Indications
Dopamine is a catecholamine and vasopressor commonly used to treat low blood pressure, low heart rate, and cardiac arrest, especially in acute neonatal cases, where it is administered as a continuous intravenous.[1] Dopamine exhibits dose-dependent effects. At low doses (<2 mcg/kg/min), dopamine predominantly stimulates dopaminergic (D1) receptors; however, this does not confer renal benefits. At moderate doses (5-10 mcg/kg/min), it primarily stimulates beta-1 receptors, increasing cardiac output by enhancing heart rate and contractility. At higher doses (>10 mcg/kg/min), dopamine stimulates alpha-1 receptor stimulation, resulting in peripheral vasoconstriction.[2]
Indications for dopamine include the maintenance of blood pressure for chronic congestive heart failure, trauma, renal failure, and even open-heart surgery and shock from myocardial infarction or septicemia. Dopamine administration in low doses may hypothetically improve hypotension, low cardiac output, and inadequate organ perfusion, often indicated by low urine production; however, current evidence does not support a clear clinical benefit.[3]
Dopamine also gained significant clinical importance in the central nervous system (CNS) following Hornykiewicz's experiments, which demonstrated a reduction in dopamine levels within the caudate nucleus of patients with Parkinson disease. Furthermore, the intravenous administration of its amino acid precursor, L-dihydroxyphenylalanine (L-DOPA), attenuated the Parkinsonian symptoms.[4]
As the blood–brain barrier prevents dopamine from entering the CNS from the systemic circulation, it is ineffective for treating central neurologic conditions such as Parkinson disease. In contrast, L-DOPA readily crosses the blood–brain barrier and can be administered systemically, including in oral form formulations. Although dopaminergic replacement therapy effectively alleviates motor symptoms, it may lead to motor adverse effects and behavioral issues associated with addiction, including impulse control disorders (see Image. Summary of Key Clinical Pearls).[5]
FDA-Approved Indications
Dopamine injection is indicated by the US Food and Drug Administration (FDA) to improve hemodynamic status in patients with distributive shock or shock due to reduced cardiac output. Prescribing information recommends correcting hypoxia, hypovolemia, and acidosis prior to initiating dopamine therapy.
Off-Label Uses
- According to the Society of Critical Care Medicine guidelines, norepinephrine is strongly recommended as the first-line vasopressor for adults with septic shock. When norepinephrine is unavailable, epinephrine or dopamine may be used as alternatives; however, efforts to ensure access to norepinephrine are strongly encouraged. Although the β1 activity of dopamine may be helpful in patients with myocardial dysfunction, its higher risk of arrhythmias limits routine use. Clinicians should exercise caution with dopamine and epinephrine, particularly in patients at high risk for cardiac arrhythmias.[6][7]
- The 2022 American Heart Association/American College of Cardiology/Heart Failure Society of America guideline for heart failure indicates that parenteral inotropes continue to be a viable option for supporting a subset of patients with heart failure who are refractory to other treatments and are experiencing the effects of end-organ hypoperfusion. Dopamine may be utilized; however, it is associated with an increased risk of tachyarrhythmias, nausea, headache, and tissue necrosis, and should be administered cautiously in patients receiving monoamine oxidase (MAO) inhibitors.[8]
- According to the 2018 American College of Cardiology/American Heart Association/Heart Rhythm Society guidelines for the acute medical management of bradycardia attributable to sinus node dysfunction or atrioventricular block, atropine is preferred; however, dopamine and other agents can be used based on patient factors. Higher doses of dopamine may be needed for a chronotropic response; however, they should be used carefully due to the risk of significant vasoconstriction and proarrhythmias.[9]
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
Dopamine biosynthesis follows the same enzymatic pathway as norepinephrine, with dopamine serving as a precursor in norepinephrine production (see Image. Biosynthesis of Catecholamines).[10][11] The first step of dopamine synthesis is rate-limiting and involves the conversion of L-tyrosine to L-DOPA by the enzyme tyrosine hydroxylase.[12][13][14] This conversion requires oxygen, an iron cofactor, and tetrahydrobiopterin (BH4), resulting in the addition of a hydroxyl group to the aromatic ring to form L-DOPA. This molecule is subsequently converted to dopamine by aromatic L-amino acid decarboxylase, which removes the carboxyl group. Once synthesized, dopamine is transported into synaptic vesicles via the vesicular monoamine transporter 2 to the synaptic terminals.[15][16][17]
If an individual regularly consumes L-tyrosine in abundance, it readily crosses the blood-brain barrier, as does L-DOPA.[18] However, its utility is spatially restricted because dopamine cannot cross the blood-brain barrier. In cases where L-tyrosine levels are low, L-phenylalanine may be converted into L-tyrosine by phenylalanine hydroxylase.
After dopamine is released into the synaptic cleft, it binds to receptors on both pre- and postsynaptic terminals, causing neuronal excitation or inhibition at the target neuron. Dopamine receptors are classified into 2 major families, comprising 5 distinct isoforms, each influencing specific intracellular signaling pathways.[19] Both families of dopamine receptors, D1 and D2, are, by definition, G protein–coupled receptors; however, D1 receptors result in the depolarization of neurons, whereas D2 receptors inhibit neuronal firing.[20]
After release into the synaptic cleft, dopamine is either transported back into the presynaptic neuron via dopamine transporters for repackaging or remains in the extracellular space to be taken up by glial cells or metabolized at the cellular membrane. Dopamine may be metabolized extraneuronally by catechol-O-methyltransferase (COMT) to 3-methoxytyramine, whereas MAO-B rapidly metabolizes 3-methoxytyramine to homovanillic acid.[21][22] Alternatively, it may undergo metabolism inside the cytoplasm, where the dual action of MAO-A and aldehyde dehydrogenase converts dopamine to the phenolic acid 3,4-dihydroxyphenylacetic acid.[23]
Given this complex sequence, dopamine modulation can occur at various levels, including the entire neuron, its projections, or the neuronal circuitry across the nervous system. Additionally, dopamine is regulated at multiple stages—during its synthesis (transcriptional, translational, and posttranslational regulation), synaptic packaging (regulation of the vesicular monoamine transporter and vesicle transport to the synapse), dopamine release (neuronal depolarization, calcium signaling, and vesicle fusion), and reuptake and metabolism through regulation of the respective enzymes and their spatial localization relative to their substrate.[23][24]
As indicated earlier, the systemic action of dopamine is mediated by various receptors (D1, D2, D3, D4, and D5) and the alpha- and beta-adrenergic receptors. These G protein–coupled receptors are typically classified as either D1 or D2 based on their canonical biochemical functions, reflecting dopamine's ability to modulate adenylyl cyclase activity.[11][25] However, based on their molecular structure, biochemical properties, and pharmacological functions, dopamine receptors are further classified into either the D1 class (D1 and D5) or the D2 class (D2, D3, and D4).[26][27][28]
Activation of D1 receptors on smooth muscle, the proximal renal tubule, and the cortical collecting duct increases diuresis.[29] D2 receptors are located presynaptically on the renal nerves and within the glomeruli and adrenal cortex. The activation of these receptors results in increased renal sodium and water excretion.[30] Apomorphine is a dopamine receptor agonist that may have a similar effect on these dopamine receptors.[31][32] Adrenergic receptors also bind dopamine, increasing arterial smooth muscle contraction and cardiac sinoatrial node conductivity, which explains its therapeutic benefits in the heart.
Although the blood-brain barrier specifically restricts the transport of dopamine from the systemic circulation into the CNS, further research has established its central role in reward-seeking behavior, where dopaminergic transmission becomes markedly increased. Current research on dopamine includes epigenetic changes and their involvement in a variety of psychiatric conditions, including substance use disorders and addiction, schizophrenia, and attention-deficit/hyperactivity disorder.[33][34] Altogether, these conditions involve disorders of the mesolimbic and mesocortical dopamine pathways.
A common effect of addictive drugs in the CNS is the increased release of dopamine in the striatum, classically associated with high locomotor activity and stereotypy.[35][36] The striatal dopamine increase results from axon projections arising directly from the pars compacta of the substantia nigra and the ventral tegmental area, respectively, which project to the nucleus accumbens and the amygdala, both of which are implicated in reward stimulation and the fear response.[35][37][38][39]
Another dopamine circuit, the tuberoinfundibular pathway, is primarily responsible for regulating the neuroendocrine secretion of prolactin from the anterior pituitary gland. Although prolactin is best known for its role in lactation, it also contributes to water and salt homeostasis, immune function, and cell-cycle regulation.[40][41] The nigrostriatal pathway is the main pathway involved in the motor deficits observed in Parkinson disease.[42] This pathway comprises dopaminergic neurons originating in the substantia nigra (pars compacta) and projects to the striatum via the medial forebrain bundle. These neurons form synapses with several neuronal populations at the putamen, caudate nucleus, globus pallidus internus, and the subthalamic nucleus. This elaborated network forms the afferent connections of the substantia nigra to the circuitry involved in motor movement, namely the basal ganglia. In the latter, dopamine plays a pivotal role in controlling motor movement and learning new motor skills.[43]
Pharmacokinetics
Absorption: Dopamine is not effectively absorbed when administered orally because it undergoes extensive first-pass metabolism in the gastrointestinal tract and liver. Consequently, it must be administered parenterally, typically via continuous intravenous infusion, to achieve therapeutic plasma concentrations. Following intravenous administration, its onset of action is rapid, typically within 5 minutes, reflecting its direct entry into the systemic circulation.
Distribution: Once in circulation, dopamine is rapidly distributed to highly perfused tissues, including the kidneys, mesenteric bed, heart, and vascular smooth muscle. Dopamine's volume of distribution is relatively small, indicating limited tissue penetration beyond extracellular fluid. Importantly, dopamine does not cross the blood-brain barrier in appreciable amounts, so its central dopaminergic effects are minimal when given peripherally.
Metabolism: Dopamine is extensively metabolized by MAO and COMT, which are widely distributed in the liver, kidneys, and plasma.[44] These enzymatic pathways convert dopamine into inactive metabolites, including homovanillic acid and 3,4-dihydroxyphenylacetic acid. Due to its rapid metabolism, dopamine has a very short plasma half-life of approximately 2 minutes. Therefore, it requires continuous infusion to maintain therapeutic effects.
Excretion: Dopamine metabolites are excreted primarily in urine, with more than 80% eliminated within 24 hours. Only trace amounts of unchanged dopamine appear in the urine.
Administration
Available Dosage Forms and Strengths
Dopamine hydrochloride injection is available as an intravenous solution at a concentration of 40 mg/mL (5- and 10-mL vials). For stimulation of the sympathetic nervous system, it is administered as a continuous intravenous infusion. Dopamine has a short half-life of approximately 1 to 5 minutes in systemic circulation; therefore, alternative slower forms of administration, such as oral administration, are typically ineffective.[45] Infusion solutions in 5% dextrose (D5W) are available at concentrations of 80 mg/100 mL, 160 mg/100 mL, and 320 mg/100 mL.
In addition to its peripheral sympathetic effects, dopamine is also critical for neurological movement function in Parkinson disease.[42] L-DOPA is administered via the oral route, and after absorption, a small portion crosses the blood–brain barrier, where it is utilized by neurons in the basal ganglia. L-DOPA is generally administered concomitantly with carbidopa to inhibit the peripheral effects of L-DOPA in the sympathetic nervous system. Carbidopa is a decarboxylase inhibitor that prevents the systemic conversion of L-DOPA to dopamine, which decreases the presentation of common adverse effects such as nausea and emesis.[46]
Dosage
According to the FDA label, the recommended starting dosage for adults and pediatric patients is 2 to 5 mcg/kg/min as a continuous intravenous infusion. The infusion rate may be adjusted in increments of 5 to 10 mcg/kg/min based on hemodynamic response. The maximum recommended dosage is 50 mcg/kg/min.
Dopamine injection should be administered only after dilution by intravenous infusion. Dopamine is administered into a large vein using an infusion pump, preferably in an intensive care setting. Before administration, the solution should be inspected for particulate matter or discoloration and should not be used if it appears darker or discolored. Higher-concentration solutions (eg, 3200 or 1600 mcg/mL strengths) are recommended for patients requiring fluid restriction. When discontinuing dopamine, the infusion rate should be tapered gradually based on the patient’s hemodynamic status.
Specific Patient Populations
Hepatic impairment: The hemodynamic profile of acute liver failure resembles that of septic shock, characterized by a hyperdynamic circulation with increased cardiac output, decreased systemic vascular resistance, and reduced effective circulating volume. The American College of Gastroenterology notes that pulse pressure variation may be used to assess fluid responsiveness; however, it requires expertise and further confirmation. When intravenous fluids fail to restore adequate blood pressure, vasopressors should be initiated to maintain a mean arterial pressure of 60 to 80 mm Hg sufficient to achieve a cerebral perfusion pressure. Norepinephrine is recommended as the first-line agent due to its survival benefit and lower risk of adverse outcomes.[47]
Renal impairment: Limited data are available; dopamine should be used with caution. However, due to its short half-life, the effect is likely minimal.
Pregnancy considerations: Adequate data from human studies regarding the use of dopamine in pregnancy are lacking, although animal studies have shown developmental toxicity at exposures lower than those used clinically. Because untreated maternal shock is life-threatening, dopamine should not be withheld if considered essential for maternal survival. Concomitant use with oxytocic drugs may precipitate severe maternal hypertension and should therefore be approached with caution.
Breastfeeding considerations: Caution is advised when administering to lactating women; no information is available regarding its use during breastfeeding. Due to its poor oral bioavailability and short half-life, dopamine in milk is unlikely to affect the infant. Although dopamine reduces serum prolactin in non-nursing women, its effect on milk production in nursing mothers is unknown.[48]
Pediatric patients: Dopamine has been used in neonates, infants, children, and adolescents, with weight-based dosing generally comparable to adults. The adverse event profile is similar to that observed in adults. However, inadvertent infusion into the umbilical artery has resulted in serious complications, including vasospasm and ischemia, and must be avoided. The Surviving Sepsis Guidelines recommend using epinephrine or norepinephrine instead of dopamine in pediatric patients with septic shock (weak recommendation, low-quality evidence).[49]
Older patients: Clinical studies involving patients aged 65 or older have been limited; however, existing data suggest that responses are similar to those in younger adults. As older patients are more likely to have impaired liver, kidney, or heart function, dopamine should be initiated at the lower end of the dosing range and carefully titrated.
Adverse Effects
Dopamine administration affects kidney function, leading to increased urinary output and a risk of arrhythmias.[50] Excessive dosing may lead to serious complications, including cerebrovascular events due to increased blood pressure.[51]
As previously stated, the neurotransmitter dopamine functions centrally within the mesocorticolimbic pathway, where it is involved in reward processing, fear responses, attention, and executive function, including complex planning.[37][38] Although systemic dopamine does not cross the blood-brain barrier, central dopaminergic activity is implicated in conditions such as somnolence, schizophrenia, addiction, and impulse control disorders.[18][33][52] Patients with neurological conditions using high doses of L-DOPA for Parkinson disease may experience physiological alterations due to the dysregulation of dopamine within the CNS pathways.
Drug-Drug Interactions
- Monoamine oxidase inhibitors: Dopamine is metabolized by MAO. The inhibition of dopamine metabolism by MAO results in prolonged effects, which increases the risk of severe hypertension and arrhythmias. In patients receiving MAO inhibitors within the past 2 to 3 weeks, the initial dopamine dose should be reduced to one-tenth of the usual starting dose. Examples of such inhibitors include phenelzine, rasagiline, selegiline, and linezolid.[53]
- Tricyclic antidepressants: Concomitant administration of dopamine may increase dopamine's cardiovascular effects, particularly hypertension. Blood pressure should be closely monitored in patients receiving agents such as amitriptyline, doxepin, imipramine, or nortriptyline.
- Other vasopressors: Concomitant use of dopamine with agents such as norepinephrine, epinephrine, or oxytocin may result in severe hypertension due to additive vasoconstrictive effects. Blood pressure should be closely monitored, and therapy should be carefully titrated.[54]
-
Antipsychotics: Haloperidol may block the systemic effects of dopamine.
-
Phenytoin: The anticonvulsant phenytoin may cause hypotension and decreased heart rate when used concomitantly with dopamine.
- Halogenated anesthetics: Concurrent use may increase myocardial sensitivity and autonomic irritability, predisposing patients to ventricular arrhythmias and hypertension. Cardiac rhythm should be monitored when dopamine is administered with agents such as desflurane, sevoflurane, or isoflurane.[55]
Contraindications
Dopamine is absolutely contraindicated in patients with pheochromocytoma.
Warnings and Precautions
- Tissue ischemia: Severe peripheral and visceral vasoconstriction may occur. Hypovolemia should be corrected before initiation, extremities should be monitored, and administration should occur via a large vein.
- Cardiac disorders: In patients with conditions of the heart or circulatory system, the intravenous administration of dopamine is relatively contraindicated. These conditions may include ventricular arrhythmias and tachycardia, blood vessel blockage, hypoxia, hypovolemia, and acidosis.
- Arrhythmias: The risk is greater in patients with underlying cardiac disorders, electrolyte imbalances, or structural heart disease. Management includes reducing or discontinuing dopamine and correcting electrolytes. In severe or sustained arrhythmias, antiarrhythmic therapy or cardioversion may be necessary.[56][57]
- Abrupt discontinuation: Sudden cessation of the infusion may result in marked hypotension; therefore, the dopamine infusion should be gradually tapered while administering intravenous fluids to maintain adequate blood volume.
- Severe hypersensitivity reactions: Dopamine may contain sodium metabisulfite, which may cause allergic reactions.[58] In susceptible individuals, this may result in life-threatening anaphylaxis or severe asthma exacerbations.
Monitoring
Monitoring of blood pressure and urine output is essential. Assessment of advanced hemodynamic parameters, including cardiac output, cardiac rhythm, and pulmonary capillary wedge pressure, is also recommended.
Importantly, dopamine agonists and mimetics that cross the blood-brain barrier interact with the neurological circuitry involved in motor, executive, and limbic functions, including addiction-linked reward systems, impulse-control mechanisms, and arousal. Thus, the cessation of dopamine therapies may lead to a condition called dopamine agonist withdrawal syndrome, which can present with symptoms such as anxiety, depression, panic attacks, fatigue, hypotension, nausea, irritability, and suicidal ideation.[59] Accordingly, centrally acting dopamine agonists should be tapered rather than abruptly discontinued.
Toxicity
Signs and Symptoms of Overdose or Toxicity
According to Sax's Dangerous Properties of Industrial Materials (by Richard J. Lewis, 2004; DOI: 10.1002/0471701343), studies in rodents showed an LD50 (lethal dose in 50% of subjects) ranging from 59 to 163 mg/kg. In humans, dopamine can lead to peripheral vasoconstriction, resulting in gangrenous extremities and cardiac arrhythmias.[60][61][62] Additionally, it can cause severe hypertension, tachycardia, confusion, and agitation.
Management of Overdose or Toxicity
No specific antidote exists for a dopamine overdose. If overdose is suspected, the infusion should be discontinued immediately. Symptoms generally resolve rapidly due to dopamine’s short half-life. If symptoms persist, an alpha-adrenergic blocker such as phentolamine may be administered.
Phentolamine can also be used to treat tissue necrosis resulting from dopamine extravasation.[63] Dopamine extravasation leads to intense local alpha-1–mediated vasoconstriction, ischemia, and potential necrosis. Phentolamine, a nonselective alpha-adrenergic antagonist, blocks these receptors, reversing vasoconstriction and restoring perfusion. Phentolamine is administered subcutaneously around the site of extravasation to prevent or treat ischemic injury. Topical nitroglycerin and subcutaneous terbutaline can be used as alternatives if phentolamine is unavailable or contraindicated.[64]
Enhancing Healthcare Team Outcomes
Dopamine administration has widespread effects on the cardiovascular system, kidneys, and CNS. Safe and effective use requires awareness of contraindications, including drug interactions with other pharmaceutical agents, lifestyle factors, and conditions that place similar strain on these organ systems. Medications such as psychopharmacological agents, neuroleptics, and general anesthetics, along with physiological stressors such as exercise-induced cardiac demand, may alter dopamine's impact and patient safety. An evidence-based approach, aligned with clear outcome objectives, is essential for optimal care.
An interprofessional approach is critical to the safe and effective use of dopamine. Clinicians determine the indication for therapy, initiate treatment, and titrate dosing based on the patient’s hemodynamic status. Emergency medicine clinicians are often involved in the early recognition and management of complications, including accidental overdose or extravasation injuries. Clinical pharmacists enhance patient safety by reviewing prescriptions for accuracy, monitoring for potential drug interactions, and providing guidance to the healthcare team on best practices, such as the use of phentolamine for extravasation management. Nurses provide continuous bedside monitoring, focusing on vital signs, infusion rates, and patient concerns, and serve as key communicators of changes in patient status.
Effective interprofessional communication and coordination among primary care providers, emergency clinicians, pharmacists, nurses, and therapists are critical to patient-centered care. By sharing information, anticipating complications, and reinforcing one another's responsibilities, the healthcare team can enhance patient outcomes, minimize risks, and support safe and ethical use of dopamine therapy.
Media
(Click Image to Enlarge)
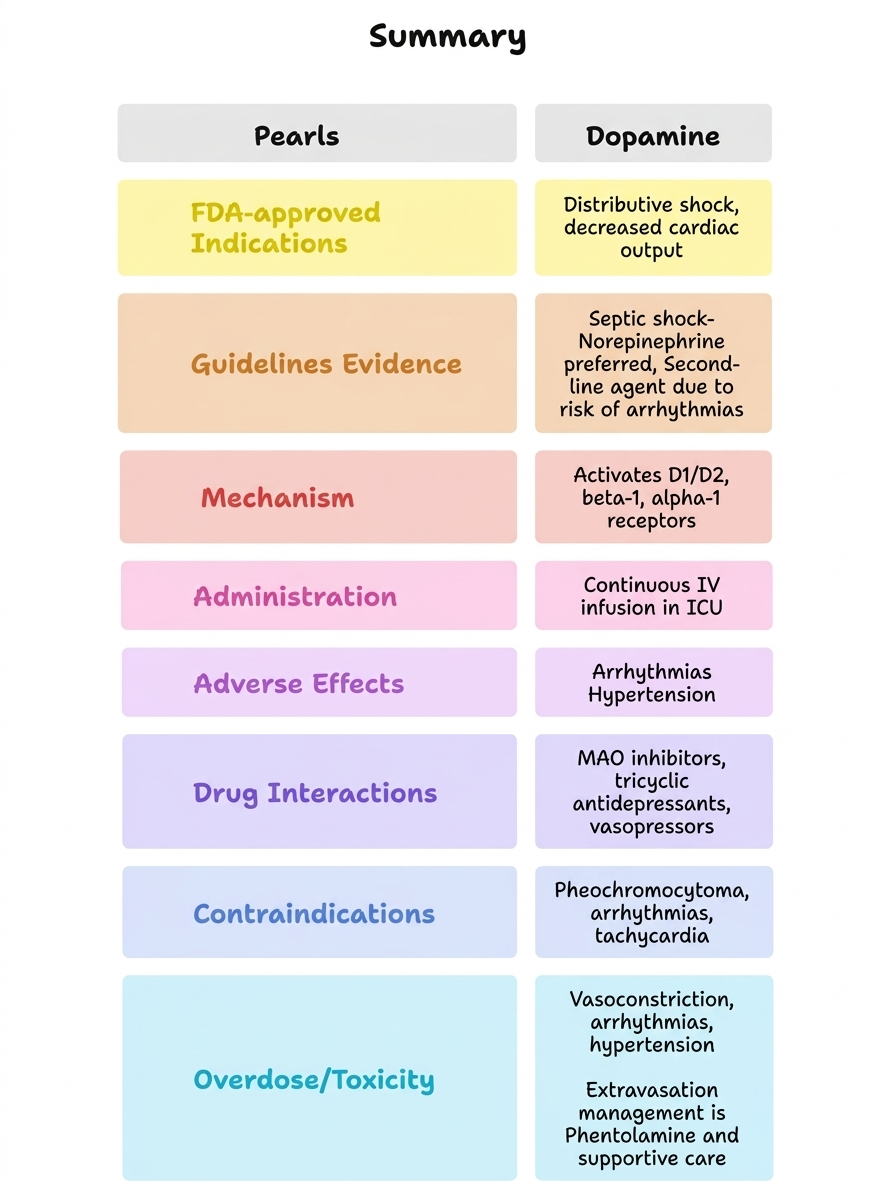
Summary of Key Clinical Pearls.
Abbreviations: FDA, Food and Drug Administration; ICU, intensive care unit; IV, intravenous; MOA, monoamine oxidase.
Contributed by P Patel, PharmD
(Click Image to Enlarge)
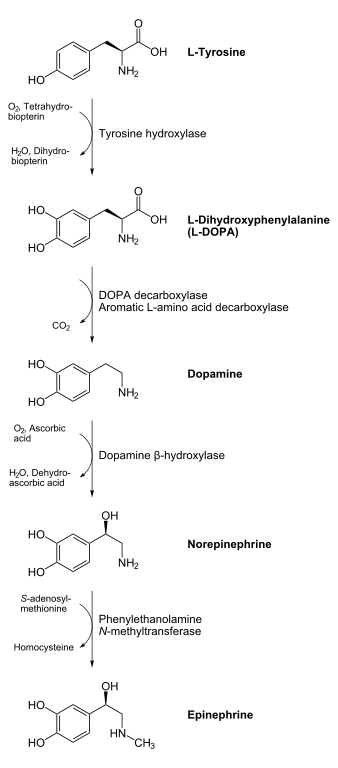
Biosynthesis of Catecholamines. Pathway illustrating the synthesis of adrenaline (epinephrine) and noradrenaline (norepinephrine), including key intermediates such as DOPA and dopamine.
NEUROtiker, Public Domain, via Wikimedia Commons
References
Bhatt-Mehta V, Nahata MC. Dopamine and dobutamine in pediatric therapy. Pharmacotherapy. 1989:9(5):303-14 [PubMed PMID: 2682552]
De Backer D, Biston P, Devriendt J, Madl C, Chochrad D, Aldecoa C, Brasseur A, Defrance P, Gottignies P, Vincent JL, SOAP II Investigators. Comparison of dopamine and norepinephrine in the treatment of shock. The New England journal of medicine. 2010 Mar 4:362(9):779-89. doi: 10.1056/NEJMoa0907118. Epub [PubMed PMID: 20200382]
Level 1 (high-level) evidenceSharma K, Vaishnav J, Kalathiya R, Hu JR, Miller J, Shah N, Hill T, Sharp M, Tsao A, Alexander KM, Gupta R, Montemayor K, Kovell L, Chasler JE, Lee YJ, Fine DM, Kass DA, Weiss RG, Thiemann DR, Ndumele CE, Schulman SP, Russell SD, Osler Medical Housestaff. Randomized Evaluation of Heart Failure With Preserved Ejection Fraction Patients With Acute Heart Failure and Dopamine: The ROPA-DOP Trial. JACC. Heart failure. 2018 Oct:6(10):859-870. doi: 10.1016/j.jchf.2018.04.008. Epub 2018 Aug 8 [PubMed PMID: 30098962]
Level 1 (high-level) evidenceHornykiewicz O. A brief history of levodopa. Journal of neurology. 2010 Nov:257(Suppl 2):S249-52. doi: 10.1007/s00415-010-5741-y. Epub [PubMed PMID: 21080185]
Level 3 (low-level) evidenceGhadery C, Valli M, Mihaescu A, Strafella R, Navalpotro I, Kim J, Strafella AP. Molecular Imaging of Addictive Behavior in Idiopathic Parkinson's Disease. International review of neurobiology. 2018:141():365-404. doi: 10.1016/bs.irn.2018.07.030. Epub 2018 Aug 13 [PubMed PMID: 30314604]
Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, Machado FR, Mcintyre L, Ostermann M, Prescott HC, Schorr C, Simpson S, Wiersinga WJ, Alshamsi F, Angus DC, Arabi Y, Azevedo L, Beale R, Beilman G, Belley-Cote E, Burry L, Cecconi M, Centofanti J, Coz Yataco A, De Waele J, Dellinger RP, Doi K, Du B, Estenssoro E, Ferrer R, Gomersall C, Hodgson C, Møller MH, Iwashyna T, Jacob S, Kleinpell R, Klompas M, Koh Y, Kumar A, Kwizera A, Lobo S, Masur H, McGloughlin S, Mehta S, Mehta Y, Mer M, Nunnally M, Oczkowski S, Osborn T, Papathanassoglou E, Perner A, Puskarich M, Roberts J, Schweickert W, Seckel M, Sevransky J, Sprung CL, Welte T, Zimmerman J, Levy M. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive care medicine. 2021 Nov:47(11):1181-1247. doi: 10.1007/s00134-021-06506-y. Epub 2021 Oct 2 [PubMed PMID: 34599691]
Marchetto L, Zanetto L, Comoretto RI, Padrin D, Menon K, Amigoni A, Daverio M. OUTCOMES OF PEDIATRIC FLUID-REFRACTORY SEPTIC SHOCK ACCORDING TO DIFFERENT VASOACTIVE STRATEGIES: A SYSTEMATIC REVIEW AND META-ANALYSIS. Shock (Augusta, Ga.). 2024 Nov 1:62(5):599-611. doi: 10.1097/SHK.0000000000002427. Epub 2024 Aug 8 [PubMed PMID: 39158574]
Level 1 (high-level) evidenceHeidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson LW, Vardeny O, Vest AR, Yancy CW. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Journal of the American College of Cardiology. 2022 May 3:79(17):e263-e421. doi: 10.1016/j.jacc.2021.12.012. Epub 2022 Apr 1 [PubMed PMID: 35379503]
Level 1 (high-level) evidenceKusumoto FM, Schoenfeld MH, Barrett C, Edgerton JR, Ellenbogen KA, Gold MR, Goldschlager NF, Hamilton RM, Joglar JA, Kim RJ, Lee R, Marine JE, McLeod CJ, Oken KR, Patton KK, Pellegrini CN, Selzman KA, Thompson A, Varosy PD. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2019 Aug 20:140(8):e382-e482. doi: 10.1161/CIR.0000000000000628. Epub 2018 Nov 6 [PubMed PMID: 30586772]
Level 1 (high-level) evidenceBlaschko H. The activity of l(-)-dopa decarboxylase. The Journal of physiology. 1942 Nov 30:101(3):337-49 [PubMed PMID: 16991567]
Snyder SH. What dopamine does in the brain. Proceedings of the National Academy of Sciences of the United States of America. 2011 Nov 22:108(47):18869-71. doi: 10.1073/pnas.1114346108. Epub 2011 Nov 21 [PubMed PMID: 22106252]
CARLSSON A, LINDQVIST M, MAGNUSSON T. 3,4-Dihydroxyphenylalanine and 5-hydroxytryptophan as reserpine antagonists. Nature. 1957 Nov 30:180(4596):1200 [PubMed PMID: 13483658]
Abbott A. Neuroscience: the molecular wake-up call. Nature. 2007 May 24:447(7143):368-70 [PubMed PMID: 17522649]
Level 3 (low-level) evidenceMONTAGU KA. Catechol compounds in rat tissues and in brains of different animals. Nature. 1957 Aug 3:180(4579):244-5 [PubMed PMID: 13451690]
Level 3 (low-level) evidenceSANO I, GAMO T, KAKIMOTO Y, TANIGUCHI K, TAKESADA M, NISHINUMA K. Distribution of catechol compounds in human brain. Biochimica et biophysica acta. 1959 Apr:32():586-7 [PubMed PMID: 14441532]
Carlsson A, Kehr W, Lindqvist M, Magnusson T, Atack CV. Regulation of monoamine metabolism in the central nervous system. Pharmacological reviews. 1972 Jun:24(2):371-84 [PubMed PMID: 4564607]
Level 3 (low-level) evidenceHaavik J, Toska K. Tyrosine hydroxylase and Parkinson's disease. Molecular neurobiology. 1998 Jun:16(3):285-309 [PubMed PMID: 9626667]
Level 3 (low-level) evidenceHardebo JE, Edvinsson L, Owman C, Rosengren E. Quantitative evaluation of the blood-brain barrier capacity to form dopamine from circulating L-DOPA. Acta physiologica Scandinavica. 1977 Mar:99(3):377-84 [PubMed PMID: 848309]
Level 3 (low-level) evidenceSibley DR, Monsma FJ Jr, Shen Y. Molecular neurobiology of dopaminergic receptors. International review of neurobiology. 1993:35():391-415 [PubMed PMID: 8463063]
Level 3 (low-level) evidenceDavid C, Fishburn CS, Monsma FJ Jr, Sibley DR, Fuchs S. Synthesis and processing of D2 dopamine receptors. Biochemistry. 1993 Aug 17:32(32):8179-83 [PubMed PMID: 8347618]
Level 3 (low-level) evidenceTank AW, Weiner H, Thurman JA. Enzymology and subcellular localization of aldehyde oxidation in rat liver. Oxidation of 3,4-dihydroxyphenylacetaldehyde derived from dopamine to 3,4-dihydroxyphenylacetic acid. Biochemical pharmacology. 1981 Dec 15:30(24):3265-75 [PubMed PMID: 7034733]
Level 3 (low-level) evidenceKopin IJ. Catecholamine metabolism: basic aspects and clinical significance. Pharmacological reviews. 1985 Dec:37(4):333-64 [PubMed PMID: 3915090]
Level 3 (low-level) evidenceMeiser J, Weindl D, Hiller K. Complexity of dopamine metabolism. Cell communication and signaling : CCS. 2013 May 17:11(1):34. doi: 10.1186/1478-811X-11-34. Epub 2013 May 17 [PubMed PMID: 23683503]
Seamans JK, Yang CR. The principal features and mechanisms of dopamine modulation in the prefrontal cortex. Progress in neurobiology. 2004 Sep:74(1):1-58 [PubMed PMID: 15381316]
Level 3 (low-level) evidenceMeder D, Herz DM, Rowe JB, Lehéricy S, Siebner HR. The role of dopamine in the brain - lessons learned from Parkinson's disease. NeuroImage. 2019 Apr 15:190():79-93. doi: 10.1016/j.neuroimage.2018.11.021. Epub 2018 Nov 20 [PubMed PMID: 30465864]
Mills A. Dopamine: from Cinderella to Holy Grail. Trends in pharmacological sciences. 1992 Nov:13(11):399-400 [PubMed PMID: 1440875]
Level 3 (low-level) evidenceBeaulieu JM, Gainetdinov RR. The physiology, signaling, and pharmacology of dopamine receptors. Pharmacological reviews. 2011 Mar:63(1):182-217. doi: 10.1124/pr.110.002642. Epub 2011 Feb 8 [PubMed PMID: 21303898]
Level 3 (low-level) evidenceAndersen PH, Gingrich JA, Bates MD, Dearry A, Falardeau P, Senogles SE, Caron MG. Dopamine receptor subtypes: beyond the D1/D2 classification. Trends in pharmacological sciences. 1990 Jun:11(6):231-6 [PubMed PMID: 2200181]
Level 3 (low-level) evidenceGoldberg LI. Dopamine receptors and hypertension. Physiologic and pharmacologic implications. The American journal of medicine. 1984 Oct 5:77(4A):37-44 [PubMed PMID: 6148892]
Level 3 (low-level) evidenceVelasco M, Luchsinger A. Dopamine: pharmacologic and therapeutic aspects. American journal of therapeutics. 1998 Jan:5(1):37-43 [PubMed PMID: 10099036]
Montastruc JL, Chamontin B, Rostin M, Rascol O, Valet P, Gaillard G, Tran MA, Van TT, Ader JL, Montastruc P. Experimental and clinical approaches to treatment of hypertension by dopamine receptor agonists. Clinical and experimental hypertension. Part A, Theory and practice. 1987:9(5-6):1069-84 [PubMed PMID: 3304729]
Houvenaghel JF, Meyer M, Schmitt E, Arifi A, Benchetrit E, Bichon A, Cau C, Lavigne L, Le Mercier E, Czernecki V, Dujardin K. Influence of continuous subcutaneous apomorphine infusion on cognition and behavior in Parkinson's disease: A systematic review. Revue neurologique. 2025 Mar:181(3):156-171. doi: 10.1016/j.neurol.2024.06.008. Epub 2024 Aug 6 [PubMed PMID: 39112115]
Level 1 (high-level) evidenceFeng J, Nestler EJ. Epigenetic mechanisms of drug addiction. Current opinion in neurobiology. 2013 Aug:23(4):521-8. doi: 10.1016/j.conb.2013.01.001. Epub 2013 Jan 29 [PubMed PMID: 23374537]
Level 3 (low-level) evidenceHowes OD, McCutcheon R, Owen MJ, Murray RM. The Role of Genes, Stress, and Dopamine in the Development of Schizophrenia. Biological psychiatry. 2017 Jan 1:81(1):9-20. doi: 10.1016/j.biopsych.2016.07.014. Epub 2016 Aug 6 [PubMed PMID: 27720198]
Wise RA. Addictive drugs and brain stimulation reward. Annual review of neuroscience. 1996:19():319-40 [PubMed PMID: 8833446]
Level 3 (low-level) evidenceWise RA. Drug-activation of brain reward pathways. Drug and alcohol dependence. 1998 Jun-Jul:51(1-2):13-22 [PubMed PMID: 9716927]
Level 3 (low-level) evidenceJellinger KA. Post mortem studies in Parkinson's disease--is it possible to detect brain areas for specific symptoms? Journal of neural transmission. Supplementum. 1999:56():1-29 [PubMed PMID: 10370901]
Level 3 (low-level) evidenceRoot DH, Fabbricatore AT, Ma S, Barker DJ, West MO. Rapid phasic activity of ventral pallidal neurons during cocaine self-administration. Synapse (New York, N.Y.). 2010 Sep:64(9):704-13. doi: 10.1002/syn.20792. Epub [PubMed PMID: 20340176]
Level 3 (low-level) evidenceHou G, Hao M, Duan J, Han MH. The Formation and Function of the VTA Dopamine System. International journal of molecular sciences. 2024 Mar 30:25(7):. doi: 10.3390/ijms25073875. Epub 2024 Mar 30 [PubMed PMID: 38612683]
Grattan DR. 60 YEARS OF NEUROENDOCRINOLOGY: The hypothalamo-prolactin axis. The Journal of endocrinology. 2015 Aug:226(2):T101-22. doi: 10.1530/JOE-15-0213. Epub 2015 Jun 22 [PubMed PMID: 26101377]
Dobolyi A, Grattan DR, Stolzenberg DS. Preoptic inputs and mechanisms that regulate maternal responsiveness. Journal of neuroendocrinology. 2014 Oct:26(10):627-40. doi: 10.1111/jne.12185. Epub [PubMed PMID: 25059569]
Level 3 (low-level) evidenceChristine CW, Aminoff MJ. Clinical differentiation of parkinsonian syndromes: prognostic and therapeutic relevance. The American journal of medicine. 2004 Sep 15:117(6):412-9 [PubMed PMID: 15380498]
Mink JW. Basal ganglia mechanisms in action selection, plasticity, and dystonia. European journal of paediatric neurology : EJPN : official journal of the European Paediatric Neurology Society. 2018 Mar:22(2):225-229. doi: 10.1016/j.ejpn.2018.01.005. Epub 2018 Jan 17 [PubMed PMID: 29396175]
Cho HU, Kim S, Sim J, Yang S, An H, Nam MH, Jang DP, Lee CJ. Redefining differential roles of MAO-A in dopamine degradation and MAO-B in tonic GABA synthesis. Experimental & molecular medicine. 2021 Jul:53(7):1148-1158. doi: 10.1038/s12276-021-00646-3. Epub 2021 Jul 9 [PubMed PMID: 34244591]
Perrin G, Papazian L, Martin C. [Dopexamine: a new dopaminergic agonist]. Annales francaises d'anesthesie et de reanimation. 1993:12(3):308-20 [PubMed PMID: 7902685]
Level 3 (low-level) evidenceGilbert JA, Frederick LM, Ames MM. The aromatic-L-amino acid decarboxylase inhibitor carbidopa is selectively cytotoxic to human pulmonary carcinoid and small cell lung carcinoma cells. Clinical cancer research : an official journal of the American Association for Cancer Research. 2000 Nov:6(11):4365-72 [PubMed PMID: 11106255]
Shingina A, Mukhtar N, Wakim-Fleming J, Alqahtani S, Wong RJ, Limketkai BN, Larson AM, Grant L. Acute Liver Failure Guidelines. The American journal of gastroenterology. 2023 Jul 1:118(7):1128-1153. doi: 10.14309/ajg.0000000000002340. Epub 2023 Mar 20 [PubMed PMID: 37377263]
. Dopamine. Drugs and Lactation Database (LactMed®). 2006:(): [PubMed PMID: 30000702]
Weiss SL, Peters MJ, Alhazzani W, Agus MSD, Flori HR, Inwald DP, Nadel S, Schlapbach LJ, Tasker RC, Argent AC, Brierley J, Carcillo J, Carrol ED, Carroll CL, Cheifetz IM, Choong K, Cies JJ, Cruz AT, De Luca D, Deep A, Faust SN, De Oliveira CF, Hall MW, Ishimine P, Javouhey E, Joosten KFM, Joshi P, Karam O, Kneyber MCJ, Lemson J, MacLaren G, Mehta NM, Møller MH, Newth CJL, Nguyen TC, Nishisaki A, Nunnally ME, Parker MM, Paul RM, Randolph AG, Ranjit S, Romer LH, Scott HF, Tume LN, Verger JT, Williams EA, Wolf J, Wong HR, Zimmerman JJ, Kissoon N, Tissieres P. Surviving Sepsis Campaign International Guidelines for the Management of Septic Shock and Sepsis-Associated Organ Dysfunction in Children. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies. 2020 Feb:21(2):e52-e106. doi: 10.1097/PCC.0000000000002198. Epub [PubMed PMID: 32032273]
Stoker TB, Torsney KM, Barker RA. Emerging Treatment Approaches for Parkinson's Disease. Frontiers in neuroscience. 2018:12():693. doi: 10.3389/fnins.2018.00693. Epub 2018 Oct 8 [PubMed PMID: 30349448]
De Vecchis R, Ciccarelli A, Pucciarelli A. Unloading therapy by intravenous diuretic in chronic heart failure: a double-edged weapon? Journal of cardiovascular medicine (Hagerstown, Md.). 2010 Aug:11(8):571-4. doi: 10.2459/JCM.0b013e32833d37b9. Epub [PubMed PMID: 20588135]
Cho JR, Treweek JB, Robinson JE, Xiao C, Bremner LR, Greenbaum A, Gradinaru V. Dorsal Raphe Dopamine Neurons Modulate Arousal and Promote Wakefulness by Salient Stimuli. Neuron. 2017 Jun 21:94(6):1205-1219.e8. doi: 10.1016/j.neuron.2017.05.020. Epub 2017 Jun 8 [PubMed PMID: 28602690]
Tan YY, Jenner P, Chen SD. Monoamine Oxidase-B Inhibitors for the Treatment of Parkinson's Disease: Past, Present, and Future. Journal of Parkinson's disease. 2022:12(2):477-493. doi: 10.3233/JPD-212976. Epub [PubMed PMID: 34957948]
Kittner SJ, Stern BJ, Feeser BR, Hebel R, Nagey DA, Buchholz DW, Earley CJ, Johnson CJ, Macko RF, Sloan MA, Wityk RJ, Wozniak MA. Pregnancy and the risk of stroke. The New England journal of medicine. 1996 Sep 12:335(11):768-74 [PubMed PMID: 8703181]
Votaw J, Byas-Smith M, Hua J, Voll R, Martarello L, Levey AI, Bowman FD, Goodman M. Interaction of isoflurane with the dopamine transporter. Anesthesiology. 2003 Feb:98(2):404-11 [PubMed PMID: 12552200]
Neumann J, Hofmann B, Dhein S, Gergs U. Role of Dopamine in the Heart in Health and Disease. International journal of molecular sciences. 2023 Mar 6:24(5):. doi: 10.3390/ijms24055042. Epub 2023 Mar 6 [PubMed PMID: 36902474]
Yamaguchi T, Sumida TS, Nomura S, Satoh M, Higo T, Ito M, Ko T, Fujita K, Sweet ME, Sanbe A, Yoshimi K, Manabe I, Sasaoka T, Taylor MRG, Toko H, Takimoto E, Naito AT, Komuro I. Cardiac dopamine D1 receptor triggers ventricular arrhythmia in chronic heart failure. Nature communications. 2020 Aug 31:11(1):4364. doi: 10.1038/s41467-020-18128-x. Epub 2020 Aug 31 [PubMed PMID: 32868781]
Ekstein SF, Warshaw EM. Sulfites: Allergen of the Year 2024. Dermatitis : contact, atopic, occupational, drug. 2024 Jan-Feb:35(1):6-12. doi: 10.1089/derm.2023.0154. Epub 2023 Aug 17 [PubMed PMID: 37590472]
Yu XX, Fernandez HH. Dopamine agonist withdrawal syndrome: A comprehensive review. Journal of the neurological sciences. 2017 Mar 15:374():53-55. doi: 10.1016/j.jns.2016.12.070. Epub 2017 Jan 2 [PubMed PMID: 28104232]
Colak T, Erdogan O, Yerebakan O, Arici C, Gurkan A. Symmetrical peripheral gangrene and dopamine. Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES. 2003 Jul:9(3):222-4 [PubMed PMID: 12923702]
Level 3 (low-level) evidenceGelfman DM, Ornato JP, Gonzalez ER. Dopamine-induced increase in atrioventricular conduction in atrial fibrillation-flutter. Clinical cardiology. 1987 Nov:10(11):671-3 [PubMed PMID: 3677500]
Level 3 (low-level) evidenceTakeshita J, Kawaguchi A, Kawasaki T, Ishihara T, Shime N. Local Adverse Events Associated with Peripheral Vasoactive Infusion in Children: A Systematic Review with Meta-analysis. Journal of cardiothoracic and vascular anesthesia. 2024 Dec:38(12):3215-3223. doi: 10.1053/j.jvca.2024.08.020. Epub 2024 Aug 13 [PubMed PMID: 39227190]
Level 1 (high-level) evidenceSubhani M, Sridhar S, DeCristofaro JD. Phentolamine use in a neonate for the prevention of dermal necrosis caused by dopamine: a case report. Journal of perinatology : official journal of the California Perinatal Association. 2001 Jul-Aug:21(5):324-6 [PubMed PMID: 11536027]
Level 3 (low-level) evidencePlum M, Moukhachen O. Alternative Pharmacological Management of Vasopressor Extravasation in the Absence of Phentolamine. P & T : a peer-reviewed journal for formulary management. 2017 Sep:42(9):581-592 [PubMed PMID: 28890646]