Introduction
Emergency department thoracotomy (EDT), also known as resuscitative thoracotomy, is a lifesaving high-acuity, low-occurrence (HALO) procedure performed to identify and address potentially repairable thoracic injuries as a bridge to definitive operative management. The procedure enables immediate therapeutic interventions for hemorrhage and circulatory control, including relief of pericardial tamponade, aortic cross-clamping, and open cardiac massage. EDT has limited indications, and overall survival remains low at approximately 7.4%. However, among survivors, approximately 92.4% achieve intact neurologic recovery.[1] The primary goals of this intervention include the following:
- Hemorrhage control through identification and management of the bleeding source
- Relief of cardiac tamponade [2][3]
- Performance of open cardiac massage [4][5]
- Exposure of the descending thoracic aorta for cross-clamping
- Repair of cardiac or pulmonary injuries [6]
EDT is typically performed in the emergency department or operating room. The emergency care provider plays a critical role in patient selection, activation of surgical support, procedural performance when indicated, airway management, blood product mobilization, and postthoracotomy resuscitation. Simulation-based training has gained increasing recognition as a valuable preparatory tool that improves provider confidence and procedural efficiency.[7][8] This activity reviews the appropriate techniques, indications, and contraindications for EDT.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The thorax is anatomically situated between the neck superiorly and the diaphragm inferiorly. Critical organs within the thorax include the bronchi, lungs, heart, and major vascular structures, including the ascending aorta, aortic arch, and descending thoracic aorta. The heart lies just left of the midline, with the aortic root centrally positioned. The aortic arch curves posterolaterally to the left, transitioning into the descending aorta, which courses adjacent to the thoracic spine. The aortic arch gives rise to 3 primary branches: the brachiocephalic trunk, the left common carotid artery, and the left subclavian artery. The brachiocephalic trunk divides into the right common carotid artery and the right subclavian artery. All aortic arch branches lie posterior to the manubrium.
The pericardial sac surrounds the heart and covers the myocardium. The left phrenic nerve courses along the lateral pericardium and supplies motor innervation to the diaphragm, enabling spontaneous respiration. The left phrenic nerve is particularly vulnerable to injury during pericardiotomy, as visualization often remains difficult for novices performing this procedure. Anterior to the aortic arch and near the left subclavian artery, the left vagus nerve gives rise to the recurrent laryngeal nerve, which innervates the vocal cord muscles responsible for phonation, before traveling posteriorly around the root of the left lung and continuing adjacent to the esophagus into the posterior mediastinum. The esophagus runs anterior to the spinal column and medial to the aorta. Placement of an orogastric tube within the esophagus can provide tactile confirmation. The thoracic duct courses anterolaterally to the spine and is often challenging to visualize. Awareness of these anatomical relationships and physiological significance is essential to prevent iatrogenic injury and improve postoperative outcomes.
Indications
According to the 2015 Practice Management Guidelines from the Eastern Association for the Surgery of Trauma (EAST), EDT is a high-acuity, last-resort intervention performed in select trauma patients presenting in extremis. Decision-making to proceed with EDT is based on mechanism of injury, duration of cardiopulmonary resuscitation (CPR), and presence of signs of life (SOL). The reported success remains exceedingly rare outside these indications, particularly in cases of blunt trauma and prolonged CPR.[9] The Western Trauma Association (WTA) further identifies profound refractory shock as an additional indication for EDT.
Strong indications for EDT include penetrating thoracic trauma with SOL, such as pupillary response, spontaneous movement, cardiac electrical activity, or respiratory effort, in the absence of a palpable pulse. Cardiac tamponade in the setting of penetrating chest trauma is also a strong indication, particularly when suspected on clinical examination or confirmed by focused assessment with sonography for trauma (FAST) ultrasound. Conditional indications include penetrating thoracic or extrathoracic trauma without SOL when CPR duration is less than 15 minutes; blunt trauma with SOL and less than 10 minutes of CPR; and witnessed traumatic arrest (penetrating or blunt) with brief prehospital downtime and SOL on emergency department arrival.
In addition to the EAST and WTA recommendations, the European Resuscitation Council guidelines outline 4 essential conditions for successful resuscitative thoracotomy, summarized as the “4 E’s”: expertise, equipment, environment, and elapsed time. The procedure should be performed by trained providers (expertise), using appropriate surgical instruments (equipment), in a resuscitation-ready setting (environment), and ideally within 10 minutes of cardiac arrest (elapsed time), as survival declines significantly beyond this window. According to these guidelines, failure to meet any of the 4 criteria constitutes a contraindication to resuscitative thoracotomy, as performance of the procedure under such conditions is considered futile and exposes the clinical team to unnecessary risk.[10]
Contraindications
EDT should not be performed in patients who continue to have vital signs, including those with hypotension but measurable blood pressure.[11] The procedure is also considered inappropriate in clearly futile clinical circumstances, such as when SOL are absent at the scene of injury, asystole presents without pericardial tamponade, pulselessness exceeds 15 minutes, or injuries are massive and nonsurvivable. Blunt trauma without signs of life is a contraindication to EDT.[12]
In the pediatric population, available evidence indicates that patients aged 0 to 14 years with blunt thoracic injury and otherwise qualifying criteria, such as witnessed loss of pulse and absence of nonsurvivable injuries, should generally not undergo EDT due to extremely poor outcomes. Patients younger than 15 to 18 years with blunt thoracic injury, as well as pediatric patients with penetrating thoracic trauma, are not considered to have a relative contraindication based on age alone.[13][14][15]
Age over 57 years may be a relative contraindication to EDT.[16][17] However, more recent data in penetrating trauma indicate that age alone does not reliably predict failure to rescue and should not exclude patients who otherwise meet favorable criteria for intervention.[18]
EDT should not be performed in the absence of immediately available resources, including operating room capability and appropriately trained surgical personnel, as the procedure functions as a temporizing measure intended to facilitate rapid transfer to definitive surgical care. [Source: American College of Surgeons. ATLS®: Advanced Trauma Life Support® Student Course Manual, 10th Edition. 2018] EDT is also contraindicated when essential equipment is unavailable, including capability for internal cardiac defibrillation. Additional contraindications include severe head injury and severe multisystem injury.[19]
Equipment
Personal protective equipment (PPE) includes sterile gloves, a gown, a mask, and a face shield or eye protection. Skin preparation requires an antiseptic solution, such as chlorhexidine gluconate (Chloraprep). Incision and dissection instruments include a scalpel with a #10 or #22 blade, trauma shears or heavy-duty scissors, and a Gigli saw, which may be used for sternal division when indicated. Hemorrhage control and repair instruments include a rib spreader (such as a Finochietto retractor), tissue forceps (such as Spencer-Wells artery forceps), needle holders in long and short configurations, non-absorbable sutures such as 2-0 silk, vascular clamps including Satinsky clamps, and an aortic cross-clamp (see Image. Emergency Department Thoracotomy Clinical Field). Additional supplies include sterile drapes and towels, laparotomy sponges, a high-volume suction device, chest tubes (typically 30F), internal defibrillator paddles, a 20F Foley catheter with a 30-mL balloon, and a skin stapler.
These items are essential for executing EDT successfully and managing the complex challenges associated with traumatic thoracic injury. Failure to secure essential equipment before the procedure should prompt reconsideration of whether EDT is appropriate.
Personnel
EDT requires a highly coordinated interprofessional team. Clear role delineation is essential to ensure efficiency under time-critical conditions. Effective communication and teamwork among physicians, nurses, and ancillary staff are essential to maximize the likelihood of successful outcomes in these high-acuity scenarios.
Resuscitation Lead
One clinician should serve as the resuscitation lead, coordinating ongoing resuscitative efforts, including Advanced Cardiovascular Life Support measures, such as airway management and blood product administration. This clinician should work alongside a nurse responsible for preparing and administering medications, setting up defibrillation equipment when indicated, and documenting interventions in real time.
Procedural Team
A second clinician, ideally the most experienced available provider, should perform the thoracotomy. A dedicated assistant should support the procedure by facilitating exposure, passing instruments, managing suction, and assisting with key steps, such as pericardiotomy, aortic cross-clamping, and cardiac repair. A circulating nurse or scrub nurse should assist by maintaining sterility, preparing instruments, and anticipating procedural needs.
Nursing Support
Additional nursing personnel should be assigned to maintain intravenous access, manage fluid and blood product administration, coordinate with the blood bank, and ensure availability of surgical supplies and medications. One nurse should also assist with preparation for transport to the operating room if return of spontaneous circulation is achieved.
Surgical Coordination
Surgical coordination should simultaneously activate a pathway to definitive care, including immediate notification of the trauma surgeon, operating room team, and intensive care unit staff. Preparations should ensure that surgical instruments, transfusion support, and postoperative critical care resources are readily available.
Preparation
EDT is an emergent procedure that allows little time for preparation once indicated. Most preparation should occur in advance of the need for intervention, including familiarization with equipment location and proper use. Providers should be well-versed in procedural steps and indications for EDT. All personnel and equipment should ideally be assembled and immediately available prior to initiation of the procedure.
Antibiotics are recommended before cardiothoracic surgery. However, EDT should not be delayed for antibiotic administration. All personnel involved in resuscitative efforts should follow universal precautions by using gowns, gloves, and eye protection.
Technique or Treatment
The patient should be positioned supine with both arms abducted to 90° and extended. A left-sided approach is generally used, as it provides access to the left thorax, pericardium, heart, and aorta (see Image. Surgical Incision Pathways for Thoracotomy Procedures). A skin incision is made with a #10 blade scalpel from the sternum through the 4th or 5th intercostal space below the nipple and extended laterally to the posterior midaxillary line following the curvature of the ribs. Breast tissue should be retracted superiorly. The initial incision passes through skin and subcutaneous fat and may extend to the ribs in lean patients.
A right-sided approach may be used when right thoracic bleeding is suspected. Extension of the incision from left to right inferior to the sternum creates a clamshell incision, which exposes the anterior mediastinum, aortic arch, and great vessels. Ongoing debate exists regarding the optimal approach, with some authors suggesting that, for emergency providers with limited procedural familiarity and incomplete injury information, the clamshell incision should be preferred.[20]
A 1- to 2-inch incision should be made laterally to avoid cardiac injury, along the superior margin of the inferior rib to avoid the intercostal neurovascular bundle (see Image. Dissection of the Left Posterior Thoracic Wall Showing Intercostal Spaces 3 and 4). The incision should penetrate and separate the intercostal muscles and parietal pleura, with care taken to avoid injury to the underlying lung tissue. Mayo scissors or sterile trauma shears are then used to extend the incision from the initial defect anteriorly toward the sternum, separating the intercostal muscles. The incision is completed by extending posteriorly toward the posterior midaxillary line.
After entry into the chest, a rib spreader is inserted between the ribs with the arm directed toward the axilla and the ratchet bar oriented inferiorly. The rib spreader is then expanded maximally to optimize exposure.
Optional right mainstem bronchus intubation may reduce left lung ventilation and further improve exposure after entry into the chest. Visible bleeding should be controlled with direct pressure or laparotomy sponges. Vascular clamps should be reserved for last-resort use. Bleeding from major pulmonary vasculature may be controlled by direct clamping of injured lung tissue or vessel, clamping of the pulmonary hilum, or using the “pulmonary hilar twist” maneuver to reduce the risk of air embolism.
Further damage control measures are reasonable prior to pericardiotomy if no pericardial effusion or apparent pericardial injury is present. Open cardiac massage may be performed with the pericardium intact.
Pericardiotomy should be performed if the myocardium cannot be visualized through the pericardium, and the heart should be delivered from the pericardial sac. The phrenic nerve should be identified along the lateral pericardium and protected from injury during pericardiectomy. The pericardium should be grasped with toothed forceps, and a small incision should be made with a scalpel or scissors, avoiding injury to the myocardium and phrenic nerve. This incision is extended parallel to the phrenic nerve in a superior direction and should expose the great vessels. Pericardial fluid and clot should be removed, followed by evaluation of the great vessels. The heart should then be delivered from the pericardial sac.
The heart should be palpated for injury and inspected for bleeding or hemorrhage. Bleeding should initially be controlled with direct pressure. If direct pressure proves insufficient or hemorrhage is too brisk, further interventions that may be considered include ligation with suture, closure of the laceration with staples, or insertion of the tip of a Foley catheter with balloon inflation followed by gentle traction to achieve internal compression. The Foley catheter technique is most effective for ventricular puncture injuries, where the catheter tip is inserted into the defect, and the balloon is inflated to tamponade bleeding.
Superficial myocardial lacerations or cardiac vessel injuries may be managed with temporary repair using sutures or staples to control hemorrhage until definitive surgical repair in the operating theater. Care should be taken to avoid tamponade or ligation of a coronary vessel.
Next, the aorta is typically cross-clamped to improve cerebral perfusion. Aortic cross-clamping should be avoided in normotensive patients due to increased afterload and reduced cardiac perfusion.[21]
The left lung is retracted superiorly, and the pulmonary ligament is divided. The esophagus may be differentiated from the aorta by palpation of a nasogastric or orogastric tube within the esophageal lumen. The overlying pleura is then separated, and the aorta is mobilized from the esophagus and the vertebral column posteriorly, creating sufficient space for cross-clamping. Aortic cross-clamping should be performed within an intervertebral space to reduce the risk of intercostal vessel injury. Optimal clamp placement is just above the diaphragm, although placement just below the left pulmonary hilum may also be used when required.
Advanced Cardiovascular Life Support and Advanced Trauma Life Support resuscitative measures may continue following aortic cross-clamping. Open cardiac massage and internal defibrillation may be performed as indicated.
Complications
EDT is a lifesaving procedure. However, potential benefits must be weighed against the risk of complications before administering this intervention.
Operator injury is a frequent complication, and appropriate use of PPE is the primary preventive measure. Occupational exposure to blood-borne pathogens, such as HIV, is slightly higher than baseline risk, although strict adherence to PPE use significantly reduces exposure risk.[22]
Rib transection may occur during the primary incision, creating sharp edges capable of injuring the operator. A curvilinear incision following the rib contour is essential to minimize this risk. Use of a scalpel for deep thoracic entry may also cause inadvertent injury to the pericardium and underlying structures. Such iatrogenic injury is most effectively avoided by using Mayo scissors to divide intercostal muscles and soft tissues under controlled dissection.
Pericardiotomy carries a risk of phrenic nerve damage. Coronary artery injury may occur during cardiac exposure and manipulation. A functional understanding of thoracic anatomy and operative technique is essential to minimize inadvertent structural injury.
Complete exposure of the aorta is required to prevent incomplete cross-clamping, inadvertent clamping of the esophagus, or simultaneous clamping of the esophagus with the aorta. Additional complications include phrenic nerve injury, distal organ ischemia secondary to aortic cross-clamping, and recurrent hemorrhage from the chest wall or internal mammary artery.[23]
Clinical Significance
Indications for EDT have evolved significantly over the past 6 decades based on increasing clinical experience and more robust outcome data.[24] The procedure may be lifesaving when performed in appropriately selected patients, particularly those with penetrating thoracic injuries and SOL, with measurable reductions in mortality in select clinical scenarios.
Despite these potential benefits, overall morbidity and mortality associated with EDT remain high. Reported survival rates range from less than 1% to 35%, depending on mechanism of injury, location of major injury, and presence of physiologic SOL at presentation.[25] Outcomes are notably improved in penetrating trauma, with survivability approaching 8.8%, and, in isolated cardiac injuries, survival approximating 20%. Presence of SOL on hospital arrival is associated with approximately 11.5% survival. The survival rate after EDT for blunt trauma is extremely low, particularly in the absence of witnessed SOL in the hospital, with even poorer outcomes when SOL are absent in the field.
At present, no strong consensus supports the routine use of EDT in blunt trauma, and most guidelines recommend its administration only in cases with clearly defined indications and SOL present on arrival to the emergency department. Inappropriately performed thoracotomies contribute to resource overutilization, increased occupational risk, and reduced likelihood of favorable outcomes. Up-to-date knowledge of EDT indications, contraindications, and techniques remains critical for appropriate application. Continued education, review of cases, and adherence to institutional protocols may reduce futile interventions and improve decision-making in the emergency department.
Enhancing Healthcare Team Outcomes
EDT is a last-resort intervention for lifesaving treatment in a narrowly defined patient population. Resuscitation of patients undergoing EDT requires an interprofessional team, including an emergency medicine physician, nurses, and, potentially, assistants, technicians, or other available staff. EDT cannot be performed in isolation, and coordinated team function improves efficiency and outcomes. A trauma surgeon and supporting staff are often present during the procedure. When not immediately available, the surgical team should be activated without delay to provide definitive operative management.
Clear identification of appropriate candidates for EDT may improve outcomes by reducing futile intervention in patients with unsurvivable injuries. Review of procedural steps and anticipated next actions may further enhance interprofessional communication and workflow efficiency during time-critical resuscitation.[26]
Media
(Click Image to Enlarge)
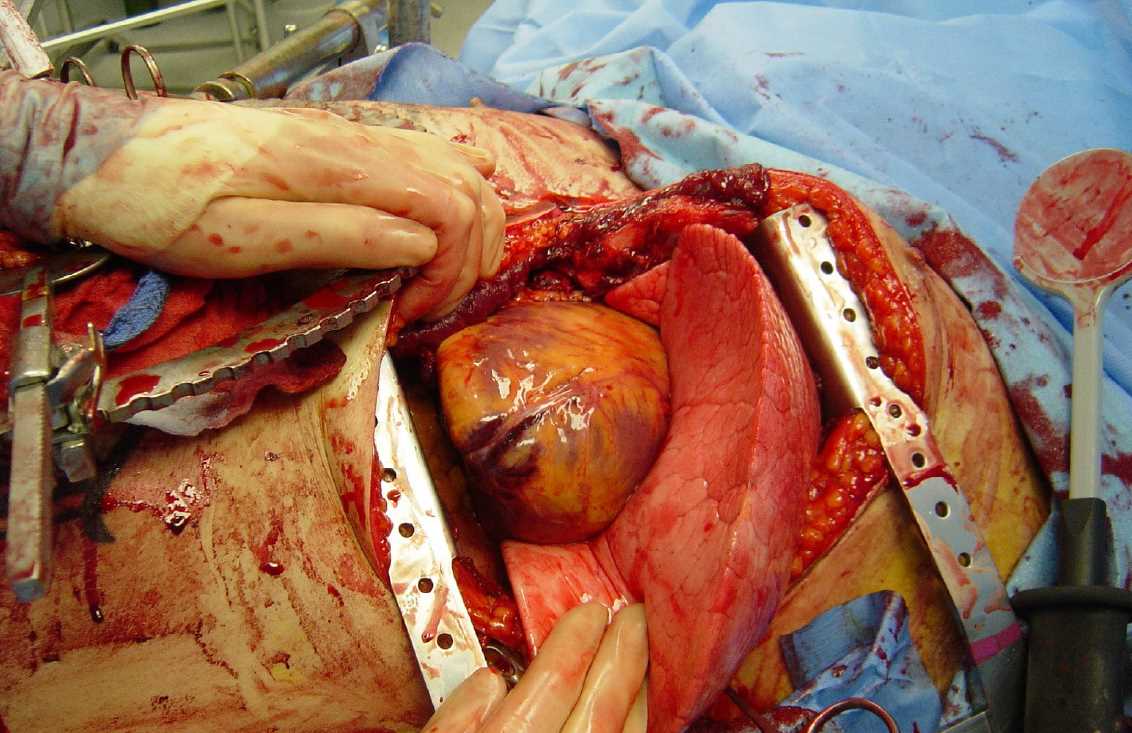
Emergency Department Thoracotomy Clinical Field. This image shows an emergency department thoracotomy performed to manage critical thoracic trauma. A Finochietto rib retractor is placed to open the left anterolateral intercostal space widely, providing rapid direct exposure of the heart within the pericardial sac and the adjacent lung field for immediate resuscitation.
Contributed by Wikimedia Commons (CC BY 2.0) https://creativecommons.org/licenses/by/2.0/deed.en
(Click Image to Enlarge)
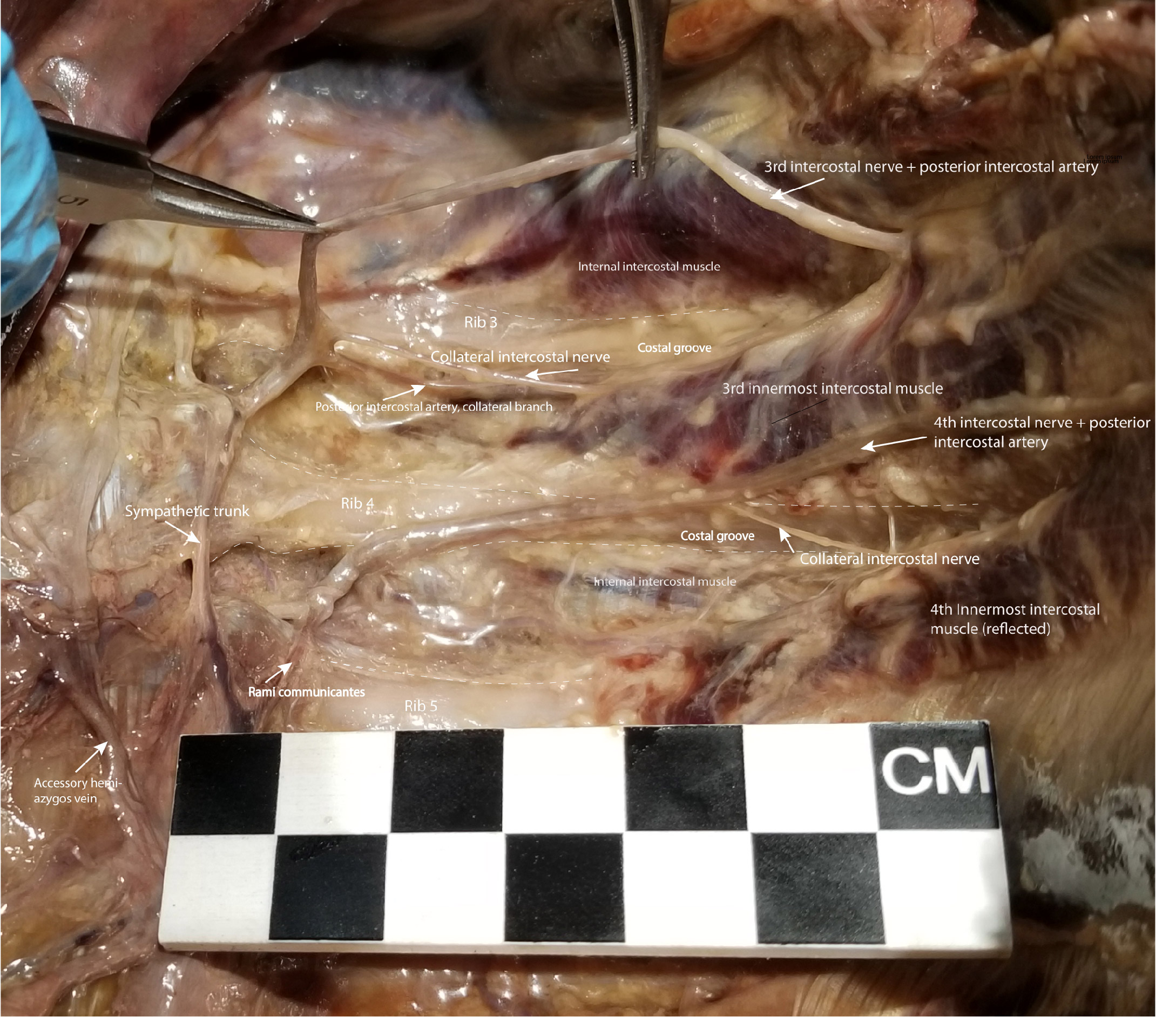
Dissection of the Left Posterior Thoracic Wall Showing Intercostal Spaces 3 and 4. The intercostal neurovascular bundle, including intercostal nerve 3, has been elevated from the costal groove to demonstrate the collateral intercostal nerve branching near the rib angle. The collateral intercostal nerve is vulnerable to injury during thoracotomy because of its location immediately superior to the rib. To minimize injury to the intercostal nerve and its collateral branch, surgical entry into the intercostal space should be performed midway between the superior and inferior rib borders. Also visible are ribs 3 through 5, the 4th intercostal nerve and posterior intercostal artery, collateral branches of the posterior intercostal arteries, the internal and innermost intercostal muscles, costal grooves, the sympathetic trunk, rami communicantes, and the accessory hemiazygos vein.
Contributed by NT Boaz, MD. Dissection by K Meshida, R Bernor, and NT Boaz, MD
(Click Image to Enlarge)
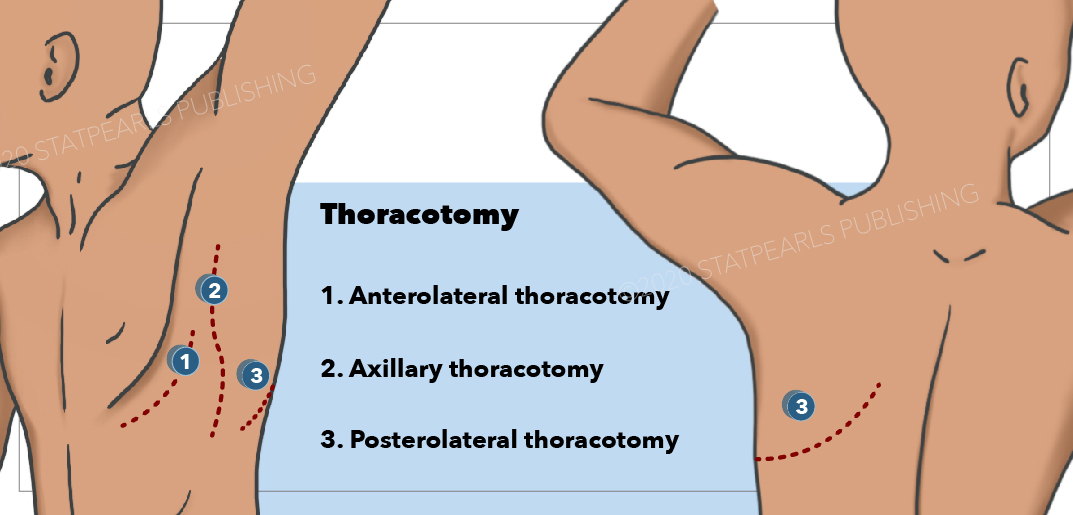
Surgical Incision Pathways for Thoracotomy Procedures. This illustration maps out the standard anatomical landmarks and skin incision lines utilized for exposing the thoracic cavity. The diagram details 3 primary surgical approaches: anterolateral, axillary, and posterolateral.
StatPearls Publishing
References
Rhee PM, Acosta J, Bridgeman A, Wang D, Jordan M, Rich N. Survival after emergency department thoracotomy: review of published data from the past 25 years. Journal of the American College of Surgeons. 2000 Mar:190(3):288-98 [PubMed PMID: 10703853]
Level 2 (mid-level) evidenceMenaker J, Cushman J, Vermillion JM, Rosenthal RE, Scalea TM. Ultrasound-diagnosed cardiac tamponade after blunt abdominal trauma-treated with emergent thoracotomy. The Journal of emergency medicine. 2007 Jan:32(1):99-103 [PubMed PMID: 17239739]
Level 3 (low-level) evidenceLeidel BA, Kanz KG, Kirchhoff C, Bürklein D, Wismüller A, Mutschler W. [Cardiac arrest following blunt chest injury. Emergency thoracotomy without ifs or buts?]. Der Unfallchirurg. 2007 Oct:110(10):884-90 [PubMed PMID: 17909734]
Level 3 (low-level) evidenceBoczar ME, Howard MA, Rivers EP, Martin GB, Horst HM, Lewandowski C, Tomlanovich MC, Nowak RM. A technique revisited: hemodynamic comparison of closed- and open-chest cardiac massage during human cardiopulmonary resuscitation. Critical care medicine. 1995 Mar:23(3):498-503 [PubMed PMID: 7874901]
Jackson RE, Freeman SB. Hemodynamics of cardiac massage. Emergency medicine clinics of North America. 1983 Dec:1(3):501-13 [PubMed PMID: 6396069]
Level 3 (low-level) evidenceKirkpatrick AW, Ball CG, D'Amours SK, Zygun D. Acute resuscitation of the unstable adult trauma patient: bedside diagnosis and therapy. Canadian journal of surgery. Journal canadien de chirurgie. 2008 Feb:51(1):57-69 [PubMed PMID: 18248707]
Misra A, Chapman A, Watson WD, Bach JA, Bonta MJ, Elliott JO, Dominguez EP. Use of Low-Cost Task Trainer for Emergency Department Thoracotomy Training in General Surgery Residency Program. Journal of surgical education. 2024 Jan:81(1):134-144. doi: 10.1016/j.jsurg.2023.09.009. Epub 2023 Nov 4 [PubMed PMID: 37926660]
Clifford E, Stourton F, Willers J, Colucci G. Development of a Low-Cost, High-Fidelity, Reusable Model to Simulate Clamshell Thoracotomy. Surgical innovation. 2023 Dec:30(6):739-744. doi: 10.1177/15533506231208572. Epub 2023 Oct 24 [PubMed PMID: 37876028]
Yamamoto R, Suzuki M, Nakama R, Kase K, Sekine K, Kurihara T, Sasaki J. Impact of cardiopulmonary resuscitation time on the effectiveness of emergency department thoracotomy after blunt trauma. European journal of trauma and emergency surgery : official publication of the European Trauma Society. 2019 Aug:45(4):697-704. doi: 10.1007/s00068-018-0967-y. Epub 2018 May 31 [PubMed PMID: 29855670]
Greif R, Lauridsen KG, Djärv T, Ek JE, Monnelly V, Monsieurs KG, Nikolaou N, Olasveengen TM, Semeraro F, Spartinou A, Yeung J, Baldi E, Biarent D, Djakow J, van Gils M, van Goor S, Gräsner JT, Hogeveen M, Karageorgos V, Lott C, Madar J, Nabecker S, de Raad T, Raffay V, Rogers J, Sandroni C, Schnaubelt S, Smyth MA, Soar J, Wittig J, Perkins GD, Nolan JP, European Resuscitation Council Guidelines 2025 Collaborator Group. European Resuscitation Council Guidelines 2025 Executive Summary. Resuscitation. 2025 Oct:215 Suppl 1():110770. doi: 10.1016/j.resuscitation.2025.110770. Epub [PubMed PMID: 41117573]
L'Huillier JC, Jalal K, Nohra E, Boccardo JD, Olafuyi O, Jordan MB, Myneni AA, Schwaitzberg SD, Flynn WJ Jr, Brewer JJ, Noyes K, Cooper CA. Challenging Dogma by Skipping the Emergency Department Thoracotomy: A Propensity Score Matched Analysis of the Trauma Quality Improvement Database. The Journal of surgical research. 2024 Jun:298():24-35. doi: 10.1016/j.jss.2024.02.020. Epub 2024 Mar 28 [PubMed PMID: 38552587]
Level 2 (mid-level) evidencePanossian VS, Nederpelt CJ, El Hechi MW, Chang DC, Mendoza AE, Saillant NN, Velmahos GC, Kaafarani HMA. Emergency Resuscitative Thoracotomy: A Nationwide Analysis of Outcomes and Predictors of Futility. The Journal of surgical research. 2020 Nov:255():486-494. doi: 10.1016/j.jss.2020.05.048. Epub 2020 Jul 1 [PubMed PMID: 32622163]
Moskowitz EE, Burlew CC, Kulungowski AM, Bensard DD. Survival after emergency department thoracotomy in the pediatric trauma population: a review of published data. Pediatric surgery international. 2018 Aug:34(8):857-860. doi: 10.1007/s00383-018-4290-9. Epub 2018 Jun 6 [PubMed PMID: 29876644]
Selesner L, Yorkgitis B, Martin M, Ng G, Mukherjee K, Ignacio R, Freeman J, Wong LY, Durbin S, Crandall M, Longshore SW, Gerall C, Flynn-O'Brien KT, Jafri M. Emergency department thoracotomy in children: A Pediatric Trauma Society, Western Trauma Association, and Eastern Association for the Surgery of Trauma systematic review and practice management guideline. The journal of trauma and acute care surgery. 2023 Sep 1:95(3):432-441. doi: 10.1097/TA.0000000000003879. Epub 2023 Mar 11 [PubMed PMID: 37608453]
Level 1 (high-level) evidencePrieto JM, Van Gent JM, Calvo RY, Rooney AS, Martin MJ, Sise MJ, Sise CB, Lazar DA, Bansal V, Ignacio RC. Nationwide analysis of resuscitative thoracotomy in pediatric trauma: Time to differentiate from adult guidelines? The journal of trauma and acute care surgery. 2020 Oct:89(4):686-690. doi: 10.1097/TA.0000000000002869. Epub [PubMed PMID: 33017132]
Gil LA, Anstadt MJ, Kothari AN, Javorski MJ, Gonzalez RP, Luchette FA. The National Trauma Data Bank story for emergency department thoracotomy: How old is too old? Surgery. 2018 Mar:163(3):515-521. doi: 10.1016/j.surg.2017.12.011. Epub 2018 Feb 3 [PubMed PMID: 29398037]
Okano H, Terayama T, Okamoto H, Yamazaki T. Emergency resuscitative thoracotomy in severe trauma: Analysis of the nation-wide registry data in Japan. Acute medicine & surgery. 2024 Jan-Dec:11(1):e958. doi: 10.1002/ams2.958. Epub 2024 Apr 24 [PubMed PMID: 38660025]
Levin JH, Estroff JM, Zebley J, Butano V, Pierce A, Panahi A, Amdur R, Sarani B. Age Does Not Predict Failure to Rescue Following Resuscitative Thoracotomy in Penetrating Trauma. The Journal of emergency medicine. 2021 Jul:61(1):12-18. doi: 10.1016/j.jemermed.2021.01.021. Epub 2021 Feb 20 [PubMed PMID: 33618932]
Hatchimonji JS, Meredyth NA, Gummadi S, Kaufman EJ, Yelon JA, Cannon JW, Martin ND, Seamon MJ. The role of emergency department thoracotomy in patients with cranial gunshot wounds. The journal of trauma and acute care surgery. 2024 Aug 1:97(2):220-224. doi: 10.1097/TA.0000000000004282. Epub 2024 Feb 20 [PubMed PMID: 38374530]
Simms ER, Flaris AN, Franchino X, Thomas MS, Caillot JL, Voiglio EJ. Bilateral anterior thoracotomy (clamshell incision) is the ideal emergency thoracotomy incision: an anatomic study. World journal of surgery. 2013 Jun:37(6):1277-85. doi: 10.1007/s00268-013-1961-5. Epub [PubMed PMID: 23435679]
Garcia-Rinaldi R, Defore WW, Mattox KL, Beall AC Jr. Unimpaired renal, myocardial and neurologic function after cross clamping of the thoracic aorta. Surgery, gynecology & obstetrics. 1976 Aug:143(2):249-52 [PubMed PMID: 941082]
Nunn A, Prakash P, Inaba K, Escalante A, Maher Z, Yamaguchi S, Kim DY, Maciel J, Chiu WC, Drumheller B, Hazelton JP, Mukherjee K, Luo-Owen X, Nygaard RM, Marek AP, Morse BC, Fitzgerald CA, Bosarge PL, Jawa RS, Rowell SE, Magnotti LJ, Ong AW, Brahmbhatt TS, Grossman MD, Seamon MJ. Occupational exposure during emergency department thoracotomy: A prospective, multi-institution study. The journal of trauma and acute care surgery. 2018 Jul:85(1):78-84. doi: 10.1097/TA.0000000000001940. Epub [PubMed PMID: 29664893]
Preus R, Zeidan M, Posey C, Vira A, Miller S, Capasso T, Williams A, Butts C, Kinnard C, Simmons J, Lee YL, Mbaka M. Occupational Exposures During Emergency Department Thoracotomies. The Journal of surgical research. 2025 Jan:305():145-149. doi: 10.1016/j.jss.2024.11.019. Epub 2024 Dec 16 [PubMed PMID: 39689663]
Beall AC Jr, Diethrich EB, Crawford HW, Cooley DA, De Bakey ME. Surgical management of penetrating cardiac injuries. American journal of surgery. 1966 Nov:112(5):686-92 [PubMed PMID: 5332266]
Aseni P, Rizzetto F, Grande AM, Bini R, Sammartano F, Vezzulli F, Vertemati M. Emergency Department Resuscitative Thoracotomy: Indications, surgical procedure and outcome. A narrative review. American journal of surgery. 2021 May:221(5):1082-1092. doi: 10.1016/j.amjsurg.2020.09.038. Epub 2020 Oct 2 [PubMed PMID: 33032791]
Level 3 (low-level) evidenceFitzgerald MC, Yong MS, Martin K, Zimmet A, Marasco SF, Mathew J, Smit V, Yeung M, Tan GA, Marquez M, Cheung Z, Boo E, Mitra B. Emergency department resuscitative thoracotomy at an adult major trauma centre: Outcomes following a training programme with standardised indications. Emergency medicine Australasia : EMA. 2020 Aug:32(4):657-662. doi: 10.1111/1742-6723.13530. Epub 2020 May 13 [PubMed PMID: 32400039]