Introduction
Despite advances in diagnostic imaging and technology, physical examination of the respiratory system remains a cornerstone in the evaluation of respiratory disease. Chest auscultation is a safe, noninvasive, cost-effective technique that often reveals abnormalities associated with common pulmonary conditions.[1] Egophony is an abnormal auscultatory finding characterized by increased resonance and altered transmission of voice sounds heard over the lungs. When a patient is asked to say the vowel sound E, the examiner hears a nasal, A-like sound, classically described as resembling the bleating of a goat. This phenomenon, also referred to as the E-to-A change, reflects an alteration in the timbre of the transmitted voice.[2]
Egophony occurs when normal air-filled lung tissue becomes consolidated, compressed, or surrounded by fluid. Under normal conditions, air within the alveoli dampens sound transmission.[1] In contrast, consolidation or compression of lung tissue alters acoustic properties by selectively transmitting certain sound frequencies. As a result, the lower-frequency components of the spoken vowel E are attenuated, whereas higher-frequency components are preferentially transmitted, causing the perceived transformation to an A sound.
With pulmonary consolidation, such as pneumonia, the dense inflammatory exudate creates a medium that enhances transmission of higher-frequency sounds, producing egophony over the affected area. Likewise, in patients with pleural effusion, fluid accumulation in the pleural space compresses the adjacent lung parenchyma, thereby altering sound conduction (see Image. Consolidation and Pleural Effusion). Clinicians characteristically appreciate egophony at the upper margin of a pleural effusion, where compressed lung tissue borders the fluid layer. Recognizing egophony allows healthcare professionals to correlate physical examination findings with underlying pathology and supports the timely diagnosis of conditions such as pneumonia and pleural effusion.
Indications
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Indications
Evaluating for egophony is most clinically useful when assessing patients with suspected pneumonia, pleural effusion, or lung consolidation, as it helps distinguish fluid-filled or consolidated lung tissue from normal aerated lung or simple pleural effusion. Examining for egophony is not a screening maneuver for all patients but is used in specific clinical contexts.
Clinicians should assess for egophony in patients with the following findings or conditions:
- Suspected pneumonia where egophony may be present over areas of consolidation with patent airways,
- Suspected pleural effusion where egophony may be elicited just above the fluid level, helping to delineate the superior border of the effusion.
- Unexplained dyspnea or abnormal breath sounds requiring differentiation between consolidation, atelectasis, or effusion.
- Evaluation of focal lung pathology when imaging is unavailable or delayed.[3][4][5][6]
In contemporary practice, egophony remains a useful bedside finding when integrated with other examination findings such as percussion, fremitus, and breath sounds to guide decisions about imaging and empiric treatment, particularly in resource-limited settings where immediate radiography may not be available. However, egophony remains 1 component of the vocal resonance assessment.
Technique or Treatment
Examination Method
Inspection, percussion, palpation, and auscultation are essential components of the chest examination. Adventitious sounds provide clues regarding the underlying respiratory disease. Clinicians should auscultate the lungs in a quiet room, with the stethoscope diaphragm in direct contact with the skin. The anterior and posterior chest walls, as well as the axillary regions, should be examined. Clinicians should assess the symmetry, quality, and intensity of breath sounds throughout the respiratory cycle. Normal breath sounds include vesicular, bronchovesicular, and bronchial sounds. Vesicular breath sounds are low-pitched, soft, rustling sounds characterized by a prolonged inspiratory phase and a short, faint expiratory phase. These sounds result from airflow through the small airways and alveoli and are normally heard over most peripheral lung fields.
Bronchovesicular breath sounds are medium-pitched sounds produced by airflow through larger airways. These sounds are normally heard between the scapulae on the posterior chest and in the first and second intercostal spaces along the sternal borders anteriorly.
Bronchial breath sounds, best heard over the trachea, are loud, high-pitched, and hollow, with a longer expiratory than inspiratory phase and a distinct pause between phases. Bronchial breath sounds heard over peripheral lung fields are abnormal and suggest underlying pathology, including:
- Pulmonary consolidation (eg, pneumonia)
- Pleural effusion (typically heard just above the level of the effusion)
- Atelectasis with a patent bronchus
- Pulmonary fibrosis
- Lung mass over a patent bronchus
Abnormal Voice Sounds
When air passes through the vocal cords, they vibrate, producing sound. In healthy, air-filled lungs, these sounds are poorly transmitted to the chest wall and are not distinctly audible during auscultation. When lung tissue becomes consolidated or compressed by fluid, sound transmission increases, allowing clinicians to appreciate voice sounds more clearly.
Egophony is a type of abnormal voice sound. During auscultation, the clinician asks the patient to say E. In areas of abnormal lung transmission, the clinician appreciates a nasal A, classically described as resembling the bleating of a goat. Egophony is most commonly associated with pulmonary consolidation, such as pneumonia, and is noted just above the level of a pleural effusion, where compressed lung tissue transmits higher-frequency sounds more efficiently.
Bronchophony is assessed by asking the patient to speak normally (eg, ninety-nine) and is present when the patient's voice sounds abnormally loud and clear without distortion. The presence of bronchophony reflects enhanced sound transmission through dense lung tissue, most commonly due to lung consolidation or a mass over a patent bronchus.
Whispered pectoriloquy is assessed by asking the patient to whisper a phrase such as 1-2-3 and is present when the clinician clearly and distinctly hears the whispered words, indicating enhanced transmission of low-amplitude sounds through consolidated lung tissue, most commonly observed in early or subtle lung consolidation, such as pneumonia.
Clinical Significance
Key Clinical Findings in Pneumonia
In addition to egophony, the most important clinical findings for diagnosing pneumonia include abnormal vital signs, such as fever, tachypnea, tachycardia, and oxygen saturation; crackles on auscultation; decreased breath sounds; dullness to percussion; and the overall clinical impression.[7] With a sensitivity of 93%, the absence of abnormal vital signs is the most useful finding for excluding pneumonia.[7] Crackles (rales) are the most consistently helpful auscultatory finding, and dullness to percussion is highly specific (94%) for pneumonia when present. The clinician's overall clinical impression of community-acquired pneumonia carries the highest positive likelihood ratio. Additional findings are bronchial breath sounds appreciated on auscultation and increased tactile fremitus over the affected lung. Please see StatPearls' companion resource, "Community Acquired Pneumonia," for further information.
Key Clinical Findings in Pleural Effusion
The 2 most important findings associated with the diagnosis of a pleural effusion are dullness to percussion and unequal chest expansion. The absence of reduced tactile vocal fremitus makes pleural effusion less likely. Decreased vocal resonance, crackles, a pleural friction rub, or decreased or absent breath sounds over the fluid are additional potential findings. However, near the upper border, breath sounds may be accentuated due to increased conduction through the partially atelectatic lung compressed by the fluid.[8] Please see StatPearls' companion resource, "Pleural Effusion," for further information.
Clinical Utility of Egophony in Routine Practice
Clinicians must understand the clinical utility of egophony within the broader context of physical examination. No single maneuver is uniformly highly sensitive or highly specific for pneumonia or pleural effusion. Lung auscultation remains an essential part of the physical examination, but its usefulness depends on proper correlation with available clinical information.[9]
The available evidence supports egophony as a highly specific but infrequently observed bedside finding that functions best as a confirmatory rather than screening tool. Meta-analyses demonstrate that egophony has high specificity and a strong positive likelihood ratio for pneumonia and pleural effusion, indicating that its presence substantially increases diagnostic probability.[10][11][12] However, because egophony is uncommon and has low sensitivity, its absence does not reliably exclude disease. Current guidelines emphasize that normal vital signs are more effective for ruling out pneumonia. In contrast, more common auscultatory findings, such as crackles or decreased breath sounds, are more useful for initial assessment.
When identified in patients with compatible symptoms, abnormal vital signs, or other concerning examination findings, egophony adds meaningful diagnostic value by increasing the pretest probability of lung consolidation. The presence of egophony helps clinicians justify and prioritize chest imaging, particularly chest radiography, and guides focused interpretation by localizing disease to a specific lung region. In resource-limited settings or when imaging is delayed, egophony can inform early clinical decision-making, including the initiation of empiric therapy.[11] Early recognition of egophony may also help clinicians distinguish and localize a pleural effusion from alternative causes of abnormal lung examination findings, such as consolidation alone. This distinction can prompt timely interventions, including diagnostic thoracentesis when indicated. Although inter-examiner reliability varies, this highlights the importance of clinician training rather than diminishing the clinical relevance of egophony.[13] When integrated with other physical findings and clinical data, egophony remains a high-yield bedside sign that enhances diagnostic confidence and reinforces the value of skilled physical examination in modern practice.
Enhancing Healthcare Team Outcomes
Egophony is a classic auscultatory finding characterized by an alteration in the quality of transmitted voice sounds during lung examination, in which a spoken E is heard as a nasal A. This finding occurs when normally air-filled lung tissue becomes consolidated or compressed, most commonly in conditions such as pneumonia or at the upper border of a pleural effusion. The consolidated lung preferentially transmits higher-frequency sound vibrations, allowing voice sounds to be heard more clearly and with altered resonance. Although egophony is an infrequent finding, it is highly specific and, when present, significantly increases diagnostic confidence for focal lung pathology. As a bedside, low-cost, and noninvasive maneuver, egophony remains a valuable adjunct to modern diagnostic evaluation when integrated with clinical context and other examination findings.
Effective use of egophony requires coordinated skills and strategies across the interprofessional healthcare team. Clinicians and advanced practitioners apply auscultatory findings within clinical reasoning to guide diagnostic prioritization, imaging decisions, and early treatment. Nurses play a critical role in identifying respiratory changes, reporting abnormal breath sounds, and reinforcing timely reassessment. Pharmacists contribute by aligning antimicrobial therapy and supportive medications with suspected pulmonary diagnoses, improving safety and therapeutic effectiveness. Respiratory therapists and other healthcare professionals support comprehensive pulmonary assessment and monitoring. Clear interprofessional communication ensures that abnormal physical findings such as egophony are accurately conveyed, contextualized, and acted upon. Coordinated care enhances patient-centered outcomes by promoting earlier diagnosis, reducing unnecessary testing, improving patient understanding at the bedside, and strengthening team performance through shared clinical awareness and collaboration.
Media
(Click Image to Enlarge)
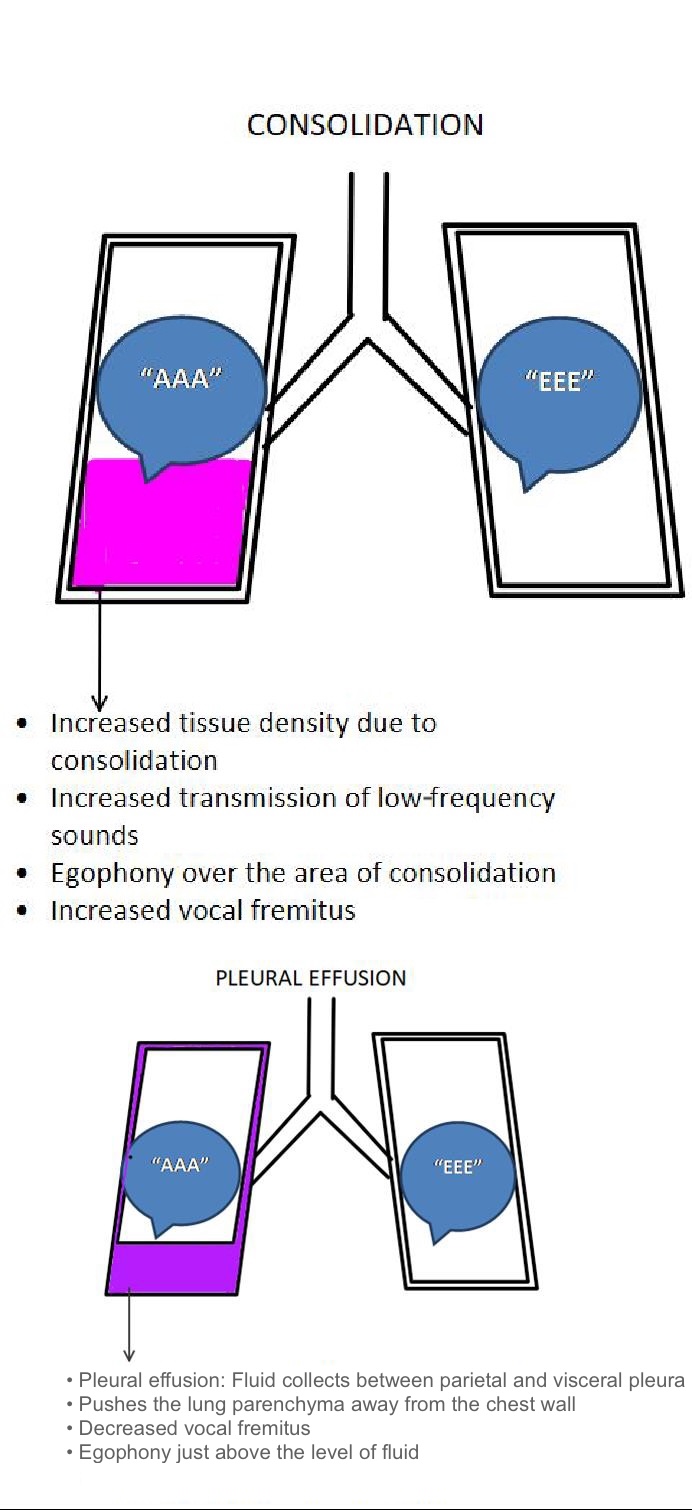
Consolidation and Pleural Effusion. The image shows a comparison between pulmonary consolidation and pleural effusion. In consolidation (eg, pneumonia), the dense inflammatory exudate creates a medium that enhances transmission of higher-frequency sounds, producing egophony over the affected area. In pleural effusion, fluid accumulation in the pleural space compresses the adjacent lung parenchyma, thereby altering sound conduction
Contributed by P Modi, MD
References
Sarkar M, Madabhavi I, Niranjan N, Dogra M. Auscultation of the respiratory system. Annals of thoracic medicine. 2015 Jul-Sep:10(3):158-68. doi: 10.4103/1817-1737.160831. Epub [PubMed PMID: 26229557]
Sapira JD. About egophony. Chest. 1995 Sep:108(3):865-7 [PubMed PMID: 7656646]
Bohadana A, Izbicki G, Kraman SS. Fundamentals of lung auscultation. The New England journal of medicine. 2014 Feb 20:370(8):744-51. doi: 10.1056/NEJMra1302901. Epub [PubMed PMID: 24552321]
Wong CL, Holroyd-Leduc J, Straus SE. Does this patient have a pleural effusion? JAMA. 2009 Jan 21:301(3):309-17. doi: 10.1001/jama.2008.937. Epub [PubMed PMID: 19155458]
Shellenberger RA, Balakrishnan B, Avula S, Ebel A, Shaik S. Diagnostic value of the physical examination in patients with dyspnea. Cleveland Clinic journal of medicine. 2017 Dec:84(12):943-950. doi: 10.3949/ccjm.84a.16127. Epub [PubMed PMID: 29244648]
Kalantri S, Joshi R, Lokhande T, Singh A, Morgan M, Colford JM Jr, Pai M. Accuracy and reliability of physical signs in the diagnosis of pleural effusion. Respiratory medicine. 2007 Mar:101(3):431-8 [PubMed PMID: 16965906]
Ebell MH, Chupp H, Cai X, Bentivegna M, Kearney M. Accuracy of Signs and Symptoms for the Diagnosis of Community-acquired Pneumonia: A Meta-analysis. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2020 Jul:27(7):541-553. doi: 10.1111/acem.13965. Epub 2020 Apr 24 [PubMed PMID: 32329557]
Level 1 (high-level) evidenceSutton AE, Modi P. Vocal Fremitus. StatPearls. 2025 Jan:(): [PubMed PMID: 29763013]
Reyes LF, Conway Morris A, Serrano-Mayorga C, Derde LPG, Dickson RP, Martin-Loeches I. Community-acquired pneumonia. Lancet (London, England). 2025 Nov 15:406(10517):2371-2388. doi: 10.1016/S0140-6736(25)01493-X. Epub 2025 Oct 16 [PubMed PMID: 41110447]
Wipf JE, Lipsky BA, Hirschmann JV, Boyko EJ, Takasugi J, Peugeot RL, Davis CL. Diagnosing pneumonia by physical examination: relevant or relic? Archives of internal medicine. 1999 May 24:159(10):1082-7 [PubMed PMID: 10335685]
Arts L, Lim EHT, van de Ven PM, Heunks L, Tuinman PR. The diagnostic accuracy of lung auscultation in adult patients with acute pulmonary pathologies: a meta-analysis. Scientific reports. 2020 Apr 30:10(1):7347. doi: 10.1038/s41598-020-64405-6. Epub 2020 Apr 30 [PubMed PMID: 32355210]
Level 1 (high-level) evidenceVaughn VM, Dickson RP, Horowitz JK, Flanders SA. Community-Acquired Pneumonia: A Review. JAMA. 2024 Oct 15:332(15):1282-1295. doi: 10.1001/jama.2024.14796. Epub [PubMed PMID: 39283629]
Benbassat J, Baumal R. Narrative review: should teaching of the respiratory physical examination be restricted only to signs with proven reliability and validity? Journal of general internal medicine. 2010 Aug:25(8):865-72. doi: 10.1007/s11606-010-1327-8. Epub 2010 Mar 27 [PubMed PMID: 20349154]
Level 3 (low-level) evidence