Introduction
The external ear forms the outer part of the auditory system and includes the auricle (pinna), the external auditory canal (external acoustic meatus), and the outer surface of the tympanic membrane. The primary role of the external ear is to initiate auditory transduction by gathering sound, shaping the sound spectrum, providing localization cues, and matching impedance between the external environment and the middle ear. The pinna functions as a funnel, directing sound into the external acoustic meatus, which focuses sound onto the tympanic membrane for further transmission.[1][2][3]
The auricle is a fibrocartilaginous structure covered by thin, adherent skin and organized into complex topographic folds, including the helix, antihelix, concha, tragus, and lobule (see Image. External Ear). These anatomic features contribute to frequency-dependent resonance and vertical sound localization by altering sound wave reflection patterns before sound enters the external auditory canal.
The external auditory canal is an approximately 2.5-cm S-shaped conduit extending from the conchal bowl to the tympanic membrane. The canal is divided into a lateral cartilaginous 1/3 and a medial bony 2/3, with the transition occurring at the narrow bony-cartilaginous junction (isthmus), the narrowest portion of the canal. The cartilaginous segment contains hair follicles, sebaceous glands, and ceruminous glands that contribute to cerumen production and maintain a protective, hydrophobic, antimicrobial environment. In contrast, the osseous segment is formed by the tympanic portion of the temporal bone and is lined by thin, tightly adherent skin that lacks adnexal structures. Periosteal innervation renders the osseous segment highly sensitive to manipulation and inflammation.
The junction between bone and cartilage is especially important clinically as a zone of biomechanical, histologic, and functional transition. The bony-cartilaginous junction is a common site of cerumen impaction due to canal narrowing and the inward movement of epithelial debris from the cartilaginous segment. The bony-cartilaginous junction also marks a transition from flexibility to rigidity, as the flexible cartilaginous canal gives way to the less distensible bony canal, resulting in increased pain sensitivity in the setting of canal edema or instrumentation. Branches of the auriculotemporal nerve, the auricular branch (Arnold nerve) of the vagus nerve (cranial nerve X), and the facial nerve (cranial nerve VII) provide rich sensory innervation to the region, which accounts for pronounced otalgia and reflex responses, such as coughing or vagal stimulation, during canal manipulation.
The external auditory canal is also characterized by continuous lateral epithelial migration originating from the tympanic membrane and canal skin, facilitating self-cleansing and the outward transport of cerumen and debris. Disruption of epithelial migration predisposes the external auditory canal to cerumen impaction, chronic inflammation, and keratin accumulation and contributes to the development of acquired canal cholesteatoma.
Cerumen serves a critical protective role by providing lubrication, a hydrophobic barrier, and antimicrobial activity through lipid constituents and an acidic pH. Excessive cleaning or disruption of cerumen homeostasis increases susceptibility to otitis externa and microtrauma of the canal epithelium.
The vascular and structural features of the external auditory canal influence disease patterns. The cartilaginous segment, which contains adnexal structures, is more commonly affected by diffuse inflammatory conditions, such as acute otitis externa. In contrast, the bony canal, characterized by thin periosteal skin that is tightly adherent to the underlying bone, often produces severe pain even during early or limited stages of disease. Edema at the narrow bony-cartilaginous junction can rapidly obstruct the canal, increasing conductive hearing loss and promoting retention of infectious material.
Anatomical defects in the cartilaginous canal, including fissures of Santorini, may permit communication between the external auditory canal and adjacent periauricular soft tissues, providing potential pathways for infection to spread in advanced cases.[4] This finding is particularly relevant in immunocompromised patients, in whom progression to malignant (necrotizing) otitis externa may occur with extension toward the skull base.
The external ear contributes to acoustic amplification by resonating at frequencies between 2 and 4 kHz (relevant to speech perception) and by directing sound energy onto the tympanic membrane. The tympanic membrane converts airborne acoustic energy into mechanical vibration transmitted to the ossicular chain (see Image. Ear Anatomy). Collectively, these mechanisms ensure efficient energy transfer from the external environment to the fluid-filled inner ear (see Image. Inner Ear Anatomy).
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The external ear consists of the auricle and the external auditory canal, terminating at the lateral surface of the tympanic membrane. The external ear functions as a specialized acoustic interface designed for sound collection, frequency-dependent spectral filtering, impedance matching, and spatial localization. Structural configuration also provides important protective functions for the middle and inner ear, including exclusion of environmental debris, microorganisms, and mechanical injury.
Functionally, the external ear operates as a structurally integrated acoustic system in which auricular architecture provides direction-dependent spectral shaping that contributes to vertical and front–back localization. The external auditory canal functions as a resonant, self-cleaning conduit that amplifies sound, particularly within the speech frequency range of 2 to 4 kHz, and maintains epithelial migration for continuous clearance of keratin and debris. A key clinical transition point is the bony-cartilaginous junction, the narrowest segment of the canal, which serves as a common site of cerumen impaction and pain amplification due to the transition from flexible cartilaginous tissue to rigid periosteum-lined bone. Collectively, these structures form a unified system that integrates acoustic optimization with protective and maintenance mechanisms essential for normal hearing and resistance to disease.
Auricle
The auricle is composed primarily of elastic cartilage, except for the lobule, which consists of fibrofatty connective tissue and contains no cartilage. The cartilaginous framework is covered by thin, tightly adherent skin, particularly on the anterior surface, and is anchored to the skull by intrinsic ligaments and extrinsic auricular muscles. Extrinsic auricular muscles are vestigial in humans but retain limited functional activity in some individuals. Auricular skin contains abundant sebaceous glands, which contribute to surface lubrication and barrier integrity and reduce desiccation and fissuring of the thin cutaneous envelope. The external surface of the auricle is highly contoured, producing acoustically relevant reflection and diffraction patterns that contribute to spatial hearing.
The helix forms the outer posterosuperior rim of the auricle and curves anteriorly and inferiorly toward the external acoustic meatus, contributing to the concave funneling geometry of the pinna. The antihelix is a prominent Y-shaped cartilaginous ridge located anterior to the helix and bifurcates superiorly into crura, forming the boundary of the deep conchal bowl. Between the helix and antihelix lies the scaphoid fossa (scapha), a narrow depression that contributes to high-frequency spectral shaping.
The concha, the deepest depression of the auricle, is subdivided into the cymba and cavum conchae and serves as the primary acoustic funnel directing sound energy into the external auditory canal. The tragus, a cartilaginous projection anterior to the concha and external acoustic meatus, partially shields the canal opening and influences anterior sound attenuation. The lobule (earlobe), located inferior to the canal opening, is a noncartilaginous structure composed of adipose and areolar connective tissue. A small anatomical variant, the Darwin tubercle, may be present on the superior helix and is considered an atavistic remnant with no known functional role.[5]
External Auditory Canal
The external auditory canal extends from the conchal bowl to the tympanic membrane and follows an S-shaped (sigmoid) course through the temporal bone. The canal is divided into a lateral cartilaginous 1/3 and a medial bony 2/3, with a critical narrowing at the bony-cartilaginous junction.
The cartilaginous portion contains hair follicles, sebaceous glands, and specialized ceruminous glands that secrete cerumen. Cerumen is a lipid-rich secretion that provides hydrophobic, antimicrobial, and mechanical protective functions, including trapping debris and deterring insect entry into the canal. The bony portion is formed by the tympanic part of the temporal bone and is lined by thin, tightly adherent skin that lacks adnexal structures, resulting in high sensitivity to manipulation and inflammation.
The external auditory canal is not a passive conduit but a dynamic structure with clinically significant functional properties. The bony-cartilaginous junction is the narrowest portion of the canal and serves as a common site of cerumen impaction due to abrupt changes in canal caliber and epithelial migration dynamics. The bony-cartilaginous junction also serves as a major site of pain generation in otitis externa due to the transition from compliant cartilaginous tissue to rigid periosteum-lined bone with dense sensory innervation.
Since the external auditory canal is not aligned linearly with the conchal bowl, otoscopic examination requires auricular manipulation, typically posterior and superior traction of the pinna in adults, to straighten the canal and improve visualization of the tympanic membrane. A cartilaginous block of the external ear canal causes more hearing loss than a block of the bony ear canal.[6]
Sound Localization and Binaural Processing
The bilateral placement of the auricles enables spatial hearing through computation of interaural differences within the central auditory pathways. Acoustic information is integrated in brainstem nuclei, including the superior olivary complex (medial and lateral superior olives), and relayed via the inferior colliculus to higher auditory centers. These structures compute interaural time (ITDs) and level (ILDs) differences based on discrepancies in arrival time and intensity between both ears.[7] ITDs and ILDs vary systematically with sound-source azimuth, defined as the left-to-right angular position of a sound in the horizontal plane around the head. ITDs and ILDs increase as sound shifts laterally from 0° (midline) to 90° (lateral) and diminish toward 180° (posterior midline). Binaural cues alone are insufficient for complete 3-dimensional localization.
Duplex Theory
The duplex theory, or Rayleigh model, of sound localization was first described by Lord Rayleigh in 1907. The theory describes the frequency-dependent reliance on ITDs and ILDs. ITD predominates in low-frequency sound localization (approximately <800 Hz), where wavelengths exceed interaural distance and phase differences are preserved. ILD predominates at high frequencies (>1600 Hz), where shorter wavelengths are attenuated by head shadowing, creating intensity differences between ears. Intermediate frequencies demonstrate overlapping use of both mechanisms. The duplex theory primarily explains horizontal-plane localization and does not fully account for vertical or front–back discrimination.[8]
Pinna Filtering and Spectral Shaping
The pinna’s complex 3-dimensional architecture introduces direction-dependent spectral filtering through reflection, diffraction, and resonance. These effects produce frequency-specific notches and peaks that vary with sound-source elevation and anterior–posterior position. Monaural spectral cues enable the auditory system to resolve front–back ambiguity and vertical localization when binaural cues are insufficient. This phenomenon is known as the pinna filtering effect, in which auricular morphology encodes individualized spectral signatures used by the central auditory pathways for spatial interpretation.[9]
Evolutionary and Functional Considerations
The structural configuration of the pinna is believed to enhance sensitivity to frequencies around 2 to 4 kHz, corresponding to the dominant frequency spectrum of human speech. Resonance of the external auditory canal, combined with this pinna effect, may have conferred an evolutionary advantage in speech perception and communication efficiency. Comparative research on the external ear has contributed foundational insights into hearing mechanisms.[10]
Embryology
External ear development results from the coordinated contributions of the 1st and 2nd pharyngeal arches and the 1st pharyngeal cleft, with epithelial–mesenchymal interactions governing morphogenesis. Auricle morphogenesis begins during the 5th to 6th week of gestation from 6 mesenchymal proliferations known as the auricular hillocks of His, which form around the 1st pharyngeal cleft. The auricular hillocks arise from mesenchyme of the 1st (mandibular) and 2nd (hyoid) arches. The 1st arch contributes to the anterior 3 hillocks, which are associated with the formation of definitive auricular structures, such as the tragus and the anterior helix. The 2nd arch contributes to the posterior 3 hillocks, which give rise to the antihelix, conchal components, and lobule. Progressive growth, fusion, and remodeling of the auricular hillocks form the definitive auricular contour, followed by cranial migration of the auricle from a lower cervical position to its adult lateral cranial location during fetal development.[11]
The external auditory canal develops from ectoderm derived from the 1st pharyngeal cleft, which invaginates to form the meatal plug during early gestation. The meatal plug persists as a solid epithelial core for several months before canalization during the late 2nd to 3rd trimester (approximately 28 to 32 weeks of gestation), establishing a patent canal lined by stratified squamous epithelium. The medial aspect of this ectodermal invagination contributes to the outer epithelial layer of the tympanic membrane. The inner mucosal layer is derived from endoderm of the 1st pharyngeal pouch, and the intermediate fibrous layer arises from mesenchyme. The cartilaginous portion of the canal later differentiates to include hair follicles, sebaceous glands, and ceruminous glands, which become functionally important in cerumen production and epithelial protection.[12]
Congenital abnormalities of the external ear result from disruptions in arch patterning, auricular hillock fusion, or canalization of the 1st pharyngeal cleft. Auricular malformations such as microtia and anotia arise from abnormal development of the 1st and 2nd arch hillocks. Clinical severity ranges from mild structural distortion to complete absence of the pinna. Preauricular tags and pits represent accessory auricular tissue due to aberrant or incomplete fusion of the auricular hillocks and are commonly associated with 1st and 2nd arch developmental anomalies. External auditory canal atresia or stenosis results from failure of canalization of the meatal plug derived from the 1st pharyngeal cleft and may occur in isolation or in association with auricular malformations. These anomalies frequently present with conductive hearing loss, reflecting impaired sound transmission at the level of the external ear, and may be syndromic, particularly in conditions involving 1st and 2nd arch derivatives, such as Treacher Collins syndrome and the oculoauriculovertebral spectrum (Goldenhar syndrome).[13]
Blood Supply and Lymphatics
The vascular and lymphatic anatomy of the external ear reflects a dual role as a cutaneous-cartilaginous appendage with high surface area exposure and as a structurally delicate acoustic organ. Blood supply is derived from branches of the external and internal carotid systems, while lymphatic drainage follows anterior, posterior, and inferior pathways to the parotid, mastoid, and deep cervical nodal basins. These vascular and lymphatic pathways have important implications for otologic infection, neoplasia, surgical flap design, and disease processes arising from adjacent head and neck structures.
Arterial Supply
Arterial supply of the external ear is rich and redundant, derived primarily from the external carotid artery system, with minor contributions from the internal carotid system via the ophthalmic artery. Dual arterial contribution reflects auricular embryologic development at the craniofacial junction and exposed cutaneous morphology.
The posterior auricular artery, a direct branch of the external carotid artery, provides the dominant vascular supply to the posterior auricle and contributes perforating branches supplying both the medial and lateral surfaces of the pinna. Posterior auricular artery branches also supply the lobule and the posterior aspect of the concha. The superficial temporal artery, another terminal branch of the external carotid artery, supplies the superior and anterior auricle, particularly the area of the helix and adjacent temporal skin, via anterior auricular branches. These vessels are clinically important in surgical approaches to the temporal region, as well as in auricular reconstruction, given their role as an important vascular basis for local flaps.
Additional contributions arise from the occipital artery, which provides small auricular branches supplying the superior and posterior auricle and anastomosing with the posterior auricular artery, thereby contributing to vascular redundancy. A minor arterial supply is also derived from the deep auricular artery, a branch of the maxillary artery, which enters the external auditory canal and supplies its deep bony portion, as well as the external surface of the tympanic membrane. The lateral aspect of the tympanic membrane also receives contributions from this system, a relationship of clinical relevance in external otitis and tympanic membrane pathology.
The internal carotid system contributes indirectly via the anterior tympanic branch of the maxillary artery and small contributions from the ophthalmic circulation to periauricular skin. However, these contributions are minor relative to the external carotid system.
Venous Drainage
Venous drainage of the external ear generally parallels the arterial supply. The anterior auricle drains primarily into the superficial temporal vein, while the posterior auricle drains into the posterior auricular vein, which subsequently contributes to the external jugular venous system. Deep portions of the external auditory canal may drain into the pterygoid venous plexus via the maxillary vein. These venous pathways are clinically relevant conduits for the spread of infection or inflammatory processes from the external ear to deeper facial and intracranial venous structures.
Lymphatic Drainage
Lymphatic drainage of the external ear is regionally organized. This network is clinically important for patterns of metastatic spread and infectious lymphadenopathy.
The anterosuperior auricle, which includes the helix and tragus, drains primarily into the preauricular (parotid) lymph nodes—components of the superficial parotid nodal group. The preauricular lymph nodes also receive lymphatic drainage from the anterior external auditory canal and adjacent temporal skin, and therefore commonly enlarge in otitis externa and periauricular skin infections.
The posterior and superior auricle drains into the mastoid (posterior auricular) lymph nodes, located over the mastoid process and associated with drainage of the posterior scalp and retroauricular region. Mastoid lymph nodes may become reactive in posterior auricular skin infections or inflammatory conditions of the scalp and pinna.
The inferior auricle and lobule, as well as portions of the inferior external auditory canal, drain into the superficial and deep cervical lymph nodes, particularly the upper deep cervical chain along the internal jugular vein. This drainage pathway is clinically significant in malignant processes involving the external ear, including cutaneous malignancies, such as squamous cell carcinoma and melanoma of the auricle.
Clinical Correlations
The vascularity of the external ear is clinically relevant in inflammatory and reconstructive contexts. The rich arterial anastomotic network supports viability of auricular skin flaps but also facilitates the rapid spread of infection in conditions like otitis externa. The relatively avascular auricular cartilage depends entirely on the perichondrial vascular supply, rendering it highly susceptible to ischemic necrosis in perichondritis or an auricular hematoma when the perichondrial blood supply is disrupted.
Lymphatic drainage patterns are critical for staging and evaluation of external ear malignancies. Enlargement of preauricular, mastoid, or upper cervical nodes may reflect localized infection, dermatologic inflammation, or metastatic disease. Persistent unilateral lymphadenopathy in these nodal basins warrants evaluation for cutaneous malignancy of the auricle or external auditory canal.
Nerves
The external ear has complex and clinically important sensory innervation due to its embryologic derivation from the 1st and 2nd pharyngeal arches and its anatomic position at the interface of cranial and cervical dermatomes. Sensory innervation arises from the contributions of multiple cranial nerves and the cervical plexus, producing overlapping sensory territories that are critical for producing pain referral patterns, evaluating otalgia, and triggering reflex phenomena, such as cough and vagal responses during otologic procedures.
Sensory Innervation of the Auricle
The auricle receives mixed somatic sensory input from branches of the trigeminal (cranial nerve V), facial, glossopharyngeal (cranial nerve IX), and vagus nerves. Additional contributions arise from the cervical plexus.
The auriculotemporal nerve, a branch of the mandibular division of the trigeminal nerve (cranial nerve V3), provides primary sensory supply to the anterosuperior auricle, including the tragus, the anterior helix, and the adjacent external auditory canal. This pattern of innervation accounts for referred ear pain seen with temporomandibular joint pathology.
The great auricular nerve (C2–C3), arising from the cervical plexus, supplies the inferior and posterior auricle, including the lobule and the lower pinna. Great auricular nerve fibers also contribute sensory input to the posterior aspect of the external auditory canal and are commonly involved in referred otalgia from cervical spine pathology or postoperative neck dissection pain. The lesser occipital nerve (C2) supplies the superior and posterior auricle, particularly the upper medial surface, and contributes to scalp–auricular sensory overlap in posterior headache syndromes.
External Auditory Canal Innervation
The external auditory canal is richly innervated and serves as a convergence point for multiple sensory pathways. The auriculotemporal nerve supplies the anterior and superior walls of the canal and is the dominant sensory nerve in this region. The auricular branch of the vagus nerve supplies the posterior and inferior canal wall and portions of the concha. Stimulation of this nerve may trigger a vagal reflex cough, gagging, or, less commonly, bradycardia during otologic instrumentation or cerumen removal.
Additional contributions arise from the facial nerve via small auricular branches, particularly in the region of the concha. Facial nerve contribution is variable and clinically minor compared with trigeminal and vagus nerve inputs. The glossopharyngeal nerve may contribute minor sensory fibers near the tympanic membrane region and is more prominently involved in deep referred otalgia via shared brainstem pathways.
Central Processing and Referred Otalgia
Sensory input from the external ear converges in the spinal trigeminal nucleus and upper cervical dorsal horn (C2–C3), where cross-talk between somatic and visceral afferents contributes to the high incidence of referred otalgia. Convergence of multiple cranial and cervical nerves on overlapping central pathways allows pathology outside the ear to manifest as ear pain, including temporomandibular joint disease, dental pathology, cervical spine disorders, tonsillopharyngeal inflammation, and laryngeal pathology. Otalgia with a normal otoscopic examination should prompt evaluation of head and neck structures innervated by the trigeminal, facial, glossopharyngeal, and vagus nerves, as well as cervical roots.
Autonomic and Reflex Phenomena
The external auditory canal, particularly the region innervated by the auricular branch of the vagus nerve, participates in clinically relevant reflex arcs. Mechanical stimulation of the canal may activate vagal afferents, producing a cough reflex (Arnold reflex), gagging, or, rarely, cardiovascular responses, such as transient bradycardia. This phenomenon is especially relevant during cerumen disimpaction, foreign body removal, and otologic instrumentation.
Clinical Correlations
The external ear receives sensory innervation from multiple cranial and cervical nerves, including the mandibular nerve for the anterosuperior auricle and canal, the cervical plexus (C2–C3) for the posterior and inferior auricle, and the vagus nerve via the auricular branch for the posterior canal and concha, with minor contributions from the facial and glossopharyngeal nerves. The overlapping innervation accounts for frequent referred otalgia and vagal reflex phenomena during external auditory canal stimulation.
Muscles
The musculature of the external ear consists of intrinsic and extrinsic auricular muscles that are vestigial but retain limited functional activity in humans. Although not essential for hearing, these muscles are clinically relevant because of their origin from the 2nd pharyngeal arch, innervation by the facial nerve, and association with auricular movement, fascial planes, and surgical dissection layers in otologic and parotid surgery.
Intrinsic Muscles of the Auricle
The intrinsic auricular muscles are confined entirely to the auricle and primarily maintain auricular shape rather than produce significant movement. These muscles include the helicis major and minor, which act on the root and crus of the helix; the tragicus and antitragicus muscles, which modify the tragus and antitragus; and the transverse auricular and oblique auricular muscles, which influence convexity of the cranial surface of the auricle and help maintain the contour of the conchal bowl and auricular folds. Although functionally limited in humans, the intrinsic auricular muscles contribute to subtle tensioning of auricular cartilage and may have played a more prominent role in ancestral species with mobile pinnae. These muscles are located within the perichondrial connective tissue plane between the skin and auricular cartilage. Dissection within this plane may disrupt vascular supply and alter auricular contour.
Extrinsic Muscles of the Auricle
The extrinsic auricular muscles include the anterior, superior, and posterior auricular muscles, which connect the auricle to surrounding cranial structures. The anterior auricular muscle extends from the temporal fascia to the anterior helix and tragus. The superior auricular muscle extends from the epicranial aponeurosis to the superior auricle. The posterior auricular muscle extends from the mastoid region to the posterior auricle. These muscles produce minimal voluntary auricular movement in most individuals. Rudimentary contraction may be observed in some patients during attempted auricular movement or facial nerve stimulation.
Innervation
All intrinsic and extrinsic auricular muscles are innervated by the facial nerve, specifically through the posterior auricular and temporal branches. This pattern of innervation reflects the embryologic origin of these muscles from the 2nd pharyngeal arch, which also gives rise to other facial nerve–supplied structures. Facial nerve dysfunction may result in subtle loss of auricular movement, although associated functional impairment is rarely significant.
Clinical Correlations
The auricular muscles are largely vestigial in modern humans. However, these muscles continue to be clinically relevant in several contexts. Facial nerve injury or paralysis, particularly from proximal lesions, may produce subtle changes in auricular tone or position. Knowledge of auricular muscle planes is important during otologic and parotid surgery to preserve soft tissue integrity and avoid disruption of the perichondrial blood supply.
The muscular layer lies between the skin and cartilage and is closely associated with the auricular perichondrium, making this layer relevant in flap design, otoplasty, and reconstruction. Excessive dissection within this plane can compromise cartilage viability and contribute to deformities, including contour irregularities.
Physiologic Variants
Physiologic variants of the external ear are common, nonpathologic deviations in auricular morphology and external auditory canal anatomy. These variants arise from normal variation in the embryologic development of 1st- and 2nd-pharyngeal arch derivatives and do not inherently indicate disease. Recognition of these variants is clinically important to avoid misdiagnosis as congenital malformations, traumatic deformities, or pathologic masses.
Auricular Morphologic Variants
The external ear demonstrates substantial normal variability in shape, size, and contour due to differences in cartilage folding, elastic recoil, and perichondrial development. Common physiologic variants include prominent ears, characterized by an increased auriculocephalic angle or underdevelopment of the antihelical fold, and lop ear configuration, marked by mild folding or inferior rotation of the superior auricle. The presence or absence of a Darwin tubercle, a small prominence along the helix, is another benign atavistic variant without functional consequence. "Microtia" is a term used to describe a wide array of phenotypic presentations of the outer ear.[14] Minor asymmetry between the auricles is common and typically reflects normal developmental variability rather than pathology. Variations in helix thickness, conchal depth, and lobular size are also common and may subtly influence auricular acoustic properties without causing clinically significant hearing impairment.
External Auditory Canal Variants
The external auditory canal also exhibits physiologic variation in length, diameter, and curvature. A more acute S-shaped curvature is present in some individuals, whereas a relatively straight canal is evident in others, influencing the ease of otoscopic visualization and cerumen clearance. Variation in the location and sharpness of the bony-cartilaginous junction may affect susceptibility to cerumen accumulation or discomfort during instrumentation.
Cerumen characteristics vary widely among individuals and are influenced by genetic polymorphisms affecting glandular secretion. Wet cerumen, predominant in many populations of European and African ancestry, is typically sticky and brown, whereas dry cerumen, more common in East Asian populations, is friable and gray. These differences are normal genetic variation and are not pathologic.
Computed tomography is often performed before ear surgery to define the nature and extent of existing pathology. Computed tomography also provides detailed information regarding anatomic landmarks and variations that may affect the surgical approach.[15]
Skin and Adjunct Variants
The density of sebaceous glands, ceruminous glands, and hair follicles within the cartilaginous canal varies considerably among individuals. Increased hair density within the external auditory canal is a benign variant observed more commonly in older men and may contribute to altered cerumen dynamics without causing clinical disease. Variation in skin thickness and perichondrial adherence also occurs throughout the auricle and external auditory canal, influencing susceptibility to trauma, frostbite, or inflammation. These variations fall within the spectrum of normal anatomy and do not indicate pathology. Accessory auricles are abnormal auricular appendages that persist following formation of the anterior auricle during early embryonic development.[16]
Functional Variability
Physiologic variants of the external ear may produce subtle differences in acoustic perception, particularly in monaural spectral shaping by the pinna. Variations in auricular contour may slightly alter pinna filtering effects, although binaural auditory processing compensates for such differences, preventing clinically meaningful deficits in sound localization or hearing acuity in otherwise healthy individuals.
Similarly, variations in external auditory canal geometry may influence resonance characteristics but remain within the adaptive range of normal auditory function. During use of hearing protection, bone conduction-induced vibrations of the cartilaginous external auditory canal and earplugs generate acoustic pressure within the canal that excites the tympanic membrane.[17]
Clinical Correlates
Recognition of physiologic variants is essential to avoid overdiagnosis of congenital malformations, such as microtia or canal stenosis. Prominent ears, auricular asymmetry, and Darwin tubercles should not be mistaken for syndromic features in the absence of additional craniofacial abnormalities. Likewise, variation in cerumen type or external auditory canal hair distribution should not be interpreted as evidence of dermatologic or infectious disease. Physiologic variants generally become clinically relevant only in procedural settings, such as otoscopic examination, cerumen removal, hearing aid fitting, or otologic surgery. Anatomic variation may influence technical difficulty during these procedures but does not indicate underlying pathology.
Surgical Considerations
Surgery of the external ear requires a detailed understanding of auricular cartilage anatomy, perichondrial blood supply, external auditory canal skin characteristics, and adjacent neurovascular structures. The external ear is particularly vulnerable to cosmetic deformity due to a thin soft-tissue envelope and dependence on perichondrial vascularity for cartilage survival. Therefore, surgical principles emphasize atraumatic tissue handling, preservation of the perichondrium, and consideration of natural auricular subunit anatomy.
Auricular Layers and Surgical Planes
The auricle is organized into 3 principal surgical layers: skin, perichondrium, and elastic cartilage. Auricular skin is thin and tightly adherent to the anterior cartilage surface, increasing susceptibility to ischemia with excessive undermining. The perichondrium is the critical vascular layer supplying avascular cartilage, and preservation of this layer is essential for cartilage viability.
Surgical dissection is typically performed in the subperichondrial plane, allowing elevation of skin flaps while maintaining cartilage perfusion. Disruption of this plane or stripping of the perichondrium may result in cartilage necrosis, deformity, or infection.
Blood Supply and Flap Viability
The external ear has a rich arterial network derived primarily from the posterior auricular, superficial temporal, and occipital arteries, forming a robust anastomotic system. Despite this vascular redundancy, auricular cartilage is avascular and depends entirely on diffusion from the perichondrium. This vascular anatomy supports the use of local auricular flaps, including postauricular advancement flaps and chondrocutaneous flaps, which maintain reliable perfusion when based on these arterial territories. Random-pattern flaps require careful design due to the thin soft-tissue envelope and limited subcutaneous vascularity of the auricle.
Considerations in External Auditory Canal Surgery
Surgery involving the external auditory canal requires awareness of its division into cartilaginous and bony segments and the critical narrowing at the isthmus. The cartilaginous canal is more forgiving and contains adnexal structures, whereas the bony canal is tightly adherent to periosteum and highly sensitive.
Key surgical principles include the following:
- Preservation of canal skin to prevent postoperative stenosis
- Avoidance of excessive cautery in the bony canal due to the risk of osteitis and fibrosis
- Careful instrumentation at the isthmus, the most common site of traumatic injury and postoperative narrowing
- Maintenance of epithelial migration pathways to reduce the risk of keratin accumulation and canal cholesteatoma
Canalplasty procedures must maintain the integrity of the thin bony canal walls. Particular attention is required anteriorly and inferiorly, where dehiscence into the temporomandibular joint or parotid space may occur.
Otoplasty and Auricular Reconstruction
Otoplasty procedures rely on modification of auricular cartilage shape while preserving perichondrial integrity. Techniques such as Mustardé sutures for antihelical fold creation and Furnas sutures for conchal setback manipulate cartilage without complete resection.[18] Key principles include the following:
- Preservation of posterior auricular skin vascularity
- Controlled cartilage scoring or suturing rather than aggressive excision
- Maintenance of auriculocephalic angle symmetry
- Avoidance of hematoma formation, which can rapidly lead to cartilage necrosis and cauliflower ear deformity
Autologous rib cartilage frameworks or porous alloplastic implants are commonly used in reconstructive surgery (eg, microtia reconstruction). Staged reconstruction is often required to recreate auricular subunits.
Potential Surgical Complications and Risks
The most important complication in auricular surgery is auricular hematoma, which separates the perichondrium from cartilage, disrupting diffusion-dependent nutrition and resulting in fibrocartilage overgrowth and permanent deformity. Prompt evacuation and compression are required to prevent permanent structural changes.[19] Other complications include perichondritis and chondritis, often associated with Pseudomonas infection in infected cases. Skin flap necrosis may occur due to compromised perichondrial blood supply. External auditory canal stenosis may develop following overly aggressive resection or postoperative scarring. Sensory nerve injury may result in dysesthesia or chronic auricular pain.
Surgical Landmarks and Neural Preservation
Knowledge of auricular innervation is essential during incision planning. The great auricular nerve is particularly vulnerable during posterior auricular and parotid incisions and requires preservation to prevent lobular and posterior auricular numbness. The auriculotemporal nerve supplies the anterior auricle and may be encountered in temporal incisions. The auricular branch of the vagus nerve may be stimulated during canal surgery, producing a cough reflex or vagal symptoms. This phenomenon is important to consider during awake procedures.[20]
Clinical Correlates
Surgical treatment of the external ear demands careful preservation of the delicate soft-tissue layer and, critically, the blood supply to the perichondrium that nourishes the avascular auricular cartilage. Procedures such as otoplasty, reconstruction, and external auditory canal surgery require precise dissection along the subperichondrial plane to sustain cartilage health and avoid deformities.
The external auditory canal presents additional challenges due to its narrow, S-shaped configuration, particularly at the bony–cartilaginous junction. Instrumentation or excision in this region increases the risk of pain, bleeding, and postoperative canal narrowing.
The most serious complication in auricular surgery is auricular hematoma. This condition separates the perichondrium from cartilage, compromises cartilage nutrition, and may rapidly progress to permanent deformity, known as cauliflower ear, if not promptly drained and compressed.
Additional risks include perichondritis, often infectious and destructive to cartilage; skin flap necrosis due to reduced blood flow; iatrogenic canal stenosis from scarring; and sensory disturbance resulting from injury to the great auricular or auriculotemporal nerve. Overall surgical success relies on gentle tissue handling, preservation of vascularized perichondrium, and prevention of hematoma formation and infection, all of which are essential to avoid long-term structural and functional complications.
Clinical Significance
The external ear comprises the auricle and external auditory canal, extending from the conchal bowl to the lateral surface of the tympanic membrane. The external ear is a specialized cutaneous–cartilaginous organ designed to optimize acoustic energy capture, frequency-dependent spectral filtering, and spatial localization while simultaneously providing mechanical protection to the middle and inner ear. Complex 3-dimensional architecture enhances sound collection and directional cueing, particularly in the vertical and anterior–posterior planes, while the external auditory canal functions as a resonant, self-cleaning conduit that amplifies speech-frequency sound and maintains epithelial migration for debris clearance. Clinically, the external ear is highly relevant due to susceptibility to trauma, infection, cerumen-related obstruction, neoplastic change, and congenital malformations, with characteristic disease patterns that closely reflect unique anatomy, vascular supply, and neurocutaneous organization.
Age-Related Changes and Physiologic Variation
The external ear demonstrates predictable age-related morphologic changes. Auricular dimensions increase over time, primarily due to ongoing elastic cartilage remodeling and loss of structural recoil. The lobule, which lacks cartilage and is composed of fibrofatty connective tissue, is particularly susceptible to gravitational elongation, resulting in progressive inferior elongation with age. These changes are physiologic and do not reflect pathology, though they may become clinically relevant in cosmetic surgery, otoplasty planning, and interpretation of auricular asymmetry in older adults.
Piercing-Related Complications and Keloid Formation
The auricle is frequently subject to body modification, particularly lobular piercing, which is generally well tolerated due to the absence of cartilage and robust vascularity. In contrast, cartilaginous ear piercings are associated with a higher rate of complications, including delayed healing, infection, and perichondritis, due to the relatively avascular nature of auricular cartilage and dependence on perichondrial diffusion for nutrient supply.
A significant complication of auricular piercing is keloid formation, particularly in genetically predisposed individuals.[21] Keloids present as firm, pruritic, hyperpigmented, or erythematous nodular masses extending beyond the original wound boundary. Epidemiologically, individuals with darker skin pigmentation have a markedly increased risk, with reported incidence up to an order of magnitude higher than in lighter-skinned populations. Clinically, counseling should emphasize avoidance of unnecessary skin trauma, as recurrence is common, and lesions may develop at new sites of injury.
Trauma and Auricular Deformity
The auricle is highly vulnerable to blunt trauma due to its exposed position and thin perichondrial envelope. Repetitive shearing injury or acute blunt force may result in auricular hematoma, characterized by blood accumulation between cartilage and perichondrium. Disruption of diffusion-dependent cartilage nutrition leads to ischemia, chondrocyte death, and fibrocartilaginous overgrowth. Untreated or recurrent hematoma results in permanent structural distortion known as cauliflower ear, classically associated with contact sports, such as boxing and wrestling.
External Ear Infections and Inflammatory Conditions
Otitis externa is an inflammatory condition of the external auditory canal, most commonly infectious in origin. Typical pathogens include Pseudomonas aeruginosa and Staphylococcus aureus, particularly in cases of swimmer’s ear, which occurs following prolonged exposure to moist or contaminated aquatic environments. Clinical manifestations include otalgia, pruritus, canal edema, and otorrhea. Otoscopic examination typically demonstrates erythematous, narrowed, and tender canal walls. Early characteristic findings may include reduced or absent cerumen due to impaired glandular function in the inflamed epithelium.[22] Management primarily involves topical antimicrobial and anti-inflammatory therapy, with systemic antibiotics reserved for complicated or invasive disease.
A distinct but related entity is surfer’s ear (external auditory canal exostosis), a reactive bone formation within the bony canal secondary to chronic cold-water exposure. This condition differs from otitis externa in that it is noninfectious, slowly progressive, and may lead to canal obstruction and conductive hearing loss.[23] Rare but important conditions include aural myiasis, in which fly larvae infest the external auditory canal, and foreign body insertion, particularly in pediatric populations, which may result in secondary infection, trauma, and conductive hearing loss.[24][25]
Cerumen Physiology and Impaction
Cerumen is continuously produced in the cartilaginous external auditory canal by ceruminous and sebaceous glands. Protective functions include lubrication, hydrophobic barrier formation, and antimicrobial activity. Disruption of normal epithelial migration or improper ear cleaning practices, particularly the use of cotton-tipped applicators, may result in cerumen impaction. Cotton swabs frequently exacerbate impaction by pushing cerumen medially toward the narrow bony–cartilaginous junction.
Clinical presentation of cerumen impaction includes conductive hearing loss, aural fullness, and, occasionally, otalgia or secondary infection. Management includes the use of cerumenolytic agents followed by irrigation or manual removal. Instrumentation requires caution due to the risk of vagal stimulation via the auricular branch of the vagus nerve, which may provoke cough, dizziness, or, rarely, bradycardia.[26]
Environmental Exposure and Cutaneous Pathology
The auricle is highly exposed to environmental stressors, making it a common site for actinic damage.[27] Chronic ultraviolet exposure predisposes to actinic keratoses, cutaneous horns, basal cell carcinoma, squamous cell carcinoma, and melanoma. Early recognition is essential due to the thin soft-tissue envelope and rich regional lymphatic drainage, which facilitates early metastatic spread. Conversely, the external ear is also highly susceptible to cold injury, including frostbite, due to minimal subcutaneous insulation and terminal vascular supply. The helical rim is particularly vulnerable.[28]
Congenital and Developmental Abnormalities
Congenital anomalies of the external ear reflect disruptions in 1st and 2nd pharyngeal arch development or failure of external auditory canal canalization. Common abnormalities include microtia, anotia, auricular dysplasia, and external auditory canal atresia, all of which may present with conductive hearing loss.[29]
Preauricular pits and tags, located anterior to the tragus, arise from abnormal fusion of auricular hillocks or supernumerary hillock formation. These lesions may occur as isolated findings or part of syndromic conditions, such as branchio-oto-renal syndrome, in which renal anomalies may coexist. Accordingly, neonatal identification of preauricular anomalies often warrants renal ultrasonography to exclude associated malformations. Additional syndromic associations include Treacher Collins and Crouzon syndromes, both involving 1st- and 2nd-arch derivatives and potentially presenting with auricular hypoplasia and external auditory canal abnormalities.[30][31]
Clinical Correlates
The external ear is susceptible to age-related elongation, trauma-induced hematoma formation, infection (otitis externa), environmental injury, and frequent involvement in congenital syndromes and dermatologic malignancies. Cartilaginous piercings are prone to infection and keloid formation due to limited vascularity, whereas auricular hematoma is the primary precursor to cauliflower ear. The external auditory canal is vulnerable to cerumen impaction, foreign bodies, and exostotic bone formation, with the narrow isthmus serving as a key site of obstruction and pain. Preauricular anomalies serve as clinical markers for underlying syndromic disease and warrant systemic evaluation when identified.[32][33][34][35][36]
Other Issues
Beyond its primary roles in sound conduction and localization, the external ear has additional anatomic, physiologic, and procedural characteristics with important clinical implications. These features often explain unexpected symptoms during routine otologic care and account for recurrent outpatient presentations, particularly involving pain, obstruction, and iatrogenic injury.
Skin-Perichondrial Vulnerability and Ischemic Risk
A defining feature of the auricle is thin, tightly adherent skin overlying avascular elastic cartilage, which depends entirely on the perichondrium for nutrient diffusion. This structural dependence creates marked vulnerability to ischemic injury. Even small degrees of perichondrial separation, such as from hematoma, infection, or aggressive instrumentation, can rapidly compromise cartilage viability. This mechanism explains the high risk of permanent deformity after auricular hematoma and the relative unpredictability of cartilage survival following infection or trauma.
Structural Basis of External Auditory Canal Pain Sensitivity
The external auditory canal demonstrates marked pain sensitivity, particularly within the bony portion, where skin is directly adherent to periosteum with minimal intervening tissue. This anatomic configuration produces a characteristic clinical pattern in which minor inflammation may result in severe otalgia, often disproportionate to visible findings. This feature is a key diagnostic indicator of otitis externa and helps distinguish it from middle ear disease, which typically produces pressure or fullness rather than focal canal tenderness.
Chondrodermatitis Nodularis Helicis
Chondrodermatitis nodularis helicis (CNH) is a benign but often highly symptomatic inflammatory condition involving auricular cartilage and the overlying skin, typically affecting the helix or antihelix. CNH presents as a small, firm, erythematous to flesh-colored papule or nodule with a central crust or ulceration, classically occurring on the superior helix in men and the antihelix in women, often on the side exposed to chronic pressure, such as during sleep. Despite its limited size, CNH is typically associated with disproportionately severe localized tenderness, often described as sharp or burning pain exacerbated by pressure. The pathophysiology is believed to involve ischemic necrosis of cartilage secondary to chronic pressure and compromised perichondrial perfusion, leading to localized inflammatory degeneration. Histology demonstrates dermal and perichondrial inflammation with underlying cartilage degeneration.
Management is often frustrating and may be only partially effective, emphasizing conservative measures, such as pressure offloading with protective padding or specialized pillows. Topical therapies and intralesional corticosteroids have variable success, while definitive treatment may require surgical excision of involved cartilage and overlying skin in refractory cases. Recurrence is not uncommon, reinforcing CNH as a painful, benign, but difficult-to-eradicate auricular lesion.[37]
Vagal Reflex Susceptibility
The external auditory canal is one of the few cutaneous regions with direct vagal sensory input via the auricular branch of the vagus nerve. Therefore, mechanical stimulation during cerumen removal, otoscopy, or foreign body extraction may trigger reflex coughing, gagging, dizziness, or, rarely, transient bradycardia. This reflex pathway is clinically important in procedural settings, particularly in pediatric or sensitive patients, and explains unexpected systemic responses during otherwise localized ear manipulation.
Cerumen Dynamics and Failure of Self-Cleaning Mechanisms
The external ear normally functions as a self-cleaning system driven by epithelial migration outward from the tympanic membrane. Failure of this system, whether due to canal narrowing, chronic inflammation, dermatologic disease, or mechanical disruption, leads to cerumen retention and impaction. Cerumen is not a waste product but a biologically active secretion with antimicrobial and hydrophobic properties. Removal beyond physiologic levels may predispose to recurrent otitis externa and canal dryness.
Overcleaning is a major iatrogenic cause of external ear disease. Cotton swab use is a frequent contributor, as cerumen is often displaced medially toward the narrow isthmus rather than removed.
Environmental Vulnerability of the External Ear
The auricle is uniquely exposed to environmental extremes, resulting in disproportionate susceptibility to ultraviolet radiation–induced actinic keratosis and squamous cell carcinoma, cold injury with frostbite of the helical rim, mechanical shear leading to auricular hematoma, and chronic moisture predisposing to infectious otitis externa. The helical rim is the most vulnerable site for frostbite and ischemic necrosis due to its distal vascular supply and a thin soft-tissue envelope.
Anatomic Variability and Procedural Complications
The external auditory canal demonstrates significant interindividual variability in curvature, diameter, and angulation, with direct clinical impact on ease of otoscopy, risk of traumatic instrumentation, cerumen retention tendency, and hearing aid fit and tolerance. Failure to appreciate canal angulation is a common cause of iatrogenic canal trauma during otoscopy or suctioning, particularly when inadequate auricular retraction prevents straightening of the canal.
Neuroanatomic Basis of Referred Ear Pain
The external ear serves as a frequent site of referred pain due to overlapping innervation from the trigeminal, facial, glossopharyngeal, and vagus nerves, as well as the cervical plexus. Therefore, a normal otoscopic examination in the setting of otalgia should prompt evaluation for temporomandibular joint dysfunction, dental pathology, pharyngeal or tonsillar inflammation, cervical spine disease, and laryngeal or hypopharyngeal pathology. A key clinical principle is that otalgia with a normal ear examination indicates a nonotologic source until proven otherwise.
Additional Clinical Pearls
Auricular cartilage survival depends entirely on an intact perichondrium. Prevention of hematoma formation is critical.
Severe otalgia with minimal otoscopic findings and marked tenderness may suggest otitis externa. This presentation is particularly relevant in children with a history of water exposure.
Canal instrumentation may trigger a vagal reflex cough or bradycardia via the auricular branch of the vagus nerve. This response may occur during otologic procedures or cerumen removal.
Cotton swabs are a leading cause of cerumen impaction and canal trauma. Medial displacement of cerumen and epithelial injury commonly result from their use.
The helical rim is the most frostbite-prone region of the external ear. Vulnerability reflects distal vascularity and a thin soft-tissue envelope.
Normal otoscopy does not exclude significant referred head and neck pathology. Evaluation of nonotologic sources is essential in unexplained otalgia.
Media
(Click Image to Enlarge)
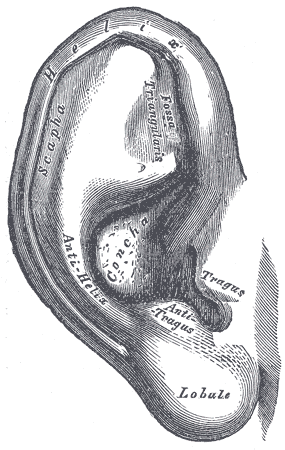
External Ear. This illustration shows the anatomic relationships between the helix, scapha, fossa triangularis, antihelix, concha, antitragus, tragus, and lobule.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
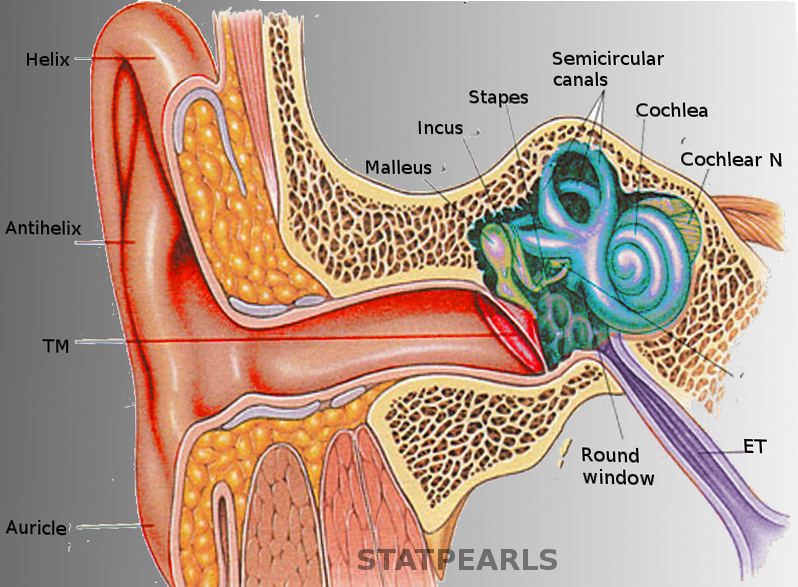
Ear Anatomy. This illustration shows the anatomic relationships between the helix, antihelix, auricle, tympanic membrane, malleus, incus, stapes, round window, semicircular canals, cochlea, cochlear nerve, and eustachian tube.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
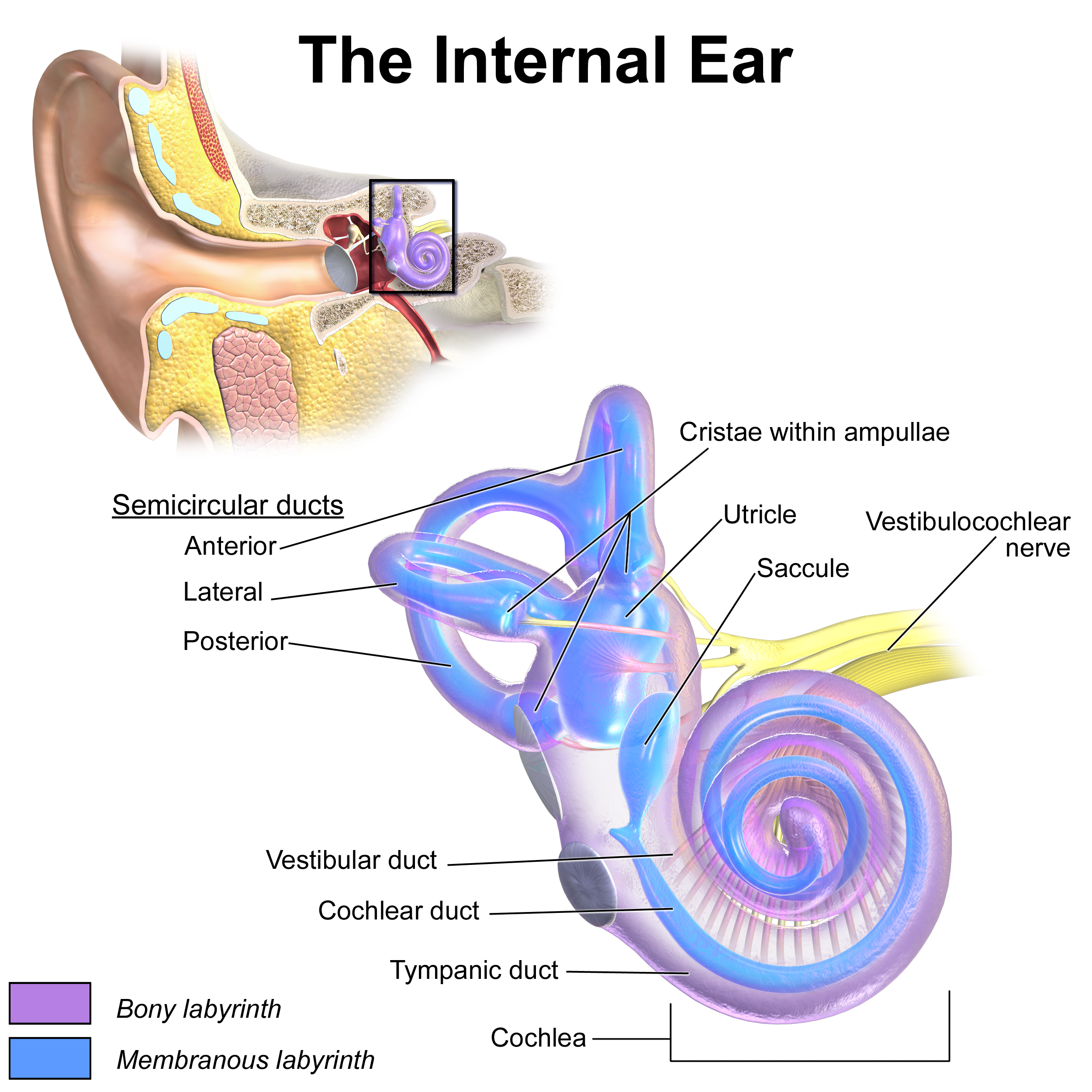
Inner Ear Anatomy. This illustration shows the semicircular ducts and parts of the cochlea.
Blausen.com staff. Medical Gallery of Blausen Medical 2014. WikiJournal of Medicine. doi: 10.15347/wjm/2014.010.
References
White HJ, Helwany M, Biknevicius AR, Peterson DC. Anatomy, Head and Neck, Ear Organ of Corti. StatPearls. 2026 Jan:(): [PubMed PMID: 30855919]
Altafulla J, Iwanaga J, Lachkar S, Prickett J, Dupont G, Yilmaz E, Ishak B, Litvack Z, Tubbs RS. The Great Auricular Nerve: Anatomical Study with Application to Nerve Grafting Procedures. World neurosurgery. 2019 May:125():e403-e407. doi: 10.1016/j.wneu.2019.01.087. Epub 2019 Jan 28 [PubMed PMID: 30703599]
Young AS, Rosengren SM, Welgampola MS. Disorders of the inner-ear balance organs and their pathways. Handbook of clinical neurology. 2018:159():385-401. doi: 10.1016/B978-0-444-63916-5.00025-2. Epub [PubMed PMID: 30482329]
Zazali S, Retinasekharan S. Otorrhea as a Resolution for a Parotid Abscess through an Unusual Natural Pathway: A Case Report and Recent Literature Review. Iranian journal of otorhinolaryngology. 2022 Mar:34(121):135-138. doi: 10.22038/IJORL.2021.58379.3014. Epub [PubMed PMID: 35655770]
Level 3 (low-level) evidenceLoh TY, Cohen PR. Darwin's Tubercle: Review of a Unique Congenital Anomaly. Dermatology and therapy. 2016 Jun:6(2):143-9. doi: 10.1007/s13555-016-0109-6. Epub 2016 Apr 7 [PubMed PMID: 27055539]
Narayanan DA, Raman R, Chong AW. The Role of Occlusion of the External Ear Canal in Hearing Loss. Turkish archives of otorhinolaryngology. 2019 Sep:57(3):122-126. doi: 10.5152/tao.2019.3875. Epub 2019 Sep 1 [PubMed PMID: 31620693]
van der Heijden K, Rauschecker JP, de Gelder B, Formisano E. Cortical mechanisms of spatial hearing. Nature reviews. Neuroscience. 2019 Oct:20(10):609-623. doi: 10.1038/s41583-019-0206-5. Epub 2019 Aug 29 [PubMed PMID: 31467450]
Hartmann WM, Rakerd B, Crawford ZD, Zhang PX. Transaural experiments and a revised duplex theory for the localization of low-frequency tones. The Journal of the Acoustical Society of America. 2016 Feb:139(2):968-85. doi: 10.1121/1.4941915. Epub [PubMed PMID: 26936576]
Fischer T, Schmid C, Kompis M, Mantokoudis G, Caversaccio M, Wimmer W. Pinna-Imitating Microphone Directionality Improves Sound Localization and Discrimination in Bilateral Cochlear Implant Users. Ear and hearing. 2021 Jan/Feb:42(1):214-222. doi: 10.1097/AUD.0000000000000912. Epub [PubMed PMID: 32701730]
Capshaw G, Brown AD, Peña JL, Carr CE, Christensen-Dalsgaard J, Tollin DJ, Womack MC, McCullagh EA. The continued importance of comparative auditory research to modern scientific discovery. Hearing research. 2023 Jun:433():108766. doi: 10.1016/j.heares.2023.108766. Epub 2023 Apr 6 [PubMed PMID: 37084504]
Level 2 (mid-level) evidenceMozaffari M, Nash R, Tucker AS. Anatomy and Development of the Mammalian External Auditory Canal: Implications for Understanding Canal Disease and Deformity. Frontiers in cell and developmental biology. 2020:8():617354. doi: 10.3389/fcell.2020.617354. Epub 2021 Jan 8 [PubMed PMID: 33553153]
Level 3 (low-level) evidenceAnthwal N, Thompson H. The development of the mammalian outer and middle ear. Journal of anatomy. 2016 Feb:228(2):217-32. doi: 10.1111/joa.12344. Epub 2015 Jul 30 [PubMed PMID: 26227955]
Helwany M, Arbor TC, Tadi P. Embryology, Ear. StatPearls. 2026 Jan:(): [PubMed PMID: 32491520]
Cox TC, Camci ED, Vora S, Luquetti DV, Turner EE. The genetics of auricular development and malformation: new findings in model systems driving future directions for microtia research. European journal of medical genetics. 2014 Aug:57(8):394-401. doi: 10.1016/j.ejmg.2014.05.003. Epub 2014 May 29 [PubMed PMID: 24880027]
Level 3 (low-level) evidenceEl-Anwar MW, Fouad YA, Elgohary AF, Saber S, Mobasher MA. External Auditory Canal: Computed Tomography Analysis and Classification. International archives of otorhinolaryngology. 2023 Oct:27(4):e565-e570. doi: 10.1055/s-0042-1758213. Epub 2023 Sep 19 [PubMed PMID: 37876695]
Hwang J, Cho J, Burm JS. Accessory auricle: Classification according to location, protrusion pattern and body shape. Archives of plastic surgery. 2018 Sep:45(5):411-417. doi: 10.5999/aps.2018.00430. Epub 2018 Sep 15 [PubMed PMID: 30282411]
Homma K, Du Y, Shimizu Y, Puria S. Ossicular resonance modes of the human middle ear for bone and air conduction. The Journal of the Acoustical Society of America. 2009 Feb:125(2):968-79. doi: 10.1121/1.3056564. Epub [PubMed PMID: 19206873]
Nazarian R, Eshraghi AA. Otoplasty for the protruded ear. Seminars in plastic surgery. 2011 Nov:25(4):288-94. doi: 10.1055/s-0031-1288921. Epub [PubMed PMID: 23115535]
Dalal PJ, Purkey MR, Price CPE, Sidle DM. Risk factors for auricular hematoma and recurrence after drainage. The Laryngoscope. 2020 Mar:130(3):628-631. doi: 10.1002/lary.28310. Epub 2019 Oct 17 [PubMed PMID: 31621925]
Ng KB, Guiu Hernandez E, Haszard J, Macrae P, Huckabee ML, Cakmak YO. Transcutaneous auricular vagus nerve stimulation alters cough sensitivity depending on stimulation parameters: potential implications for aspiration risk. Frontiers in neuroscience. 2024:18():1265894. doi: 10.3389/fnins.2024.1265894. Epub 2024 Feb 8 [PubMed PMID: 38406583]
Adigun IA, Aderibigbe AB. Earlobe keloids: emerging cosmetic complication of ear-piercing. Nigerian quarterly journal of hospital medicine. 2010 Apr-Jun:20(2):97-100 [PubMed PMID: 21243860]
Medina-Blasini Y, Sharman T. Otitis Externa. StatPearls. 2026 Jan:(): [PubMed PMID: 32310515]
Bart RM, Lau H, Cooper JS. Surfer's Ear. StatPearls. 2026 Jan:(): [PubMed PMID: 30521295]
Al Jabr I. Aural Myiasis, a Rare Cause of Earache. Case reports in otolaryngology. 2015:2015():219529. doi: 10.1155/2015/219529. Epub 2015 Aug 24 [PubMed PMID: 26380140]
Level 3 (low-level) evidenceLotterman S, Sutton AE, Hohman MH. Ear Foreign Body Removal. StatPearls. 2026 Jan:(): [PubMed PMID: 29083719]
Sevy JO, Hohman MH, Singh A. Cerumen Impaction Removal. StatPearls. 2026 Jan:(): [PubMed PMID: 28846265]
Özgür E, Kamiloğlu U, Temiz P, Eskiizmir G. Skin Cancers of the Auricle: A Retrospective Analysis of 41 Patients. Turkish archives of otorhinolaryngology. 2020 Sep:58(3):169-173. doi: 10.5152/tao.2020.5701. Epub 2020 Sep 1 [PubMed PMID: 33145501]
Level 2 (mid-level) evidenceLehmuskallio E, Lindholm H, Koskenvuo K, Sarna S, Friberg O, Viljanen A. Frostbite of the face and ears: epidemiological study of risk factors in Finnish conscripts. BMJ (Clinical research ed.). 1995 Dec 23-30:311(7021):1661-3 [PubMed PMID: 8541749]
Level 2 (mid-level) evidenceAndrews J, Kopacz AA, Hohman MH. Ear Microtia. StatPearls. 2026 Jan:(): [PubMed PMID: 33085390]
Chang CC, Steinbacher DM. Treacher collins syndrome. Seminars in plastic surgery. 2012 May:26(2):83-90. doi: 10.1055/s-0032-1320066. Epub [PubMed PMID: 23633935]
Kaushik A, Bhatia H, Sharma N. Crouzon's Syndrome: A Rare Genetic Disorder. International journal of clinical pediatric dentistry. 2016 Oct-Dec:9(4):384-387. doi: 10.5005/jp-journals-10005-1395. Epub 2016 Dec 5 [PubMed PMID: 28127173]
Hohman MH, Jamal Z, Krogmann RJ, King KC. Auricular Hematoma. StatPearls. 2026 Jan:(): [PubMed PMID: 30285394]
Szmuilowicz J, Young R. Infections of the Ear. Emergency medicine clinics of North America. 2019 Feb:37(1):1-9. doi: 10.1016/j.emc.2018.09.001. Epub [PubMed PMID: 30454772]
Osborn HA, Goldsmith TA, Varvares MA. Assessing functional outcomes in head and neck surgical oncology. Head & neck. 2019 Jul:41(7):2051-2057. doi: 10.1002/hed.25656. Epub 2019 Jan 30 [PubMed PMID: 30698897]
Markkanen S, Niemi P, Rautiainen M, Saarenpää-Heikkilä O, Himanen SL, Satomaa AL, Peltomäki T. Craniofacial and occlusal development in 2.5-year-old children with obstructive sleep apnoea syndrome. European journal of orthodontics. 2019 May 24:41(3):316-321. doi: 10.1093/ejo/cjz009. Epub [PubMed PMID: 30925192]
Birgfeld C, Heike C. Craniofacial Microsomia. Clinics in plastic surgery. 2019 Apr:46(2):207-221. doi: 10.1016/j.cps.2018.12.001. Epub [PubMed PMID: 30851752]
Morgado-Carrasco D, Fustà-Novell X, Podlipnik S, Ferrandiz L. Dermoscopic Features of Chondrodermatitis Nodularis Chronica Helicis: A Case Series. Dermatology practical & conceptual. 2019 Jan:9(1):52-53. doi: 10.5826/dpc.0901a12. Epub 2019 Jan 31 [PubMed PMID: 30775149]
Level 2 (mid-level) evidence