Introduction
Congenital diaphragmatic hernia (CDH) is a developmental defect of the diaphragm that allows herniation of abdominal viscera into the thoracic cavity. Herniation of the abdominal viscera results in a spectrum of cardiopulmonary abnormalities, including pulmonary hypoplasia, abnormal pulmonary vascular remodeling, secondary pulmonary hypertension, and cardiac strain.[1] CDH is classified according to the anatomic location of the defect. Bochdalek hernias, which arise from a posterolateral defect, occur predominantly on the left side and are typically the most clinically severe. Morgagni hernias originate from an anteromedial defect. Effective treatment requires coordinated prenatal diagnosis, postnatal stabilization, and timely surgical repair through interdisciplinary collaboration.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
CDH arises from the failed closure or fusion of the pleuroperitoneal membranes or other muscular components between 8 and 12 weeks of gestation. For example, the anterior central tendon develops from the septum transversum, while the posterolateral sections, where Bochdalek hernias occur, develop from the pleuroperitoneal folds. A Bochdalek hernia occurs if the pleuroperitoneal folds fail to fuse with the septum transversum and the dorsal mesentery of the esophagus by the 10th week of gestation.
Congenital diaphragmatic hernias may be classified as intrapleural or mediastinal. Intrapleural hernias, such as Bochdalek hernias, contain organs that compress intrathoracic viscera, causing pulmonary hypoplasia. Conversely, mediastinal hernias, such as true Morgagni hernias, typically do not cause pulmonary hypoplasia or communicate with the pericardial space. The causes of CDH are often multifactorial, with genetic, environmental, and nutritional factors contributing to development rather than a single etiology.[1][2] Approximately 10% to 15% of CDH cases are associated with chromosomal anomalies, such as trisomies 13, 18, and 21, or copy number variants and single-gene defects, such as GATA4 and LRP2.[1][2][3] Syndromic associations include Fryns syndrome, Cornelia de Lange syndrome, and Donnai-Barrow syndrome.
Epidemiology
The incidence of CDH is estimated at 1 to 4 per 10,000 live births.[1][2][4] The 6 distinct types of CDH include posterolateral hernias (Bochdalek), parasternal hernias (Morgagni), other anterior hernias associated with pentalogy of Cantrell, central hernias, hiatal hernias, and diaphragmatic eventration. The posterolateral (Bochdalek) type is the most common, accounting for 70% to 85% of cases, with a left-sided predominance in approximately 80% of cases.[1][4][5] Right-sided and bilateral defects occur less frequently and are associated with a worse prognosis.[4][5] Morgagni (anteromedial) hernias constitute approximately 2% to 5% of cases.[5][6] Approximately 30% to 40% of infants with CDH have additional congenital anomalies, especially cardiac or central nervous system defects.[2][3]
Pathophysiology
Herniation of abdominal contents into the thoracic cavity compresses the developing lung, reducing alveolar branching, capillary density, and overall lung volume. Pulmonary hypoplasia is bilateral but more severe ipsilateral to the defect.[1][3] Concurrently, pulmonary arterioles undergo abnormal remodeling characterized by medial hypertrophy and adventitial thickening, leading to elevated pulmonary vascular resistance and persistent pulmonary hypertension.[1][3] In severe cases, left ventricular hypoplasia or cardiac compression further worsens hemodynamics.[1] Pulmonary hypoplasia, altered pulmonary vasoreactivity, and pulmonary hypertension are the principal drivers of morbidity and mortality in CDH.[7]
Histopathology
If a hernia sac is present, it is composed of the pleuroperitoneal membrane and lacks diaphragmatic muscle. Pulmonary histology findings include fewer alveoli, thicker alveolar septa, reduced vascularity, and muscularization of the arterioles. Chronic pulmonary hypertension leads to right ventricular hypertrophy in advanced cases.[3]
History and Physical
Prenatal
With modern obstetric imaging, roughly 60% to 70% of patients with CDH are diagnosed prenatally.[1][3] Ultrasonography may show intrathoracic abdominal organs, mediastinal shift, polyhydramnios, or an absent stomach bubble in the abdomen. Liver herniation is a key adverse prognostic sign.[3][4] Fetal MRI is used to assess lung volumes and defect anatomy more accurately. Metrics such as the observed-to-expected lung-to-head ratio are powerful predictors of survival, according to results from a recent meta-analysis by Mustafa et al.[8] Comprehensive anomaly screening, including fetal echocardiography and microarray testing, is standard.[3]Postnatal
Neonates with substantial defects rapidly present with respiratory distress, cyanosis, a scaphoid or concave abdomen, diminished breath sounds on the affected side, and occasionally bowel sounds in the chest. The contralateral mediastinum may be shifted.[1][2] Milder or later-presenting cases may present with feeding difficulties, recurrent respiratory tract infections, or developmental abnormalities.[3][8]
Evaluation
More than half of CDH cases are detected prenatally during the routine 18- to 24-week anatomy scan, with ultrasonography showing intrathoracic abdominal contents, mediastinal shift, and the positions of the stomach and liver. Right-sided defects may be more difficult to identify due to similar liver and lung echogenicity, with color Doppler ultrasonography aiding detection of intrahepatic vessels. Fetal MRI provides more precise quantification of lung volumes and associated anomalies. Prognostic assessment relies on metrics such as the lung-to-head ratio and the observed-to-expected lung-to-head ratio. Results from earlier studies showed that a lung-to-head ratio greater than 1.35 was associated with approximately 100% survival and a ratio less than 0.6 was associated with no survival. Results from more recent studies suggested that an observed-to-expected lung-to-head ratio less than 15% is associated with near-universal mortality, whereas a ratio greater than 45% predicts survival greater than 75% in fetuses with isolated left-sided CDH.[9][10][11][12] The MRI-derived observed-to-expected total fetal lung volume and liver herniation further refine prognosis (see Image. Delayed Diaphragmatic Hernia). Polyhydramnios may occur because of impaired fetal swallowing and increase the risk of preterm delivery. Given the frequent association with chromosomal and structural anomalies, genetic evaluation is recommended. After birth, chest radiography typically shows bowel loops within the thorax, mediastinal shift, and an absent diaphragmatic contour, while echocardiography is essential to evaluate pulmonary hypertension and cardiac anatomy. Arterial blood gas analysis guides respiratory treatment, and additional imaging may be used to distinguish CDH from other thoracic lesions.[2][5]
Treatment / Management
Antenatal Management
Once CDH is diagnosed, close antenatal surveillance with serial ultrasonography and Doppler ultrasonography is recommended to monitor fetal growth and well-being. Interdisciplinary counseling and delivery planning should also be provided at a tertiary center with neonatal surgical and extracorporeal membrane oxygenation capabilities.[13] In selected cases of moderate to severe CDH, fetal endoscopic tracheal occlusion may be offered, particularly in severe disease, such as an observed-to-expected lung-to-head ratio less than 25% with liver herniation. Fetal endoscopic tracheal occlusion involves endoscopic placement of a balloon in the fetal trachea at approximately 26 to 30 weeks of gestation to promote lung growth through fluid accumulation and pulmonary stretch. Balloon removal is performed at approximately 33-34 weeks' gestation to allow surfactant production.[3][14][15] Although fetal endoscopic tracheal occlusion is associated with an increased risk of preterm delivery, results from studies suggested improved survival in selected patients.[16][17][18](A1)
Delivery Timing
Delivery of neonates with CDH is not recommended before the completion of 37 weeks of gestation. Results from a study by Hutcheon et al showed that gestational age at delivery significantly affected outcomes in pregnancies complicated by CDH, with delivery before 37 weeks associated with increased neonatal mortality and progressively improved outcomes observed with advancing gestational age. The findings do not support routine early delivery in otherwise stable patients and instead favor expectant treatment to term in the absence of other obstetric or fetal indications.[19]
Perinatal Stabilization
In newborns with prenatally diagnosed CDH, clinicians should perform endotracheal intubation and place a nasogastric tube promptly after delivery to decompress the stomach and intestines. Bag-mask ventilation should be avoided. Gentle ventilation with low peak inspiratory pressures of 25 cm H2O or less minimizes the risk of barotrauma. High-frequency oscillatory ventilation may be used if necessary. Preload and inotropy should be optimized, and pulmonary hypertension should be treated with inhaled nitric oxide, sildenafil, prostacyclins, or milrinone.[20] The remainder of delivery room treatment should follow current Neonatal Resuscitation Program guidelines.(A1)
Ventilator Management
Gentle ventilation strategies to minimize ventilator-induced lung injury are the cornerstone of respiratory treatment in infants with CDH. Target parameters include preductal oxygen saturation values of 85% to 95%, peak inspiratory pressure less than 25 cm H2O, positive end-expiratory pressure of 3 to 5 cm H2O, and permissive hypercapnia with a partial pressure of carbon dioxide of 45 to 60 mm Hg. High-frequency ventilation may be used if conventional ventilation is inadequate. However, results from the VICI trial showed shorter ventilation duration and reduced use of extracorporeal membrane oxygenation with conventional ventilation, with no difference in the primary outcome of bronchopulmonary dysplasia or death.[15] Routine surfactant administration is not recommended in term neonates and should be considered selectively in preterm neonates, as studies have not shown a clear benefit.[21][22](A1)
Pulmonary Hypertension Management
Abnormal remodeling of the pulmonary vasculature in infants with CDH contributes to pulmonary hypertension. Clinical findings that raise concern for pulmonary hypertension include hypoxemia, cyanosis, and differential preductal and postductal oxygen saturation values caused by right-to-left shunting across the ductus arteriosus. Echocardiography should be obtained within 48 hours after pulmonary hypertension is suspected and typically shows right ventricular dysfunction, valvular regurgitation, and bidirectional or right-to-left shunting. Treatment includes optimizing ventilation and oxygenation, maintaining systemic blood pressure with vasopressors as needed, and using pulmonary vasodilators to improve pulmonary blood flow. Inhaled nitric oxide is first-line therapy in neonates older than 34 weeks of gestation, although results from the Neonatal Inhaled Nitric Oxide Study trial showed that the treatment did not reduce extracorporeal membrane oxygenation use or mortality in CDH.[20] Additional agents, such as milrinone, sildenafil, bosentan, prostacyclin, and prostaglandin E1, may be used selectively, particularly in neonates with ventricular dysfunction. Extracorporeal membrane oxygenation is reserved for neonates with refractory pulmonary hypertension despite maximal medical therapy, in accordance with established criteria. For long-term treatment and transition off inhaled nitric oxide, authorities recommend oral pulmonary vasodilators, noting that tadalafil or sildenafil should be strongly considered.[6](A1)
Surgical Repair
CDH was historically treated as an emergent surgical condition. However, high mortality related to pulmonary hypertension led to delayed repair, which is now typically performed 48 to 72 hours after birth to allow stabilization, with further delay in neonates with severe pulmonary hypertension. Survival decreases to approximately 50% in neonates requiring extracorporeal membrane oxygenation. The timing of repair during extracorporeal membrane oxygenation varies, as this approach carries a higher bleeding risk but may yield benefits with modified anticoagulation strategies at select centers. Surgical repair is performed via open or increasingly thoracoscopic approaches in stable patients, with minimally invasive techniques potentially reducing morbidity. Large defects often require patch repair with prosthetic or biologic materials or muscle flaps, all of which carry a risk of recurrence.[3][15](A1)
Extracorporeal Membrane Oxygenation
Extracorporeal membrane oxygenation is reserved for refractory hypoxemia with an oxygenation index greater than 40 in newborns at least 34 weeks of gestation and weighing at least 2 kg without lethal anomalies.[3][15]Postoperative Care(A1)
Postoperative care focuses on ventilator weaning, control of pulmonary hypertension, nutrition, infection prevention, and growth. Long-term monitoring assesses respiratory tract, gastrointestinal tract, and neurodevelopmental outcomes.
Differential Diagnosis
The differential diagnosis of congenital diaphragmatic hernia includes other thoracic lesions, such as congenital pulmonary airway malformation, bronchopulmonary sequestration, diaphragmatic eventration, bronchogenic cyst, bronchial atresia, tension pneumothorax, and teratomas. The presence of intra-abdominal contents within the thorax on chest radiography helps distinguish congenital diaphragmatic hernia from these lesions. Prenatally, identification of a stomach bubble and intestinal peristalsis within the thorax on ultrasonography supports the diagnosis. Diaphragmatic eventration, in which the diaphragm is intact but thin and elevated, can be difficult to differentiate from congenital diaphragmatic hernia prenatally.
Prognosis
Outcomes in congenital diaphragmatic hernia are influenced by prematurity, defect size, degree of lung hypoplasia and pulmonary hypertension, associated anomalies, and institutional experience. Prenatal predictors, such as the observed-to-expected lung-to-head ratio and liver herniation, further refine the prognosis. With advances in ventilation strategies, pulmonary hypertension treatment, and surgical techniques, survival has improved, with overall rates of approximately 60% to 70%, including approximately 70% to 80% in neonates not requiring extracorporeal membrane oxygenation and 40% to 60% in infants requiring it.[3][15][23] Despite improved survival, long-term complications remain common and include chronic lung disease, gastroesophageal reflux, feeding difficulties, recurrence, hearing loss, and developmental delays.[24]
Complications
Infants with congenital diaphragmatic hernia may experience multiple complications beyond infancy that significantly affect quality of life. Respiratory sequelae include chronic lung disease, the need for supplemental oxygen at home, aspiration pneumonia, pulmonary hypertension, and obstructive airway disease. Gastrointestinal complications, such as feeding aversion, gastroesophageal reflux, and developmental abnormalities, are common, along with neurocognitive delays, behavioral disorders, and sensorineural hearing loss. Hernia recurrence may occur months to years later, particularly in infants with large defects. Orthopedic abnormalities, including pectus deformities, chest wall asymmetry, and scoliosis, are also frequently reported.[25][26]
Postoperative and Rehabilitation Care
Because infants with congenital diaphragmatic hernia are at high risk of sudden episodic pulmonary hypertension and subsequent right-sided heart failure, clinicians should maintain a low threshold for repeat echocardiography throughout the postoperative period. Repeat echocardiography is critical for monitoring right ventricular function and assessing cardiac output. Echocardiographic monitoring also enables the prompt detection of worsening atrioventricular valve regurgitation.[27][28][29]
Deterrence and Patient Education
Patients with congenital diaphragmatic hernia require periodic long-term monitoring because of associated complications. Patients and their parents should be educated about the need for regular follow-up with the pediatrician for preventive health care visits and with appropriate subspecialists to minimize disability associated with these complications. A detailed list of follow-up recommendations for infants with congenital diaphragmatic hernia is summarized in the American Academy of Pediatrics' guidance.[25]
Enhancing Healthcare Team Outcomes
Treatment of infants with congenital diaphragmatic hernia requires a coordinated, interprofessional approach. Following antenatal diagnosis, parents should receive counseling from an interdisciplinary team that includes specialists in maternal–fetal medicine, pediatric surgery, neonatology, cardiology, genetics, nursing, nutrition, developmental services, and social work, as appropriate. Genetic evaluation and counseling are recommended to assess the risk of recurrence. Standardized care pathways, simulation training, and structured postnatal follow-up with ongoing surveillance and screening improve the consistency of care and optimize outcomes.
Media
(Click Image to Enlarge)

Delayed Diaphragmatic Hernia. A delayed diaphragmatic hernia is seen on computed tomography imaging.
Contributed by M Pellegrini, MD
(Click Image to Enlarge)
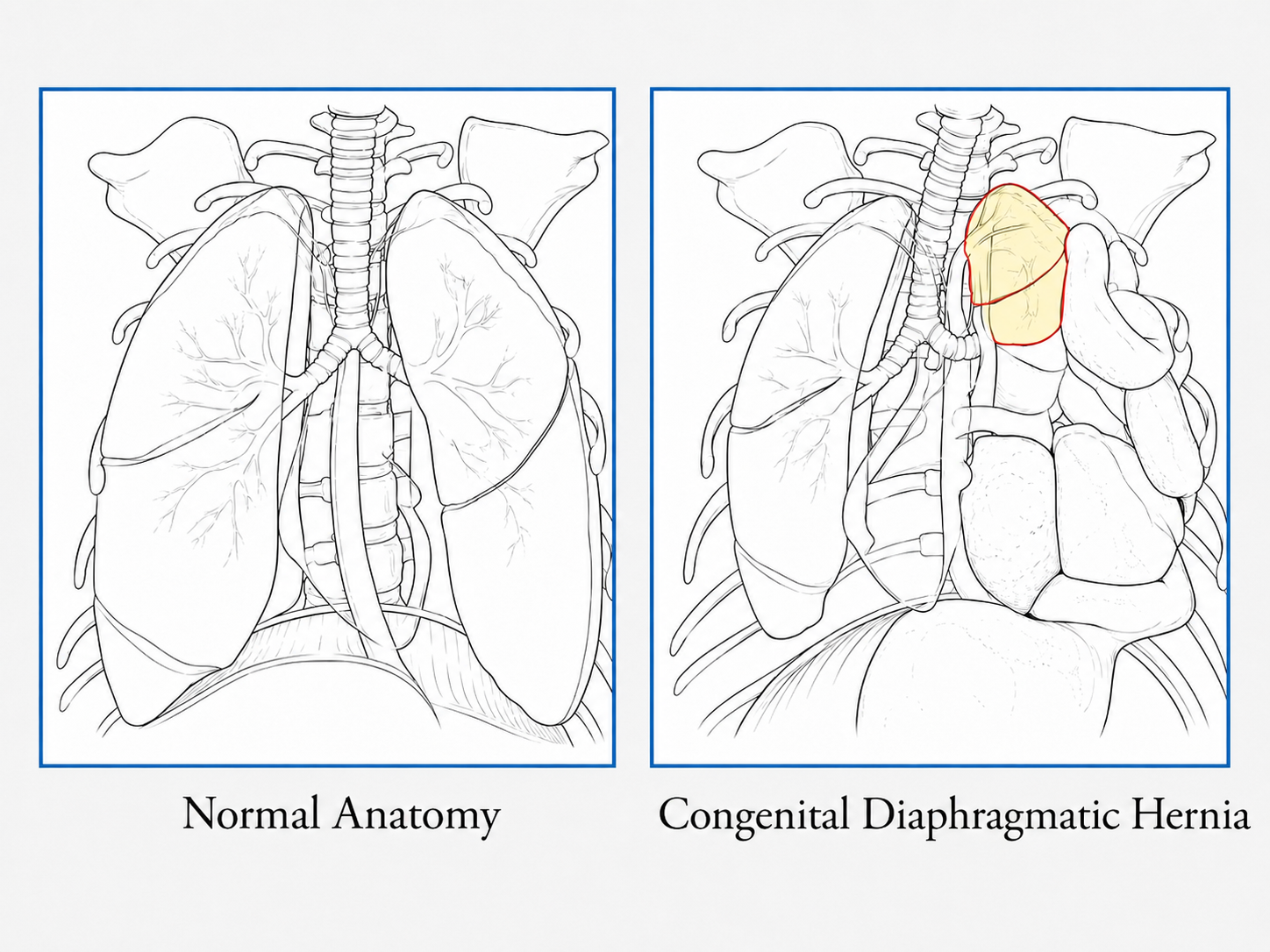
Normal anatomy vs CDH anatomy
Mhamed Hussein Mohammed Alahmadi BSc, MBBS, MS, MBA, CPHE
References
Dumpa V, Chandrasekharan P. Congenital Diaphragmatic Hernia. StatPearls. 2026 Jan:(): [PubMed PMID: 32310536]
Canadian Congenital Diaphragmatic Hernia Collaborative, Puligandla PS, Skarsgard ED, Offringa M, Adatia I, Baird R, Bailey M, Brindle M, Chiu P, Cogswell A, Dakshinamurti S, Flageole H, Keijzer R, McMillan D, Oluyomi-Obi T, Pennaforte T, Perreault T, Piedboeuf B, Riley SP, Ryan G, Synnes A, Traynor M. Diagnosis and management of congenital diaphragmatic hernia: a clinical practice guideline. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2018 Jan 29:190(4):E103-E112. doi: 10.1503/cmaj.170206. Epub [PubMed PMID: 29378870]
Level 1 (high-level) evidenceChandrasekharan PK, Rawat M, Madappa R, Rothstein DH, Lakshminrusimha S. Congenital Diaphragmatic hernia - a review. Maternal health, neonatology and perinatology. 2017:3():6. doi: 10.1186/s40748-017-0045-1. Epub 2017 Mar 11 [PubMed PMID: 28331629]
Hedrick HL. Management of prenatally diagnosed congenital diaphragmatic hernia. Seminars in fetal & neonatal medicine. 2010 Feb:15(1):21-7. doi: 10.1016/j.siny.2009.07.012. Epub 2009 Nov 2 [PubMed PMID: 19884051]
Nio M, Haase G, Kennaugh J, Bui K, Atkinson JB. A prospective randomized trial of delayed versus immediate repair of congenital diaphragmatic hernia. Journal of pediatric surgery. 1994 May:29(5):618-21 [PubMed PMID: 8035269]
Level 1 (high-level) evidenceSnoek KG, Reiss IK, Greenough A, Capolupo I, Urlesberger B, Wessel L, Storme L, Deprest J, Schaible T, van Heijst A, Tibboel D, CDH EURO Consortium. Standardized Postnatal Management of Infants with Congenital Diaphragmatic Hernia in Europe: The CDH EURO Consortium Consensus - 2015 Update. Neonatology. 2016:110(1):66-74. doi: 10.1159/000444210. Epub 2016 Apr 15 [PubMed PMID: 27077664]
Level 3 (low-level) evidenceAntounians L, Zani A. Beyond the diaphragm and the lung: a multisystem approach to understanding congenital diaphragmatic hernia. Pediatric surgery international. 2023 May 9:39(1):194. doi: 10.1007/s00383-023-05471-5. Epub 2023 May 9 [PubMed PMID: 37160490]
Level 3 (low-level) evidenceFoglia EE, Ades A, Hedrick HL, Rintoul N, Munson DA, Moldenhauer J, Gebb J, Serletti B, Chaudhary A, Weinberg DD, Napolitano N, Fraga MV, Ratcliffe SJ. Initiating resuscitation before umbilical cord clamping in infants with congenital diaphragmatic hernia: a pilot feasibility trial. Archives of disease in childhood. Fetal and neonatal edition. 2020 May:105(3):322-326. doi: 10.1136/archdischild-2019-317477. Epub 2019 Aug 28 [PubMed PMID: 31462406]
Level 2 (mid-level) evidenceMetkus AP, Filly RA, Stringer MD, Harrison MR, Adzick NS. Sonographic predictors of survival in fetal diaphragmatic hernia. Journal of pediatric surgery. 1996 Jan:31(1):148-51; discussion 151-2 [PubMed PMID: 8632269]
Level 2 (mid-level) evidenceJani J, Nicolaides KH, Keller RL, Benachi A, Peralta CF, Favre R, Moreno O, Tibboel D, Lipitz S, Eggink A, Vaast P, Allegaert K, Harrison M, Deprest J, Antenatal-CDH-Registry Group. Observed to expected lung area to head circumference ratio in the prediction of survival in fetuses with isolated diaphragmatic hernia. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2007 Jul:30(1):67-71 [PubMed PMID: 17587219]
Level 2 (mid-level) evidenceJani J, Nicolaides KH, Benachi A, Moreno O, Favre R, Gratacos E, Deprest J. Timing of lung size assessment in the prediction of survival in fetuses with diaphragmatic hernia. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2008 Jan:31(1):37-40 [PubMed PMID: 18069722]
Level 2 (mid-level) evidenceShue EH, Miniati D, Lee H. Advances in prenatal diagnosis and treatment of congenital diaphragmatic hernia. Clinics in perinatology. 2012 Jun:39(2):289-300. doi: 10.1016/j.clp.2012.04.005. Epub [PubMed PMID: 22682380]
Level 3 (low-level) evidenceZani A, Chung WK, Deprest J, Harting MT, Jancelewicz T, Kunisaki SM, Patel N, Antounians L, Puligandla PS, Keijzer R. Congenital diaphragmatic hernia. Nature reviews. Disease primers. 2022 Jun 1:8(1):37. doi: 10.1038/s41572-022-00362-w. Epub 2022 Jun 1 [PubMed PMID: 35650272]
Deprest J, Brady P, Nicolaides K, Benachi A, Berg C, Vermeesch J, Gardener G, Gratacos E. Prenatal management of the fetus with isolated congenital diaphragmatic hernia in the era of the TOTAL trial. Seminars in fetal & neonatal medicine. 2014 Dec:19(6):338-48. doi: 10.1016/j.siny.2014.09.006. Epub 2014 Nov 11 [PubMed PMID: 25447987]
Snoek KG, Capolupo I, van Rosmalen J, Hout Lde J, Vijfhuize S, Greenough A, Wijnen RM, Tibboel D, Reiss IK, CDH EURO Consortium. Conventional Mechanical Ventilation Versus High-frequency Oscillatory Ventilation for Congenital Diaphragmatic Hernia: A Randomized Clinical Trial (The VICI-trial). Annals of surgery. 2016 May:263(5):867-74. doi: 10.1097/SLA.0000000000001533. Epub [PubMed PMID: 26692079]
Level 1 (high-level) evidenceJani JC, Nicolaides KH, Gratacós E, Valencia CM, Doné E, Martinez JM, Gucciardo L, Cruz R, Deprest JA. Severe diaphragmatic hernia treated by fetal endoscopic tracheal occlusion. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2009 Sep:34(3):304-10. doi: 10.1002/uog.6450. Epub [PubMed PMID: 19658113]
Belfort MA, Olutoye OO, Cass DL, Olutoye OA, Cassady CI, Mehollin-Ray AR, Shamshirsaz AA, Cruz SM, Lee TC, Mann DG, Espinoza J, Welty SE, Fernandes CJ, Ruano R. Feasibility and Outcomes of Fetoscopic Tracheal Occlusion for Severe Left Diaphragmatic Hernia. Obstetrics and gynecology. 2017 Jan:129(1):20-29. doi: 10.1097/AOG.0000000000001749. Epub [PubMed PMID: 27926636]
Level 2 (mid-level) evidenceAl-Maary J, Eastwood MP, Russo FM, Deprest JA, Keijzer R. Fetal Tracheal Occlusion for Severe Pulmonary Hypoplasia in Isolated Congenital Diaphragmatic Hernia: A Systematic Review and Meta-analysis of Survival. Annals of surgery. 2016 Dec:264(6):929-933 [PubMed PMID: 26910202]
Level 1 (high-level) evidenceHutcheon JA, Butler B, Lisonkova S, Marquette GP, Mayer C, Skoll A, Joseph KS. Timing of delivery for pregnancies with congenital diaphragmatic hernia. BJOG : an international journal of obstetrics and gynaecology. 2010 Dec:117(13):1658-62 [PubMed PMID: 21125710]
. Inhaled nitric oxide and hypoxic respiratory failure in infants with congenital diaphragmatic hernia. The Neonatal Inhaled Nitric Oxide Study Group (NINOS). Pediatrics. 1997 Jun:99(6):838-45 [PubMed PMID: 9190553]
Level 1 (high-level) evidenceVan Meurs K, Congenital Diaphragmatic Hernia Study Group. Is surfactant therapy beneficial in the treatment of the term newborn infant with congenital diaphragmatic hernia? The Journal of pediatrics. 2004 Sep:145(3):312-6 [PubMed PMID: 15343181]
Lally KP, Lally PA, Langham MR, Hirschl R, Moya FR, Tibboel D, Van Meurs K, Congenital Diaphragmatic Hernia Study Group. Surfactant does not improve survival rate in preterm infants with congenital diaphragmatic hernia. Journal of pediatric surgery. 2004 Jun:39(6):829-33 [PubMed PMID: 15185206]
Level 2 (mid-level) evidenceHarting MT, Lally KP. The Congenital Diaphragmatic Hernia Study Group registry update. Seminars in fetal & neonatal medicine. 2014 Dec:19(6):370-5. doi: 10.1016/j.siny.2014.09.004. Epub 2014 Oct 11 [PubMed PMID: 25306471]
Yamoto M, Nagata K, Terui K, Hayakawa M, Okuyama H, Amari S, Yokoi A, Masumoto K, Okazaki T, Inamura N, Toyoshima K, Koike Y, Yazaki Y, Furukawa T, Usui N. Long-Term Outcomes of Congenital Diaphragmatic Hernia: Report of a Multicenter Study in Japan. Children (Basel, Switzerland). 2022 Jun 8:9(6):. doi: 10.3390/children9060856. Epub 2022 Jun 8 [PubMed PMID: 35740795]
Level 2 (mid-level) evidenceAmerican Academy of Pediatrics Section on Surgery, American Academy of Pediatrics Committee on Fetus and Newborn, Lally KP, Engle W. Postdischarge follow-up of infants with congenital diaphragmatic hernia. Pediatrics. 2008 Mar:121(3):627-32. doi: 10.1542/peds.2007-3282. Epub [PubMed PMID: 18310215]
Jancelewicz T, Lucke A, Guillory C, Section on Surgery, Committee on Fetus and Newborn. Postdischarge Follow-Up of Infants With Congenital Diaphragmatic Hernia: Clinical Report. Pediatrics. 2026 Feb 1:157(2):. pii: e2025074114. doi: 10.1542/peds.2025-074114. Epub [PubMed PMID: 41581796]
Ali K, Nandunjappa M, Homedi A, Arattu Thodika FM, Subba-Rao R, Almahdi M, Alsaif S, Ali I, Bhat R, Harris C, Dassios T, Greenough A. Early post-operative hemodynamic recovery in infants with congenital diaphragmatic hernia. European journal of pediatrics. 2026 Apr 20:185(5):. doi: 10.1007/s00431-026-06907-5. Epub 2026 Apr 20 [PubMed PMID: 42008013]
Toyoshima K, Saito T, Katsumata K, Shimokaze T, Kishigami M, Kimura S, Aoki H, Ohmura J, Shibasaki J, Kawataki M, Mochizuki K, Kitagawa N, Saito N, Masutani S. Perioperative biventricular function in congenital diaphragmatic hernia: a three-dimensional echocardiographic study. Pediatric research. 2026 Apr 24:():. doi: 10.1038/s41390-026-04970-0. Epub 2026 Apr 24 [PubMed PMID: 42032188]
Ting JY, Sehgal A, Kuan MTY, Soraisham A, Vorhies E, Castaldo M, McNamara PJ. Echocardiographic predictors of adverse outcomes in infants with congenital diaphragmatic hernia. Journal of perinatology : official journal of the California Perinatal Association. 2026 Jun:46(6):1020-1026. doi: 10.1038/s41372-026-02670-5. Epub 2026 Apr 14 [PubMed PMID: 41981122]