Introduction
Diabetes mellitus poses a major global health challenge, contributing substantially to morbidity, mortality, and economic strain. In addition to acute and chronic complications, diabetic foot ulcers cause significant disability and loss of quality of life while contributing heavily to overall morbidity and mortality. As many as one-third of individuals with diabetes develop foot ulcers during their lifetime, making this condition the leading cause of atraumatic lower extremity amputations worldwide.[1][2]
Foot ulcers in patients with diabetes arise from a complex interaction of peripheral neuropathy, peripheral arterial disease (PAD), and impaired wound healing, frequently exacerbated by infection.[3] Beyond localized tissue damage, diabetic foot ulceration reflects widespread systemic vascular disease and heightens the risk of cardiovascular morbidity and premature mortality.[4][5] Major lower extremity amputation is associated with significant morbidity and mortality, with postamputation 5-year mortality rates exceeding 50% in patients with diabetes.[6]
Several factors predict poor outcomes in individuals with diabetic foot ulcers, including ulcer severity, prolonged duration, infection, PAD, neuropathy, chronic kidney disease, cardiovascular disease, smoking, and male gender. These variables influence healing rates, recurrence, and the likelihood of progression to major amputation and death.[1][7][8][9][10]
Effective management of diabetic foot ulcers and their complications demands a comprehensive, evidence-based strategy. Essential interventions include pressure offloading, infection control, revascularization, surgical intervention, glycemic control optimization, and management of comorbidities. Because of the condition’s multifactorial nature, patients achieve better outcomes when treated through coordinated, interprofessional care.[11][12][13][14]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Ulcer Classification
Foot ulcers in individuals with diabetes primarily develop from neuropathy, ischemia, or a combination of both. They fall into 3 main categories: neuropathic, ischemic, and neuro-ischemic ulcers.
Neuropathic ulcers
Neuropathic ulcers result from peripheral neuropathy and commonly appear on the plantar surface, especially at pressure points, eg, the metatarsal heads and heel. These ulcers present as painless lesions with punched-out edges surrounded by callus (see Images. Diabetic Foot Ulcer and Neuropathic Ulceration). Their development reflects the combined effects of sensory and motor neuropathy, leading to abnormal pressure distribution across the foot. Neuropathy contributes to 60% to 70% of diabetic foot ulcers. Patients with sensory neuropathy fail to perceive minor trauma, allowing injuries to progress untreated in the setting of diminished pain sensation.[1][11]
Ischemic ulcers
Ischemic ulcers arise from PAD and usually occur on the tips of the toes or lateral borders of the feet. These ulcers tend to be painful, with irregular margins, pale skin, and cold extremities accompanied by absent peripheral pulses. PAD accounts for up to 50% of diabetic foot ulcers.[7][11][15]
Neuro-ischemic ulcers
Neuro-ischemic ulcers develop when both neuropathy and PAD coexist. They occur more frequently in older patients with long-standing diabetes and multiple comorbidities. The ulcer’s location depends on which factor predominates, and pain intensity varies between patients.[11][16][17]
Diabetic Foot Ulceration Risk Factors
Peripheral neuropathy represents a major risk factor for diabetic foot ulcers.[17] Motor neuropathy distorts normal foot anatomy, producing claw and hammer toe deformities, contracted medial arches (pes cavus), and prominent metatarsal heads, which lead to callus formation and plantar ulceration. Sensory neuropathy eliminates protective sensation, preventing awareness of pain, pressure, and temperature changes; repetitive micro-trauma then results in skin breakdown, significantly increasing the risk of ulcer development.[18][19] Autonomic neuropathy further contributes to reduced sweating, promoting dry, fissured skin, impaired microvascular regulation, and arteriovenous shunting, which increases vulnerability to ulceration and infection.[17]
PAD doubles in prevalence among patients with diabetes compared to the general population and serves as a strong predictor of ulcer formation and poor healing. Diminished distal vascularization independently heightens the risk of ulcer formation, particularly when combined with neuropathy.[20] Decreased lower-extremity perfusion also correlates with increased risk of ulceration. Intersocietal guidelines recommend routine PAD screening and risk-based follow-up to improve early detection and management.[21]
Chronic kidney disease (CKD) independently increases the likelihood of diabetic foot ulcers. Over one-third of individuals with diabetes develop CKD, and up to one-third of those individuals experience a foot ulcer during their lifetime. CKD elevates ulcer risk through higher rates of neuropathy, PAD, and immune dysfunction.[22] Dialysis further increases the prevalence to 21%, compared with 5% among those not on dialysis.[23] Patients with stage 4 and 5 CKD or those on dialysis face a 10- to 15-fold increase in major amputation risk.[24] Regular skin surveillance remains essential for individuals with end-stage renal disease.[25]
Additional risk factors include prolonged duration of diagnosed diabetes, poor glycemic control, history of prior ulcer or amputation, older age, male sex, elevated body mass index, hypertension, and hyperlipidemia.[26][18] Each comorbidity compounds the risk of ulcer formation and impedes healing, underscoring the need for proactive, interprofessional prevention and management strategies.
Epidemiology
Foot ulcers among individuals with diabetes represent a common and serious global health problem with significant clinical consequences. A 2017 systematic review of data from 16 countries reported a prevalence of 6.3%. Lifetime risk estimates for diabetic foot ulcers range from 19% to 34%.[1] Prevalence varies widely by region, with North America recording the highest rate (13%) and Oceania the lowest (3%). In Africa, the prevalence reached 7.2%, while 5.5% prevalnce was observed in Asia. Within the United States, Medicare fee-for-service data revealed a point prevalence of 8% among individuals with diabetes, with variation across regions and ethnic groups. The highest rates occurred among American Indian, Black, and Hispanic populations. Foot ulcers also occur more frequently in men (4.5%) than in women (3.5%). Patients with type 2 diabetes show a higher prevalence of 6.4%, compared with 5.5% in those with type 1 diabetes.[2]
The risk of ulcer recurrence remains high, reaching 42% after 1 year and 65% after 5 years.[1] Mortality following a diabetic foot ulcer is considerable, with meta-analyses showing a 5-year mortality rate of approximately 50%. Patients undergoing major amputation face an even higher risk of death.[6][27] As global diabetes prevalence continues to rise, the total number of foot ulcer cases is expected to increase further, particularly in regions where access to interprofessional foot care teams remains limited.
Pathophysiology
Foot ulcers in individuals with diabetes develop through a complex interaction of neuropathy, abnormal foot biomechanics, PAD, impaired wound healing, and infection.[28] Hyperglycemic-driven metabolic and vascular injury results in loss of protective sensation, dry skin, muscle wasting, foot deformities, and elevated plantar pressures.[28] Increased plantar pressure combined with callus formation creates a mechanical environment highly susceptible to ulceration.[29]
PAD occurs frequently among people with diabetes and accelerates tissue damage through increased vascular stiffness and reduced perfusion, ultimately contributing to ulcer formation and complications, eg, amputation.[7][30] Impaired wound healing further compounds these issues. Chronic low-grade inflammation, defective angiogenesis, fibroblast dysfunction, excessive matrix metalloproteinase activity, and accumulation of advanced glycation end products all hinder tissue repair, prolong ulcer persistence, and contribute to complications of diabetic foot ulcers.[31][32]
Infection adds another layer of complexity. Polymicrobial biofilms commonly develop within diabetic foot ulcers, reducing immune system effectiveness and preventing adequate clearance of pathogens with antibiotic treatment. These biofilms perpetuate infection and inflammation, delaying healing and heightening the risk of severe complications.[33]
Histopathology
In histopathologic analysis, diabetic foot ulcers demonstrate a constellation of changes reflecting chronic ischemia, neuropathy, repetitive trauma, and impaired wound healing. The epidermis typically shows ulceration with loss of normal stratification at the wound edge, often accompanied by hyperkeratosis and acanthosis in adjacent skin due to chronic pressure. Re-epithelialization is frequently incomplete, and keratinocyte migration is disorganized.[34]
The dermis is characterized by dense fibrocollagenous tissue with reduced and disarrayed granulation tissue formation. Fibroblasts are decreased in number and exhibit impaired proliferative activity. Capillary density is diminished, and small vessels often show basement membrane thickening, endothelial swelling, and hyaline change consistent with diabetic microangiopathy, contributing to local hypoxia.[35]
Inflammatory infiltrates are typically chronic and mixed, composed predominantly of lymphocytes, plasma cells, and macrophages, with variable neutrophilic components in the setting of secondary infection. These inflammatory cells are often dysfunctional, resulting in a prolonged inflammatory phase. Areas of necrosis and fibrin deposition are common.[36] In longstanding ulcers, deeper tissues may demonstrate myonecrosis, fat necrosis, or osteomyelitis, with trabecular bone showing inflammatory destruction and reactive sclerosis. Overall, the histopathologic features of diabetic foot ulcers reflect a failure to transition from inflammation to effective tissue repair, underlying their chronicity and propensity for infection.
History and Physical
Clinical History
A holistic assessment of every patient with diabetes presenting with a foot ulcer is the foundation of effective management. The evaluation begins with a detailed history that captures the ulcer’s location, duration, and precipitating cause (eg, trauma, barefoot ambulation). Clinicians should inquire about ulcer discharge, odor, and pain, as well as systemic symptoms, including fever, rigors, and malaise. Previous foot ulcers, antibiotic exposure, and any history of minor or major amputations or vascular surgery (eg, lower limb angioplasty or bypass procedures) must be documented.
A thorough diabetes history should identify the type and duration of diabetes and any associated complications. Microvascular complications include retinopathy and neuropathy, while macrovascular conditions may involve cerebrovascular accidents, transient ischemic attacks, carotid artery disease, ischemic heart disease, and PAD. Glycemic control requires careful review, including frequency of hypoglycemic episodes, osmotic symptoms, and any episodes of diabetic ketoacidosis (DKA) or hyperglycemic hyperosmolar state. Medication use, particularly sodium-glucose cotransporter 2 (SGLT2) inhibitors, antiplatelet agents, statins, and anticoagulants, should be noted, along with adherence to therapeutic footwear or offloading devices.
The history must also explore neuropathic symptoms, including hypoesthesia, hyperesthesia, paresthesia, dysesthesia, or anesthesia, and PAD-related symptoms (intermittent claudication, rest pain, and nonhealing ulcers). Smoking status and pack-year history, alcohol consumption, occupation, mobility, use of walking aids, and visual acuity require documentation. Medical comorbidities, eg, congestive heart failure or renal failure, can contribute to leg edema and must be addressed to optimize healing. The history concludes with an understanding of the patient’s ideas, concerns, and expectations to support patient-centered care.
Clinical Examination
A meticulous clinical examination follows. The lower limbs should be exposed from the knees to the toes and compared bilaterally. Inspection focuses on pallor, cyanosis, dependent rubor, mottling, edema, callus, corns, fissures, tinea pedis, and gangrene. Scars from revascularization or amputations, along with trophic changes, eg, hair loss, atrophic skin, muscle wasting, and nail deformities, should be noted. Interdigital maceration, heel cracks, and deformities, including claw toes, hammer toes, hallux valgus, pes cavus, and pes planus, require attention. Furthermore, signs of Charcot neuroarthropathy, including midfoot collapse, rocker-bottom deformity, bony prominence, erythema, and increased warmth, must be assessed.
Additionally, the ulcer should be described in detail, noting its location, number, size, shape, edge, base, and surrounding callus (see Image. Diabetic Ulcer). The ulcer base may reveal granulation tissue, slough, necrosis, or exposed tendon, bone, or joint capsule. Edges may appear punched out, undermined, or macerated, while the surrounding skin may display erythema, warmth, induration, or edema. Exudate type and quantity—serous, purulent, or serosanguineous—should be recorded. The probe-to-bone test helps identify osteomyelitis when a gritty or bony resistance is felt. Sensory testing includes assessment of light touch, pinprick, vibration, joint position, and monofilament sensation.
Palpation should assess temperature, tenderness, and soft-tissue swelling, distinguishing between localized and diffuse edema. Peripheral pulses (dorsalis pedis, posterior tibial, popliteal, and femoral) must be palpated bilaterally, along with the abdomen, to detect an expansile pulsation suggestive of an abdominal aortic aneurysm. Charcot neuroarthropathy typically presents as a red, hot, swollen foot with bounding pulses and neuropathy, usually without ulceration. Chronic cases often present with foot deformity, strong pulses, and sensory loss. Examination also includes assessment of footwear and offloading techniques (eg, total contact casts, walkers, or insoles). Evaluation of the cardiovascular system helps identify heart failure contributing to extremity edema, while renal and liver assessment assist in detecting other causes of swelling.
Diabetic Ulcer Classification Systems
Several classification systems support standardized assessment of ulcer severity and infection.
IWGDF/IDSA classification
The International Working Group on the Diabetic Foot (IWGDF)/Infectious Diseases Society of America (IDSA) classification grades infection severity as follows:
- Grade 1: uninfected ulcers with no local or systemic signs
- Grade 2: mild infection with erythema ≤2 cm
- Grade 3: moderate infection with deeper involvement of muscle, joint, or bone, or erythema >2 cm without systemic toxicity
- Grade 4: severe infection with systemic inflammatory response [37]
SINBAD score
The SINBAD score (site, ischemia, neuropathy, bacterial infection, and depth) provides a simple bedside tool for evaluating ulcer severity. Each domain receives a score of 0 or 1, yielding a total between 0 and 6. Higher scores correspond to worse healing rates and increased risk of amputation. Standardized documentation using SINBAD enhances audit and communication.[38]
WIfI system
The WIfI (Wound, Ischemia, foot Infection) system assigns scores from 0 to 3 across its domains and groups them into stages 1 to 4, estimating the 1-year risk of major amputation and the potential benefit of revascularization. A higher WIfI stage correlates with poorer healing outcomes and greater amputation risk, offering clinicians a structured approach to evaluating limb threat and guiding management decisions.[39]
Evaluation
Laboratory Studies
Laboratory evaluation plays a crucial role in the assessment of diabetic foot ulcers, particularly for detecting infection and monitoring overall patient status. A complete blood count may reveal leukocytosis, specifically neutrophilia, though this finding may be absent even in severe infections due to diabetes-related immune alterations. C-reactive protein (CRP) is a nonspecific marker of infection or inflammation and may be elevated in various diabetic foot infections; however, normal CRP values should not be used to exclude infection. Erythrocyte sedimentation rate (ESR) often rises in inflammatory conditions; values of 70 mm/hour or higher suggest osteomyelitis. Elevated procalcitonin supports the presence of bacterial infection. These inflammatory markers function as adjuncts to clinical assessment and imaging rather than as sole diagnostic criteria.[33][40][41][42]
Additionally, assessment of renal and liver function remains essential, as abnormalities may result from infection, sepsis, or antibiotic therapy. Measurement of HbA1c helps determine whether glycemic control needs to be optimized, as poor glycemic control impairs wound healing. Stress from infection may further destabilize glycemia, necessitating adjustment of oral hypoglycemic agents or escalation of insulin therapy.[43][44] Culture of suspected infected ulcers should prioritize tissue specimens obtained via curettage or biopsy for Gram staining and microbial identification. Superficial swab cultures are discouraged, and a bone biopsy should be considered if osteomyelitis is suspected and feasible.[33]
Imaging Studies
Imaging contributes significantly to diagnosis and management. Plain radiographs are indicated for ulcers extending beyond the skin, the presence of gas in soft tissue, visible bone exposure, or a positive probe-to-bone test (see Image. Right Foot Radiograph). Radiographs aid in identifying osteomyelitis, Charcot neuroarthropathy, and other pathologies (eg, fractures). However, early bone infection may not be detected, warranting magnetic resonance imaging (MRI) evaluation.[45] MRI provides a detailed assessment of osteomyelitis, deep soft-tissue infections, abscesses, septic arthritis, and Charcot neuroarthropathy when x-ray findings are inconclusive (see Image. Right Foot Osteomyelitis). Advanced imaging, including radionuclide scans or positron emission tomography (PET), may occasionally be required for confirmation.[33][45]
Evaluation of Peripheral Artery Disease
Evaluation of PAD utilizes multiple modalities (see Image. Peripheral Arterial Disease). Pedal Doppler waveform analysis, ankle-brachial index (ABI), and toe-brachial index (TBI) provide an initial noninvasive assessment. PAD is less likely with ABI values between 0.9 and 1.3, TBI 0.70 or greater, and triphasic or biphasic pedal waveforms. Low ankle pressures (<50 mm Hg) or ABI less than 0.5 correlate with impaired healing and increased risk of major amputation.
Toe pressure measured with a pneumatic plethysmograph indicates healing probability; pressures 30 mm Hg or more improve healing odds by up to 30%, while values less than 30 mm Hg increase amputation likelihood by approximately 20%. Transcutaneous oxygen pressure (TcPO2) provides an alternative assessment when toe pressures cannot be obtained; TcPO2 values of 25 mm Hg or higher increase the probability of healing by 45%, and values below 25 mm Hg increase the risk of major amputation by 20%.[7]
ABI may be falsely elevated in patients with diabetes due to vessel calcification, making toe pressures, TBI, and TcPO2 preferred measures. When revascularization is considered, imaging of the arterial system from the aorta to the pedal arch using computed tomography (CT) angiography, magnetic resonance angiography (MRA), or catheter-based digital subtraction angiography offers precise anatomical detail to guide intervention.[46][47]
Treatment / Management
Diabetic Foot Ulcer Management
Management of foot ulcers and their complications requires a structured, evidence-based approach coordinated by an interprofessional diabetic foot team. Early referral is recommended following systematic evaluation, with urgent consultation warranted in cases of ischemia or moderate-to-severe infection.[33]
Offloading remains the cornerstone of treatment for neuropathic plantar ulcers. For forefoot and midfoot ulcers, nonremovable knee-high devices, eg, total contact casts or nonremovable walkers, provide optimal pressure relief.[25][29] Regular sharp debridement of callus and necrotic tissue promotes healing, while dressings should be selected according to wound status, exudate level, patient-specific factors, and cost-effectiveness.[28](B3)
Antibiotic therapy is indicated only when clinical infection is present. Mild soft-tissue infections typically require 1 to 2 weeks of oral therapy, whereas moderate-to-severe infections often require 4 to 6 weeks of intravenous therapy, often initiated in a hospital setting. Treatment may be prolonged in cases with delayed resolution due to factors, eg, PAD.[33] Staphylococcus aureus predominates in mild infections, whereas severe or chronic infections are often polymicrobial, including gram-negative rods and anaerobes. Empiric therapy should cover gram-positive cocci in mild infections, with broader-spectrum antibiotics for moderate-to-severe infections or ischemic ulcers.
Management of osteomyelitis complicating foot ulcers
Osteomyelitis complicating foot ulcers may respond to medical management alone, particularly forefoot infections without PAD, exposed bone, or urgent drainage requirements, with antibiotics administered for approximately 6 weeks.[33][48] Minor amputations, eg, toe, ray, or transmetatarsal procedures, may be necessary for localized osteomyelitis, metatarsal involvement, necrotic tissue, septic arthritis, or exposed bone.[33] Following minor amputation with clean bone margins, antibiotics are recommended for 2 to 5 days, or up to 3 weeks if bone margin cultures are positive.(A1)
Urgent surgical consultation is critical for moderate-to-severe infection with necrotizing fasciitis, deep abscesses, compartment syndrome, severe limb ischemia, or gangrene (see Image. Gangrenous Ulcers). Early debridement within 24 to 48 hours, combined with antibiotic therapy, improves outcomes. Ulcers showing less than 50% area reduction within 4 weeks should prompt reassessment for PAD.[33]
Surgical interventions, eg, Achilles tendon lengthening, gastrocnemius recession, and metatarsal head resection, effectively prevent recurrence of plantar ulcers. Flexor tenotomy and hallux osteotomy address apical ulcers. Protective footwear and orthoses are essential to reduce the risk of recurrent ulceration.[29]
Peripheral artery disease management
Management of PAD requires urgent vascular evaluation for any infected ulcer with suspected ischemia or gangrene.[33] Revascularization, through endovascular angioplasty or bypass surgery, is indicated for significant arterial stenosis or critical limb ischemia, with decisions guided by vascular anatomy and patient comorbidities.[7][46] Major below-knee amputation may become necessary when infection and ischemia persist despite optimal medical, surgical, and vascular interventions.[33] Optimizing glycemic control, maintaining blood pressure within target ranges, and initiating statins and antiplatelet therapy are fundamental to improving outcomes and preventing recurrence.
Differential Diagnosis
Clinicians managing patients with diabetes must maintain a broad diagnostic perspective and consider alternative causes of foot and leg ulcers, guided by clinical presentation. Complications commonly linked to diabetes, eg, neuropathy and PAD, often coexist with other conditions and hinder healing, underscoring the need for comprehensive evaluation.
Pressure Ulcers
Pressure ulcers arise from prolonged immobility or poorly fitting footwear and typically develop over bony prominences, eg, the heel or lateral malleolus. Neuropathy and leg edema, particularly in older adults or bedbound individuals, heighten susceptibility to these ulcers. Preventive strategies rely on adequate offloading of pressure using simple assistive devices to avoid complications, eg, infection, sepsis, or osteomyelitis.[49]
Vasculitis and Autoimmune Conditions
Vasculitis and autoimmune disorders, including polyarteritis nodosa (PAN), anti-neutrophil cytoplasmic antibody (ANCA)–associated vasculitis, rheumatoid arthritis, scleroderma, and antiphospholipid syndrome, may contribute to ulcer formation. Such ulcers often appear in multiple sites across the lower legs and feet. Vasculitic processes account for up to 5% of cutaneous ulcers.[50][51] Pyoderma gangrenosum, a neutrophilic dermatosis associated with ulceration, begins as a pustule or bulla that progresses to a purulent ulcer with necrotic edges and surrounding erythema.[52] This condition frequently occurs in association with inflammatory bowel disease or ankylosing spondylitis.
Venous Leg Ulcers
Venous leg ulcers are the most common type of leg ulcer, affecting up to 3% of individuals older than 65 years. These ulcers usually occupy the gaiter region, most often above the medial malleolus, and result from chronic venous insufficiency and venous hypertension. They present as shallow wounds with irregular borders, sloping edges, and a yellow fibrinous base (see Images. Venous Leg Ulcer and Venous Stasis Ulcer). Accompanying features often include varicose veins, hyperpigmentation, and lipodermatosclerosis. When a person with diabetes presents with gaiter-area ulcers, evaluation for venous insufficiency and varicosities becomes essential.[53]
Necrobiosis Lipoidica Diabeticorum
Necrobiosis lipoidica diabeticorum, often called shin spots, manifests as purplish-red papules or plaques on the shins that may become atrophic and yellow over time (see Image. Necrobiosis Lipoidica). This uncommon condition affects approximately 0.3% to 1.2% of individuals with diabetes. Lesions are generally asymptomatic and rarely require specific treatment.[54]
Prognosis
Healing of foot ulcers in individuals with diabetes depends on multiple clinical variables that shape both recovery and long-term outcomes. Poor prognostic indicators include the presence of PAD, extended ulcer duration, and multiple ulcers at initial presentation.[1][8] Nonmodifiable factors, eg, bony deformities—including prominent metatarsal heads or pes cavus—heighten the risk of recurrence and correlate with unfavorable results.[9] Ischemic ulcers generally predict poorer healing than neuropathic ulcers because of diminished perfusion and increased infection risk (see Image. Diabetic Neuropathic Ulcer).[7] Optimizing modifiable elements, eg, glycemic control, effective offloading, and management of comorbidities (eg, edema related to heart failure or renal disease), remains critical for promoting wound closure and recovery.[10]
Risk of Amputation
People with diabetes have a 10- to 20-fold higher likelihood of lower-limb amputation compared with the nondiabetic population.[15][55] Predictors of amputation include demographic and clinical features (eg, male gender, smoking, elevated body mass index, and advanced age).[15][56] Comorbidities, including PAD, neuropathy, chronic kidney disease, dependence on haemodialysis, and cardiovascular disease, further elevate risk.[15] Ulcer severity and infection play decisive roles; advanced lesions, gangrene, or severe infection greatly increase the likelihood of limb loss.[57]
Cardiovascular Outcomes and Mortality
The presence of diabetic foot ulcers often reflects widespread vascular pathology. Individuals with both diabetes and foot ulcers face markedly higher risks of ischemic heart disease, cerebrovascular accidents, and overall cardiovascular mortality compared with those without ulcers.[58] These patients experience significant mortality rates—approximately 15% within 12 months of ulcer onset and a 60% reduction in 5-year survival. Cardiovascular disease accounts for most deaths within this group.[8] Age, smoking, PAD, neuropathy, chronic kidney disease, and established cardiovascular disease all predict higher mortality.[4][8] Moreover, ulcer severity itself serves as an independent prognostic marker for mortality, highlighting the systemic nature of diabetic foot disease and its close link with vascular health.[4][57]
Complications
Foot ulcers in individuals with diabetes are associated with various complications, including:
- Infected ulcer and cellulitis (occur in over half of all foot ulcers) [59]
- Abscess
- Bacteremia/sepsis
- Osteomyelitis (common complication seen in up to 50% of foot ulcers) [60]
- Gangrene [16][61][8]
- Minor and major amputation (occurs in up to 30% of foot ulcer cases) [8][15][55][56]
- Poor glycemic control [43][44]
- Impaired quality of life
- Increased mortality [8][58]
Postoperative and Rehabilitation Care
Postoperative management following surgical intervention in diabetic patients demands careful optimization of blood glucose levels, maintaining values between 100 and 180 mg/dL (5.6–10.0 mmol/L). Medication review forms a critical part of preparation, with SGLT2 inhibitors withheld for 3 days prior to surgery to reduce the risk of euglycemic DKA. These agents can be restarted once the surgical wound or ulcer has fully healed.[7]
Antibiotic use after surgery requires precision and clinical judgment. Since multiple factors contribute to the development of diabetic foot ulcers, antibiotics should be prescribed only when clinical signs of infection are present.[33] Following endovascular revascularisation, dual antiplatelet therapy (commonly aspirin and clopidogrel) is typically recommended for up to 6 months, after which single antiplatelet therapy may suffice.[7][62]
Debridement, callus removal, and wound irrigation remain central to ulcer management. Negative-pressure wound therapy (NPWT) benefits wounds left to heal by secondary intention, achieving superior healing rates compared with standard care.[63] Simple bedside tests, including toe pressure and TcPO2 measurements, can guide assessment of wound-healing potential and the need for further revascularization.[7][28]
Proper offloading remains essential to postoperative recovery. Use of postoperative shoes, moulded insoles, total contact casts, or removable total contact footwear enhances healing and prevents recurrent injury. Orthotist involvement at multiple stages—from initial presentation to ulcer resolution—ensures optimal support. Once healing occurs, patients should receive therapeutic footwear, including bespoke shoes or custom insoles, which reduce plantar pressure and prevent recurrence, particularly in individuals with neuropathy or structural deformities.[29] Early outpatient follow-up with the interprofessional team ensures coordinated care and timely intervention.[28] Safety-net advice must always accompany discharge, clearly outlining when and where to seek urgent medical attention.
Because individuals with diabetes and foot ulcers face high cardiovascular mortality, addressing modifiable risk factors remains a central goal. Education, specialist input (eg, dietitian consultation), weight reduction through dietary and exercise measures, and pharmacologic interventions with GLP-1 agonists all contribute to improved cardiovascular outcomes. Use of SGLT2 inhibitors and GLP-1 agonists, when appropriate, further reduces cardiovascular mortality and enhances long-term prognosis.[64][65]
Consultations
Early detection and interprofessional management reduce short-term and long-term complications, including amputations and mortality.[12][13][14] The core members of the interprofessional team include the endocrinologist, vascular surgeon, orthopaedic surgeon, podiatrist, orthotist, and the limb rehabilitation team. Regular input is needed from the microbiologist, interventional radiologist, and sometimes from the plastic surgeon.
Deterrence and Patient Education
Preventing diabetic foot ulcers demands early identification of risk factors and consistent patient engagement. Education should focus on daily foot inspection, prompt reporting of blisters, calluses, or other skin changes, and proper foot hygiene. Patients must understand the importance of maintaining optimal glycemic control to reduce the risk of neuropathy and vascular complications. Regular podiatric or orthopedic evaluation, nail care by trained professionals, and the use of well-fitting, cushioned footwear significantly reduce the likelihood of ulcer development. Individuals with previous ulcers or deformities require ongoing follow-up and protective offloading devices to prevent recurrence. Teaching patients to avoid barefoot walking and exposure to extreme temperatures further limits trauma and skin breakdown.
Effective patient education also extends to lifestyle modification and cardiovascular risk reduction. Encouraging smoking cessation, weight management, and regular physical activity enhances peripheral circulation and overall health.[25] Explicit instruction regarding medication adherence, including antiplatelet and lipid-lowering agents, strengthens preventive care. Interprofessional collaboration among physicians, nurses, podiatrists, orthotists, pharmacists, and diabetes educators enhances consistency in messaging and reinforces self-management behaviors. Empowering patients to recognize early warning signs and seek timely medical attention not only prevents complications, eg, infections and amputations, but also improves quality of life and long-term survival.[66]
Pearls and Other Issues
Foot ulcers frequently develop in individuals with diabetes as a consequence of neuropathy and PAD. Complications range from localized infection to severe outcomes, eg, sepsis, bacteremia, osteomyelitis, septic arthritis, gangrene, and ultimately minor or major amputation. These ulcers significantly increase both morbidity and mortality, underscoring the need for vigilance and proactive care.
Early detection and thorough assessment of foot ulcers and their complications remain vital to prevent progression. Prompt referral to an interprofessional diabetic foot team promotes optimal management, while hospital admission becomes necessary for patients presenting with moderate to severe infection, rapidly advancing tissue necrosis, systemic toxicity, or critical limb ischemia.
Several pitfalls hinder effective management. Delayed recognition of infection or ischemia accelerates tissue destruction, and failure to assess for associated PAD and osteomyelitis compromises outcomes. Empirical antibiotic use without reference to the local antibiogram often leads to suboptimal treatment, and fragmented care lacking interprofessional coordination further worsens prognosis.
Prevention relies on continuous patient education that emphasizes daily foot inspection, appropriate footwear, and early reporting of any lesions. Routine screening of high-risk individuals for neuropathy and PAD, coupled with optimization of glycemic control and lipid management, enhances protective measures. Timely correction of modifiable risk factors, eg, callus formation and structural deformities, through podiatric and orthotic intervention strengthens long-term prevention and promotes durable limb preservation.
Enhancing Healthcare Team Outcomes
Diabetic foot ulcers are one of the most serious complications of diabetes, arising from neuropathy, peripheral arterial disease, and impaired wound healing. These ulcers predispose patients to infections, osteomyelitis, gangrene, and amputation, contributing to high morbidity and mortality. Early detection, prompt referral, and comprehensive interprofessional management are vital to improving outcomes and preventing recurrence.
Effective management demands collaboration among healthcare professionals who integrate clinical expertise, communication, and shared decision-making. Physicians and advanced practitioners assess vascular and neurological status, optimize glycaemic control, and coordinate surgical or vascular interventions. Nurses provide wound care, patient education, and infection monitoring, while pharmacists ensure safe and effective use of antibiotics and cardiovascular medications. Podiatrists and orthotists play key roles in offloading pressure and preventing deformity-related recurrence. Continuous communication across the team fosters seamless transitions between inpatient and outpatient care, enhances safety, and strengthens adherence to individualized treatment plans that promote healing and limb preservation.
Media
(Click Image to Enlarge)

Diabetic Foot Ulcer. Neuropathic ulceration in a patient with diabetes. Note periwound callous formation. Wagner Grade 2.
Contributed by MA Dreyer, DPM, FACFAS
(Click Image to Enlarge)

Necrobiosis Lipoidica. Necrobiosis lipoidica diabeticorum, often called shin spots, manifests as purplish-red papules or plaques on the shins that may become atrophic and yellow over time.
Dermatologic Institute of Jalisco, México
(Click Image to Enlarge)

Diabetic Ulcer. Diabetic ulcer due to neuropathy, vasculopathy, and foot deformity. Note periwound callous formation. Wagner Grade 2
Contributed by MA Dreyer, DPM, FACFAS
(Click Image to Enlarge)

Right Foot Osteomyelitis. This T2-weighted image shows a patient’s right foot. The patient had a history of uncontrolled diabetes, peripheral neuropathy, and a longstanding ulceration under the fifth metatarsal head, resulting in osteomyelitis of the fifth metatarsal head and shaft. The patient subsequently underwent a partial fifth ray resection with long-term intravenous antibiotics for treatment and healed uneventfully.
Contributed by AR Chambers, DPM, FACFAS
(Click Image to Enlarge)

Right Foot Radiograph. This x-ray shows a patient's right foot after undergoing a partial resection of the fifth metatarsal for acute osteomyelitis. The patient had a history of uncontrolled diabetes, peripheral neuropathy, and a chronic ulcer beneath the fifth metatarsal head, which led to osteomyelitis of the fifth metatarsal head and shaft. The patient underwent partial fifth ray resection followed by long-term intravenous antibiotic treatment and healed uneventfully.
Contributed by AR Chambers, DPM, FACFAS
(Click Image to Enlarge)

Venous Leg Ulcer. The base of the ulcer, affecting the gaiter area, shows considerable slough and scarce granulation tissue. The borders are irregular but well-defined. The surrounding skin shows hyperpigmentation, and no notable leg edema is observed.
Contributed by ADC Rodriguez-Mena, MD
(Click Image to Enlarge)

Neuropathic Ulceration. Ulceration in a patient with diabetes. Note the prior hallux amputation
Contributed by MA Dreyer, DPM, FACFAS
(Click Image to Enlarge)

Diabetic Neuropathic Ulcer. Ischemic ulcers generally predict poorer healing than neuropathic ulcers because of diminished perfusion and increased infection risk.
Contributed by S Verma, MBBS, DVD, FRCP, FAAD
(Click Image to Enlarge)

Gangrenous Ulcers. Image showing severe gangrenous changes in a patient. Urgent surgical consultation is critical for moderate-to-severe infection with necrotizing fasciitis, deep abscesses, compartment syndrome, severe limb ischemia, or gangrene.
Contributed by MA Dreyer, DPM, FACFAS
(Click Image to Enlarge)
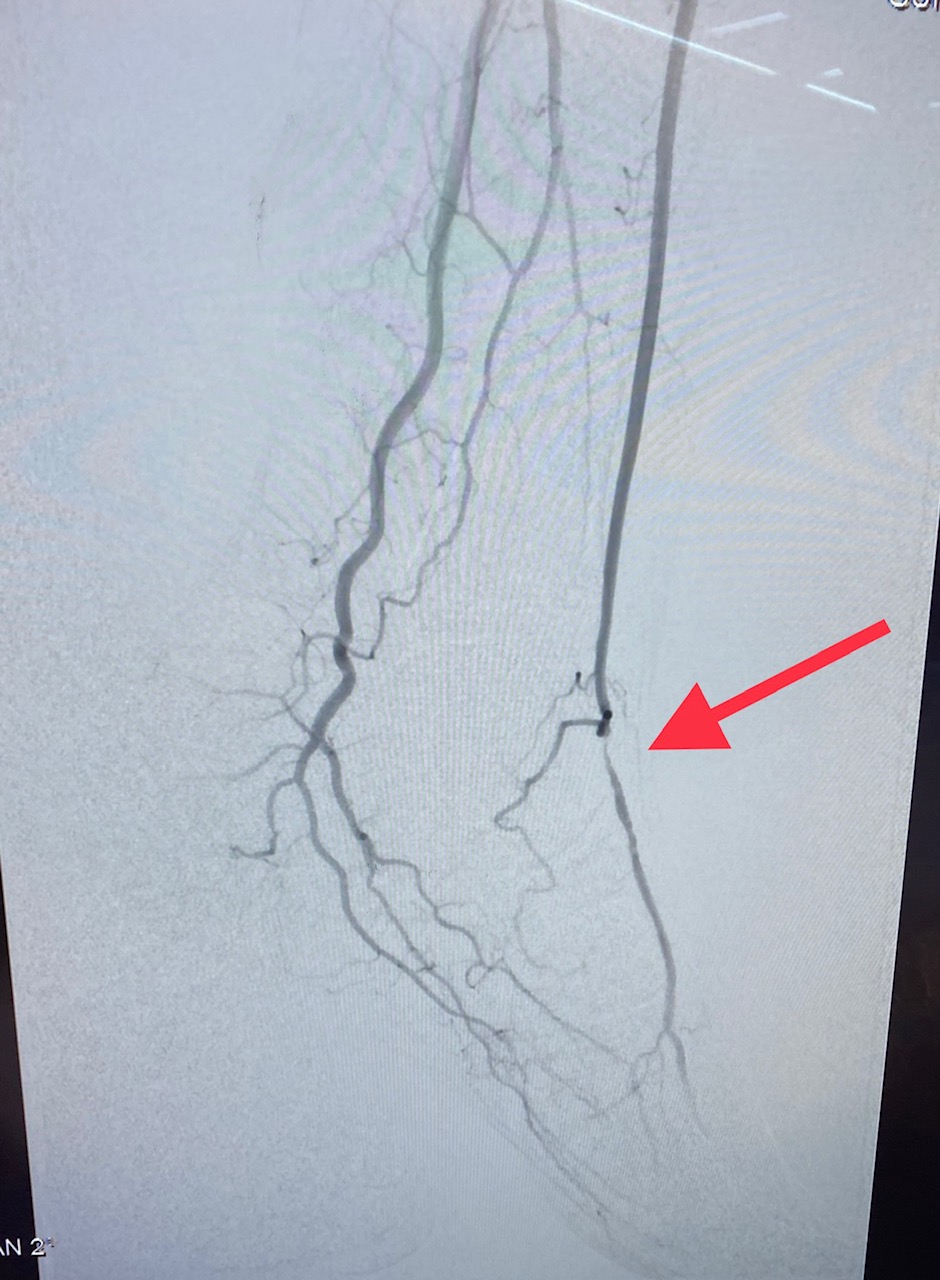
Peripheral Arterial Disease. Image showing chronic total occlusion of the left superficial femoral artery.
Contributed by MA Dreyer, DPM, FACFAS
(Click Image to Enlarge)

Venous Stasis Ulcer. Venous leg ulcers represent the most common type of leg ulcer, affecting up to 3% of persons 65 years and older. These ulcers usually occupy the gaiter region, most often above the medial malleolus, and result from chronic venous insufficiency and venous hypertension.
References
Armstrong DG, Boulton AJM, Bus SA. Diabetic Foot Ulcers and Their Recurrence. The New England journal of medicine. 2017 Jun 15:376(24):2367-2375. doi: 10.1056/NEJMra1615439. Epub [PubMed PMID: 28614678]
Zhang P, Lu J, Jing Y, Tang S, Zhu D, Bi Y. Global epidemiology of diabetic foot ulceration: a systematic review and meta-analysis (†). Annals of medicine. 2017 Mar:49(2):106-116. doi: 10.1080/07853890.2016.1231932. Epub 2016 Nov 3 [PubMed PMID: 27585063]
Level 1 (high-level) evidenceBoulton AJ, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic foot disease. Lancet (London, England). 2005 Nov 12:366(9498):1719-24 [PubMed PMID: 16291066]
Iversen MM, Tell GS, Riise T, Hanestad BR, Østbye T, Graue M, Midthjell K. History of foot ulcer increases mortality among individuals with diabetes: ten-year follow-up of the Nord-Trøndelag Health Study, Norway. Diabetes care. 2009 Dec:32(12):2193-9. doi: 10.2337/dc09-0651. Epub 2009 Sep 3 [PubMed PMID: 19729524]
Brownrigg JR, Davey J, Holt PJ, Davis WA, Thompson MM, Ray KK, Hinchliffe RJ. The association of ulceration of the foot with cardiovascular and all-cause mortality in patients with diabetes: a meta-analysis. Diabetologia. 2012 Nov:55(11):2906-12. doi: 10.1007/s00125-012-2673-3. Epub 2012 Aug 14 [PubMed PMID: 22890823]
Level 1 (high-level) evidenceArmstrong DG, Swerdlow MA, Armstrong AA, Conte MS, Padula WV, Bus SA. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. Journal of foot and ankle research. 2020 Mar 24:13(1):16. doi: 10.1186/s13047-020-00383-2. Epub 2020 Mar 24 [PubMed PMID: 32209136]
Fitridge R, Chuter V, Mills J, Hinchliffe R, Azuma N, Behrendt CA, Boyko EJ, Conte MS, Humphries M, Kirksey L, McGinigle KC, Nikol S, Nordanstig J, Rowe V, Russell D, van den Berg JC, Venermo M, Schaper N. The intersocietal IWGDF, ESVS, SVS guidelines on peripheral artery disease in people with diabetes and a foot ulcer. Diabetes/metabolism research and reviews. 2024 Mar:40(3):e3686. doi: 10.1002/dmrr.3686. Epub 2023 Sep 19 [PubMed PMID: 37726988]
Ndosi M, Wright-Hughes A, Brown S, Backhouse M, Lipsky BA, Bhogal M, Reynolds C, Vowden P, Jude EB, Nixon J, Nelson EA. Prognosis of the infected diabetic foot ulcer: a 12-month prospective observational study. Diabetic medicine : a journal of the British Diabetic Association. 2018 Jan:35(1):78-88. doi: 10.1111/dme.13537. Epub 2017 Nov 20 [PubMed PMID: 29083500]
Level 2 (mid-level) evidencevan Netten JJ, Raspovic A, Lavery LA, Monteiro-Soares M, Rasmussen A, Sacco ICN, Bus SA. Prevention of foot ulcers in the at-risk patient with diabetes: a systematic review. Diabetes/metabolism research and reviews. 2020 Mar:36 Suppl 1():e3270. doi: 10.1002/dmrr.3270. Epub 2020 Jan 19 [PubMed PMID: 31957213]
Level 1 (high-level) evidenceKilic M, Olgun N, Dündar M, Celik Advan S, Kücük FZ, Okcuoglu S, Sahin S, Kır Bicer E, Ülker Y, Sahin P, Taskiran Z. Prevalence, risk level and risk factors of diabetic foot ulcer among adult individuals with diabetes in the Southeastern Anatolia Region of Turkiye. Journal of tissue viability. 2025 Feb:34(1):100839. doi: 10.1016/j.jtv.2024.12.003. Epub 2024 Dec 9 [PubMed PMID: 39665941]
van Netten JJ, Bus SA, Apelqvist J, Chen P, Chuter V, Fitridge R, Game F, Hinchliffe RJ, Lazzarini PA, Mills J, Monteiro-Soares M, Peters EJG, Raspovic KM, Senneville E, Wukich DK, Schaper NC, International Working Group on the Diabetic Foot. Definitions and criteria for diabetes-related foot disease (IWGDF 2023 update). Diabetes/metabolism research and reviews. 2024 Mar:40(3):e3654. doi: 10.1002/dmrr.3654. Epub 2023 May 15 [PubMed PMID: 37186781]
Musuuza J, Sutherland BL, Kurter S, Balasubramanian P, Bartels CM, Brennan MB. A systematic review of multidisciplinary teams to reduce major amputations for patients with diabetic foot ulcers. Journal of vascular surgery. 2020 Apr:71(4):1433-1446.e3. doi: 10.1016/j.jvs.2019.08.244. Epub 2019 Oct 30 [PubMed PMID: 31676181]
Level 1 (high-level) evidenceRubio JA, Aragón-Sánchez J, Jiménez S, Guadalix G, Albarracín A, Salido C, Sanz-Moreno J, Ruiz-Grande F, Gil-Fournier N, Álvarez J. Reducing major lower extremity amputations after the introduction of a multidisciplinary team for the diabetic foot. The international journal of lower extremity wounds. 2014 Mar:13(1):22-6. doi: 10.1177/1534734614521234. Epub [PubMed PMID: 24659624]
Meloni M, Giurato L, Monge L, Miranda C, Scatena A, Ragghianti B, Silverii GA, Vermigli C, De Cassai A, Volpe A, Tramonta R, Medea G, Bordieri C, Falcone M, Stefanon L, Bernetti A, Cappella C, Gargiulo M, Lorenzoni V, Scevola G, Stabile E, Da Ros R, Murdolo G, Bianchini E, Gaggia F, Gauna C, Romeo F, Apicella M, Mantuano M, Monami M, Uccioli L, Panel of the Italian Guidelines for the Treatment of Diabetic Foot Syndrome and on behalf of SID and AMD. Effect of a multidisciplinary team approach in patients with diabetic foot ulcers on major adverse limb events (MALEs): systematic review and meta-analysis for the development of the Italian guidelines for the treatment of diabetic foot syndrome. Acta diabetologica. 2024 May:61(5):543-553. doi: 10.1007/s00592-024-02246-9. Epub 2024 Mar 10 [PubMed PMID: 38461443]
Level 1 (high-level) evidenceAzhar A, Basheer M, Abdelgawad MS, Roshdi H, Kamel MF. Prevalence of Peripheral Arterial Disease in Diabetic Foot Ulcer Patients and its Impact in Limb Salvage. The international journal of lower extremity wounds. 2023 Sep:22(3):518-523. doi: 10.1177/15347346211027063. Epub 2021 Jun 18 [PubMed PMID: 34142882]
Rümenapf G, Abilmona N, Morbach S, Sigl M. Peripheral Arterial Disease and the Diabetic Foot Syndrome: Neuropathy Makes the Difference! A Narrative Review. Journal of clinical medicine. 2024 Apr 8:13(7):. doi: 10.3390/jcm13072141. Epub 2024 Apr 8 [PubMed PMID: 38610906]
Level 3 (low-level) evidenceVolmer-Thole M, Lobmann R. Neuropathy and Diabetic Foot Syndrome. International journal of molecular sciences. 2016 Jun 10:17(6):. doi: 10.3390/ijms17060917. Epub 2016 Jun 10 [PubMed PMID: 27294922]
Tang WH, Zhao YN, Cheng ZX, Xu JX, Zhang Y, Liu XM. Risk factors for diabetic foot ulcers: A systematic review and meta-analysis. Vascular. 2024 Jun:32(3):661-669. doi: 10.1177/17085381231154805. Epub 2023 Feb 5 [PubMed PMID: 36740805]
Level 1 (high-level) evidenceCrawford F, Cezard G, Chappell FM, Murray GD, Price JF, Sheikh A, Simpson CR, Stansby GP, Young MJ. A systematic review and individual patient data meta-analysis of prognostic factors for foot ulceration in people with diabetes: the international research collaboration for the prediction of diabetic foot ulcerations (PODUS). Health technology assessment (Winchester, England). 2015 Jul:19(57):1-210. doi: 10.3310/hta19570. Epub [PubMed PMID: 26211920]
Level 1 (high-level) evidenceAbbott CA, Carrington AL, Ashe H, Bath S, Every LC, Griffiths J, Hann AW, Hussein A, Jackson N, Johnson KE, Ryder CH, Torkington R, Van Ross ER, Whalley AM, Widdows P, Williamson S, Boulton AJ, North-West Diabetes Foot Care Study. The North-West Diabetes Foot Care Study: incidence of, and risk factors for, new diabetic foot ulceration in a community-based patient cohort. Diabetic medicine : a journal of the British Diabetic Association. 2002 May:19(5):377-84 [PubMed PMID: 12027925]
Boyko EJ, Ahroni JH, Stensel V, Forsberg RC, Davignon DR, Smith DG. A prospective study of risk factors for diabetic foot ulcer. The Seattle Diabetic Foot Study. Diabetes care. 1999 Jul:22(7):1036-42 [PubMed PMID: 10388963]
Bonnet JB, Sultan A. Narrative Review of the Relationship Between CKD and Diabetic Foot Ulcer. Kidney international reports. 2022 Mar:7(3):381-388. doi: 10.1016/j.ekir.2021.12.018. Epub 2021 Dec 21 [PubMed PMID: 35257052]
Level 3 (low-level) evidenceNdip A, Rutter MK, Vileikyte L, Vardhan A, Asari A, Jameel M, Tahir HA, Lavery LA, Boulton AJ. Dialysis treatment is an independent risk factor for foot ulceration in patients with diabetes and stage 4 or 5 chronic kidney disease. Diabetes care. 2010 Aug:33(8):1811-6. doi: 10.2337/dc10-0255. Epub 2010 May 18 [PubMed PMID: 20484126]
Otte J, van Netten JJ, Woittiez AJ. The association of chronic kidney disease and dialysis treatment with foot ulceration and major amputation. Journal of vascular surgery. 2015 Aug:62(2):406-11. doi: 10.1016/j.jvs.2015.02.051. Epub 2015 May 1 [PubMed PMID: 25937604]
Bus SA, Sacco ICN, Monteiro-Soares M, Raspovic A, Paton J, Rasmussen A, Lavery LA, van Netten JJ. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2023 update). Diabetes/metabolism research and reviews. 2024 Mar:40(3):e3651. doi: 10.1002/dmrr.3651. Epub 2023 Jun 11 [PubMed PMID: 37302121]
Boyko EJ, Ahroni JH, Cohen V, Nelson KM, Heagerty PJ. Prediction of diabetic foot ulcer occurrence using commonly available clinical information: the Seattle Diabetic Foot Study. Diabetes care. 2006 Jun:29(6):1202-7 [PubMed PMID: 16731996]
Chen L, Sun S, Gao Y, Ran X. Global mortality of diabetic foot ulcer: A systematic review and meta-analysis of observational studies. Diabetes, obesity & metabolism. 2023 Jan:25(1):36-45. doi: 10.1111/dom.14840. Epub 2022 Sep 4 [PubMed PMID: 36054820]
Level 1 (high-level) evidenceSchaper NC, van Netten JJ, Apelqvist J, Bus SA, Fitridge R, Game F, Monteiro-Soares M, Senneville E, IWGDF Editorial Board. Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes/metabolism research and reviews. 2024 Mar:40(3):e3657. doi: 10.1002/dmrr.3657. Epub 2023 May 27 [PubMed PMID: 37243927]
Level 3 (low-level) evidenceBus SA, Armstrong DG, Crews RT, Gooday C, Jarl G, Kirketerp-Moller K, Viswanathan V, Lazzarini PA. Guidelines on offloading foot ulcers in persons with diabetes (IWGDF 2023 update). Diabetes/metabolism research and reviews. 2024 Mar:40(3):e3647. doi: 10.1002/dmrr.3647. Epub 2023 May 25 [PubMed PMID: 37226568]
Chen L, Chen D, Gong H, Wang C, Gao Y, Li Y, Tang W, Zha P, Ran X. Pedal medial arterial calcification in diabetic foot ulcers: A significant risk factor of amputation and mortality. Journal of diabetes. 2024 Apr:16(4):e13527. doi: 10.1111/1753-0407.13527. Epub [PubMed PMID: 38584152]
Wu X, He W, Mu X, Liu Y, Deng J, Liu Y, Nie X. Macrophage polarization in diabetic wound healing. Burns & trauma. 2022:10():tkac051. doi: 10.1093/burnst/tkac051. Epub 2022 Dec 29 [PubMed PMID: 36601058]
Fu K, Zheng X, Chen Y, Wu L, Yang Z, Chen X, Song W. Role of matrix metalloproteinases in diabetic foot ulcers: Potential therapeutic targets. Frontiers in pharmacology. 2022:13():1050630. doi: 10.3389/fphar.2022.1050630. Epub 2022 Oct 20 [PubMed PMID: 36339630]
Senneville É, Albalawi Z, van Asten SA, Abbas ZG, Allison G, Aragón-Sánchez J, Embil JM, Lavery LA, Alhasan M, Oz O, Uçkay I, Urbančič-Rovan V, Xu ZR, Peters EJG. IWGDF/IDSA guidelines on the diagnosis and treatment of diabetes-related foot infections (IWGDF/IDSA 2023). Diabetes/metabolism research and reviews. 2024 Mar:40(3):e3687. doi: 10.1002/dmrr.3687. Epub 2023 Oct 1 [PubMed PMID: 37779323]
Wang R, Gu S, Kim YH, Lee A, Lin H, Jiang D. Diabetic Wound Repair: From Mechanism to Therapeutic Opportunities. MedComm. 2025 Oct:6(10):e70406. doi: 10.1002/mco2.70406. Epub 2025 Sep 29 [PubMed PMID: 41030912]
Fiordaliso F, Clerici G, Maggioni S, Caminiti M, Bisighini C, Novelli D, Minnella D, Corbelli A, Morisi R, De Iaco A, Faglia E. Prospective study on microangiopathy in type 2 diabetic foot ulcer. Diabetologia. 2016 Jul:59(7):1542-1548. doi: 10.1007/s00125-016-3961-0. Epub 2016 Apr 28 [PubMed PMID: 27121168]
Koreyba K, Silina E, Tsyplakov D, Litvitskiy P, Manturova N, Balkizov Z, Achar RR, Raju NR, Stupin V. Prognostic Value of Histological and Immunohistochemical Data in Diabetic Foot Ulcers. Journal of clinical medicine. 2022 Dec 4:11(23):. doi: 10.3390/jcm11237202. Epub 2022 Dec 4 [PubMed PMID: 36498776]
Lipsky BA, Berendt AR, Cornia PB, Pile JC, Peters EJ, Armstrong DG, Deery HG, Embil JM, Joseph WS, Karchmer AW, Pinzur MS, Senneville E, Infectious Diseases Society of America. 2012 Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2012 Jun:54(12):e132-73. doi: 10.1093/cid/cis346. Epub [PubMed PMID: 22619242]
Level 1 (high-level) evidenceInce P, Abbas ZG, Lutale JK, Basit A, Ali SM, Chohan F, Morbach S, Möllenberg J, Game FL, Jeffcoate WJ. Use of the SINBAD classification system and score in comparing outcome of foot ulcer management on three continents. Diabetes care. 2008 May:31(5):964-7. doi: 10.2337/dc07-2367. Epub 2008 Feb 25 [PubMed PMID: 18299441]
Mills JL Sr, Conte MS, Armstrong DG, Pomposelli FB, Schanzer A, Sidawy AN, Andros G, Society for Vascular Surgery Lower Extremity Guidelines Committee. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: risk stratification based on wound, ischemia, and foot infection (WIfI). Journal of vascular surgery. 2014 Jan:59(1):220-34.e1-2. doi: 10.1016/j.jvs.2013.08.003. Epub 2013 Oct 12 [PubMed PMID: 24126108]
Chen H, Mei S, Zhou Y, Dai J. Systematic review and meta-analysis of the diagnostic accuracy of inflammatory markers for infected diabetic foot ulcer. Journal of tissue viability. 2024 Nov:33(4):598-607. doi: 10.1016/j.jtv.2024.09.007. Epub 2024 Sep 26 [PubMed PMID: 39358181]
Level 1 (high-level) evidenceSharma H, Sharma S, Krishnan A, Yuan D, Vangaveti VN, Malabu UH, Haleagrahara N. The efficacy of inflammatory markers in diagnosing infected diabetic foot ulcers and diabetic foot osteomyelitis: Systematic review and meta-analysis. PloS one. 2022:17(4):e0267412. doi: 10.1371/journal.pone.0267412. Epub 2022 Apr 27 [PubMed PMID: 35476639]
Level 1 (high-level) evidenceWang W, Zhou P, Nie X, Hua Q. Procalcitonin and Diabetic Foot Ulcer Infections: A Meta-Analysis. Endocrinology, diabetes & metabolism. 2025 Jul:8(4):e70066. doi: 10.1002/edm2.70066. Epub [PubMed PMID: 40653844]
Level 1 (high-level) evidenceCritchley JA, Carey IM, Harris T, DeWilde S, Hosking FJ, Cook DG. Glycemic Control and Risk of Infections Among People With Type 1 or Type 2 Diabetes in a Large Primary Care Cohort Study. Diabetes care. 2018 Oct:41(10):2127-2135. doi: 10.2337/dc18-0287. Epub 2018 Aug 13 [PubMed PMID: 30104296]
Caruso P, Scappaticcio L, Gicchino M, Castaldo F, Barrasso M, Carbone C, Caputo M, Tomasuolo M, Paglionico VA, Bellastella G, Maiorino MI, Esposito K. Short-term glucose variability as a determinant of the healing rate of diabetic foot ulcer: A retrospective study. Diabetes & metabolic syndrome. 2024 Mar:18(3):102990. doi: 10.1016/j.dsx.2024.102990. Epub 2024 Mar 16 [PubMed PMID: 38508037]
Level 2 (mid-level) evidenceLlewellyn A, Kraft J, Holton C, Harden M, Simmonds M. Imaging for detection of osteomyelitis in people with diabetic foot ulcers: A systematic review and meta-analysis. European journal of radiology. 2020 Oct:131():109215. doi: 10.1016/j.ejrad.2020.109215. Epub 2020 Aug 13 [PubMed PMID: 32862106]
Level 1 (high-level) evidenceConte MS, Bradbury AW, Kolh P, White JV, Dick F, Fitridge R, Mills JL, Ricco JB, Suresh KR, Murad MH, Aboyans V, Aksoy M, Alexandrescu VA, Armstrong D, Azuma N, Belch J, Bergoeing M, Bjorck M, Chakfé N, Cheng S, Dawson J, Debus ES, Dueck A, Duval S, Eckstein HH, Ferraresi R, Gambhir R, Gargiulo M, Geraghty P, Goode S, Gray B, Guo W, Gupta PC, Hinchliffe R, Jetty P, Komori K, Lavery L, Liang W, Lookstein R, Menard M, Misra S, Miyata T, Moneta G, Munoa Prado JA, Munoz A, Paolini JE, Patel M, Pomposelli F, Powell R, Robless P, Rogers L, Schanzer A, Schneider P, Taylor S, De Ceniga MV, Veller M, Vermassen F, Wang J, Wang S, GVG Writing Group for the Joint Guidelines of the Society for Vascular Surgery (SVS), European Society for Vascular Surgery (ESVS), and World Federation of Vascular Societies (WFVS). Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2019 Jul:58(1S):S1-S109.e33. doi: 10.1016/j.ejvs.2019.05.006. Epub 2019 Jun 8 [PubMed PMID: 31182334]
Gornik HL, Aronow HD, Goodney PP, Arya S, Brewster LP, Byrd L, Chandra V, Drachman DE, Eaves JM, Ehrman JK, Evans JN, Getchius TSD, Gutiérrez JA, Hawkins BM, Hess CN, Ho KJ, Jones WS, Kim ESH, Kinlay S, Kirksey L, Kohlman-Trigoboff D, Long CA, Pollak AW, Sabri SS, Sadwin LB, Secemsky EA, Serhal M, Shishehbor MH, Treat-Jacobson D, Wilkins LR, Peer Review Committee Members. 2024 ACC/AHA/AACVPR/APMA/ABC/SCAI/SVM/SVN/SVS/SIR/VESS Guideline for the Management of Lower Extremity Peripheral Artery Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024 Jun 11:149(24):e1313-e1410. doi: 10.1161/CIR.0000000000001251. Epub 2024 May 14 [PubMed PMID: 38743805]
Level 1 (high-level) evidenceLázaro-Martínez JL, Aragón-Sánchez J, García-Morales E. Antibiotics versus conservative surgery for treating diabetic foot osteomyelitis: a randomized comparative trial. Diabetes care. 2014:37(3):789-95. doi: 10.2337/dc13-1526. Epub 2013 Oct 15 [PubMed PMID: 24130347]
Level 1 (high-level) evidenceMervis JS, Phillips TJ. Pressure ulcers: Pathophysiology, epidemiology, risk factors, and presentation. Journal of the American Academy of Dermatology. 2019 Oct:81(4):881-890. doi: 10.1016/j.jaad.2018.12.069. Epub 2019 Jan 18 [PubMed PMID: 30664905]
Papi M, Papi C. Vasculitic Ulcers. The international journal of lower extremity wounds. 2016 Mar:15(1):6-16. doi: 10.1177/1534734615621220. Epub 2015 Dec 11 [PubMed PMID: 26657344]
Shanmugam VK, Angra D, Rahimi H, McNish S. Vasculitic and autoimmune wounds. Journal of vascular surgery. Venous and lymphatic disorders. 2017 Mar:5(2):280-292. doi: 10.1016/j.jvsv.2016.09.006. Epub 2016 Dec 14 [PubMed PMID: 28214498]
Marzuk Z, Homsi Y, Moshiri AS, Karagounis TK. Pyoderma gangrenosum-like ulcer association in small vessel vasculitis (Vasculitis presenting as pyoderma gangrenosum-like ulcer). The American journal of the medical sciences. 2025 Nov:370(5):483-485. doi: 10.1016/j.amjms.2025.08.006. Epub 2025 Aug 5 [PubMed PMID: 40759365]
Xie T, Ye J, Rerkasem K, Mani R. The venous ulcer continues to be a clinical challenge: an update. Burns & trauma. 2018:6():18. doi: 10.1186/s41038-018-0119-y. Epub 2018 Jun 15 [PubMed PMID: 29942813]
Hashemi DA, Brown-Joel ZO, Tkachenko E, Nelson CA, Noe MH, Imadojemu S, Vleugels RA, Mostaghimi A, Wanat KA, Rosenbach M. Clinical Features and Comorbidities of Patients With Necrobiosis Lipoidica With or Without Diabetes. JAMA dermatology. 2019 Apr 1:155(4):455-459. doi: 10.1001/jamadermatol.2018.5635. Epub [PubMed PMID: 30785603]
Barnes JA, Eid MA, Creager MA, Goodney PP. Epidemiology and Risk of Amputation in Patients With Diabetes Mellitus and Peripheral Artery Disease. Arteriosclerosis, thrombosis, and vascular biology. 2020 Aug:40(8):1808-1817. doi: 10.1161/ATVBAHA.120.314595. Epub 2020 Jun 25 [PubMed PMID: 32580632]
Luo Y, Liu C, Li C, Jin M, Pi L, Jin Z. The incidence of lower extremity amputation and its associated risk factors in patients with diabetic foot ulcers: A meta-analysis. International wound journal. 2024 Jul:21(7):e14931. doi: 10.1111/iwj.14931. Epub [PubMed PMID: 38972836]
Level 1 (high-level) evidenceBrennan MB, Hess TM, Bartle B, Cooper JM, Kang J, Huang ES, Smith M, Sohn MW, Crnich C. Diabetic foot ulcer severity predicts mortality among veterans with type 2 diabetes. Journal of diabetes and its complications. 2017 Mar:31(3):556-561. doi: 10.1016/j.jdiacomp.2016.11.020. Epub 2016 Dec 10 [PubMed PMID: 27993523]
Chin BZ, Lee P, Sia CH, Hong CC. Diabetic foot ulcer is associated with cardiovascular-related mortality and morbidity - a systematic review and meta-analysis of 8062 patients. Endocrine. 2024 Jun:84(3):852-863. doi: 10.1007/s12020-024-03696-5. Epub 2024 Jan 27 [PubMed PMID: 38280983]
Level 1 (high-level) evidenceArmstrong DG, Tan TW, Boulton AJM, Bus SA. Diabetic Foot Ulcers: A Review. JAMA. 2023 Jul 3:330(1):62-75. doi: 10.1001/jama.2023.10578. Epub [PubMed PMID: 37395769]
Giurato L, Meloni M, Izzo V, Uccioli L. Osteomyelitis in diabetic foot: A comprehensive overview. World journal of diabetes. 2017 Apr 15:8(4):135-142. doi: 10.4239/wjd.v8.i4.135. Epub [PubMed PMID: 28465790]
Level 3 (low-level) evidenceNather A, Bee CS, Huak CY, Chew JL, Lin CB, Neo S, Sim EY. Epidemiology of diabetic foot problems and predictive factors for limb loss. Journal of diabetes and its complications. 2008 Mar-Apr:22(2):77-82. doi: 10.1016/j.jdiacomp.2007.04.004. Epub [PubMed PMID: 18280436]
Twine CP, Kakkos SK, Aboyans V, Baumgartner I, Behrendt CA, Bellmunt-Montoya S, Jilma B, Nordanstig J, Saratzis A, Reekers JA, Zlatanovic P, ESVS Guidelines Committee, Antoniou GA, de Borst GJ, Bastos Gonçalves F, Chakfé N, Coscas R, Dias NV, Hinchliffe RJ, Kolh P, Lindholt JS, Mees BME, Resch TA, Trimarchi S, Tulamo R, Vermassen FEG, Wanhainen A, Document Reviewers, Koncar I, Fitridge R, Matsagkas M, Valgimigli M. Editor's Choice - European Society for Vascular Surgery (ESVS) 2023 Clinical Practice Guidelines on Antithrombotic Therapy for Vascular Diseases. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2023 May:65(5):627-689. doi: 10.1016/j.ejvs.2023.03.042. Epub 2023 Apr 3 [PubMed PMID: 37019274]
Level 1 (high-level) evidenceArmstrong DG, Lavery LA, Diabetic Foot Study Consortium. Negative pressure wound therapy after partial diabetic foot amputation: a multicentre, randomised controlled trial. Lancet (London, England). 2005 Nov 12:366(9498):1704-10 [PubMed PMID: 16291063]
Level 1 (high-level) evidenceMarso SP, Bain SC, Consoli A, Eliaschewitz FG, Jódar E, Leiter LA, Lingvay I, Rosenstock J, Seufert J, Warren ML, Woo V, Hansen O, Holst AG, Pettersson J, Vilsbøll T, SUSTAIN-6 Investigators. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. The New England journal of medicine. 2016 Nov 10:375(19):1834-1844 [PubMed PMID: 27633186]
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, Broedl UC, Inzucchi SE, EMPA-REG OUTCOME Investigators. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. The New England journal of medicine. 2015 Nov 26:373(22):2117-28. doi: 10.1056/NEJMoa1504720. Epub 2015 Sep 17 [PubMed PMID: 26378978]
Coppola A, Montalcini T, Gallotti P, Ferrulli A, Pujia A, Luzi L, Gazzaruso C. A Comprehensive Therapeutic Patient Education May Improve Wound Healing and Reduce Ulcer Recurrence and Mortality in Persons With Type 2 Diabetes. Canadian journal of diabetes. 2023 Feb:47(1):73-77. doi: 10.1016/j.jcjd.2022.08.004. Epub 2022 Aug 23 [PubMed PMID: 36154986]