Introduction
Eagle syndrome was named after Dr Watt W Eagle, MD, an otolaryngologist at Duke University, who described the first cases in 1937. This rare condition is caused by an elongated or disfigured styloid process, which interferes with the functioning of neighboring structures and gives rise to orofacial and cervical pain often triggered by neck movements. (See Image. Eagle Syndrome.) Eagle syndrome is also referred to as stylohyoid syndrome, styloid syndrome, or styloid–carotid artery syndrome by some authors. Please see StatPearls' companion resource, "Anatomy, Head and Neck, Styloid Process," for further information.[1][2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
There is debate regarding the etiology of Eagle syndrome. Dr Watt Eagle proposed that surgical trauma (eg, tonsillectomy) or local chronic irritation could cause osteitis, periostitis, or tendonitis of the styloid process and the stylohyoid ligaments, leading to reactive, ossifying hyperplasia. In 1975, Francesco Lentini proposed that persistent mesenchymal elements, also known as Reichert cartilage residues, could undergo osseous metaplasia in response to an appropriate traumatic or stressful event.
In 1962, Epifanio proposed that ossification of the styloid process was associated with endocrine disorders in women during menopause, who also had ossification of other ligaments in the body. In 2008, Gokce et al reported that patients with end-stage renal disease and abnormal calcium, phosphorus, and vitamin D metabolism developed heterotopic calcification, which elongated the styloid process and led to Eagle syndrome.[3] Finally, a 2015 retrospective study by Sekerci indicated that an arcuate foramen is associated with an elongated styloid process. Results were derived from data from 542 patients using 3-dimensional (3D) computed tomography scans.[4][5]
Epidemiology
Dr Watt Eagle initially reported that the normal styloid process was approximately 2.5 cm in length, and any styloid process longer than 2.5 cm might be considered abnormally elongated. Results from a postmortem study of 80 cadavers found that the styloid process ranged from 1.52 to 4.77 cm in length. An elongated styloid process is incidental in about 4% of the general population, but of these, only about 4% present with symptoms that are attributable to the elongation of the styloid. Therefore, the true incidence is about 0.16%, with a female-to-male predominance of 3:1. Patients are usually older than 30 years, and the elongated styloid process is usually bilateral (although unilateral cases also occur).[6][7]
Pathophysiology
Previously, it was hypothesized that scar tissue formation around the styloid apex after tonsillectomy would compress and strain the neurovascular structures in the retrostyloid compartment. However, Eagle syndrome also presents in patients who have never had a tonsillectomy. Several mechanisms have been proposed to explain the pathogenesis of pain in Eagle syndrome. The first theory is that the elongated styloid process compresses cranial nerves, most commonly cranial nerve IX (glossopharyngeal nerve), leading to throat and neck pain. Alternatively, the styloid process can compress the internal carotid artery, causing transient ischemic attacks, or compress the sympathetic nerves that run alongside the artery, leading to a range of symptoms.
The pain in Eagle syndrome often resembles glossopharyngeal neuralgia but is typically dull and more constant. However, cases of sharp, intermittent pain along the course of the glossopharyngeal nerve have also been reported. Furthermore, theories of reactive hyperplasia and reactive metaplasia exist, which attribute the elongation to either overgrowth of the styloid process itself or to ossification of the stylohyoid ligament complex after trauma. This phenomenon may explain the incidence of Eagle syndrome after tonsillectomy, as originally described by Dr Eagle.
Other possible causes include angulation of an abnormally long styloid process, which can irritate adjacent musculature or mucosa. Stretching and fibrosis involving cranial nerves V, VII, IX, and X in the posttonsillectomy period could also be a possible etiology. Finally, the symptoms may be due to normal aging. Because aging is associated with decreased soft-tissue elasticity, degenerative changes, and inflammatory conditions in the tendinous portion of the stylohyoid insertion, insertion tendinosis may cause pain in the distribution of the glossopharyngeal nerve that resembles Eagle syndrome. To avoid confusion, this manifestation is called pseudostyloid syndrome.[8][9][10]
History and Physical
Eagle syndrome most frequently presents in the third or fourth decades of life. Although there is no significant sex predilection in the mineralization of the styloid process, symptoms are more common in women. Symptoms range from mild discomfort to acute neurologic and referred pain, and are divided into 2 groups: classic Eagle syndrome and vascular Eagle syndrome.
Classic Eagle syndrome usually occurs after pharyngeal trauma or tonsillectomy. Pain is presumably a consequence of stretching or compression of the cranial nerves V, VII, VIII, IX, or X or their nerve endings in the tonsillar fossa during healing (eg, scar tissue). Although an elongated styloid process may cause episodic tic-like pain attacks typical of glossopharyngeal neuralgia, most patients present with constant, dull pharyngeal pain in the ipsilateral tonsillar fossa that may radiate to the ear and is aggravated by head rotation.
Other symptoms include the sensation of a foreign body in the pharynx (55%), dysphagia, odynophagia, otalgia, headache, pain along the distribution of the external and internal carotid arteries, pain on cervical rotation or mastication, facial pain, and tinnitus. Furthermore, a mass or bulge may be palpated in the ipsilateral tonsillar fossa, exacerbating the patient’s symptoms. Classic Eagle syndrome is usually unilateral, but can present bilaterally in rare cases.
Vascular Eagle syndrome, or stylocarotid syndrome, results from compression of the internal or external carotid artery (along with its perivascular sympathetic fibers) by a laterally or medially deviated styloid process. In these cases, turning the head can compress the artery, causing pain along its distribution. This compression can lead to transient ischemic attacks, vertigo, and syncope. Usually, there is no history of tonsillectomy. In cases of internal carotid artery impingement, pain is often referred to the supraorbital region. In cases of irritation of the external carotid artery, the pain radiates to the infraorbital region.
In patients presenting with throat pain, dysphagia, or foreign body sensation, cervical spine disease such as ankylosing spondylitis should be a consideration. Cervical spinal pain may mimic symptoms of Eagle syndrome, particularly when cervical motion is limited and ossification is evident on imaging. Differences in underlying cervical pathology can be clarified with targeted imaging and rheumatologic assessment.[11]
Evaluation
The diagnosis of Eagle syndrome is based on a complete medical history and physical examination. Pain in the throat that radiates to the neck, ear, or face is often nonspecific and may be due to several conditions, including a malignant neoplasm of the upper aerodigestive tract, neuralgia, or temporomandibular joint dysfunction. These conditions should be excluded before considering Eagle syndrome. Eagle syndrome usually presents with a characteristic dull, throbbing pain in the elongated styloid process that worsens with deglutition and can be reproduced by palpation of the tonsillar fossa.
Insertion tendonitis can also resemble Eagle syndrome. However, tendonitis usually causes tenderness over the greater horn of the hyoid bone. An elongated styloid process can be palpated intraorally by placing the index finger in the tonsillar fossa and applying gentle pressure. If the pain is reproduced by palpation and is referred to the ear, face, or head, the diagnosis of an elongated styloid process is most likely. A normal-length styloid process is usually impalpable.
The diagnosis of an elongated styloid process is then confirmed by imaging. Elongation of the styloid process is often defined by length, but specific measurement thresholds vary across populations. Recent evidence suggests that a diagnostic cutoff of 32.5 mm on imaging provides superior accuracy compared with historically arbitrary length criteria, improving differentiation between normal variation and clinically significant elongation.[12]
Several imaging techniques have been used, but CT is the most accurate. Three-dimensional CT reconstruction of the neck enables precise measurement of the lengths of the styloid process and the ossified stylohyoid ligament. The normal length of the adult styloid process is approximately 2.5 cm, while a length greater than 3 cm is considered elongated. If this criterion is used, almost 4% of the population has an elongated process. However, only a small proportion (4%-10%) is symptomatic. Orthopantomography and CT can both be used to assess the styloid process and stylohyoid ligament complex.
If mechanical vascular compression is a potential cause of ischemic symptoms, angiographic examination (CT angiography or catheter angiography) should be performed with the patient's head positioned to reproduce symptoms and demonstrate mechanical stenosis of the carotid artery. CT angiography is recommended when vascular symptoms are present because it can demonstrate carotid artery compression, dissection, or irritation in the stylocarotid variant of Eagle syndrome.[13] Dynamic magnetic resonance angiography can evaluate the relationship between the internal carotid artery and the styloid process during neck motion, and may therefore be a useful diagnostic technique for vascular Eagle syndrome in patients who cannot receive contrast media.[14]
Treatment / Management
The elongated styloid process syndrome can be managed conservatively or surgically. Conservative treatments include analgesics, antidepressant medications, anticonvulsants, transpharyngeal injection of corticosteroids and lidocaine, diazepam, nonsteroidal anti-inflammatory drugs, and topical heat. Transpharyngeal manipulation with manual fracture of the elongated styloid process rarely relieves symptoms and risks damage to adjacent neurovascular structures. Patients who do not improve after multiple medication trials may require surgical intervention.[15](B3)
The most effective treatment is the surgical shortening of the styloid process, either via an intraoral or external approach, because it produces better long-term results. The advantages of an intraoral approach include the simplicity of the technique, reduced operating time, feasibility under local anesthesia, and the absence of a visible external scar. However, the main disadvantages are a lack of access, particularly in the event of hemorrhage and deep neck space infections, poor visualization of the surgical field (especially in patients with significantly reduced jaw opening), risk of iatrogenic injury to major neurovascular structures, and alterations of speech and swallowing from postoperative edema.
The most significant advantage of an external approach is optimal exposure of the styloid process and adjacent structures. This approach also facilitates the removal of a partially ossified stylohyoid ligament. Major disadvantages include a longer operative time, the risk of injury to the facial nerve and its branches, a disfiguring neck scar, and a longer recovery period.
The surgeon's specialty usually determines the surgical approach. However, surgical failures have been reported in up to 20% of patients.[16][17][18] When patients are appropriately selected, surgical styloidectomy provides durable symptom relief, with results from recent systematic reviews demonstrating high success rates and acceptable complication profiles for both transcervical and transoral approaches.[19](A1)
Differential Diagnosis
The following conditions must be excluded before arriving at a diagnosis of Eagle syndrome:
- Cervical arthritis
- Cervical mass
- Ill-fitting dental prostheses
- Migraine-type headaches
- Esophageal diverticula
- Otitis
- Tumors
- Salivary gland disease
- Temporal arteritis
- Trigeminal neuralgia
Prognosis
The prognosis of Eagle syndrome is generally favorable when the condition is accurately diagnosed and appropriately managed. Many patients experience partial symptom relief with conservative measures such as analgesics, anti-inflammatory medications, or local anesthetic and corticosteroid injections. However, symptoms often persist in patients with significant styloid elongation or neurovascular involvement.
Surgical treatment, usually styloidectomy, is associated with high rates of symptom improvement and patient satisfaction. Results from a retrospective cohort study demonstrated significant reductions in pain scores and improvements in quality of life following transcervical styloidectomy.[20] Furthermore, findings from systematic reviews and meta-analyses indicate that surgical management generally yields superior outcomes compared with conservative therapy, particularly in patients with the neurovascular (stylocarotid) variant of Eagle syndrome.[21]
Findings from large surgical case series report that the majority of patients experience either complete resolution or substantial improvement of symptoms after operative intervention, including relief of pain, dysphagia, and dizziness.[22] More recent study findings of minimally invasive cervical styloidectomy techniques demonstrate high effectiveness, with more than 90% of patients reporting significant pain reduction or overall procedural success at follow-up.[23]
Patients with the vascular variant of Eagle syndrome may have a higher risk of serious complications if untreated. Therefore, early recognition and appropriate imaging evaluation are important to optimize outcomes. Overall, with timely diagnosis and individualized management, most patients with Eagle syndrome can expect meaningful and sustained symptom improvement.
Complications
Complications of Eagle syndrome may arise from mechanical compression or irritation of adjacent neurovascular structures, particularly in the stylocarotid variant. Compression of the internal or external carotid artery can result in symptoms ranging from localized cervicofacial pain to serious vascular events, including transient ischemic attacks or ischemic stroke in rare cases.[13] Moreover, chronic irritation of adjacent cranial nerves (usually V, VII, IX, and X) may result in persistent throat pain, dysphagia, otalgia, a foreign-body sensation, or voice changes. Symptoms may worsen with head rotation or swallowing, and dynamic imaging has demonstrated positional vascular and neural compression in patients with symptoms.[24]
Surgical management is generally effective but carries procedure-related risks. Reported complications of styloidectomy include infection, hemorrhage, cranial nerve injury, dysphagia, and transient sensory disturbances. Transoral approaches may carry a higher risk of deep neck space infection, whereas transcervical approaches may result in visible scarring or injury to the marginal mandibular nerve.[19] Rarely, incomplete resection or misidentification of the pain generator may lead to persistent or recurrent symptoms. Careful preoperative imaging, accurate diagnosis, and appropriate surgical planning are essential to reduce recurrence and improve long-term outcomes.[20]
Deterrence and Patient Education
Patient education plays a critical role in the management of Eagle syndrome, particularly in preventing symptom exacerbation, avoiding unnecessary interventions, and promoting timely evaluation. Patients should be informed that Eagle syndrome results from elongation or abnormal angulation of the styloid process or calcification of the stylohyoid ligament, and that symptoms may be triggered or worsened by head and neck movement, swallowing, or prolonged neck extension. Patients should be counseled to seek medical evaluation if they experience persistent throat pain, facial pain, dysphagia, foreign body sensation, or neurologic symptoms such as dizziness or transient visual disturbances, as these may suggest neurovascular involvement. Education regarding potential warning signs of vascular compression (such as transient ischemic symptoms, syncope, or focal neurologic deficits) is critical, as these warrant urgent medical assessment.
During conservative treatment, patients should be advised that symptom control may be variable and that avoidance of provocative neck positions may reduce symptom severity. Those undergoing interventional or surgical treatment should be counseled on realistic expectations, potential complications, and the importance of postoperative follow-up. Clear communication and shared decision-making improve adherence, reduce anxiety, and support optimal long-term outcomes.
Pearls and Other Issues
The following are pearls and pitfalls of managing Eagle syndrome:
- Eagle syndrome should be considered in patients with chronic cervicofacial pain, dysphagia, or throat discomfort when routine otolaryngologic and neurologic evaluations are unrevealing.
- Symptoms are often positional, exacerbated by head rotation, neck extension, or swallowing, which may help distinguish Eagle syndrome from more common causes of oropharyngeal pain.
- Imaging is essential for diagnosis, and CT with 3D reconstruction remains the preferred modality to evaluate styloid process length, angulation, and proximity to neurovascular structures. Dynamic or vascular imaging should be considered when symptoms suggest carotid artery involvement. Failure to obtain appropriate imaging is a common diagnostic pitfall and may delay definitive treatment.
- Elongation of the styloid process alone does not establish the diagnosis, as many asymptomatic individuals have elongated styloid processes. Clinical correlation with symptomatology is critical to avoid overdiagnosis and unnecessary intervention.
- Conservative treatment may provide temporary symptom relief, but persistent or progressive symptoms often require surgical intervention.
- Inadequate patient selection or incomplete resection can lead to symptom recurrence.
- Preventive strategies center on early recognition, appropriate imaging, and referral to experienced surgical teams when intervention is indicated.
Enhancing Healthcare Team Outcomes
Optimal management of Eagle syndrome requires coordinated collaboration among an interprofessional healthcare team to ensure accurate diagnosis, appropriate treatment selection, and patient-centered care. Clinicians, including otolaryngologists, neurologists, radiologists, and pain specialists, play a central role in recognizing symptom patterns, ordering appropriate imaging, and determining whether conservative or surgical management is indicated. Accurate interpretation of imaging studies, particularly CT with 3D reconstruction or vascular imaging when indicated, is essential for diagnosis and surgical planning.
Advanced practice clinicians and nurses contribute significantly by conducting thorough symptom assessments, monitoring for neurologic or vascular changes, and educating patients on expected outcomes, procedural risks, and postoperative care. Their role in early recognition of complications such as worsening neurologic deficits, dysphagia, or signs of vascular compromise is critical to patient safety. Pharmacists support the care team by reviewing analgesic regimens, identifying drug interactions, and assisting with perioperative medication management, including pain control strategies and anticoagulation considerations. Radiologic technologists and imaging specialists ensure optimal image acquisition and radiation safety during diagnostic evaluations.
Effective interprofessional communication promotes shared decision-making, aligns expectations, and reduces diagnostic delays. Coordinated care planning is particularly important in patients with atypical presentations or vascular involvement, where timely referral and interdisciplinary discussion can prevent serious complications. Through collaborative practice, the healthcare team enhances diagnostic accuracy, optimizes treatment outcomes, and improves overall patient satisfaction.
Media
(Click Image to Enlarge)
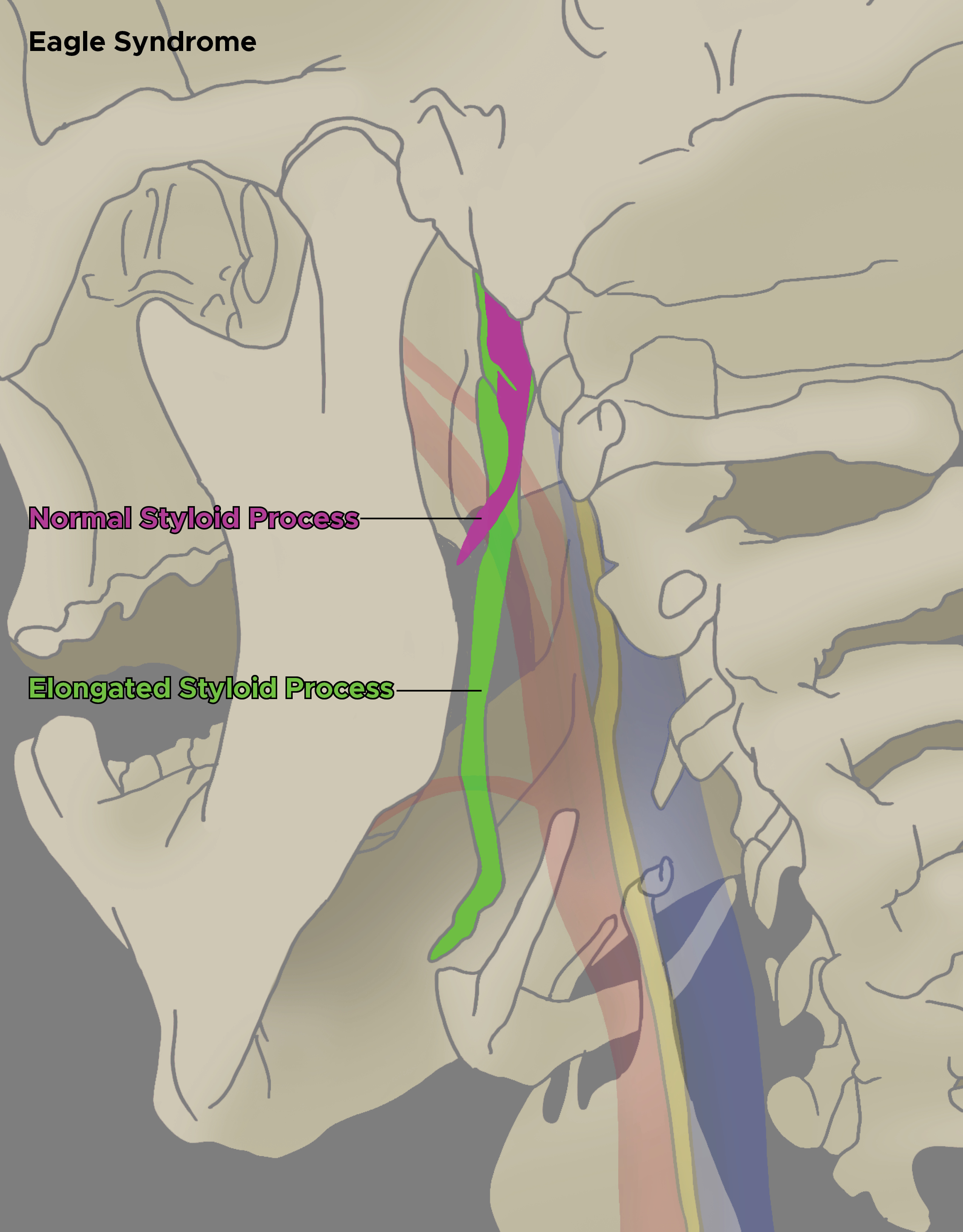
Eagle Syndrome. The illustration shows an elongated styloid process, which can compress adjacent structures, compared to a normal styloid process.
Illustration by C Rowe
References
Zhang FL, Zhou HW, Guo ZN, Yang Y. Eagle Syndrome as a Cause of Cerebral Venous Sinus Thrombosis. The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques. 2019 May:46(3):344-345. doi: 10.1017/cjn.2019.17. Epub 2019 Apr 1 [PubMed PMID: 30932799]
Qureshi S, Farooq MU, Gorelick PB. Ischemic Stroke Secondary to Stylocarotid Variant of Eagle Syndrome. The Neurohospitalist. 2019 Apr:9(2):105-108. doi: 10.1177/1941874418797763. Epub 2018 Sep 4 [PubMed PMID: 30915189]
Gokce C, Sisman Y, Sipahioglu M. Styloid Process Elongation or Eagle's Syndrome: Is There Any Role for Ectopic Calcification? European journal of dentistry. 2008 Jul:2(3):224-8 [PubMed PMID: 19212553]
. . :(): [PubMed PMID: 30896522]
Omami G. Retromandibular Pain Associated With Eagle Syndrome. Headache. 2019 Jun:59(6):915-916. doi: 10.1111/head.13502. Epub 2019 Mar 18 [PubMed PMID: 30883724]
Zammit M, Chircop C, Attard V, D'Anastasi M. Eagle's syndrome: a piercing matter. BMJ case reports. 2018 Nov 28:11(1):. doi: 10.1136/bcr-2018-226611. Epub 2018 Nov 28 [PubMed PMID: 30567108]
Level 3 (low-level) evidencePéus D, Kollias SS, Huber AM, Huber GF. Recurrent unilateral peripheral facial palsy in a patient with an enlarged styloid process. Head & neck. 2019 Mar:41(3):E34-E37. doi: 10.1002/hed.25384. Epub 2018 Dec 24 [PubMed PMID: 30584676]
Montevecchi F, Caranti A, Cammaroto G, Meccariello G, Vicini C. Transoral Robotic Surgery (TORS) for Bilateral Eagle Syndrome. ORL; journal for oto-rhino-laryngology and its related specialties. 2019:81(1):36-40. doi: 10.1159/000493736. Epub 2018 Dec 11 [PubMed PMID: 30537726]
Sullivan T, Rosenblum J. Eagle syndrome: Transient ischemic attack and subsequent carotid dissection. Ear, nose, & throat journal. 2018 Oct-Nov:97(10-11):342-344 [PubMed PMID: 30481841]
Colby CC, Del Gaudio JM. Stylohyoid complex syndrome: a new diagnostic classification. Archives of otolaryngology--head & neck surgery. 2011 Mar:137(3):248-52. doi: 10.1001/archoto.2011.25. Epub [PubMed PMID: 21422308]
Fares S, Soyfoo M, Tant L, Madani A. Clinical Images: Unusual cervical pain in ankylosing spondylitis: Eagle syndrome. Arthritis & rheumatology (Hoboken, N.J.). 2025 Nov 28:():. doi: 10.1002/art.70005. Epub 2025 Nov 28 [PubMed PMID: 41312606]
Caraballo-Meza S, Barakat-Polo N, Plazas-Román J, Díaz-Caballero A, Ardila CM. Predictive Models for Stylohyoid Complex Elongation: A Multivariate Statistical Analysis with Evidence-Based Diagnostic Criteria. Journal of clinical and experimental dentistry. 2025 Oct:17(10):e1172-e1179. doi: 10.4317/jced.63097. Epub 2025 Oct 1 [PubMed PMID: 41255394]
Maamouri R, Ouederni M, Oueslati Y, Mbarek C, Chammakhi C, Cheour M. Acute Painful Horner's Syndrome Revealing Eagle's Syndrome: A Report of Two Cases. Neuro-ophthalmology (Aeolus Press). 2022:46(4):244-247. doi: 10.1080/01658107.2021.2003821. Epub 2021 Nov 19 [PubMed PMID: 35859629]
Level 3 (low-level) evidenceNakajima H, Sato Y, Hakozaki K, Yago T, Tsuda K, Suzuki H. Vascular Eagle Syndrome in Elderly Patients Diagnosed by Dynamic Magnetic Resonance Angiography: A Case Report and Literature Review. NMC case report journal. 2025:12():519-524. doi: 10.2176/jns-nmc.2025-0175. Epub 2025 Nov 21 [PubMed PMID: 41404097]
Level 3 (low-level) evidenceCeylan A, Köybaşioğlu A, Celenk F, Yilmaz O, Uslu S. Surgical treatment of elongated styloid process: experience of 61 cases. Skull base : official journal of North American Skull Base Society ... [et al.]. 2008 Sep:18(5):289-95. doi: 10.1055/s-0028-1086057. Epub [PubMed PMID: 19240828]
Level 3 (low-level) evidenceCaylakli F. Important factor for pain relief in patients with eagle syndrome: Excision technique of styloid process. American journal of otolaryngology. 2019 Mar-Apr:40(2):337. doi: 10.1016/j.amjoto.2018.10.009. Epub 2018 Oct 21 [PubMed PMID: 30477910]
Hettiarachchi PVKS, Jayasinghe RM, Fonseka MC, Jayasinghe RD, Nanayakkara CD. Evaluation of the styloid process in a Sri Lankan population using digital panoramic radiographs. Journal of oral biology and craniofacial research. 2019 Jan-Mar:9(1):73-76. doi: 10.1016/j.jobcr.2018.10.001. Epub 2018 Oct 4 [PubMed PMID: 30302305]
Shereen R, Gardner B, Altafulla J, Simonds E, Iwanaga J, Litvack Z, Loukas M, Shane Tubbs R. Pediatric glossopharyngeal neuralgia: a comprehensive review. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2019 Mar:35(3):395-402. doi: 10.1007/s00381-018-3995-3. Epub 2018 Oct 25 [PubMed PMID: 30361762]
Ferreira MS, Miranda G, Almeida FT, Gasperini G, Silva BSF, Valladares-Neto J, Santiago Junior JF, Silva MAG. Complications in intraoral versus external approach for surgical treatment of Eagle syndrome: A systematic review and meta-analysis. Cranio : the journal of craniomandibular practice. 2024 Sep:42(5):570-582. doi: 10.1080/08869634.2021.2020995. Epub 2022 Jan 10 [PubMed PMID: 35007190]
Level 1 (high-level) evidenceHuang K, Sanjuan-Sanjuan A, Cannavo M, Cass T, Ramirez CA. Does Transcervical Styloidectomy for Eagle Syndrome Improve Quality of Life? Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2022 Dec:80(12):1989-1995. doi: 10.1016/j.joms.2022.08.021. Epub 2022 Sep 3 [PubMed PMID: 36174663]
Level 2 (mid-level) evidenceHassani M, Grønlund EW, Albrechtsen SS, Kondziella D. Neurological phenotypes and treatment outcomes in Eagle syndrome: systematic review and meta-analysis. PeerJ. 2024:12():e17423. doi: 10.7717/peerj.17423. Epub 2024 Jun 26 [PubMed PMID: 38948209]
Level 1 (high-level) evidenceHeld ME, Farsi S, Creighton ERW, Davis KP, King DL, Suen JY. Eagle syndrome presentation and outcomes in a large surgical case series. Laryngoscope investigative otolaryngology. 2024 Aug:9(4):e1289. doi: 10.1002/lio2.1289. Epub 2024 Jul 26 [PubMed PMID: 39071203]
Level 2 (mid-level) evidenceBargiel J, Gontarz M, Gąsiorowski K, Marecik T, Wyszyńska-Pawelec G. Outcomes of Elongated Styloid Process Syndrome Treated with Minimally Invasive Cervical Styloidectomy (MICS)-A Single-Center Retrospective Study. Journal of clinical medicine. 2024 Oct 25:13(21):. doi: 10.3390/jcm13216409. Epub 2024 Oct 25 [PubMed PMID: 39518548]
Level 2 (mid-level) evidenceSharifi A, Kouhi A. Management of eagle syndrome. Current opinion in otolaryngology & head and neck surgery. 2023 Aug 1:31(4):276-280. doi: 10.1097/MOO.0000000000000903. Epub 2023 Jun 8 [PubMed PMID: 37387673]
Level 3 (low-level) evidence