Introduction
Clinical trials are prospectively planned studies in humans that test medical interventions, such as drugs, vaccines, biologics, and medical devices, to evaluate safety, dose-response relationships, the efficacy of the intervention, and whether it produces clinical benefit. The drug trial is a type of clinical trial specifically designed to evaluate the safety and effectiveness of a new pharmaceutical or medicinal intervention in human subjects. The goal is to discover new or improved treatments for prevention and therapy, and to reassess existing medicines as new questions arise.[1][2] Randomized controlled trials are studies where subjects are randomly assigned to receive a new drug or treatment (experimental group), standard treatment (comparison group), or no treatment at all (placebo group).[3]
RCTs are considered the “gold standard” as they offer the best answer on the efficacy of a treatment or intervention. Robust trials also incorporate independent safety monitoring and adherence to good clinical practice guidelines.[4] Blinding, randomization, adequate power, and a clinically relevant population of patients are considered the hallmarks of high-quality drug trials.[5][6][7] This allows researchers to assess the benefit-risk balance logically. Adaptive trials are a prospectively planned approach. An integrated phase 2/3 study is one example that combines elements of phase 2 and phase 3, using interim analysis to make predefined, valid modifications. Instead of waiting for a phase 2 trial to conclude before making decisions on the next steps, a seamless phase 2/3 trial can facilitate mid-study choices, saving time, money, and resources.[8] Trial methodology can vary depending on the design and the endpoints.[9][10]
Biologic clinical trials have focused on the risk of immunogenicity, as therapeutic proteins can induce anti-drug antibodies that impact efficacy and safety.[11] Both biologics and small-molecule drugs begin under an investigational new drug application. Most biologic trial application is submitted as a biologics license application (BLA) to the Center for Biologics Evaluation and Research (CBER). Traditional drug trials conclude with a new drug application to the Center for Drug Evaluation and Research (CDER). Notably, that not all biologics fall under CBER; CDER reviews many monoclonal antibodies, cytokines, and growth factors, while vaccines, blood products, and certain cell and gene therapies remain with CBER.[12] See the illustrative diagrams which provide a rapid overview of the clinical trial phases for both conventional drugs and biologics, Images. Drug Development Overview and Clinical Development and Regulatory Overview of Biologics.
Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Function
Drug development refers to the process of introducing a new pharmaceutical agent to the market following the discovery, synthesis, or modification of a compound. This includes preclinical research as well as drug trials involving human subjects. Preclinical investigations are nonhuman studies that involve testing the drug in microorganisms and animal subjects to generate data on its toxicity, pharmacokinetics, and pharmacodynamics. If further studies will take place in human subjects in the United States (US), this data requires submission to the US Food and Drug Administration (FDA) for approval of an investigational new drug (IND) application. Other countries typically have a similar approval process. Once the IND application gets approved, the investigational drug undergoes various phases of human drug trials. If the drug tests as safe and efficacious during phases I to III of the drug trials, the drug sponsor can submit a new drug application (NDA) to the FDA. The national drug regulatory authority then reviews the application to determine whether the drug can receive final marketing approval.[13]
Drug trials in human subjects are generally subdivided into multiple phases, with each phase comprised of at least 1 distinct clinical trial. The drug is usually approved for use in the general population by the national regulatory authority if it successfully passes through drug trial phases I, II, and III. The entire drug development process usually takes several years to proceed through all the phases.Phase 0 trials are optional, and microdosing trials are also available. These involve the administration of low, non-therapeutic doses of the study drug to a small number of participants (typically 10 to 15), helping to gather preliminary data on the pharmacokinetics and pharmacodynamics of the drug in human subjects.[14][15]
Phase I drug trials assess the safety of the investigational drug. These trials help determine a safe dose range and identify any adverse effects associated with the new drug. Drug testing occurs over a few weeks or a month in a small group of healthy volunteers (usually 20 to 80).[16] A single ascending dose (SAD) study and a multiple ascending dose (MAD) study are components of Phase I clinical trials, identifying the maximum tolerated dose (MTD).[17] Oncology drugs are an exception, as Phase I studies are conducted in patients with cancer rather than healthy volunteers.[18][19]
In phase II clinical trials, the experimental drug is tested within a larger group of participants (typically 100 to 300) to determine its efficacy and further evaluate its safety. Phase II trials usually last for several months and involve participants with the target disease or condition.[20][21] Phase 2 clinical trials are often separated into phase IIa (proof of concept) and phase IIb (dose ranging) studies, though sometimes these objectives are combined.[22][23]
Once preliminary evidence from phase II trials establishes the efficacy of the drug, phase III trials are conducted to obtain final confirmation of its safety and effectiveness. This phase involves a comprehensive examination of the risk-benefit profile of the drug, typically comparing it to commonly used treatments in a broader population (usually 1000 to 3000 subjects) over a more extended period (often 6 months).[24][25] Phase III trials are also called pivotal trials. The phase III trial is considered a pivotal/therapeutic confirmatory trial because it provides the evidence needed for regulatory approval. For regulatory approval, an NDA is submitted primarily based on phase III clinical trial data, along with all data from preclinical studies, phase I trials, and phase II trials.
Phase IV drug trials take place following the approval of the drug to be sold in the market and provide additional evidence regarding the risks, benefits, and optimal use of the drug. Of the phase IV studies, those noninterventional studies that are mandated by the regulatory authority to verify the tolerability, safety, and effectiveness of a marketed drug in the real-world setting are termed postmarketing surveillance (PMS) studies. Postmarketing safety surveillance helps detect any long-term or rare adverse effects over a longer period of time and in a much larger patient population than is possible in any of the other phases of drug trials. In addition to safety monitoring, PMS studies also facilitate the planned collection of clinical data related to the use of a drug in a diverse range of patients, thereby yielding data that researchers may not have gathered during phase III studies.[26][27] Phase IV also includes pharmacovigilance activities, such as reporting adverse events in MedWatch forms and submitting the aggregate risk-benefit analysis of the approved drug.[28][29]
Safety reports provide a comprehensive risk-benefit analysis of the drug. The overall assessment of risks and benefits associated with an approved drug (aggregate report) is submitted as a Periodic Adverse Drug Experience Report (PADER) or PBRER (Periodic Risk Benefit Evaluation) to the United States FDA.[30] During the clinical trial phases, the development safety update report (DSUR) is a safety report submitted at various stages of the trials.[30] Investigator-initiated or academic clinical trials are clinical studies initiated and conducted by a non-pharmaceutical company researcher, who could be an individual investigator, a collaborative study group, or an institution. The key premise in this type of clinical trial is that the responsibility of being the sponsor as well as the investigator may lie with the person who designs and conducts the study.
However, sponsors sometimes fund these trials, especially if they think it may lend support for a new indication. Investigator-initiated trials help generate data on the safety and effectiveness of a drug in the real-world setting. They are largely driven by questions that remain unanswered from phases I to III of drug trials.[31][32] The International Council for Harmonisation (ICH) offers globally accepted guidelines that the FDA adopts to standardize clinical trial design, conduct, safety, and reporting, ensuring higher quality and more efficient drug development. As per the FDA, the ICH document makes suggestions on information that should be incorporated in a core clinical study report of an individual study of any therapeutic, diagnostic, or prophylactic agent conducted in human subjects. https://www.fda.gov/science-research/clinical-trials-and-human-subject-protection/ich-guidance-documents
Issues of Concern
Participation in a drug trial carries an increased level of risk as compared to ordinary medical care, mainly due to the potential of being exposed to the unexpected effects of a new drug. Drug trials also encompass several ethical dilemmas. These dilemmas generally stem from the fact that those who bear the burden and risk of participation in the trials are not the same as those who stand to gain from them.
Current research ethics place significant weight on the informed consent process. However, the notion of informed consent is sometimes questionable due to the difficulty in determining the adequate level of information that should be provided to the participant for the consent to be valid, especially in a new compound that has not been tested before and which may be associated with unknown risks. Either too little information is given, or in some cases, too much information is provided in a language that is too technical for the participant to comprehend.[33][34]
Placebos are commonly used in drug trials. An issue of concern associated with using a placebo is the possibility of harming the participating subjects, who, instead of receiving active treatment, are receiving a placebo. If the participant is not receiving active treatment, this may expose the subjects to an aggravation of their conditions, increased levels of pain, or even the risk of death. Therefore, the use of placebos is acceptable only if it does not subject the participant to any risk of serious or irreversible harm.[35][36] The nocebo effect is the opposite, where patients may experience adverse effects or negative symptoms from the same inert treatment due to negative expectations. They must be understood by researchers and clinicians to accurately interpret clinical trial results, as they can significantly influence patient outcomes and adherence.[37][38]
Randomization is a crucial component used to minimize bias in clinical trials. However, randomization between the two arms of a drug trial may raise serious ethical concerns. By participating in a randomized controlled trial, the participants may receive a treatment that eventually turns out to be inferior. This is particularly problematic if the experimental drug is found to be worse than the standard treatment available outside of the trial or if the participant is assigned to a placebo. Participants may thus be denied the best-proven standard of care available.[39]
Publication bias occurs when only clinically or statistically significant results of drug trials are published. Unfavorable results are often not publicized or published, thus generating a false impression of the effectiveness of a medication. For instance, a pharmaceutical company sponsoring a drug trial typically has the right to review the research results before publication and may withhold the publication of unfavorable results. Thus, the research findings remain unavailable to the scientific community, making it difficult for healthcare providers to determine if a particular drug is suitable for their patients.[40][41]
Sponsorship bias, also known as funding bias, is another concern that may arise during drug trials. Funding for a trial is often provided by a pharmaceutical company that has manufactured or sponsored the drug. This produces a conflict of interest, as the company is inherently biased towards favorable research outcomes and would help enhance the sale of its product.[42][43][44]
Clinical Significance
Preclinical investigations answer basic questions regarding a drug's safety; however, they are not a substitute for studies that evaluate the effects of a drug on the human body.[45][46] Well-conducted randomized controlled trials are widely accepted as the principal source of evidence on the safety and effectiveness of medical interventions. The ultimate goal of the drug development process is to introduce a new or significantly improved compound with a proven therapeutic effect to the market. Hence, the transition from preclinical research to clinical phases marks a critical juncture, as many potential medications do not progress beyond this point. Trials of first-in-class drugs are also helpful in providing the most rigorous testing of causal mechanisms in human disease.[5] Postmarketing surveillance helps monitor a drug once it reaches the market and is used by individuals under various circumstances and in real-life situations, rather than in carefully controlled laboratory conditions typical of pre-approval drug trials. This ongoing work helps detect previously unrecognized positive or negative effects of the drug.[47]
Cluster randomized controlled trials in healthcare are increasingly common but require careful statistical consideration of intra-cluster correlation to avoid falsely significant results due to dependencies between patients within the same healthcare facility or provider. Ignoring this dependence leads to increased type I errors, where interventions appear effective when they're not, potentially resulting in adoption of ineffective treatments or quality improvement strategies. Proper sample size calculation must account for design effects and intracluster correlation values to ensure valid conclusions about healthcare interventions at the facility or provider level.[48]
Adaptive trials are approaches that allow planned changes during a study based on ongoing results, such as adjusting sample size, treatment groups, or patient allocation, without compromising trial integrity. They help detect safety issues, effectiveness, or futility earlier, reducing participant burden and speeding up the process. Examples include adaptive dose-finding, response-adaptive randomization, group sequential, seamless, and adaptive enrichment designs. Regulatory agencies, including the FDA, support these designs for their efficiency, ethical benefits, and ability to produce reliable evidence.[49]
A pragmatic trial is a type of clinical study conducted in real-world healthcare settings to assess the effectiveness of an intervention in clinical practice. Unlike tightly controlled trials, these studies include a broad and diverse patient population and use typical clinical care conditions, making the results more applicable to everyday medical practice. They are beneficial for assessing complex interventions or outcomes in patients with multiple coexisting conditions, providing evidence that is directly relevant to clinicians.[50][51][52] In clinical trials, surrogate markers are measurements used as a substitute for actual clinical outcomes. For example, lowering low-density lipoprotein cholesterol is often used to gauge cardiovascular risk, but it doesn't always guarantee a decrease in atherosclerotic cardiovascular disease or major adverse cardiovascular events.[53]
Other Issues
Artificial intelligence (AI) and machine learning can transform clinical trials by enhancing participant recruitment, adherence, data analysis, and overall efficiency, enabling faster, cost-effective, and more inclusive drug development. Considerable challenges remain, including issues with data quality, algorithmic bias, ethical concerns, and limited regulatory supervision. As tools and standards evolve, AI has the potential to revolutionize clinical research.
Advantages of AI in Clinical Trials
AI enhances trial efficiency by improving study design, patient recruitment, and protocol optimization, leading to higher success rates. It enables real-time patient monitoring and advanced data analysis for more accurate result interpretation. The predictive capabilities support precision medicine by decreasing statistical variability. Furthermore, AI provides more in-depth insights into data patterns and comprehensive data analysis.
Limitations of AI in Clinical Trials
Implementation requires substantial investments in technology and specialized expertise in both clinical research and machine learning. Critical ethical concerns arise regarding data privacy and informed consent. In contrast, the lack of practical validation data for AI-based interventions remains a barrier to the use of AI in clinical research. Furthermore, AI algorithms must be rigorously validated against established clinical standards for accuracy, sensitivity, and specificity before they can be reliably applied in clinical settings.[54]
Digital Twins
Digital twins are digital replicas of biological systems, ranging from single cells to entire patients, built using either mechanistic modeling or generative artificial intelligence. These models enable us to simulate real-world experiments and predict how patients might respond to treatments or experience adverse events, providing a glimpse into the future of patient care. For instance, in Alzheimer disease clinical trials, Unlearn.AI created digital twins for each participant and combined them into a virtual placebo cohort. This approach enabled researchers to compare outcomes with treated patients without enrolling large numbers of patients into a traditional control arm. Regulatory frameworks are beginning to recognize the potential of these models.
The FDA Modernization Act 2.0 provides guidance on computational methods as alternatives to animal testing, and the European Medicines Agency has provided guidance on qualifying digital twin predictions for statistical analyses. However, clear regulations for their use in clinical trials are still limited. While digital twins offer the promise of faster trials, lower costs, and better patient safety, we still face practical challenges, such as the need for large, high-quality datasets, improved transparency of the models, and consistent validation standards to ensure that clinicians can rely on their predictions.[55][56]
Blinding and Unblinding
There are 3 types of blinding in a clinical trial, and blinding helps to decrease bias. Single-blind means only the participant is unaware of treatment, double-blind extends to both participant and investigator, and triple-blind also includes outcome assessors and analysts, though definitions vary. Blinding is essential to maintain the scientific validity of results, following predefined procedures that maintain trial integrity. In certain situations, unblinding may be done only in emergencies/safety concerns.[57]
Enhancing Healthcare Team Outcomes
Drug trials provide the best evidence of the efficacy and safety of a drug in human subjects. However, this is only true if the trial activity is transparent, discoverable, and high quality. All stakeholders must understand the various ethical and moral issues commonly encountered in clinical trials and fulfill their responsibilities in conducting high-quality research to produce the best and most accurate information possible, informing clinical decisions and practice. All parties need to fully understand the results of drug trials so that findings are applicable in clinical practice in an appropriate, relevant, and ethical manner.[58][59] Good clinical practice should be followed throughout the conduct of the clinical trial; this is an international ethical and scientific quality standard for the design, conduct, implementation, monitoring, audit, analysis, and reporting of clinical trials, mainly serving to safeguard the rights, integrity, and confidentiality of trial subjects.[60]
All interprofessional healthcare team members bear a responsibility to remain current on clinical trials, so they can use the latest data-driven models to direct patient care and question practices that are not supported by the latest research. This responsibility will, of necessity, be specialty-driven, so the focus on trials will be on studies that pertain to the discipline of the provider; clinicians will exhibit a great interest and need for knowledge on trials that deal with their specialty area. Likewise, pharmacists will be more inclined to look into drug trials that line up with their specialties if they have them.
Nurses (again, especially within specialty certifications) and advanced clinicians should be aware of the latest pertinent research and be willing to share this knowledge with other healthcare team members where needed and/or appropriate. Only through open collaboration and communication can all members of the interprofessional team optimize patient outcomes. The implementation of good clinical practice guidelines is essential for the ethical conduct of clinical trials. An interprofessional team approach and clear communication among principal investigator, clinicians, pharmacists, nurses, clinical research associates, and biostatisticians are essential in randomized controlled trials to protect patient safety, rigorously assess efficacy, and minimize adverse effects. The FDA emphasizes the importance of multidisciplinary collaboration to ensure that trial results are reliable, ethically sound, and applicable to patient care.
An interprofessional team approach and clear communication among the principal investigator, pharmacists, clinical research associates/assistants, regulatory affairs experts, nurses, biostatisticians, and scientific experts are essential to ensure the smooth conduct of a randomized controlled trial. The responsibility for trial transparency, safety, and regulatory compliance includes the marketing authorization holder (MAH/sponsor), contract research organizations (CROs), the FDA, and institutional review boards (IRBs). MAHs and CROs oversee protocol adherence, data monitoring, and adverse event reporting (eg, via MedWatch or PADER/DSUR submissions). IRBs ensure ethical review and independent oversight, while the FDA evaluates the overall benefit-risk balance before approving a drug and provides ongoing monitoring and oversight. This is especially important in a multiregional clinical trial, where communication between the regional regulatory agency and the sponsor is important.[61][62][63]
Media
(Click Image to Enlarge)
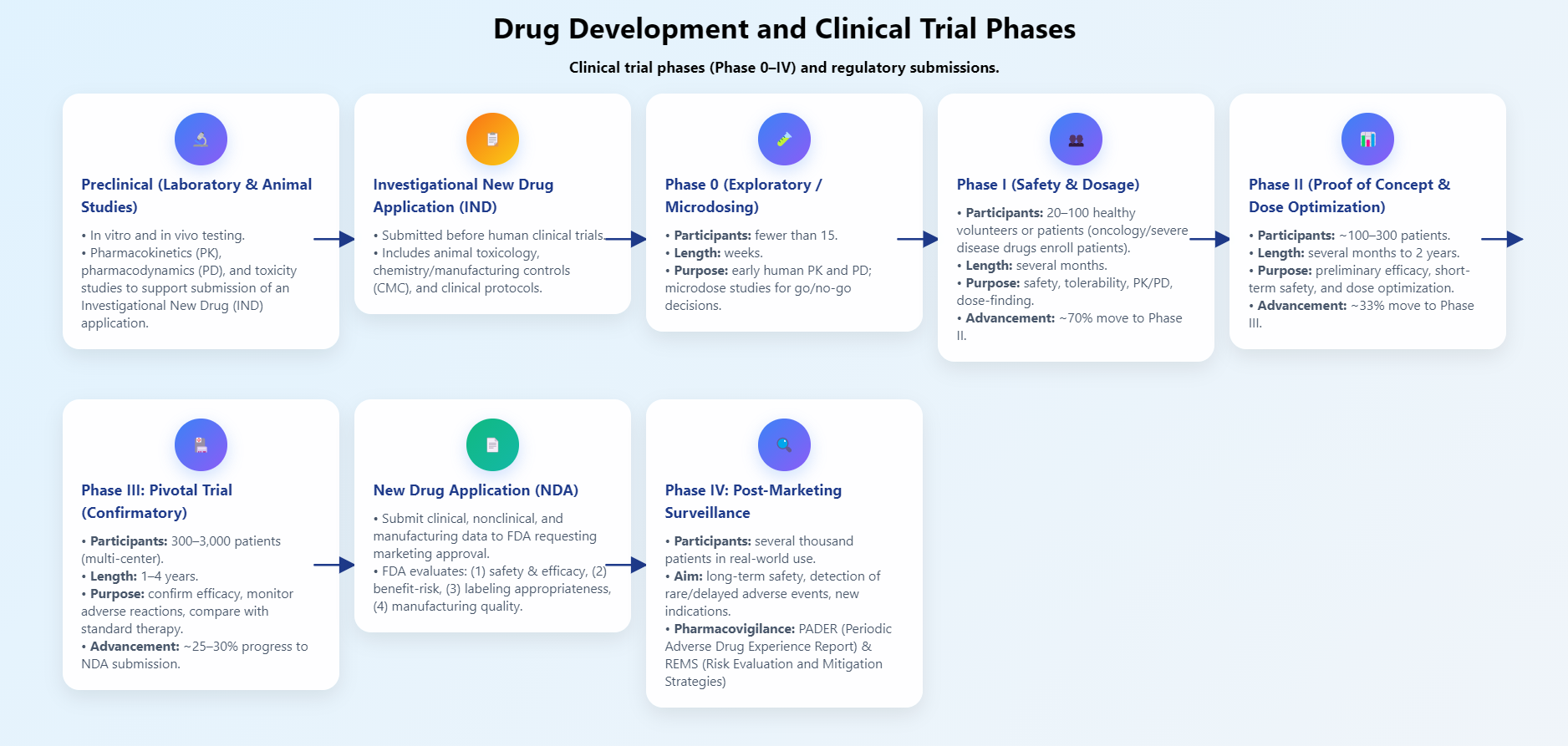
Drug Development Overview. This image shows a concise overview of drug development, phases of clinical trials, and regulatory submissions.
Contributed by P Patel, PharmD
(Click Image to Enlarge)

Clinical Development and Regulatory Overview of Biologics. This image shows a concise overview of biologics' clinical development and regulatory approval through the clinical trial process.
Contributed by P Patel, PharmD
References
Kandi V, Vadakedath S. Clinical Trials and Clinical Research: A Comprehensive Review. Cureus. 2023 Feb:15(2):e35077. doi: 10.7759/cureus.35077. Epub 2023 Feb 16 [PubMed PMID: 36938261]
Su G, Shen D, Deng D, Bai Q, Xie H. Characterization of medical device randomized controlled trials with adaptive designs. Journal of comparative effectiveness research. 2025 Jan:14(1):e240011. doi: 10.57264/cer-2024-0011. Epub 2024 Dec 9 [PubMed PMID: 39656083]
Level 1 (high-level) evidenceBraga LH, Farrokhyar F, Dönmez Mİ, Nelson CP, Haid B, Herbst K, Garriboli M, Cascio S, Nieuwhof-Leppink A, Kaefer M, Bägli DJ, Kalfa N, Ching C, Fossum M, Harper L. Randomized controlled trials - The what, when, how and why. Journal of pediatric urology. 2025 Apr:21(2):397-404. doi: 10.1016/j.jpurol.2024.11.021. Epub 2024 Dec 3 [PubMed PMID: 39701869]
Level 1 (high-level) evidenceDavis S. Embedding good clinical practice into investigator-initiated studies or trials. Perspectives in clinical research. 2020 Jan-Mar:11(1):1-2. doi: 10.4103/picr.PICR_2_20. Epub 2020 Jan 31 [PubMed PMID: 32154141]
Level 3 (low-level) evidenceZwierzyna M, Davies M, Hingorani AD, Hunter J. Clinical trial design and dissemination: comprehensive analysis of clinicaltrials.gov and PubMed data since 2005. BMJ (Clinical research ed.). 2018 Jun 6:361():k2130. doi: 10.1136/bmj.k2130. Epub 2018 Jun 6 [PubMed PMID: 29875212]
Hariton E, Locascio JJ. Randomised controlled trials - the gold standard for effectiveness research: Study design: randomised controlled trials. BJOG : an international journal of obstetrics and gynaecology. 2018 Dec:125(13):1716. doi: 10.1111/1471-0528.15199. Epub 2018 Jun 19 [PubMed PMID: 29916205]
Level 1 (high-level) evidenceMentz RJ, Hernandez AF, Berdan LG, Rorick T, O'Brien EC, Ibarra JC, Curtis LH, Peterson ED. Good Clinical Practice Guidance and Pragmatic Clinical Trials: Balancing the Best of Both Worlds. Circulation. 2016 Mar 1:133(9):872-80. doi: 10.1161/CIRCULATIONAHA.115.019902. Epub [PubMed PMID: 26927005]
Level 2 (mid-level) evidenceYang JY, Li GC, Yuan Y. Accelerate vaccine development using seamless phase 2/3 trial designs. Expert review of vaccines. 2024 Jan-Dec:23(1):523-534. doi: 10.1080/14760584.2024.2348612. Epub 2024 May 7 [PubMed PMID: 38682812]
Youn A, Yang Y. Improving phase 2/3 trials with an enhanced 2-in-1 adaptive design. Contemporary clinical trials communications. 2025 Oct:47():101524. doi: 10.1016/j.conctc.2025.101524. Epub 2025 Jul 14 [PubMed PMID: 40822703]
Level 1 (high-level) evidenceKiani AK, Naureen Z, Pheby D, Henehan G, Brown R, Sieving P, Sykora P, Marks R, Falsini B, Capodicasa N, Miertus S, Lorusso L, Dondossola D, Tartaglia GM, Ergoren MC, Dundar M, Michelini S, Malacarne D, Bonetti G, Donato K, Medori MC, Beccari T, Samaja M, Connelly ST, Martin D, Morresi A, Bacu A, Herbst KL, Kapustin M, Stuppia L, Lumer L, Farronato G, Bertelli M, INTERNATIONAL BIOETHICS STUDY GROUP. Methodology for clinical research. Journal of preventive medicine and hygiene. 2022 Jun:63(2 Suppl 3):E267-E278. doi: 10.15167/2421-4248/jpmh2022.63.2S3.2769. Epub 2022 Oct 17 [PubMed PMID: 36479476]
Bots SJ, Parker CE, Brandse JF, Löwenberg M, Feagan BG, Sandborn WJ, Jairath V, D'Haens G, Vande Casteele N. Anti-Drug Antibody Formation Against Biologic Agents in Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. BioDrugs : clinical immunotherapeutics, biopharmaceuticals and gene therapy. 2021 Nov:35(6):715-733. doi: 10.1007/s40259-021-00507-5. Epub 2021 Nov 19 [PubMed PMID: 34797516]
Level 1 (high-level) evidenceInnes GK, Smith KA, Kuzucan A, Li J, Rivera D, Panagiotou OA, Concato J. Real-World Evidence in New Drug and Biologics License Application Approvals During Fiscal Years 2020-2022. Clinical pharmacology and therapeutics. 2025 Jul:118(1):85-89. doi: 10.1002/cpt.3688. Epub 2025 Apr 25 [PubMed PMID: 40276902]
Umscheid CA, Margolis DJ, Grossman CE. Key concepts of clinical trials: a narrative review. Postgraduate medicine. 2011 Sep:123(5):194-204. doi: 10.3810/pgm.2011.09.2475. Epub [PubMed PMID: 21904102]
Level 3 (low-level) evidenceHill TP. Phase 0 clinical trials: towards a more complete ethics critique. Ecancermedicalscience. 2012:6():248. doi: 10.3332/ecancer.2012.248. Epub 2012 Mar 27 [PubMed PMID: 22518199]
Level 1 (high-level) evidenceWieschowski S, Chin WWL, Federico C, Sievers S, Kimmelman J, Strech D. Preclinical efficacy studies in investigator brochures: Do they enable risk-benefit assessment? PLoS biology. 2018 Apr:16(4):e2004879. doi: 10.1371/journal.pbio.2004879. Epub 2018 Apr 5 [PubMed PMID: 29621228]
Ivy SP, Siu LL, Garrett-Mayer E, Rubinstein L. Approaches to phase 1 clinical trial design focused on safety, efficiency, and selected patient populations: a report from the clinical trial design task force of the national cancer institute investigational drug steering committee. Clinical cancer research : an official journal of the American Association for Cancer Research. 2010 Mar 15:16(6):1726-36. doi: 10.1158/1078-0432.CCR-09-1961. Epub 2010 Mar 9 [PubMed PMID: 20215542]
Level 1 (high-level) evidenceMeier A, Papapetropoulos S, Marsh A, Neelon K, Stiles D, O'Mara R, Thackaberry EA, Colonna M, Rajagovindan R. Phase 1, First-In-Human, Single-/Multiple-Ascending Dose Study of Iluzanebart in Healthy Volunteers. Annals of clinical and translational neurology. 2025 May:12(5):1065-1076. doi: 10.1002/acn3.70033. Epub 2025 Apr 1 [PubMed PMID: 40166927]
Corr BR, Moroney M, Sheeder J, Eckhardt SG, Sawyer B, Behbakht K, Diamond JR. Survival and clinical outcomes of patients with ovarian cancer who were treated on phase 1 clinical trials. Cancer. 2020 Oct 1:126(19):4289-4293. doi: 10.1002/cncr.33073. Epub 2020 Jul 22 [PubMed PMID: 32697381]
Level 1 (high-level) evidenceGainor JF, Patel MR, Weber JS, Gutierrez M, Bauman JE, Clarke JM, Julian R, Scott AJ, Geiger JL, Kirtane K, Robert-Tissot C, Coder B, Tasneem M, Sun J, Zheng W, Gerbereux L, Laino A, Porichis F, Pollard JR, Hou P, Sehgal V, Chen X, Morrissey M, Daghestani HN, Feldman I, Srinivasan L, Frederick JP, Brown M, Aanur P, Meehan R, Burris HA 3rd. T-cell Responses to Individualized Neoantigen Therapy mRNA-4157 (V940) Alone or in Combination with Pembrolizumab in the Phase 1 KEYNOTE-603 Study. Cancer discovery. 2024 Nov 1:14(11):2209-2223. doi: 10.1158/2159-8290.CD-24-0158. Epub [PubMed PMID: 39115419]
Hunsberger S, Zhao Y, Simon R. A comparison of phase II study strategies. Clinical cancer research : an official journal of the American Association for Cancer Research. 2009 Oct 1:15(19):5950-5. doi: 10.1158/1078-0432.CCR-08-3205. Epub 2009 Sep 29 [PubMed PMID: 19789306]
Torres-Saavedra PA, Winter KA. An Overview of Phase 2 Clinical Trial Designs. International journal of radiation oncology, biology, physics. 2022 Jan 1:112(1):22-29. doi: 10.1016/j.ijrobp.2021.07.1700. Epub 2021 Aug 4 [PubMed PMID: 34363901]
Level 1 (high-level) evidenceLi QH, Deng Q, Ting N. Proof of Concept: Drug Selection? Or Dose Selection? Thoughts on Multiplicity Issues. Therapeutic innovation & regulatory science. 2021 Sep:55(5):1001-1005. doi: 10.1007/s43441-021-00299-4. Epub 2021 May 24 [PubMed PMID: 34028669]
Level 2 (mid-level) evidenceYuan J, Pang H, Tong T, Xi D, Guo W, Mesenbrink P. Seamless Phase IIa/IIb and enhanced dose-finding adaptive design. Journal of biopharmaceutical statistics. 2016:26(5):912-23. doi: 10.1080/10543406.2015.1094807. Epub 2015 Sep 21 [PubMed PMID: 26390951]
Saw SM, Lim SG. Clinical drug trials: practical problems of phase III. Annals of the Academy of Medicine, Singapore. 2000 Sep:29(5):598-605 [PubMed PMID: 11126694]
Bhide A, Shah PS, Acharya G. A simplified guide to randomized controlled trials. Acta obstetricia et gynecologica Scandinavica. 2018 Apr:97(4):380-387. doi: 10.1111/aogs.13309. Epub 2018 Feb 27 [PubMed PMID: 29377058]
Level 1 (high-level) evidenceSuvarna V. Phase IV of Drug Development. Perspectives in clinical research. 2010 Apr:1(2):57-60 [PubMed PMID: 21829783]
Level 3 (low-level) evidenceTrailokya A, Srivastava A, Mukaddam Q, Chaudhry S, Patel K, Suryawanshi S, Naik M. Phase IV Studies: What Clinicians Need to Know! The Journal of the Association of Physicians of India. 2024 Jan:72(1):85-87. doi: 10.59556/japi.71.0444. Epub [PubMed PMID: 38736079]
Zhang X, Zhang Y, Ye X, Guo X, Zhang T, He J. Overview of phase IV clinical trials for postmarket drug safety surveillance: a status report from the ClinicalTrials.gov registry. BMJ open. 2016 Nov 23:6(11):e010643. doi: 10.1136/bmjopen-2015-010643. Epub 2016 Nov 23 [PubMed PMID: 27881517]
Level 1 (high-level) evidenceSilva L, Pacheco T, Araújo E, Duarte RJ, Ribeiro-Vaz I, Ferreira-da-Silva R. Unveiling the future: precision pharmacovigilance in the era of personalized medicine. International journal of clinical pharmacy. 2024 Jun:46(3):755-760. doi: 10.1007/s11096-024-01709-x. Epub 2024 Feb 28 [PubMed PMID: 38416349]
Kulkarni TN, Kulkarni NG. Authoring a periodic adverse drug experience report…here's what you need to know! Perspectives in clinical research. 2019 Apr-Jun:10(2):95-99. doi: 10.4103/picr.PICR_126_18. Epub [PubMed PMID: 31008077]
Level 3 (low-level) evidenceKonwar M, Bose D, Gogtay NJ, Thatte UM. Investigator-initiated studies: Challenges and solutions. Perspectives in clinical research. 2018 Oct-Dec:9(4):179-183. doi: 10.4103/picr.PICR_106_18. Epub [PubMed PMID: 30319949]
Level 3 (low-level) evidenceSuvarna V. Investigator initiated trials (IITs). Perspectives in clinical research. 2012 Oct:3(4):119-21. doi: 10.4103/2229-3485.103591. Epub [PubMed PMID: 23293757]
Level 3 (low-level) evidenceNardini C. The ethics of clinical trials. Ecancermedicalscience. 2014:8():387. doi: 10.3332/ecancer.2014.387. Epub 2014 Jan 16 [PubMed PMID: 24482672]
Goldstein CE, Weijer C, Brehaut JC, Fergusson DA, Grimshaw JM, Horn AR, Taljaard M. Ethical issues in pragmatic randomized controlled trials: a review of the recent literature identifies gaps in ethical argumentation. BMC medical ethics. 2018 Feb 27:19(1):14. doi: 10.1186/s12910-018-0253-x. Epub 2018 Feb 27 [PubMed PMID: 29482537]
Level 1 (high-level) evidenceMillum J, Grady C. The ethics of placebo-controlled trials: methodological justifications. Contemporary clinical trials. 2013 Nov:36(2):510-4. doi: 10.1016/j.cct.2013.09.003. Epub 2013 Sep 12 [PubMed PMID: 24035802]
Gupta U, Verma M. Placebo in clinical trials. Perspectives in clinical research. 2013 Jan:4(1):49-52. doi: 10.4103/2229-3485.106383. Epub [PubMed PMID: 23533982]
Level 3 (low-level) evidenceTavel ME. Nocebo vs Placebo Effects: Their Clinical Relevance. The American journal of medicine. 2022 Nov:135(11):1296-1299. doi: 10.1016/j.amjmed.2022.06.007. Epub 2022 Jul 9 [PubMed PMID: 35820462]
Tu Y, Zhang L, Kong J. Placebo and nocebo effects: from observation to harnessing and clinical application. Translational psychiatry. 2022 Dec 24:12(1):524. doi: 10.1038/s41398-022-02293-2. Epub 2022 Dec 24 [PubMed PMID: 36564374]
Colli A, Pagliaro L, Duca P. The ethical problem of randomization. Internal and emergency medicine. 2014 Oct:9(7):799-804. doi: 10.1007/s11739-014-1118-z. Epub 2014 Sep 7 [PubMed PMID: 25194693]
Dalton JE, Bolen SD, Mascha EJ. Publication Bias: The Elephant in the Review. Anesthesia and analgesia. 2016 Oct:123(4):812-3. doi: 10.1213/ANE.0000000000001596. Epub [PubMed PMID: 27636569]
Mlinarić A, Horvat M, Šupak Smolčić V. Dealing with the positive publication bias: Why you should really publish your negative results. Biochemia medica. 2017 Oct 15:27(3):030201. doi: 10.11613/BM.2017.030201. Epub [PubMed PMID: 29180912]
Lexchin J. Sponsorship bias in clinical research. The International journal of risk & safety in medicine. 2012:24(4):233-42. doi: 10.3233/JRS-2012-0574. Epub [PubMed PMID: 23135338]
Steel D. If the Facts Were Not Untruths, Their Implications Were: Sponsorship Bias and Misleading Communication. Kennedy Institute of Ethics journal. 2018:28(2):119-144. doi: 10.1353/ken.2018.0011. Epub [PubMed PMID: 30100597]
Kakazu VA, Assis M, Bacelar A, Bezerra AG, Ciutti GLR, Conway SG, Galduróz JCF, Drager LF, Khoury MP, Leite IPA, Luciano YM, Poyares D, Tufik S, Pires GN. Industry sponsorship bias in randomized controlled trials of digital cognitive behavioral therapy for insomnia: a meta-research study based on the 2023 Brazilian guidelines on the diagnosis and treatment of insomnia in adults. Frontiers in neurology. 2025:16():1600767. doi: 10.3389/fneur.2025.1600767. Epub 2025 Jul 22 [PubMed PMID: 40765616]
Level 1 (high-level) evidenceAkhondzadeh S. The Importance of Clinical Trials in Drug Development. Avicenna journal of medical biotechnology. 2016 Oct-Dec:8(4):151 [PubMed PMID: 27920881]
Mahalmani V, Sinha S, Prakash A, Medhi B. Translational research: Bridging the gap between preclinical and clinical research. Indian journal of pharmacology. 2022 Nov-Dec:54(6):393-396. doi: 10.4103/ijp.ijp_860_22. Epub [PubMed PMID: 36722550]
Vlahović-Palčevski V, Mentzer D. Postmarketing surveillance. Handbook of experimental pharmacology. 2011:205():339-51. doi: 10.1007/978-3-642-20195-0_17. Epub [PubMed PMID: 21882120]
Netuveli G. Cluster randomized controlled trial: A matter of independence. International journal for quality in health care : journal of the International Society for Quality in Health Care. 2022 Apr 12:34(2):. pii: mzac022. doi: 10.1093/intqhc/mzac022. Epub [PubMed PMID: 35349693]
Level 1 (high-level) evidenceBen-Eltriki M, Rafiq A, Paul A, Prabhu D, Afolabi MOS, Baslhaw R, Neilson CJ, Driedger M, Mahmud SM, Lacaze-Masmonteil T, Marlin S, Offringa M, Butcher N, Heath A, Kelly LE. Adaptive designs in clinical trials: a systematic review-part I. BMC medical research methodology. 2024 Oct 4:24(1):229. doi: 10.1186/s12874-024-02272-9. Epub 2024 Oct 4 [PubMed PMID: 39367313]
Level 1 (high-level) evidenceFord I, Norrie J. Pragmatic Trials. The New England journal of medicine. 2016 Aug 4:375(5):454-63. doi: 10.1056/NEJMra1510059. Epub [PubMed PMID: 27518663]
Garrison SR, Bakal JA, Kolber MR, Korownyk CS, Green LA, Kirkwood JEM, McAlister FA, Padwal RS, Lewanczuk R, Hill MD, Singer AG, Katz A, Kelmer MD, Gayayan A, Campbell FN, Vucenovic A, Archibald NR, Yeung JMS, Youngson ERE, McGrail K, O'Neill BG, Greiver M, Manca DP, Kraut RY, Wang T, Manns BJ, Mangin DA, MacLean C, McCormack J, Wong ST, Norris C, Allan GM. Antihypertensive Medication Timing and Cardiovascular Events and Death: The BedMed Randomized Clinical Trial. JAMA. 2025 Jun 17:333(23):2061-2072. doi: 10.1001/jama.2025.4390. Epub [PubMed PMID: 40354045]
Level 1 (high-level) evidenceOmerovic E, Petrie M, Redfors B, Fremes S, Murphy G, Marquis-Gravel G, Lansky A, Velazquez E, Perera D, Reid C, Smith J, van der Meer P, Lipsic E, Juni P, McMurray J, Bauersachs J, Køber L, Rouleau JL, Doenst T. Pragmatic randomized controlled trials: strengthening the concept through a robust international collaborative network: PRIME-9-Pragmatic Research and Innovation through Multinational Experimentation. Trials. 2024 Jan 23:25(1):80. doi: 10.1186/s13063-024-07935-y. Epub 2024 Jan 23 [PubMed PMID: 38263138]
Level 1 (high-level) evidenceHyun MH, Jang JW, Choi BG, Na JO, Choi CU, Kim JW, Kim EJ, Rha SW, Park CG, Lee E, Seo HS. The low-density lipoprotein cholesterol lowering is an ineffective surrogate marker of statin responsiveness to predict cardiovascular outcomes: The 10-year experience of matched population (a STROBE-compliant article). Medicine. 2019 Dec:98(51):e18510. doi: 10.1097/MD.0000000000018510. Epub [PubMed PMID: 31861037]
Chopra H, Annu, Shin DK, Munjal K, Priyanka, Dhama K, Emran TB. Revolutionizing clinical trials: the role of AI in accelerating medical breakthroughs. International journal of surgery (London, England). 2023 Dec 1:109(12):4211-4220. doi: 10.1097/JS9.0000000000000705. Epub 2023 Dec 1 [PubMed PMID: 38259001]
Adashi EY, O'Mahony DP, Cohen IG. The FDA Modernization Act 2.0: Drug Testing in Animals is Rendered Optional. The American journal of medicine. 2023 Sep:136(9):853-854. doi: 10.1016/j.amjmed.2023.03.033. Epub 2023 Apr 18 [PubMed PMID: 37080328]
Level 3 (low-level) evidenceBordukova M, Makarov N, Rodriguez-Esteban R, Schmich F, Menden MP. Generative artificial intelligence empowers digital twins in drug discovery and clinical trials. Expert opinion on drug discovery. 2024 Jan-Jun:19(1):33-42. doi: 10.1080/17460441.2023.2273839. Epub 2024 Jan 8 [PubMed PMID: 37887266]
Level 3 (low-level) evidenceBhatia A, Appelbaum PS, Wisner KL. Unblinding in Randomized Controlled Trials: A Research Ethics Case. Ethics & human research. 2021 Mar:43(2):28-34. doi: 10.1002/eahr.500084. Epub [PubMed PMID: 33683016]
Level 1 (high-level) evidenceSilverman H. Ethical issues during the conduct of clinical trials. Proceedings of the American Thoracic Society. 2007 May:4(2):180-4; discussion 184 [PubMed PMID: 17494728]
Babiker A, El Husseini M, Al Nemri A, Al Frayh A, Al Juryyan N, Faki MO, Assiri A, Al Saadi M, Shaikh F, Al Zamil F. Health care professional development: Working as a team to improve patient care. Sudanese journal of paediatrics. 2014:14(2):9-16 [PubMed PMID: 27493399]
Vijayananthan A, Nawawi O. The importance of Good Clinical Practice guidelines and its role in clinical trials. Biomedical imaging and intervention journal. 2008 Jan:4(1):e5. doi: 10.2349/biij.4.1.e5. Epub 2008 Jan 1 [PubMed PMID: 21614316]
Level 1 (high-level) evidenceFleming TR, Demets DL, McShane LM. Discussion: The role, position, and function of the FDA-The past, present, and future. Biostatistics (Oxford, England). 2017 Jul 1:18(3):417-421. doi: 10.1093/biostatistics/kxx023. Epub [PubMed PMID: 28633307]
Ndebele P, Blanchard-Horan C, Shahkolahi A, Sanne I. Regulatory challenges associated with conducting multicountry clinical trials in resource-limited settings. Journal of acquired immune deficiency syndromes (1999). 2014 Jan 1:65 Suppl 1(0 1):S29-31. doi: 10.1097/QAI.0000000000000037. Epub [PubMed PMID: 24321981]
Thor S, Vetter T, Marcal A, Kweder S. EMA-FDA Parallel Scientific Advice: Optimizing Development of Medicines in the Global Age. Therapeutic innovation & regulatory science. 2023 Jul:57(4):656-661. doi: 10.1007/s43441-023-00501-9. Epub 2023 Mar 4 [PubMed PMID: 36871110]