Introduction
The duodenum comprises the initial C-shaped segment of the small intestine, coursing from the pylorus to the jejunum and measuring approximately 25 to 30 cm. Positioned inferior to the stomach, this segment represents the shortest and widest portion of the small intestine. Four parts are recognized: the duodenal bulb, descending, horizontal, and ascending segments, which closely relate to the liver, pancreas, aorta, inferior vena cava (IVC), and superior mesenteric vessels. Except for the 1st segment, the duodenum occupies a retroperitoneal position, anchored against the posterior abdominal wall. The duodenal wall consists of mucosa, submucosa, muscularis, and serosa, enabling digestion, mixing of chyme, and regulated transit while receiving biliary and pancreatic secretions.
Duodenal anatomy carries major medical and surgical significance due to the proximity of this gut segment to crucial vascular and biliary structures. The major duodenal papilla serves as a critical landmark during endoscopic retrograde cholangiopancreatography and biliary interventions (see Image. Anatomy of the Pancreaticobiliary Junction). Congenital and acquired disorders, including duodenal atresia, superior mesenteric artery (SMA) syndrome, and peptic ulcer disease, reflect the importance of regional relationships and vascular supply. Precise understanding of duodenal structure and physiology supports timely diagnosis, procedural safety, and prevention of life-threatening complications.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Structure
The duodenum is the initial C-shaped segment of the small intestine and represents the direct continuation of the pylorus of the stomach. Distally, this segment transitions into the jejunum and ileum, with the proximal portion constituting the shortest and widest region of the small intestine. Located inferior to the stomach, the duodenum measures approximately 25 to 30 cm in length. The designation derives from the Latin term duodenum, meaning “12 fingers,” reflecting the segment's approximate length.
Four anatomically distinct segments are recognized. The duodenal bulb forms the proximal segment and connects to the undersurface of the liver via the hepatoduodenal ligament, which encloses the portal vein, hepatic artery, and common bile duct. The 2nd, or descending, segment lies anterior to the IVC and right kidney, with the head of the pancreas occupying a C-shaped concavity. The 3rd segment courses from right to left anterior to the aorta and IVC, with the superior mesenteric vessels positioned anteriorly. The 4th segment ascends to continue as the jejunum.
The duodenal wall consists of 4 layers, consistent with the remainder of the gastrointestinal tract. These layers include the mucosa, submucosa, muscularis, and serosa, arranged from luminal to external surfaces. The mucosa comprises simple columnar epithelium with microvilli and abundant mucous glands. The submucosa contains connective tissue traversed by blood vessels and nerves. The muscularis layer consists of smooth muscle responsible for mixing and peristaltic propulsion of chyme. The serosa is formed by a squamous epithelium that provides a protective interface with adjacent organs.[1][2]
Function
The primary function of the duodenum is the continuation of the digestive process initiated in the stomach. Chyme enters this segment through the pylorus, a controlled valvular junction between the stomach and duodenum. Digestive activity within the duodenum is mediated by enzymes and intestinal secretions produced by the mucosa, in addition to bile from the gallbladder, bile acids synthesized by the liver, and pancreatic enzymes from the pancreas. These secretions enter the lumen through the major and minor duodenal papillae located in the 2nd portion of the duodenum. The major duodenal papilla is bordered superiorly by a semicircular mucosal fold and is regulated by the sphincter of Oddi, which prevents reflux of duodenal contents into the biliary and pancreatic ducts.[3][4]
The duodenum also regulates the intraluminal environment through hormones produced by the duodenal epithelium. Secretin is released in response to decreased luminal pH and stimulates the secretion of water and bicarbonate to neutralize acidity. This regulation facilitates digestion, as pancreatic amylase and lipase require a narrow pH range for optimal activity. Cholecystokinin is released in the presence of fatty acids and amino acids within the duodenal lumen. This hormone inhibits gastric emptying, stimulates gallbladder contraction, and induces relaxation of the sphincter of Oddi, thereby promoting bile delivery and nutrient digestion and absorption.
Embryology
The duodenum arises in close association with other regions of intestinal organogenesis during embryologic gut development. Craniocaudal and lateral folding of the embryo cause closure of the communication between the primitive gut tube and the yolk sac, resulting in the formation of a pocket at the superior end of the embryo that later differentiates into the foregut. The duodenum arises from the caudalmost portion of the foregut.
Current understanding suggests that the duodenum does not undergo true rotation. The characteristic C-shaped configuration instead develops secondary to leftward growth of the stomach and relative fixation imposed by the enlarging liver and pancreas. As a consequence of these positional changes, the inferior portion of the duodenum becomes located posterior to the SMA.
By the end of development, the duodenal loop lies along the right posterior abdominal wall. The peritoneal layers associated with the duodenum are incorporated into the parietal peritoneum lining the abdominal cavity. This developmental sequence accounts for the classification of the duodenum as a secondarily retroperitoneal structure.
Blood Supply and Lymphatics
The blood supply of the C-shaped duodenum is shared with the head of the pancreas. The proximal segment receives arterial inflow from the gastroduodenal artery and its branches, including the superior pancreaticoduodenal artery. The distal segment is supplied by branches of the SMA, primarily the inferior pancreaticoduodenal artery. Venous outflow parallels the arterial supply and ultimately drains into the portal venous system. Lymphatic drainage follows the pancreaticoduodenal vessels to the pancreaticoduodenal lymph nodes and, subsequently, to the superior mesenteric lymph nodes.
Nerves
Duodenal innervation courses primarily within the submucosal layer. Parasympathetic input emanates from branches of the anterior and posterior vagal trunks. These fibers traverse the celiac plexuses and accompany the celiac trunk toward the duodenum. Synaptic transmission occurs within the enteric plexuses of the duodenal wall, with short postganglionic fibers supplying target tissues. Sympathetic innervation arises from thoracic spinal segments T5 to T9. Preganglionic fibers pass through the sympathetic chain and travel via the greater splanchnic nerve to synapse within the celiac ganglia. Postganglionic sympathetic fibers subsequently follow branches of the celiac trunk to reach the duodenum.
Muscles
The muscularis layer of the duodenum consists of circular and longitudinal smooth muscle fibers. Coordinated contractions of these muscle layers generate peristaltic waves, facilitating the propulsion of chyme throughout the gastrointestinal tract, including the duodenum.
Surgical Considerations
The duodenojejunal flexure is a sharp angulation of the small intestine and is typically identified intraoperatively by the inferior mesenteric vein, which lies immediately to its left. This flexure is anchored to the posterior abdominal wall by the ligament of Treitz. With the exception of the 1st segment, the remainder of the duodenum is retroperitoneal, lacking a mesentery, and remains fixed to the posterior abdominal cavity.
The distal portion of the common bile duct unites with the pancreatic duct to form the biliopancreatic ampulla, which opens at the dome of the major duodenal papilla within the 2nd segment of the C-shaped duodenum. This structure serves as a critical anatomical landmark for gastroenterologists performing endoscopic retrograde cholangiopancreatography, enabling accurate cannulation of the major papilla.
Clinical Significance
Hypertrophic pyloric stenosis results from hyperproliferation of the smooth muscle of the pyloric sphincter. The condition affects 0.5% to 1% of infants and presents with forceful, projectile, nonbilious vomiting shortly after feeding. Gastric emptying into the duodenum is impeded by the enlarged pyloric sphincter, producing characteristic vomiting. Vomitus remains nonbilious because obstruction occurs proximal to the entry of the duodenal papilla. The hypertrophic pyloric sphincter may be palpated as an “olive-shaped mass” or small knot at the right costal margin in the epigastric region. Management is typically surgical, commonly involving myomectomy of the pyloric sphincter.[5]
Duodenal atresia arises from the complete closure of the duodenal lumen. Diagnosis may be suspected prenatally in cases of maternal polyhydramnios or postnatally in neonates presenting with signs of intestinal obstruction. Abdominal radiography often demonstrates the “double-bubble sign,” representing air in the stomach and proximal duodenum separated by the pyloric sphincter. Etiology frequently involves vascular accidents or ischemic events during development. Duodenal atresia exhibits an association with Down syndrome. Surgical correction, most commonly duodenoduodenostomy, constitutes definitive management.[6]
SMA syndrome arises when the 3rd or 4th portion of the duodenum becomes compressed between the SMA and the abdominal aorta.[7][8] Clinical manifestations include nausea, vomiting, abdominal pain, early satiety, and abdominal distention. Compression occurs when the retroperitoneal fat or lymphatic tissue that cushions the duodenum is diminished. Predisposing congenital factors include an asthenic body habitus, high insertion of the duodenum at the ligament of Treitz, or low origin of the SMA. Superimposed acquired or acute factors, such as retroperitoneal tumors, lumbar lordosis, abdominal trauma, rapid linear growth, weight loss, or starvation, can further reduce this protective tissue, permitting duodenal compression by the SMA and aorta.
The duodenum demonstrates clinical significance due to susceptibility to ulceration, most commonly in patients infected with Helicobacter pylori. Ulceration of the posterior portion of the duodenum carries particular risk, as it may cause life-threatening injury to the gastroduodenal artery.[9]
Additional clinical considerations include evaluation for celiac disease, which requires a duodenal biopsy for diagnosis. Traumatic duodenal hematomas may result from seatbelt injuries or direct abdominal blows. Neoplastic conditions, although rare, include duodenal adenocarcinoma, which may be associated with polyposis syndromes such as familial polyposis coli.
Media
(Click Image to Enlarge)
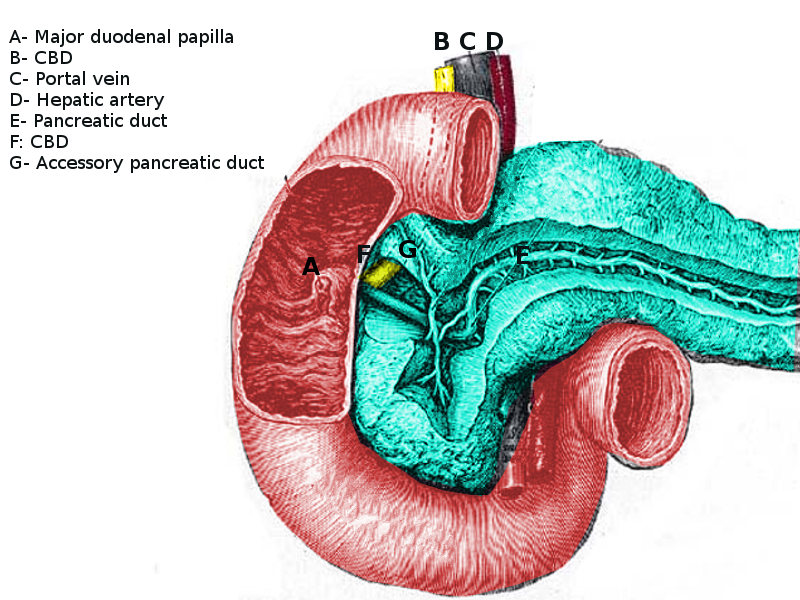
Anatomy of the Pancreaticobiliary Junction. The image illustrates the anatomical relationship between the duodenum, pancreas, and biliary structures, including the major duodenal papilla, common bile duct (CBD), portal vein, hepatic artery, pancreatic duct, and accessory pancreatic duct.
Contributed by S Bhimji, MD
References
Shaikh H, Wehrle CJ, Khorasani-Zadeh A. Anatomy, Abdomen and Pelvis: Superior Mesenteric Artery. StatPearls. 2025 Jan:(): [PubMed PMID: 30137844]
Garza FA, Leslie SW. Anatomy, Abdomen and Pelvis: Kidneys. StatPearls. 2025 Jan:(): [PubMed PMID: 29494007]
Hundt M, Wu CY, Young M. Anatomy, Abdomen and Pelvis: Biliary Ducts. StatPearls. 2025 Jan:(): [PubMed PMID: 29083810]
Collins JT, Nguyen A, Omole AE, Badireddy M. Anatomy, Abdomen and Pelvis, Small Intestine. StatPearls. 2025 Jan:(): [PubMed PMID: 29083773]
El-Gohary Y, Abdelhafeez A, Paton E, Gosain A, Murphy AJ. Pyloric stenosis: an enigma more than a century after the first successful treatment. Pediatric surgery international. 2018 Jan:34(1):21-27. doi: 10.1007/s00383-017-4196-y. Epub 2017 Oct 13 [PubMed PMID: 29030700]
Miscia ME, Lauriti G, Lelli Chiesa P, Zani A. Duodenal atresia and associated intestinal atresia: a cohort study and review of the literature. Pediatric surgery international. 2019 Jan:35(1):151-157. doi: 10.1007/s00383-018-4387-1. Epub 2018 Nov 1 [PubMed PMID: 30386906]
Oka A, Awoniyi M, Hasegawa N, Yoshida Y, Tobita H, Ishimura N, Ishihara S. Superior mesenteric artery syndrome: Diagnosis and management. World journal of clinical cases. 2023 May 26:11(15):3369-3384. doi: 10.12998/wjcc.v11.i15.3369. Epub [PubMed PMID: 37383896]
Level 3 (low-level) evidenceVan Horne N, Jackson JP. Superior Mesenteric Artery Syndrome. StatPearls. 2025 Jan:(): [PubMed PMID: 29489172]
Shishido Y, Mitsuoka E, Tanigawa Y, Ooki H, Shio S, Monzawa S, Ishii M, Fujimoto K. Duodenal ulcer bleeding from a branch of the middle colic artery: A case report. Medicine. 2023 Nov 3:102(44):e35955. doi: 10.1097/MD.0000000000035955. Epub [PubMed PMID: 37933022]
Level 3 (low-level) evidence