Gorenjak de Souza B, Petrovski G, Lumi X. Severe Retinal Necrosis Due to Klebsiella pneumoniae After Acute Prostatitis. The American journal of case reports. 2022 Oct 19:23():e937512. doi: 10.12659/AJCR.937512. Epub 2022 Oct 19 [PubMed PMID: 36260534]
Level 3 (low-level) evidenceLallier S, Deaner JD, Feng H, Jaffe GJ. PSEUDOMONAS ENDOPHTHALMITIS AFTER 0.59 MG FLUOCINOLONE ACETONIDE SURGICAL IMPLANT IN A PATIENT WITH A LONG-STANDING CRAWFORD TUBE. Retinal cases & brief reports. 2023 Sep 1:17(5):515-518. doi: 10.1097/ICB.0000000000001237. Epub [PubMed PMID: 37643034]
Level 3 (low-level) evidenceHudson JL, Fan JC, Smiddy WE, Sridhar J, Yannuzzi NA, Flynn HW Jr. ACUTE- AND DELAYED-ONSET ENDOPHTHALMITIS AFTER OPEN GLOBE INJURIES: Clinical Features and Visual Acuity Outcomes. Retina (Philadelphia, Pa.). 2023 Apr 1:43(4):594-599. doi: 10.1097/IAE.0000000000003707. Epub [PubMed PMID: 36729611]
Adam CR, Abrams GW. TOXOPLASMOSIS RETINOCHOROIDITIS MASQUERADING AS ENDOGENOUS ENDOPHTHALMITIS IN A CASE OF CONGENITAL LONG QT SYNDROME. Retinal cases & brief reports. 2022 Sep 1:16(5):637-642. doi: 10.1097/ICB.0000000000001048. Epub [PubMed PMID: 32910025]
Level 3 (low-level) evidenceWitkin AJ, Shah AR, Engstrom RE, Kron-Gray MM, Baumal CR, Johnson MW, Witkin DI, Leung J, Albini TA, Moshfeghi AA, Batlle IR, Sobrin L, Eliott D. Postoperative Hemorrhagic Occlusive Retinal Vasculitis: Expanding the Clinical Spectrum and Possible Association with Vancomycin. Ophthalmology. 2015 Jul:122(7):1438-51. doi: 10.1016/j.ophtha.2015.03.016. Epub 2015 Apr 15 [PubMed PMID: 25886796]
Zungu T, Mdala S, Manda C, Kayange P. Ocular infection from Staphylococcus aureus bacteraemia in a sero-positive HIV patient from Queen Elizabeth Central Hospital, Blantyre, Malawi. Malawi medical journal : the journal of Medical Association of Malawi. 2020 Dec:32(4):232-234. doi: 10.4314/mmj.v32i4.10. Epub [PubMed PMID: 34457210]
Baquet-Walscheid K, Heinz C. [Intermediate and Posterior Uveitis - Disease entities]. Klinische Monatsblatter fur Augenheilkunde. 2024 Jan:241(1):119-135. doi: 10.1055/a-2193-2568. Epub 2023 Nov 17 [PubMed PMID: 37977201]
Jeroudi A, Yeh S. Diagnostic vitrectomy for infectious uveitis. International ophthalmology clinics. 2014 Spring:54(2):173-97. doi: 10.1097/IIO.0000000000000017. Epub [PubMed PMID: 24613892]
Doft BH. The endophthalmitis vitrectomy study. Archives of ophthalmology (Chicago, Ill. : 1960). 1991 Apr:109(4):487-9 [PubMed PMID: 2012545]
Rathi VM, Sharma S, Das T, Khanna RC. Endophthalmitis Prophylaxis Study, Report 2: Intracameral antibiotic prophylaxis with or without postoperative topical antibiotic in cataract surgery. Indian journal of ophthalmology. 2020 Nov:68(11):2451-2455. doi: 10.4103/ijo.IJO_1738_19. Epub [PubMed PMID: 33120637]
Christy NE, Sommer A. Antibiotic prophylaxis of postoperative endophthalmitis. Annals of ophthalmology. 1979 Aug:11(8):1261-5 [PubMed PMID: 318049]
Level 1 (high-level) evidenceEndophthalmitis Study Group, European Society of Cataract & Refractive Surgeons. Prophylaxis of postoperative endophthalmitis following cataract surgery: results of the ESCRS multicenter study and identification of risk factors. Journal of cataract and refractive surgery. 2007 Jun:33(6):978-88 [PubMed PMID: 17531690]
Level 1 (high-level) evidenceYu CQ, Ta CN. Prevention of postcataract endophthalmitis: evidence-based medicine. Current opinion in ophthalmology. 2012 Jan:23(1):19-25. doi: 10.1097/ICU.0b013e32834cd5a9. Epub [PubMed PMID: 22081026]
Level 3 (low-level) evidenceSromicki JW, Stahel M, Blum RA, Rudolph KA, Barthelmes D. Early Vitrectomy in Endophthalmitis: Visual Outcomes and Complication Rates. Ophthalmology and therapy. 2025 Aug:14(8):2031-2042. doi: 10.1007/s40123-025-01196-x. Epub 2025 Jul 9 [PubMed PMID: 40632428]
Hussain I, Ishrat S, Ho DCW, Khan SR, Veeraraghavan MA, Palraj BR, Molton JS, Abid MB. Endogenous endophthalmitis in Klebsiella pneumoniae pyogenic liver abscess: Systematic review and meta-analysis. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases. 2020 Dec:101():259-268. doi: 10.1016/j.ijid.2020.09.1485. Epub 2020 Oct 6 [PubMed PMID: 33035676]
Level 1 (high-level) evidenceGurnani B, Kaur K. Renaissance of an Emerging Pathogen-Pythium insidiosum Keratitis: An Indian Perspective. Clinical ophthalmology (Auckland, N.Z.). 2025:19():4811-4830. doi: 10.2147/OPTH.S568552. Epub 2025 Dec 18 [PubMed PMID: 41446894]
Level 3 (low-level) evidenceMiller JJ, Scott IU, Flynn HW Jr, Smiddy WE, Corey RP, Miller D. Endophthalmitis caused by Streptococcus pneumoniae. American journal of ophthalmology. 2004 Aug:138(2):231-6 [PubMed PMID: 15289132]
Level 2 (mid-level) evidenceGong JJ, Perkins W, Frenkel J, Greco J, Desmond-Combs K. Endophthalmitis diagnosis supported by bedside ultrasound. Journal of the American College of Emergency Physicians open. 2022 Oct:3(5):e12802. doi: 10.1002/emp2.12802. Epub 2022 Sep 10 [PubMed PMID: 36176502]
Ota I, Takahashi H, Ono M, Yamamoto S, Kogita A, Tsuda H, Funai S, Shigeoka H, Hiraide A. Liver Abscess due to Streptococcus intermedius Bacteremia and Its Association with Colonic Carcinoma: Is Bacteremia with Streptococcus intermedius an Alert for Colonic Carcinoma? Case reports in gastroenterology. 2022 May-Aug:16(2):488-495. doi: 10.1159/000526158. Epub 2022 Aug 19 [PubMed PMID: 36157604]
Level 3 (low-level) evidenceChen N, Chalam KV. Successful management of a rare case of endogenous endophthalmitis from soft tissue (gluteal) abscess. Journal of surgical case reports. 2022 Sep:2022(9):rjac412. doi: 10.1093/jscr/rjac412. Epub 2022 Sep 19 [PubMed PMID: 36148144]
Level 3 (low-level) evidencePatterson TJ, McKinney D, Ritson J, McLean C, Gu W, Colyer M, McClellan SF, Miller SC, Justin GA, Hoskin AK, Cavuoto K, Leong J, Ascarza AR, Woreta FA, Miller KE, Caldwell MC, Gensheimer WG, Williamson T, Dhawahir-Scala F, Shah P, Coombes A, Sundar G, Mazzoli RA, Woodcock M, Kuhn F, Watson SL, Gomes RSM, Agrawal R, Blanch RJ. The Use of Preoperative Prophylactic Systemic Antibiotics for the Prevention of Endopthalmitis in Open Globe Injuries: A Meta-Analysis. Ophthalmology. Retina. 2023 Nov:7(11):972-981. doi: 10.1016/j.oret.2023.06.022. Epub 2023 Jul 4 [PubMed PMID: 37406735]
Level 1 (high-level) evidenceSchimansky S, Schwember P, Chervenkoff J, Liyanage SE, Keller J. Retinal detachment after post-operative endophthalmitis: clinical characteristics, outcomes and risk factors. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2023 Aug:261(8):2181-2187. doi: 10.1007/s00417-023-06021-4. Epub 2023 Mar 2 [PubMed PMID: 36859736]
Kvopka M, Chan W, Baranage D, Sia D. Morganella morganii and Enterococcus faecalis endophthalmitis following intravitreal injection. BMC ophthalmology. 2023 Nov 10:23(1):450. doi: 10.1186/s12886-023-03198-4. Epub 2023 Nov 10 [PubMed PMID: 37950172]
Poon E, Poon A, McKelvie P, Levitz L, Zamir E. Delayed Bacterial Endotheliitis and Endophthalmitis 11 Years after Cataract Surgery. Case reports in ophthalmology. 2023 Jan-Dec:14(1):376-381. doi: 10.1159/000531501. Epub 2023 Aug 16 [PubMed PMID: 37901637]
Level 3 (low-level) evidenceSborgia G, Niro A, Pastore V, Favale RA, Sborgia A, Gigliola S, Giuliani G, Grassi MO, Coassin M, Aiello F, Iaculli C, Reibaldi M, Boscia F, Alessio G. Mid-term safety and effectiveness of intravitreal dexamethasone implant to treat persistent cystoid macular edema in vitrectomized eyes for bacterial endophthalmitis. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2022 Aug:260(8):2703-2710. doi: 10.1007/s00417-022-05615-8. Epub 2022 Mar 7 [PubMed PMID: 35254512]
Sevcik KM, Fortenbach CR, Russell JF. Subacute mycobacterial endophthalmitis after glaucoma valve surgery. American journal of ophthalmology. 2023 Feb:246():e3-e4. doi: 10.1016/j.ajo.2022.10.014. Epub 2022 Nov 1 [PubMed PMID: 36328201]
Shekhar M, Lamba P, Haripriya A, Ravindran S, Palod S, Mishra C, Sundar B, Sen S. Acute postoperative endophthalmitis after resurgery following primary cataract surgery: 9 years experience from a tertiary eyecare center. Journal of cataract and refractive surgery. 2021 Aug 1:47(8):1050-1055. doi: 10.1097/j.jcrs.0000000000000584. Epub [PubMed PMID: 34292890]
Ruby A, Shaikh S, Khammar AJ, Trese M. Suprachoroidal septic effusion leading to panophthalmitis following strabismus surgery. Journal of pediatric ophthalmology and strabismus. 2005 Jul-Aug:42(4):250-2 [PubMed PMID: 16121559]
Level 3 (low-level) evidenceOgawa M, Sugita S, Watanabe K, Shimizu N, Mochizuki M. Novel diagnosis of fungal endophthalmitis by broad-range real-time PCR detection of fungal 28S ribosomal DNA. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2012 Dec:250(12):1877-83. doi: 10.1007/s00417-012-2015-7. Epub 2012 Apr 15 [PubMed PMID: 22527320]
Jabbour S, Harissi-Dagher M, Agoumi Y, Singh H, Robert MC. Cyclophotocoagulation in the Control of Glaucoma in Patients With the Boston Keratoprosthesis Type 1. Cornea. 2020 Feb:39(2):181-185. doi: 10.1097/ICO.0000000000002064. Epub [PubMed PMID: 31335536]
Solborg Bjerrum S, Prause JU, Fuchs J, la Cour M, Kiilgaard JF. Morphological features in eyes with endophthalmitis after cataract surgery - histopathology and optical coherence tomography assessment. Acta ophthalmologica. 2016 Feb:94(1):26-30. doi: 10.1111/aos.12858. Epub 2015 Sep 26 [PubMed PMID: 26407533]
Lartey S, Armah P, Ampong A. A sudden total loss of vision after routine cataract surgery. Ghana medical journal. 2013 Jun:47(2):96-9 [PubMed PMID: 23966748]
Level 3 (low-level) evidenceKolomeyer AM, Bhagat N, Chu DS. Haemophilus influenza endophthalmitis after pterygium surgery. Eye & contact lens. 2013 Mar:39(2):186-7. doi: 10.1097/ICL.0b013e31822f664f. Epub [PubMed PMID: 21912259]
Level 3 (low-level) evidenceLi KK, Tang EW, Lai JS, Wong D. Pseudomonas aeruginosa choroidal abscess in a patient with bronchiectasis. International ophthalmology. 2008 Aug:28(4):287-90 [PubMed PMID: 17687520]
Level 3 (low-level) evidenceAndroudi S, Theodoridou A, Praidou A, Brazitikos PD. Sympathetic ophthalmia following postoperative endophthalmitis and evisceration. Hippokratia. 2010 Apr:14(2):131-2 [PubMed PMID: 20596271]
Level 3 (low-level) evidencePatil R, Dehari D, Chaudhuri A, Kumar DN, Kumar D, Singh S, Nath G, Agrawal AK. Recent advancements in nanotechnology-based bacteriophage delivery strategies against bacterial ocular infections. Microbiological research. 2023 Aug:273():127413. doi: 10.1016/j.micres.2023.127413. Epub 2023 May 18 [PubMed PMID: 37216845]
Byrd LB, Gurnani B, Martin N. Corneal Ulcer. StatPearls. 2026 Jan:(): [PubMed PMID: 30969511]
Gunalda J, Williams D, Koyfman A, Long B. High risk and low prevalence diseases: Endophthalmitis. The American journal of emergency medicine. 2023 Sep:71():144-149. doi: 10.1016/j.ajem.2023.06.029. Epub 2023 Jun 20 [PubMed PMID: 37393773]
Joshi PH, Youssef AAA, Ghonge M, Varner C, Tripathi S, Dudhipala N, Majumdar S. Gatifloxacin Loaded Nano Lipid Carriers for the Management of Bacterial Conjunctivitis. Antibiotics (Basel, Switzerland). 2023 Aug 15:12(8):. doi: 10.3390/antibiotics12081318. Epub 2023 Aug 15 [PubMed PMID: 37627738]
Emami S, Kitayama K, Coleman AL. Adjunctive steroid therapy versus antibiotics alone for acute endophthalmitis after intraocular procedure. The Cochrane database of systematic reviews. 2022 Jun 6:6(6):CD012131. doi: 10.1002/14651858.CD012131.pub3. Epub 2022 Jun 6 [PubMed PMID: 35665485]
Level 1 (high-level) evidence