Indications
Disopyramide, a class 1A antiarrhythmic drug, received Food and Drug Administration approval on September 29, 1978, for established ventricular arrhythmias like sustained ventricular tachycardia that, in the physician's judgment, are life-threatening. As a Class Ia antiarrhythmic agent, disopyramide functions by blocking sodium channels in the cardiac cell membranes, which stabilizes cardiac electrical activity and can help restore a normal heart rhythm.
Food and Drug Administration–Approved Indications
- Ventricular arrhythmias: Disopyramide is used for the management of symptomatic sustained ventricular arrhythmias, particularly in patients who do not respond to or cannot tolerate other antiarrhythmic therapies. Due to the proarrhythmic effects of disopyramide and the emergence of newer agents with reduced toxicity profiles, the use of disopyramide for this indication has significantly declined in clinical practice.[1]
Off-Label Uses
- Atrial fibrillation/atrial flutter: Although not officially approved for this indication, disopyramide may be used off-label for rate control in patients with atrial fibrillation or flutter.[2] Additionally, based on a randomized, double-blind, placebo-controlled 1-year follow-up study, disopyramide (n = 44) was found to be more effective than placebo (n = 46) in maintaining sinus rhythm after electrocardioversion for atrial fibrillation. The difference is significant at 1-month follow-up (70% versus 39%) and persists after twelve months (54% versus 30%).[3]
- Hypertrophic cardiomyopathy: Disopyramide has demonstrated symptomatic improvement in patients with obstructive hypertrophic cardiomyopathy who have not adequately responded to first-line treatments, such as beta-blockers, verapamil, or diltiazem.[4][5][6] This agent serves as a crucial therapeutic alternative, especially for patients who are not suitable candidates for septal reduction therapies.[7] However, it is important to note that disopyramide can increase conduction through the atrioventricular node, potentially precipitating rapid conduction in the context of atrial fibrillation. Therefore, its use should be combined with another agent that possesses atrioventricular nodal blocking properties, such as a beta-blocker, verapamil, or diltiazem, to mitigate the risk of atrial fibrillation–related complications.[8] Data from the multicenter study of safety and efficacy of disopyramide in obstructive cardiomyopathy showed that disopyramide significantly decreases (P < 0.0001) the left ventricular outflow tract gradient from 75±33 to 40±32 mm Hg in 78 patients (66% of the study subjects) and improves New York Heart Association functional class from 23±07 to 17±06 (P < 0.0001).[9][10] According to the 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR guidelines, patients with obstructive hypertrophic cardiomyopathy who remain symptomatic due to left ventricular outflow tract obstruction—despite treatment with beta-blockers or nondihydropyridine calcium channel blockers—may require additional therapeutic interventions. Recommended options include the addition of a myosin inhibitor, such as disopyramide (administered in conjunction with an atrioventricular nodal blocking agent), or septal reduction therapy performed at experienced centers.[5]
-
According to recent meta-analyses, pharmacological treatments effectively lower left ventricular outflow tract gradients in patients with obstructive hypertrophic cardiomyopathy, with disopyramide and cardiac myosin inhibitors having the greatest impact, followed by beta-blockers and calcium channel blockers.[11]
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
According to the Vaughan Williams classification, antiarrhythmic drugs are classified into 5 main classes based on their mechanism of action. The class of antiarrhythmic agents primarily works by blocking sodium ion channels, which are responsible for the fast inward depolarizing current in cardiomyocytes. Type 1 drugs are sodium channel blockers, further divided into subclasses 1A, 1B, and 1C, each with distinct properties and mechanisms of action. Class 1A antiarrhythmic drugs moderate the influx of sodium and also have effects on potassium channels. Disopyramide is an antiarrhythmic drug that belongs to class Ia. As with other class I antiarrhythmic drugs, such as quinidine, ajmaline, and procainamide, the mechanism of action of disopyramide is to lengthen the action potential duration of cardiomyocytes, reflected by the rightward shift of the action potential curve. Additionally, it lowers the rate of diastolic depolarization (phase 4) in cells with augmented automaticity and the upstroke velocity (phase 1).[12] Therefore, disopyramide decreases myocardial excitability and conduction velocity.
In animal studies, disopyramide has been observed to reduce the rate of diastolic depolarization (phase 4) in cells exhibiting heightened automaticity. Additionally, it decreases the upstroke velocity (phase 0) and prolongs the action potential duration in normal cardiac cells. Disopyramide also diminishes the refractoriness disparity between infarcted myocardium and adjacent normally perfused tissue, while showing no interaction with alpha- or beta-adrenergic receptors.[13]
In humans, therapeutic plasma levels of disopyramide are associated with a reduction in sinus node recovery time and an extension of the effective refractory period in the atrium, while exerting only a minimal impact on the effective refractory period of the atrioventricular node. The drug has little effect on atrioventricular nodal and His-Purkinje conduction times or QRS duration. However, it does lead to prolonged conduction within accessory pathways.[14]
In vitro studies show that the anticholinergic activity of disopyramide is approximately 0.06% that of atropine. The usual dosing schedule for disopyramide is 150 mg administered every 6 hours, whereas disopyramide CR is dosed at 300 mg every 12 hours. By comparison, the standard dose of atropine typically ranges from 0.4 to 0.6 mg.[15]
Disopyramide and other class Ia antiarrhythmics also block the rapid component of the delayed rectifier potassium current when blocking the sodium channel, resulting in QT interval prolongation.[16][17]
Pharmacokinetics
Absorption: The drug is rapidly absorbed and is almost completely bioavailable, ensuring that effective plasma concentrations are achieved quickly after administration. The onset of therapeutic effects occurs within 0.5 to 3.5 hours. For the immediate release formulation, the pharmacological effects last approximately 1.5 to 8.5 hours, which informs dosing schedules based on the desired effect. The peak serum concentration for immediate-release formulations is achieved within 2 hours, whereas controlled-release formulations reach their peak levels within 4 to 7 hours after administration. Therapeutic plasma concentrations of disopyramide base generally range from 2 to 4 mcg/mL, during which protein binding fluctuates between 50% and 65%. Due to concentration-dependent protein binding, predicting the free drug concentration from total drug levels is a complex process. For the immediate-release formulation, the pharmacological effects last approximately 1.5 to 8.5 hours, which informs dosing schedules based on the desired effect.[18]
Distribution: In children aged 5 to 12, the volume of distribution is 1.02±0.2 L/kg (as reported by Chiba in 1992), reflecting the drug's distribution within the body tissues. In adults, volume distribution (Vd) ranges from 0.8 to 2 L/kg, indicating variability based on individual patient characteristics.
Metabolism: The drug undergoes hepatic metabolism, primarily through the process of N-dealkylation, producing the active metabolite N-despropyldisopyramide, along with several inactive metabolites that are less pharmacologically relevant. A recent study suggests that obesity may affect the pharmacokinetics of disopyramide; however, further research is required.[2]
Excretion: In children aged 5 to 12, the elimination half-life is approximately 3.15±0.64 hours, which may necessitate adjustments in the dosing frequency. In adults, the half-life ranges from 4 to 10 hours, with notable prolongation in patients suffering from heart failure or with hepatic or renal impairment, highlighting the need for monitoring in these populations. The drug is primarily excreted through the urine, with approximately 50% of the dose eliminated as the unchanged drug, 20% as the metabolite N-despropyldisopyramide, and 10% as other metabolites. Additional excretion occurs through feces, accounting for 10% to 15% of elimination. In children aged 5 to 12, the clearance rate is calculated at 3.79±0.82 mL/min/kg, which is higher than that typically observed in adults, suggesting a need for adjusted dosing in pediatric populations based on their enhanced metabolic capacity.[19]
Administration
Available Dosage Forms and Strengths
Disopyramide is an orally administered medication in capsule form. There are 2 types of capsule formulations, differing in their drug delivery system properties—the immediate-release and extended-release disopyramide capsules. When using the standard release capsules, an initial dose of 200 to 300 mg of disopyramide is administered, followed by 100 to 150 mg every 6 hours. The dosage of disopyramide CR must be tailored to each patient based on their response and tolerance.
Adult Dosage
Ventricular arrhythmias: For patients weighing less than 110 pounds (50 kg), the recommended dosage is 400 mg/d, administered in divided doses. This total daily dose can be achieved by taking 100 mg every 6 hours for immediate-release disopyramide or 200 mg every 12 hours for disopyramide CR. In cases where increased anticholinergic adverse effects occur, plasma levels of disopyramide should be monitored, and the dose may need to be adjusted. A reduction in dosage by one-third—from the standard 600 to 400 mg/d—may be reasonable without changing the dosing interval.
For patients requiring rapid control of ventricular arrhythmia, an initial loading dose of 300 mg of immediate-release disopyramide is recommended (or 200 mg for patients weighing less than 110 pounds), followed by the appropriate maintenance dosage. Therapeutic effects are typically observed within 30 minutes to 3 hours after administering a 300 mg loading dose. If there is no response or signs of toxicity within 6 hours, 200 mg of immediate-release disopyramide may be prescribed every 6 hours instead of the usual 150 mg.
If there is no response to this dosage within 48 hours, the clinician should consider discontinuing disopyramide or hospitalizing the patient for careful monitoring while administering subsequent immediate-release disopyramide doses of 250 or 300 mg every 6 hours. Although a limited number of patients with severe refractory ventricular tachycardia have tolerated doses of disopyramide up to 1600 mg/d (400 mg every 6 hours), resulting in plasma levels as high as 9 mcg/mL, such treatment should only occur in a hospital setting with close evaluation and continuous monitoring. Disopyramide should not be initiated if rapid establishment of control is required.
To promote less variation in peak and trough serum levels, disopyramide should be administered around the clock (4 times per day; 12-6-12 6, not 9-1-5-9). The controlled-release capsules should not be broken or chewed.
Hypertrophic cardiomyopathy with left ventricular outflow tract obstruction (off-label): Consideration may be given to disopyramide as an adjunct therapy for patients experiencing persistent symptoms due to left ventricular outflow tract obstruction, particularly if they have not responded adequately to beta-blockers or nondihydropyridine calcium channel blockers.[10] The combination of disopyramide with an atrioventricular blocking agent (eg, beta-blocker or nondihydropyridine calcium channel blocker) is advised to mitigate the risk of increased conduction through the atrioventricular node associated with disopyramide use. Additionally, the use of pyridostigmine can be considered to alleviate anticholinergic adverse effects, such as urinary retention, constipation, and dry mouth, that may arise from disopyramide administration.
Dosage Guidelines
For oral administration, the initial dose of the controlled-release formulation should be between 200 and 250 mg, administered twice daily. If symptomatic improvement is not observed, the dose may be titrated upwards by 100 mg/d at 2-week intervals, with a maximum daily dose of 600 mg divided into 2 doses.
Furthermore, in patients with hypertrophic cardiomyopathy, initiation of disopyramide in the outpatient setting is safe, and the subsequent risk of sudden cardiac death is low.[20]
Specific Patient Populations
Hepatic impairment: According to the manufacturer's labeling, for patients with moderate hepatic insufficiency, the recommended dosage is 400 mg/d in divided doses, either 100 mg every 6 hours for immediate-release disopyramide or 200 mg every 12 hours for disopyramide CR.
Renal impairment: According to the manufacturer's labeling, the following dosage adjustments are provided.
- Immediate release:
- CrCl >40 mL/minute: 100 mg every 6 hours
- CrCl 30 to 40 mL/minute: 100 mg every 8 hours
- CrCl 15 to 30 mL/minute: 100 mg every 12 hours
- CrCl <15 mL/minute: 100 mg every 24 hours
- Controlled release:
- CrCl >40 mL/minute: 200 mg every 12 hours
- CrCl ≤40 mL/minute: Not recommended for use
- Alternative recommendations for immediate release:
- CrCl >50 mL/minute: 100 to 200 mg every 8 hours
- CrCl 10 to 50 mL/minute: 100 to 200 mg every 12 to 24 hours
- CrCl <10 mL/minute: 100 to 200 mg every 24 to 48 hours
- Dialysis considerations: Not dialyzable (0% to 5%) by either hemodialysis or peritoneal methods; a supplemental dose is not necessary.
Pregnancy considerations: Disopyramide has been detected in human fetal circulation. The use of disopyramide in pregnant patients may provoke uterine contractions. A case report documented the emergence of painful uterine contractions following the initial dose during the third trimester, with subsequent dosing leading to hemorrhagic complications.[21][22][23]
Breastfeeding considerations: Disopyramide is excreted in breast milk. Given the risk of serious adverse effects in neonates, the manufacturer advises healthcare providers to weigh the benefits of continuing disopyramide therapy against the need to either halt breastfeeding or the medication, based on the significance of the treatment for the mother's condition. Disopyramide can be used with caution during breastfeeding if no other options are suitable.[15]
Pediatric patients: The use of disopyramide in pediatric patients is off-label; however, it may be prescribed with caution in certain clinical situations.[24] Controlled-release capsules should not be crushed, broken, or chewed and must be swallowed whole. The following recommendations pertain to the immediate-release dosing of disopyramide.
- Infants: 10 to 30 mg/kg/d in divided doses every 6 hours
- Children aged 1 to 4: 10 to 20 mg/kg/d in divided doses every 6 hours
- Children older than 4 to 12: 10 to 15 mg/kg/day in divided doses every 6 hours
- Children older than 12 and adolescents aged 18 or younger: 6 to 15 mg/kg/d in divided doses every 6 hours
Regarding its adverse effects, disopyramide should be initiated during in-hospital treatment.[25]
Older patients: Disopyramide was removed from the 2023 American Geriatrics Society Beers criteria due to low utilization in clinical practice. However, in the 2019 Beers criteria, its use in older adults was advised against due to its strong anticholinergic properties. Therefore, it should be avoided.[26][27]
Adverse Effects
The most serious adverse reactions identified include hypotension and congestive heart failure. Common adverse reactions, which may be dose-dependent, are linked to the drug's anticholinergic properties. Although these effects can be transitory, they may also persist or become severe.
- Anticholinergic: Urinary retention is a serious adverse effect associated with drugs that have anticholinergic properties, such as disopyramide. Anticholinergic reactions include xerostomia (32%), urinary hesitancy (14%), constipation (11%), and blurred vision, as well as dryness of the nose/eyes/throat. Accordingly, to circumvent disopyramide's anticholinergic effects, pyridostigmine could be used.[28]
- Genitourinary: Urinary retention, urinary frequency, and urgency
- Cardiovascular: Hypotension, congestive heart failure, cardiac conduction disorders, edema/weight gain, syncope, shortness of breath, chest pain, and long QT syndromes.[16]
- Gastrointestinal: Nausea, bloating, diarrhea, and vomiting.
- General: Fatigue, headache, malaise, pain, and anorexia.
- Dermatologic: Generalized rash or dermatoses and itching.
- Central nervous system: Nervousness and dizziness
- Frequency (<1%): Depression, insomnia, dysuria, increased cholesterol or triglycerides, numbness or tingling, elevated liver enzymes, atrioventricular block, elevated blood urea nitrogen, elevated creatinine, and decreased hemoglobin or hematocrit. Hypoglycemia has also been associated with disopyramide administration.
- Rare adverse events: Case reports have described adverse events such as agranulocytosis, cholestatic jaundice, malignant arrhythmia, and other electrocardiographic abnormalities.[29][30][31]
Drug-Drug Interactions
Disopyramide is primarily metabolized in the liver by cytochrome CYP3A4. The activity of this enzyme can be induced or inhibited by various substances; therefore, these substances should be avoided or used cautiously to prevent unpredictable modifications to disopyramide pharmacokinetics. Several known CYP3A4 inducers and inhibitors are listed below.[32]
- CYP3A4 inducers: These inducers increase disopyramide metabolism, thereby reducing its plasma half-life. Examples include rifampin, phenobarbital, and phenytoin.
- CYP3A4 inhibitors: These inducers decrease disopyramide metabolism, thereby increasing its plasma half-life. Examples include verapamil, diltiazem, ketoconazole, clarithromycin, erythromycin, protease inhibitors, and grapefruit juice. If any of these substances are used concurrently with disopyramide, monitoring disopyramide's plasma concentration is warranted to prevent adverse consequences.
-
Antiarrhythmic drugs: The combined use of disopyramide with other type 1A antiarrhythmic drugs, such as quinidine or procainamide, or type 1C antiarrhythmics, including encainide, flecainide, or propafenone, or propranolol, should be limited to patients with life-threatening arrhythmias who have not responded to single-drug antiarrhythmic treatment. Such use may cause serious negative inotropic effects or excessively prolonged conduction, particularly in patients with current or prior cardiac decompensation. Patients on more than 1 antiarrhythmic drug must be carefully monitored.
Contraindications
Several conditions contraindicate the use of disopyramide as an antiarrhythmic drug:[32][33]
- Disopyramide can cause or worsen congestive heart failure and may lead to severe hypotension due to its negative inotropic effects. Hypotension is mainly observed in patients with primary cardiomyopathy or those who have poorly compensated congestive heart failure. Disopyramide should not be used in patients with uncompensated or marginally compensated congestive heart failure or hypotension, unless these conditions are secondary to a cardiac arrhythmia.
- Long QT syndromes: Disopyramide and other class Ia antiarrhythmics can prolong the QT interval.[34]
- Second- or third-degree atrioventricular block without a pacemaker present; in a heart free from the influence of vagal tone, disopyramide can worsen the current atrioventricular conduction status.
- Hypersensitivity to the drugs themselves or their components.
Box Warnings
- The Cardiac Arrhythmia Suppression Trial, conducted by the National Heart, Lung, and Blood Institute, was a long-term, multi-center, randomized, double-blind study involving patients with asymptomatic, non–life-threatening ventricular arrhythmias. These patients had experienced a myocardial infarction more than 6 days but less than 2 years prior. The study revealed a concerning mortality rate and incidence of non-fatal cardiac arrests of 7.7% in those treated with encainide or flecainide, compared to just 3.0% in the carefully matched placebo group.[35] Participants in the trial received treatment with either encainide or flecainide for an average of 10 months. The same warning applies to disopyramide as a class 1 antiarrhythmic.
Warnings/Precautions
- Risk of medication error: Disopyramide may be confused with dipyridamole.
- Atrial tachyarrhythmias: Patients with atrial fibrillation or atrial flutter should be digitalized before disopyramide administration.[36] This precaution helps prevent drug-induced enhancement of atrioventricular conduction, which could otherwise result in a ventricular rate exceeding physiologically acceptable limits.
- Cardiac conduction system disorders: Caution is advised when prescribing disopyramide in Wolff-Parkinson-White syndrome, sick sinus syndrome, or bundle branch block. The impact of disopyramide on these conditions remains presently uncertain.
- Potassium abnormalities: Antiarrhythmic drugs may be ineffective in hypokalemia and more toxic in hyperkalemia. Correct potassium abnormalities before disopyramide therapy.[37][38]
- Cardiomyopathy: Patients with myocarditis or other cardiomyopathy may experience significant hypotension in response to the standard dose of disopyramide, likely due to cardiodepressant effects. Therefore, a loading dose of disopyramide should not be administered to such patients, and initial doses, as well as any future adjustments, should be made carefully under close supervision. For patients with hypertrophic cardiomyopathy who develop systolic dysfunction (left ventricular ejection fraction <50%), it is advisable to stop previously recommended negative inotropic agents such as disopyramide.[5]
Monitoring
Heart failure: Patients with a history of heart failure may be treated with disopyramide, but it is crucial to monitor cardiac function closely and ensure optimal digitalization. If hypotension develops or if congestive heart failure worsens, disopyramide should be discontinued. If necessary, it may be restarted at a lower dosage only after adequate cardiac compensation has been achieved.[39]
QRS widening: QRS widening is uncommon; however, a significant widening exceeding 25% of the QRS complex may occur during disopyramide administration. In such instances, discontinuation of disopyramide is recommended.
QTc prolongation: Disopyramide, such as other class 1A antiarrhythmics, may prolong the QTc interval and worsen arrhythmias, including ventricular tachycardia and fibrillation.[1] Disopyramide has been associated with torsade de pointes, particularly in patients with prior QT prolongation due to quinidine. If QT increases by more than 25% and ectopy persists, close monitoring is required, and treatment discontinuation should be considered.
Hypoglycemia: Significant hypoglycemia has been reported rarely with disopyramide. This risk is higher in patients with heart failure, malnutrition, liver or kidney disease, or those on drugs that impair glucose regulation. Blood glucose should be closely monitored in such cases.
Heart block management: In cases where a patient presents with first-degree heart block while on disopyramide therapy, it is advisable to reduce the dosage. Should the block remain despite dosage adjustment, the decision to continue the medication should be based on a careful evaluation of the therapeutic benefits relative to the potential risks associated with advancing to higher degrees of heart block.[37] The emergence of second- or third-degree atrioventricular block, as well as unifascicular, bifascicular, or trifascicular blocks, necessitates the discontinuation of disopyramide, unless there is adequate control of the ventricular rate through the implementation of a temporary or permanent ventricular pacemaker.
Myasthenia gravis: Disopyramide should be used with caution in patients with myasthenia gravis, as its anticholinergic properties may precipitate a myasthenic crisis.
Glaucoma: Disopyramide's anticholinergic action can increase intraocular pressure. Therefore, it should be avoided in patients with glaucoma unless pressure is medically controlled. Baseline intraocular pressure should be assessed in patients with a family history of glaucoma.[40]
Urinary retention: Due to its anticholinergic properties, disopyramide can impair bladder emptying. Caution is advised in patients at risk; males with benign prostatic hyperplasia are especially vulnerable.
Hepatic/renal impairment: In patients with severe renal dysfunction (renal clearance of <8 mL/min), disopyramide's half-life is prolonged, ranging from 14 to 43 hours.[41] In contrast, disopyramide's plasma half-life in healthy adults ranges from 6 to 8 hours.[42] Therefore, dose modification of the drug is warranted. This information is acquirable through the manufacturer's labeling. Moreover, in patients with hepatic impairment and heart failure, disopyramide's half-life is also increased.[30] Additionally, impairment of liver function can decrease alpha-1-acid-glycoprotein, a protein that binds disopyramide, resulting in increased free disopyramide concentrations.[43]
Toxicity
Signs and Symptoms of Overdose
The safe therapeutic disopyramide concentrations range from 2 to 5 mg/mL. Notably, in patients with cirrhosis, lower concentrations are preferable due to increased free form.[44] Toxic signs and symptoms of disopyramide typically occur when plasma concentrations exceed 7mg/mL.[45][46][47] Accidental or intentional overdose of oral disopyramide may lead to serious complications, including apnea, loss of consciousness, cardiac arrhythmias, and respiratory arrest. Fatal outcomes have been reported. Toxic plasma concentrations are associated with marked QRS and QTc prolongation, exacerbation of heart failure, hypotension, bradycardia, conduction abnormalities, and progression to asystole.
Management of Overdose
Due to its relatively small volume of distribution (Vd), low protein binding at toxic concentrations, and low intrinsic clearance, extracorporeal drug removal techniques (hemoperfusion or hemodialysis) can help remove disopyramide from the circulation in cases of intoxication.[48]
Generally, the initial priority is to decontaminate the patient's gastrointestinal system through lavage and repeat doses of oral activated charcoal. These effects are observed even when several hours have passed since the first ingestion, as it can significantly delay the absorption of class Ia antiarrhythmics. The patient should then be admitted to an intensive care unit for continuous electrocardiographic monitoring. Hemodialysis or hemoperfusion can be helpful if the patient has ingested large doses or has a high drug concentration, or in the setting of circulatory collapse or renal insufficiency. Symptomatic drugs should be given accordingly. For seizures, administration of benzodiazepines can be helpful. In hypotensive patients, fluid challenges and intravenous inotropic and vasopressor agents should be used. Mechanical supports, such as intra-aortic balloon pumps or cardiopulmonary bypass, should be considered in cases of refractory cardiogenic shock. Lastly, in the setting of arrhythmia, whether it is bradyarrhythmia or ventricular tachycardia (torsade de pointes), the appropriate medication should be given. Although based only on theoretical considerations, NaHCO3 (50 mmol) can be given intravenously and repeated every 5 to 10 minutes. The primary goal is to maintain an arterial pH of 7.4 to 7.5. The drug reversal mechanism is likely multifactorial, involving increases in blood pH, blood plasma sodium concentration, and a decrease in plasma potassium concentration.[30]
Enhancing Healthcare Team Outcomes
To enhance patient-centered care, outcomes, patient safety, and team performance related to disopyramide, it is essential for healthcare professionals, including clinicians, advanced practitioners, nurses, pharmacists, and other team members, to cultivate a diverse set of skills and strategies. Key competencies include strong clinical assessment skills to closely monitor patients for potential adverse effects and effective interprofessional communication to ensure coordinated care. Ethical considerations, such as respecting patient autonomy and adhering to the principles of beneficence and non-maleficence, are fundamental in fostering trust and ensuring that patients are informed about their treatment options.[49] Each member of the healthcare team has specific responsibilities, from medication management to patient education, which are critical in managing the complexities of disopyramide therapy. Regular interdisciplinary meetings, shared electronic health records, and clear documentation practices help strengthen care coordination, enabling a comprehensive approach to managing treatment and minimizing risks. The use of disopyramide is already approved by several clinical guidelines, including those of the Heart Rhythm Society, the American Heart Association, the American College of Cardiology, and the European Heart Rhythm Association (EHRA). Disopyramide is indicated as a third-line agent for the treatment of life-threatening arrhythmias (ventricular arrhythmias) and atrial fibrillation, especially sleep-induced or vagal-induced.[32][16][33] Disopyramide can also be used in hypertrophic obstructive cardiomyopathy in combination with beta-blockers.[9] Ultimately, a collaborative and patient-centric framework between clinicians, advanced practice providers, pharmacists, and nurses ensures that healthcare teams are equipped to provide high-quality care, improve outcomes, and maintain patient safety throughout the treatment process.
Media
(Click Image to Enlarge)
This image depict the molecular structure of disopyramide Contributed by Wikimedia User: Hengsheng120 (Public Domain)
(Click Image to Enlarge)
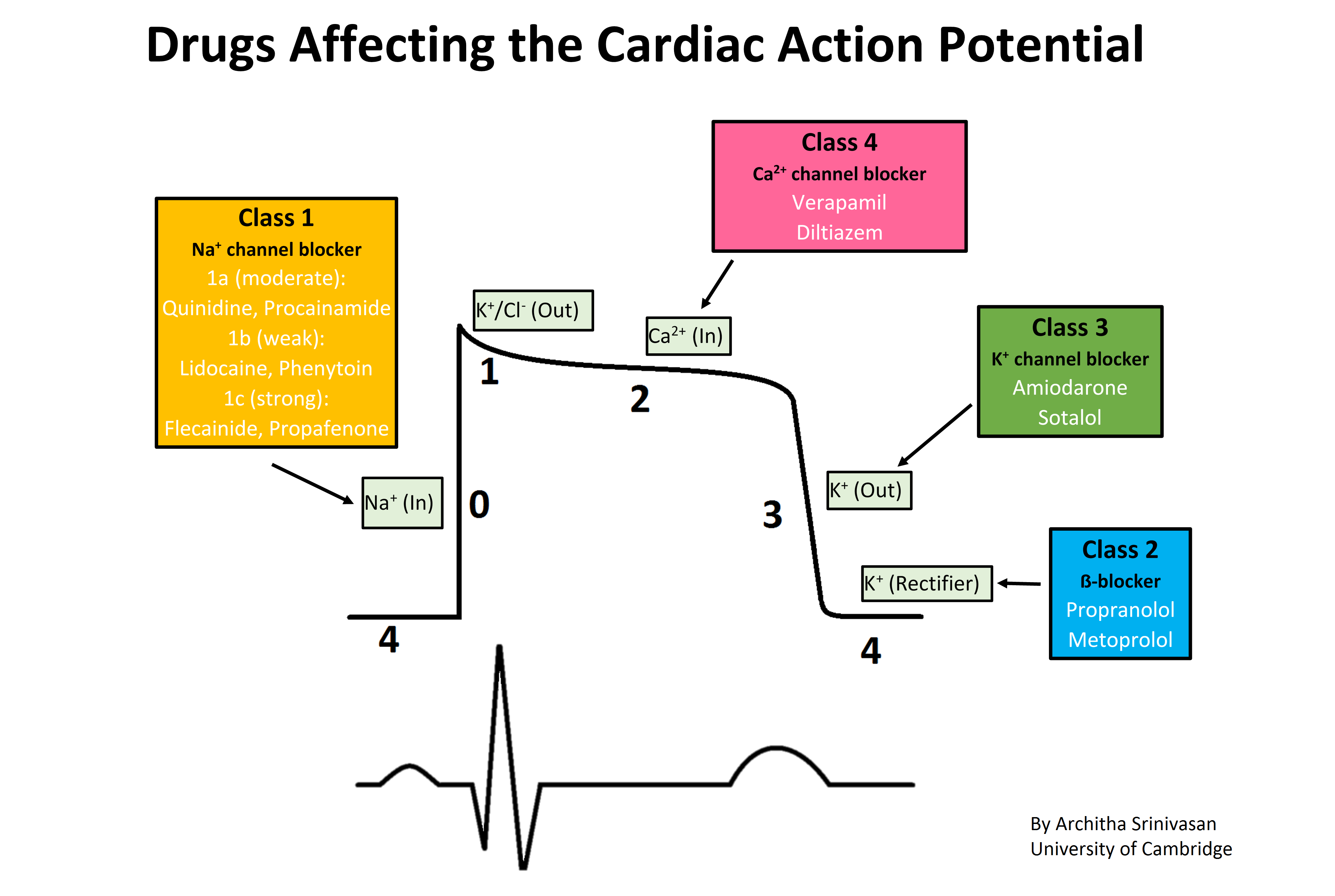
Drugs affecting the cardiac action potential. The sharp rise in voltage ("0") corresponds to the influx of sodium ions, whereas the two decays ("1" and "3", respectively) correspond to the sodium-channel inactivation and the repolarizing efflux of potassium ions. The characteristic plateau ("2") results from the opening of voltage-sensitive calcium channels. Contributed by Wikimedia User: Architha Srinivasan (CC BY-SA 4.0 https://creativecommons.org/licenses/by-sa/4.0/deed.en)
References
Al-Khatib SM, Stevenson WG, Ackerman MJ, Bryant WJ, Callans DJ, Curtis AB, Deal BJ, Dickfeld T, Field ME, Fonarow GC, Gillis AM, Granger CB, Hammill SC, Hlatky MA, Joglar JA, Kay GN, Matlock DD, Myerburg RJ, Page RL. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2018 Sep 25:138(13):e272-e391. doi: 10.1161/CIR.0000000000000549. Epub [PubMed PMID: 29084731]
Level 1 (high-level) evidenceShaikh F, Wynne R, Castelino RL, Davidson PM, Inglis SC, Ferguson C. Effect of Obesity on the Use of Antiarrhythmics in Adults With Atrial Fibrillation: A Narrative Review. Clinical cardiology. 2024 Aug:47(8):e24336. doi: 10.1002/clc.24336. Epub [PubMed PMID: 39169682]
Level 3 (low-level) evidenceKarlson BW, Torstensson I, Abjörn C, Jansson SO, Peterson LE. Disopyramide in the maintenance of sinus rhythm after electroconversion of atrial fibrillation. A placebo-controlled one-year follow-up study. European heart journal. 1988 Mar:9(3):284-90 [PubMed PMID: 3289932]
Level 1 (high-level) evidenceOmmen SR, Ho CY, Asif IM, Balaji S, Burke MA, Day SM, Dearani JA, Epps KC, Evanovich L, Ferrari VA, Joglar JA, Khan SS, Kim JJ, Kittleson MM, Krittanawong C, Martinez MW, Mital S, Naidu SS, Saberi S, Semsarian C, Times S, Waldman CB, Peer Review Committee Members. 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for the Management of Hypertrophic Cardiomyopathy: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2024 Jun 4:149(23):e1239-e1311. doi: 10.1161/CIR.0000000000001250. Epub 2024 May 8 [PubMed PMID: 38718139]
Level 1 (high-level) evidenceWriting Committee Members, Ommen SR, Ho CY, Asif IM, Balaji S, Burke MA, Day SM, Dearani JA, Epps KC, Evanovich L, Ferrari VA, Joglar JA, Khan SS, Kim JJ, Kittleson MM, Krittanawong C, Martinez MW, Mital S, Naidu SS, Saberi S, Semsarian C, Times S, Waldman CB. 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for the Management of Hypertrophic Cardiomyopathy: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Journal of the American College of Cardiology. 2024 Jun 11:83(23):2324-2405. doi: 10.1016/j.jacc.2024.02.014. Epub 2024 May 8 [PubMed PMID: 38727647]
Level 1 (high-level) evidenceDicorato MM, Citarelli G, Mangini F, Alemanni R, Albanese M, Cicco S, Greco CA, Forleo C, Basile P, Carella MC, Ciccone MM, Guaricci AI, Dentamaro I. Integrative Approaches in the Management of Hypertrophic Cardiomyopathy: A Comprehensive Review of Current Therapeutic Modalities. Biomedicines. 2025 May 21:13(5):. doi: 10.3390/biomedicines13051256. Epub 2025 May 21 [PubMed PMID: 40427081]
Güler A, Erata YE, Demirtola Aİ, Türkmen İ, Atmaca S, Şahin H, Aydın S, Almasri M, Tekin M, Coşkun G, Uygur B, Cansever AT, Güler GB. The effect of disopyramide therapy on functional capacity improvement in patients with obstructive hypertrophic cardiomyopathy. International journal of cardiology. 2025 Feb 15:421():132913. doi: 10.1016/j.ijcard.2024.132913. Epub 2024 Dec 18 [PubMed PMID: 39706304]
Mehra N, Ali AH, Desai MY. Obstructive hypertrophic cardiomyopathy: a review of new therapies. Future cardiology. 2023 Oct:19(13):661-670. doi: 10.2217/fca-2023-0056. Epub 2023 Nov 7 [PubMed PMID: 37933625]
Sherrid MV, Barac I, McKenna WJ, Elliott PM, Dickie S, Chojnowska L, Casey S, Maron BJ. Multicenter study of the efficacy and safety of disopyramide in obstructive hypertrophic cardiomyopathy. Journal of the American College of Cardiology. 2005 Apr 19:45(8):1251-8 [PubMed PMID: 15837258]
Level 2 (mid-level) evidenceSherrid MV, Massera D. Disopyramide for symptomatic obstructive hypertrophic cardiomyopathy. International journal of cardiology. 2025 Mar 15:423():133030. doi: 10.1016/j.ijcard.2025.133030. Epub 2025 Feb 1 [PubMed PMID: 39900191]
Awad K, Pereyra Pietri M, Farina JM, Pathangey G, Abbas MT, Scalia IG, Le Couteur D, Wilanksy S, Lester SJ, Ommen SR, Geske JB, Arsanjani R, Ayoub C. Efficacy of pharmacological therapies in reducing outflow tract obstruction in patients with obstructive hypertrophic cardiomyopathy: a systematic review and meta-analysis. European heart journal. Cardiovascular pharmacotherapy. 2025 Aug 12:11(5):469-482. doi: 10.1093/ehjcvp/pvaf036. Epub [PubMed PMID: 40377024]
Level 1 (high-level) evidenceKus T, Sasyniuk BI. Electrophysiological actions of disopyramide phosphate on canine ventricular muscle and purkinje fibers. Circulation research. 1975 Dec:37(6):844-54 [PubMed PMID: 1192576]
Level 3 (low-level) evidenceIrie M, Hiiro H, Kato S, Kuramochi M, Hamaguchi S, Namekata I, Tanaka H. Differential effects of class I antiarrhythmic drugs on the guinea pig pulmonary vein myocardium: Inhibition of automatic activity correlates with blockade of a diastolic sodium current component. Journal of pharmacological sciences. 2020 Aug:143(4):325-329. doi: 10.1016/j.jphs.2020.05.004. Epub 2020 May 16 [PubMed PMID: 32487451]
Kotake H, Hasegawa J, Hata T, Mashiba H. Electrophysiological effect of disopyramide on rabbit sinus node cells. Journal of electrocardiology. 1985 Oct:18(4):377-83 [PubMed PMID: 2415649]
Disopyramide,,, 2006 [PubMed PMID: 30000949]
Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, Kirchhof P, Kjeldsen K, Kuck KH, Hernandez-Madrid A, Nikolaou N, Norekvål TM, Spaulding C, Van Veldhuisen DJ, ESC Scientific Document Group. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). European heart journal. 2015 Nov 1:36(41):2793-2867. doi: 10.1093/eurheartj/ehv316. Epub 2015 Aug 29 [PubMed PMID: 26320108]
Li S, Xu Z, Guo M, Li M, Wen Z. Drug-induced QT Prolongation Atlas (DIQTA) for enhancing cardiotoxicity management. Drug discovery today. 2022 Mar:27(3):831-837. doi: 10.1016/j.drudis.2021.10.009. Epub 2021 Oct 27 [PubMed PMID: 34718206]
Mehvar R, Brocks DR, Vakily M. Impact of stereoselectivity on the pharmacokinetics and pharmacodynamics of antiarrhythmic drugs. Clinical pharmacokinetics. 2002:41(8):533-58 [PubMed PMID: 12102640]
Chiba K, Koike K, Nakamoto M, Echizen H, Ishizawa A, Ishizaki T. Steady-state pharmacokinetics and bioavailability of total and unbound disopyramide in children with cardiac arrhythmias. Therapeutic drug monitoring. 1992 Apr:14(2):112-8 [PubMed PMID: 1585394]
Adler A, Fourey D, Weissler-Snir A, Hindieh W, Chan RH, Gollob MH, Rakowski H. Safety of Outpatient Initiation of Disopyramide for Obstructive Hypertrophic Cardiomyopathy Patients. Journal of the American Heart Association. 2017 May 26:6(6):. doi: 10.1161/JAHA.116.005152. Epub 2017 May 26 [PubMed PMID: 28550094]
Abbi M, Kriplani A, Singh B. Preterm labor and accidental hemorrhage after disopyramide therapy in pregnancy. A case report. The Journal of reproductive medicine. 1999 Jul:44(7):653-5 [PubMed PMID: 10442335]
Level 3 (low-level) evidenceDeFilippis EM, Haythe JH, Walsh MN, Kittleson MM. Intersection of Heart Failure and Pregnancy: Beyond Peripartum Cardiomyopathy. Circulation. Heart failure. 2021 May:14(5):e008223. doi: 10.1161/CIRCHEARTFAILURE.120.008223. Epub 2021 May 13 [PubMed PMID: 33980039]
Halpern DG, Weinberg CR, Pinnelas R, Mehta-Lee S, Economy KE, Valente AM. Use of Medication for Cardiovascular Disease During Pregnancy: JACC State-of-the-Art Review. Journal of the American College of Cardiology. 2019 Feb 5:73(4):457-476. doi: 10.1016/j.jacc.2018.10.075. Epub [PubMed PMID: 30704579]
Del Vecchio K, Rizzardi C, Pozza A, Prati F, Ye L, Fattoretto A, Reffo E, Di Salvo G. How effective is disopyramide in treating pediatric hypertrophic cardiomyopathy? State of the art and future directions. Monaldi archives for chest disease = Archivio Monaldi per le malattie del torace. 2024 Sep 19:94(3):. doi: 10.4081/monaldi.2024.3084. Epub 2024 Sep 19 [PubMed PMID: 39297578]
Level 3 (low-level) evidenceEchizen H, Takahashi H, Nakamura H, Ochiai K, Chiba K, Koike K, Ogata H, Ishizaki T. Stereoselective disposition and metabolism of disopyramide in pediatric patients. The Journal of pharmacology and experimental therapeutics. 1991 Dec:259(3):953-60 [PubMed PMID: 1762088]
By the 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. Journal of the American Geriatrics Society. 2019 Apr:67(4):674-694. doi: 10.1111/jgs.15767. Epub 2019 Jan 29 [PubMed PMID: 30693946]
By the 2023 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. Journal of the American Geriatrics Society. 2023 Jul:71(7):2052-2081. doi: 10.1111/jgs.18372. Epub 2023 May 4 [PubMed PMID: 37139824]
Sherrid MV, Arabadjian M. A primer of disopyramide treatment of obstructive hypertrophic cardiomyopathy. Progress in cardiovascular diseases. 2012 May-Jun:54(6):483-92. doi: 10.1016/j.pcad.2012.04.003. Epub [PubMed PMID: 22687589]
Conrad ME, Cumbie WG, Thrasher DR, Carpenter JT. Agranulocytosis associated with disopyramide therapy. JAMA. 1978 Oct 20:240(17):1857-8 [PubMed PMID: 691193]
Level 3 (low-level) evidenceKim SY, Benowitz NL. Poisoning due to class IA antiarrhythmic drugs. Quinidine, procainamide and disopyramide. Drug safety. 1990 Nov-Dec:5(6):393-420 [PubMed PMID: 2285495]
Level 3 (low-level) evidenceEdmonds ME, Hayler AM. A case of intra-hepatic cholestasis after disopyramide therapy. European journal of clinical pharmacology. 1980 Oct:18(3):285-6 [PubMed PMID: 7439249]
Level 3 (low-level) evidenceJanuary CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW, American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Journal of the American College of Cardiology. 2014 Dec 2:64(21):e1-76. doi: 10.1016/j.jacc.2014.03.022. Epub 2014 Mar 28 [PubMed PMID: 24685669]
Level 1 (high-level) evidenceKirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P, Agewall S, Camm J, Baron Esquivias G, Budts W, Carerj S, Casselman F, Coca A, De Caterina R, Deftereos S, Dobrev D, Ferro JM, Filippatos G, Fitzsimons D, Gorenek B, Guenoun M, Hohnloser SH, Kolh P, Lip GY, Manolis A, McMurray J, Ponikowski P, Rosenhek R, Ruschitzka F, Savelieva I, Sharma S, Suwalski P, Tamargo JL, Taylor CJ, Van Gelder IC, Voors AA, Windecker S, Zamorano JL, Zeppenfeld K. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2016 Nov:18(11):1609-1678 [PubMed PMID: 27567465]
Asajima H, Saito N, Ohmura Y, Ohmura K. Lansoprazole precipitated QT prolongation and torsade de pointes associated with disopyramide. European journal of clinical pharmacology. 2012 Mar:68(3):331-3. doi: 10.1007/s00228-011-1119-z. Epub 2011 Sep 7 [PubMed PMID: 21898101]
Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, Barker AH, Arensberg D, Baker A, Friedman L, Greene HL. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial. The New England journal of medicine. 1991 Mar 21:324(12):781-8 [PubMed PMID: 1900101]
Level 1 (high-level) evidenceGarcía-Barreto D, Groning E, González-Gómez A, Pérez A, Hernández-Cañero A, Toruncha A. Enhancement of the antiarrhythmic action of disopyramide by digoxin. Journal of cardiovascular pharmacology. 1981 Nov-Dec:3(6):1236-42 [PubMed PMID: 6173523]
Zhang Y, El Harchi A, James AF, Oiki S, Dempsey CE, Hancox JC. Stereoselective block of the hERG potassium channel by the Class Ia antiarrhythmic drug disopyramide. Cellular and molecular life sciences : CMLS. 2024 Nov 28:81(1):466. doi: 10.1007/s00018-024-05498-4. Epub 2024 Nov 28 [PubMed PMID: 39607488]
Maddux BD, Whiting RB. Toxic synergism of disopyramide and hyperkalemia. Chest. 1980 Oct:78(4):654-6 [PubMed PMID: 7418494]
Argirò A, Zampieri M, Marchi A, Del Franco A, Pàlinkàs ED, Biagioni G, Chiti C, Mazzoni C, Fornaro A, Targetti M, Cappelli F, Olivotto I. [Therapeutic approaches in hypertrophic cardiomyopathy: from symptom relief to precision therapy]. Giornale italiano di cardiologia (2006). 2023 Oct:24(10):792-799. doi: 10.1714/4100.40979. Epub [PubMed PMID: 37767831]
January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW, ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014 Dec 2:130(23):e199-267. doi: 10.1161/CIR.0000000000000041. Epub 2014 Mar 28 [PubMed PMID: 24682347]
Level 1 (high-level) evidenceWhiting B, Elliott HL. Disopyramide in renal impairment. Lancet (London, England). 1977 Dec 24-31:2(8052-8053):1363 [PubMed PMID: 74774]
Level 3 (low-level) evidenceBryson SM, Whiting B, Lawrence JR. Disopyramide serum and pharmacologic effect kinetics applied to the assessment of bioavailability. British journal of clinical pharmacology. 1978 Nov:6(5):409-19 [PubMed PMID: 728284]
Level 1 (high-level) evidenceBonde J, Graudal NA, Pedersen LE, Balsløv S, Angelo HR, Svendsen TL, Kampmann JP. Kinetics of disopyramide in decreased hepatic function. European journal of clinical pharmacology. 1986:31(1):73-7 [PubMed PMID: 3780831]
Echizen H, Saima S, Umeda N, Ishizaki T. Protein binding of disopyramide in liver cirrhosis and in nephrotic syndrome. Clinical pharmacology and therapeutics. 1986 Sep:40(3):274-80 [PubMed PMID: 3742934]
Gosselin B, Mathieu D, Chopin C, Wattel F, Dupuis B, Haguenoer JM, Desprez M. Acute intoxication with diisopyramide: clinical and experimental study by hemoperfusion an Amberlite XAD 4 resin. Clinical toxicology. 1980 Oct:17(3):439-49 [PubMed PMID: 7449357]
Level 3 (low-level) evidenceHayler AM, Holt DW, Volans GN. Fatal overdosage with disopyramide. Lancet (London, England). 1978 May 6:1(8071):968-9 [PubMed PMID: 76895]
Level 3 (low-level) evidenceSathyavagiswaran L. Fatal disopyramide intoxication from suicidal/accidental overdose. Journal of forensic sciences. 1987 Nov:32(6):1813-8 [PubMed PMID: 3323413]
Level 3 (low-level) evidenceHinderling PH, Garrett ER. Pharmacokinetics of the antiarrhythmic disopyramide in healthy humans. Journal of pharmacokinetics and biopharmaceutics. 1976 Jun:4(3):199-230 [PubMed PMID: 978389]
Cirillo C, Perillo A, Monda E, Palmiero G, Verrillo F, Rubino M, Diana G, Dongiglio F, Caiazza M, Cirillo A, Fusco A, Fumagalli C, Bossone E, Russo MG, Calabro P, Limongelli G. Treatment options for hypertrophic obstructive cardiomyopathy: a patient-centric review. Expert review of cardiovascular therapy. 2024 Nov:22(11):625-637. doi: 10.1080/14779072.2024.2436659. Epub 2024 Dec 5 [PubMed PMID: 39633307]