Introduction
Complex ear lacerations are those that present with irregular tissue injury or loss, exposure of underlying cartilage, or involvement of the external auditory canal. These are often seen in various settings, including the emergency department and primary care. The ear presents a unique challenge due to its intricate surface anatomy, composition, and function. The ears are particularly susceptible to lacerations, avulsions, and blunt trauma because they are positioned prominently over bony surfaces. Additionally, the pinna's unique composition and relatively tenuous blood supply pose specific challenges and considerations for ear laceration repair.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Anatomical Structures
An understanding of the ear's anatomy is imperative for the clinician to adequately repair an ear laceration. The surface anatomy of the auricle is essential to understand when appropriately characterizing an injury and when communicating with subspecialist colleagues (see Image. Auricle Surface Anatomy). Most ear lacerations occur on the exposed auricle, also known as the pinna. This is the area of skin-covered cartilage that forms the vast majority of the external ear and is most prone to injury. However, lacerations may extend into the external auditory canal or the preauricular area. The lobule lacks underlying cartilage and is composed of fibroadipose tissue, surrounded by skin.
The cartilage that makes up the auricle is relatively avascular, dependent upon a watershed blood supply, and is in continuity with the cartilage of the external auditory canal. The cartilage relies on the perichondrium, the connective tissue that covers the cartilage, for its blood supply. In the absence of trauma, the perichondrium is tightly adherent to the underlying cartilage but has an areolar layer that allows some motion between the perichondrium and the overlying skin.
Blood Supply and Nerve Innervation
The skin of the ear has a dual blood supply, with the anterior portion of the auricle supplied by branches of the superficial temporal artery (STA). In contrast, the posterior auricular artery (PAA) supplies the posterior aspect of the pinna as well as the skin overlying the mastoid. These arteries are both terminal branches of the external carotid artery. The superficial temporal artery gives branches off to the superior, middle, and inferior anterior auricular arteries. The posterior auricular artery lies medial to the meatal cartilage. The superior branch of the anterior auricular artery and upper, nonperforating branches of the PAA join to form an arcade of blood supply that runs along the upper third of the helical rim.
Additionally, in about 75% of patients, a continuous arterial branch of the superior auricular artery extends from the helical rim to the lobule. The posterior auricle also receives some blood supply from collateral branches of the occipital artery.[1] The PAA predominantly supplies the cranial side of the auricle and the concha via perforating branches. The STA network supplies the upper third of the lateral aspect of the auricle. Both the PAA and STA networks routinely develop anastamoses in the upper third of the auricle.[2]
The innervation of the ear is slightly more complicated. The superior, anterior, and medial aspects of the auricle are innervated by the auriculotemporal nerve, which is a branch of the trigeminal nerve. The inferior, posterior, and lateral aspects of the auricle are dually innervated by the lesser occipital and greater auricular nerves, which arise from the C2 and C3 roots of the cervical plexus. The vagus nerve innervates the majority of the concha with some scattered innervation from the facial nerve. The external auditory canal, including the tympanic membrane, is innervated by branches of the auriculotemporal nerve, the facial nerve, the glossopharyngeal nerve, and the vagus nerve.[3]
Indications
Auricular lacerations should ideally be repaired within 24 hours. Immediate primary closure of auricular lacerations, even when complex, yields high success rates with the best outcomes in nonhelical injuries and in the absence of complete avulsion of the auricle.[4] If the auricular cartilage is exposed, the ear must be repaired to reduce the risk of complications, including infection, chondritis, necrosis, and deformities, eg, "cauliflower ear," a phenomenon that occurs when a hematoma is replaced by fibrous connective tissue.[5]
Delayed closure or a staged repair should be considered for patients who present after 24 hours, for those with evidence of infection around the laceration, for those with relatively devascularized portions of the pinna, and for those at increased risk of infection. Emergency clinicians should refer the patient to otolaryngology or plastic surgery if the patient has an avulsion of the auricle, lacerations extending into the external auditory canal, lacerations associated with internal or middle ear damage, or lacerations concurrent with a skull base fracture. Partial avulsion injuries can be repaired by the primary or emergency clinician as long as a wide pedicle remains and adequate capillary refill are present at the most distal segment of injury. Narrow pedicle injuries need specialist and surgical attention due to the tenuous blood supply.
Contraindications
An overtly infected wound is the primary contraindication to the primary repair of an ear laceration. Clinicians should also be alert to signs of more serious concurrent injury, eg, vertigo, nausea and vomiting, ataxia, hemotympanum, cerebrospinal fluid otorrhea, Battle sign, or facial nerve dysfunction. These are more common in high-velocity injuries and polytrauma patients.
Equipment
As with any laceration, the primary materials for repair of a complex ear laceration include sterile irrigation, appropriate surgical preparation, including forceps, needle drivers, suture, sterile drapes, local anesthetic, 1.5-inch, small-gauge needles (27-30 gauge), syringes for local anesthesia, scalpel or scissors, and sterile gauze. For cartilage or perichondrium repair, consider using synthetic, absorbable, sterile, surgical sutures composed of a copolymer made from 90% glycolide and 10% L-lactide or a sterile, synthetic, absorbable monofilament suture made from polyester (including monocryl or polydioxanone suture). These will retain tensile strength for at least 30 days and have minimal tissue reactivity. The overlying auricular skin may be closed with 5-0 or 6-0 sutures. The choice between absorbable and nonabsorbable suture material can be guided by the clinician's inclination to the patient's ability and willingness to follow up. Absorbable suture material would be preferred in patients at high risk of being lost to follow-up. In contrast, nonabsorbable sutures may be considered for those who are reliable in attending postinjury appointments. Generally, nonabsorbable sutures should be removed in 5 to 7 days following placement. Data suggest no difference in cosmetic outcomes between absorbable and nonabsorbable sutures when studied elsewhere in the body, but no specific studies have been performed on ear lacerations.[6]
Personnel
While only the primary practitioner performing the repair may be needed, having additional assistance during sterile procedures, eg, a nurse, surgical tech, medical assistant, or other qualified professional, could be beneficial. Additionally, having personnel available to provide distractions could be helpful when managing a pediatric patient with an ear laceration under local anesthetic.
Preparation
An auricular block (also known as a "ring" block) can provide greater patient comfort before irrigation and help avoid distortion of the laceration edges. In general, lacerations can be irrigated with copious sterile saline, using about 50 to 100 mL of solution per centimeter of wound, at approximately 5 to 8 psi.[7] After the wound is cleansed, a sterile drape should be applied to isolate the field. If necessary, the physician may debride or excise macerated or devitalized tissue to create clean wound margins, which facilitates cosmetic approximation and a durable repair, while taking care not to remove excessive healthy tissue that could compromise the outcome.
Technique or Treatment
Physicians should anesthetize the area around the laceration before initiating the repair. The choice of local anesthetic is at the clinician's discretion, but adding a vasoconstrictor, eg, epinephrine, increases the duration of action and aids hemostasis. Extensive studies have not demonstrated a significant risk of vascular compromise when epinephrine is used during ear surgical procedures, despite this prevalent and persistent myth among emergency room physicians.[8]
Anesthesia Techniques
Anesthesia may be achieved with a regional auricular block or by injecting an anesthetic into and around the wound edges. One advantage of using a regional block is that the instillation of the anesthetic agent will not distort the wound edges, and such a block will provide total anesthesia to the majority of the ear, except the concha and meatus (see Image. Diamond Auricular Block). To perform a regional auricular block, clinicians should instill an anesthetic in a box or diamond shape around the ear. This is accomplished by injecting an anesthetic in the shape of a "V," one inferior to the ear, and an inverted "V" superior to the ear (see Image. Diamond Auricular Block).
The clinicians should start by inserting the needle inferior to the ear near the lobule, aiming toward the mastoid process. The needle should be withdrawn while instilling 1 mL of anesthetic per inch of tissue in a subcutaneous plane to avoid anesthetizing the facial nerve. Using the same technique, the needle should be inserted from the same starting point toward the skin anterior to the tragus, and an anesthetic should be injected while withdrawing the needle.[9] Next, the physician will inject an anesthetic in an inverted "V," starting from the skin superior to the ear and aiming towards the mastoid, followed by the installation of a line of anesthetic from the starting point above the ear towards the skin anterior to the tragus. Allow 5 to 10 minutes for complete anesthesia to take effect, and be sure to test the patient's sensation before initiating the repair. Additional local anesthetic can be injected directly adjacent to the laceration; however, this can distort normal anatomy, making a cosmetic repair more challenging.
Repair Techniques
Once the patient's wound has been cleaned and prepped and the area anesthetized, the repair can begin. Resection of tissue should be minimized, with only obviously devascularized tissues resected before repair. The key tenets of repairing a complex ear laceration are properly aligning the cartilage to maintain aesthetics and ensuring that the overlying skin adequately covers the area. The cartilage itself is avascular and relies on the overlying skin for its blood supply.
To initiate the repair, clinicians should ensure that the skin covers the exposed cartilage. If the skin cannot stretch to cover the cartilage, a 5-mm triangular wedge of cartilage through the helix can be excised without significantly affecting ear shape, aesthetics, or function; anything larger than this may require local flaps for coverage or a staged repair. Minor ear lacerations can be sutured with simple interrupted or running sutures through the overlying skin. When significant cartilage involvement and deformity of the ear are present, the cartilage must be realigned with deep sutures, eg, 5-0 monocryl, to reapproximate the injured cartilage in a separate layer.
Ideally, sutures should be thrown through the outer perichondrium, rather than through the entirety of the cartilage itself, as the cartilage has a greater tendency to pull through or tear. That said, sutures through the cartilage itself can be used if needed, and horizontal mattress sutures are less prone to cutting or tearing of the cartilage. Deep suture knots should be buried. Cartilage and perichondrium should be approximated with the fewest possible stitches to avoid a local inflammatory reaction or infection. Next, the clinician should close the overlying skin with 5-0 or 6-0 simple interrupted sutures at 2- to 3-mm intervals.[10]
Hematoma Prevention Techniques
Once the laceration has been repaired, applying a pressure dressing to the ear to prevent hematoma formation is essential. Several modalities can be used based on the clinician's experience and preference. One common method is to apply petroleum-impregnated gauze to the area over the laceration, usually the antihelix or scapha, and into the helix, and to pack it tightly against the adjacent skin to prevent fluid or blood from accumulating and distorting the anatomy. Following this, a ball of unfolded, "fluffed" gauze should be applied to the entire ear and held in place with a gauze bandage wrapped around the patient's head, which applies pressure to the repaired ear.
Another option is to use a series of simple interrupted "quilting" sutures in a through-and-through fashion. This can be performed by piercing the posterior aspect of the auricle with a suture, advancing 1 cm superiorly, then going back through the anterior aspect of the auricle and tying the knot posteriorly. Space these sutures out by a few millimeters and cover the entire ear surface that may be at risk of hematoma formation. This may also be achieved with mattress sutures. Either absorbable or nonabsorbable suture material can be used, depending on the patient's reliability. Bolstering is another option for preventing hematoma formation, in which a soft dressing (eg, petroleum-impregnated gauze or a dental roll) is stitched to the surface of the auricle.
Lastly, a plaster mold of the auricular surface can be made to compress the skin and prevent hematomas; however, this is more time-intensive and may not be practical in an emergent setting. The bolster and any nonabsorbable sutures should be removed in 5 to 7 days. At this time, no robust data support the routine use of prophylactic antibiotics in ear lacerations, including those with exposed cartilage before repair. However, in practice, they are routinely prescribed because the potential outcomes of a wound infection are devastating, and selected agents should cover Pseudomonas spp.[11][12][13]
Additional Considerations
For additional considerations in managing complex ear lacerations, partial auricular avulsions involving smaller helical rim defects can often be successfully addressed with local reconstructive options that yield excellent cosmetic and functional outcomes. Among the commonly employed techniques for auricular reconstruction is the Antia–Buch chondrocutaneous advancement flap, which provides reliable helical rim restoration and can be performed under local or general anesthesia.[14] When the injury involves significant or circumferential trauma to the external auditory canal, a small amount of packing—eg, an ear wick or dissolvable GelFoam material—may be placed within the canal to prevent cicatricial scarring and subsequent stenosis; this packing is typically removed in about 7 days and replaced as needed.
If a full-thickness laceration leaves only a small pedicle of skin attaching the avulsed portion to the remainder of the ear, consultation with an otolaryngologist or plastic surgeon for repair is indicated. This can be managed either as described above with meticulous, multilayer repair or through staged repair. A staged repair often involves de-epithelializing the avulsed segment and burying it in a postauricular pocket to allow for revascularization of the cartilage. A second procedure elevates this construct back onto the pinna, and often a posterior skin graft is required.[15]
Complete avulsions of the ear can also be treated in this way, though attempts at microvascular reimplantation at the time of injury have also been described with varying success.[16] Factors that improve the success of microvascular reimplantation include preserved vascular pedicles, particularly at the inferior site, short injury-to-surgery time, and careful technique.[17] If a complete avulsion of the ear occurs in the acute setting, with no microvascular surgeon available, direct reattachment can be performed with good cosmetic outcomes; however, there is limited data on direct reattachment compared with microvascular reanastamosis.[18]
Complications
As with all lacerations, potential complications include scarring, infection, pain, and the need for additional repair. Chondritis and hematoma formation are complications specific to ear lacerations. Patients should be reevaluated 24 to 48 hours after the repair to assess for the development of these complications. These should be addressed immediately with medications or drainage and bolstering, respectively. Pseudomonas aeruginosa causes the vast majority of chondritis and should be treated with ciprofloxacin because of its excellent cartilage penetration; however, patients should be appropriately counseled on potential adverse effects, eg, tendon rupture.[19][20] Lacerations of the external auditory canal put the patient at risk for canal stenosis, conductive hearing loss, and acute otitis externa.
Clinical Significance
Major considerations in ear laceration repair include preserving as much native, healthy tissue as possible to maintain the normal functions of the auricle, eg, cosmesis, sound conduction into the external auditory canal, sound localization, and support for eyewear. Additionally, optimizing the repair of complex ear lacerations is essential to minimize complications, including auricular hematoma, tissue loss, and deformity, and to achieve an aesthetic outcome with a functional auricle.
Enhancing Healthcare Team Outcomes
While ear lacerations may appear simple, the ear's unique anatomy and relative hypovascularity pose several challenges that the clinician must be familiar with. Thus, when patients present to the emergency department, having a very low threshold for consulting a plastic surgeon or an otolaryngologist is essential. The emergency department physician or mid-level provider may irrigate the wound and confirm tetanus status, but if there is any question about the wound's severity or the potential need for staged procedures, the wound should not be closed until evaluated by the specialist. A poorly repaired ear laceration can lead to hematoma formation, nerve damage, flap necrosis, and asymmetry or deformity that may be irreversible.[21][3][22]
High-quality care relies on coordinated interprofessional practice. Physicians, general practitioners, and advanced practitioners must assess injury severity, select evidence-based repair techniques, and determine the need for referral. Nurses support wound preparation, patient education, pressure dressings, and early monitoring of complications. Pharmacists contribute by advising on appropriate antimicrobial use and counseling on medication risks. Additionally, effective interprofessional communication and coordinated teamwork have been shown to improve patient safety and clinical outcomes in the emergency care setting.[23] The emergency department depends on individuals with specialized skills and specific roles, which require collaboration. Managing complex ear lacerations requires teamwork among emergency clinicians, nurses, pharmacists, and consultants. Clear communication and timely consultation ensure appropriate management regarding wound assessment, antibiotic selection, and optimized closure technique.
Media
(Click Image to Enlarge)
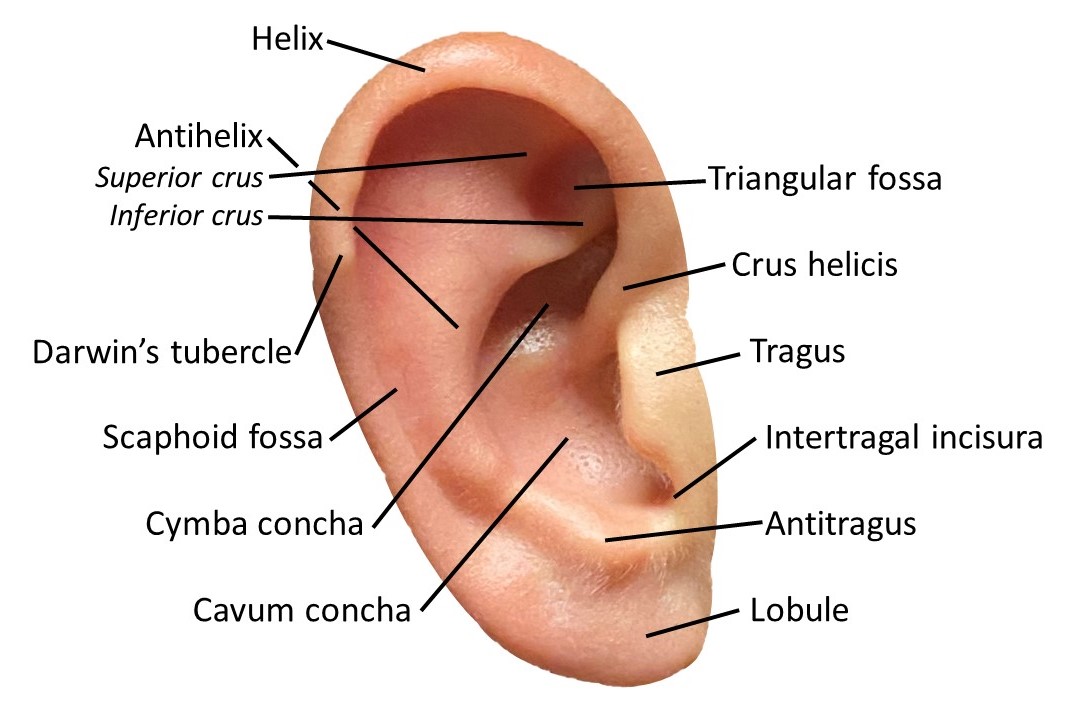
Auricle Surface Anatomy. This image shows the ear auricle's parts, parts, including the helix and its crus, the antihelix and its superior and inferior crura, the Darwin tubercle, triangular and scaphoid fossae, the tragus, conchal cymba and cavum, the intertragal incisura, antitragus, and lobule.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
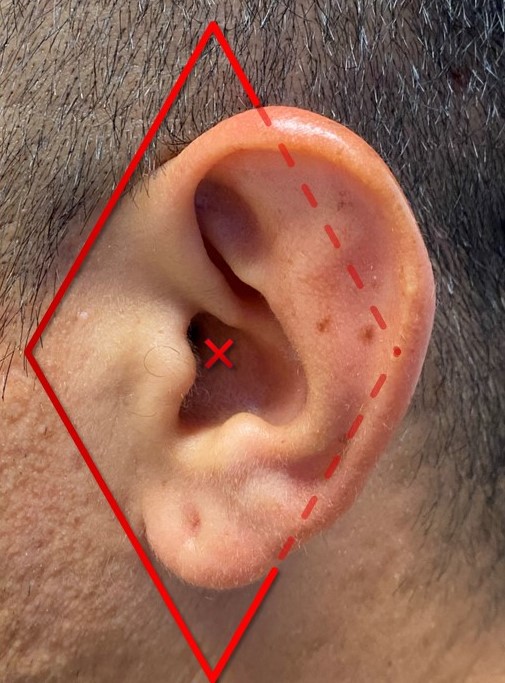
Diamond Auricular Block. The dashed lines represent injections posterior to the auricle, and the X indicates a conchal bowl injection to anesthetize the sensory auricular branch of the facial nerve. The diamond block anesthetizes the auriculotemporal, lesser occipital, and greater auricular nerves, providing complete anesthesia of the auricle.
Contributed by MH Hohman, MD, FACS
References
Zilinsky I, Erdmann D, Weissman O, Hammer N, Sora MC, Schenck TL, Cotofana S. Reevaluation of the arterial blood supply of the auricle. Journal of anatomy. 2017 Feb:230(2):315-324. doi: 10.1111/joa.12550. Epub 2016 Oct 11 [PubMed PMID: 27726131]
Hénoux M, Espitalier F, Hamel A, Dréno B, Michel G, Malard O. Vascular Supply of the Auricle: Anatomical Study and Applications to External Ear Reconstruction. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 2017 Jan:43(1):87-97. doi: 10.1097/DSS.0000000000000928. Epub [PubMed PMID: 28027200]
Osetinsky LM, Hamilton GS 3rd, Carlson ML. Sport Injuries of the Ear and Temporal Bone. Clinics in sports medicine. 2017 Apr:36(2):315-335. doi: 10.1016/j.csm.2016.11.005. Epub [PubMed PMID: 28314420]
Zwemstra M, Geerse S, de Wolf M, Ebbens F, Smits C, van Spronsen E. Surgical outcome following primary closure of auricular lacerations. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2025 Oct:282(10):5147-5152. doi: 10.1007/s00405-025-09453-2. Epub 2025 May 15 [PubMed PMID: 40369216]
Fujiwara M, Suzuki A, Nagata T, Fukamizu H. Cauliflower ear dissection. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2011 Nov:64(11):e279-82. doi: 10.1016/j.bjps.2011.04.018. Epub 2011 May 25 [PubMed PMID: 21612992]
Tejani C, Sivitz AB, Rosen MD, Nakanishi AK, Flood RG, Clott MA, Saccone PG, Luck RP. A comparison of cosmetic outcomes of lacerations on the extremities and trunk using absorbable versus nonabsorbable sutures. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2014 Jun:21(6):637-43. doi: 10.1111/acem.12387. Epub [PubMed PMID: 25039547]
Level 1 (high-level) evidenceForsch RT, Little SH, Williams C. Laceration Repair: A Practical Approach. American family physician. 2017 May 15:95(10):628-636 [PubMed PMID: 28671402]
Häfner HM, Röcken M, Breuninger H. Epinephrine-supplemented local anesthetics for ear and nose surgery: clinical use without complications in more than 10,000 surgical procedures. Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG. 2005 Mar:3(3):195-9 [PubMed PMID: 16372813]
Usuga D, Everett SC, Shalaby M. Auricular nerve block for otitis externa: A case series. The American journal of emergency medicine. 2025 May:91():218.e1-218.e3. doi: 10.1016/j.ajem.2025.01.081. Epub 2025 Feb 5 [PubMed PMID: 39952849]
Level 2 (mid-level) evidenceLavasani L, Leventhal D, Constantinides M, Krein H. Management of acute soft tissue injury to the auricle. Facial plastic surgery : FPS. 2010 Dec:26(6):445-50. doi: 10.1055/s-0030-1267718. Epub 2010 Nov 17 [PubMed PMID: 21086230]
Greywoode JD, Pribitkin EA, Krein H. Management of auricular hematoma and the cauliflower ear. Facial plastic surgery : FPS. 2010 Dec:26(6):451-5. doi: 10.1055/s-0030-1267719. Epub 2010 Nov 17 [PubMed PMID: 21086231]
Roy S, Smith LP. A novel technique for treating auricular hematomas in mixed martial artists (ultimate fighters). American journal of otolaryngology. 2010 Jan-Feb:31(1):21-4. doi: 10.1016/j.amjoto.2008.09.005. Epub 2009 Mar 26 [PubMed PMID: 19944894]
Level 2 (mid-level) evidenceGiles WC, Iverson KC, King JD, Hill FC, Woody EA, Bouknight AL. Incision and drainage followed by mattress suture repair of auricular hematoma. The Laryngoscope. 2007 Dec:117(12):2097-9 [PubMed PMID: 17921905]
Level 2 (mid-level) evidenceSakiyama PH, Ferrari TA, Garbin RR, Tarlé RG. Old but gold - Antia and Buch chondrocutaneous advancement flap for helical reconstruction: a series of cases. Anais brasileiros de dermatologia. 2022 Nov-Dec:97(6):835-837. doi: 10.1016/j.abd.2021.01.010. Epub 2022 Sep 6 [PubMed PMID: 36075799]
Level 3 (low-level) evidenceGailey AD, Farquhar D, Clark JM, Shockley WW. Auricular avulsion injuries and reattachment techniques: A systematic review. Laryngoscope investigative otolaryngology. 2020 Jun:5(3):381-389. doi: 10.1002/lio2.372. Epub 2020 Apr 14 [PubMed PMID: 32596480]
Level 1 (high-level) evidenceLin PY, Chiang YC, Hsieh CH, Jeng SF. Microsurgical replantation and salvage procedures in traumatic ear amputation. The Journal of trauma. 2010 Oct:69(4):E15-9. doi: 10.1097/TA.0b013e3181bbd644. Epub [PubMed PMID: 20938253]
Widiarni WD, Putri B, Respati WR. Prognostic factors in partial auricular avulsion after one-stage reconstruction. Trauma case reports. 2023 Oct:47():100891. doi: 10.1016/j.tcr.2023.100891. Epub 2023 Aug 7 [PubMed PMID: 37608873]
Level 3 (low-level) evidenceAl-Ali MA, Abu-Zidan FM. Auricular avulsion injuries: Literature review and management algorithm. Turkish journal of emergency medicine. 2022 Apr-Jun:22(2):59-66. doi: 10.4103/2452-2473.342811. Epub 2022 Apr 11 [PubMed PMID: 35529026]
Fisher CG, Kacica MA, Bennett NM. Risk factors for cartilage infections of the ear. American journal of preventive medicine. 2005 Oct:29(3):204-9 [PubMed PMID: 16168869]
Level 2 (mid-level) evidenceSangiorgio A, Sirone M, Adravanti FM, Testa EA, Riegger M, Filardo G. Achilles tendon complications of fluoroquinolone treatment: a molecule-stratified systematic review and meta-analysis. EFORT open reviews. 2024 Jul 1:9(7):581-588. doi: 10.1530/EOR-23-0181. Epub 2024 Jul 1 [PubMed PMID: 38949172]
Level 1 (high-level) evidenceMenon A, G A. Traumatic Partial Avulsion of Pinna Reconstruction with Limberg Flap. World journal of plastic surgery. 2018 May:7(2):231-234 [PubMed PMID: 30083508]
Brown DJ, Jaffe JE, Henson JK. Advanced laceration management. Emergency medicine clinics of North America. 2007 Feb:25(1):83-99 [PubMed PMID: 17400074]
Courtenay M, Nancarrow S, Dawson D. Interprofessional teamwork in the trauma setting: a scoping review. Human resources for health. 2013 Nov 5:11():57. doi: 10.1186/1478-4491-11-57. Epub 2013 Nov 5 [PubMed PMID: 24188523]
Level 2 (mid-level) evidence