Definition/Introduction
The oculocephalic reflex (doll's eyes reflex) is an application of the vestibular-ocular reflex used for neurologic examination of cranial nerves III, VI, and VIII, the reflex arc including brainstem nuclei, and overall gross brainstem function. This reflex is used to examine patients in the neurologic critical care setting and may be useful for assessing neonates, anesthetized patients, or patients with dizziness.[1][2][3][4][5] The reflex derives its name from the characteristic doll-like appearance of a patient's eyes when the reflex is positive.[6]
The oculocephalic reflex is performed by holding a patient's eyelids open and moving their head from side to side. The examination should be performed only on patients with a stable cervical spine and no C-spine precautions. With the patient's eyelids open, the examiner briskly rotates the patient's head from side to side while observing the patient's eyes. The examiner observes a positive oculocephalic reflex when the patient moves their eyes in the opposite direction of their head's rotation, so that their eyes remain looking forward (like a doll's eyes). The examiner observes a negative oculocephalic reflex when the patient's eyes stay midline and do not move while the examiner rotates the head.
A similar examination can be performed for vertical eye movements.[6] Note that the designation of a positive result (eyes moving in the opposite direction of head movement, indicating an intact brainstem function) or a negative result (eyes moving towards the same direction of head movement, indicating severe brainstem dysfunction) for the doll's eyes reflex is an oversimplification, and that some eye movement with nystagmus can occur in pathologic states.[7] The reflex is suppressed in a conscious adult with normal neurologic function but is active in a comatose patient with gross brainstem function, absent if there is damage to the reflex arc.[6]
The reflex arc in the doll's eyes has been extensively studied. The vestibulo-ocular reflex arc consists of a series of brainstem nuclei and the nerves connecting them, as well as the vestibular system and the extraocular muscles of the eye. In the simplest version of the reflex arc, angular rotation of the head causes the endolymph in the horizontal semicircular canals to rotate in the opposite direction to the head's rotation; this causes the ipsilateral vestibular nerve to activate the ipsilateral vestibular nucleus and the contralateral vestibular nerve to inhibit the contralateral vestibular nucleus. Both vestibular nuclei then activate or inhibit the abducens nuclei, which send signals to the corresponding ipsilateral lateral rectus and the contralateral oculomotor nucleus through the medial longitudinal fasciculus. The oculomotor nuclei then activate or inhibit the corresponding ipsilateral medial recti. Ultimately, the reflex is elicited if all components of the arc are intact and if consciousness does not suppress it.[8]
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
The examiner should not perform the reflex on those patients with head or neck injuries who could be further injured by the reflex technique.
Clinical Significance
There are several areas of clinical practice where the doll's eye reflex has significance:
- Vestibular lesions: Lesions to the vestibular nerve or vestibular nuclei have been shown to impair the ipsilateral doll's eyes reflex.[7]
- Assessing dizziness: The doll's eyes reflex can be used in the office to assess dizziness with rapid vestibular-ocular reflex testing. An abnormal response would show refixation saccades. The reflex is 39% sensitive and 97% specific.[4]
- Psychiatric patients: Patients with bipolar adisorder nd schizophrenia can show abnormal smooth pursuit eye movements, both vertical and horizontal. However, there is evidence that these patients should show an intact doll's eyes reflex.[9]
- Intensive care units: The doll's eyes reflex (oculocephalic response) in critically ill intensive care patients can independently predict altered mental status (delirium, coma, confusion) after cessation of sedation.[1]
- Neonates: Most neonates exhibit an unsuppressed doll's eyes reflex before 11.5 weeks; this can serve as a neonatal milestone in neurologic development.[2][10]
- Anesthesia: Assessing the doll's eye reflex can be helpful in ophthalmologic surgery.[3]
- Nursing: -Like other reflexes, nursing staff can receive training to evaluate the doll's eye reflex in select patients.[11]
Nursing, Allied Health, and Interprofessional Team Interventions
The nurses should know how to elicit the reflex and its prognostic implications. Also, it would be wise to remind the doctor whether a cervical spine injury has been cleared before the reflex is elicited in a trauma patient.
Media
(Click Image to Enlarge)
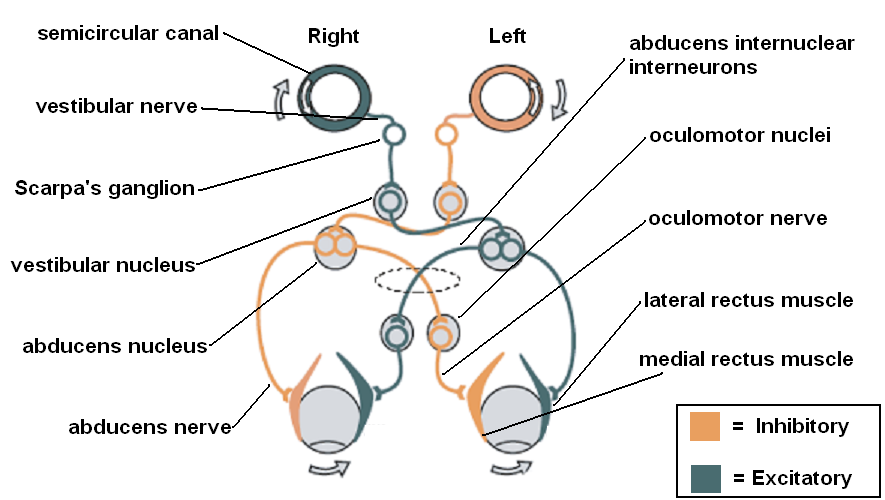
Vestibulo-ocular reflex Courtesy: https://commons.wikimedia.org/wiki/File:Vestibulo-ocular_reflex.PNG
References
Sharshar T, Porcher R, Siami S, Rohaut B, Bailly-Salin J, Hopkinson NS, Clair B, Guidoux C, Iacobone E, Sonneville R, Polito A, Aboab J, Gaudry S, Morla O, Amouyal G, Azuar J, Allary J, Vieillard-Baron A, Wolff M, Cariou A, Annane D, Paris-Ouest Study Group on Neurological Effect of Sedation (POSGNES). Brainstem responses can predict death and delirium in sedated patients in intensive care unit. Critical care medicine. 2011 Aug:39(8):1960-7. doi: 10.1097/CCM.0b013e31821b843b. Epub [PubMed PMID: 21532477]
Level 2 (mid-level) evidenceSnir M, Hasanreisoglu M, Goldenberg-Cohen N, Friling R, Katz K, Nachum Y, Benjamini Y, Herscovici Z, Axer-Siegel R. Suppression of the oculocephalic reflex (doll's eyes phenomenon) in normal full-term babies. Current eye research. 2010 May:35(5):370-4. doi: 10.3109/02713680903576708. Epub [PubMed PMID: 20450249]
Wong RV, Craddock MK, Whitten ME. Using the oculocephalic reflex to assess effective retrobulbar anesthesia. Ophthalmic surgery. 1993 May:24(5):339-42 [PubMed PMID: 8515952]
Harvey SA, Wood DJ. The oculocephalic response in the evaluation of the dizzy patient. The Laryngoscope. 1996 Jan:106(1 Pt 1):6-9 [PubMed PMID: 8544630]
Somisetty S, Das JM. Neuroanatomy, Vestibulo-ocular Reflex. StatPearls. 2026 Jan:(): [PubMed PMID: 31424881]
Pullen RL. Checking for oculocephalic reflex. Nursing. 2005 Jun:35(6):24 [PubMed PMID: 15931097]
Foster CA, Foster BD, Spindler J, Harris JP. Functional loss of the horizontal doll's eye reflex following unilateral vestibular lesions. The Laryngoscope. 1994 Apr:104(4):473-8 [PubMed PMID: 8164488]
Ito M. Cerebellar control of the vestibulo-ocular reflex--around the flocculus hypothesis. Annual review of neuroscience. 1982:5():275-96 [PubMed PMID: 6803651]
Level 3 (low-level) evidenceLipton RB, Levin S, Holzman PS. Horizontal and vertical pursuit eye movements, the oculocephalic reflex, and the functional psychoses. Psychiatry research. 1980 Oct:3(2):193-203 [PubMed PMID: 6947312]
Sheth RD, Bodensteiner JB, Riggs JE. The unmodulated oculocephalic reflex: clinical feature of the persistent vegetative state in the neonate. Journal of child neurology. 1996 May:11(3):255-6 [PubMed PMID: 8734036]
Level 3 (low-level) evidenceZegeer LJ. Oculocephalic and vestibulo-ocular responses: significance for nursing care. The Journal of neuroscience nursing : journal of the American Association of Neuroscience Nurses. 1989 Feb:21(1):46-55 [PubMed PMID: 2523440]