Introduction
Endometrial polyps are localized epithelial proliferations composed of endometrial glands, stroma, and a central vascular core arising from the uterine cavity. These lesions vary widely in size, from a few millimeters to several centimeters, and may occur as solitary growths or as multiple polyps that occupy the entire endometrial cavity. Although they can develop at any age, the peak incidence is observed between 40 and 49 years. Most polyps are benign; however, a small but clinically meaningful risk of premalignant or malignant transformation exists, particularly in postmenopausal individuals or those with specific risk factors, eg, unopposed estrogen exposure or tamoxifen therapy.
Understanding the natural history of endometrial polyps is essential for guiding evaluation and management. Hormonal influences, especially estrogen-driven endometrial proliferation, play a central role in their development, while molecular alterations may contribute to neoplastic progression in a minority of cases. Patterns of spread are typically localized to the uterine cavity, but polyps may coexist with diffuse endometrial pathology, including hyperplasia or carcinoma. Recognizing these relationships is critical for appropriate risk stratification, diagnostic selection, and individualized treatment planning.[1][2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Endometrial polyps are localized overgrowths of endometrial glands, stroma, and blood vessels that project from the endometrial surface into the uterine cavity. Although the precise cause remains unknown, several well-established risk factors contribute to their development, including increasing age, hypertension, obesity, and tamoxifen therapy. Because polyp formation is closely associated with endometrial hyperplasia, exposure to unopposed estrogen is considered a major etiologic driver and is frequently implicated in both premenopausal and postmenopausal populations.
Additional proposed mechanisms include increased endometrial aromatase activity, dysregulation of growth factors, eg, transforming growth factor-β (TGF-β) and vascular endothelial growth factor (VEGF), and overexpression of the anti-apoptotic protein B-cell lymphoma-2 (BCL-2). Genetic alterations have also been identified in some polyps, supporting a multifactorial pathogenesis. Endometrial abnormalities, including polyps, occur in approximately 20% to 35% of individuals receiving chronic tamoxifen therapy, reflecting the drug’s partial estrogen-agonist effects on the endometrium.
Although most polyps are benign, malignant transformation occurs in up to 13% of cases. Risk is influenced by age, menopausal status, and symptomatology; in postmenopausal individuals, malignancy is identified in 4.47% of symptomatic cases compared with 1.51% of asymptomatic cases. Additional risk factors for malignant transformation include individuals older than 60 years, large polyp size, postmenopausal status, symptomatic bleeding, and polycystic ovary syndrome.[3][4]
Epidemiology
Endometrial polyps occur across all age groups but are most frequently identified in individuals aged between 40 and 49 years, reflecting the hormonal milieu of the late reproductive years. Among reproductive-aged individuals presenting with abnormal uterine bleeding, the prevalence of endometrial polyps is estimated at 20% to 40%, making them one of the most common structural causes of bleeding in this population.
Autopsy studies demonstrate that approximately 10% of individuals have endometrial polyps, including many who were asymptomatic during life. The likelihood of malignant transformation varies by age and menopausal status; premenopausal individuals have a substantially lower risk compared with postmenopausal individuals, in whom the prevalence of atypia or carcinoma is higher. These epidemiologic patterns underscore the importance of risk-stratified evaluation when polyps are identified in postmenopausal patients or those with additional risk factors.[5]
Pathophysiology
Endometrial polyps arise from focal overgrowths of endometrial glands and stroma around a central vascular core, driven primarily by estrogen-mediated proliferation and reduced apoptosis. Increased local aromatase expression and overexpression of anti-apoptotic proteins (eg, BCL-2) promote persistent endometrial growth, while dysregulation of growth factors, including TGF-β and VEGF, contributes to abnormal angiogenesis within the polyp.
These lesions often exhibit monoclonal stromal proliferation, supporting a neoplastic rather than purely hyperplastic origin. Most polyps remain benign; however, atypical hyperplasia or carcinoma may develop, particularly in postmenopausal individuals or those with unopposed estrogen exposure. Common findings include abnormal uterine bleeding, infertility, or incidental detection on imaging performed for unrelated indications.[6][7] Please see StatPearls' companion resource, "Abnormal Uterine Bleeding," for further information on PALM-COEIN etiologies.
Histopathology
Endometrial polyps are epithelial proliferations composed of vascular tissue, glandular structures, fibromuscular components, and connective tissue. They are typically covered by the surface endometrial epithelium and contain a prominent, thick-walled vascular core, a characteristic microscopic feature. Polyps may be sessile, pedunculated, or prolapsing, and prolapsed lesions can demonstrate secondary changes, eg, squamous metaplasia, inflammation, or ulceration due to exposure through the cervical os.
Most polyps consist of endometrial tissue that differs from the surrounding cycling endometrium and often shows reduced responsiveness to hormonal fluctuations, contributing to persistent growth. Histologic variants include atrophic, hyperplastic, and carcinomatous forms, the latter representing progression to atypical hyperplasia or carcinoma within the polyp. Stromal monoclonality and altered expression of proteins (eg, BCL-2) support a neoplastic rather than purely hyperplastic origin in many cases.[8]
History and Physical
Clinical History
Patients with endometrial polyps frequently remain asymptomatic, and many lesions are identified incidentally during evaluation for unrelated gynecologic conditions. When symptoms develop, abnormal uterine bleeding represents the most common clinical presentation. Approximately 25% of reproductive-aged individuals undergoing evaluation for abnormal uterine bleeding receive a diagnosis of endometrial polyps. Less common manifestations include pelvic pain, abdominal pain, and infertility.
Evaluation of abnormal uterine bleeding requires careful assessment of the underlying etiology, symptom severity, associated clinical features, and existing comorbidities. Please see StatPearls' companion resource, "Abnormal Uterine Bleeding," for further information. No specific bleeding pattern definitively identifies endometrial polyps; however, menorrhagia and intermenstrual spotting rank among the most frequently reported presentations. A thorough medical and surgical history remains essential for excluding alternative causes of bleeding, including coagulopathies, thyroid disorders, and structural uterine abnormalities.
Tamoxifen, a medication widely used in the treatment of breast cancer, exhibits both estrogen-agonist and estrogen-antagonist properties. Although antiestrogenic within breast tissue, tamoxifen exerts estrogenic effects on the endometrium, increasing the risk of endometrial pathology. Chronic use is associated with a 20% to 35% incidence of endometrial polyp formation. Hormone replacement therapy used to manage menopausal symptoms has also been linked to the development of endometrial polyps and commonly presents with irregular bleeding accompanied by increased endometrial thickness on ultrasonography. Please see StatPearls' companion resource, "Hormone Replacement Therapy," for further information.
Physical Examination
Physical examination should include a general assessment, a bimanual pelvic examination, and a sterile speculum examination. Careful evaluation of the cervix and vaginal vault helps exclude other structural sources of bleeding. In some patients, a pedunculated endometrial polyp extends through the external cervical os, permitting direct visualization during examination.[9][10]
Evaluation
Transvaginal ultrasound (TVUS) is the most commonly used and widely available imaging modality for evaluating suspected endometrial polyps (see Image. Endometrial Polyp). Typical findings include focal or diffuse echogenic endometrial thickening or a well-circumscribed intracavitary lesion. In individuals with postmenopausal bleeding, an endometrial thickness less than 4 mm is strongly associated with atrophy, whereas a thickness of greater than 4 mm raises concern for endometrial pathology, including polyps. Polyp size, number, and location do not reliably correlate with symptom severity.
Saline infusion sonography (SIS) is a valuable adjunct when TVUS findings are inconclusive. During SIS, 5 to 30 mL of warmed saline is instilled into the uterine cavity to enhance visualization of intracavitary structures (see Image. Saline Infusion Sonogram). This technique improves delineation of the endometrial cavity, facilitates distinction between endometrial polyps (arising from the endometrium) and submucosal fibroids (arising beneath the endometrium), and provides superior assessment of the cornua and adnexa. Contraindications include pregnancy and active cervical or uterine infection.
Additional diagnostic tools include hysterosalpingography and hysteroscopy. Hysteroscopy offers direct visualization and is considered the gold standard for diagnosis; however, it does not provide a tissue diagnosis unless combined with biopsy or polypectomy. Because of the potential risk of premalignant or malignant pathology, histologic sampling is recommended when polyps are identified, particularly in postmenopausal individuals or those with risk factors.
Tissue diagnosis may be obtained via endometrial biopsy, dilation and curettage (D&C), or hysteroscopic polypectomy. Blind sampling with biopsy or D&C has limited sensitivity for focal lesions and should be reserved for situations in which hysteroscopic evaluation is unavailable. Laboratory studies may include a urine pregnancy test, complete blood count, and coagulation profile to assess for pregnancy, anemia, or bleeding disorders. These tests support a comprehensive evaluation but do not directly diagnose polyps.[11][12][13][14]
| Reflect |
A 62-year-old postmenopausal patient presents with intermittent vaginal spotting. The patient has a history of obesity and has been receiving tamoxifen therapy following treatment for breast cancer. Transvaginal ultrasound demonstrates focal endometrial thickening suggestive of an intracavitary lesion.
|
Treatment / Management
Conservative management with observation represents an acceptable approach for asymptomatic individuals with a low risk of malignancy. Spontaneous regression occurs in some cases; one study reported resolution of 29% of endometrial polyps within 1 year among premenopausal individuals. Conservative management generally involves periodic monitoring with transvaginal ultrasound to assess for persistence, regression, or progression of lesions. Hormonal therapy has limited supporting evidence and lacks endorsement from major clinical guidelines as a routine treatment option for endometrial polyps.[15][11](B2)
Hysteroscopic polypectomy remains the gold standard treatment for endometrial polyps. This procedure enables complete lesion removal under direct visualization while providing tissue for histopathologic evaluation. Because endometrial polyps may coexist with additional endometrial abnormalities, microscopic examination of both the excised polyp and the surrounding endometrium remains essential. Benign polyps have been identified in 20% of individuals diagnosed with endometrial carcinoma, highlighting the importance of comprehensive tissue assessment and pathologic review.
The optimal timing of polypectomy for asymptomatic, low-risk patients remains uncertain. A retrospective study evaluating routine polyp removal identified no malignancies in histologic specimens, suggesting that universal polypectomy may not be necessary in all cases. However, polyps measuring more than 1.5 cm demonstrate a lower likelihood of spontaneous regression. Surgical removal generally remains appropriate for symptomatic individuals and for those with risk factors associated with malignant transformation.
Hysterectomy provides a definitive surgical option by eliminating both recurrence risk and the potential for future malignant transformation. However, this approach carries substantially greater morbidity and cost than less invasive interventions and warrants consideration only after comprehensive counseling and when alternative management strategies are unsuitable. Patients who develop anemia secondary to abnormal uterine bleeding should receive iron supplementation as part of supportive management to correct iron deficiency and improve hematologic status.[7][16][17](B2)
Differential Diagnosis
Accurate differentiation relies on a combination of clinical history, imaging characteristics, and histologic evaluation, with hysteroscopy and tissue sampling providing the highest diagnostic precision.[18][19] Several gynecologic conditions can mimic the presentation or imaging appearance of endometrial polyps and must be considered during evaluation. Submucosal leiomyomas are a common alternative diagnosis; these lesions arise from the myometrium beneath the endometrium and may appear as intracavitary masses on ultrasound or hysteroscopy. Adenomyomas can also resemble polyps but typically demonstrate myometrial involvement and heterogeneous echotexture.
Retained products of conception should be considered in individuals with recent pregnancy, miscarriage, or postpartum bleeding, as they may present with irregular bleeding and intracavitary tissue. Endometrial hyperplasia and endometrial carcinoma may produce focal or diffuse endometrial thickening and require tissue sampling to exclude premalignant or malignant pathology. Finally, uterine sarcoma, although rare, should be considered when lesions are large, rapidly growing, or associated with atypical imaging features or systemic symptoms.
Staging
Endometrial polyps lack a formal staging system because they are benign, localized intracavitary lesions that neither invade the myometrium nor metastasize. Management and prognostic assessment, therefore, do not rely on a polyp-specific classification system. When atypical hyperplasia or carcinoma is identified within an endometrial polyp, staging follows the underlying endometrial carcinoma rather than the polyp itself. In these cases, clinicians apply the FIGO staging system for endometrial cancer, with stage assignment based on factors, eg, the depth of myometrial invasion, cervical involvement, extrauterine spread, and lymph node status. Although endometrial polyps are not independently staged, any malignant transformation requires evaluation and management in accordance with established endometrial carcinoma staging guidelines.[20][21]
Prognosis
Most individuals experience significant improvement in abnormal uterine bleeding following hysteroscopic polypectomy, particularly those with intermenstrual spotting or heavy menstrual bleeding. Treatment is generally effective, with low recurrence rates, especially in patients who initially present with a small number of polyps. The recurrence rate of histologically confirmed polyps is approximately 2.5% to 3.7%, reflecting the durability of hysteroscopic removal.
Recurrence may be further reduced when polypectomy is combined with endometrial ablation or placement of a levonorgestrel-releasing intrauterine device (LNG-IUD); however, evidence supporting these adjunctive strategies remains limited, and their use is largely restricted to research settings. In individuals with tamoxifen-associated polyps, the LNG-IUD has demonstrated benefit in reducing the formation of new polyps.
Fertility outcomes after hysteroscopic polypectomy are generally favorable. Several studies report improved spontaneous pregnancy and term delivery rates following removal, with outcomes appearing similar regardless of whether polyps are 1 cm or less, greater than 1 cm, or multiple. Likewise, first-trimester miscarriage rates do not differ significantly based on polyp size or number, supporting polypectomy as a beneficial intervention for patients seeking conception.[5][22][23]
Complications
All resected specimens from hysteroscopic polypectomy should be submitted for pathologic evaluation to exclude atypia or carcinoma. If malignancy is identified, referral to gynecologic oncology is recommended for comprehensive staging and management. Procedural complications are uncommon; hysteroscopic polypectomy carries a low risk of infection, bleeding, or uterine perforation, and the incidence of intrauterine adhesions is rare.
Infertility Considerations
The relationship between endometrial polyps and infertility remains an area of active investigation. A prospective randomized controlled trial demonstrated that hysteroscopic polypectomy before intrauterine insemination significantly improves pregnancy rates, suggesting a beneficial effect on implantation. Polyps also appear more prevalent in individuals with fallopian tube obstruction compared with those with tubal patency, indicating a possible association with other infertility factors.
However, a retrospective study of patients undergoing in vitro fertilization (IVF) found no significant differences in pregnancy, miscarriage, or live birth rates among individuals with untreated polyps. Despite these mixed findings, current expert recommendations favor the removal of polyps before IVF, given the potential for improved endometrial receptivity and the low risk associated with hysteroscopic removal.[24][7][3]
Deterrence and Patient Education
Deterrence and patient education play important roles in the management of endometrial polyps by promoting early recognition of symptoms, timely evaluation, and informed participation in treatment decisions. Patients presenting with abnormal uterine bleeding should receive clear explanations regarding the potential causes of bleeding and the role of endometrial polyps as a common structural etiology. Education should include discussion of typical symptoms, available diagnostic tests, and the rationale for further evaluation, particularly in individuals with risk factors for premalignant or malignant disease. Providing accurate information regarding the generally favorable prognosis of benign polyps can help alleviate anxiety while encouraging adherence to recommended follow-up.
Counseling should address the full spectrum of management options, including observation for selected asymptomatic, low-risk patients and hysteroscopic polypectomy for symptomatic individuals or those with risk factors for malignancy. Patients should understand the benefits and limitations of each approach, the importance of histopathologic evaluation following removal, and the low but clinically meaningful risk of malignant transformation. Balanced discussions regarding cancer risk are essential to support informed decision-making while minimizing unnecessary psychological distress.
Education also offers an opportunity to address modifiable factors associated with the development and recurrence of endometrial polyps. Clinicians should counsel patients regarding the relationship between obesity, unopposed estrogen exposure, hormone therapy, and endometrial pathology. Encouraging weight management, regular medical follow-up, and prompt reporting of new or recurrent abnormal uterine bleeding may contribute to earlier detection of recurrent disease and other endometrial abnormalities. Patients receiving tamoxifen therapy should be informed of the increased risk of endometrial changes and the importance of promptly reporting gynecologic symptoms.
For individuals experiencing infertility or pursuing pregnancy, counseling should include discussion of the potential impact of polyps on implantation and fertility outcomes, as well as the possible benefits of hysteroscopic removal before fertility treatment. Effective patient education is strengthened through interprofessional collaboration among gynecologists, primary care clinicians, advanced practitioners, nurses, radiologists, pharmacists, and, when appropriate, fertility specialists. Consistent communication across the healthcare team supports shared decision-making, reinforces key educational messages, improves adherence to evaluation and treatment recommendations, and promotes patient-centered care focused on safety, quality, and long-term reproductive health.[25][5]
Pearls and Other Issues
Endometrial polyps are a common and often benign cause of abnormal uterine bleeding, with hysteroscopic polypectomy serving as both a diagnostic and therapeutic gold standard. Because blind sampling may miss focal lesions, direct visualization with hysteroscopy is preferred whenever available. All removed tissue should undergo histopathologic evaluation, as benign polyps may coexist with atypical hyperplasia or carcinoma. A key pitfall is assuming that small or asymptomatic polyps are uniformly low-risk; although malignancy is uncommon, risk increases with postmenopausal status, symptomatic bleeding, large size, and unopposed estrogen exposure. Another common oversight is failing to recognize the impact of medications such as tamoxifen, which significantly increases polyp prevalence and warrants closer surveillance.
Recurrence is generally low but may be higher in individuals with multiple polyps, chronic inflammation, or persistent estrogen stimulation. Preventive strategies include addressing modifiable risk factors, eg, obesity, and optimizing the management of conditions associated with estrogen excess. For patients pursuing pregnancy, timely removal of polyps may improve fertility outcomes, particularly before intrauterine insemination. Clear communication, shared decision-making, and coordinated care among gynecologists, radiologists, primary care clinicians, and nurses help ensure accurate diagnosis, appropriate intervention, and effective long-term follow-up.[25][26]
Enhancing Healthcare Team Outcomes
Endometrial polyps are localized proliferations of endometrial glands, stroma, and vascular tissue that project into the uterine cavity. They commonly occur between ages 40 and 49 and are associated with risk factors including obesity, hypertension, unopposed estrogen exposure, tamoxifen therapy, and postmenopausal status. Although most polyps are benign, a subset undergoes premalignant or malignant transformation, making accurate risk stratification essential. Patients may be asymptomatic or present with abnormal uterine bleeding, pelvic discomfort, or infertility. Evaluation typically includes transvaginal ultrasound, with saline infusion sonography and hysteroscopy providing enhanced visualization of intracavitary lesions. Histologic assessment remains critical because imaging alone cannot exclude atypia or malignancy. Hysteroscopic polypectomy serves as the diagnostic and therapeutic gold standard, while selected low-risk asymptomatic patients may be managed with observation.
Interprofessional collaboration promotes timely diagnosis, evidence-based management, and prevention of complications. Primary care clinicians, gynecologists, and advanced practice providers collaborate to identify symptoms, assess risk factors, coordinate diagnostic testing, and guide treatment selection. Nurses support patient education, procedural preparation, symptom monitoring, and follow-up care, while pharmacists evaluate medication-related factors, such as tamoxifen or hormone therapy, and provide counseling on treatment plans. Pathologists play a critical role in identifying atypia or malignancy, and gynecologic oncologists provide staging and management when cancer is detected. Effective communication among team members supports shared decision-making, appropriate referral, surveillance planning, management of abnormal uterine bleeding and anemia, and coordinated follow-up, improving patient safety, quality of care, and clinical outcomes.[27][28]
Media
(Click Image to Enlarge)
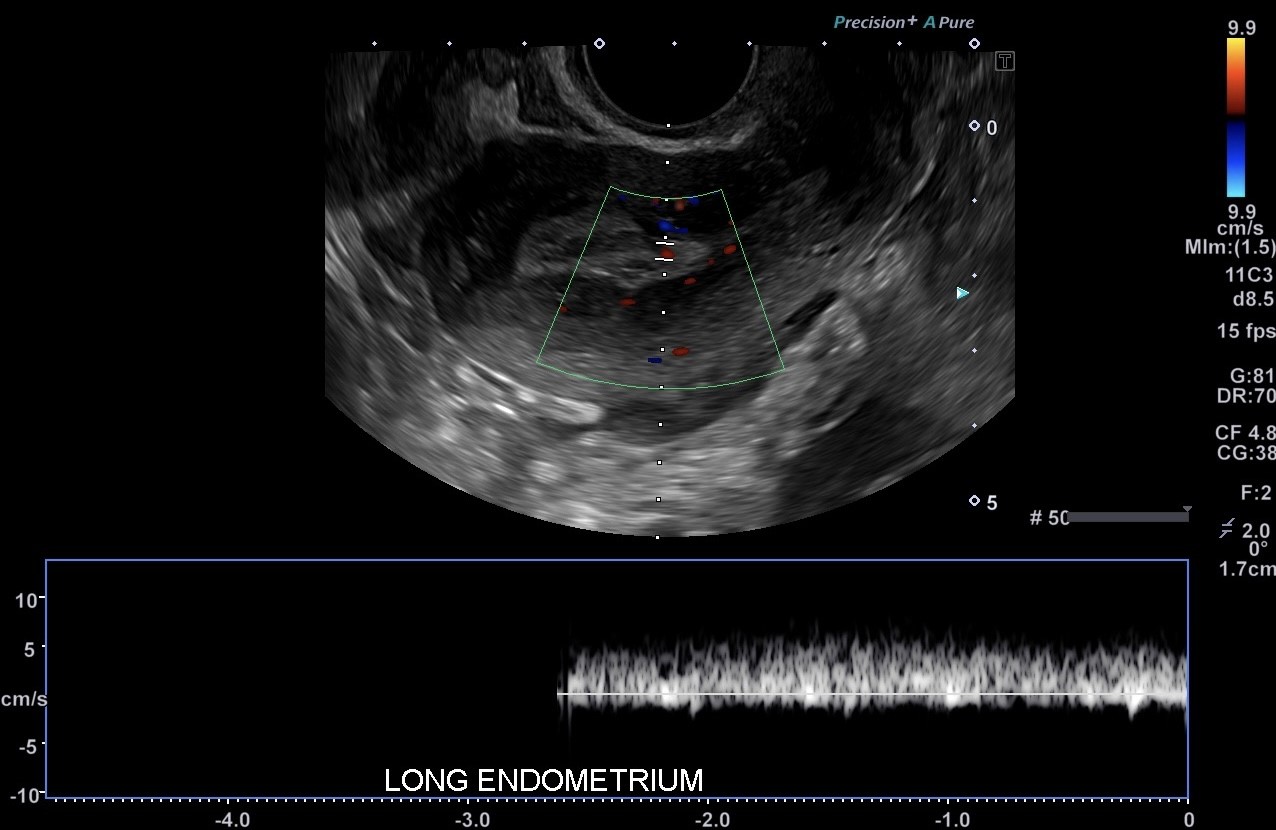
Endometrial Polyp. Transvaginal ultrasound is the most commonly used and widely available imaging modality for evaluating suspected endometrial polyps.
Contributed by S Lange, MD
(Click Image to Enlarge)
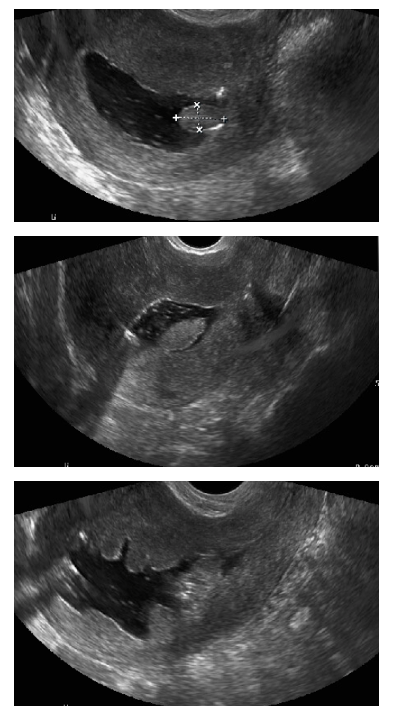
Saline Infusion Sonogram. Image demonstrating an endometrial polyp visualized with saline infusion sonogram.
Contributed by L Kondagari, MD
References
Silva AR, Santos M, Coelho A, Condeço R, Alpendre F, Ambrósio P, Pinto P, Bernardo MJ, Djokovic D. Expectant management as a primary approach for asymptomatic endometrial polyps: An ambispective cohort study. European journal of obstetrics, gynecology, and reproductive biology. 2026 Mar:319():114986. doi: 10.1016/j.ejogrb.2026.114986. Epub 2026 Feb 1 [PubMed PMID: 41637906]
Leal CRV, Vannuccini S, Jain V, Dolmans MM, Di Spiezio Sardo A, Al-Hendy A, Reis FM. Abnormal uterine bleeding: The well-known and the hidden face. Journal of endometriosis and uterine disorders. 2024 Jun:6():. pii: 100071. doi: 10.1016/j.jeud.2024.100071. Epub 2024 Apr 1 [PubMed PMID: 38764520]
Kuroda K, Kuribayashi Y, Moriyama A, Hobo R, Motoyama H, Tsutsumi R, Sugiyama R, Sugiyama R. Comparison of resectoscope and tissue removal device in managing chronic endometritis associated with endometrial polyps. Journal of reproductive immunology. 2026 Jun:175():104878. doi: 10.1016/j.jri.2026.104878. Epub 2026 Mar 24 [PubMed PMID: 41903504]
La Torre F, Hurni Y, Farsi E, Campatelli C, Nardi E, Vannuccini S, Sorbi F, Fambrini M, Castiglione F, Petraglia F. Adenomyosis is associated with proliferative endometrial disorders. F&S science. 2026 May:7(3):260-264. doi: 10.1016/j.xfss.2026.03.001. Epub 2026 Mar 6 [PubMed PMID: 41796796]
Soiffer JL, Suresh D, Jalai C, Xu Y, Fnu S, Hussein NM, Lanjewar SD, Lin J, Scanlon LR, Lin KY, Nevadunsky NS, Isani SS. Risk of endometrial carcinoma in patients with atypical endometrial hyperplasia in a population of predominantly racial and ethnic minorities, a single institution study. Gynecologic oncology. 2026 May 30:210():77-83. doi: 10.1016/j.ygyno.2026.05.020. Epub 2026 May 30 [PubMed PMID: 42217257]
Raimondo D, Raffone A, Salucci P, Raimondo I, Capobianco G, Galatolo FA, Cimino MGCA, Travaglino A, Maletta M, Ferla S, Virgilio A, Neola D, Casadio P, Seracchioli R. Detection and Classification of Hysteroscopic Images Using Deep Learning. Cancers. 2024 Mar 28:16(7):. doi: 10.3390/cancers16071315. Epub 2024 Mar 28 [PubMed PMID: 38610993]
Goc G, Birge O. Endometrial Polyps and Subfertility in Women Under 40: Pathophysiology, Fertility Outcomes, and Clinical Management. Medicina (Kaunas, Lithuania). 2026 Apr 3:62(4):. doi: 10.3390/medicina62040692. Epub 2026 Apr 3 [PubMed PMID: 42075564]
Korczyńska L, Dąbrowska M, Kulecka M, Hennig EE, Ali M, Bałabas A, Czarnowski P, Olcha P, Łoziński T, Laganà AS, Ostrowski J, Ciebiera M, Zeber-Lubecka N. Comparative transcriptomic analysis of endometrial tissue associated with uterine fibroids and endometrial polyps. Scientific reports. 2026 Jun 8:():. doi: 10.1038/s41598-026-57099-9. Epub 2026 Jun 8 [PubMed PMID: 42259941]
Level 2 (mid-level) evidenceLebduska E, Beshear D, Spataro BM. Abnormal Uterine Bleeding. The Medical clinics of North America. 2023 Mar:107(2):235-246. doi: 10.1016/j.mcna.2022.10.014. Epub 2022 Dec 26 [PubMed PMID: 36759094]
Tsakiridis I, Giouleka S, Koutsouki G, Kostakis N, Kalogiannidis I, Kourtis A, Athanasiadis A, Goulis DG, Dagklis T. Investigation and management of abnormal uterine bleeding in reproductive-aged women: a descriptive review of national and international recommendations. The European journal of contraception & reproductive health care : the official journal of the European Society of Contraception. 2022 Dec:27(6):504-517. doi: 10.1080/13625187.2022.2112169. Epub 2022 Sep 2 [PubMed PMID: 36053280]
Sheng KK, Lyons SD. To treat or not to treat? An evidence-based practice guide for the management of endometrial polyps. Climacteric : the journal of the International Menopause Society. 2020 Aug:23(4):336-342. doi: 10.1080/13697137.2020.1742107. Epub 2020 Jun 4 [PubMed PMID: 32496825]
Chen X, Chen G, Bao D, Liu J, Zhang X. Prediction of Recurrence After Endometrial Polypectomy in Women of Childbearing Age Based on Machine Learning Algorithm. International journal of women's health. 2026:18():591932. doi: 10.2147/IJWH.S591932. Epub 2026 Mar 30 [PubMed PMID: 41938180]
Ghosh T, Choudhury S, Kumar A. Evaluation of Gynecological Mass Lesions Using Magnetic Resonance Imaging: An Observational Study. Cureus. 2026 Feb:18(2):e104200. doi: 10.7759/cureus.104200. Epub 2026 Feb 24 [PubMed PMID: 41909383]
Level 2 (mid-level) evidenceErkal N, Kaba M, Erdoğan K, Eryılmaz FEI, Sivri Z, Mayır YA. Factors associated with hysterectomy after failure of levonorgestrel-releasing intrauterine system treatment in women with abnormal uterine bleeding. BMC women's health. 2026 Mar 16:26(1):. doi: 10.1186/s12905-026-04398-y. Epub 2026 Mar 16 [PubMed PMID: 41840553]
Mak KS, Huang YT, Su YY, Pan YB, Lin YS, Weng CH, Wu KY, Chao AS, Wang CJ. Clinical outcomes in women with endometrial polyps underwent conservative management. Taiwanese journal of obstetrics & gynecology. 2023 Jul:62(4):553-558. doi: 10.1016/j.tjog.2022.08.022. Epub [PubMed PMID: 37407193]
Level 2 (mid-level) evidenceBayyarapu VB, Gundabattula SR, Rangaram P, Ashrafi S. Ultrasound-Guided Endometrial Polypectomy Performed in an Office Setting Without Hysteroscopy. Cureus. 2026 Apr:18(4):e107420. doi: 10.7759/cureus.107420. Epub 2026 Apr 20 [PubMed PMID: 42181325]
Salman A, Tambawala ZY, Saquib S, Fatima N, Waheed S, Hamza LK. Correlation of Ultrasound, Hysteroscopy, and Histology in Postmenopausal Women: A Five-Year Retrospective Observational Study in Dubai. Cureus. 2026 Mar:18(3):e106068. doi: 10.7759/cureus.106068. Epub 2026 Mar 29 [PubMed PMID: 42058345]
Level 2 (mid-level) evidenceRajaram S, Singh L, - B, Nagar S. Serous endometrial cancer with an elusive preoperative diagnosis. BMJ case reports. 2026 Mar 11:19(3):. pii: e270356. doi: 10.1136/bcr-2025-270356. Epub 2026 Mar 11 [PubMed PMID: 41813027]
Level 3 (low-level) evidenceIncognito GG, Ettore C, De Tommasi O, Tozzi R, Ettore G. Ultrasound Assessment of Retained Products of Conception (RPOC): Insights from the Current Literature. Journal of clinical medicine. 2025 Aug 19:14(16):. doi: 10.3390/jcm14165864. Epub 2025 Aug 19 [PubMed PMID: 40869690]
Gayete-Lafuente S, Mian U, Choong E, Guijarro-Baude L, Barad D, Gleicher N. Incidental endometrial cancer diagnosis during pre-IVF workup: fertility-sparing treatment and embryo preservation. JCEM case reports. 2026 Apr:4(4):luag044. doi: 10.1210/jcemcr/luag044. Epub 2026 Mar 24 [PubMed PMID: 41884088]
Level 3 (low-level) evidenceSaleem Z. Association of endometrial pathologies with infertility and malignant potential in pre- and postmenopausal women-a systematic review. The British journal of radiology. 2026 May 1:99(1181):859-865. doi: 10.1093/bjr/tqag031. Epub [PubMed PMID: 41671103]
Level 1 (high-level) evidenceHowells P, Vigneswaran K, Sarris I, Melo P, Bhandari H, Subramanian V. Management of endometrial polyps in fertility: British fertility Society policy and practice guideline. Human fertility (Cambridge, England). 2026 Dec:29(1):2633925. doi: 10.1080/14647273.2026.2633925. Epub 2026 Feb 25 [PubMed PMID: 41736557]
Level 1 (high-level) evidenceWang K, Du J, Zhao X, Zhao X, Li C. Reproductive outcomes of different management strategies after hysteroscopic resection of the uterine septum with endometrial polyps: a retrospective study. PeerJ. 2026:14():e20669. doi: 10.7717/peerj.20669. Epub 2026 Jan 28 [PubMed PMID: 41623392]
Level 2 (mid-level) evidenceMa X, Tang R, Chen R. An atypical case of adenomyosis coexisting with simple endometrial hyperplasia: A case report. Medicine. 2026 May 15:105(20):e48940. doi: 10.1097/MD.0000000000048940. Epub [PubMed PMID: 42152406]
Level 3 (low-level) evidenceBarakat M, Massoud R, Alhalabi M. Deep learning-based automated classification of endometrial lesions in IVF patients using hysteroscopic images. Scientific reports. 2026 Jun 6:():. doi: 10.1038/s41598-026-57032-0. Epub 2026 Jun 6 [PubMed PMID: 42251153]
Harada K, Kurata Y, Himoto Y, Kido A, Kirita M, Yoshida A, Matsumoto YK, Hamanishi J, Minamiguchi S, Ito H, Nakashima A, Minamisaka T, Daido S, Abiko K, Moriyoshi K, Ando K, Arizono S, Aoki T, Hara S, Mandai M, Nakamoto Y. Correction: Differentiating uterine adenosarcoma from endometrial polyps: MRI imaging features. Abdominal radiology (New York). 2026 Jun 1:():. doi: 10.1007/s00261-025-05269-0. Epub 2026 Jun 1 [PubMed PMID: 42223588]
Metwally M, McKendrick K, Ridsdale K, Pye C, Walters S, Amer S, Barr A, Chatters R, Cheong Y, Choudhary M, Connor M, Desoysa L, El-Toukhy T, Keetharuth A, Latimer N, Loban A, Mohiyiddeen L, Mostafa M, Scaife C, Stone T, Taylor L, Turtle C, White D. Removal of small fibroids and polyps in patients with infertility and recurrent miscarriage: The HELP Fertility? RCT. Health technology assessment (Winchester, England). 2026 Feb 25:():1-35. doi: 10.3310/GJMM1915. Epub 2026 Feb 25 [PubMed PMID: 41773973]
De Silva PM, Smith PP, Cooper NAM, Clark TJ, Royal College of Obstetricians and Gynaecologists. Outpatient Hysteroscopy: (Green-top Guideline no. 59). BJOG : an international journal of obstetrics and gynaecology. 2024 Dec:131(13):e86-e110. doi: 10.1111/1471-0528.17907. Epub 2024 Aug 19 [PubMed PMID: 39160077]