Introduction
Diffuse intrinsic pontine glioma (DIPG) remains one of the most devastating diagnoses in the field of pediatric neurooncology. Arising within the pons, DIPG is a highly aggressive, infiltrative tumor that primarily affects children between the ages of 5 and 10.[1] Despite decades of research, the prognosis remains poor, with a median survival of less than 1 year from the time of diagnosis.[2] The deep anatomic tumor location, diffuse infiltration into vital brainstem structures, and the resistance to conventional therapies collectively contribute to its formidable clinical challenge. Initially described as a distinct clinicopathologic entity in the mid-twentieth century, DIPG is now recognized as a biologically and molecularly unique tumor subgroup within the spectrum of pediatric high-grade gliomas. In the 2021 World Health Organization (WHO) update on central nervous system tumors, DIPGs are classified as diffuse midline glioma, H3K27M mutant, highlighting their characteristic epigenetic dysregulation rather than their purely anatomic location.[3]
Clinically, DIPGs present insidiously with the triad of rapidly evolving cranial nerve deficits, long tract signs, and ataxia that reflect their intrinsic involvement of pontine nuclei and adjacent fiber tracts. Magnetic resonance imaging (MRI) typically demonstrates an expanded, T2-hyperintense lesion centered in the pons with indistinct margins and minimal contrast enhancement. The mainstay of treatment is fractionated radiotherapy, which offers only transient symptom relief and minimal survival benefit. Emerging research has demonstrated the efficacy of dordaviprone, formerly known as ONC201, a dopamine receptor antagonist, in treating DIPG beyond conventional radiotherapy.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of DIPG is multifactorial, encompassing aberrant neurodevelopmental processes, distinct molecular alterations, and the unique cellular microenvironment of the pediatric brainstem. Unlike adult high-grade gliomas, which are often linked to acquired genetic instability and environmental carcinogenesis, DIPG arises during normal brain development, implicating disruptions in developmental signaling pathways and epigenetic regulation as the primary drivers of tumorigenesis. DIPG arises within the ventral pons, a region undergoing active neuronal differentiation and myelination during early childhood, at the same age that the disease most commonly presents. This spatial and temporal coincidence supports the concept that DIPG originates from neural progenitor or oligodendrocyte precursor cells (OPCs) intrinsic to the developing brainstem.[5][6][7] Transcriptomic analyses support OPC-like signatures in DIPG tumors, further reinforcing their developmental cellular origin.[8]
To date, no environmental or hereditary risk factors have been definitively associated with DIPG development. The tumor is not linked to prior radiation exposure, chemical carcinogens, or familial cancer predisposition syndromes such as Li-Fraumeni or neurofibromatosis.[9] This absence of known external factors suggests that DIPG arises primarily from intrinsic developmental and molecular perturbations within the brainstem.
Epidemiology
Brainstem gliomas affect approximately 300 children in the United States each year and are the major cause of death in children with brain tumors.[10][11] The most common of these is the DIPG, comprising 80% of the fatal cases. The incidence is 1 to 2 cases per 100,000 population. DIPG has a peak incidence of 6 to 9 years of age and a slight preference for males.[1][12]
Pathophysiology
The defining etiologic event in approximately 80% of DIPGs is a mutation in the histone H3 genes, specifically a lysine-to-methionine substitution at position 27 (K27M) in H3F3A (H3.3) or HIST1H3B/C (H3.1).[13][14] This mutation disrupts the enzymatic activity of the polycomb repressive complex 2, resulting in a global loss of trimethylation of histone H3 at lysine 27 (H3K27me3) and extensive epigenetic reprogramming.[15][16][17] The resultant chromatin landscape promotes transcriptional activation of normally repressed developmental genes, maintaining cells in an undifferentiated, proliferative state.[18]
Results from several studies have shown the cooccurrence of mutations in activin receptor type 1 (ACVR1) and phosphoinositide 3-kinase (PI3K) in H3.1K27M mutant tumors.[19][20][21][22] In H3.3K27M mutant tumors, mutations in the tumor suppressor 53 and platelet-derived growth factor alpha are present.[19][20] These pathways converge on dysregulated cell-cycle control, enhanced growth-factor signaling, and evasion of apoptosis. The cooperative effects of these genetic and epigenetic alterations define the core molecular landscape of DIPG. The pontine microenvironment also plays a crucial etiologic role. The pons possesses dense axonal tracts, relatively low immune surveillance, and a tightly regulated blood–brain barrier, all of which contribute to DIPG’s infiltrative nature and therapeutic resistance.[23][24] Interactions between tumor cells, astrocytes, and microglia generate a protumorigenic environment characterized by immunosuppression and paracrine support of tumor growth.
History and Physical
The clinical course for children with DIPG typically progresses rapidly. Most symptoms develop 4 weeks before seeking medical attention. Due to the tumor's intrinsic nature, symptoms result from dysfunction of pontine neural structures, including long tracts and cranial nerve nuclei. Diplopia is often the first sign to present and is due to an abducens nerve palsy.
Dysfunction of the facial nucleus will result in facial weakness or paralysis. Long-tract signs can produce motor weakness and hyperreflexia, while dysfunction of the cerebellopontine connections will result in ataxia, dysmetria, and dysarthria. The classic triad of long-tract signs, cerebellar dysfunction, and cranial nerve palsies is present in approximately 50% of patients.[25][26] Hydrocephalus occurs in less than 10% of cases, but if left untreated, it can progress to coma and death.[27]
Evaluation
An MRI of the brain, with and without contrast, is the most useful diagnostic study for evaluating a patient with suspected DIPG (see Image. Diffuse Intrinsic Pontine Glioma, Magnetic Resonance Image [MRI]).[28] These tumors are expansile lesions centered within the pons and are hypointense on T1-weighted images and hyperintense on T2-weighted images.[29][30][31] Hemorrhage and edema are uncommon radiographic findings, and some degree of contrast enhancement can be seen in nearly 70% of cases, most often in a patchy pattern.[30] Restricted diffusion can occasionally be seen, although usually to a mild degree.[32] Higher values of the apparent diffuse coefficient derived from diffusion-weighted MRI images correlate with a better median survival.[33][30] MRIs of the entire spinal axis are typically recommended to exclude drop metastases.[34]
In recent years, research has focused on the efficacy of liquid biopsies.[35][36] Suppose patients do not have evidence of hydrocephalus. In that case, a lumbar puncture can be performed to obtain cerebrospinal fluid for analysis to detect tumor cells and circulating tumor DNA harboring the H3K27 mutation.[37][38][39][40]
Although many DIPGs can be diagnosed based on classic imaging features and clinical presentation, some cases with atypical imaging findings may require biopsy to obtain a tissue diagnosis.[41] Furthermore, biopsies enable patient enrollment in clinical trials in which tissue is used to identify molecular and genetic derangements, thereby enabling targeted therapy. While historically deferred because of the tumor location in the brainstem, stereotactic biopsies are now commonly performed in many highly specialized pediatric medical centers.[42][43][44] A study comparing microsurgical biopsies with frameless robotic-assisted stereotactic biopsies showed shorter operative time, a shorter postoperative intensive care unit stay, a lower rate of neurological impairment, and lower overall cost in patients undergoing stereotactic biopsies.[45] Several other studies have shown that stereotactic biopsies are safe and efficacious, with diagnostic yields of 90% to 100%.[46][47][48][49]
Treatment / Management
Corticosteroids, specifically dexamethasone, are often administered after diagnosis and during radiation therapy. Complications due to long-term use should be avoided; therefore, they should be tapered as quickly as tolerated by the patient.[50][51] Steroids stabilize the blood-brain barrier and can affect tissue penetration of systemic drug therapies.[52] Over the course of the disease, less than 10% of patients diagnosed with DIPGs will develop hydrocephalus, although it has been reported that up to 55% of patients can have ventriculomegaly.[53] In cases of hydrocephalus, cerebrospinal fluid diversion by ventriculoperitoneal shunting or endoscopic third ventriculostomy is often required.[53][54](A1)
Conventionally fractionated radiotherapy remains the standard of care for children with DIPGs, although hypofractionated radiotherapy has shown promising results when compared to conventional radiotherapy.[55][56][57] Radiotherapy is usually delivered at a total dose of 54 Gy over 6 weeks (1.8-Gy daily fractions). Hypofractionated radiation to a total dose of 39 Gy has similar outcomes and is better tolerated in young children.[58][59] Reirradiation for tumor progression can be considered, with mild symptoms and survival benefits.[60][61][62][63][64] Results from recent studies have shown the efficacy of Dordaviprone, a dopamine receptor antagonist, in the treatment of recurrent H3K27M-mutant diffuse midline gliomas.[4][65][66][67] This drug is now approved by the United States Food and Drug Administration for patients 1 year or older with H3K27M-mutant diffuse midline gliomas with progressive disease following prior treatment.(A1)
Other novel therapies are being studied and include those listed below.[68][69]
- Oncolytic viruses [70][71]
- Chimeric antigen receptor T-cell therapy [72][73][74][75]
- Convection-enhanced drug delivery systems [76][77][78]
- Focused ultrasound [79][80] (A1)
Phase 1/2 trials of the oral histone deacetylase inhibitor, vorinostat, have also been recently published.[81][82]
Differential Diagnosis
The differential diagnoses for DPIGs include:
- Midbrain gliomas
- Cervicomedullary glioma
- Pilocytic astrocytoma
- Cavernous malformation
- Demyelinating disease
- Infectious diseases
Prognosis
The prognosis of DPIG is poor due to the absence of effective therapies. This tumor is the primary cause of death among brain tumors in children. In a report from international registries, the median survival time was 11 months among 1008 patients. Long-term survivors living for more than 2 years were more commonly found to present at ages younger than 3 and older than 10, and had longer symptom duration.[2] Similar results were observed among 1183 patients, including children diagnosed before age 3, who demonstrated improved overall survival.[83] Other negative prognostic factors include extrapontine extension, contrast enhancement, larger size, necrosis, and metastatic disease.[30][84]
Complications
In a systematic review of 192 stereotactic biopsies, complications were reported in 13% of patients, with cranial neuropathies being the most prevalent at 4.2%. Perioperative hemorrhage (3.6%), hemiparesis (2.1%), and speech disturbances (1.6%) were also reported.[47]
Consultations
The following consultations will likely be needed in patients with DPIGs:
- Neurooncology
- Radiation oncology
- Neuroradiology
- Neurosurgery
- Neurology
- Neuropathology
- Pediatric intensive care
Early consideration should be given to consulting advanced pediatric care or pediatric palliative care specialists. Offering palliative care services to all patients with DIPG early in the course of the disease provides support for the immediate and ongoing physical, psychological, and social effects that this lethal disease will have on the patient and the family. Combined neurooncologic and palliative care support will influence how patients and their families function during treatment and can even help identify disease-related changes before clinically or radiographically suspected progression.[85]
Deterrence and Patient Education
Deterrence in DIPG is limited because the disease stems from non-modifiable molecular changes within the brainstem, leaving no viable preventive strategies or modifiable risk factors. As a result, the clinical focus centers on early recognition of progressive neurologic symptoms—such as cranial nerve palsies, gait instability, dysphagia, or rapid functional decline—to ensure timely imaging, diagnosis, and initiation of symptom-directed management. Patient and family education, therefore, becomes essential in optimizing outcomes and supporting informed decision-making. Families must receive clear, compassionate explanations of the disease process, prognosis, expected treatment responses, and the realistic limitations of radiation, corticosteroids, and clinical trial therapies. The timeline of diagnosis significantly influences how families emotionally process the situation, underscoring the importance of involving psychologists, psychiatrists, and family therapists in comprehensive care.
Education should also prepare caregivers for the functional changes that accompany disease progression and treatment. This includes understanding the development of neurologic deficits and physical impairments, and learning practical skills required for home-based care, such as nasogastric feeding, Foley catheter management, prevention of sacral decubitus ulcers, and the challenges associated with becoming bedridden. Thorough instruction on these aspects empowers families, enhances safety, and reduces preventable complications. By integrating early recognition, realistic education, psychosocial support, and hands-on caregiver training, clinicians can improve patient-centered care, support families through the trajectory of DIPG, and maintain dignity and comfort throughout the disease course.
Enhancing Healthcare Team Outcomes
Interprofessional management of DIPG requires highly coordinated, patient-centered collaboration due to the tumor’s aggressive biology, limited therapeutic options, and the profound emotional and functional impact on patients and families. Physicians and advanced practitioners lead diagnostic clarification, communicate prognosis with clarity and compassion, and coordinate multimodal therapies such as radiation, targeted agents in clinical trials, and symptom-directed care. Nurses provide continuous assessment of neurologic function, manage treatment-related toxicities, and reinforce education to families, ensuring early recognition of complications. Pharmacists optimize dosing, review potential toxicities, and monitor interactions between chemotherapy, targeted therapies, corticosteroids, and supportive medications—critical for maintaining safety in a population highly vulnerable to adverse events. Rehabilitation specialists, social workers, child-life experts, and palliative care teams contribute essential support by addressing functional decline, cognitive changes, psychosocial stressors, and quality-of-life priorities.
Effective team strategy relies on structured communication—such as tumor board reviews, daily care huddles, and unified care plans—to align goals, anticipate complications, and ensure seamless transitions between outpatient, inpatient, and home-based care. Clear documentation of steroid weaning plans, neuroprotective strategies, and management of symptoms such as dysphagia, cranial nerve deficits, and airway compromise enhances safety and reduces variability. The team prioritizes shared decision-making with families, highlighting realistic outcomes, integrating palliative principles early, and offering access to clinical trials when appropriate. By synchronizing roles and maintaining open, anticipatory communication, the interprofessional team enhances patient safety, supports families through complex decisions, and maximizes functional outcomes and quality of life despite the disease’s poor prognosis.
Media
(Click Image to Enlarge)
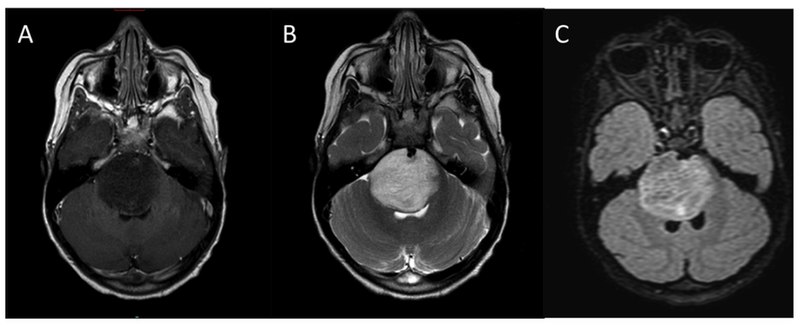
Diffuse Intrinsic Pontine Glioma, Magnetic Resonance Image (MRI). This image shows the typical MRI appearance of diffuse intrinsic pontine glioma: (A) T1-weighted postcontrast, (B) T2-weighted, (C) Fluid-attenuated inversion recovery.
Warren KE. Diffuse intrinsic pontine glioma: poised for progress. Front Oncol. 2012;2:205. doi: 10.3389/fonc.2012.00205.
References
Panditharatna E, Yaeger K, Kilburn LB, Packer RJ, Nazarian J. Clinicopathology of diffuse intrinsic pontine glioma and its redefined genomic and epigenomic landscape. Cancer genetics. 2015 Jul-Aug:208(7-8):367-73. doi: 10.1016/j.cancergen.2015.04.008. Epub 2015 May 1 [PubMed PMID: 26206682]
Hoffman LM, Veldhuijzen van Zanten SEM, Colditz N, Baugh J, Chaney B, Hoffmann M, Lane A, Fuller C, Miles L, Hawkins C, Bartels U, Bouffet E, Goldman S, Leary S, Foreman NK, Packer R, Warren KE, Broniscer A, Kieran MW, Minturn J, Comito M, Broxson E, Shih CS, Khatua S, Chintagumpala M, Carret AS, Escorza NY, Hassall T, Ziegler DS, Gottardo N, Dholaria H, Doughman R, Benesch M, Drissi R, Nazarian J, Jabado N, Boddaert N, Varlet P, Giraud G, Castel D, Puget S, Jones C, Hulleman E, Modena P, Giagnacovo M, Antonelli M, Pietsch T, Gielen GH, Jones DTW, Sturm D, Pfister SM, Gerber NU, Grotzer MA, Pfaff E, von Bueren AO, Hargrave D, Solanki GA, Jadrijevic Cvrlje F, Kaspers GJL, Vandertop WP, Grill J, Bailey S, Biassoni V, Massimino M, Calmon R, Sanchez E, Bison B, Warmuth-Metz M, Leach J, Jones B, van Vuurden DG, Kramm CM, Fouladi M. Clinical, Radiologic, Pathologic, and Molecular Characteristics of Long-Term Survivors of Diffuse Intrinsic Pontine Glioma (DIPG): A Collaborative Report From the International and European Society for Pediatric Oncology DIPG Registries. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2018 Jul 1:36(19):1963-1972. doi: 10.1200/JCO.2017.75.9308. Epub 2018 May 10 [PubMed PMID: 29746225]
Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, Hawkins C, Ng HK, Pfister SM, Reifenberger G, Soffietti R, von Deimling A, Ellison DW. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro-oncology. 2021 Aug 2:23(8):1231-1251. doi: 10.1093/neuonc/noab106. Epub [PubMed PMID: 34185076]
Venneti S, Kawakibi AR, Ji S, Waszak SM, Sweha SR, Mota M, Pun M, Deogharkar A, Chung C, Tarapore RS, Ramage S, Chi A, Wen PY, Arrillaga-Romany I, Batchelor TT, Butowski NA, Sumrall A, Shonka N, Harrison RA, de Groot J, Mehta M, Hall MD, Daghistani D, Cloughesy TF, Ellingson BM, Beccaria K, Varlet P, Kim MM, Umemura Y, Garton H, Franson A, Schwartz J, Jain R, Kachman M, Baum H, Burant CF, Mottl SL, Cartaxo RT, John V, Messinger D, Qin T, Peterson E, Sajjakulnukit P, Ravi K, Waugh A, Walling D, Ding Y, Xia Z, Schwendeman A, Hawes D, Yang F, Judkins AR, Wahl D, Lyssiotis CA, de la Nava D, Alonso MM, Eze A, Spitzer J, Schmidt SV, Duchatel RJ, Dun MD, Cain JE, Jiang L, Stopka SA, Baquer G, Regan MS, Filbin MG, Agar NYR, Zhao L, Kumar-Sinha C, Mody R, Chinnaiyan A, Kurokawa R, Pratt D, Yadav VN, Grill J, Kline C, Mueller S, Resnick A, Nazarian J, Allen JE, Odia Y, Gardner SL, Koschmann C. Clinical Efficacy of ONC201 in H3K27M-Mutant Diffuse Midline Gliomas Is Driven by Disruption of Integrated Metabolic and Epigenetic Pathways. Cancer discovery. 2023 Nov 1:13(11):2370-2393. doi: 10.1158/2159-8290.CD-23-0131. Epub [PubMed PMID: 37584601]
Level 2 (mid-level) evidenceAziz-Bose R, Monje M. Diffuse intrinsic pontine glioma: molecular landscape and emerging therapeutic targets. Current opinion in oncology. 2019 Nov:31(6):522-530. doi: 10.1097/CCO.0000000000000577. Epub [PubMed PMID: 31464759]
Level 3 (low-level) evidenceBallester LY, Wang Z, Shandilya S, Miettinen M, Burger PC, Eberhart CG, Rodriguez FJ, Raabe E, Nazarian J, Warren K, Quezado MM. Morphologic characteristics and immunohistochemical profile of diffuse intrinsic pontine gliomas. The American journal of surgical pathology. 2013 Sep:37(9):1357-64. doi: 10.1097/PAS.0b013e318294e817. Epub [PubMed PMID: 24076776]
Monje M, Mitra SS, Freret ME, Raveh TB, Kim J, Masek M, Attema JL, Li G, Haddix T, Edwards MS, Fisher PG, Weissman IL, Rowitch DH, Vogel H, Wong AJ, Beachy PA. Hedgehog-responsive candidate cell of origin for diffuse intrinsic pontine glioma. Proceedings of the National Academy of Sciences of the United States of America. 2011 Mar 15:108(11):4453-8. doi: 10.1073/pnas.1101657108. Epub 2011 Mar 1 [PubMed PMID: 21368213]
Filbin MG, Tirosh I, Hovestadt V, Shaw ML, Escalante LE, Mathewson ND, Neftel C, Frank N, Pelton K, Hebert CM, Haberler C, Yizhak K, Gojo J, Egervari K, Mount C, van Galen P, Bonal DM, Nguyen QD, Beck A, Sinai C, Czech T, Dorfer C, Goumnerova L, Lavarino C, Carcaboso AM, Mora J, Mylvaganam R, Luo CC, Peyrl A, Popović M, Azizi A, Batchelor TT, Frosch MP, Martinez-Lage M, Kieran MW, Bandopadhayay P, Beroukhim R, Fritsch G, Getz G, Rozenblatt-Rosen O, Wucherpfennig KW, Louis DN, Monje M, Slavc I, Ligon KL, Golub TR, Regev A, Bernstein BE, Suvà ML. Developmental and oncogenic programs in H3K27M gliomas dissected by single-cell RNA-seq. Science (New York, N.Y.). 2018 Apr 20:360(6386):331-335. doi: 10.1126/science.aao4750. Epub [PubMed PMID: 29674595]
Warren KE. Diffuse intrinsic pontine glioma: poised for progress. Frontiers in oncology. 2012:2():205. doi: 10.3389/fonc.2012.00205. Epub 2012 Dec 28 [PubMed PMID: 23293772]
Damodharan S, Lara-Velazquez M, Williamsen BC, Helgager J, Dey M. Diffuse Intrinsic Pontine Glioma: Molecular Landscape, Evolving Treatment Strategies and Emerging Clinical Trials. Journal of personalized medicine. 2022 May 20:12(5):. doi: 10.3390/jpm12050840. Epub 2022 May 20 [PubMed PMID: 35629262]
Argersinger DP, Rivas SR, Shah AH, Jackson S, Heiss JD. New Developments in the Pathogenesis, Therapeutic Targeting, and Treatment of H3K27M-Mutant Diffuse Midline Glioma. Cancers. 2021 Oct 21:13(21):. doi: 10.3390/cancers13215280. Epub 2021 Oct 21 [PubMed PMID: 34771443]
Chen J, Lin Z, Barrett L, Dai L, Qin Z. Identification of new therapeutic targets and natural compounds against diffuse intrinsic pontine glioma (DIPG). Bioorganic chemistry. 2020 Jun:99():103847. doi: 10.1016/j.bioorg.2020.103847. Epub 2020 Apr 13 [PubMed PMID: 32311581]
Level 2 (mid-level) evidenceKhuong-Quang DA, Buczkowicz P, Rakopoulos P, Liu XY, Fontebasso AM, Bouffet E, Bartels U, Albrecht S, Schwartzentruber J, Letourneau L, Bourgey M, Bourque G, Montpetit A, Bourret G, Lepage P, Fleming A, Lichter P, Kool M, von Deimling A, Sturm D, Korshunov A, Faury D, Jones DT, Majewski J, Pfister SM, Jabado N, Hawkins C. K27M mutation in histone H3.3 defines clinically and biologically distinct subgroups of pediatric diffuse intrinsic pontine gliomas. Acta neuropathologica. 2012 Sep:124(3):439-47. doi: 10.1007/s00401-012-0998-0. Epub 2012 Jun 3 [PubMed PMID: 22661320]
Schwartzentruber J, Korshunov A, Liu XY, Jones DT, Pfaff E, Jacob K, Sturm D, Fontebasso AM, Quang DA, Tönjes M, Hovestadt V, Albrecht S, Kool M, Nantel A, Konermann C, Lindroth A, Jäger N, Rausch T, Ryzhova M, Korbel JO, Hielscher T, Hauser P, Garami M, Klekner A, Bognar L, Ebinger M, Schuhmann MU, Scheurlen W, Pekrun A, Frühwald MC, Roggendorf W, Kramm C, Dürken M, Atkinson J, Lepage P, Montpetit A, Zakrzewska M, Zakrzewski K, Liberski PP, Dong Z, Siegel P, Kulozik AE, Zapatka M, Guha A, Malkin D, Felsberg J, Reifenberger G, von Deimling A, Ichimura K, Collins VP, Witt H, Milde T, Witt O, Zhang C, Castelo-Branco P, Lichter P, Faury D, Tabori U, Plass C, Majewski J, Pfister SM, Jabado N. Driver mutations in histone H3.3 and chromatin remodelling genes in paediatric glioblastoma. Nature. 2012 Jan 29:482(7384):226-31. doi: 10.1038/nature10833. Epub 2012 Jan 29 [PubMed PMID: 22286061]
Lewis PW, Müller MM, Koletsky MS, Cordero F, Lin S, Banaszynski LA, Garcia BA, Muir TW, Becher OJ, Allis CD. Inhibition of PRC2 activity by a gain-of-function H3 mutation found in pediatric glioblastoma. Science (New York, N.Y.). 2013 May 17:340(6134):857-61. doi: 10.1126/science.1232245. Epub 2013 Mar 28 [PubMed PMID: 23539183]
Venneti S, Garimella MT, Sullivan LM, Martinez D, Huse JT, Heguy A, Santi M, Thompson CB, Judkins AR. Evaluation of histone 3 lysine 27 trimethylation (H3K27me3) and enhancer of Zest 2 (EZH2) in pediatric glial and glioneuronal tumors shows decreased H3K27me3 in H3F3A K27M mutant glioblastomas. Brain pathology (Zurich, Switzerland). 2013 Sep:23(5):558-64. doi: 10.1111/bpa.12042. Epub 2013 Mar 6 [PubMed PMID: 23414300]
Weisbrod LJ, Thiraviyam A, Vengoji R, Shonka N, Jain M, Ho W, Batra SK, Salehi A. Diffuse intrinsic pontine glioma (DIPG): A review of current and emerging treatment strategies. Cancer letters. 2024 May 28:590():216876. doi: 10.1016/j.canlet.2024.216876. Epub 2024 Apr 10 [PubMed PMID: 38609002]
Level 3 (low-level) evidencePiunti A, Hashizume R, Morgan MA, Bartom ET, Horbinski CM, Marshall SA, Rendleman EJ, Ma Q, Takahashi YH, Woodfin AR, Misharin AV, Abshiru NA, Lulla RR, Saratsis AM, Kelleher NL, James CD, Shilatifard A. Therapeutic targeting of polycomb and BET bromodomain proteins in diffuse intrinsic pontine gliomas. Nature medicine. 2017 Apr:23(4):493-500. doi: 10.1038/nm.4296. Epub 2017 Feb 27 [PubMed PMID: 28263307]
Cooney TM, Lubanszky E, Prasad R, Hawkins C, Mueller S. Diffuse midline glioma: review of epigenetics. Journal of neuro-oncology. 2020 Oct:150(1):27-34. doi: 10.1007/s11060-020-03553-1. Epub 2020 Aug 17 [PubMed PMID: 32804378]
Mackay A, Burford A, Carvalho D, Izquierdo E, Fazal-Salom J, Taylor KR, Bjerke L, Clarke M, Vinci M, Nandhabalan M, Temelso S, Popov S, Molinari V, Raman P, Waanders AJ, Han HJ, Gupta S, Marshall L, Zacharoulis S, Vaidya S, Mandeville HC, Bridges LR, Martin AJ, Al-Sarraj S, Chandler C, Ng HK, Li X, Mu K, Trabelsi S, Brahim DH, Kisljakov AN, Konovalov DM, Moore AS, Carcaboso AM, Sunol M, de Torres C, Cruz O, Mora J, Shats LI, Stavale JN, Bidinotto LT, Reis RM, Entz-Werle N, Farrell M, Cryan J, Crimmins D, Caird J, Pears J, Monje M, Debily MA, Castel D, Grill J, Hawkins C, Nikbakht H, Jabado N, Baker SJ, Pfister SM, Jones DTW, Fouladi M, von Bueren AO, Baudis M, Resnick A, Jones C. Integrated Molecular Meta-Analysis of 1,000 Pediatric High-Grade and Diffuse Intrinsic Pontine Glioma. Cancer cell. 2017 Oct 9:32(4):520-537.e5. doi: 10.1016/j.ccell.2017.08.017. Epub 2017 Sep 28 [PubMed PMID: 28966033]
Level 1 (high-level) evidenceWu G, Diaz AK, Paugh BS, Rankin SL, Ju B, Li Y, Zhu X, Qu C, Chen X, Zhang J, Easton J, Edmonson M, Ma X, Lu C, Nagahawatte P, Hedlund E, Rusch M, Pounds S, Lin T, Onar-Thomas A, Huether R, Kriwacki R, Parker M, Gupta P, Becksfort J, Wei L, Mulder HL, Boggs K, Vadodaria B, Yergeau D, Russell JC, Ochoa K, Fulton RS, Fulton LL, Jones C, Boop FA, Broniscer A, Wetmore C, Gajjar A, Ding L, Mardis ER, Wilson RK, Taylor MR, Downing JR, Ellison DW, Zhang J, Baker SJ. The genomic landscape of diffuse intrinsic pontine glioma and pediatric non-brainstem high-grade glioma. Nature genetics. 2014 May:46(5):444-450. doi: 10.1038/ng.2938. Epub 2014 Apr 6 [PubMed PMID: 24705251]
Fontebasso AM, Papillon-Cavanagh S, Schwartzentruber J, Nikbakht H, Gerges N, Fiset PO, Bechet D, Faury D, De Jay N, Ramkissoon LA, Corcoran A, Jones DT, Sturm D, Johann P, Tomita T, Goldman S, Nagib M, Bendel A, Goumnerova L, Bowers DC, Leonard JR, Rubin JB, Alden T, Browd S, Geyer JR, Leary S, Jallo G, Cohen K, Gupta N, Prados MD, Carret AS, Ellezam B, Crevier L, Klekner A, Bognar L, Hauser P, Garami M, Myseros J, Dong Z, Siegel PM, Malkin H, Ligon AH, Albrecht S, Pfister SM, Ligon KL, Majewski J, Jabado N, Kieran MW. Recurrent somatic mutations in ACVR1 in pediatric midline high-grade astrocytoma. Nature genetics. 2014 May:46(5):462-6. doi: 10.1038/ng.2950. Epub 2014 Apr 6 [PubMed PMID: 24705250]
Hambardzumyan D, Bergers G. Glioblastoma: Defining Tumor Niches. Trends in cancer. 2015 Dec:1(4):252-265 [PubMed PMID: 27088132]
Venkatesh HS, Johung TB, Caretti V, Noll A, Tang Y, Nagaraja S, Gibson EM, Mount CW, Polepalli J, Mitra SS, Woo PJ, Malenka RC, Vogel H, Bredel M, Mallick P, Monje M. Neuronal Activity Promotes Glioma Growth through Neuroligin-3 Secretion. Cell. 2015 May 7:161(4):803-16. doi: 10.1016/j.cell.2015.04.012. Epub 2015 Apr 23 [PubMed PMID: 25913192]
Fisher PG, Breiter SN, Carson BS, Wharam MD, Williams JA, Weingart JD, Foer DR, Goldthwaite PT, Tihan T, Burger PC. A clinicopathologic reappraisal of brain stem tumor classification. Identification of pilocystic astrocytoma and fibrillary astrocytoma as distinct entities. Cancer. 2000 Oct 1:89(7):1569-76 [PubMed PMID: 11013373]
Level 2 (mid-level) evidenceDonaldson SS, Laningham F, Fisher PG. Advances toward an understanding of brainstem gliomas. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2006 Mar 10:24(8):1266-72 [PubMed PMID: 16525181]
Level 3 (low-level) evidenceSchroeder KM, Hoeman CM, Becher OJ. Children are not just little adults: recent advances in understanding of diffuse intrinsic pontine glioma biology. Pediatric research. 2014 Jan:75(1-2):205-9. doi: 10.1038/pr.2013.194. Epub 2013 Nov 5 [PubMed PMID: 24192697]
Level 3 (low-level) evidenceCooney TM, Cohen KJ, Guimaraes CV, Dhall G, Leach J, Massimino M, Erbetta A, Chiapparini L, Malbari F, Kramer K, Pollack IF, Baxter P, Laughlin S, Patay Z, Young Poussaint T, Warren KE. Response assessment in diffuse intrinsic pontine glioma: recommendations from the Response Assessment in Pediatric Neuro-Oncology (RAPNO) working group. The Lancet. Oncology. 2020 Jun:21(6):e330-e336. doi: 10.1016/S1470-2045(20)30166-2. Epub [PubMed PMID: 32502459]
Lovibond S, Gewirtz AN, Pasquini L, Krebs S, Graham MS. The promise of metabolic imaging in diffuse midline glioma. Neoplasia (New York, N.Y.). 2023 May:39():100896. doi: 10.1016/j.neo.2023.100896. Epub 2023 Mar 20 [PubMed PMID: 36944297]
Leach JL, Roebker J, Schafer A, Baugh J, Chaney B, Fuller C, Fouladi M, Lane A, Doughman R, Drissi R, DeWire-Schottmiller M, Ziegler DS, Minturn JE, Hansford JR, Wang SS, Monje-Deisseroth M, Fisher PG, Gottardo NG, Dholaria H, Packer R, Warren K, Leary SES, Goldman S, Bartels U, Hawkins C, Jones BV. MR imaging features of diffuse intrinsic pontine glioma and relationship to overall survival: report from the International DIPG Registry. Neuro-oncology. 2020 Nov 26:22(11):1647-1657. doi: 10.1093/neuonc/noaa140. Epub [PubMed PMID: 32506137]
Tisnado J, Young R, Peck KK, Haque S. Conventional and Advanced Imaging of Diffuse Intrinsic Pontine Glioma. Journal of child neurology. 2016 Oct:31(12):1386-93. doi: 10.1177/0883073816634855. Epub 2016 Apr 12 [PubMed PMID: 27071471]
Löbel U, Sedlacik J, Reddick WE, Kocak M, Ji Q, Broniscer A, Hillenbrand CM, Patay Z. Quantitative diffusion-weighted and dynamic susceptibility-weighted contrast-enhanced perfusion MR imaging analysis of T2 hypointense lesion components in pediatric diffuse intrinsic pontine glioma. AJNR. American journal of neuroradiology. 2011 Feb:32(2):315-22. doi: 10.3174/ajnr.A2277. Epub 2010 Nov 18 [PubMed PMID: 21087935]
Lober RM, Cho YJ, Tang Y, Barnes PD, Edwards MS, Vogel H, Fisher PG, Monje M, Yeom KW. Diffusion-weighted MRI derived apparent diffusion coefficient identifies prognostically distinct subgroups of pediatric diffuse intrinsic pontine glioma. Journal of neuro-oncology. 2014 Mar:117(1):175-82. doi: 10.1007/s11060-014-1375-8. Epub 2014 Feb 13 [PubMed PMID: 24522717]
Vitanza NA, Monje M. Diffuse Intrinsic Pontine Glioma: From Diagnosis to Next-Generation Clinical Trials. Current treatment options in neurology. 2019 Jul 10:21(8):37. doi: 10.1007/s11940-019-0577-y. Epub 2019 Jul 10 [PubMed PMID: 31290035]
Gavrjushin AV, Papusha LI, Veselkov AA, Zaitseva MA, Khukhlaeva EA, Konovalov AN, Druy AE. Liquid biopsy for the detection of H3K27m in patients with brainstem tumors. Neurosurgical review. 2025 May 26:48(1):442. doi: 10.1007/s10143-025-03593-z. Epub 2025 May 26 [PubMed PMID: 40415124]
Lu VM, Power EA, Zhang L, Daniels DJ. Liquid biopsy for diffuse intrinsic pontine glioma: an update. Journal of neurosurgery. Pediatrics. 2019 Nov 1:24(5):593-600. doi: 10.3171/2019.6.PEDS19259. Epub 2019 Sep 6 [PubMed PMID: 31491754]
Huang TY, Piunti A, Lulla RR, Qi J, Horbinski CM, Tomita T, James CD, Shilatifard A, Saratsis AM. Detection of Histone H3 mutations in cerebrospinal fluid-derived tumor DNA from children with diffuse midline glioma. Acta neuropathologica communications. 2017 Apr 17:5(1):28. doi: 10.1186/s40478-017-0436-6. Epub 2017 Apr 17 [PubMed PMID: 28416018]
Level 2 (mid-level) evidenceSaratsis AM, Yadavilli S, Magge S, Rood BR, Perez J, Hill DA, Hwang E, Kilburn L, Packer RJ, Nazarian J. Insights into pediatric diffuse intrinsic pontine glioma through proteomic analysis of cerebrospinal fluid. Neuro-oncology. 2012 May:14(5):547-60. doi: 10.1093/neuonc/nos067. Epub 2012 Apr 5 [PubMed PMID: 22492959]
Level 2 (mid-level) evidencePan C, Diplas BH, Chen X, Wu Y, Xiao X, Jiang L, Geng Y, Xu C, Sun Y, Zhang P, Wu W, Wang Y, Wu Z, Zhang J, Jiao Y, Yan H, Zhang L. Molecular profiling of tumors of the brainstem by sequencing of CSF-derived circulating tumor DNA. Acta neuropathologica. 2019 Feb:137(2):297-306. doi: 10.1007/s00401-018-1936-6. Epub 2018 Nov 20 [PubMed PMID: 30460397]
Patel J, Aittaleb R, Doherty R, Gera A, Lau B, Messinger D, Wadden J, Franson A, Saratsis A, Koschmann C. Liquid biopsy in H3K27M diffuse midline glioma. Neuro-oncology. 2024 May 3:26(Supplement_2):S101-S109. doi: 10.1093/neuonc/noad229. Epub [PubMed PMID: 38096156]
Sheikh SR, Recinos VMR, Thompson EM, Mangum R, Wright-Nadkarni M, Gampel B, Patel NJ. The role of brainstem biopsy and targeted therapies in pediatric diffuse midline glioma/diffuse intrinsic pontine glioma. Frontiers in oncology. 2024:14():1504440. doi: 10.3389/fonc.2024.1504440. Epub 2024 Dec 23 [PubMed PMID: 39763605]
Carai A, Mastronuzzi A, De Benedictis A, Messina R, Cacchione A, Miele E, Randi F, Esposito G, Trezza A, Colafati GS, Savioli A, Locatelli F, Marras CE. Robot-Assisted Stereotactic Biopsy of Diffuse Intrinsic Pontine Glioma: A Single-Center Experience. World neurosurgery. 2017 May:101():584-588. doi: 10.1016/j.wneu.2017.02.088. Epub 2017 Feb 27 [PubMed PMID: 28254596]
Puget S, Beccaria K, Blauwblomme T, Roujeau T, James S, Grill J, Zerah M, Varlet P, Sainte-Rose C. Biopsy in a series of 130 pediatric diffuse intrinsic Pontine gliomas. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2015 Oct:31(10):1773-80. doi: 10.1007/s00381-015-2832-1. Epub 2015 Sep 9 [PubMed PMID: 26351229]
Kieran MW. Time to rethink the unthinkable: upfront biopsy of children with newly diagnosed diffuse intrinsic pontine glioma (DIPG). Pediatric blood & cancer. 2015 Jan:62(1):3-4. doi: 10.1002/pbc.25266. Epub 2014 Oct 4 [PubMed PMID: 25284709]
Wang M, Zhang Y, Shi W, Zhu R, Li H, Zhao R. Frameless robot-assisted stereotactic biopsy: an effective and minimally invasive technique for pediatric diffuse intrinsic pontine gliomas. Journal of neuro-oncology. 2022 Oct:160(1):107-114. doi: 10.1007/s11060-022-04122-4. Epub 2022 Aug 23 [PubMed PMID: 35997920]
Chaturvedi A, Sadashiva N, Kalahasti S, Konar S, Krishna U, Ar P, Shukla D, Beniwal M, Pruthi N, Arima A, Saini J, Rao S, Santosh V. Safety and Efficacy of Biopsy in Patients with Diffuse Intrinsic Pontine Gliomas. World neurosurgery. 2024 Jul:187():e870-e882. doi: 10.1016/j.wneu.2024.05.003. Epub 2024 May 9 [PubMed PMID: 38734176]
Dalmage M, LoPresti MA, Sarkar P, Ranganathan S, Abdelmageed S, Pagadala M, Shlobin NA, Lam S, DeCuypere M. Survival and neurological outcomes after stereotactic biopsy of diffuse intrinsic pontine glioma: a systematic review. Journal of neurosurgery. Pediatrics. 2023 Dec 1:32(6):665-672. doi: 10.3171/2023.7.PEDS22462. Epub 2023 Sep 8 [PubMed PMID: 37724839]
Level 1 (high-level) evidenceWilliams JR, Young CC, Vitanza NA, McGrath M, Feroze AH, Browd SR, Hauptman JS. Progress in diffuse intrinsic pontine glioma: advocating for stereotactic biopsy in the standard of care. Neurosurgical focus. 2020 Jan 1:48(1):E4. doi: 10.3171/2019.9.FOCUS19745. Epub [PubMed PMID: 31896081]
Gupta N, Goumnerova LC, Manley P, Chi SN, Neuberg D, Puligandla M, Fangusaro J, Goldman S, Tomita T, Alden T, DiPatri A, Rubin JB, Gauvain K, Limbrick D, Leonard J, Geyer JR, Leary S, Browd S, Wang Z, Sood S, Bendel A, Nagib M, Gardner S, Karajannis MA, Harter D, Ayyanar K, Gump W, Bowers DC, Weprin B, MacDonald TJ, Aguilera D, Brahma B, Robison NJ, Kiehna E, Krieger M, Sandler E, Aldana P, Khatib Z, Ragheb J, Bhatia S, Mueller S, Banerjee A, Bredlau AL, Gururangan S, Fuchs H, Cohen KJ, Jallo G, Dorris K, Handler M, Comito M, Dias M, Nazemi K, Baird L, Murray J, Lindeman N, Hornick JL, Malkin H, Sinai C, Greenspan L, Wright KD, Prados M, Bandopadhayay P, Ligon KL, Kieran MW. Prospective feasibility and safety assessment of surgical biopsy for patients with newly diagnosed diffuse intrinsic pontine glioma. Neuro-oncology. 2018 Oct 9:20(11):1547-1555. doi: 10.1093/neuonc/noy070. Epub [PubMed PMID: 29741745]
Level 2 (mid-level) evidenceCoutinho AE, Chapman KE. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Molecular and cellular endocrinology. 2011 Mar 15:335(1):2-13. doi: 10.1016/j.mce.2010.04.005. Epub 2010 Apr 14 [PubMed PMID: 20398732]
Level 3 (low-level) evidencePappachan JM, Hariman C, Edavalath M, Waldron J, Hanna FW. Cushing's syndrome: a practical approach to diagnosis and differential diagnoses. Journal of clinical pathology. 2017 Apr:70(4):350-359. doi: 10.1136/jclinpath-2016-203933. Epub 2017 Jan 9 [PubMed PMID: 28069628]
Hue CD, Cho FS, Cao S, Dale Bass CR, Meaney DF, Morrison B 3rd. Dexamethasone potentiates in vitro blood-brain barrier recovery after primary blast injury by glucocorticoid receptor-mediated upregulation of ZO-1 tight junction protein. Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism. 2015 Jul:35(7):1191-8. doi: 10.1038/jcbfm.2015.38. Epub 2015 Mar 11 [PubMed PMID: 25757751]
Level 3 (low-level) evidenceFonseca A, Solano P, Ramaswamy V, Tabori U, Huang A, Drake JM, Tsang DS, Laperriere N, Bartels U, Kulkarni AV, Bouffet E. Ventricular size determination and management of ventriculomegaly and hydrocephalus in patients with diffuse intrinsic pontine glioma: an institutional experience. Journal of neurosurgery. 2021 Oct 1:135(4):1139-1145. doi: 10.3171/2020.10.JNS203257. Epub 2021 Mar 5 [PubMed PMID: 33668028]
Guida L, Roux FE, Massimino M, Marras CE, Sganzerla E, Giussani C. Safety and Efficacy of Endoscopic Third Ventriculostomy in Diffuse Intrinsic Pontine Glioma Related Hydrocephalus: A Systematic Review. World neurosurgery. 2019 Apr:124():29-35. doi: 10.1016/j.wneu.2018.12.096. Epub 2018 Dec 30 [PubMed PMID: 30599251]
Level 1 (high-level) evidenceGallitto M, Lazarev S, Wasserman I, Stafford JM, Wolden SL, Terezakis SA, Bindra RS, Bakst RL. Role of Radiation Therapy in the Management of Diffuse Intrinsic Pontine Glioma: A Systematic Review. Advances in radiation oncology. 2019 Jul-Sep:4(3):520-531. doi: 10.1016/j.adro.2019.03.009. Epub 2019 Mar 30 [PubMed PMID: 31360809]
Level 3 (low-level) evidenceMankuzhy NP, Tringale KR, Dunkel IJ, Farouk Sait S, Souweidane MM, Khakoo Y, Karajannis MA, Wolden S. Hypofractionated re-irradiation for diffuse intrinsic pontine glioma. Pediatric blood & cancer. 2024 May:71(5):e30929. doi: 10.1002/pbc.30929. Epub 2024 Mar 2 [PubMed PMID: 38430472]
Hayashi A, Ito E, Omura M, Aida N, Tanaka M, Tanaka Y, Sato H, Miyagawa N, Yokosuka T, Iwasaki F, Hamanoue S, Goto H. Hypofractionated radiotherapy in children with diffuse intrinsic pontine glioma. Pediatrics international : official journal of the Japan Pediatric Society. 2020 Jan:62(1):47-51. doi: 10.1111/ped.14070. Epub [PubMed PMID: 31785177]
Janssens GO, Jansen MH, Lauwers SJ, Nowak PJ, Oldenburger FR, Bouffet E, Saran F, Kamphuis-van Ulzen K, van Lindert EJ, Schieving JH, Boterberg T, Kaspers GJ, Span PN, Kaanders JH, Gidding CE, Hargrave D. Hypofractionation vs conventional radiation therapy for newly diagnosed diffuse intrinsic pontine glioma: a matched-cohort analysis. International journal of radiation oncology, biology, physics. 2013 Feb 1:85(2):315-20. doi: 10.1016/j.ijrobp.2012.04.006. Epub 2012 Jun 9 [PubMed PMID: 22682807]
Level 2 (mid-level) evidenceZaghloul MS, Eldebawy E, Ahmed S, Mousa AG, Amin A, Refaat A, Zaky I, Elkhateeb N, Sabry M. Hypofractionated conformal radiotherapy for pediatric diffuse intrinsic pontine glioma (DIPG): a randomized controlled trial. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2014 Apr:111(1):35-40. doi: 10.1016/j.radonc.2014.01.013. Epub 2014 Feb 20 [PubMed PMID: 24560760]
Level 1 (high-level) evidenceFreese C, Takiar V, Fouladi M, DeWire M, Breneman J, Pater L. Radiation and subsequent reirradiation outcomes in the treatment of diffuse intrinsic pontine glioma and a systematic review of the reirradiation literature. Practical radiation oncology. 2017 Mar-Apr:7(2):86-92. doi: 10.1016/j.prro.2016.11.005. Epub 2016 Nov 23 [PubMed PMID: 28274399]
Level 1 (high-level) evidenceLassaletta A, Strother D, Laperriere N, Hukin J, Vanan MI, Goddard K, Lafay-Cousin L, Johnston DL, Zelcer S, Zapotocky M, Rajagopal R, Ramaswamy V, Hawkins C, Tabori U, Huang A, Bartels U, Bouffet E. Reirradiation in patients with diffuse intrinsic pontine gliomas: The Canadian experience. Pediatric blood & cancer. 2018 Jun:65(6):e26988. doi: 10.1002/pbc.26988. Epub 2018 Jan 25 [PubMed PMID: 29369515]
Shariff N, Moreno AS, Bennett J, Ramaswamy V, Das A, Liu AP, Huang A, Tabori U, Hawkins C, Dirks P, Bouffet E, Keilty DM, Millar BA, Hodgson DC, Tsang DS. Re-irradiation for children with diffuse intrinsic pontine glioma and diffuse midline glioma. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2025 Jun:207():110865. doi: 10.1016/j.radonc.2025.110865. Epub 2025 Mar 24 [PubMed PMID: 40139463]
Wawrzuta D, Chojnacka M, Drogosiewicz M, Pędziwiatr K, Dembowska-Bagińska B. Reirradiation for diffuse intrinsic pontine glioma: prognostic radiomic factors at progression. Strahlentherapie und Onkologie : Organ der Deutschen Rontgengesellschaft ... [et al]. 2024 Sep:200(9):797-804. doi: 10.1007/s00066-024-02241-7. Epub 2024 May 15 [PubMed PMID: 38748214]
Chavaz L, Janssens GO, Bolle S, Mandeville H, Ramos-Albiac M, Van Beek K, Benghiat H, Hoeben B, Morales La Madrid A, Seidel C, Kortmann RD, Hargrave D, Gandola L, Pecori E, van Vuurden DG, Biassoni V, Massimino M, Kramm CM, von Bueren AO. Neurological Symptom Improvement After Re-Irradiation in Patients With Diffuse Intrinsic Pontine Glioma: A Retrospective Analysis of the SIOP-E-HGG/DIPG Project. Frontiers in oncology. 2022:12():926196. doi: 10.3389/fonc.2022.926196. Epub 2022 Jun 22 [PubMed PMID: 35814457]
Level 2 (mid-level) evidenceArrillaga-Romany I, Gardner SL, Odia Y, Aguilera D, Allen JE, Batchelor T, Butowski N, Chen C, Cloughesy T, Cluster A, de Groot J, Dixit KS, Graber JJ, Haggiagi AM, Harrison RA, Kheradpour A, Kilburn LB, Kurz SC, Lu G, MacDonald TJ, Mehta M, Melemed AS, Nghiemphu PL, Ramage SC, Shonka N, Sumrall A, Tarapore RS, Taylor L, Umemura Y, Wen PY. ONC201 (Dordaviprone) in Recurrent H3 K27M-Mutant Diffuse Midline Glioma. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2024 May 1:42(13):1542-1552. doi: 10.1200/JCO.23.01134. Epub 2024 Feb 9 [PubMed PMID: 38335473]
Duchatel RJ, Mannan A, Woldu AS, Hawtrey T, Hindley PA, Douglas AM, Jackson ER, Findlay IJ, Germon ZP, Staudt D, Kearney PS, Smith ND, Hindley KE, Cain JE, André N, La Madrid AM, Nixon B, De Iuliis GN, Nazarian J, Irish K, Alvaro F, Eisenstat DD, Beck A, Vitanza NA, Mueller S, Morris JC, Dun MD. Preclinical and clinical evaluation of German-sourced ONC201 for the treatment of H3K27M-mutant diffuse intrinsic pontine glioma. Neuro-oncology advances. 2021 Jan-Dec:3(1):vdab169. doi: 10.1093/noajnl/vdab169. Epub 2021 Nov 19 [PubMed PMID: 34988452]
Level 3 (low-level) evidenceHall MD, Odia Y, Allen JE, Tarapore R, Khatib Z, Niazi TN, Daghistani D, Schalop L, Chi AS, Oster W, Mehta MP. First clinical experience with DRD2/3 antagonist ONC201 in H3 K27M-mutant pediatric diffuse intrinsic pontine glioma: a case report. Journal of neurosurgery. Pediatrics. 2019 Jun 1:23(6):719-725. doi: 10.3171/2019.2.PEDS18480. Epub 2019 Apr 5 [PubMed PMID: 30952114]
Level 3 (low-level) evidenceMcVeigh L, Patel T, Miclea M, Schwark K, Ajaero D, Momen F, Clausen M, Adam T, Aittaleb R, Wadden J, Lau B, Franson AT, Koschmann C, Marupudi NI. Updates in Diagnostic Techniques and Experimental Therapies for Diffuse Intrinsic Pontine Glioma. Cancers. 2025 Mar 10:17(6):. doi: 10.3390/cancers17060931. Epub 2025 Mar 10 [PubMed PMID: 40149267]
Lin C, Smith C, Rutka J. Current immunotherapeutic approaches to diffuse intrinsic pontine glioma. Frontiers in genetics. 2024:15():1349612. doi: 10.3389/fgene.2024.1349612. Epub 2024 May 7 [PubMed PMID: 38774284]
Qian X, Ning W, Yang J, Dunmall LC, Pandha HS, Shang G, Guo Y, Zhang D, Qu Y, Wang H, Gu C, Zhang M, Wang Y, Wang S, Zhang H. The oncolytic adenovirus Ad-TD-nsIL12 in primary or progressive pediatric IDH wild-type diffuse intrinsic pontine glioma results of two phase I clinical trials. Nature communications. 2025 Jul 28:16(1):6934. doi: 10.1038/s41467-025-62260-5. Epub 2025 Jul 28 [PubMed PMID: 40721414]
Level 1 (high-level) evidenceGállego Pérez-Larraya J, Garcia-Moure M, Labiano S, Patiño-García A, Dobbs J, Gonzalez-Huarriz M, Zalacain M, Marrodan L, Martinez-Velez N, Puigdelloses M, Laspidea V, Astigarraga I, Lopez-Ibor B, Cruz O, Oscoz Lizarbe M, Hervas-Stubbs S, Alkorta-Aranburu G, Tamayo I, Tavira B, Hernandez-Alcoceba R, Jones C, Dharmadhikari G, Ruiz-Moreno C, Stunnenberg H, Hulleman E, van der Lugt J, Idoate MÁ, Diez-Valle R, Esparragosa Vázquez I, Villalba M, de Andrea C, Núñez-Córdoba JM, Ewald B, Robbins J, Fueyo J, Gomez-Manzano C, Lang FF, Tejada S, Alonso MM. Oncolytic DNX-2401 Virus for Pediatric Diffuse Intrinsic Pontine Glioma. The New England journal of medicine. 2022 Jun 30:386(26):2471-2481. doi: 10.1056/NEJMoa2202028. Epub [PubMed PMID: 35767439]
Timpanaro A, Song EZ, Toumi R, Elena-Sanchez L, Meechan M, Piccand C, Nemec K, Kordowski A, Lau D, Johnson S, Winter L, Rajendran A, Ronsley R, Oda SK, Gustafson J, Wendler JP, Koschmann C, Evans M, Pattwell S, Jensen MC, Foster JB, Dun MD, Biery MC, Vitanza NA. Preclinical efficacy of combinatorial B7-H3 CAR T cells and ONC206 against diffuse intrinsic pontine glioma. bioRxiv : the preprint server for biology. 2025 Sep 4:():. pii: 2025.09.01.673023. doi: 10.1101/2025.09.01.673023. Epub 2025 Sep 4 [PubMed PMID: 40950080]
Vitanza NA, Ronsley R, Choe M, Seidel K, Huang W, Rawlings-Rhea SD, Beam M, Steinmetzer L, Wilson AL, Brown C, Beebe A, Lindgren C, Gustafson JA, Wein A, Holtzclaw S, Hoeppner C, Goldstein HE, Browd SR, Hauptman JS, Lee A, Ojemann JG, Crotty EE, Leary SES, Perez FA, Wright JN, Alonso MM, Dun MD, Foster JB, Hurst D, Kong A, Thomsen A, Orentas RJ, Albert CM, Pinto N, Annesley C, Gardner RA, Ho O, Pattabhi S, Gust J, Wendler JP, Park JR, Jensen MC. Intracerebroventricular B7-H3-targeting CAR T cells for diffuse intrinsic pontine glioma: a phase 1 trial. Nature medicine. 2025 Mar:31(3):861-868. doi: 10.1038/s41591-024-03451-3. Epub 2025 Jan 7 [PubMed PMID: 39775044]
Tykocki T. Diffuse Intrinsic Pontine Glioma and Chimeric Antigen Receptor T-Cell Therapy: An Emerging Frontier. World neurosurgery. 2025 Feb:194():123579. doi: 10.1016/j.wneu.2024.123579. Epub 2025 Jan 22 [PubMed PMID: 39694135]
Vitanza NA, Wilson AL, Huang W, Seidel K, Brown C, Gustafson JA, Yokoyama JK, Johnson AJ, Baxter BA, Koning RW, Reid AN, Meechan M, Biery MC, Myers C, Rawlings-Rhea SD, Albert CM, Browd SR, Hauptman JS, Lee A, Ojemann JG, Berens ME, Dun MD, Foster JB, Crotty EE, Leary SES, Cole BL, Perez FA, Wright JN, Orentas RJ, Chour T, Newell EW, Whiteaker JR, Zhao L, Paulovich AG, Pinto N, Gust J, Gardner RA, Jensen MC, Park JR. Intraventricular B7-H3 CAR T Cells for Diffuse Intrinsic Pontine Glioma: Preliminary First-in-Human Bioactivity and Safety. Cancer discovery. 2023 Jan 9:13(1):114-131. doi: 10.1158/2159-8290.CD-22-0750. Epub [PubMed PMID: 36259971]
Nonnenbroich LF, Bouchal SM, Millesi E, Rechberger JS, Khatua S, Daniels DJ. H3K27-Altered Diffuse Midline Glioma of the Brainstem: From Molecular Mechanisms to Targeted Interventions. Cells. 2024 Jun 28:13(13):. doi: 10.3390/cells13131122. Epub 2024 Jun 28 [PubMed PMID: 38994974]
van Vuurden DG. Convection-enhanced delivery: chemosurgery in diffuse intrinsic pontine glioma. The Lancet. Oncology. 2018 Aug:19(8):1001-1003. doi: 10.1016/S1470-2045(18)30408-X. Epub 2018 Jun 18 [PubMed PMID: 29914797]
Souweidane MM, Kramer K, Pandit-Taskar N, Zhou Z, Haque S, Zanzonico P, Carrasquillo JA, Lyashchenko SK, Thakur SB, Donzelli M, Turner RS, Lewis JS, Cheung NV, Larson SM, Dunkel IJ. Convection-enhanced delivery for diffuse intrinsic pontine glioma: a single-centre, dose-escalation, phase 1 trial. The Lancet. Oncology. 2018 Aug:19(8):1040-1050. doi: 10.1016/S1470-2045(18)30322-X. Epub 2018 Jun 18 [PubMed PMID: 29914796]
Filieri S, Miciaccia M, Armenise D, Baldelli OM, Liturri A, Ferorelli S, Sardanelli AM, Perrone MG, Scilimati A. Can Focused Ultrasound Overcome the Failure of Chemotherapy in Treating Pediatric Diffuse Intrinsic Pontine Glioma Due to a Blood-Brain Barrier Obstacle? Pharmaceuticals (Basel, Switzerland). 2025 Apr 3:18(4):. doi: 10.3390/ph18040525. Epub 2025 Apr 3 [PubMed PMID: 40283959]
Ishida J, Alli S, Bondoc A, Golbourn B, Sabha N, Mikloska K, Krumholtz S, Srikanthan D, Fujita N, Luck A, Maslink C, Smith C, Hynynen K, Rutka J. MRI-guided focused ultrasound enhances drug delivery in experimental diffuse intrinsic pontine glioma. Journal of controlled release : official journal of the Controlled Release Society. 2021 Feb 10:330():1034-1045. doi: 10.1016/j.jconrel.2020.11.010. Epub 2020 Nov 11 [PubMed PMID: 33188825]
Stitzlein LM, Baig MU, Chandra J, McGovern S, Paulino A, Ketonen LM, Khatua S, Zaky W. Phase I Study of Vorinostat and Temsirolimus in Newly Diagnosed or Progressive Diffuse Intrinsic Pontine Glioma. Pediatric blood & cancer. 2025 May:72(5):e31619. doi: 10.1002/pbc.31619. Epub 2025 Feb 25 [PubMed PMID: 40000388]
Su JM, Kilburn LB, Mansur DB, Krailo M, Buxton A, Adekunle A, Gajjar A, Adamson PC, Weigel B, Fox E, Blaney SM, Fouladi M. Phase I/II trial of vorinostat and radiation and maintenance vorinostat in children with diffuse intrinsic pontine glioma: A Children's Oncology Group report. Neuro-oncology. 2022 Apr 1:24(4):655-664. doi: 10.1093/neuonc/noab188. Epub [PubMed PMID: 34347089]
Bartlett AL, Lane A, Chaney B, Escorza NY, Black K, Cochrane A, Minturn J, Bartels U, Warren K, Hansford J, Ziegler D, Diez B, Goldman S, Packer R, Kieran M, DeWire-Schottmiller M, Erker C, Monje-Deisseroth M, Wagner L, Koschmann C, Dorris K, Shih CS, Hassall T, Samson Y, Fisher P, Wang SS, Tsui K, Sevlever G, Zhu X, Dexheimer P, Asher A, Fuller C, Drissi R, Jones B, Leach J, Fouladi M. Characteristics of children ≤36 months of age with DIPG: A report from the international DIPG registry. Neuro-oncology. 2022 Dec 1:24(12):2190-2199. doi: 10.1093/neuonc/noac123. Epub [PubMed PMID: 35552452]
Spencer D, Bonner ER, Tor-Díez C, Liu X, Bougher K, Prasad R, Gordish-Dressman H, Eze A, Packer RJ, Nazarian J, Linguraru MG, Bornhorst M. Tumor volume features predict survival outcomes for patients diagnosed with diffuse intrinsic pontine glioma. Neuro-oncology advances. 2024 Jan-Dec:6(1):vdae151. doi: 10.1093/noajnl/vdae151. Epub 2024 Aug 30 [PubMed PMID: 39434924]
Level 3 (low-level) evidenceMandrell BN, Baker J, Levine D, Gattuso J, West N, Sykes A, Gajjar A, Broniscer A. Children with minimal chance for cure: parent proxy of the child's health-related quality of life and the effect on parental physical and mental health during treatment. Journal of neuro-oncology. 2016 Sep:129(2):373-81. doi: 10.1007/s11060-016-2187-9. Epub 2016 Jun 25 [PubMed PMID: 27344555]
Level 2 (mid-level) evidence